
Right-to-Left Shunt in Divers with Neurological Decompression Sickness: A Systematic Review and Meta-Analysis
 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Methods
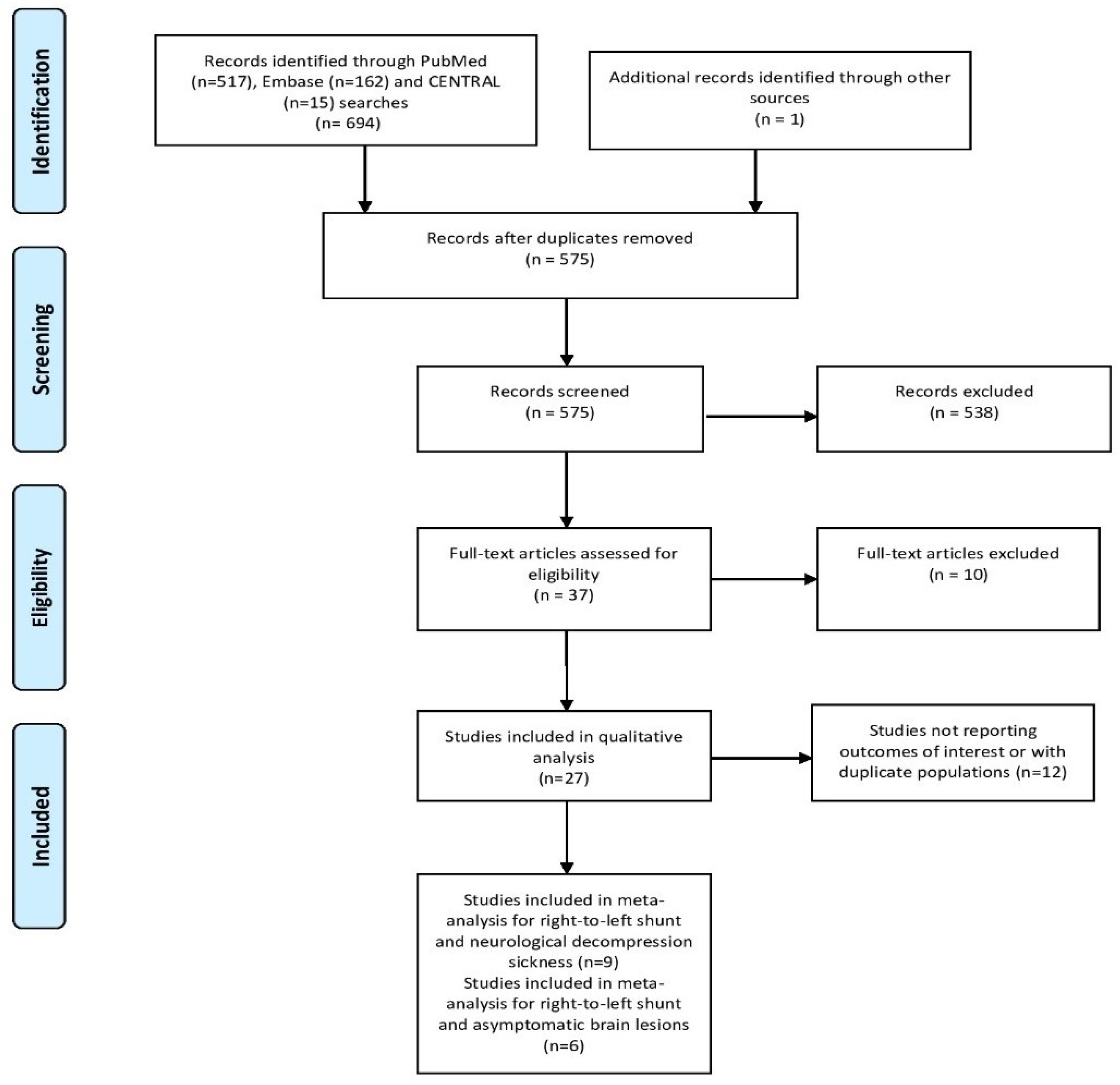
2.1. Literature Search
2.2. Data Extraction and Outcome Measures
2.3. Risk of Bias Assessment
2.4. Statistical Analysis
3. Results
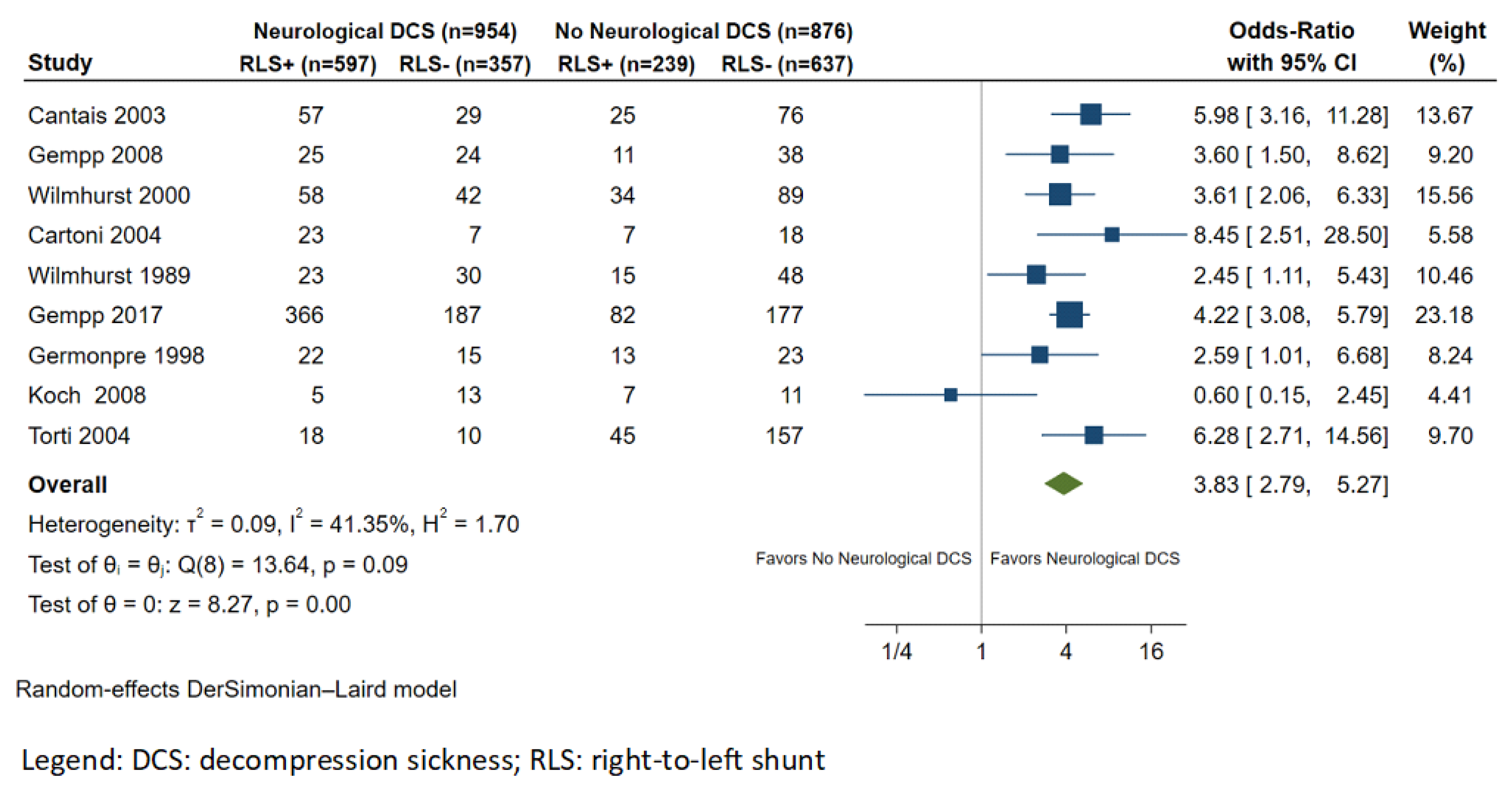
3.1. RLS and Neurological DCS
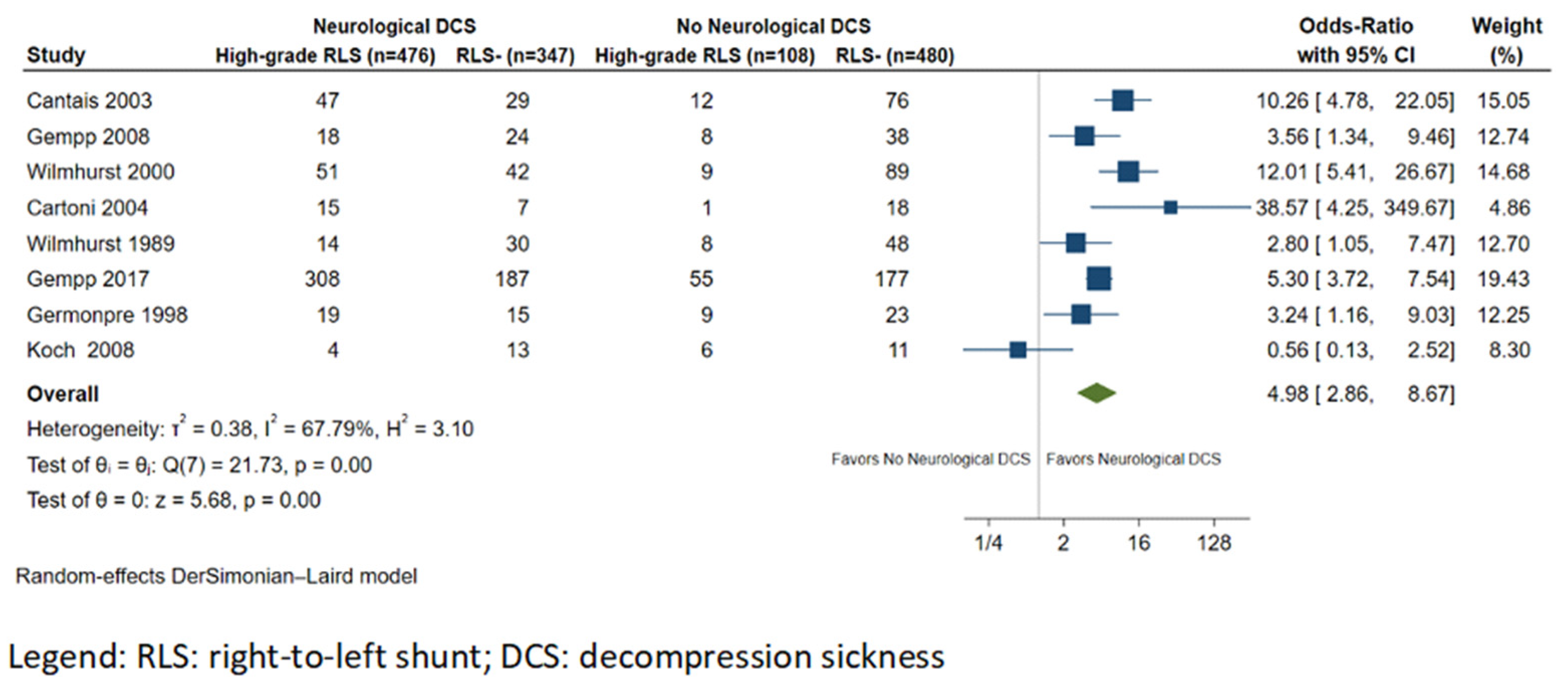
3.2. RLS Size and Neurological DCS
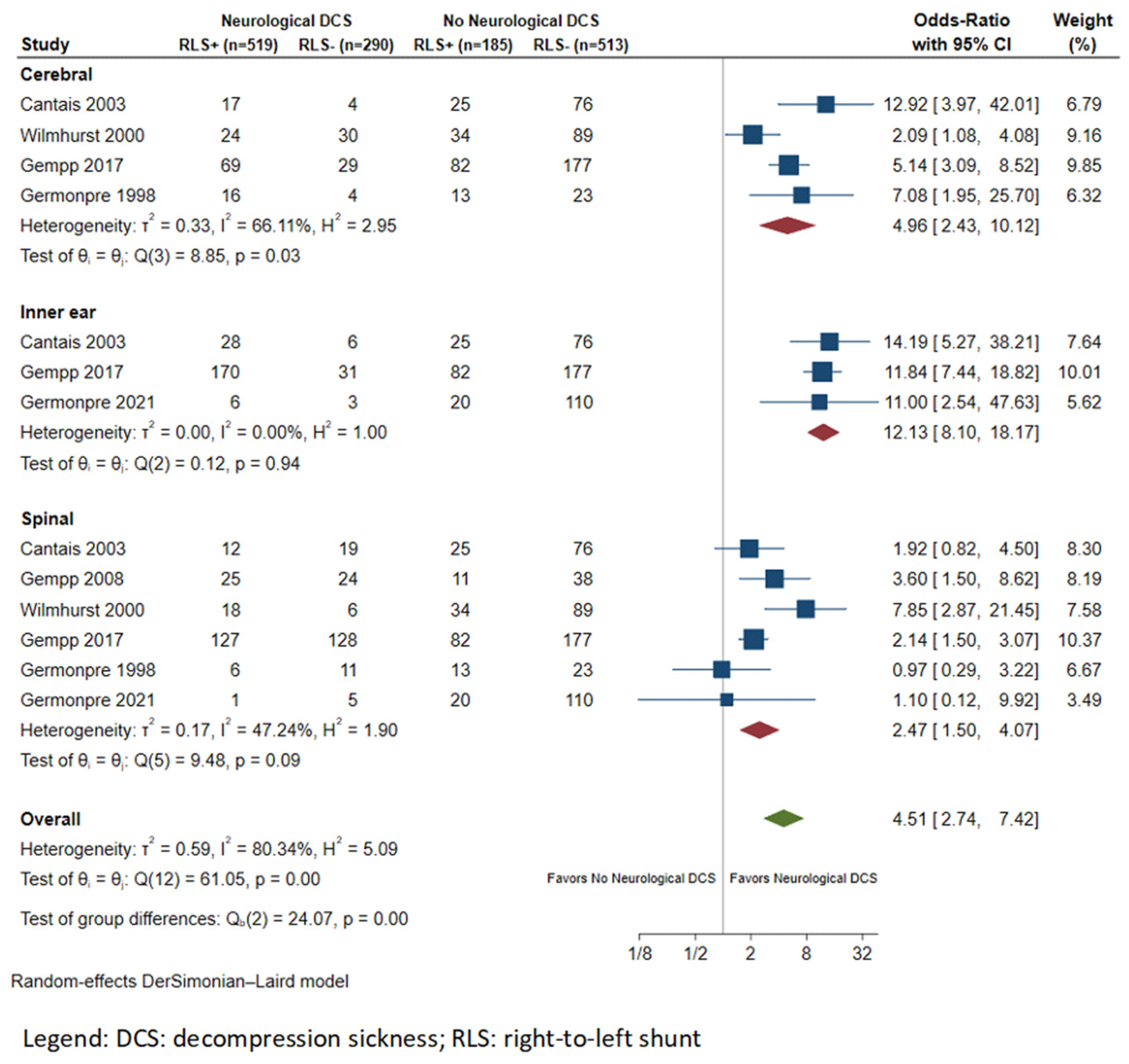
3.3. Subgroup Analysis
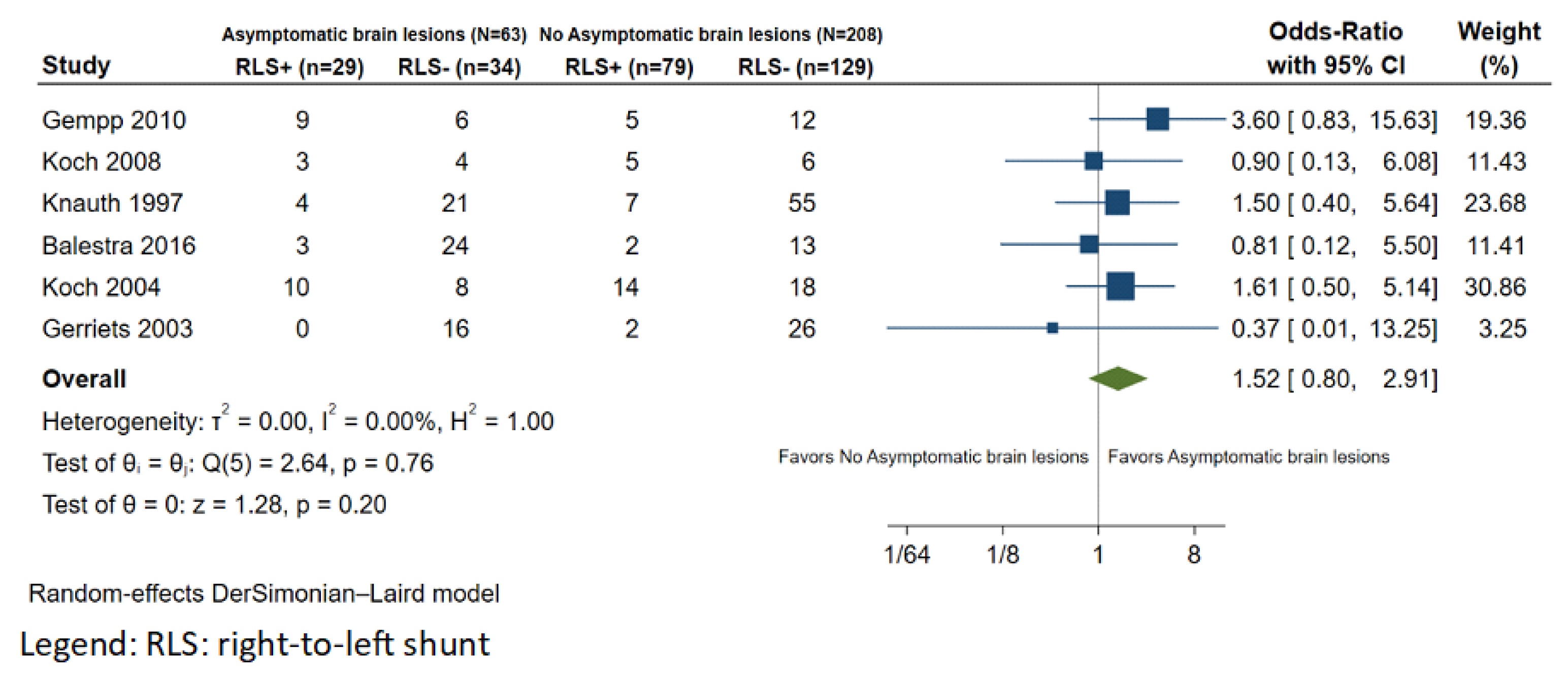
3.4. RLS and Asymptomatic Brain Lesions
3.5. Summary of Observational Data
4. Discussion
4.1. RLS and Neurological DCS
4.2. RLS and Asymptomatic Brain Lesions
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Palaiodimos, L.; Mahato, P.; Gershon, A.; Faillace, R.T. Less Recognized Conditions Associated with PFO: Decompression Illness, Carcinoid Heart Disease, Coronary Spasm. In Patent Foramen Ovale Closure for Stroke, Myocardial Infarction, Peripheral Embolism, Migraine, and Hypoxemia; Mojadidi, M.K., Meier, B., Tobis, J.M., Eds.; Academic Press: Cambridge, MA, USA, 2020; Chapter 13; pp. 155–167. [Google Scholar] [CrossRef]
- Vann, R.D.; Butler, F.K.; Mitchell, S.J.; Moon, R.E. Decompression illness. Lancet 2011, 377, 153–164. [Google Scholar] [CrossRef] [PubMed]
- Cooper, J.S.; Hanson, K.C. Decompression Sickness; StatPearls: Treasure Island, FL, USA, 2021. [Google Scholar]
- Honěk, J.; Šefc, L.; Honěk, T.; Šrámek, M.; Horváth, M.; Veselka, J. Patent Foramen Ovale in Recreational and Professional Divers: An Important and Largely Unrecognized Problem. Can. J. Cardiol. 2015, 31, 1061–1066. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, S.J.; Bennett, M.H.; Moon, R.E. Decompression Sickness and Arterial Gas Embolism. N. Engl. J. Med. 2022, 386, 1254–1264. [Google Scholar] [CrossRef]
- Newton, H.B. Neurologic complications of scuba diving. Am. Fam. Physician 2001, 63, 2211–2218. [Google Scholar] [PubMed]
- Greer, H.D.; Massey, E.W. Neurologic Injury from Undersea Diving. Neurol. Clin. 1992, 10, 1031–1045. [Google Scholar] [CrossRef]
- Van Hulst, R.A.; Klein, J.; Lachmann, B. Gas embolism: Pathophysiology and treatment. Clin. Physiol. Funct. Imaging 2003, 23, 237–246. [Google Scholar] [CrossRef]
- Favilla, C.G.; Messé, S.R. Patent foramen ovale and stroke: Current evidence and treatment options. Curr. Opin. Neurol. 2020, 33, 10–16. [Google Scholar] [CrossRef]
- Palaiodimos, L.; Kokkinidis, D.G.; Faillace, R.T.; Foley, T.R.; Dangas, G.D.; Price, M.J.; Mastoris, I. Percutaneous closure of patent foramen ovale vs. medical treatment for patients with history of cryptogenic stroke: A systematic review and meta-analysis of randomized controlled trials. Cardiovasc. Revasculariz. Med. 2018, 19, 852–858. [Google Scholar] [CrossRef]
- Klingmann, C.; Praetorius, M.; Baumann, I.; Plinkert, P.K. Barotrauma and Decompression Illness of the Inner Ear. Otol. Neurotol. 2007, 28, 447–454. [Google Scholar] [CrossRef]
- Cantais, E.; Louge, P.; Suppini, A.; Foster, P.P.; Palmier, B. Right-to-left shunt and risk of decompression illness with cochleovestibular and cerebral symptoms in divers: Case control study in 101 consecutive dive accidents. Crit. Care Med. 2003, 31, 84–88. [Google Scholar] [CrossRef]
- Dardeau, M.R.; Pollock, N.W.; McDonald, C.M.; Lang, M.A. The incidence of decompression illness in 10 years of scientific diving. Diving Hyperb. Med. J. 2012, 42, 195–200. [Google Scholar]
- Meissner, I.; Khandheria, B.K.; Heit, J.A.; Petty, G.W.; Sheps, S.G.; Schwartz, G.L.; Whisnant, J.P.; Wiebers, D.O.; Covalt, J.L.; Petterson, T.M.; et al. Patent Foramen Ovale: Innocent or Guilty? Evidence from a Prospective Population-Based Study. J. Am. Coll. Cardiol. 2006, 47, 440–445. [Google Scholar] [CrossRef] [PubMed]
- Palaiodimos, L.; Kokkinidis, D.G. Questions on Percutaneous Patent Foramen Ovale Closure for Secondary Stroke Prevention: The Heads of the Lernaean Hydra. Cardiology 2019, 144, 50–52. [Google Scholar] [CrossRef] [PubMed]
- Schwerzmann, M.; Seiler, C.; Lipp, E.; Guzman, R.; Lövblad, K.O.; Kraus, M.; Kucher, N. Relation between directly detected patent foramen ovale and ischemic brain lesions in sport divers. Ann. Intern. Med. 2001, 134, 21–24. [Google Scholar] [CrossRef]
- Gerriets, T.; Tetzlaff, K.; Hutzelmann, A.; Liceni, T.; Kopiske, G.; Struck, N.; Reuter, M.; Kaps, M. Association between right-to-left shunts and brain lesions in sport divers. Aviat. Space Environ. Med. 2003, 74, 1058–1060. [Google Scholar]
- Koch, A.E.; Kampen, J.; Tetzlaff, K.; Reuter, M.; McCormack, P.; Schnoor, P.W.; Struck, N.; Heine, L.; Prytulla, I.; Rieckert, H. Incidence of abnormal cerebral findings in the MRI of clinically healthy divers: Role of a patent foramen ovale. Undersea Hyperb. Med. 2004, 31, 261–268. [Google Scholar] [PubMed]
- Balestra, C.; Germonpre, P. Correlation between Patent Foramen Ovale, Cerebral “Lesions” and Neuropsychometric Testing in Experienced Sports Divers: Does Diving Damage the Brain? Front. Psychol. 2016, 7, 696. [Google Scholar] [CrossRef]
- UHMS. UHMS Best Practice Guidelines Prevention and Treatment of Decompression Sickness and Arterial Gas Embolism. 2011, pp. 1–17. Available online: https://www.uhms.org/images/DCS-AGE-Committee/dcsandage_prevandmgt_uhms-fi.pdf (accessed on 6 September 2021).
- Moon, R.E.; Mitchell, S. Hyperbaric treatment for decompression sickness: Current recommendations. Undersea Hyperb. Med. 2019, 46, 685–693. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Healthcare Interventions: Explanation and Elaboration. BMJ (Clin. Res. Ed.) 2009, 339, b2700. [Google Scholar] [CrossRef]
- Hayden, J.A.; Van Der Windt, D.A.; Cartwright, J.L.; Côté, P.; Bombardier, C. Assessing Bias in Studies of Prognostic Factors. Ann. Intern. Med. 2013, 158, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Der Simonian, R.; Laird, N. Meta-analysis in clinical trials revisited. Contemp. Clin. Trials 2015, 45, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Germonpré, P.; Dendale, P.; Unger, P.; Balestra, C. Patent foramen ovale and decompression sickness in sports divers. J. Appl. Physiol. 1998, 84, 1622–1626. [Google Scholar] [CrossRef] [PubMed]
- Torti, S.R.; Billinger, M.; Schwerzmann, M.; Vogel, R.; Zbinden, R.; Windecker, S.; Seiler, C. Risk of decompression illness among 230 divers in relation to the presence and size of patent foramen ovale. Eur. Heart J. 2004, 25, 1014–1020. [Google Scholar] [CrossRef]
- Liou, K.; Wolfers, D.; Turner, R.; Bennett, M.; Allan, R.; Jepson, N.; Cranney, G. Patent Foramen Ovale Influences the Presentation of Decompression Illness in SCUBA Divers. Heart Lung Circ. 2015, 24, 26–31. [Google Scholar] [CrossRef]
- Gempp, E.; Sbardella, F.; Stephant, E.; Constantin, P.; De Maistre, S.; Louge, P.; Blatteau, J.-E. Brain MRI signal abnormalities and right-to-left shunting in asymptomatic military divers. Aviat. Space Environ. Med. 2010, 81, 1008–1012. [Google Scholar] [CrossRef]
- Knauth, M.; Ries, S.; Pohimann, S.; Kerby, T.; Forsting, M.; Daffertshofer, M.; Hennerici, M.; Sartor, K. Cohort study of multiple brain lesions in sport divers: Role of a patent foramen ovale. BMJ 1997, 314, 701. [Google Scholar] [CrossRef]
- Germonpré, P.; Lafère, P.; Portier, W.; Germonpré, F.-L.; Marroni, A.; Balestra, C. Increased Risk of Decompression Sickness When Diving With a Right-to-Left Shunt: Results of a Prospective Single-Blinded Observational Study (The “Carotid Doppler” Study). Front. Physiol. 2021, 12, 763408. [Google Scholar] [CrossRef]
- Cartoni, D.; De Castro, S.; Valente, G.; Costanzo, C.; Pelliccia, A.; Beni, S.; Di Angelantonio, E.; Papetti, F.; Serdoz, L.V.; Fedele, F. Identification of professional scuba divers with patent foramen ovale at risk for decompression illness. Am. J. Cardiol. 2004, 94, 270–273. [Google Scholar] [CrossRef]
- Gempp, E.; Blatteau, J.; Stephant, E.; Louge, P. Relation Between Right-to-Left Shunts and Spinal Cord Decompression Sickness in Divers. Int. J. Sports Med. 2009, 30, 150–153. [Google Scholar] [CrossRef]
- Gempp, E.; Lyard, M.; Louge, P. Reliability of right-to-left shunt screening in the prevention of scuba diving related-decompression sickness. Int. J. Cardiol. 2017, 248, 155–158. [Google Scholar] [CrossRef]
- Koch, E.A.; Kirsch, H.; Reuter, M.; Warninghoff, V.; Rieckert, H.; Deuschl, G. Prevalence of patent foramen ovale (PFO) and MRI-lesions in mild neurological decompression sickness (type B-DCS/AGE). Undersea Hyperb. Med. 2008, 35, 197–205. [Google Scholar] [PubMed]
- Wilmshurst, P.; Bryson, P. Relationship between the clinical features of neurological decompression illness and its causes. Clin. Sci. 2000, 99, 65–75. [Google Scholar] [CrossRef]
- Wilmshurst, P.; Byrne, J.; Webb-Peploe, M. Relation between interatrial shunts and decompression sickness in divers. Lancet 1989, 334, 1302–1306. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Gempp, E.; Louge, P. Inner ear decompression sickness in scuba divers: A review of 115 cases. Eur. Arch. Oto-Rhino-Laryngol. 2013, 270, 1831–1837. [Google Scholar] [CrossRef]
- Ignatescu, M.; Bryson, P.; Klingmann, C. Susceptibility of the inner ear structure to shunt-related decompression sickness. Aviat. Space Environ. Med. 2012, 83, 1145–1151. [Google Scholar] [CrossRef]
- Klingmann, C.; Benton, P.J.; Ringleb, P.A.; Knauth, M. Embolic Inner Ear Decompression Illness: Correlation with a Right-to-Left Shunt. Laryngoscope 2003, 113, 1356–13611. [Google Scholar] [CrossRef]
- Klingmann, C. Inner ear decompression sickness in compressed-air diving. Undersea Hyperb. Med. 2012, 39, 589–594. [Google Scholar]
- Harrah, J.D.; O’Boyle, P.S.; Piantadosi, C.A. Underutilization of echocardiography for patent foramen ovale in divers with serious decompression sickness. Undersea Hyperb. Med. 2008, 35, 207–211. [Google Scholar]
- Guenzani, S.; Mereu, D.; Messersmith, M.; Olivari, D.; Arena, M.; Spanò, A. Inner-ear decompression sickness in nine trimix recreational divers. Diving Hyperb. Med. 2016, 46, 111–116. [Google Scholar] [PubMed]
- Lafère, P.; Balestra, C.; Caers, D.; Germonpré, P. Patent Foramen Ovale (PFO), Personality Traits, and Iterative Decompression Sickness. Retrospective Analysis of 209 Cases. Front. Psychol. 2017, 8, 1328. [Google Scholar] [CrossRef] [PubMed]
- Moon, R.E.; Camporesi, E.M.; Kisslo, J.A. Patient foramen ovale and decompression sickness in divers. Lancet 1989, 1, 513–514. Available online: https://www.embase.com/search/results?subaction=viewrecord&id=L19075203&from=export (accessed on 6 September 2021). [CrossRef]
- Kerut, E.K.; Truax, W.D.; Borreson, T.E.; Van Meter, K.W.; Given, M.B.; Giles, T.D. Detection of Right to Left Shunts in Decompression Sickness in Divers. Am. J. Cardiol. 1997, 79, 377–378. [Google Scholar] [CrossRef] [PubMed]
- Lairez, O.; Cournot, M.; Minville, V.; Roncalli, J.; Austruy, J.; Elbaz, M.; Galinier, M.; Carrié, D. Risk of Neurological Decompression Sickness in the Diver with a Right-to-Left Shunt: Literature Review and Meta-Analysis. Clin. J. Sport Med. 2009, 19, 231–235. [Google Scholar] [CrossRef]
- Billinger, M.; Zbinden, R.; Mordasini, R.; Windecker, S.; Schwerzmann, M.; Meier, B.; Seiler, C. Patent foramen ovale closure in recreational divers: Effect on decompression illness and ischaemic brain lesions during long-term follow-up. Heart 2011, 97, 1932–1937. [Google Scholar] [CrossRef]
- Henzel, J.; Rudziński, P.N.; Kłopotowski, M.; Konka, M.; Dzielińska, Z.; Demkow, M. Transcatheter closure of patent foramen ovale for the secondary prevention of decompression illness in professional divers: A single-centre experience with long-term follow-up. Kardiol. Pol. 2018, 76, 153–157. [Google Scholar] [CrossRef]
- Pearman, A.; Bugeja, L.; Nelson, M.; Szantho, G.V.; Turner, M. An audit of persistent foramen ovale closure in 105 divers. Diving Hyperb. Med. J. 2015, 45, 94–97. [Google Scholar]
- Abdelfattah, O.M.; Sayed, A.; Elgendy, I.Y.; Munir, M.; Saleh, Y.; Kapadia, S.R.; Abela, G.S.; Jneid, H. Patent Foramen Ovale Closure and Decompression Sickness among Divers. Cardiovasc. Revasc. Med. 2021, 40, 160–162. [Google Scholar] [CrossRef]
- Honěk, J.; Šrámek, M.; Šefc, L.; Januška, J.; Fiedler, J.; Horváth, M.; Tomek, A.; Novotný, Š.; Honěk, T.; Veselka, J. Effect of Catheter-Based Patent Foramen Ovale Closure on the Occurrence of Arterial Bubbles in Scuba Divers. JACC Cardiovasc. Interv. 2014, 7, 403–408. [Google Scholar] [CrossRef]
- Marabotti, C.; Scalzini, A.; Menicucci, D.; Passera, M.; Bedini, R.; L’Abbate, A. Cardiovascular changes during SCUBA diving: An underwater Doppler echocardiographic study. Acta Physiol. 2013, 209, 62–68. [Google Scholar] [CrossRef]
- Mojadidi, M.K.; Christia, P.; Salamon, J.; Liebelt, J.; Zaman, T.; Gevorgyan, R.; Nezami, N.; Mojaddedi, S.; Elgendy, I.Y.; Tobis, J.M.; et al. Patent foramen ovale: Unanswered questions. Eur. J. Intern. Med. 2015, 26, 743–751. [Google Scholar] [CrossRef]
- Gempp, E.; Louge, P.; Blatteau, J.E.; Hugon, M. Risks factors for recurrent neurological decompression sickness in recreational divers: A case-control study. J. Sports Med. Phys. Fit. 2012, 52, 530–536. [Google Scholar]
- Wilmshurst, P.T.; Morrison, W.L.; Walsh, K.P. Comparison of the size of persistent foramen ovale and atrial septal defects in divers with shunt-related decompression illness and in the general population. Diving Hyperb. Med. J. 2015, 45, 89–93. [Google Scholar]
- Mitchell, S.J.; Doolette, D.J. Pathophysiology of inner ear decompression sickness: Potential role of the persistent foramen ovale. Diving Hyperb. Med. J. 2015, 45, 105–110. [Google Scholar]
- Rozycki, S.W.; Brown, M.J.; Camacho, M. Inner ear barotrauma in divers: An evidence-based tool for evaluation and treatment. Diving Hyperb. Med. J. 2018, 48, 186–193. [Google Scholar] [CrossRef]
- Erdem, I.; Yildiz, S.; Uzun, G.; Sonmez, G.; Senol, M.G.; Mutluoglu, M.; Mutlu, H.; Oner, B. Cerebral white-matter lesions in asymptomatic military divers. Aviat. Space, Environ. Med. 2009, 80, 2–4. [Google Scholar] [CrossRef]
- Cordes, P.; Keil, R.; Bartsch, T.; Tetzlaff, K.; Reuter, M.; Hutzelmann, A.; Friege, L.; Meyer, T.; Bettinghausen, E.; Deuschl, G. Neurologic outcome of controlled compressed-air diving. Neurology 2000, 55, 1743–1746. [Google Scholar] [CrossRef] [PubMed]
- Todnem, K.; Skeidsvoll, H.; Svihus, R.; Rinck, P.; Riise, T.; Kambestad, B.; Aarli, J. Electroencephalography, evoked potentials and MRI brain scans in saturation divers. An epidemiological study. Electroencephalogr. Clin. Neurophysiol. 1991, 79, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Hutzelmann, A.; Tetzlaff, K.; Reuter, M.; Müller-Hülsbeck, S.; Heller, M. Does diving damage the brain? MR control study of divers’ central nervous system. Acta Radiol. 2000, 41, 18–21. [Google Scholar] [CrossRef]
- Connolly, D.M.; Lee, V.M. Odds Ratio Meta-Analysis and Increased Prevalence of White Matter Injury in Healthy Divers. Aerosp. Med. Hum. Perform. 2015, 86, 928–935. [Google Scholar] [CrossRef] [PubMed]
- Gempp, E.; Louge, P.; Soulier, B.; Alla, P. Cerebellar infarction presenting as inner ear decompression sickness following scuba diving: A case report. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2014, 131, 313–315. [Google Scholar] [CrossRef] [PubMed]
- Smart, D.; Mitchell, S.; Wilmshurst, P.; Turner, M.; Banham, N. Joint position statement on persistent foramen ovale (PFO) and diving. South Pacific Underwater Medicine Society (SPUMS) and the United Kingdom Sports Diving Medical Committee (UKSDMC). Diving Hyperb. Med. 2015, 45, 129–131. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Author, Year) | NDCS Group, N | No NDCS Group, N | Professional Divers | Age, Years | Males, % | N of Dives | Depth of Diving (m) | Diving Experience, Years | NDCS Type | Predisposing Factors for NDCS (N) |
|---|---|---|---|---|---|---|---|---|---|---|
| Case–control studies | ||||||||||
| Cantais, 2003 | 86 (101 DCS patients) | 101 | Ν/A | 35 ± 10.3 (all DCS patients) a 33 ± 9.3 (no NDCS) a | 84.1 (all DCS patients) 76.2 (no NDCS) | N/A | >30 m (n = 63) (NDCS group) | Ν/A | Cerebral (21) Spinal (31) Inner ear (34) | Table limits violations (46) |
| Gempp, 2008 | 49 | 49 | N/A | 46 ± 12 (NDCS) a 41 ± 7 (no NDCS) a | 77.6 (NDCS) 84.7 (no NDCS) | N/A | 40 ± 11 (NDCS group)a | N/A | Spinal (49) | No |
| Wilmshurst, 2000 | 100 | 123 | 9 (NDCS group) | N/A | 66 (NDCS) | N/A | N/A | N/A | Cerebral (54) Spinal (24) Combined (14) Indeterminate (8) | Lung disease, rapid ascent, missed deco stops (30) (PFO−) No (PFO+) |
| Wilmshurst, 1989 | 53 (61 DCS patients) | 63 | 2 (DCS patients) 0 (no NDCS) | Ν/A | 77.4 (NDCS) 80.3 (no NDCS) | Ν/A | N/A | N/A | Ν/A | Rapid ascent, missed deco stop, dive > 50 m, repeat diving (31 DCS episodes) |
| Gempp, 2017 | 553 (634 DCI patients) | 259 | N/A | 43.6 ± 11.3 (all DCS patients) a 34.6 ± 9.0 (no NDCS) a | N/A | N/A | N/A | Ν/A | Cerebral (97) Spinal (255) Inner ear (201) | Ν/A |
| Germonpre, 1998 | 37 | 36 | N/A | 37.5 ± 9(NDCS) a | N/A | 327 ± 282 (cerebral) a 481 ± 465 (spinal) a | 35 ± 11 (cerebral) 41 ± 8 (spinal)a | 8 ± 6 (cerebral) a 12 ± 10 (spinal) a | Cerebral (20) Spinal (17) | Fault during diving: (8, cerebral), (3, spinal) |
| Koch, 2008 | 18 | 18 | N/A | 37 ± 10.2 (NDCS) a 40.3 ± 12.7 (no NDCS) a | 83.3 (NDCS) 83.3 (no NDCS) | 888 (7–6000) (NDCS) b 870 (110–5500) (no NDCS) b | N/A | N/A | N/A | No |
| Cross sectional/cohort studies | ||||||||||
| Cartoni, 2004 | 30 (41 DCS patients) | 25 | All | 35 ± 8 (DCS patients) a | 90.9 (all) | N/A | 42 ± 11 (RLS+) a 31 ± 11 (RLS-) a | N/A | N/A | Repetitive dives (10) Missed deco stops/rapid ascent (21) |
| Torti, 2004 | 28 | 202 | N/A | 39 ± 8 (all) a | 80 (all) | 650 (250–1200) (RLS+) c 400 (214–800) (RLS−) c | 29 ± 9 (RLS+) a 28 ± 9 (RLS−) a | 11 ± 8(RLS+) 9 ± 7 (RLS−) a | N/A | No |
| Liou, 2015 | 32 | 43 * | N/A | 39 ± 13 (all) a | 61 (all) | 100 ± 178 (RLS+) a 65 ± 202 (RLS−) a | 29 ± 10 (RLS+) a 32 ± 28 (RLS−) a | N/A | N/A | N/A |
| Germonpre, 2021 | 18 (all DCS) ** | 130 | N/A | 38.3 | 68 (all) | 441.0 ± 751.2 (RLS+) a 524.7 ± 843.56 (RLS−) a | N/A | N/A | Inner ear (9) Spinal (6) | Most cases in PFO+ group refer to provocative dives |
| Study | Diagnostic Modality | Criteria for the Diagnosis of RLS | Criteria for the Diagnosis of High-Grade RLS | RLS in NDCS Group, N (%) | RLS in No NDCS Group, N (%) | Large RLS in NDCS Group, N (%) | Large RLS in no NDCS Group, N (%) | |||
| Case–control studies | ||||||||||
| Wilmshurst, 1989 | TTE | Passage of microbubbles in the L atrium within two cardiac cycles after complete opacification of the R atrium | >20 microbubbles | 23 (43.4) | 15 (23.8) | 14 (26.4) | 8 (12.7) | |||
| Germonpre, 1998 | TEE | Passage of microbubbles in the L atrium within three heart cycles after complete opacification of the R atrium | ≥20 microbubbles at rest or after Valsalva strain | 22 (59.5) | 13 (36.1) | 19 (51.3) | 9 (25) | |||
| Wilmshurst, 2000 | TTE | Passage of microbubbles in the L atrium after the first injection at rest or up to five injections performed with the Valsalva maneuver | >20 microbubbles | 58 (58) | 34 (27.6) | 51 (51) | 9 (7.3) | |||
| Cantais, 2003 | TCD | >5 HITS 5–15 s after injection | >20 HITS within 20 s | 57 (66.3) | 25 (24.8) | 47 (54.7) | 12 (11.9) | |||
| Cartoni, 2004 | TEE/TTE | ≥3 microbubbles within three cardiac cycles | Shunts occurring at rest | 23 (76.7) | 7 (28) | 15 (50) | 1 (4) | |||
| Gempp, 2008 | TCD | >5 HITS within 20 s after injection or <10 s after release phase | >20 HITS | 25 (51) | 11 (22) | 18 (37) | 8 (16) | |||
| Gempp, 2017 | TCD | >5 HITS within 15 s after normal breathing or 10 s after the end of provocative maneuver | >20 HITS | 366 (66.2) | 82 (31.7) | 308 (55.7) | 55 (21.2) | |||
| Cross-sectional studies | ||||||||||
| Torti, 2004 | TEE | Passage of bubbles from the R to L atrium within four cardiac cycles | Visualization of a cloud of bubbles | 18 (64.3) | 45 (22.3) | N/A | N/A | |||
| Koch, 2008 | TCD, TTE | Signals of contrast visualized in the L atrium after complete opacification of the R atrium OR > 5 HITS within 10 s after Valsalva release | >20 HITS or spontaneous shunting | 5 (27.8) | 7 (38.9) | 4 (22.2) | 6 (33.3) | |||
| Liou, 2015 | TTE | Passage of bubbles from the R to L atrium within four cardiac cycles | N/A | 23 (71.9) | 16 (37.2) | N/A | N/A | |||
| Germonpre, 2021 | Carotid Doppler | Visualization of microbubbles after up to three injections with straining maneuvers | N/A | 6 (Inner ear) (66.6) 1 (Spinal) (20) | 20 (15.4) | N/A | N/A | |||
| Study (Author, Year) | Design | Divers, N | ABLs Group, N (%) | No ABLs Group, N (%) | Professional Divers, N | Age, Years | Males, % | Diving Depth (m) | N of Dives |
|---|---|---|---|---|---|---|---|---|---|
| Knauth, 1997 | Cross sectional | 87 | 11 (12.6) | 76 (87.4) | All amateur | 35.7 ± 8.9 b | 77.0 | N/A | 565.3 ± 509.1 b |
| Gerriets, 2003 | Cross sectional | 42 | 1 (2.4) | 41 (97.6) | All amateur | 35.7 ± 7.9 b (RLS+) 32.2 ± 7.5 b (RLS-) | 97.6 | 27.7 (15.5–39.8) c | 305 (20–4970) (RLS+) a 295 (21–2000) (RLS-) a |
| Koch, 2004 | Cross sectional | 50 | 24 (48) | 26 (52) | Military & Civilian | 34.7 ± 10.6 b | 94 | N/A | 500 (21–5500) a |
| Koch, 2008 | Case–control | 18 | 8 (44.4) | 10 (55.6) | Military | 40.3 ± 12.7 b | 83.3 | N/A | 870 (110–5500) a |
| Gempp, 2010 | Case–control | 32 | 14 (43.7) | 18 (56.3) | Military | 35 ± 5 b | 100 | All < 60 m | 1659 ± 122 b |
| Balestra, 2016 | Cross sectional | 42 | 5 (11.9) | 37 (88.1) | All amateur | 36 ± 4.85 b | 90.5 | 57.9% dives < 30 m | 620 ± 465 b |
| Study (Author, Year) | Diagnostic Modalities (RLS/ABLs) | Criteria for the Diagnosis of RLS | Criteria for the Diagnosis of High-Grade RLS | RLS in ABLs Group, N (%) | RLS in No ABLs Group, N (%) | Large RLS in ABLs Group, N (%) | Large RLS in No ABLs Group, N (%) | ||
| Knauth, 1997 | TCD/MRI | ≥5 HITS after the Valsalva maneuver | ≥20 HITS | 4/11 (36.4) | 21/76 (27.6) | N/A | N/A | ||
| Gerriets, 2003 | TCD/MRI | >3 HITS | ≥20 HITS | 0/1 (0) | 16/41 (39) | N/A | N/A | ||
| Koch, 2004 | TCD, TTE/MRI | Signals of contrast visualized in the L atrium after complete opacification of the R atrium OR >5 HITS within 10 s after Valsalva release | N/A | 10/24 (41.7) | 8/26 (30.8) | N/A | N/A | ||
| Koch, 2008 | TCD, TTE/MRI | Signals of contrast visualized in the L atrium after complete opacification of the R atrium OR >5 HITS within 10 s after Valsalva release | >20 HITS or spontaneous shunting | 3/8 (37.5) | 4/10 (40) | N/A | N/A | ||
| Gempp, 2010 | TCD/MRI | >5 HITS within 20 s after injection or 10 s after the release phase of the Valsalva maneuver | >15 HITS | 9/14 (64.3) | 6/18 (33.3) | 9/14 (64.3) | 3/18 (16.6) | ||
| Balestra, 2016 | TEE/MRI | Passage of microbubbles in the L atrium within three heart cycles after complete opacification of R atrium | >20 microbubbles | 3/5 (60) | 24/37 (64.9) | 2/5 (40) | 14/37 (37.8) | ||
| Study (Author, Year) | Design | Ν of Divers | Age, Years (mean ± SD) | Males, N (%) | Predisposing Factors for NDCS (N) | Diagnostic Modality | Divers with NDCS, N | NDCS Type (N) | RLS in Divers with NDCS, N (%) | Large RLS in Divers with NDCS, N (%) |
|---|---|---|---|---|---|---|---|---|---|---|
| Moon, 1989 | Case–control | 30 | 33.5 (12–48) | 23 (76.6) | N/A | TTE | 18 | N/A | 11 (61.1) | N/A |
| Kerut, 1997 | Retrospective cohort | 26 | 29.1 ± 6.4 | 23 (88.4) | N/A | TEE | 15 * | N/A | 9 (60) | N/A |
| Schwerzmann, 2001 ** | Retrospective cohort | 52 | 38 ± 10 (RLS group) 35 ± 8 (no RLS group) | 10 (77) (RLS group) 30 (77) (no RLS group) | N/A | TEE | 4/13 (RLS group) 4/39 (no RLS group) | Spinal or cerebral | N/A | N/A |
| Klingmann 2003 | Case series | 9 | N/A | N/A | No | TCD | 9 | IEDCS | 9 (100) | 9 (100) |
| Klingmann, 2007 | Retrospective cohort | 18 | 43 (25–61) | 15 (83.3) | N/A | TCD | 18 | IEDCS | 15 (83.3) | 15 (83.3) |
| Harrah, 2008 | Retrospective cohort | 113 | 40 (19–67) | 83% | N/A | TTE | 48 | N/A | 6/12 (50) | N/A |
| Klingmann, 2012 | Retrospective cohort | 30 | 43 ± 9 (25–60) | 23 (76.6) | Repetitive diving (26) | TCD | 30 | IEDCS | 22 (73) | N/A |
| Gempp, 2012 | Retrospective cohort | 115 | 44 ± 11 | 99 (86) | Provocative decompression schedule (4) Repetitive dives within 24 h (38) | TCD | 115 | IEDCS (all) | 95 (82.6) | 89 (77) |
| Ignatescu, 2012 | Retrospective cohort | 33 | 46 (31–61) | 31 (94) | Decompression diving or dehydration (22) Previous DCS episode (6) | TTE | 33 | IEDCS (all) | 24/30 (80) | 23 (76.6) |
| Guenzani, 2016 | Case series | 9 | 47.3 | 9 (100) | Omitted stops (2) | N/A | 9 | IEDCS (all) | 5 (55.5) | N/A |
| Lafere, 2017 | Retrospective cohort | 209 | 40.5 ± 11.2 | 80.4% | N/A | TEE/TTE | 209 | Cerebral (all) | 167 (80) | 133 (63.6) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peppas, S.; Palaiodimos, L.; Nagraj, S.; Kokkinidis, D.G.; Tiwari, N.; Kharawala, A.; Mojadidi, M.K.; Mojaddedi, S.; Ntaios, G.; Faillace, R.T.; et al. Right-to-Left Shunt in Divers with Neurological Decompression Sickness: A Systematic Review and Meta-Analysis. Healthcare 2023, 11, 1407. https://doi.org/10.3390/healthcare11101407
Peppas S, Palaiodimos L, Nagraj S, Kokkinidis DG, Tiwari N, Kharawala A, Mojadidi MK, Mojaddedi S, Ntaios G, Faillace RT, et al. Right-to-Left Shunt in Divers with Neurological Decompression Sickness: A Systematic Review and Meta-Analysis. Healthcare. 2023; 11(10):1407. https://doi.org/10.3390/healthcare11101407
Chicago/Turabian StylePeppas, Spyros, Leonidas Palaiodimos, Sanjana Nagraj, Damianos G. Kokkinidis, Nidhish Tiwari, Amrin Kharawala, Mohammad K. Mojadidi, Sanauallah Mojaddedi, George Ntaios, Robert T. Faillace, and et al. 2023. "Right-to-Left Shunt in Divers with Neurological Decompression Sickness: A Systematic Review and Meta-Analysis" Healthcare 11, no. 10: 1407. https://doi.org/10.3390/healthcare11101407