
Evaluating the Effectiveness of Return-to-Work Interventions for Individuals with Work-Related Mental Health Conditions: A Systematic Review and Meta-Analysis

 , ,
, ,  ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Overview
2.2. Search Strategy and Study Selection
2.3. Critical Appraisal of Included Studies
2.4. Data Extraction
2.5. Meta-Analysis
2.6. Intervention Categorization
3. Results
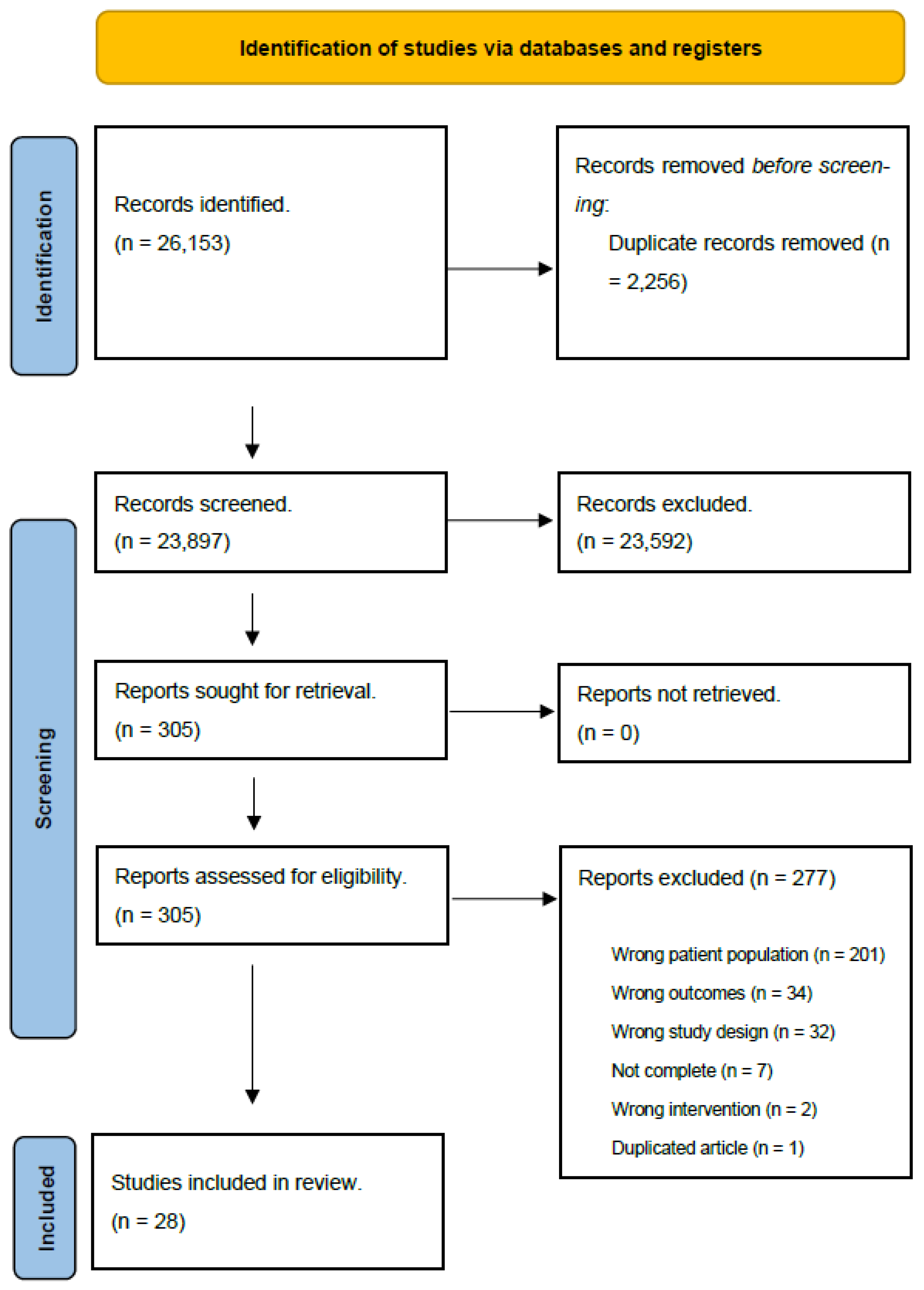
3.1. Search Outcome
3.2. Critical Appraisal of Included Studies
3.3. Interventions
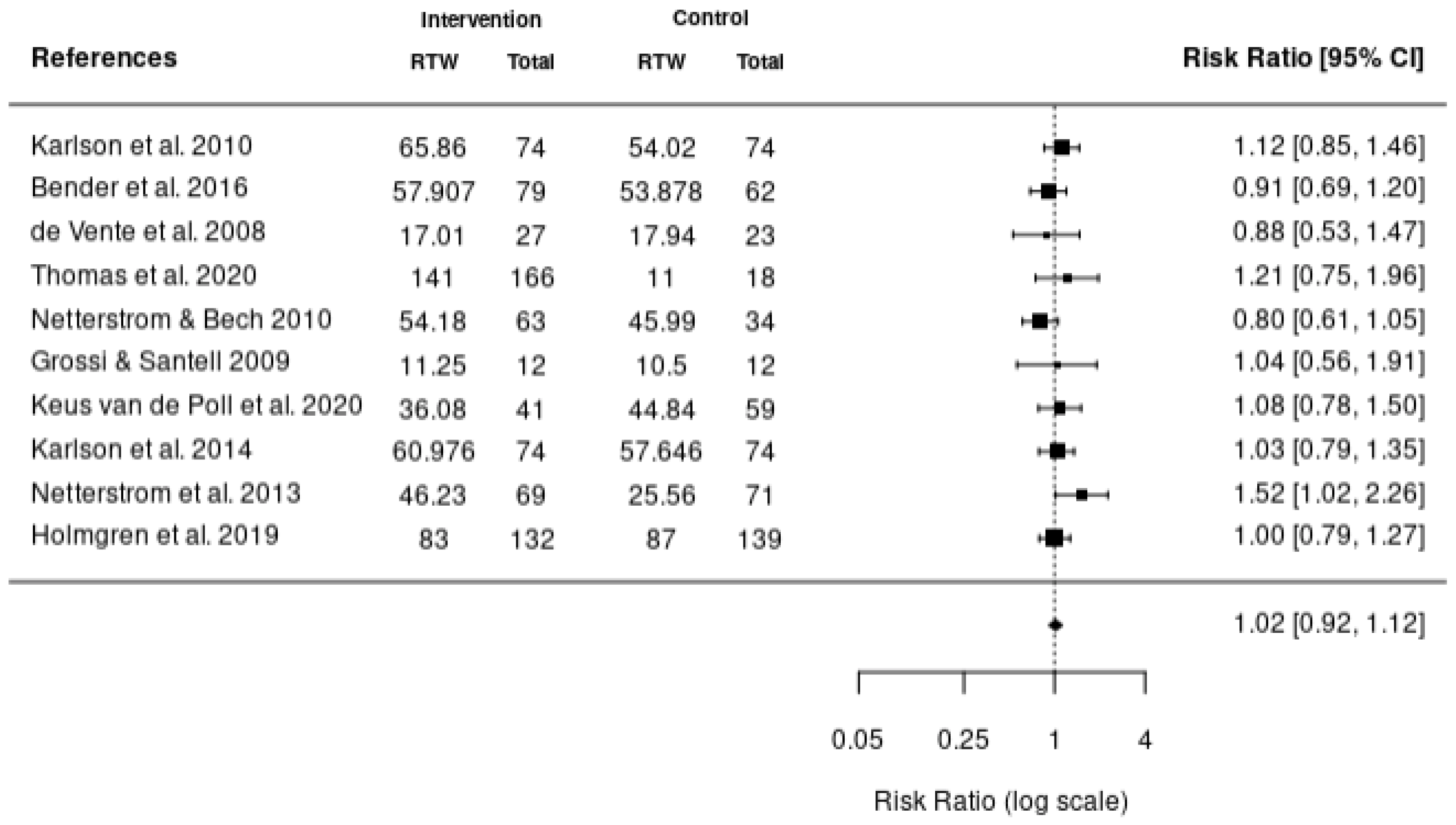
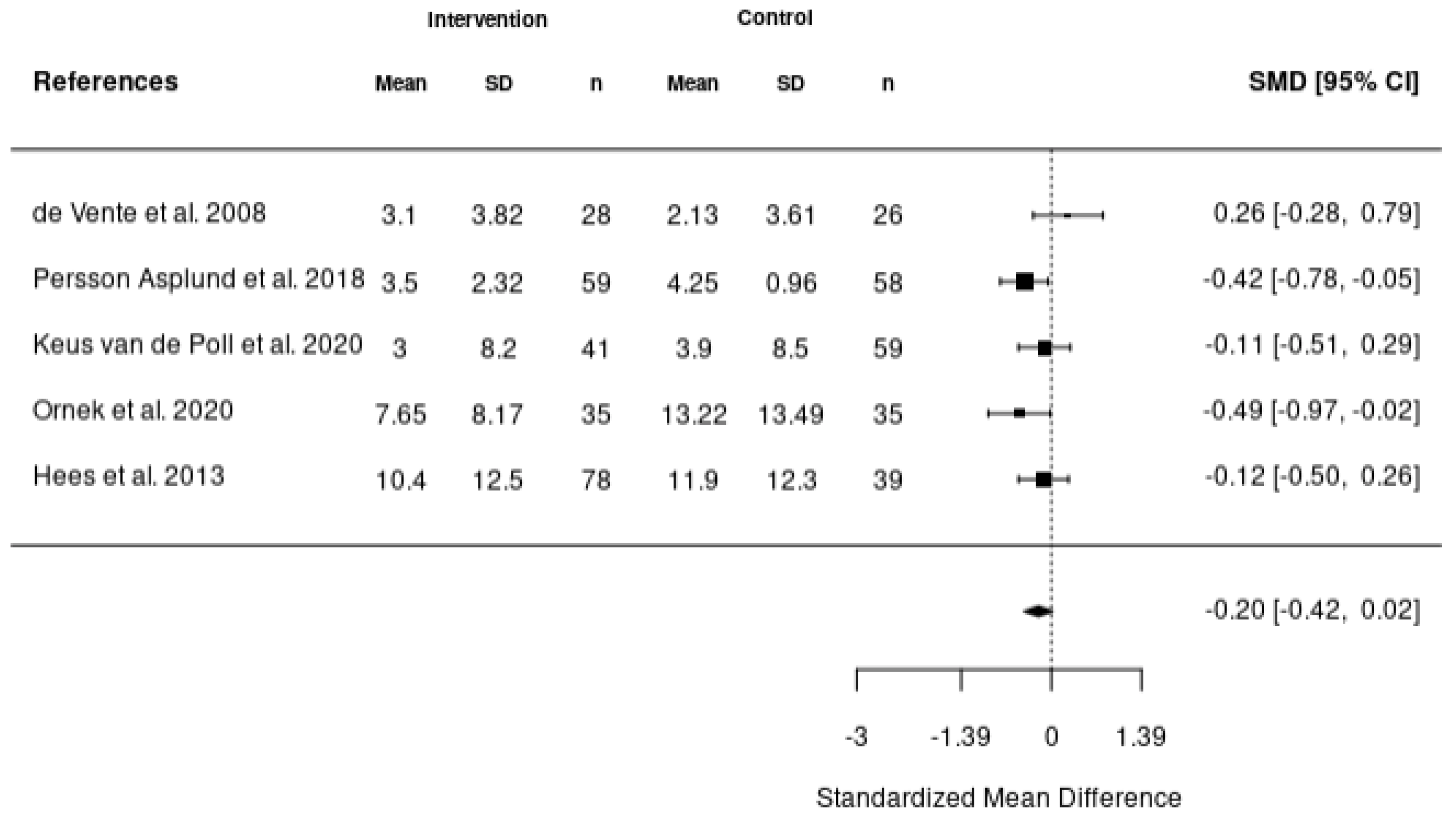
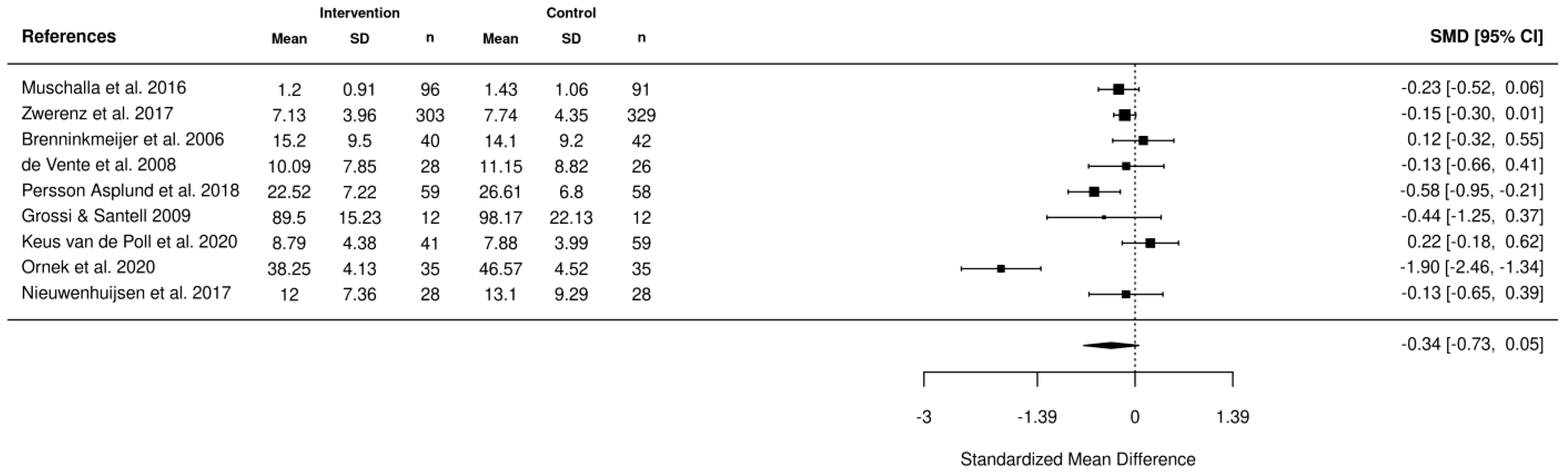
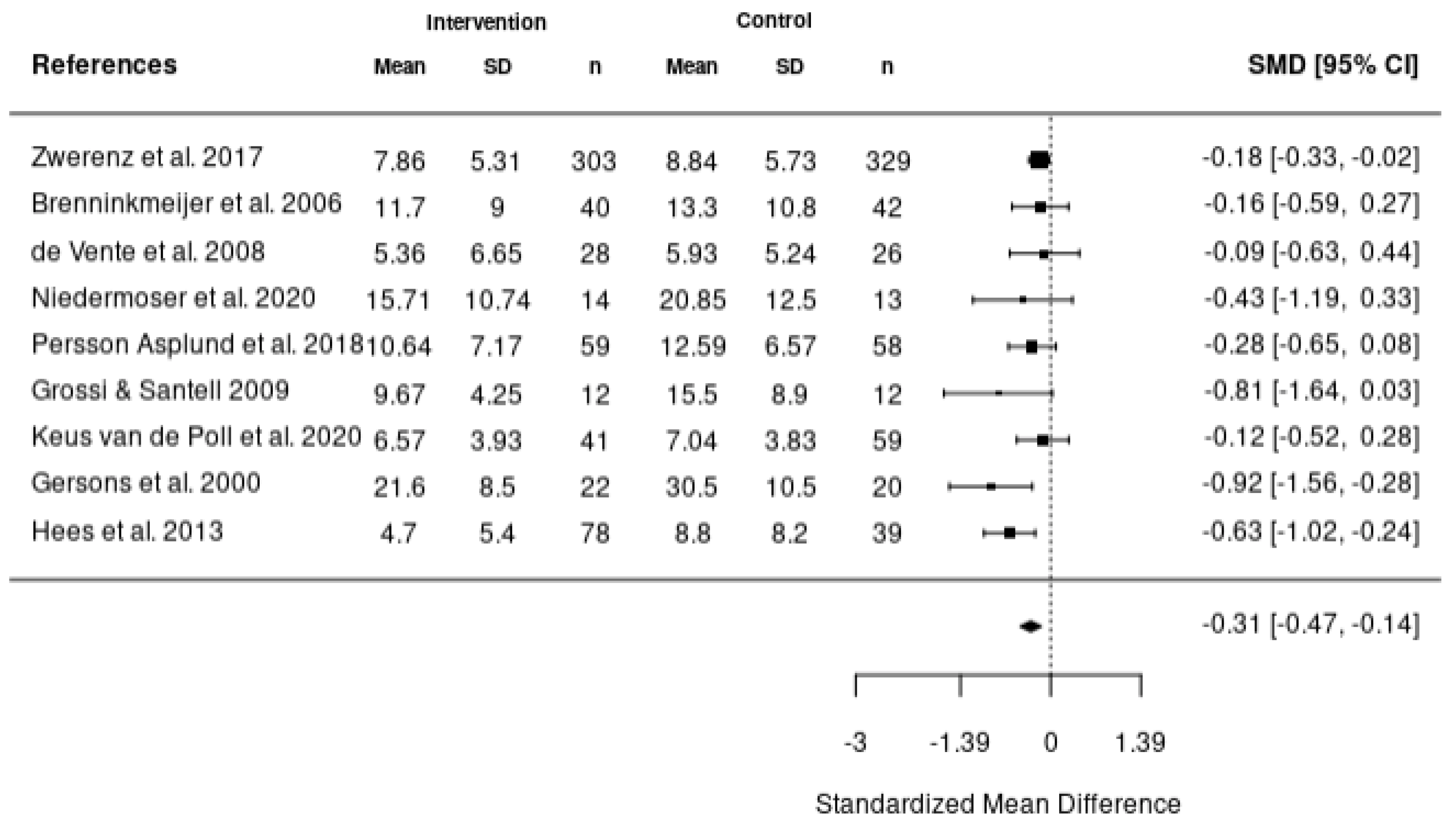
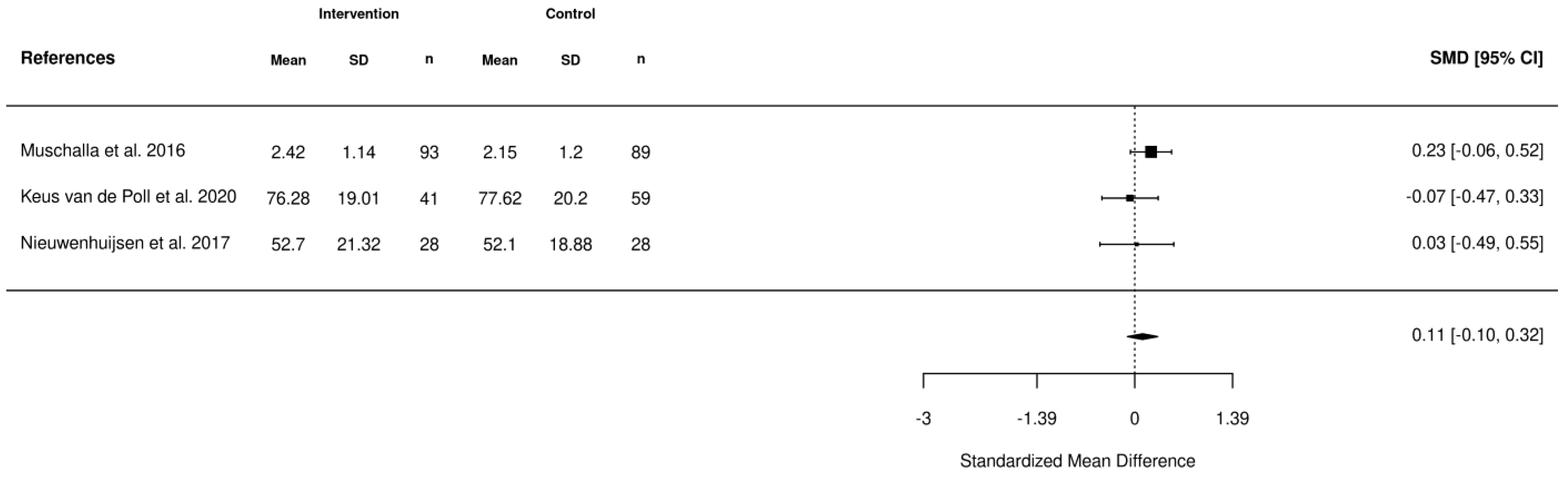
3.4. Meta-Analytic Findings
4. Discussion
4.1. Implications
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1. MEDLINE
Appendix A.2. APA PsycInfo
Appendix A.3. CINAHL
Appendix A.4. Cochrane
Appendix A.5. EMBASE
References
- World Health Organization. World Mental Health Report: Transforming Mental Health for All; World Health Organization: Geneva, Switzerland, 2022.
- Garrido Larrea, P.; Ansoleaga Moreno, E.; Tomicic Suñer, A.; Domínguez Valverde, C.; Castillo Vergara, S.; Lucero Chenevard, C.; Martínez Guzmán, C. Afecciones de Salud Mental y El Proceso de Retorno al Trabajo: Una Revisión Sistemática. Cienc. Trab. 2013, 15, 105–113. [Google Scholar] [CrossRef]
- Aranibar, L.A. Proceso de Reconocimiento de Una Enfermedad Mental de Origen Laboral: La Experiencia Chilena. Rev. Bras. De Med. Do Trab. 2018, 16, 100–105. [Google Scholar] [CrossRef]
- Dobson, K.G.; Vigod, S.N.; Mustard, C.; Smith, P.M. Trends in the Prevalence of Depression and Anxiety Disorders among Working-Age Canadian Adults between 2000 and 2016. Stat. Can. 2020, 31, 12–23. [Google Scholar]
- Harvey, S.B.; Modini, M.; Joyce, S.; Milligan-Saville, J.S.; Tan, L.; Mykletun, A.; Bryant, R.A.; Christensen, H.; Mitchell, P.B. Can Work Make You Mentally Ill? A Systematic Meta-Review of Work-Related Risk Factors for Common Mental Health Problems. Occup. Environ. Med. 2017, 74, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Lagerveld, S.E.; Blonk, R.W.B.; Brenninkmeijer, V.; Schaufeli, W.B. Return to Work among Employees with Mental Health Problems: Development and Validation of a Self-Efficacy Questionnaire. Work Stress 2010, 24, 359–375. [Google Scholar] [CrossRef]
- Mental Health Commission of Canada; Canadian Psychological Association. Extended Mental Health Benefits in Canadian Workplaces: Employee and Employer Perspectives; Mental Health Commission of Canada; Canadian Psychological Association: Ottawa, ON, Canada, 2022. [Google Scholar]
- Mental Health Commission of Canada. Issue Brief: Workplace Mental Health; Mental Health Commission of Canada: Ottawa, ON, Canada, 2016. [Google Scholar]
- Hendriks, S.M.; Spijker, J.; Licht, C.M.M.; Hardeveld, F.; de Graaf, R.; Batelaan, N.M.; Penninx, B.W.J.H.; Beekman, A.T.F. Long-Term Work Disability and Absenteeism in Anxiety and Depressive Disorders. J. Affect. Disord. 2015, 178, 121–130. [Google Scholar] [CrossRef]
- Henderson, M.; Harvey, S.; Øverland, S.; Mykletun, A.; Hotopf, M. Work and Common Psychiatric Disorders. J. R. Soc. Med. 2011, 104, 198–207. [Google Scholar] [CrossRef]
- Nigatu, Y.T.; Liu, Y.; Uppal, M.; McKinney, S.; Rao, S.; Gillis, K.; Wang, J. Interventions for Enhancing Return to Work in Individuals with a Common Mental Illness: Systematic Review and Meta-Analysis of Randomized Controlled Trials. Psychol. Med. 2016, 46, 3263–3274. [Google Scholar] [CrossRef]
- Björk Brämberg, E.; Holmgren, K.; Bültmann, U.; Gyllensten, H.; Hagberg, J.; Sandman, L.; Bergström, G. Increasing Return-to-Work among People on Sick Leave Due to Common Mental Disorders: Design of a Cluster-Randomized Controlled Trial of a Problem-Solving Intervention versus Care-as-Usual Conducted in the Swedish Primary Health Care System (PROSA). BMC Public Health 2018, 18, 889. [Google Scholar] [CrossRef]
- Cullen, K.L.; Irvin, E.; Collie, A.; Clay, F.; Gensby, U.; Jennings, P.A.; Hogg-Johnson, S.; Kristman, V.; Laberge, M.; McKenzie, D.; et al. Effectiveness of Workplace Interventions in Return-to-Work for Musculoskeletal, Pain-Related and Mental Health Conditions: An Update of the Evidence and Messages for Practitioners. J. Occup. Rehabil. 2018, 28, 1–15. [Google Scholar] [CrossRef]
- Dewa, C.S.; Loong, D.; Bonato, S.; Joosen, M.C.W. The Effectiveness of Return-to-Work Interventions That Incorporate Work-Focused Problem-Solving Skills for Workers with Sickness Absences Related to Mental Disorders: A Systematic Literature Review. BMJ Open 2015, 5, e007122. [Google Scholar] [CrossRef] [PubMed]
- Salomonsson, S.; Hedman-Lagerlöf, E.; Öst, L.-G. Sickness Absence: A Systematic Review and Meta-Analysis of Psychological Treatments for Individuals on Sick Leave Due to Common Mental Disorders. Psychol. Med. 2018, 48, 1954–1965. [Google Scholar] [CrossRef] [PubMed]
- Mikkelsen, M.B.; Rosholm, M. Systematic Review and Meta-Analysis of Interventions Aimed at Enhancing Return to Work for Sick-Listed Workers with Common Mental Disorders, Stress-Related Disorders, Somatoform Disorders and Personality Disorders. Occup. Environ. Med. 2018, 75, 675–686. [Google Scholar] [CrossRef] [PubMed]
- Karlson, B.; Jönsson, P.; Pålsson, B.; Åbjörnsson, G.; Malmberg, B.; Larsson, B.; Österberg, K. Return to Work after a Workplace-Oriented Intervention for Patients on Sick-Leave for Burnout—A Prospective Controlled Study. BMC Public Health 2010, 10, 301. [Google Scholar] [CrossRef] [PubMed]
- Bender, A.; Eynan, R.; O’Grady, J.; Nisenbaum, R.; Shah, R.; Links, P.S. Best Practice Intervention for Post-Traumatic Stress Disorder among Transit Workers. Work 2016, 54, 59–71. [Google Scholar] [CrossRef]
- Netterstrøm, B.; Friebel, L.; Ladegaard, Y. Effects of a Multidisciplinary Stress Treatment Programme on Patient Return to Work Rate and Symptom Reduction: Results from a Randomised, Wait-List Controlled Trial. Psychother. Psychosom. 2013, 82, 177–186. [Google Scholar] [CrossRef]
- Thomas, T.E.; Eyal, R.; Menchavez, F.; Mocci, T.; Goldblatt, G.; Lanoff, J.; Hays, M.; Shim, J.J.; Barry, T.P. Reducing Workplace Absenteeism Caused by Work Stress in a Health Maintenance Organization Department of Psychiatry. Perm J. 2020, 24, 19.027. [Google Scholar] [CrossRef]
- de Vente, W.; Kamphuis, J.H.; Emmelkamp, P.M.G.; Blonk, R.W.B. Individual and Group Cognitive-Behavioral Treatment for Work-Related Stress Complaints and Sickness Absence: A Randomized Controlled Trial. J. Occup. Health Psychol. 2008, 13, 214–231. [Google Scholar] [CrossRef]
- Netterstrøm, B.; Bech, P. Effect of a Multidisciplinary Stress Treatment Programme on the Return to Work Rate for Persons with Work-Related Stress. A Non-Randomized Controlled Study from a Stress Clinic. BMC Public Health 2010, 10, 658. [Google Scholar] [CrossRef]
- Karlson, B.; Jönsson, P.; Österberg, K. Long-Term Stability of Return to Work after a Workplace-Oriented Intervention for Patients on Sick Leave for Burnout. BMC Public Health 2014, 14, 821. [Google Scholar] [CrossRef]
- Grossi, G.; Santell, B. Quasi-Experimental Evaluation of a Stress Management Programme for Female County and Municipal Employees on Long-Term Sick Leave Due to Work-Related Psychological Complaints. J. Rehabil. Med. 2009, 41, 632–638. [Google Scholar] [CrossRef] [PubMed]
- Keus van de Poll, M.; Nybergh, L.; Lornudd, C.; Hagberg, J.; Bodin, L.; Kwak, L.; Jensen, I.; Lohela-Karlsson, M.; Torgén, M.; Bergstrom, G. Preventing Sickness Absence among Employees with Common Mental Disorders or Stress-Related Symptoms at Work: A Cluster Randomised Controlled Trial of a Problem-Solving-Based Intervention Conducted by the Occupational Health Services. Occup. Environ. Med. 2020, 77, 454–461. [Google Scholar] [CrossRef] [PubMed]
- Kellermeyer, L.; Harnke, B.; Knight, S. Covidence and Rayyan. J. Med. Libr. Assoc. 2018, 106, 580–583. [Google Scholar] [CrossRef]
- Critical Appraisal Skills Programme. CASP Randomized Controlled Trial Checklist. Available online: https://casp-uk.net/casp-tools-checklists/ (accessed on 4 April 2023).
- Joan Briggs Institute. JBI Critical Appraisal Tools: Checklist for Quasi-Experimental Studies. Available online: https://jbi.global/critical-appraisal-tools (accessed on 5 April 2023).
- Dalgaard, V.L.; Aschbacher, K.; Andersen, J.H.; Glasscock, D.J.; Willert, M.V.; Carstensen, O.; Biering, K. Return to Work after Work-Related Stress: A Randomized Controlled Trial of a Work-Focused Cognitive Behavioral Intervention. Scand. J. Work Environ. Health 2017, 43, 436–446. [Google Scholar] [CrossRef]
- Glasscock, D.J.; Carstensen, O.; Dalgaard, V.L. Recovery from Work-Related Stress: A Randomized Controlled Trial of a Stress Management Intervention in a Clinical Sample. Int. Arch. Occup. Environ. Health 2018, 91, 675–687. [Google Scholar] [CrossRef]
- Willert, M.V.; Thulstrup, A.M.; Bonde, J.P. Effects of a Stress Management Intervention on Absenteeism and Return to Work–Results from a Randomized Wait-List Controlled Trial. Scand. J. Work Environ. Health 2011, 37, 186–195. [Google Scholar] [CrossRef] [PubMed]
- Beck, B.D.; Hansen, Å.M.; Gold, C. Coping with Work-Related Stress through Guided Imagery and Music (GIM): Randomized Controlled Trial. J. Music 2015, 52, 323–352. [Google Scholar] [CrossRef]
- Collins, D.A.J.; Harvey, S.B.; Lavender, I.; Glozier, N.; Christensen, H.; Deady, M. A Pilot Evaluation of a Smartphone Application for Workplace Depression. Int. J. Environ. Res. Public Health 2020, 17, 6753. [Google Scholar] [CrossRef] [PubMed]
- Gersons, B.P.R.; Carlier, I.V.E.; Lamberts, R.D.; van der Kolk, B.A. Randomized Clinical Trial of Brief Eclectic Psychotherapy for Police Officers with Posttraumatic Stress Disorder. J. Trauma. Stress 2000, 13, 333–347. [Google Scholar] [CrossRef]
- Hees, H.L.; de Vries, G.; Koeter, M.W.J.; Schene, A.H. Adjuvant Occupational Therapy Improves Long-Term Depression Recovery and Return-to-Work in Good Health in Sick-Listed Employees with Major Depression: Results of a Randomised Controlled Trial. Occup. Environ. Med. 2013, 70, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Muschalla, B.; Linden, M.; Jöbges, M. Work-Anxiety and Sickness Absence After a Short Inpatient Cognitive Behavioral Group Intervention in Comparison to a Recreational Group Meeting. J. Occup. Environ. Med. 2016, 58, 398–406. [Google Scholar] [CrossRef]
- Niedermoser, D.W.; Kalak, N.; Kiyhankhadiv, A.; Brand, S.; Walter, C.; Schweinfurth, N.; Lang, U.E. Workplace-Related Interpersonal Group Psychotherapy to Improve Life at Work in Individuals with Major Depressive Disorders: A Randomized Interventional Pilot Study. Front. Psychiatry 2020, 11, 168. [Google Scholar] [CrossRef] [PubMed]
- Schene, A.H.; Koeter, M.W.J.; Kikkert, M.J.; Swinkels, J.A.; McCrone, P. Adjuvant Occupational Therapy for Work-Related Major Depression Works: Randomized Trial Including Economic Evaluation. Psychol. Med. 2007, 37, 351. [Google Scholar] [CrossRef] [PubMed]
- Schramm, E.; Mack, S.; Thiel, N.; Jenkner, C.; Elsaesser, M.; Fangmeier, T. Interpersonal Psychotherapy vs. Treatment as Usual for Major Depression Related to Work Stress: A Pilot Randomized Controlled Study. Front. Psychiatry 2020, 11, 193. [Google Scholar] [CrossRef]
- Holmgren, K.; Hensing, G.; Bültmann, U.; Hadzibajramovic, E.; Larsson, M.E.H. Does Early Identification of Work-Related Stress, Combined with Feedback at GP-Consultation, Prevent Sick Leave in the Following 12 Months? A Randomized Controlled Trial in Primary Health Care. BMC Public Health 2019, 19, 1110. [Google Scholar] [CrossRef]
- Nieuwenhuijsen, K.; Schoutens, A.M.C.; Frings-Dresen, M.H.W.; Sluiter, J.K. Evaluation of a Randomized Controlled Trial on the Effect on Return to Work with Coaching Combined with Light Therapy and Pulsed Electromagnetic Field Therapy for Workers with Work-Related Chronic Stress. BMC Public Health 2017, 17, 761. [Google Scholar] [CrossRef]
- Rannard, A.; Gabbay, M.; Sen, D.; Riley, R.; Britt, D. Feasibility Trial of GP and Case-Managed Support for Workplace Sickness Absence. Prim. Health Care Res. Dev. 2014, 15, 252–261. [Google Scholar] [CrossRef] [PubMed]
- Van de Leur, J.C.; Buhrman, M.; Åhs, F.; Rozental, A.; Jansen, G.B. Standardized Multimodal Intervention for Stress-Induced Exhaustion Disorder: An Open Trial in a Clinical Setting. BMC Psychiatry 2020, 20, 526. [Google Scholar] [CrossRef]
- Ornek, O.K.; Esin, M.N. Effects of a Work-Related Stress Model Based Mental Health Promotion Program on Job Stress, Stress Reactions and Coping Profiles of Women Workers: A Control Groups Study. BMC Public Health 2020, 20, 1658. [Google Scholar] [CrossRef] [PubMed]
- Zwerenz, R.; Becker, J.; Gerzymisch, K.; Siepmann, M.; Holme, M.; Kiwus, U.; Spörl-Dönch, S.; Beutel, M.E. Evaluation of a Transdiagnostic Psychodynamic Online Intervention to Support Return to Work: A Randomized Controlled Trial. PLoS ONE 2017, 12, e0176513. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration. 2011. Available online: https://www.cochrane-handbook.org/ (accessed on 6 April 2023).
- R Development Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2006. [Google Scholar]
- Blonk, R.W.B.; Brenninkmeijer, V.; Lagerveld, S.E.; Houtman, I.L.D. Return to Work: A Comparison of Two Cognitive Behavioural Interventions in Cases of Work-Related Psychological Complaints among the Self-Employed. Work Stress 2006, 20, 129–144. [Google Scholar] [CrossRef]
- Persson Asplund, R.; Dagöö, J.; Fjellström, I.; Niemi, L.; Hansson, K.; Zeraati, F.; Ziuzina, M.; Geraedts, A.; Ljótsson, B.; Carlbring, P.; et al. Internet-Based Stress Management for Distressed Managers: Results from a Randomised Controlled Trial. Occup. Environ. Med. 2018, 75, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Winter, L.; Geldmacher, J.; Plücker-Boss, K.; Kahl, K.G. Integration of a Return-to-Work Module in Cognitive Behavioral Therapy in Patients with Major Depressive Disorder and Long-Term Sick Leave—A Feasibility Study. Front. Psychiatry 2020, 11, 512. [Google Scholar] [CrossRef] [PubMed]
- Ansoleaga, E.; Garrido, P.; Domínguez, C.; Castillo, S.; Lucero, C.; Tomicic, A.; Martínez, C. Facilitadores Del Reintegro Laboral En Trabajadores Con Patología Mental de Origen Laboral: Una Revisión Sistemática. Rev. Med. Chil. 2015, 143, 85–95. [Google Scholar] [CrossRef]
- Office of the Surgeon General. The US Surgeon General’s Framework for Workplace Mental Health & Well-Being; U.S. Department of Health & Human Services: Washington, DC, USA, 2022. [Google Scholar]
- van Gordon, W.; Shonin, E.; Zangeneh, M.; Griffiths, M.D. Work-Related Mental Health and Job Performance: Can Mindfulness Help? Int. J. Ment. Health Addict. 2014, 12, 129–137. [Google Scholar] [CrossRef]
- Bjørndal, M.T.; Giæver, F.; Aschim, B.M.; Gjengedal, R.G.H.; Lending, H.D.; Bull-Hansen, B.; Hannisdal, M.; Hjemdal, O. Work after Mental-Health-Related Absence: A Qualitative Study of Perceived Change after a Combination of Metacognitive Therapy and Work-Focused Interventions. BMC Public Health 2022, 22, 2231. [Google Scholar] [CrossRef]
- Nowrouzi-Kia, B.; Nadesar, N.; Sun, Y.; Ott, M.; Sithamparanathan, G.; Thakkar, P. Prevalence and Predictors of Return to Work Following a Spinal Cord Injury Using a Work Disability Prevention Approach: A Systematic Review and Meta-Analysis. Trauma 2022, 24, 14–23. [Google Scholar] [CrossRef]
- Martin, M.H.T.; Nielsen, M.B.D.; Petersen, S.M.A.; Jakobsen, L.M.; Rugulies, R. Implementation of a Coordinated and Tailored Return-to-Work Intervention for Employees with Mental Health Problems. J. Occup. Rehabil. 2012, 22, 427–436. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
|
|
| Author, Year, Country | Study Design; Sample Size | Diagnostic Criteria | Intervention and Domain Category | CASP Grade | JBI Grade |
|---|---|---|---|---|---|
| CBT-based intervention | |||||
| Brenninkmeijer et al., 2006, Netherlands [6] | RCT; n = 122 | Work-Related Adjustment Disorder | Cognitive behavioral therapy (CBT) and Combined intervention and Multi-Domain | 7 | n/a |
| Dalgaard et al. 2017., Denmark [29] | RCT; n = 163 | Work-Related Stress | Work-focused CBT intervention + “optional workplace intervention and Multi-Domain | 10 | n/a |
| de Vente et al., 2008, Netherlands [21] | RCT; n = 82 | Work-Related Stress | Group and Individual CBT based stress management training (SMT) and Health-Focused | 4 | n/a |
| Glasscock et al. 2018., Denmark [30] | RCT; n = 137 | Work-Related Stress | Stress Management Intervention-Individual CBT + Workplace Intervention and Multi-Domain | 6 | n/a |
| Willert et al. 2011., Denmark [31] | Randomized waitlist-controlled trial; n = 102 | Work-Related Stress | Group-format cognitive behavioral stress management intervention and Health-Focused | 9 | n/a |
| Health-focused intervention | |||||
| Beck et al., 2015, Denmark [32] | Randomized waitlist-controlled trial; n = 20 | Work-Related Stress | Guided Imagery and Music (GIM) Intervention and Health-Focused | 8 | n/a |
| Collins et al., 2020, Australia [33] | Pilot pre-post intervention design; n = 81 | Work-Related Stress | App-based intervention called “Anchored” and Health-Focused | n/a | 3 |
| Gersons et al., 2000, Netherlands [34] | Randomized controlled clinical trial; n = 42 | Work-Related PTSD | “Brief Eclectic Psychotherapy” and Health-Focused | 8 | n/a |
| Hees et al., 2013, Netherlands [35] | RCT; n = 117 | Work-Related Depression | Adjuvant occupational therapy and Health-Focused | 10 | n/a |
| Muschalla et al., 2016, Germany [36] | cluster RCT; n = 345 | Work-Related Anxiety Disorder | Work-anxiety coping group (WAG) and Recreational Group (RG) and Health-Focused | 6 | n/a |
| Niedermoser et al., 2020, Switzerland [37] | Randomized interventional pilot study; n = 27 | Work-Related Depression | Work-related Interpersonal Psychotherapy (W-IPT) and Health-Focused | 7 | n/a |
| Schene et al., 2007, Netherlands [38] | RCT; n = 62 | Work-Related Depression | Treatment as usual + Occupational Therapy and Health-Focused | 10 | n/a |
| Schramm et al., 2020, Germany [39] | Monocentric RCT; n = 28 | Work-Related Depression | Work-related Interpersonal Psychotherapy (W-IPT) and Health-Focused | 10 | n/a |
| Thomas et al., 2020, USA [20] | Pilot program; n = 166 | Work-Related Stress | Work Recovery Group (WRG) and Health-Focused | n/a | 4 |
| Multi-domain intervention | |||||
| Bender et al. 2016, Canada [18] | Pre-post intervention design; n = 141 | Work-Related PTSD | Best Practice Intervention (BPI) and Multi-Domain | n/a | 7 |
| Grossi & Santell 2009, Sweden [24] | Quasi-experimental study; n = 24 | Work-Related Stress | Stress Management Program and Multi-Domain | n/a | 6 |
| Holmgren et al., 2019, Sweden [40] | Two-armed RCT; n = 271 | Work-Related Stress | Work Stress Questionnaire brief intervention + feedback from a general practitioner and Multi-Domain | 7 | n/a |
| Netterstrom & Bech 2010, Netherlands [22] | Prospective longitudinal study; n = 107 | Work-Related Adjustment Disorder | Multi-disciplinary stress treatment program and Multi-Domain | n/a | 7 |
| Nieuwenhuijsen et al., 2017, Netherlands [41] | Randomized placebo-controlled trial; n = 96 | Work-Related Stress | Coaching + light therapy and pulsed electromagnetic field (PEMF) therapy and Multi-Domain | 7 | n/a |
| Persson Asplund et al., 2018, Sweden [42] | RCT; n = 117 | Work-Related Adjustment Disorder | Guided internet-based stress management (iSMI) and Multi-Domain | 10 | n/a |
| Rannard et al., 2014, United Kingdom [43] | Feasibility-controlled trial; n = 60 | Work-Related Stress | Case-managed support received from general practitioners + workplace health advisers and Multi-Domain | n/a | 4 |
| van de Leur et al., 2020, Sweden [44] | Standardized clinical multimodal intervention; n = 393 | Work-Related Burnout | Multimodal Intervention (MMI) and Multi-Domain | n/a | 6 |
| Workplace Service Coordination Intervention | |||||
| Karlson et al., 2010, Sweden [17] | Prospective controlled study; n = 148 | Work-Related Stress | Workplace oriented Intervention and Service Coordination | n/a | 9 |
| Karlson et al., 2014, Sweden [23] | Follow-up analysis; n = 136 | Work-Related Burnout | Workplace oriented Intervention and Service Coordination | n/a | 9 |
| Keus van de Poll et al., 2020, Sweden [25] | Two-armed RCT; n = 100 | Work-Related Stress | Brief problem-solving intervention (PSI) and Service Coordination | 8 | n/a |
| Ornek et al., 2020, Turkey [45] | Pre-post non-equivalent control groups design; n = 70 | Work-Related Stress | Workplace Mental Health Promotion Program based on Work-related stress model and Service Coordination | 9 | n/a |
| Zwerenz et al., 2017, Germany [46] | RCT; n = 664 | Work-Related Stress | Transdiagnostic psychodynamic online intervention and Service Coordination | 6 | n/a |
| Multi-domain and health-focused intervention | |||||
| Netterstrom et al., 2013, Denmark [19] | Randomized waitlist-controlled trial; n = 198 | Work-Related Stress | Multi-disciplinary stress treatment program and Multi-Domain and Health-Focused | 1 | n/a |
| Diagnosis | Sample Size | CASP Mean (SD) | JBI Mean (SD) |
|---|---|---|---|
| Work-Related Adjustment Disorder | 3 | 8.500 (2.121) | 7 (0.000) |
| Work-Related Anxiety Disorder | 1 | 6.000 (0.000) | n/a (n/a) |
| Work-Related Burnout | 2 | n/a (n/a) | 7.5 (2.121) |
| Work-Related Depression | 4 | 9.250 (1.500) | n/a (n/a) |
| Work-Related PTSD | 2 | 8.000 (0.000) | 7 (0.000) |
| Work-Related Stress | 16 | 6.818 (2.562) | 5.2 (2.387) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nowrouzi-Kia, B.; Garrido, P.; Gohar, B.; Yazdani, A.; Chattu, V.K.; Bani-Fatemi, A.; Howe, A.; Duncan, A.; Riquelme, M.P.; Abdullah, F.; et al. Evaluating the Effectiveness of Return-to-Work Interventions for Individuals with Work-Related Mental Health Conditions: A Systematic Review and Meta-Analysis. Healthcare 2023, 11, 1403. https://doi.org/10.3390/healthcare11101403
Nowrouzi-Kia B, Garrido P, Gohar B, Yazdani A, Chattu VK, Bani-Fatemi A, Howe A, Duncan A, Riquelme MP, Abdullah F, et al. Evaluating the Effectiveness of Return-to-Work Interventions for Individuals with Work-Related Mental Health Conditions: A Systematic Review and Meta-Analysis. Healthcare. 2023; 11(10):1403. https://doi.org/10.3390/healthcare11101403
Chicago/Turabian StyleNowrouzi-Kia, Behdin, Pablo Garrido, Basem Gohar, Amin Yazdani, Vijay Kumar Chattu, Ali Bani-Fatemi, Aaron Howe, Andrea Duncan, Maria Paz Riquelme, Faizah Abdullah, and et al. 2023. "Evaluating the Effectiveness of Return-to-Work Interventions for Individuals with Work-Related Mental Health Conditions: A Systematic Review and Meta-Analysis" Healthcare 11, no. 10: 1403. https://doi.org/10.3390/healthcare11101403