
Structural Origins of Poor Health Outcomes in Documented Temporary Foreign Workers and Refugees in High-Income Countries: A Review
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Search Strategy
2.3. Inclusion and Exclusion Criteria
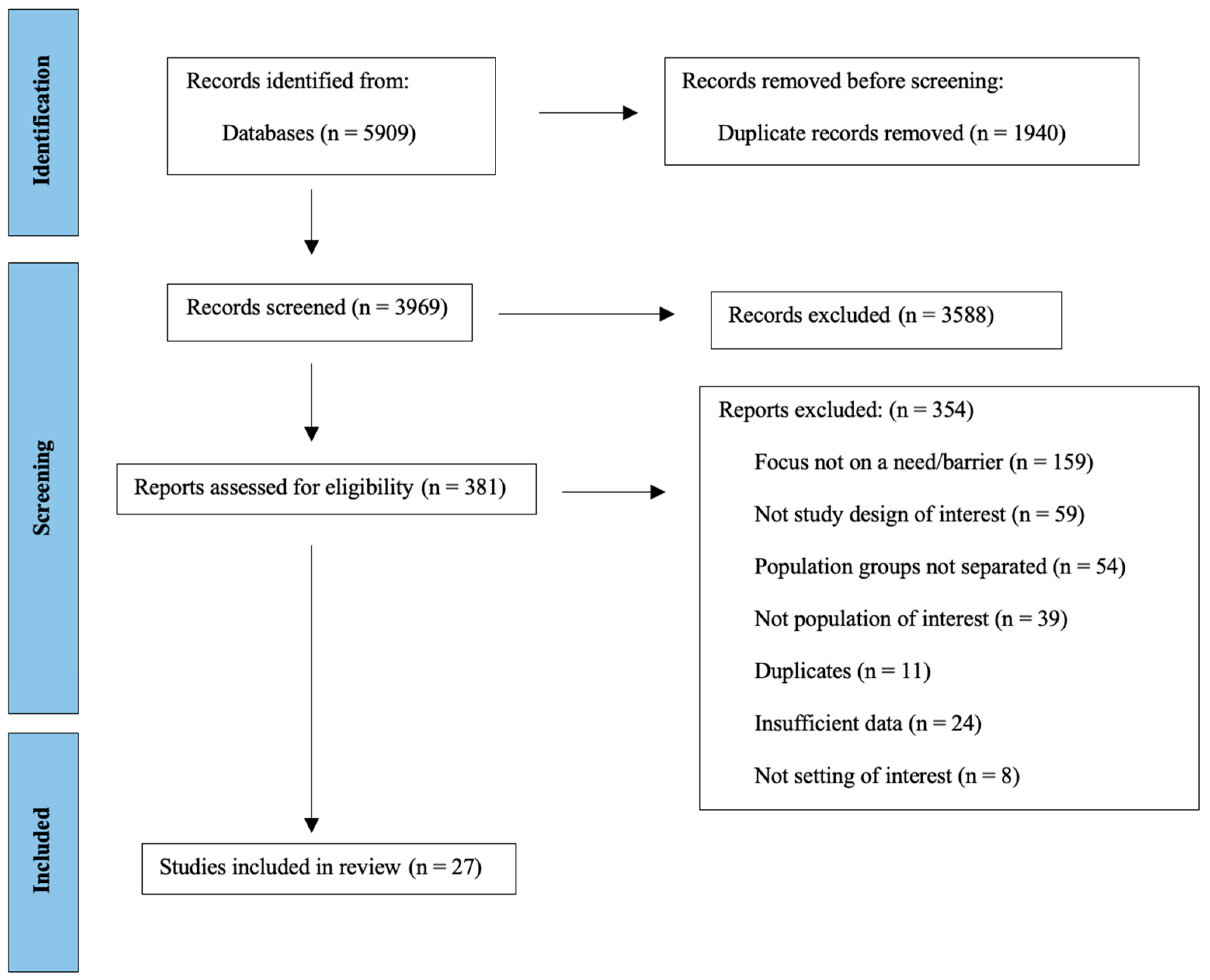
2.4. Data Selection
2.5. Data Extraction and Analysis
3. Results
3.1. Study Characteristics
3.2. Barriers for Documented Temporary Foreign Workers
3.2.1. Housing Conditions
3.2.2. Immigration Policies
3.2.3. Structural Discrimination
3.2.4. Exploitative Labour Practices
3.3. Barriers for Refugees
3.3.1. Housing Conditions
3.3.2. Immigration Policies
3.3.3. Structural Discrimination
4. Discussion
4.1. Housing Conditions
4.2. Immigration Policies
4.3. Structural Discrimination
4.4. Exploitative Labour Practices
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Documented Temporary Foreign Worker Papers Included | ||||||
|---|---|---|---|---|---|---|
| Author(s) | Year | Study Type | Study Location | Research Question | Sample Size | Main Findings |
| Bhuyan et al. [28] | 2018 | Mixed methods | Greater Toronto Area, Ontario and Calgary, Alberta, Canada | This study examined several questions including: how do migrant caregivers make sense of changes to the Canada’s caregiver policy in 2014? How do the chances impact their access to permanent residence? How does it shape their response to workplace abuse and exploitation? | 33 caregivers under the Live-in Caregiver program, Caring for Children Program, or Caring for People with High Medical Needs Program. 31 from the Philippines | This study found that despite the potential benefit of removing the “live-in” requirement, conditions of the new policy reinforced broader immigrant trends that restricted access to permanent residence and produced longer periods of precarious status. The bureaucratic management of the program forced caregivers to go for long periods without work authorization, which contributed to the production of “illegality” due to increasing financial insecurity, vulnerability for abuse and exploitation of migrant caregivers. |
| Carlos and Wilson [27] | 2018 | Qualitative | Greater Toronto Area, Ontario, Canada | The paper sought to gain insight into perceived changes in health status and access to healthcare services related to employment among a group of Filipina live-in caregivers in the Greater Toronto Area. | 21 documented temporary foreign workers (4 current live-in caregivers, 17 former live-in caregivers), all from Philippines. | The results of the study revealed that 43% of workers perceived a decline in health status postmigration, and 67% reported experiencing new physical and mental health issues. Four key aspects of caregiver work were seen to contribute to health:
|
| Caxaj and Cohen [26] | 2019 | Qualitative | British Columbia, Canada | This qualitative study intended to understand the workplace experiences of migrant agricultural workers as well as how those experiences influenced their health. | 23 seasonal agricultural worker’s program workers, 1 key informant (volunteer support person) from Mexico, Jamaica. | The study revealed 2 over-arching themes that determined workers’ health:
|
| Caxaj and Diaz [18] | 2018 | Qualitative | British Columbia, Canada | This paper intended to examine the experiences of temporary migrant agricultural workers pertaining to belonging and wellbeing in a rural setting within British Columbia, Canada. | 17 documented temporary foreign workers (seasonal agricultural worker’s program workers) from Mexico, Jamaica. | The study revealed an overarching theme of marginal living among migrant workers. Workers reported having limited access to the social and public spheres of life due to various forms of cultural and institutional exclusion. These contributed to a sense of hopelessness, anxiety, depression, and suicide. They also struggled for their basic needs, frequently facing poor housing conditions, despite housing inspections, and access to necessary hygiene. With the limited social ties and lack of work/home division, workers were seen to be vulnerable to disrespectful behavior or negative interpersonal encounters. |
| Cedillo et al. [20] | 2019 | Mixed methods | Alberta and Manitoba, Canada | This study aimed to shed light on working conditions reported by documented temporary foreign workers in Canada, and to document hazards to which these workers were exposed and the challenges they faced in exercising their OHS (Occupational Health and Safety) rights. | 22 documented temporary foreign workers (8 meat processing workers, 4 hotel workers, 6 food industry workers, 3 construction industry workers, 1 unknown) | The results revealed the presence of OHS hazards specific to sectors such as exposures to heavy workloads in the hospitality industry, breaching of work contracts in food services, and a lack of proper PPE and ergonomic hazards in construction. This study found that the workers’ migrant status and the employer’s role in applying for permanent residency was the main determinant for a worker’s inability to speak up against work and health violations. A key factor that showed a positive impact on protecting workers against abusive practices was the presence of an active union. Unionized workers in a meat-processing facility were seen to receive language support as well as assistance with filing taxes. |
| Cole et al. [30] | 2019 | Qualitative | Rural Southern Ontario, Canada | The purpose of this study was to explore rural health professionals’ perspectives on caring for migrant agricultural workers in rural Ontario, Canada. | 108 actors working in the field of migrant health (rural primary care physicians, nurse, allied healthcare professionals) | The study identified structural and intercultural challenges in providing proper care for migrant agricultural workers:
|
| Hill et al. [29] | 2019 | Qualitative | Fort McMurray, Alberta, Canada | This study looked to examine the occupational health and safety experiences of migrant workers employed as live-in caregivers in Fort McMurray, Alberta Canada. | 120 documented temporary foreign workers (live-in caregivers) | The study revealed how various occupational hazards could be traced to the organization and conditions of work and how (im)mobility could intensify them. These included federal policies that tied legal status to employers and employment, blurred relations with employers that resulted in an unpredictable and elastic scope of work, and lack of appropriate oversight. |
| Salami et al. [19] | 2018 | Qualitative | Alberta, Canada | This study examined the perspectives of the actors working in the field of migrant health on the health and well-being of documented temporary foreign workers in Alberta, Canada. | 13 actors working in the field of migrant health (7 social and immigrant service providers, 4 TFW advocates, and 2 policymakers) | The results of this study indicated that for documented temporary foreign workers, their immigration status was the single most important determinant of health. Their status determined which services workers had access to. Contributing factors were a lack of regulation, capacity, and willingness by employers to attend to workers’ health. |
| Vahabi and Wong [17] | 2017 | Mixed methods | Greater Toronto Area, Ontario, Canada | This study aimed to gain an understanding of the work-related experiences and mental health of migrant live-in caregivers in the Greater Toronto Area in Ontario, Canada. | 30 documented temporary foreign workers (live-in caregivers) Philippines, Hungary, Ukraine, Poland | This study revealed a number of key themes relating to caregivers’ experiences:
|
| Refugee Papers Included | ||||||
| Author(s) | Year | Study Type | Study Location | Research Question | Sample Size | Main Findings |
| Alwan et al. [21] | 2020 | Qualitative | Cincinnati, United States | This study sought to explore Syrian refugee parents’ beliefs, perspectives, and practices regarding their children’s health through in-depth interviews. | 18 Syrian refugees | The study found that refugees reported experiencing stressors that precluded them from seeking care and maintaining their children’s health. Stressors were both environmental and psychosocial, including poor housing and neighborhoods as well as inadequate transportation and translation services. |
| Baauw et al. [39] | 2018 | Quantitative | Netherlands | The aim of the study was to gain insight into the barriers in the healthcare for refugee children perceived by pediatricians by analyzing logistical problems reported by pediatricians through the Dutch Pediatric Surveillance Unit. | 1300 pediatricians | The study identified 74 cases of pediatrician-reported logistical problems during the care of refugee children. The barriers identified included policies and regulations that resulted in frequent relocations of refugee children. This led to missing health history, poor communication, and faulty medical handoffs that disrupted the continuity of medical care for refugee children. |
| Clark et al. [32] | 2014 | Qualitative | South Australia | This qualitative study sought to identify barriers to accessing primary healthcare services and explore medicine-related issues as experienced by refugee women in South Australia. | 38 refugees | The results found that language was a key barrier in accessing healthcare for refugees. Refugees reported an inconsistent provision of interpreters, including many occasions when they did not ask for an interpreter and an interpreter was not provided for them. This often left the children or neighbors acting as informal translators. |
| Floyd and Sakellariou [25] | 2017 | Qualitative | Vancouver, British Columbia, Canada | This study explored the lived experiences of recently arrived, government-assisted refugee women, who were nonliterate and non-English-speaking when they arrived in the country, who attempted to access healthcare services. | 8 refugees | The results illustrated the intersection of a limited knowledge of the local language with low literacy, gender, and refugee status and how it impacted women’s access to healthcare. Three themes identified from the results included dependence, isolation, and resourcefulness as factors influencing healthcare access. |
| Guruge et al. [43] | 2018 | Qualitative | Greater Toronto Area, Ontario, Canada | This study focused on exploring the healthcare needs of newcomer Syrian women, their experiences in accessing and using health services, and the factors and conditions that shaped whether and how they accessed and utilized health services in the Greater Toronto Area. | 58 refugees | Results from the study included the identification of participant’s health concerns, which included chronic conditions as well as new and emerging issues. Factors enabling access to services included initial health insurance and coverage, whereas language and social disconnection were barriers. Additionally, it was identified that beliefs about naturopathic medicine, settlement in suburban areas with limited public transportation, and lack of linguistically, culturally, and gender-appropriate services negatively affected access to and use of healthcare services. |
| Hahn et al. [23] | 2020 | Qualitative | Germany | This qualitative study intended to explore the health experiences of refugees and the experiences of healthcare professionals and administrators involved in providing refugee healthcare. | 12 refugees and 13 actors working in the field of migrant health (7 physicians, practice assistants and 6 “administrators involved in refugee matters”) | Legal, sociocultural, environmental, and communication aspects were the four main categories identified as crucial for equity in healthcare. |
| Kay et al. [41] | 2016 | Qualitative | Brisbane, Australia | This qualitative study focused on exploring the barriers to and facilitators of quality use of medicines as experienced by refugees, from the perspectives of pharmacists, general practitioners, and nurses working in the primary healthcare setting. | 12 actors working in the field of migrant health (2 GPs, 3 RNs, 4 pharmacists, 3 refugee health leaders) | Barriers identified in the results included communication barriers, cultural barriers, limited health literacy, financial cost, and systematic barriers. Additionally, facilitators of access to medicines were identified and included better coordination between healthcare providers, community engagement, providing appropriate education, and improved healthcare provider training. |
| Mirza and Heinemann [33] | 2011 | Qualitative | Midwestern United States | This qualitative study sought to examine the adequacy of service systems that existed for addressing disabled refugees’ needs who had resettled in the United States. | 15 refugees and 10 actors working in the field of migrant health (3 senior staff members at local resettlement agencies, 2 workers in refugee resource and advocacy agencies working on the international platform, 1 coordinator of refugee services at a local rehabilitation hospital, 1 staff at a local center for independent living, 3 staff at ethnic community-based organization) | Disabled refugee participants had unmet disability-related needs and poor access to resettlement resources due to their disabilities. There was a disconnect between disabled refugees and service providers, as the providers had minimal awareness about disability and lacked knowledge about the biomedical perspective, which led to mistrust, a lack of culturally safe care, and limited resources available to the refugees. |
| Newbold and McKeary [24] | 2017 | Qualitative | Hamilton, Ontario, Canada | This qualitative study explored the difficulties faced by local healthcare providers in providing care to refugee populations in the face of constantly evolving refugee policies, programs, and arrivals. | 14 actors working in the field of migrant health (executive directors, program managers, nurses, physicians, health educators, settlement workers, and community health center employees) | Results identified new challenges faced by healthcare providers, including the difficulty of providing care and services to a diverse refugee population and the lack of knowledge associated with constantly evolving policies and programs. |
| Novak et al. [40] | 2021 | Mixed methods | Australia | This mixed-methods study aimed to describe the perceptions of healthcare workers working with refugee patients at a large metropolitan public health service with respect to how they identified, managed, and cared for their patients. | 215 actors working in the field of migrant health (disciplines identified: 48 physicians, 85 nurses, 15 midwives, 50 allied heath clinicians) | The results identified potential service barriers which included insufficient identification, a lack of interpreter availability, education, healthcare worker capacity, and providing culturally specific treatment. |
| Ogunsiji et al. [37] | 2018 | Qualitative | Sydney, New South Wales, Australia | This qualitative study focused on exploring the experiences of the nursing workforce caring for refugees. | 6 actors working in the field of migrant health (refugee health nurses) | Results identified three main themes including caring for clients with challenging needs, challenges in the course of caring for refugees, and passion in caring for refugees. |
| Pejic et al. [42] | 2019 | Qualitative | Colorado, United States | This qualitative study looked at understanding the training experience of psychiatry residents working with refugees and to assess the level of satisfaction of refugees who sought psychological treatment at the University of Colorado Hospital (UCH)’s Refugee Mental Health Program of Colorado (RMHPC). | 10 refugees and 9 actors working in the field of migrant health (psychiatry residents) | Results consisted of five major themes that summarized the psychiatry resident’s experiences, including adapting practices to meet refugee needs, the value of supervision, cultural barriers, the need for extra resources, and the effect on future practice. Additionally, four major themes emerged summarizing the refugee’s experiences, including reasons for seeking treatment, barriers to treatment, a resident’s knowledge of culture and needs, and quality of treatment. |
| Richard et al. [38] | 2019 | Qualitative | Southern region of New Zealand | This qualitative study sought to explore the perspectives of primary healthcare professionals providing care to refugees through mainstream general practice. | 15 actors working in the field of migrant health (9 general practitioners and 6 practice nurses) | The results illustrated three analytical constructs including a meaningful relational engagement with refugees, appropriate refugee healthcare delivery, and a provider’s professional development shaped by complexity. |
| Shannon et al. [34] | 2016 | Mixed methods | Midwestern states, United States | This mixed-methods study examined the characteristics of successful and unsuccessful mental health referrals with respect to what providers did across diverse practice settings. | 64 actors working in the field of migrant health (social service provider, nonclinical social worker, case manager, care coordinator, mental health provider, nurse, primary care provider or nurse practitioner, school social worker) | Results separated the characteristics of both successful and unsuccessful referrals. Active care coordination, establishing trust, a proactive resolution of barriers, and culturally responsive care were facilitating successful referrals, whereas unsuccessful referrals were characterized by cultural barriers, a lack of care coordination, a refusal to see refugees, and system and language barriers. |
| Shrestha-Ranjit et al. [31] | 2020 | Qualitative | 2 regions in New Zealand | This qualitative study explored the perspectives of Bhutanese refugee women who used interpreter services in primary healthcare settings after relocation to New Zealand. | 40 refugees and 12 actors working in the field of migrant health (5 nurses, 4 general practitioners, and 3 midwives) | The results revealed inadequacies and constraints in the delivery of sociocultural and linguistically effective interpreting services to refugee women as well as provided evidence for recommendations to address these insufficiencies. |
| Vermette et al. [22] | 2015 | Qualitative | Dallas, Texas, United States | This qualitative study focused on identifying persistent barriers to healthcare access for Iraqi refugee children and potential solutions from the perspectives of parents and refugee service providers. | 24 refugees | Results highlighted that provider availability, Medicaid maintenance and renewal, language issues, and inadequate recognition of post-traumatic stress disorder were barriers to care for the children of the Iraqi families. |
| Winn et al. [36] | 2018 | Qualitative | Calgary, Alberta, Canada | This qualitative study intended to understand the experiences of healthcare professionals caring for pregnant refugee women while taking into consideration recent contextual changes to the refugee landscape in Canada. | 10 actors working in the field of migrant health (any healthcare professional who had experience caring for pregnant refugee women) | Several barriers when caring for pregnant refugees were described in the results, including language barriers, difficulty navigating the healthcare system, and cultural barriers such as managing traditional gender dynamics, only wanting a female provider, and differences in medical practices. |
| Zeidan et al. [35] | 2019 | Qualitative | Northeast United States | This qualitative study aimed to understand the barriers to accessing acute care by newly arrived refugees and identify potential improvements from refugees and resettlement agencies. | 16 refugees and 12 actors working in the field of migrant health (employees from refugee resettlement/post-resettlement agencies) | Results reported several barriers to accessing acute care, including challenges in understanding the U.S. healthcare system, difficulty scheduling timely outpatient acute care visits, significant language barriers, and confusion over the complexity of health insurance. |
References
- McAuliffe, M.; Khadria, B. Chapter 1: Report overview: Providing perspective on migration and mobility in increasingly uncertain times. In World Migration Report; International Organization for Migration, IOM: Grand-Saconnex, Switzerland, 2019; Available online: https://worldmigrationreport.iom.int/ (accessed on 10 December 2022).
- De Maio, F.G.; Kemp, E. The Deterioration of Health Status among Immigrants to Canada. Glob. Public Health 2010, 5, 462–478. [Google Scholar] [CrossRef] [PubMed]
- Ben, J.; Cormack, D.; Harris, R.; Paradies, Y. Racism and Health Service Utilisation: A Systematic Review and Meta-Analysis. PLoS ONE 2017, 12, e0189900. [Google Scholar] [CrossRef] [PubMed]
- Viruell-Fuentes, E.A.; Miranda, P.Y.; Abdulrahim, S. More than Culture: Structural Racism, Intersectionality Theory, and Immigrant Health. Soc. Sci. Med. 2012, 75, 2099–2106. [Google Scholar] [CrossRef]
- Rust, G.S. Health Status of Migrant Farmworkers: A Literature Review and Commentary. Am. J. Public Health 1990, 80, 1213–1217. [Google Scholar] [CrossRef] [PubMed]
- Bailey, Z.D.; Krieger, N.; Agénor, M.; Graves, J.; Linos, N.; Bassett, M.T. Structural Racism and Health Inequities in the USA: Evidence and Interventions. Lancet 2017, 389, 1453–1463. [Google Scholar] [CrossRef]
- Heard, E.; Fitzgerald, L.; Wigginton, B.; Mutch, A. Applying Intersectionality Theory in Health Promotion Research and Practice. Health Promot. Int. 2020, 35, 866–876. [Google Scholar] [CrossRef] [PubMed]
- Parajuli, J.; Horey, D. Barriers to and Facilitators of Health Services Utilisation by Refugees in Resettlement Countries: An Overview of Systematic Reviews. Aust. Health Rev. 2020, 44, 132–142. [Google Scholar] [CrossRef] [PubMed]
- Lane, G.; Farag, M.; White, J.; Nisbet, C.; Vatanparast, H. Chronic Health Disparities among Refugee and Immigrant Children in Canada. Appl. Physiol. Nutr. Metab. 2018, 43, 1043–1058. [Google Scholar] [CrossRef]
- Cheng, I.-H.; Drillich, A.; Schattner, P. Refugee Experiences of General Practice in Countries of Resettlement: A Literature Review. Br. J. Gen. Pract. 2015, 65, e171–e176. [Google Scholar] [CrossRef]
- Chowdhury, N.; Naeem, I.; Ferdous, M.; Chowdhury, M.; Goopy, S.; Rumana, N.; Turin, T.C. Unmet Healthcare Needs Among Migrant Populations in Canada: Exploring the Research Landscape Through a Systematic Integrative Review. J. Immigr. Minor. Health 2021, 23, 353–372. [Google Scholar] [CrossRef]
- Salami, B.; Meharali, S.; Salami, A. The Health of Temporary Foreign Workers in Canada: A Scoping Review. Can. J. Public Health 2015, 106, e546–e554. [Google Scholar] [CrossRef] [PubMed]
- Krieger, N. Discrimination and Health Inequities. Int. J. Health Serv. 2014, 44, 643–710. [Google Scholar] [CrossRef]
- Cochrane Handbook for Systematic Reviews of Interventions. Available online: https://training.cochrane.org/handbook/current (accessed on 26 July 2021).
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A Comparison Study of Specificity and Sensitivity in Three Search Tools for Qualitative Systematic Reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Thematic Analysis. In APA Handbook of Research Methods in Psychology, Volume 2: Research Designs: Quantitative, Qualitative, Neuropsychological, and Biological; Cooper, H., Camic, P.M., Long, D.L., Panter, A.T., Rindskopf, D., Sher, K.J., Eds.; American Psychological Association: Washington, DC, USA, 2012; Volume 2, pp. 57–71. [Google Scholar] [CrossRef]
- Vahabi, M.; Wong, J.P.-H. Caught between a Rock and a Hard Place: Mental Health of Migrant Live-in Caregivers in Canada. BMC Public Health 2017, 17, 498. [Google Scholar] [CrossRef] [PubMed]
- Caxaj, S.; Diaz, L. Migrant Workers’ (Non)Belonging in Rural British Columbia, Canada: Storied Experiences of Marginal Living. Int. J. Migr. Health Soc. Care 2018, 14, 208–220. [Google Scholar] [CrossRef]
- Salami, B.; Hegadoren, K.; Kirova, A.; Meherali, S.; Nsaliwa, C.; Chiu, Y. “And When a Certain Health Issue Happen, They Try to Cover It”: Stakeholder Perspectives on the Health of Temporary Foreign Workers and Their Families. Soc. Work Health Care 2018, 57, 13–26. [Google Scholar] [CrossRef]
- Cedillo, L.; Lippel, K.; Nakache, D. Factors Influencing the Health and Safety of Temporary Foreign Workers in Skilled and Low-Skilled Occupations in Canada. New Solut. J. Environ. Occup. Health Policy 2019, 29, 422–458. [Google Scholar] [CrossRef]
- Alwan, R.M.; Schumacher, D.J.; Cicek-Okay, S.; Jernigan, S.; Beydoun, A.; Salem, T.; Vaughn, L.M. Beliefs, Perceptions, and Behaviors Impacting Healthcare Utilization of Syrian Refugee Children. PLoS ONE 2020, 15, e0237081. [Google Scholar] [CrossRef]
- Vermette, D.; Shetgiri, R.; Al Zuheiri, H.; Flores, G. Healthcare Access for Iraqi Refugee Children in Texas: Persistent Barriers, Potential Solutions, and Policy Implications. J. Immigr. Minor. Health 2015, 17, 1526–1536. [Google Scholar] [CrossRef]
- Hahn, K.; Steinhauser, J.; Goetz, K. Equity in Health Care: A Qualitative Study with Refugees, Health Care Professionals, and Administrators in One Region in Germany. BioMed Res. Int. 2020, 2020, 4647389. [Google Scholar] [CrossRef]
- Newbold, B.; McKeary, M. Investigating the Diversity of Canada’s Refugee Population and Its Health Implications: Does One Size Fit All? Int. J. Migr. Health Soc. Care 2017, 13, 145–156. [Google Scholar] [CrossRef]
- Floyd, A.; Sakellariou, D. Healthcare Access for Refugee Women with Limited Literacy: Layers of Disadvantage. Int. J. Equity Health 2017, 16, 195. [Google Scholar] [CrossRef] [PubMed]
- Caxaj, C.S.; Cohen, A. “I Will Not Leave My Body Here”: Migrant Farmworkers’ Health and Safety Amidst a Climate of Coercion. Int. J. Environ. Res. Public Health 2019, 16, 2643. [Google Scholar] [CrossRef] [PubMed]
- Carlos, J.K.; Wilson, K. Migration among Temporary Foreign Workers: Examining Health and Access to Health Care among Filipina Live-in Caregivers. Soc. Sci. Med. 2018, 209, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Bhuyan, R.; Valmadrid, L.; Panlaqui, E.L.; Pendon, N.L.; Juan, P. Responding to the Structural Violence of Migrant Domestic Work: Insights from Participatory Action Research with Migrant Caregivers in Canada. J. Fam. Violence 2018, 33, 613–627. [Google Scholar] [CrossRef]
- Hill, N.S.; Dorow, S.; Barnetson, B.; Martinez, J.F.; Matsunaga-Turnbull, J. Occupational Health and Safety for Migrant Domestic Workers in Canada: Dimensions of (Im)Mobility. New Solut. J. Environ. Occup. Health Policy 2019, 29, 397–421. [Google Scholar] [CrossRef]
- Cole, D.C.; McLaughlin, J.E.; Hennebry, J.L.; Tew, M.A. Precarious Patients: Health Professionals’ Perspectives on Providing Care to Mexican and Jamaican Migrants in Canada’s Seasonal Agricultural Worker Program. Rural Remote Health 2019, 19, 5313. [Google Scholar] [CrossRef]
- Shrestha-Ranjit, J.; Payne, D.; Koziol-McLain, J.; Crezee, I.; Manias, E. Availability, Accessibility, Acceptability, and Quality of Interpreting Services to Refugee Women in New Zealand. Qual. Health Res. 2020, 30, 1697–1709. [Google Scholar] [CrossRef]
- Clark, A.; Gilbert, A.; Rao, D.; Kerr, L. “Excuse Me, Do Any of You Ladies Speak English?” Perspectives of Refugee Women Living in South Australia: Barriers to Accessing Primary Health Care and Achieving the Quality Use of Medicines. Aust. J. Prim. Health 2014, 20, 92–97. [Google Scholar] [CrossRef]
- Mirza, M.; Heinemann, A.W. Service Needs and Service Gaps among Refugees with Disabilities Resettled in the United States. Disabil. Rehabil. 2012, 34, 542–552. [Google Scholar] [CrossRef]
- Shannon, P.J.; Vinson, G.A.; Cook, T.L.; Lennon, E. Characteristics of Successful and Unsuccessful Mental Health Referrals of Refugees. Adm. Policy Ment. Health 2016, 43, 555–568. [Google Scholar] [CrossRef] [PubMed]
- Zeidan, A.J.; Khatri, U.G.; Munyikwa, M.; Barden, A.; Samuels-Kalow, M. Barriers to Accessing Acute Care for Newly Arrived Refugees. West. J. Emerg. Med. 2019, 20, 842–850. [Google Scholar] [CrossRef]
- Winn, A.; Hetherington, E.; Tough, S. Caring for Pregnant Refugee Women in a Turbulent Policy Landscape: Perspectives of Health Care Professionals in Calgary, Alberta. Int. J. Equity Health 2018, 17, 91. [Google Scholar] [CrossRef] [PubMed]
- Ogunsiji, O.; Ng Chok, H.; Mashingaidze, G.; Wilkes, L. “I Am Still Passionate despite the Challenges”: Nurses Navigating the Care for Refugees. J. Clin. Nurs. 2018, 27, 3335–3344. [Google Scholar] [CrossRef]
- Richard, L.; Richardson, G.; Jaye, C.; Stokes, T. Providing Care to Refugees through Mainstream General Practice in the Southern Health Region of New Zealand: A Qualitative Study of Primary Healthcare Professionals’ Perspectives. BMJ Open 2019, 9, e034323. [Google Scholar] [CrossRef]
- Baauw, A.; Rosiek, S.; Slattery, B.; Chinapaw, M.; van Hensbroek, M.B.; van Goudoever, J.B.; Kist-van Holthe, J. Pediatrician-Experienced Barriers in the Medical Care for Refugee Children in the Netherlands. Eur. J. Pediatr. 2018, 177, 995–1002. [Google Scholar] [CrossRef] [PubMed]
- Novak, A.; Hitch, D.; Bongiovanni, L.; Mucic, A. Identification, Management and Care of Refugee Patients at a Metropolitan Public Health Service: A Healthcare Worker Perspective. Aust. Health Rev. 2021, 45, 338–343. [Google Scholar] [CrossRef] [PubMed]
- Kay, M.; Wijayanayaka, S.; Cook, H.; Hollingworth, S. Understanding Quality Use of Medicines in Refugee Communities in Australian Primary Care: A Qualitative Study. Br. J. Gen. Pract. 2016, 66, e397–e409. [Google Scholar] [CrossRef]
- Pejic, V.; Thant, T.; Hess, R.S.; Cornell, S.; DeJesus, J.; Yager, J.; Savin, D. Learning from Our Patients: Training Psychiatry Residents in Refugee Mental Health. Acad. Psychiatry 2019, 43, 471–479. [Google Scholar] [CrossRef]
- Guruge, S.; Sidani, S.; Illesinghe, V.; Younes, R.; Bukhari, H.; Altenberg, J.; Rashid, M.; Fredericks, S. Healthcare Needs and Health Service Utilization by Syrian Refugee Women in Toronto. Confl. Health 2018, 12, 46. [Google Scholar] [CrossRef]
- Hernández, D. Affording Housing at the Expense of Health: Exploring the Housing and Neighborhood Strategies of Poor Families. J. Fam. Issues 2016, 37, 921–946. [Google Scholar] [CrossRef] [PubMed]
- Mikkonen, J.; Raphael, D. Social Determinants of Health: The Canadian Facts; York University School of Health Policy and Management: Toronto, ON, Canada, 2010. [Google Scholar]
- Paradies, Y.; Ben, J.; Denson, N.; Elias, A.; Priest, N.; Pieterse, A.; Gupta, A.; Kelaher, M.; Gee, G. Racism as a Determinant of Health: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0138511. [Google Scholar] [CrossRef] [PubMed]

| Population | Phenomenon of Interest | Context | Study Type |
|---|---|---|---|
| Documented temporary foreign workers, refugees | Health barriers | OECD high-income countries | Peer-reviewed, primary research |
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| OECD high-income country | OECD middle- or low-income country/non-OECD country |
| Documented temporary foreign worker, or refugee population | General or nonspecific migrant population (i.e., undocumented immigrants, asylum seekers, illegal migrants) |
| Focus of paper is health barriers, challenges, or needs | Paper focused on policy review, changes, or adaptations |
| Perspective of key informant or population in question | Papers focused on describing disease prevalence |
| Population of interest is the main focus of the paper | Papers focused on a topic other than healthcare needs, access, barriers, or challenges |
| Published in English | Papers published in a language other than English |
| Published between January 2011 and July 2021 | Papers published before 2011 |
| Primary research | Reviews, editorials, commentaries, letters, perspectives, news articles, presentations, conference abstracts, symposium summaries, or another type of nonprimary research |
| Documented Temporary Foreign Worker Excerpts | |
|---|---|
| Theme | Example |
| Housing conditions | “My house, the family that I live with, it’s stuffed with cameras…it is not like you do something bad to the kids but you have to all the time think about what you are doing—maybe they are not watching me but I think maybe they were; like my self-esteem goes very down and you feel, okay, no I’m not gonna do this thing because may be someone’s watching me” [17] (p. 5). Jose pays 800 dollars to live here. He suggests to the interviewer that a report be written, “a report of what the living conditions are here”. “The boss should out of obligation put a bed, a little one, for each worker. He doesn’t have [provide] anything. So I’m expected to throw myself on the ground” [18] (p. 214). |
| Immigration policies | The last thing they have in mind is their health issue. And when a certain health issue happen, they try to cover it, right? Because part of having a successful immigration application is having a positive medical exam. There’s a couple that we worked with recently, whose husband contracted a liver issue, and um, and they hid it from, you know (the doctors)? But when they were forced to take the medical exam from the doctor provided by the immigration, they failed. And that’s the basis of their denial … So the whole family is now facing deportation [19] (p. 17). |
| Structural discrimination | In Beaumont [fictional name], when we were in Beaumont, we couldn’t do [nothing]. If a black guy comes in the community or in the city or in the town of Beaumont—haven’t done anything—the cops would be coming straight to us. It was only 4 black guys […] and everyone, oh those are the Jamaicans [18] (p. 212). |
| Exploitative labour practices | I got into an accident, because they are supposed to change you every forty-five minutes or every hour to prevent any injury in your body. They are supposed to rotate all the personnel. But they left me there for four hours. So I started having a lot of pain from my neck to my back, and then my shoulder. And I was there for four hours so nobody was changing me … So I deal with them and say, you know what, I have to take some days off and [the manager of the company] told me, no, you can’t because we need you [19,20] (p. 437). I make thirty-two kidney stones, they took me to the hospital and I get surgery”. When he explained the situation to his boss and asked, without success, to work fewer hours in order to rest, “[h]e took my papers, threw them to the floor and said to me ‘your health is not my business’ …” [20] (p. 437). |
| Refugee Excerpts | |
| Theme | Examples |
| Housing conditions | We did not feel safe and secure here at all. When we first arrived we had shots fired on our home. We had to keep the windows and doors locked constantly. We did not dare to go out. Even when we needed to go out to get food, the kids would be too afraid to leave the house [21] (p. 5). |
| Immigration policies | ‘‘I don’t know what is the reason that my daughter doesn’t have Medicaid at the current time, and since two months she is without Medicaid, and she is a child, and why the Medicaid stopped. We filled application for Medicaid two times. First time they asked us to fill it again, and second time before one week we sent another application, and there is no replay or interview appointment or any thing from Medicaid office yet” [22] (p. 1531). “And of course this makes it very difficult in everyday life, so if a doctor first has to think about what the Government agencies will approve and what they will not approve, then, yes, it can be difficult for the medical side of the process” [23] (p. 3). There’s a couple of key disconnects in the [government] system [that need to be] bridged in order to actually do systems level planning for the intake of refugees […] two key disconnects […] are the fact that refugee intake is a federal issue, [while] provision of health and social services is a provincial issue and they’re just not linked [24] (p. 152). |
| Structural discrimination | The doctor was an old man and when he see our ID [identification card], he said, “oh, from Sudan. Oh, Sudanese, they are the worst people” … I felt really bad. I’m a human like them. I have everything; the only thing that I cannot understand is language [25] (p. 5). |
| Challenge | Refugees | Temporary Foreign Workers |
|---|---|---|
| Housing conditions | X | X |
| Immigration policies | X | X |
| Structural discrimination | X | X |
| Exploitative labour practices | X |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, B.; Kelly, C.; Shamputa, I.C.; Barker, K.; Thi Kim Nguyen, D. Structural Origins of Poor Health Outcomes in Documented Temporary Foreign Workers and Refugees in High-Income Countries: A Review. Healthcare 2023, 11, 1295. https://doi.org/10.3390/healthcare11091295
Yang B, Kelly C, Shamputa IC, Barker K, Thi Kim Nguyen D. Structural Origins of Poor Health Outcomes in Documented Temporary Foreign Workers and Refugees in High-Income Countries: A Review. Healthcare. 2023; 11(9):1295. https://doi.org/10.3390/healthcare11091295
Chicago/Turabian StyleYang, Borum, Clara Kelly, Isdore Chola Shamputa, Kimberley Barker, and Duyen Thi Kim Nguyen. 2023. "Structural Origins of Poor Health Outcomes in Documented Temporary Foreign Workers and Refugees in High-Income Countries: A Review" Healthcare 11, no. 9: 1295. https://doi.org/10.3390/healthcare11091295