
The Impact of Multidrug-Resistant Acinetobacter baumannii Infection in Critically Ill Patients with or without COVID-19 Infection
 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Methods
Study Design and Patient Selection
3. Data Analyses
4. Results
4.1. MDR-AB and COVID-19 Infections
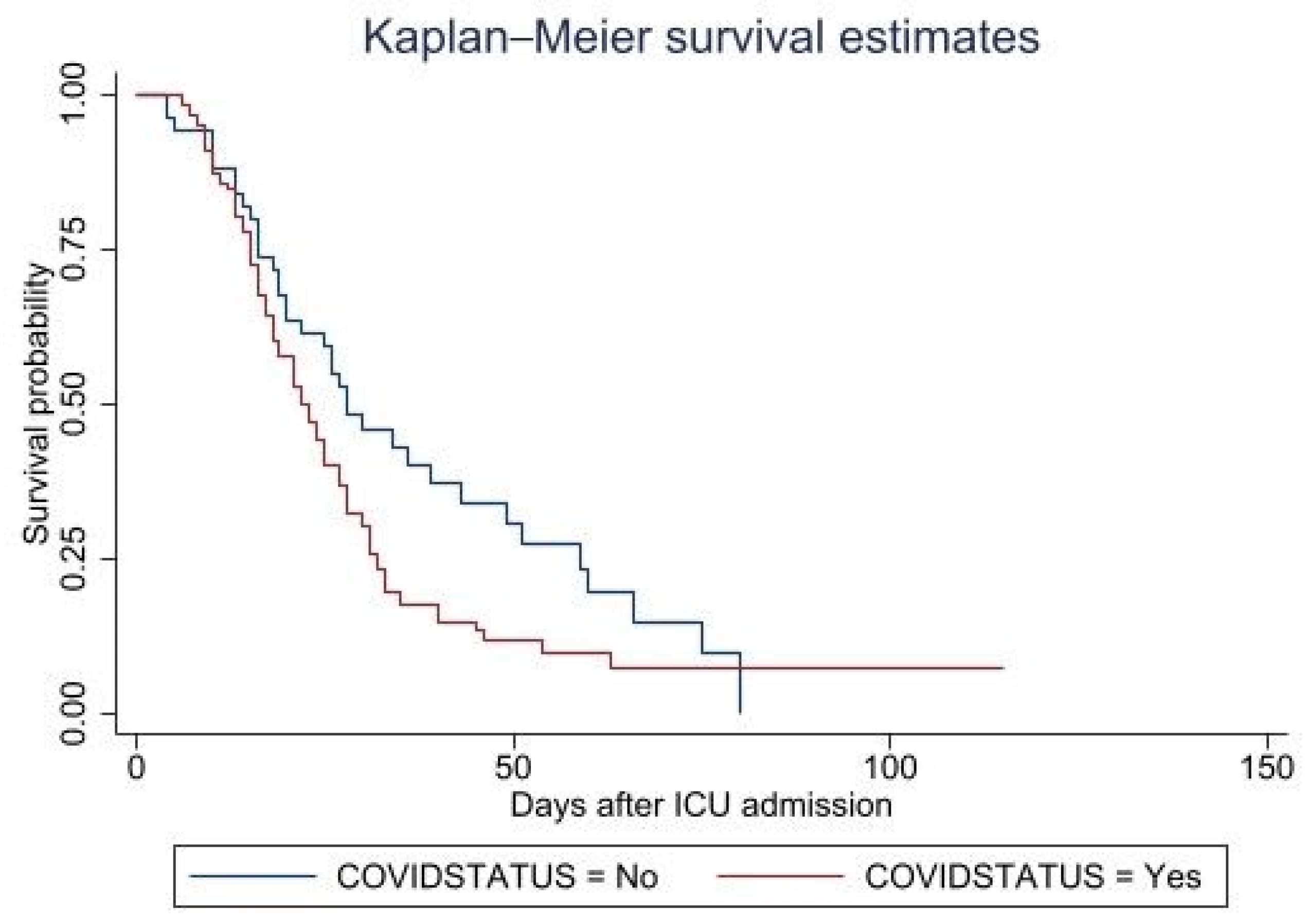
4.2. Mortality Hazards in MDR-AB Patients
4.3. MDR-AB and Bloodstream Infection
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Asif, M.; Alvi, I.A.; Rehman, S.U. Insight into Acinetobacter baumannii: Pathogenesis, global resistance, mechanisms of resistance, treatment options, and alternative modalities. Infect. Drug Resist. 2018, 11, 1249. [Google Scholar] [CrossRef] [PubMed]
- Jawad, A.; Seifert, H.; Snelling, A.M.; Heritage, J.; Hawkey, P.M. Survival of Acinetobacter baumannii on dry surfaces: Comparison of outbreak and sporadic isolates. J. Clin. Microbiol. 1998, 36, 1938–1941. [Google Scholar] [CrossRef] [PubMed]
- Magill, S.S.; Edwards, J.R.; Bamberg, W.; Beldavs, Z.G.; Dumyati, G.; Kainer, M.A.; Lynfield, R.; Maloney, M.; McAllister-Hollod, L.; Nadle, J. Multistate point-prevalence survey of health care–associated infections. N. Engl. J. Med. 2014, 370, 1198–1208. [Google Scholar] [CrossRef] [PubMed]
- Lob, S.H.; Hoban, D.J.; Sahm, D.F.; Badal, R.E. Regional differences and trends in antimicrobial susceptibility of Acinetobacter baumannii. Int. J. Antimicrob. Agents 2016, 47, 317–323. [Google Scholar] [CrossRef]
- Giammanco, A.; Calà, C.; Fasciana, T.; Dowzicky, M.J. Global assessment of the activity of tigecycline against multidrug-resistant Gram-negative pathogens between 2004 and 2014 as part of the tigecycline evaluation and surveillance trial. Msphere 2017, 2, e00310-16. [Google Scholar] [CrossRef]
- Espinal, P.; Martí, S.; Vila, J. Effect of biofilm formation on the survival of Acinetobacter baumannii on dry surfaces. J. Hosp. Infect. 2012, 80, 56–60. [Google Scholar] [CrossRef]
- Bassetti, M.; Righi, E.; Vena, A.; Graziano, E.; Russo, A.; Peghin, M. Risk stratification and treatment of ICU-acquired pneumonia caused by multidrug-resistant/extensively drug-resistant/pandrug-resistant bacteria. Curr. Opin. Crit. Care 2018, 24, 385–393. [Google Scholar] [CrossRef]
- Russo, A.; Giuliano, S.; Ceccarelli, G.; Alessandri, F.; Giordano, A.; Brunetti, G.; Venditti, M. Comparison of septic shock due to multidrug-resistant Acinetobacter baumannii or Klebsiella pneumoniae carbapenemase-producing K. pneumoniae in intensive care unit patients. Antimicrob. Agents Chemother. 2018, 62, e02562-17. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19). Available online: https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf (accessed on 27 September 2022).
- Huang, C.; Soleimani, J.; Herasevich, S.; Pinevich, Y.; Pennington, K.M.; Dong, Y.; Pickering, B.W.; Barwise, A.K. Clinical characteristics, treatment, and outcomes of critically ill patients with COVID-19: A scoping review. In Proceedings of the Mayo Clinic Proceedings; Elsevier: Amsterdam, The Netherlands, 2021; Volume 96, pp. 183–202. [Google Scholar]
- Siddiqi, H.K.; Mehra, M.R. COVID-19 illness in native and immunosuppressed states: A clinical–therapeutic staging proposal. J. Heart Lung Transplant. 2020, 39, 405–407. [Google Scholar] [CrossRef] [Green Version]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef] [PubMed]
- Jamilloux, Y.; Henry, T.; Belot, A.; Viel, S.; Fauter, M.; El Jammal, T.; Walzer, T.; François, B.; Sève, P. Should we stimulate or suppress immune responses in COVID-19? Cytokine and anti-cytokine interventions. Autoimmun. Rev. 2020, 19, 102567. [Google Scholar] [CrossRef] [PubMed]
- Pettit, N.N.; Nguyen, C.T.; Mutlu, G.M.; Wu, D.; Kimmig, L.; Pitrak, D.; Pursell, K. Late onset infectious complications and safety of tocilizumab in the management of COVID-19. J. Med. Virol. 2021, 93, 1459–1464. [Google Scholar] [CrossRef]
- Lai, C.-C.; Wang, C.-Y.; Hsueh, P.-R. Co-infections among patients with COVID-19: The need for combination therapy with non-anti-SARS-CoV-2 agents? J. Microbiol. Immunol. Infect. 2020, 53, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Contou, D.; Claudinon, A.; Pajot, O.; Micaëlo, M.; Longuet Flandre, P.; Dubert, M.; Cally, R.; Logre, E.; Fraissé, M.; Mentec, H. Bacterial and viral co-infections in patients with severe SARS-CoV-2 pneumonia admitted to a French ICU. Ann. Intensive Care 2020, 10, 1–9. [Google Scholar] [CrossRef]
- Nebreda-Mayoral, T.; Miguel-Gómez, M.A.; March-Rosselló, G.A.; Puente-Fuertes, L.; Cantón-Benito, E.; Martínez-García, A.M.; Muñoz-Martín, A.B.; Orduña-Domingo, A. Infección bacteriana/fúngica en pacientes con COVID-19 ingresados en un hospital de tercer nivel de Castilla y León, España. Enferm. Infecc. Microbiol. Clin. 2020, 40, 158–165. [Google Scholar] [CrossRef]
- Yang, S.; Hua, M.; Liu, X.; Du, C.; Pu, L.; Xiang, P.; Wang, L.; Liu, J. Bacterial and fungal co-infections among COVID-19 patients in intensive care unit. Microbes Infect. 2021, 23, 104806. [Google Scholar] [CrossRef]
- Cultrera, R.; Barozzi, A.; Libanore, M.; Marangoni, E.; Pora, R.; Quarta, B.; Spadaro, S.; Ragazzi, R.; Marra, A.; Segala, D. Co-infections in critically ill patients with or without COVID-19: A comparison of clinical microbial culture findings. Int. J. Environ. Res. Public Health 2021, 18, 4358. [Google Scholar] [CrossRef]
- Russo, A.; Gavaruzzi, F.; Ceccarelli, G.; Borrazzo, C.; Oliva, A.; Alessandri, F.; Magnanimi, E.; Pugliese, F.; Venditti, M. Multidrug-resistant Acinetobacter baumannii infections in COVID-19 patients hospitalized in intensive care unit. Infection 2022, 50, 83–92. [Google Scholar] [CrossRef]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [Green Version]
- Kharaba, A.; Algethamy, H.; Hussein, M.; Al-Hameed, F.M.; Alghamdi, A.; Hamdan, A.; Fatani, J.; Elhazmi, A.; Alkhalaf, H.; Barghash, B.; et al. Incidence, outcomes, and predictors of Acinetobacter infection in Saudi Arabian critical care units. J. Crit. Care 2021, 66, 109–116. [Google Scholar] [CrossRef]
- Ibrahim, M.E. Prevalence of Acinetobacter baumannii in Saudi Arabia: Risk factors, antimicrobial resistance patterns and mechanisms of carbapenem resistance Annals of Clinical Microbiology and Antimicrobials. Ibrahim. Ann. Clin. Microbiol. Antimicrob. 2019, 18, 1. [Google Scholar] [CrossRef] [PubMed]
- Wong, D.; Nielsen, T.B.; Bonomo, R.A.; Pantapalangkoor, P.; Luna, B.; Spellberg, B. Clinical and pathophysiological overview of Acinetobacter infections: A century of challenges. Clin. Microbiol. Rev. 2017, 30, 409–447. [Google Scholar] [CrossRef] [PubMed]
- Peleg, A.Y.; Seifert, H.; Paterson, D.L. Acinetobacter baumannii: Emergence of a successful pathogen. Clin. Microbiol. Rev. 2008, 21, 538–582. [Google Scholar] [CrossRef]
- Alqahtani, A.; Alamer, E.; Mir, M.; Alasmari, A.; Alshahrani, M.M.; Asiri, M.; Ahmad, I.; Alhazmi, A.; Algaissi, A. Bacterial Coinfections Increase Mortality of Severely Ill COVID-19 Patients in Saudi Arabia. Int. J. Environ. Res. Public Health 2022, 19, 2424. [Google Scholar] [CrossRef]
- Pisters, R.; Lane, D.A.; Nieuwlaat, R.; De Vos, C.B.; Crijns, H.J.G.M.; Lip, G.Y.H. A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: The Euro Heart Survey. Chest 2010, 138, 1093–1100. [Google Scholar] [CrossRef]
- Gottesman, T.; Fedorowsky, R.; Yerushalmi, R.; Lellouche, J.; Nutman, A. An outbreak of carbapenem-resistant Acinetobacter baumannii in a COVID-19 dedicated hospital. Infect. Prev. Pract. 2021, 3, 100113. [Google Scholar] [CrossRef] [PubMed]
- Syed, R.F.; Yelamanchili, S.; Thati, S. A Comparative Study of Acinetobacter Infections in COVID and Non-COVID Patients. J. Infect. Dis. Epidemiol. 2022, 8, 250. [Google Scholar]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Hu, J.; Zhu, C. Obesity aggravates COVID-19: A systematic review and meta-analysis. J. Med. Virol. 2021, 93, 257–261. [Google Scholar] [CrossRef]
- Guan, W.; Ni, Z.; Hu, Y.; Liang, W.; Ou, C.; He, J.; Liu, L.; Shan, H.; Lei, C.; Hui, D.S.C. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Group, R.C. Dexamethasone in hospitalized patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar]
- Malekzadeh, R.; Abedini, A.; Mohsenpour, B.; Sharifipour, E.; Ghasemian, R.; Javad-Mousavi, S.A.; Khodashahi, R.; Darban, M.; Kalantari, S.; Abdollahi, N. Subcutaneous tocilizumab in adults with severe and critical COVID-19: A prospective open-label uncontrolled multicenter trial. Int. Immunopharmacol. 2020, 89, 107102. [Google Scholar] [CrossRef]
- Mazzitelli, M.; Arrighi, E.; Serapide, F.; Pelle, M.C.; Tassone, B.; Lionello, R.; Marrazzo, G.; Laganà, D.; Costanzo, F.S.; Matera, G. Use of subcutaneous tocilizumab in patients with COVID-19 pneumonia. J. Med. Virol. 2021, 93, 32. [Google Scholar] [CrossRef] [PubMed]
- Mastroianni, A.; Greco, S.; Apuzzo, G.; De Santis, S.; Oriolo, C.; Zanolini, A.; Chidichimo, L.; Vangeli, V. Subcutaneous tocilizumab treatment in patients with severe COVID-19–related cytokine release syndrome: An observational cohort study. eClinicalMedicine 2020, 24, 100410. [Google Scholar] [CrossRef] [PubMed]
- Saudi MoH Protocol for Patients Suspected of/Confirmed with COVID-19. Available online: https://www.moh.gov.sa/Ministry/MediaCenter/Publications/Documents/MOH-therapeutic-protocol-for-COVID-19.pdf (accessed on 15 October 2022).
- Tamma, P.D.; Aitken, S.L.; Bonomo, R.A.; Mathers, A.J.; van Duin, D.; Clancy, C.J. Infectious Diseases Society of America Guidance on the Treatment of AmpC β-Lactamase–Producing Enterobacterales, Carbapenem-Resistant Acinetobacter baumannii, and Stenotrophomonas maltophilia Infections. Clin. Infect. Dis. 2022, 74, 2089–2114. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Non-COVID-19 n = 52 | COVID-19 n = 118 | p Value |
|---|---|---|---|
| Age | 66.77 ± 20.96 | 60.97 ± 16.32 | 0.0525 |
| Gender | 0.474 | ||
| Female (F) | 16 (30.77%) | 43 (36.44%) | |
| Male (M) | 36 (69.23%) | 75 (63.56) | |
| Body mass index (n = 160) | 27.03 ± 7.34 | 29.67 ± 7.18 | 0.0429 |
| Body mass index category | 0.025 | ||
| Underweight or normal | 16 (38.10%) | 21 (17.80%) | |
| Overweight | 13 (30.95%) | 54 (45.76%) | |
| Obese | 13 (30.95%) | 43 (36.44%) | |
| Pregnancy | 0 (0%) | 5 (4.24%) | 0.132 |
| Comorbidities | |||
| More than two comorbidities | 23 (44.23%) | 23 (19.49%) | 0.001 |
| Heart failure | 6 (11.54%) | 6 (5.08%) | 0.130 |
| Hypertension | 35 (67.31%) | 77 (65.25%) | 0.795 |
| Diabetes Mellitus (DM) | 34 (65.38%) | 82 (69.49%) | 0.596 |
| Chronic kidney disease (CKD) | 12 (23.08%) | 25 (21.19%) | 0.783 |
| Chronic liver disease (CLD) | 4 (7.69%) | 3 (2.54%) | 0.119 |
| Asthma | 5 (7.69%) | 4 (3.39%) | 0.222 |
| Chronic obstructive pulmonary disease (COPD) | 16 (30.77%) | 1 (0.85%) | 0.0001 |
| Malignancy | 4 (7.69%) | 3 (2.54%) | 0.119 |
| Clinical features | |||
| SOFA at time of admission | 6.13 ± 3.69 | 4.63 ± 4.16 | 0.0258 |
| SOFA at positive culture time | 14.23 ± 7.08 | 13.69 ± 6.32 | 0.5998 |
| Abnormal WBC count | 28 (53.85%) | 75 (63.56%) | 0.232 |
| Platelet count (×106) | 145.73 ± 133.06 | 154.56 ± 116.85 | 0.6643 |
| Abnormal CRP | 50 (96.15%) | 114 (96.61%) | 0.882 |
| Serum lactate > 2 mmol/L | 36 (69.23%) | 94 (79.66%) | 0.140 |
| Bloodstream infection | 27 (51.92%) | 75 (63.56%) | 0.154 |
| Intravascular device | 45 (86.54%) | 115 (97.46%) | 0.005 |
| Continuous renal replacement therapy (CRRT) | 14 (26.92%) | 27 (22.88%) | 0.570 |
| Extracorporeal membrane oxygenation (ECMO) | 0 (0%) | 5 (4.24%) | 0.132 |
| Mechanical ventilation | 40 (76.92%) | 116 (98.31%) | 0.0001 |
| Septic shock | 43 (82.69%) | 114 (96.61%) | 0.002 |
| Outcomes and therapy | |||
| Steroid therapy | 37 (71.15%) | 117 (99.15%) | 0.0001 |
| Tocilizumab | 0 (0%) | 39 (33.05%) | 0.0001 |
| Transfer to ICU | 1.69 ± 4.64 | 2.58 ± 4.72 | 0.2594 |
| Length of ICU-stay | 28.33 ± 19.63 | 21.2 ± 11.98 | 0.0042 |
| Length of hospitalization | 29.35 ± 19.71 | 23.81 ± 15.67 | 0.0522 |
| Discharge status | 0.005 | ||
| Discharged | 9 (17.31%) | 24 (20.34%) | |
| Transferred for other hospitals | 6 (11.54%) | 1 (0.85%) | |
| Died | 37 (71.15%) | 93 (78.81%) | |
| Mortality at 30 days | 26 (50.00%) | 75 (63.56) | 0.097 |
| Mortality more than 30 days (overall inpatient mortality) | 37 (71.15%) | 93 (78.81%) | 0.489 |
| Variables | Hazard Ratio | CI 95% | p Value |
|---|---|---|---|
| COVID-19 infection | 1.79 | 1.02–3.15 | 0.043 |
| Age | 1.01 | 0.1–1.02 | 0.119 |
| SOFA at positive culture time | 1.12 | 1.07–1.16 | 0.000 |
| Steroid therapy | 0.5 | 0.21–1.2 | 0.119 |
| Continuous renal replacement therapy (CRRT) | 0.72 | 0.46–1.13 | 0.158 |
| Chronic obstructive pulmonary disease (COPD) | 0.57 | 0.28–1.19 | 0.137 |
| Hypertension | 0.61 | 0.4–0.94 | 0.027 |
| Abnormal WBC count | 1.57 | 1.04–2.37 | 0.033 |
| Chronic kidney disease (CKD) | 2.01 | 1.26–3.19 | 0.003 |
| Variables | No Bloodstream Infection n = 66 | Bloodstream Infection n = 94 | p Value |
|---|---|---|---|
| Age | 63.79 ± 16.51 | 62.04 ± 18.98 | 0.5351 |
| Gender | 0.895 | ||
| Female (F) | 24 (35.29%) | 35 (34.31%) | |
| Male (M) | 44 (64.71%) | 67 (65.69%) | |
| Body mass index (n = 160) | 28.52 ± 6.77 | 29.3 ± 7.65 | 0.5116 |
| Body mass index category | 0.560 | ||
| Underweight or normal | 17 (25.76%) | 20 (21.28%) | |
| Overweight | 29 (43.94%) | 38 (40.43%) | |
| Obese | 20 (30.30%) | 36 (38.30%) | |
| Infected with COVID-19 | 43 (63.24%) | 75 (73.53%) | 0.154 |
| Pregnancy | 0 (0%) | 5 (4.90%) | 0.064 |
| Comorbidities | |||
| More than two comorbidities | 24 (35.29%) | 22 (21.57%) | 0.048 |
| Heart failure | 5 (7.35%) | 7 (6.86%) | 0.903 |
| Hypertension | 51 (75.00%) | 61 (59.80%) | 0.041 |
| Diabetes Mellitus (DM) | 52 (76.47%) | 64 (62.75%) | 0.060 |
| Chronic kidney disease (CKD) | 17 (25.00%) | 20 (19.61%) | 0.404 |
| Chronic liver disease (CLD) | 3 (4.41%) | 4 (3.92%) | 0.875 |
| Asthma | 4 (5.88%) | 4 (3.92%) | 0.554 |
| Chronic obstructive pulmonary disease (COPD) | 10 (14.71%) | 7 (6.86%) | 0.095 |
| Malignancy | 2 (2.94%) | 5 (4.90%) | 0.528 |
| Clinical features | |||
| SOFA at time of admission | 4.91 ± 4.27 | 5.21 ± 3.96 | 0.6462 |
| SOFA at positive culture time | 12.07 ± 6.40 | 15.07 ± 6.40 | 0.0032 |
| Abnormal WBCs count | 44 (64.71%) | 59 (57.84%) | 0.370 |
| Platelet count (×106) | 156.47 ± 113.44 | 148.78 ± 127.37 | 0.6874 |
| Abnormal CRP | 65 (95.59%) | 99 (97.06%) | 0.611 |
| Serum lactate > 2 mmol/L | 47 (69.12%) | 83 (81.37%) | 0.065 |
| Intravascular device | 61 (89.71%) | 99 (97.06%) | 0.046 |
| Continuous renal replacement therapy (CRRT) | 18 (26.47%) | 23 (22.55%) | 0.558 |
| Extracorporeal membrane oxygenation (ECMO) | 0 (0%) | 5 (4.90%) | 0.064 |
| Mechanical ventilation | 59 (86.76%) | 97 (95.10%) | 0.053 |
| Septic shock | 60 (88.24%) | 97 (95.10%) | 0.099 |
| Outcomes and therapy | |||
| Steroid therapy | 58 (85.29%) | 96 (94.12%) | 0.054 |
| Tocilizumab | 13 (19.12%) | 26 (25.49%) | 0.333 |
| Transfer to ICU | 2.25 ± 4.11 | 2.34 ± 5.07 | 0.8996 |
| Length of ICU-stay | 22.56 ± 13.47 | 23.95 ± 16.09 | 0.5575 |
| Length of hospitalization | 24.84 ± 13.91 | 25.95 ± 19.04 | 0.6796 |
| Discharge status | 0.307 | ||
| Discharged | 16 (23.53%) | 17 (16.67%) | |
| Died | 48 (70.59%) | 82 (80.39%) | |
| Transferred for other hospitals | 4 (5.88%) | 3 (2.94%) | |
| Mortality at 30 days | 39 (57.35%) | 62 (60.78%) | 0.655 |
| Mortality more than 30 days (overall mortality) | 48 (70.59%) | 82 (80.39%) | 0.140 |
| Variables | Odds Ratio | CI 95% | p Value |
|---|---|---|---|
| COVID-19 infection | 2.06 | 0.9–4.72 | 0.087 |
| Diabetes Mellitus (DM) | 0.61 | 0.26–1.39 | 0.236 |
| Abnormal WBCs count | 0.55 | 0.25–1.2 | 0.131 |
| Abnormal CRP | 5.31 | 0.46–61.62 | 0.182 |
| Intravascular device | 3.05 | 0.54–17.21 | 0.207 |
| SOFA at positive culture time | 1.13 | 1.06–1.21 | 0.001 |
| Continuous renal replacement therapy (CRRT) | 0.52 | 0.22–1.19 | 0.119 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alenazi, T.A.; Shaman, M.S.B.; Suliman, D.M.; Alanazi, T.A.; Altawalbeh, S.M.; Alshareef, H.; Lahreche, D.I.; Al-Azzam, S.; Araydah, M.; Karasneh, R.; et al. The Impact of Multidrug-Resistant Acinetobacter baumannii Infection in Critically Ill Patients with or without COVID-19 Infection. Healthcare 2023, 11, 487. https://doi.org/10.3390/healthcare11040487
Alenazi TA, Shaman MSB, Suliman DM, Alanazi TA, Altawalbeh SM, Alshareef H, Lahreche DI, Al-Azzam S, Araydah M, Karasneh R, et al. The Impact of Multidrug-Resistant Acinetobacter baumannii Infection in Critically Ill Patients with or without COVID-19 Infection. Healthcare. 2023; 11(4):487. https://doi.org/10.3390/healthcare11040487
Chicago/Turabian StyleAlenazi, Thamer A., Maryam S. Bin Shaman, Durria M. Suliman, Turkiah A. Alanazi, Shoroq M. Altawalbeh, Hanan Alshareef, Doha I. Lahreche, Sayer Al-Azzam, Mohammad Araydah, Reema Karasneh, and et al. 2023. "The Impact of Multidrug-Resistant Acinetobacter baumannii Infection in Critically Ill Patients with or without COVID-19 Infection" Healthcare 11, no. 4: 487. https://doi.org/10.3390/healthcare11040487