
Prevalence and Risk Factors of Musculoskeletal Disorders in Basketball Players: Systematic Review and Meta-Analysis

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
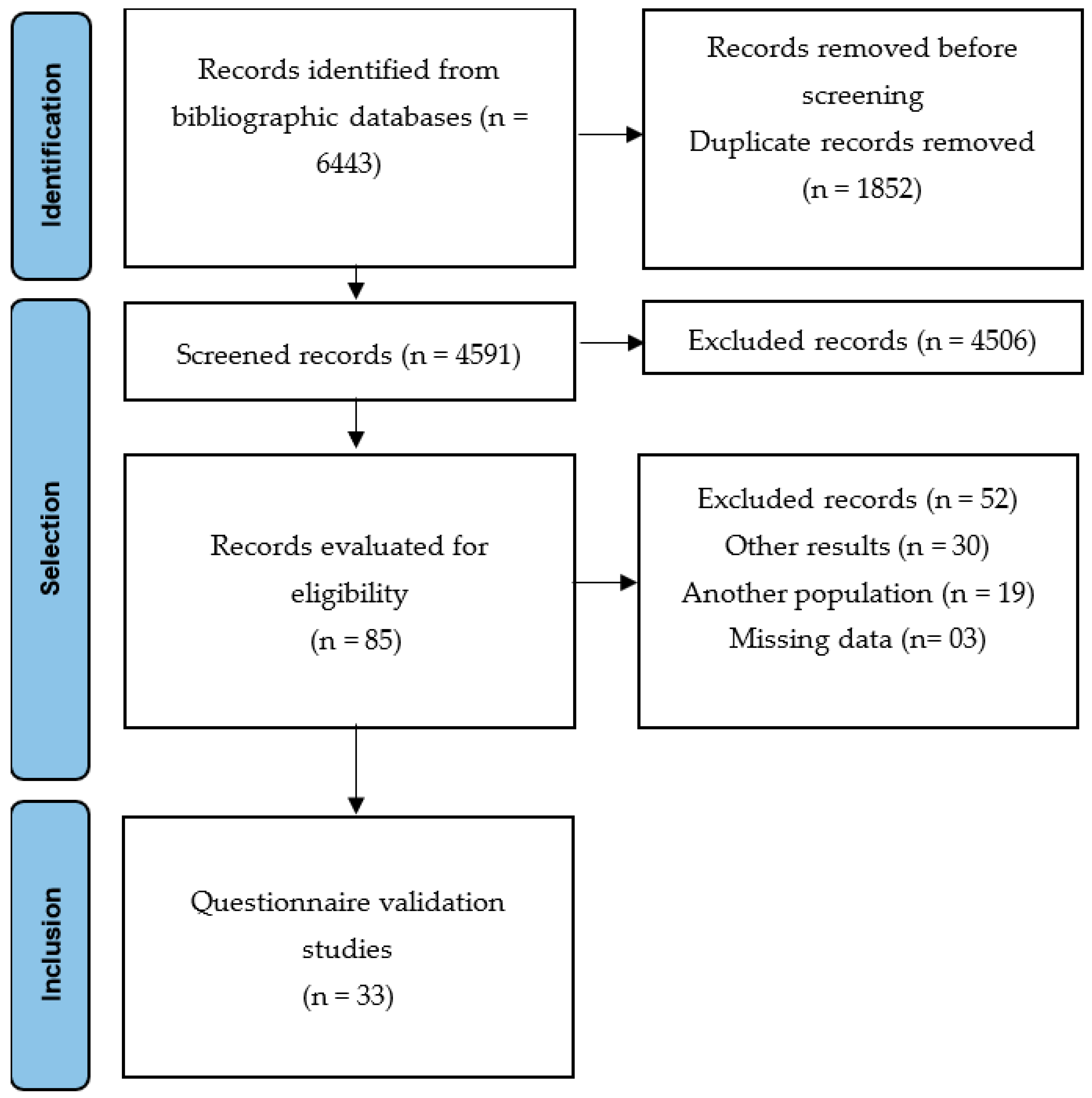
2.2. Identification of Relevant Studies

| 1 | (“musculoskeletal disorder” OR “musculoskeletal disorders” OR “musculoskeletal disease” OR “musculoskeletal diseases” OR “musculoskeletal injuries” OR “musculoskeletal injury” OR posture OR “postural evaluation” OR “postural changes” OR scoliosis OR kyphosis OR lordosis OR spondylolysis OR “back pain” OR “low back pain” OR “back injuries” OR “lumbar pain” OR “neck pain” OR “spinal pain” OR “abnormalities in spine” OR “spine pain” OR “cervical pain” OR backache OR backaches OR “back ache” OR “back aches” OR “cumulative trauma disorders”) |
| 2 | (players OR player OR sportsman OR athletes OR athlete OR sportsmen OR sportswoman OR sportswomen) |
| 3 | (basket OR basketball OR sports OR sport) |
| 4 | (1) AND (2) AND (3) |
2.3. Study Selection
2.4. Data Extraction
2.5. Examiner Training
2.6. Methodological Quality and Risk of Bias
2.7. Statistical Analysis
3. Results
3.1. Risk of Bias and Evaluation of the Quality of Studies
3.2. Main Characteristics of the Studies
| Author/Year | Design Country | No. Participants (% Male) | Age (Years/Mean and Standard Deviation) | Training Level | Tool | Postural Changes/Prevalence | Spine Injuries/Prevalence | Definition of Back Pain | Pain Location/Prevalence |
|---|---|---|---|---|---|---|---|---|---|
| Abdollahi et al. [51] | Retrospective Iran | 204 (100%) | 26.37 ± 7.42 | Professional Super League and First Division League | Retrospective Injury Questionnaire (RIQ) | * | Upper back injury: 6.38% Lumbar injury: 48.53% | * | * |
| Auvinen et al. [37] | Cross-sectional Finland | 4314 (51.5%) | 15 to 16 years | Moderate to vigorous Up to once a month, 2–4 times a month, and at least twice a week | Questionnaire | * | * | * | All: 88.5%, up to once a month 24.6%, 2–4 times a month; 9.4%, at least twice a week Neck pain: 44.5%, up to once a month (reference group) 12.2%, 2–4 times a month 4.7%, at least twice a week Backache: 44.3%, up to once a month (reference group) 12.4%, 2–4 times a month −4.7%, at least twice a week. |
| Farahbakhsh et al. [7] | Cross-sectional Iran | 52 (100%) | 16.1± 1.1 years | Hours/week 11.6± 8.2 | Questionnaire | * | * | Point prevalence, Prevalence of chronic pain Yearly prevalence, Sports-lifePrevalence, Lifetime prevalence | Total: Point prevalence 61.6% (N = 32) Prevalence of chronic pain 28.8% Neck pain: 36.53% 13.46% 36.53% 46.15% 57.69%. Low back pain: 25% 15.38% 50% 65.38% 63.46% |
| Grabara [52] | Cross-sectional Poland | 52 (57.7%) | 14 to 17 years | Training experience [years] 4.05 ± 0.58 | Rippstein plurimeter | Hyperkyphosis: 21.2% Hypolordosis: 42.3% Hyperlordosis: 13.4% | * | * | * |
| Grabara [16] | Longitudinal Follow-up: 2 years Poland | 10 (100%) | 13–15 years | Training over a 2-year period | Plurimeter-V Gravity Inclinometer | Hyperkyphosis: 70% in almost 3 months after engagement in regular sports activity 70% after 1 year 60% after 2 years Hypokyphosis: 0% in almost 3 months after engaging in regular sports activity 20% after 1 year 10% after 2 years Hyperlordosis: 0% in almost 3 months after engaging in regular sports activity 10% after 1 year 0% after 2 years Hypolordosis: 70% in nearly 3 months after engaging in regular sports activity 30% after 1 year 50% after 2 years | * | * | * |
| Greene et al. [53] | Cross-sectional Follow-up: 1 year United States | 33 (57.6%) | 19 ± 1 years | College athletes | 16-item questionnaire | * | Low back injury: Injury during the 1999/2000 season 18.2% History of low back injury in the last 5 years 27.3% | * | * |
| Habelt et al. [39] | Longitudinal Follow-up: 10 years Switzerland | 168 (100%) | 10–19 years | * | Clinical examination, Radiographic assessment (anteroposterior and lateral view), ultrasound, or MRI scan. | * | Spine injury: 1.8% | * | * |
| Hagiwara et al. [38] | Cross-sectional Japan | 590 (56.1%) | 6–15 years | Training per day on weekends (hours) ≤3304 (51.5) and >3286 (48.5) | Self-reported questionnaires | * | * | * | Low back pain: 12.9% |
| Hangai et al. [54] | Cross-sectional Japan | 63 (69.8%) | 19.7 ± 0.9 years | Athletes’ career time (years) 9.2 ± 1.8 | MRI and clinical examination/Self-reported questionnaire | * | Disk Degeneration: 42.9% | * | Low back pain: during life: 81% During the previous 4 weeks: 17.7% |
| Hickey et al. [59] | Cross-sectional Australia | 49(0%) | 16–18 years | Young elite women’s basketball players | Medical records | * | Disk-related pain, spondylolysis, and acute fracture of a lumbar transverse process: 14.9% | Mechanical/facet joint-related low back pain Acute-chronic | Low back pain: 6.3% |
| Ichikawa et al. [55] | Cross-sectional Japan | 16 male and female athletes | * | * | Radiography | * | Spondylolysis: 12.5% | * | Low back pain: 25% |
| Iwamoto et al. [43] | Retrospective 14-year period Japan | 1229 (55.2%) | 11–49 years | Class 2 = low recreational: sports activity once or twice a week; Class 3 = high recreational: sports activity; >3 times/week, and belonging to an elementary or high school team or other sports team; Class 4 = competitive: competitive sports activity and belonging to a professional, semi-professional, or university sports team | Radiographies or MRI/Database | * | Lumbar disc disease: 6.6.% Lumbar Spondylolysis: 2% | Non-traumatic pain | Low back pain: 2.9% |
| Keene et al. [44] | Cross-sectional United States | 216 (male and female athletes) | * | College athletes | Review of training room medical records and hospital files | * | Total: 5.6% Strain: 5.1% Sprain: 0.5% | * | * |
| Kerr et al. [45] | Cross-sectional United States | 19,991 (61.5%) | Athlete exposure was defined as the participation of 1 athlete in 1 school-sanctioned training or competition | Online Injury Surveillance System: Reporting Information Online | * | Trunk Displacements/Separations: 12.9% M = 7.7% F = 5.2% | * | * | |
| Leppänen et al. [46] | Prospective Study Finland | 201 (49.7%) | 15.7 ± 1.7 years | College athletes | Questionnaire including information such as age, sex, injury history, playing experience, and family history of musculoskeletal disorders | * | Muscle/tendon: 26.9% Joint/ligament: 4.5% Bone injury: 5.5% | * | Low back pain: 9.95% |
| Meron et al. [41] | Cross-sectional United States | 5,566,124 (55.6%) | * | An athlete exposure was defined as an athlete (154) participating in one practice, competition, or performance | High School Reporting Information Online injury surveillance system | * | Cervical spine injury: 0.0006% | * | * |
| Nagano et al. [56] | Prospective study Japan | 54 (0%) | 19.0 ± 2.8 years | College athletes | Modified Japanese version of the OSTRC questionnaire | * | * | * | Backache: 14.4% |
| Noormohammadpour et al. [11] | Cross-sectional Iran | 140 (0%) | 22.7 ± 2.7 years | Female college athletes competing in the National College Student Sports Olympics | Self-reported questionnaire | * | * | Point prevalence Yearly prevalence Sports-life Prevalence Lifetime Prevalence | Low back pain: 22.9% 47.9% 48.6% 68.6% |
| Nowak et al. [57] | Cross-sectional Poland | 58 (100%) | 17 ± 1.4 years | Professional players (club players), amateur league (amateur players) | Original questionnaire consisting of 28 items | * | Neck injury and back injury: 12.1% | * | * |
| Owen et al. [58] | Cross-sectional Japan | 63 male and female athletes | 20 ± 1 years | Well-trained male and female athletes who have spent a minimum of 5 years playing the sport | Subjective questionnaire | * | * | * | Back pain: 1.6% |
| Pasanen et al. [47] | Cross-sectional Finland | 207 (48.8%) | 14.9 ± 1.6 years | Young players that were official members of participating teams and had played official games in the previous season. | Questionnaire based on the Nordic standardized musculoskeletal symptoms questionnaire and on its modified version for athletes. | * | * | * | Low Back Pain: 45.4% |
| Rossi et al. [48] | Cross-sectional A retrospective analysis Italy | 174 male and female athletes | 15–27 years | Athletes referred to the Institute of Sport Sciences of the Italian Olympic Committee | Radiographic findings | * | Spondylolysis with low back pain: 9.77% | * | * |
| Rossi et al. [49] | Longitudinal 3-year follow-up Finland | 203 (49.3%) | 14.9 ± 1.6 years | Training hours (mean, standard deviation): 215.1 (102.9) | Nordic standardized questionnaire on musculoskeletal symptoms/modified version for athletes | * | * | Non-traumatic Acute Traumatic / AcuteTraumatic | Total: 11.9% Low back pain: 8.4% 3% Back pain: 0.5% |
| Rossi et al. [10] | Longitudinal 3-year follow-up Finland | 271 male and female athletes | 16.2 ± 1.7 years | Hours of team practice during follow-up, average hours: 244.8 | Nordic standardized questionnaire on musculoskeletal symptoms/modified version for athletes | * | * | * | Low back pain: 46% |
| Rossi et al. [50] | Prospective cohort study Finland | 128 male and female athletes | 14.7 ± 1.5 years | Elite basketball players | Nordic standardized questionnaire of musculoskeletal symptoms | * | * | * | Low back pain: 25% |
| Sarcevic and Tepavcevic [33] | Case-control Serbia | 38 male and female athletes Group of cases: 19 Control group: 19 | 11.5 ± 2.1 years 11.7 ± 1.9 years | Physical activity level, hours per week 3.03 ± 0.55, 3.04 ± 0.64 | Checkup-Adams’ forward Bend test and scoliometer measurement | Adolescent idiopathic scoliosis: 100% | * | * | * |
| Schneider et al. [42] | Cross-sectional Germany | 182 (70.9%) | 15.5 ± 1.3 years | Elite youth basketball players from Germany’s three elite youth leagues | Sets of items from a previously validated and tested questionnaire | * | * | * | Back pain: 7 days: 34.3% 12-month prevalence rates: 70.9% More intense pain: 16.4% Neck pain: 7 days: 26.5% 12-month prevalence rates: 65.2% More intense pain: 6.1% |
| Schulz et al. [34] | Cross-sectional Germany | 11 (18.2%) | 19 years old | Basketball played 20.6 h per week | Self-developed survey with 59 items | * | * | * | Back pain: 54.5% |
| Selhorst et al. [40] | Cross-sectional United States | 194 (60.3%) | 15.0 ± 1.8 years | * | Radiographies | * | Spondylolysis: 33% | * | * |
| Silva et al. [35] | Longitudinal Brazil | 66 (0%) | 23 years | Elite Women’s Basketball Athletes. The teams played on average twice a week, and trained on average five times a week, which resulted in 76 matches and 375 training sessions. | Injury data were recorded by a physical therapist | * | Low back/back/neck injury: 33.3% | * | Low back pain: 12.1% |
| Trompeter et al. [8] | Cross-sectional Germany | 518 (46.5%) | 20.9 ± 4.8 years | Elite German athletes participating in the German Confederation of Olympic Sports | The questionnaire was based on the Nordic Questionnaire and a questionnaire developed by von Korff | * | * | Lifetime prevalence; 12-month prevalence; Point prevalence | Back pain: 91% 91% 67% Low back pain: 91% 86% 43% |
| Weiss et al. [36] | Prospective cohort study 24-week follow-up New Zealand | 13 (100%) | 24.4 ± 4.7 years | Competitive experience, 5.9 ± 3.6 years | Self-reported OSTRC injury questionnaire | * | Excessive use of lower back: 15.4% | * | * |
| Yabe et al. [6] | Cross-sectional Japan | 592 (56.1%) | 12–14 years | Training per day during the week: 2 h on average | Self-reported questionnaire | * | * | * | Low back pain: 12.8% |
| Study (Year) | Conflicts of Interest | Ethical Approval | Downs and Black Checklist | GRADE | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Total | Score # | ||||
| Abdollahi et al. [51] | No | * | 1 | 1 | 1 | 1 | 1 | 1 | - | 1 | 1 | 1 | - | 1 | 1 | - | 1 | - | 12/12 | 100% |  |
| Auvinen et al. [37] | No | Yes | 1 | 1 | 1 | 1 | 1 | 1 | - | 1 | 1 | 1 | - | 1 | 1 | - | 1 | - | 12/12 | 100% |  |
| Farahbakhsh et al. [7] | No | Yes | 1 | 1 | 1 | 0 | 1 | 1 | - | 1 | 0 | 0 | - | 1 | 1 | - | 1 | - | 9/12 | 75% |  |
| Grabara [52] | * | Yes | 1 | 1 | 1 | 0 | 1 | 1 | - | 0 | 0 | 0 | - | 1 | 1 | - | 0 | - | 7/12 | 58.3% |  |
| Grabara [16] | No | Yes | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 12/16 | 75% |  |
| Greene et al. [53] | * | Yes | 1 | 1 | 1 | 0 | 1 | 0 | - | 1 | 0 | 0 | - | 1 | 1 | - | 0 | - | 7/12 | 58.3% |  |
| Habelt et al. [39] | * | * | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 12/16 | 75% |  |
| Hagiwara et al. [38] | No | Yes | 1 | 1 | 1 | 1 | 1 | 1 | - | 1 | 1 | 1 | - | 1 | 1 | - | 1 | - | 12/12 | 100% |  |
| Hangai et al. [54] | No | Yes | 1 | 1 | 1 | 1 | 1 | 1 | - | 1 | 0 | 1 | - | 1 | 1 | - | 1 | - | 11/12 | 91.7% |  |
| Hickey et al. [59] | * | Yes | 1 | 1 | 1 | 0 | 1 | 0 | - | 0 | 1 | 1 | - | 1 | 1 | - | 0 | - | 8/12 | 66.7% |  |
| Ichikawa et al. [55] | * | * | 1 | 1 | 0 | 0 | 1 | 1 | - | 0 | 0 | 1 | - | 1 | 1 | - | 0 | - | 7/12 | 58.3% |  |
| Iwamoto [43] | * | * | 1 | 1 | 1 | 1 | 1 | 1 | - | 1 | 1 | 1 | - | 1 | 1 | - | 0 | - | 11/12 | 91.7% |  |
| Keene et al. [44] | * | * | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 13/16 | 81.3% |  |
| Kerr et al. [45] | No | Yes | 1 | 1 | 1 | 0 | 1 | 1 | - | 1 | 1 | 1 | - | 1 | 1 | - | 0 | - | 10/12 | 83.3% |  |
| Leppänen et al. [46] | No | Yes | 1 | 1 | 1 | 0 | 1 | 0 | - | 1 | 1 | 1 | - | 1 | 1 | - | 1 | - | 10/12 | 83.3% |  |
| Meron et al. [41] | * | Yes | 1 | 1 | 1 | 0 | 1 | 1 | - | 1 | 1 | 1 | - | 1 | 1 | - | 0 | - | 10/12 | 83.3% |  |
| Nagano et al. [56] | No | Yes | 1 | 1 | 1 | 0 | 1 | 0 | - | 1 | 0 | 0 | - | 1 | 1 | - | 1 | - | 8/12 | 66.7% |  |
| Noormohammadpour et al. [11] | No | Yes | 1 | 1 | 1 | 1 | 1 | 1 | - | 1 | 1 | 1 | - | 1 | 1 | - | 1 | - | 12/12 | 100% |  |
| Nowak et al. [57] | * | * | 1 | 1 | 1 | 0 | 1 | 1 | - | 1 | 0 | 1 | - | 1 | 1 | - | 0 | - | 9/12 | 75% |  |
| Owen et al. [58] | No | Yes | 1 | 1 | 1 | 1 | 1 | 1 | - | 1 | 1 | 1 | - | 1 | 1 | - | 1 | - | 12/12 | 100% |  |
| Pasanen et al. [47] | * | Yes | 1 | 1 | 1 | 0 | 1 | 1 | - | 1 | 1 | 1 | - | 1 | 1 | - | 1 | - | 11/12 | 91.7% |  |
| Rossi et al. [48] | * | * | 1 | 1 | 1 | 0 | 1 | 0 | - | 0 | 1 | 1 | - | 1 | 1 | - | 0 | - | 8/12 | 66.7% |  |
| Rossi et al. [49] | * | Yes | 1 | 1 | 1 | 1 | 1 | 1 | - | 1 | 1 | 1 | - | 1 | 1 | - | 1 | - | 12/12 | 100% |  |
| Rossi et al. [10] | No | Yes | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 15/16 | 93.8% |  |
| Rossi et al. [50] | No | Yes | 1 | 1 | 1 | 0 | 1 | 1 | - | 1 | 1 | 1 | - | 1 | 1 | - | 1 | - | 11/12 | 91.7% |  |
| Sarcevic et al. [33] | No | Yes | 1 | 1 | 1 | 1 | 1 | 1 | - | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | - | 12/14 | 85.7% |  |
| Schneider et al. [42] | * | Yes | 1 | 1 | 1 | 0 | 1 | 1 | - | 1 | 1 | 1 | - | 1 | 1 | - | 0 | - | 10/12 | 83.3% |  |
| Schulz et al. [34] | No | * | 1 | 1 | 1 | 0 | 1 | 1 | - | 1 | 1 | 0 | - | 1 | 1 | - | 0 | - | 9/12 | 75% |  |
| Selhorst et al. [40] | * | * | 1 | 1 | 1 | 0 | 1 | 0 | - | 1 | 1 | 1 | - | 1 | 1 | - | 0 | - | 9/12 | 75% |  |
| Silva et al. [35] | * | Yes | 1 | 1 | 1 | 0 | 1 | 0 | - | 1 | 0 | 1 | - | 1 | 1 | - | 0 | - | 8/12 | 66.7% |  |
| Trompeter et al. [8] | * | * | 1 | 1 | 0 | 0 | 1 | 1 | - | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | - | 10/14 | 71.4% |  |
| Weiss et al. [36] | No | Yes | 1 | 1 | 1 | 0 | 1 | 1 | - | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | - | 11/14 | 78.6% |  |
| Yabe et al. [6] | No | Yes | 1 | 1 | 1 | 1 | 1 | 1 | - | 1 | 1 | 0 | - | 1 | 1 | - | 1 | - | 11/12 | 91.7% |  |
| Characteristics | Categories | Number of Studies (%) |
|---|---|---|
| Year of Publication | 1982–2000 | 3 (9.0%) |
| 2001–2010 | 6 (18.2%) | |
| 2011–2022 | 24 (72.7%) | |
| Region | ||
| America | Brazil USA | 1 (3.1%) 5 (15.2%) |
| Africa | - | - |
| Asia | Iran Japan | 3 (9%) 7 (21.1%) |
| Europe | Germany | 3 (9%) |
| Poland | 3 (9%) | |
| Finland | 6 (18.1%) | |
| Switzerland | 1 (3.1%) | |
| Italy | 1 (3.1%) | |
| Serbia | 1 (3.1%) | |
| Oceania | Australia New Zealand | 1 (3.1%) 1 (3.1%) |
| Study design | Case-control | 1 (3.1%) |
| Retrospective | 2 (6%) | |
| Prospective | 4 (12.1%) | |
| Longitudinal | 5 (15.2%) | |
| Cross-sectional | 21 (63.6%) | |
| Sex | Male only | 6 (18.2%) |
| Female only | 4 (12.1%) | |
| Both sexes | 23 (69.7%) | |
| Sample size | <100 | 15 (45.5%) |
| 100–500 | 12 (36.4%) | |
| 501–1000 | 2 (6%) | |
| >1000 | 4 (12.1%) | |
| Participants | Postural changes | 3 (9.1%) |
| Back pain and spine injuries | 6 (18.2%) | |
| Spine injuries | 10 (30.3%) | |
| Back pain | 14 (42.4%) |
| Author | Associated Factors |
|---|---|
| Auvinen et al. [37] | - |
| Farahbakhsh et al. [7] | The highest risk of neck pain at all times was observed among basketball players compared to other sports groups (p < 0.05; OR [95% CI 1.54–7.25]). |
| Grabara [52] | - |
| Grabara [16] | - |
| Greene et al. [53] | - |
| Habelt et al. [39] | - |
| Hagiwara et al. [38] | Upper limb pain was significantly associated with low back pain (OR: 7.86 [95% CI 3.93–15.72], p < 0.001). Shoulder pain was significantly associated with training per week (>4 days) (OR: 4.15; 95% CI: 1.29–13.40) and low back pain (OR: 13.77 [95% CI 5.70–33.24], p < 0.001). |
| Hangai et al. [54] | Logistic regression analysis of participants with disc degeneration, including a basketball group, adjusted for sex and obesity (OR: 1.61 [95% CI 0.78–3.35], p = 0.1982) |
| Hickey et al. [59] | - |
| Ichikawa et al. [55] | - |
| Iwamoto et al. [43] | - |
| Keene et al. [44] | - |
| Kerr et al. [45] | - |
| Leppãnen et al. [46] | Female players had a higher incidence of overuse injuries compared to male basketball players (IRR 1.61 [95% CI 1.07–2.46], p < 0.05. Previous injury was significantly associated with low-back overuse injuries in basketball and floorball players (OR 3.99 [CI 1.48–10.78], p = 0.01) |
| Meron et al. [41] | For sports that allow comparison between the sexes, females had higher basketball injury rates (RR, 2.02 [CI 1.01–4.03], p < 0.05) |
| Nagano et al. [56] | - |
| Noormohammadpour et al. [11] | - |
| Nowak et al. [57] | The differences in stretching before a workout or game between players training up to three times a week and players training four or more times a week were statistically significant (χ2 = 8.926, p = 0.012, V = 0.392) |
| Owen et al. [58] | After matching participants based on the status of back pain and height, basketball players showed signs of intervertebral disc hypertrophy (p ≤ 0.043) |
| Pasanen et al. [47] | Family history of musculoskeletal disorders (OR 2.02 [95% CI 1.22–3.34]) and higher age (OR 1.22 [95% CI 1.05–1.41]) were associated with low back pain in basketball and floorball players. |
| Rossi and Dragoni [48] | - |
| Rossi et al. [49] | - |
| Rossi et al. [10] | There was a small increase in the risk of low back pain with a one-degree decrease in the right leg during the SLVDJ landing (HR 1.09 [95% CI 1.02–1.17] per one-degree decrease in the APF). Basketball and floorball players. All LBP Femur–pelvic angle, right side HR 1.09 (1.02–1.17) 0.014 Gradual onset non-traumatic LBP Femur–pelvic angle, right side HR 1.09 (1.01 to 1.18) 0.021 |
| Rossi et al. [50] | None of the risk factors investigated were associated with low back pain in univariate Cox analyses. |
| Sarcevic and Tepavcevic [33] | - |
| Schneider et al. [42] | - |
| Schulz et al. [34] | - |
| Selhorst et al. [40] | Presence of spondylolysis in male basketball athletes RR (95% CI) = 1.05 (0.89–1.24) Presence of spondylolysis in female basketball athletes RR (95% CI) = 0.98 (0.86–1.12) Overall: Male athletes were 1.5 times more likely to have spondylolysis than female athletes (p = 0.01). |
| Silva et al. [35] | Older athletes were more likely to have consecutive injuries than younger athletes during the study period. This comparison was statistically significant (p = 0.010). |
| Trompeter et al. [8] | Among basketball players, these problems, along with a high frequency of jumping and landing, can lead to back pain. Compared with control subjects, significantly higher rates of back pain were found in those who participated in elite rowing, dancing, fencing, gymnastics, underwater rugby, water polo, shooting, basketball, field hockey, track and field, ice hockey, and figure skating. |
| Weiss et al. [36] | The mean weekly prevalence of all reported overuse conditions was 63% (95% CI 60–66), and that of severe overuse conditions was 7.3% (95% CI: 7.1–7.6). |
| Yabe et al. [6] | Participants with lower extremity pain had higher rates of low back pain, with an OR (95% CI) of 6.21 (3.57–10.80), than participants without lower extremity pain. Moreover, there was a significant association between knee/ankle pain and low back pain. Compared with participants without knee/ankle pain, the OR (95% CI) for low back pain was 4.25 (2.55–7.07) for participants with knee pain and 3.79 (2.26–6.36) for participants with ankle pain. |
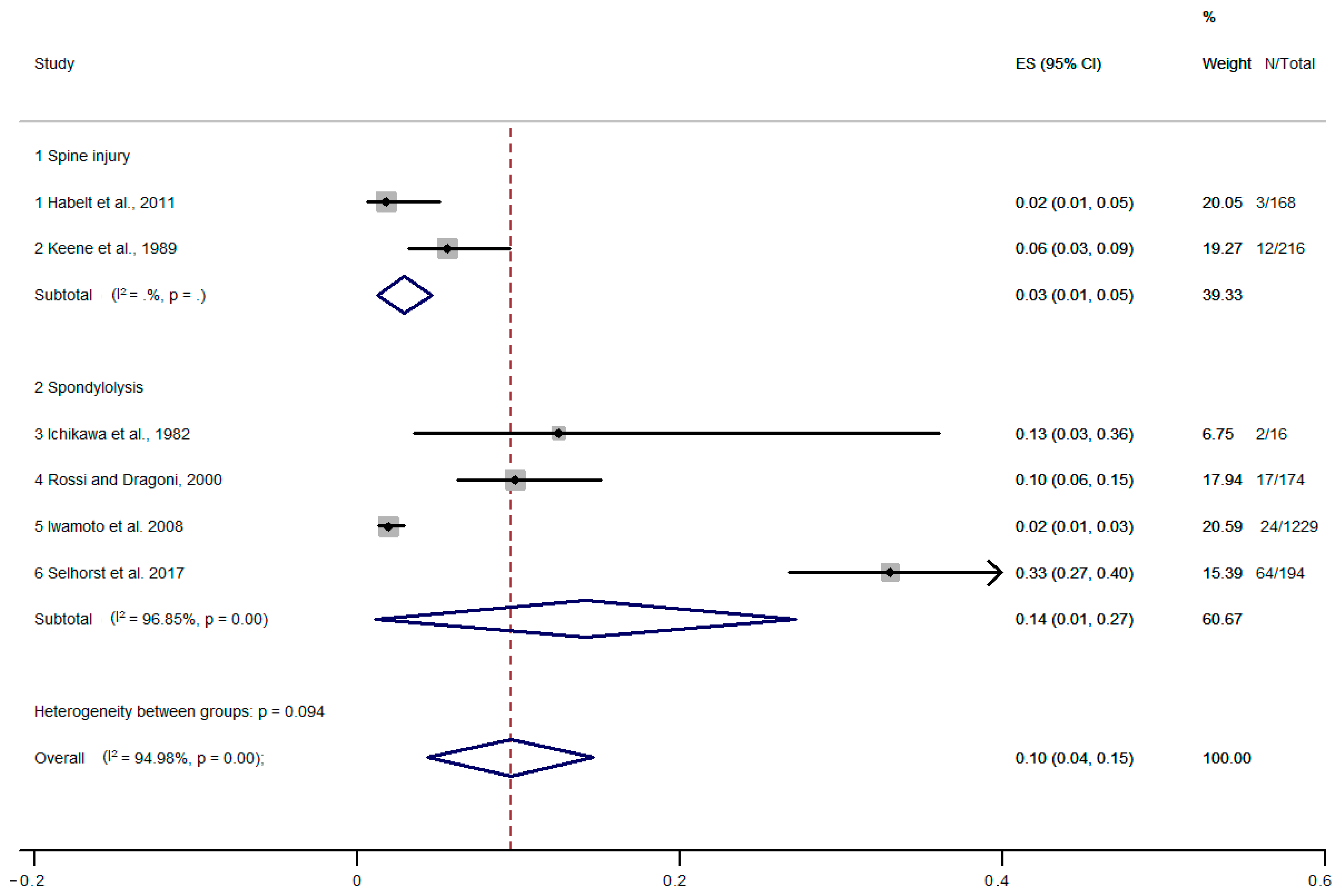
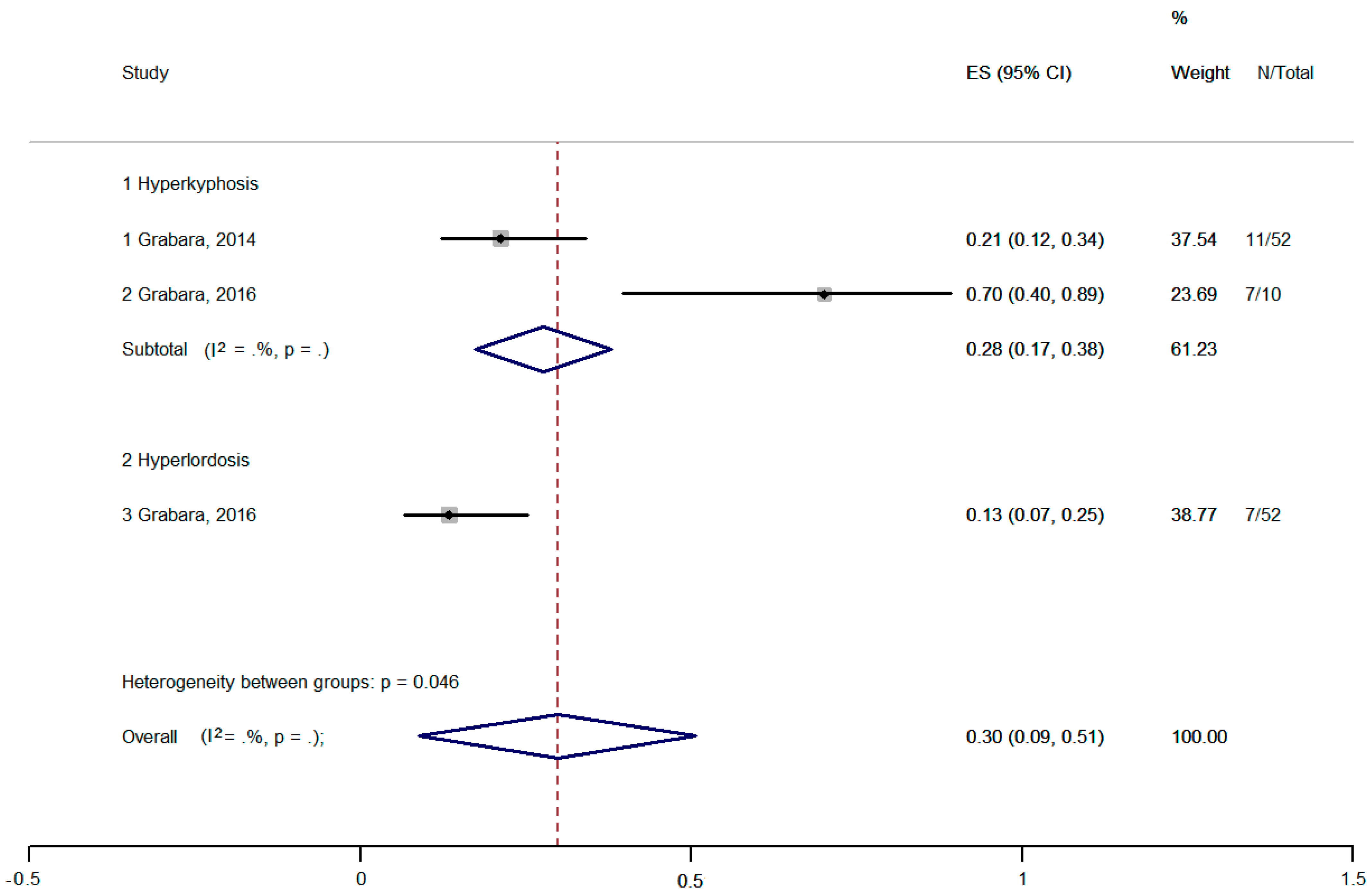
3.3. Assessment of the Prevalence of Spinal Injuries and Postural Changes
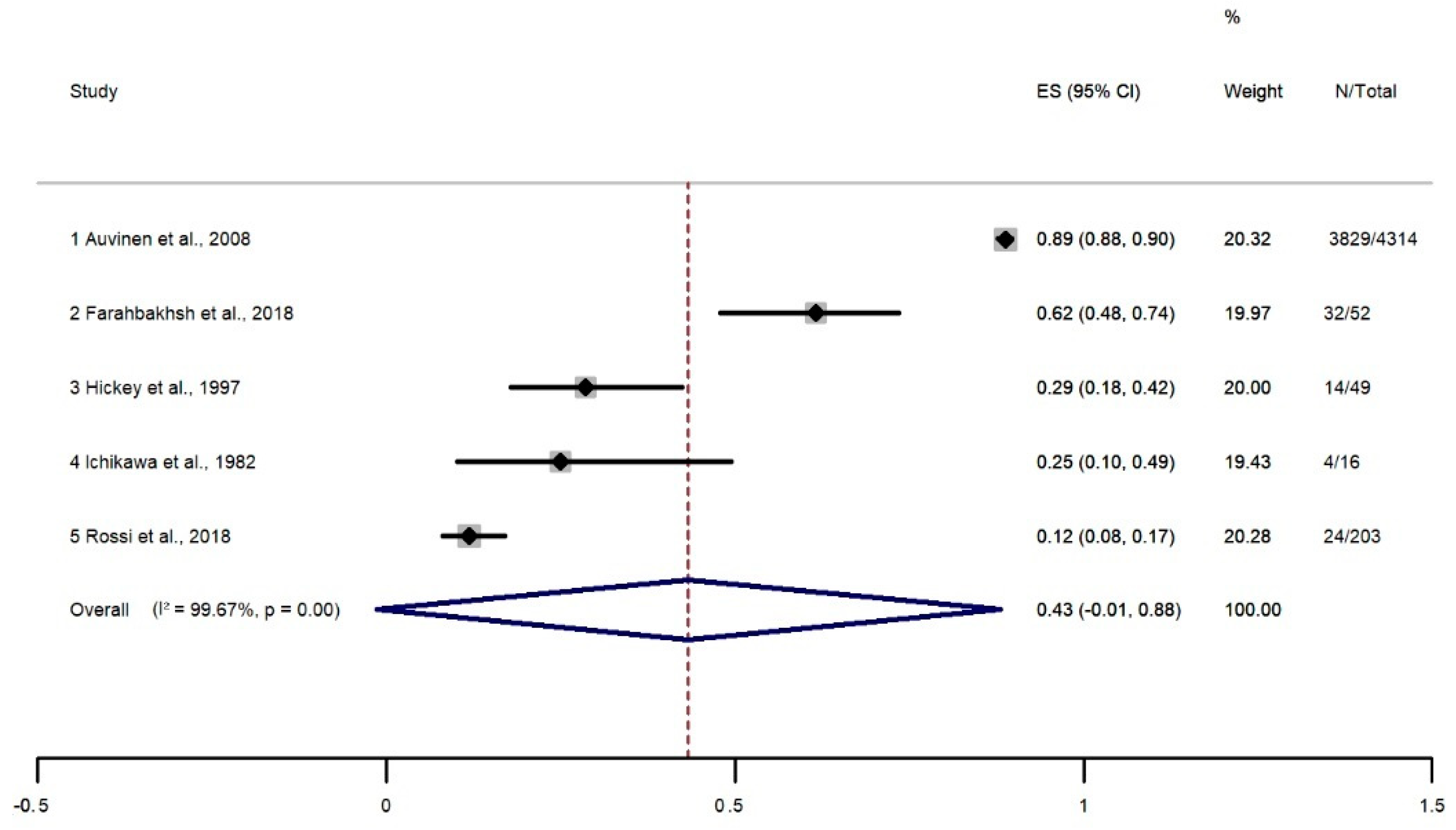
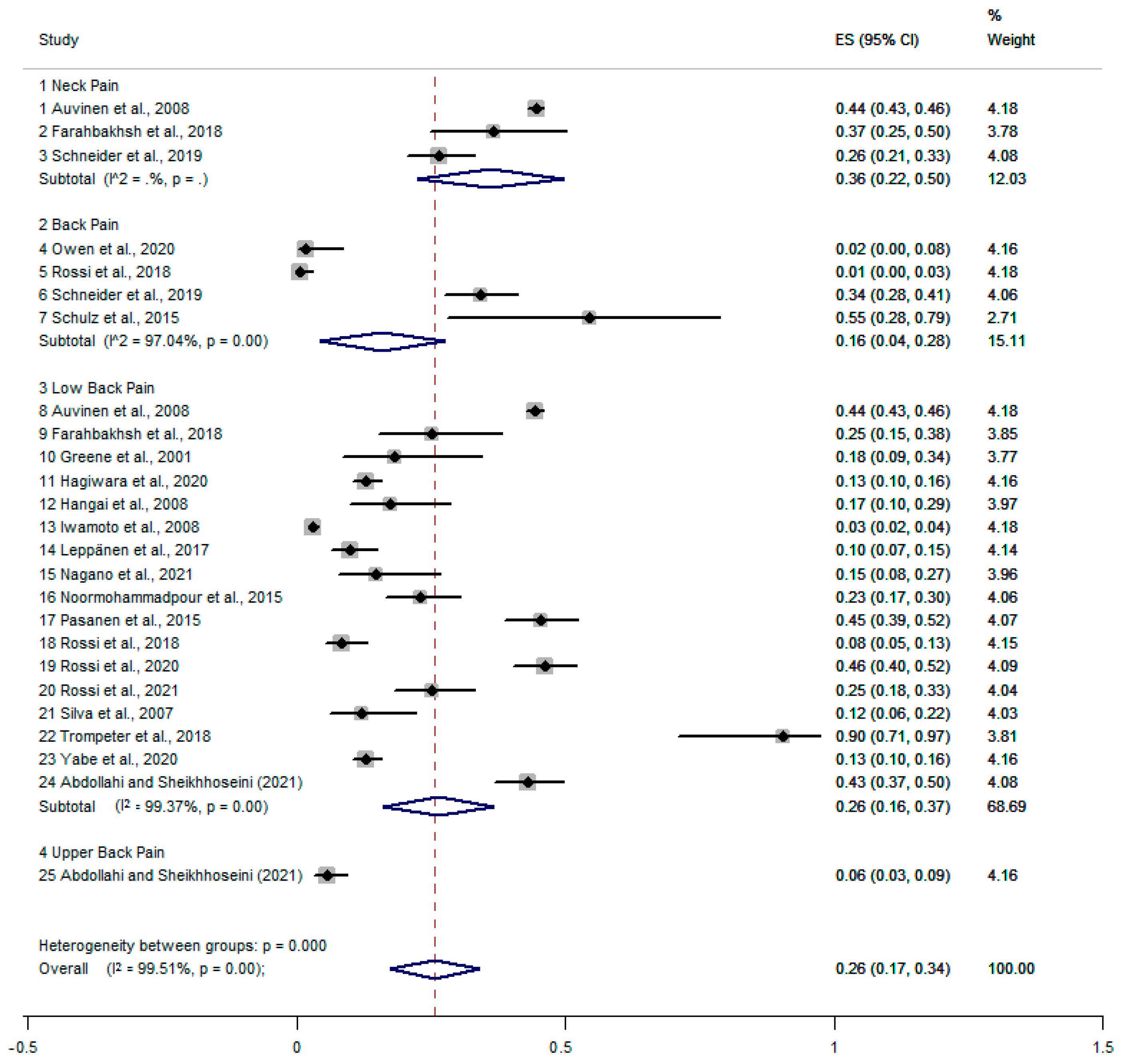
3.4. Assessment of the Prevalence of Back Pain
3.5. Associated Factors
4. Meta-Analysis
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cieza, A.; Causey, K.; Kamenov, K.; Hanson, S.W.; Chatterji, S.; Vos, T. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 2006–2017. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.; Kamper, S.J.; Wiggers, J.H.; O’Brien, K.M.; Lee, H.; Wolfenden, L.; Yoong, S.L.; Robson, E.; McAuley, J.H.; Hartvigsen, J.; et al. Musculoskeletal conditions may increase the risk of chronic disease: A systematic review and meta-analysis of cohort studies. BMC Med. 2018, 16, 167. [Google Scholar] [CrossRef]
- Hartvigsen, J.; Hancock, M.J.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J.; et al. What low back pain is and why we need to pay attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef]
- Sheikhhoseini, R.; Kavianifard, M.; Nejad, S.E.H.; Piri, H. Comparison of the Mechanical Energy Transfer of Gait in Female Athletes with and without Non-Specific Chronic Low Back Pain. Women’s Health Bull. 2020, 7, 12–17. Available online: https://womenshealthbulletin.sums.ac.ir/article_46712_f86e34cc6613495d4c04affd80e1cc91.pdf (accessed on 13 January 2021).
- Ball, J.R.; Harris, C.B.; Lee, J.; Vives, M.J. Lumbar Spine Injuries in Sports: Review of the Literature and Current Treatment Recommendations. Sports Med.-Open 2019, 5, 26. [Google Scholar] [CrossRef] [PubMed]
- Yabe, Y.; Hagiwara, Y.; Sekiguchi, T.; Momma, H.; Tsuchiya, M.; Kanazawa, K.; Itaya, N.; Yoshida, S.; Sogi, Y.; Yano, T.; et al. High prevalence of low back pain among young basketball players with lower extremity pain: A cross-sectional study. BMC Sports Sci. Med. Rehabil. 2020, 12, 40. [Google Scholar] [CrossRef]
- Farahbakhsh, F.; Akbari-Fakhrabadi, M.; Shariat, A.; Cleland, J.A.; Farahbakhsh, F.; Seif-Barghi, T.; Mansournia, M.A.; Rostami, M.; Kordi, R. Neck pain and low back pain in relation to functional disability in different sport activities. J. Exerc. Rehabil. 2018, 14, 509–515. [Google Scholar] [CrossRef]
- Fett, D.; Trompeter, K.; Platen, P. Back pain in elite sports: A cross-sectional study on 1114 athletes. PLoS ONE 2017, 12, e0180130. [Google Scholar] [CrossRef]
- Trompeter, K.; Fett, D.; Brüggemann, G.-P.; Platen, P. Prevalence of Back Pain in Elite Athletes. Ger. J. Sport. Med. Zeitschrift. Fur. Sport. 2018, 69, 240–246. Available online: https://www.germanjournalsportsmedicine.com/archive/archive-2018/issue-7-8/prevalence-of-back-pain-in-elite-athletes/ (accessed on 31 January 2021). [CrossRef]
- Rossi, M.K.; Pasanen, K.; Heinonen, A.; Äyrämö, S.; Räisänen, A.M.; Leppänen, M.; Myklebust, G.; Vasankari, T.; Kannus, P.; Parkkari, J. Performance in dynamic movement tasks and occurrence of low back pain in youth floorball and basketball players. BMC Musculoskelet. Disord. 2020, 21, 350. [Google Scholar] [CrossRef]
- Noormohammadpour, P.; Rostami, M.; Mansournia, M.A.; Farahbakhsh, F.; Shahi, M.H.P.; Kordi, R. Low back pain status of female university students in relation to different sport activities. Eur. Spine J. 2015, 25, 1196–1203. [Google Scholar] [CrossRef]
- Zuckerman, S.L.; Wegner, A.M.; Roos, K.G.; Djoko, A.; Dompier, T.P.; Kerr, Z.Y. Injuries sustained in National Collegiate Athletic Association men’s and women’s basketball, 2009/2010–2014/2015. Br. J. Sports Med. 2018, 52, 261–268. [Google Scholar] [CrossRef]
- Makovicka, J.L.; Deckey, D.G.; Patel, K.A.; Hassebrock, J.D.; Chung, A.; Tummala, S.V.; Hydrick, T.C.; Pena, A.; Chhabra, A. Epidemiology of Lumbar Spine Injuries in Men’s and Women’s National Collegiate Athletic Association Basketball Athletes. Orthop. J. Sports Med. 2019, 7, 2325967119879104. [Google Scholar] [CrossRef]
- Grabara, M.; Hadzik, A. Postural variables in girls practicing volleyball. Biomed. Hum. Kinet. 2009, 1, 67–71. [Google Scholar] [CrossRef]
- Wojtys, E.M.; Ashton-Miller, J.A.; Huston, L.J.; Moga, P.J. The Association between Athletic Training Time and the Sagittal Curvature of the Immature Spine. Am. J. Sport. Med. 2000, 28, 490–498. [Google Scholar] [CrossRef] [PubMed]
- Grabara, M. Sagittal spinal curvatures in adolescent male basketball players and non-training individuals—A two-year study. Sci. Sport. 2016, 31, e147–e153. [Google Scholar] [CrossRef]
- Borges, S.C.D.C.; Fernandes, M.D.S.V.; Noll, P.R.E.S.; Azevedo, V.D.; Silva, R.M.F.; Mendonça, C.R.; Noll, M. Musculoskeletal disorders in basketball players and associated factors: A systematic review protocol with meta-analysis. F1000Research 2021, 10, 557. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Morgan, R.L.; Whaley, P.; Thayer, K.A.; Schünemann, H.J. Identifying the PECO: A framework for formulating good questions to explore the association of environmental and other exposures with health outcomes. Environ. Int. 2018, 121, 1027–1031. [Google Scholar] [CrossRef]
- Brahme, A. Comprehensive Biomedical Physics; Newnes: Oxford, UK, 2014. [Google Scholar]
- Zhang, S.; Wadhwa, R.; Haydel, J.; Toms, J.; Johnson, K.; Guthikonda, B. Spine and Spinal Cord Trauma: Diagnosis and Management. Neurol. Clin. 2013, 31, 183–206. [Google Scholar] [CrossRef]
- Beynon, A.M.; Hebert, J.J.; Lebouef-Yde, C.; Walker, B.F. Potential risk factors and triggers for back pain in children and young adults. A scoping review, part II: Unclear or mixed types of back pain. Chiropr. Man. Ther. 2019, 27, 61. Available online: https://chiromt.biomedcentral.com/articles/10.1186/s12998-019-0281-8 (accessed on 11 January 2021). [CrossRef]
- Beynon, A.M.; Hebert, J.J.; Hodgetts, C.J.; Boulos, L.M.; Walker, B.F. Chronic physical illnesses, mental health disorders, and psychological features as potential risk factors for back pain from childhood to young adulthood: A systematic review with meta-analysis. Eur. Spine J. 2020, 29, 480–496. [Google Scholar] [CrossRef] [PubMed]
- Noll, M.; Kjaer, P.; Mendonça, C.R.; Wedderkopp, N. Motor performance and back pain in children and adolescents: A systematic review and meta-analysis protocol. Syst. Rev. 2020, 9, 212. [Google Scholar] [CrossRef] [PubMed]
- Reiswig, J. Mendeley. J. Med. Libr. Assoc. 2010, 98, 193–194. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Noll, M.; Kjaer, P.; Mendonça, C.R.; Wedderkopp, N. Motor performance and back pain in children and adolescents: A systematic review. Eur. J. Pain 2022, 26, 77–102. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [PubMed]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Noll, M.; De Mendonça, C.R.; De Souza Rosa, L.P.; Silveira, E.A. Determinants of eating patterns and nutrient intake among adolescent athletes: A systematic review. Nutr. J. 2017, 16, 46. Available online: https://nutritionj.biomedcentral.com/articles/10.1186/s12937-017-0267-0 (accessed on 12 January 2021). [CrossRef] [PubMed]
- Farrah, K.; Young, K.; Tunis, M.C.; Zhao, L. Risk of bias tools in systematic reviews of health interventions: An analysis of PROSPERO-registered protocols. Syst. Rev. 2019, 8, 280. Available online: https://systematicreviewsjournal.biomedcentral.com/articles/10.1186/s13643-019-1172-8 (accessed on 20 April 2021). [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Šarčević, Z.; Tepavčević, A. Association between adolescent idiopathic scoliosis and sacroiliac joint dysfunction in young athletes: A case control study. Medicine 2019, 98, e15161. [Google Scholar] [CrossRef] [PubMed]
- Schulz, S.S.; Lenz, K.; Büttner-Janz, K. Severe back pain in elite athletes: A cross-sectional study on 929 top athletes of Germany. Eur. Spine J. 2015, 25, 1204–1210. [Google Scholar] [CrossRef]
- Da Silva, A.S.; Abdalla, R.J.; Fisberg, M. Incidence of musculoskeletal injuries in elite female basketball athletes. Acta Ortopédica Bras. 2007, 15, 43–46. [Google Scholar] [CrossRef]
- Weiss, K.J.; McGuigan, M.R.; Besier, T.F.; Whatman, C.S. Application of a Simple Surveillance Method for Detecting the Prevalence and Impact of Overuse Injuries in Professional Men’s Basketball. J. Strength Cond. Res. 2017, 31, 2734–2739. [Google Scholar] [CrossRef] [PubMed]
- Auvinen, J.P.; Tammelin, T.H.; Taimela, S.P.; Zitting, P.J.; Mutanen, P.O.A.; Karppinen, J.I. Musculoskeletal Pains in Relation to Different Sport and Exercise Activities in Youth. Med. Sci. Sports Exerc. 2008, 40, 1890–1900. [Google Scholar] [CrossRef]
- Hagiwara, Y.; Yabe, Y.; Sekiguchi, T.; Momma, H.; Tsuchiya, M.; Kanazawa, K.; Yoshida, S.; Sogi, Y.; Yano, T.; Onoki, T.; et al. Upper Extremity Pain Is Associated with Lower Back Pain among Young Basketball Players: A Cross-Sectional Study. Tohoku J. Exp. Med. 2020, 250, 79–85. [Google Scholar] [CrossRef]
- Habelt, S.; Hasler, C.C.; Steinbrück, K.; Majewski, M. Sport injuries in adolescents. Orthop. Rev. 2011, 3, e18. [Google Scholar] [CrossRef]
- Selhorst, M.; Fischer, A.; MacDonald, J. Prevalence of Spondylolysis in Symptomatic Adolescent Athletes: An Assessment of Sport Risk in Nonelite Athletes. Clin. J. Sport Med. 2019, 29, 421–425. Available online: https://journals.lww.com/cjsportsmed/Fulltext/2019/09000/Prevalence_of_Spondylolysis_in_Symptomatic.12.aspx (accessed on 13 January 2021). [CrossRef]
- Meron, A.; McMullen, C.; Laker, S.R.; Currie, D.; Comstock, R.D. Epidemiology of Cervical Spine Injuries in High School Athletes Over a Ten-Year Period. PM&R 2018, 10, 365–372. [Google Scholar] [CrossRef]
- Schneider, S.; Sauer, J.; Berrsche, G.; Schmitt, H. No Pain, No Gain? Prevalence, Location, Context, and Coping Strategies with Regard to Pain Among Young German Elite Basketball Players. J. Hum. Kinet. 2019, 69, 179–189. [Google Scholar] [CrossRef] [PubMed]
- Iwamoto, J.; Takeda, T.; Sato, Y.; Matsumoto, H. Retrospective case evaluation of gender differences in sports injuries in a Japanese sports medicine clinic. Gend. Med. 2008, 5, 405–414. [Google Scholar] [CrossRef]
- Keene, J.S.; Albert, M.J.; Springer, S.L.; Drummond, D.S.; Clancy, W.G.J. Back Injuries in College Athletes. Clin. Spine Surg. 1989, 2, 190–195. Available online: https://journals.lww.com/jspinaldisorders/Fulltext/1989/09000/Back_Injuries_in_College_Athletes.7.aspx (accessed on 14 January 2021). [CrossRef]
- Kerr, Z.Y.; Collins, C.L.; Pommering, T.L.; Fields, S.K.; Comstock, R.D. Dislocation/Separation Injuries Among US High School Athletes in 9 Selected Sports: 2005–2009. Clin. J. Sport Med. 2011, 21, 101–108. Available online: https://journals.lww.com/cjsportsmed/Fulltext/2011/03000/Dislocation_Separation_Injuries_Among_US_High.5.aspx (accessed on 13 January 2021). [CrossRef] [PubMed]
- Leppänen, M.; Pasanen, K.; Kannus, P.; Vasankari, T.; Kujala, U.M.; Heinonen, A.; Parkkari, J. Epidemiology of Overuse Injuries in Youth Team Sports: A 3-year Prospective Study. Int. J. Sport. Med. 2017, 38, 847–856. [Google Scholar] [CrossRef]
- Pasanen, K.; Rossi, M.; Parkkari, J.; Kannus, P.; Heinonen, A.; Tokola, K.; Myklebust, G. Low Back Pain in Young Basketball and Floorball Players. Clin. J. Sport Med. 2016, 26, 376–380. Available online: https://journals.lww.com/cjsportsmed/Fulltext/2016/09000/Low_Back_Pain_in_Young_Basketball_and_Floorball.4.aspx (accessed on 14 January 2021). [CrossRef]
- Rossi, F.; Dragoni, S. The prevalence of spondylolysis and spondylolisthesis in symptomatic elite athletes: Radiographic findings. Radiography 2001, 7, 37–42. [Google Scholar] [CrossRef]
- Rossi, M.K.; Pasanen, K.; Heinonen, A.; Myklebust, G.; Kannus, P.; Kujala, U.M.; Tokola, K.; Parkkari, J. Incidence and risk factors for back pain in young floorball and basketball players: A Prospective study. Scand. J. Med. Sci. Sport. 2018, 28, 2407–2415. [Google Scholar] [CrossRef]
- Rossi, M.K.; Pasanen, K.; Heinonen, A.; Äyrämö, S.; Leppänen, M.; Myklebust, G.; Vasankari, T.; Kannus, P.; Parkkari, J. The standing knee lift test is not a useful screening tool for time loss from low back pain in youth basketball and floorball players. Phys. Ther. Sport 2021, 49, 141–148. [Google Scholar] [CrossRef]
- Abdollahi, S.; Sheikhhoseini, R. Sport-related injuries in Iranian basketball players: Evidence from a retrospective epidemiologic study (2019–20). Phys. Sportsmed. 2022, 50, 406–413. [Google Scholar] [CrossRef]
- Grabara, M. Anteroposterior curvatures of the spine in adolescent athletes. J. Back Musculoskelet. Rehabil. 2014, 27, 513–519. [Google Scholar] [CrossRef]
- Greene, H.S.; Cholewicki, J.; Galloway, M.T.; Nguyen, C.V.; Radebold, A. A History of Low Back Injury is a Risk Factor for Recurrent Back Injuries in Varsity Athletes. Am. J. Sport. Med. 2001, 29, 795–800. [Google Scholar] [CrossRef]
- Hangai, M.; Kaneoka, K.; Hinotsu, S.; Shimizu, K.; Okubo, Y.; Miyakawa, S.; Mukai, N.; Sakane, M.; Ochiai, N. Lumbar Intervertebral Disk Degeneration in Athletes. Am. J. Sport. Med. 2008, 37, 149–155. [Google Scholar] [CrossRef]
- Ichikawa, N.; Ohara, Y.; Morishita, T.; Taniguichi, Y.; Koshikawa, A.; Matsukura, N. An aetiological study on spondylolysis from a biomechanical aspect. Br. J. Sports Med. 1982, 16, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Nagano, Y.; Shimada, Y.; Sasaki, N.; Shibata, M. Prevalence and Burden of Physical Problems in Female College Basketball Athletes: A 135-Day Prospective Cohort Study. Open Access J. Sports Med. 2021, 12, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Nowak, A.; Pytel, A.; Molik, B.; Marszalek, J. Characteristics of injuries of young adult male basketball players. Adv. Rehabil. 2019, 2019, 35–46. [Google Scholar] [CrossRef]
- Owen, P.J.; Hangai, M.; Kaneoka, K.; Rantalainen, T.; Belavy, D.L. Mechanical loading influences the lumbar intervertebral disc. A cross-sectional study in 308 athletes and 71 controls. J. Orthop. Res. 2021, 39, 989–997. [Google Scholar] [CrossRef]
- Hickey, G.J.; Fricker, P.A.; McDonald, W.A. Injuries to Young Elite Female Basketball Players Over a Six-Year Period. Clin. J. Sport Med. 1997, 7, 252–256. [Google Scholar] [CrossRef]
- Safiri, S.; Kolahi, A.-A.; Hoy, D.; Buchbinder, R.; Mansournia, M.A.; Bettampadi, D.; Ashrafi-Asgarabad, A.; Almasi-Hashiani, A.; Smith, E.; Sepidarkish, M.; et al. Global, regional, and national burden of neck pain in the general population, 1990–2017: Systematic analysis of the Global Burden of Disease Study 2017. BMJ 2020, 368, m791. [Google Scholar] [CrossRef]
- Chen, S.; Chen, M.; Wu, X.; Lin, S.; Tao, C.; Cao, H.; Shao, Z.; Xiao, G. Global, regional and national burden of low back pain 1990–2019: A systematic analysis of the Global Burden of Disease study 2019. J. Orthop. Transl. 2022, 32, 49–58. [Google Scholar] [CrossRef]
- Kim, J.H.; Lee, G.H.; Cho, S.T. Prevalence of and risk factors for lower back pain in university basketball players. Arthrosc. Orthop. Sport. Med. 2021, 8, 54–60. [Google Scholar] [CrossRef]
- Ackery, A.D.; Detsky, A.S. Reducing lifelong disability from sports injuries in children. Can. Med. Assoc. J. 2011, 183, 1235. [Google Scholar] [CrossRef] [PubMed]
- Hu, S.S.; Tribus, C.B.; Diab, M.; Ghanayem, A.J. Spondylolisthesis and Spondylolysis. JBJS 2008, 90, 656–671. Available online: https://journals.lww.com/jbjsjournal/Fulltext/2008/03000/Spondylolisthesis_and_Spondylolysis.25.aspx (accessed on 13 April 2021).
- Cavalier, R.; Herman, M.J.; Cheung, E.V.; Pizzutillo, P.D. Spondylolysis and Spondylolisthesis in Children and Adolescents: I. Diagnosis, Natural History, and Nonsurgical Management. JAAOS-J. Am. Acad. Orthop. Surg. 2006, 14, 417–424. Available online: https://journals.lww.com/jaaos/Fulltext/2006/07000/Spondylolysis_and_Spondylolisthesis_in_Children.4.aspx (accessed on 13 April 2021). [CrossRef] [PubMed]
- Zusman, N.L.; Somogyi, R.D.; Barney, N.A.; Yang, S.; Halsey, M.F. Adolescents with spondylolysis have lower SRS-22 scores than controls and peers with pre-operative idiopathic scoliosis. Spine Deform. 2021, 9, 135–140. [Google Scholar] [CrossRef]
- Nam, H.J.; Lee, J.-H.; Hong, D.-S.; Jung, H.C. The Effect of Wearing a Customized Mouthguard on Body Alignment and Balance Performance in Professional Basketball Players. Int. J. Environ. Res. Public Health 2020, 17, 6431. [Google Scholar] [CrossRef]
- Chen, X.; Biro, I. Lumber Lordosis Motions Monitor Using Formetric Imaging Analysis. J. Med. Imaging Health Inform. 2020, 10, 1190–1194. [Google Scholar] [CrossRef]
- Azevedo, V.D.; Silva, R.M.F.; Borges, S.C.D.C.; Fernandes, M.D.S.V.; Miñana-Signes, V.; Monfort-Pañego, M.; Noll, P.R.E.S.; Noll, M. Evaluation Instruments for Assessing Back Pain in Athletes: A Systematic Review Protocol. Healthcare 2020, 8, 574. [Google Scholar] [CrossRef]
- Kaplan, D. Evaluating the Effect of 12 Weeks Football Training on the Posture of Young Male Basketball Players. J. Educ. Train. Stud. 2018, 6, 47–53. [Google Scholar] [CrossRef]
- Silveira, E.A.; Romeiro, A.M.D.S.; Noll, M. Guide for scientific writing: How to avoid common mistakes in a scientific article. J. Hum. Growth Dev. 2022, 32, 341–352. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Carvalho Borges, S.C.; Mendonça, C.R.; Ferreira Silva, R.M.; De Vitta, A.; Noll, M. Prevalence and Risk Factors of Musculoskeletal Disorders in Basketball Players: Systematic Review and Meta-Analysis. Healthcare 2023, 11, 1190. https://doi.org/10.3390/healthcare11081190
de Carvalho Borges SC, Mendonça CR, Ferreira Silva RM, De Vitta A, Noll M. Prevalence and Risk Factors of Musculoskeletal Disorders in Basketball Players: Systematic Review and Meta-Analysis. Healthcare. 2023; 11(8):1190. https://doi.org/10.3390/healthcare11081190
Chicago/Turabian Stylede Carvalho Borges, Silvia Cristina, Carolina Rodrigues Mendonça, Regina Márcia Ferreira Silva, Alberto De Vitta, and Matias Noll. 2023. "Prevalence and Risk Factors of Musculoskeletal Disorders in Basketball Players: Systematic Review and Meta-Analysis" Healthcare 11, no. 8: 1190. https://doi.org/10.3390/healthcare11081190