
A Systematic Review of the Aerobic Exercise Program Variables for Patients with Non-Specific Neck Pain: Effectiveness and Clinical Applications


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Methods
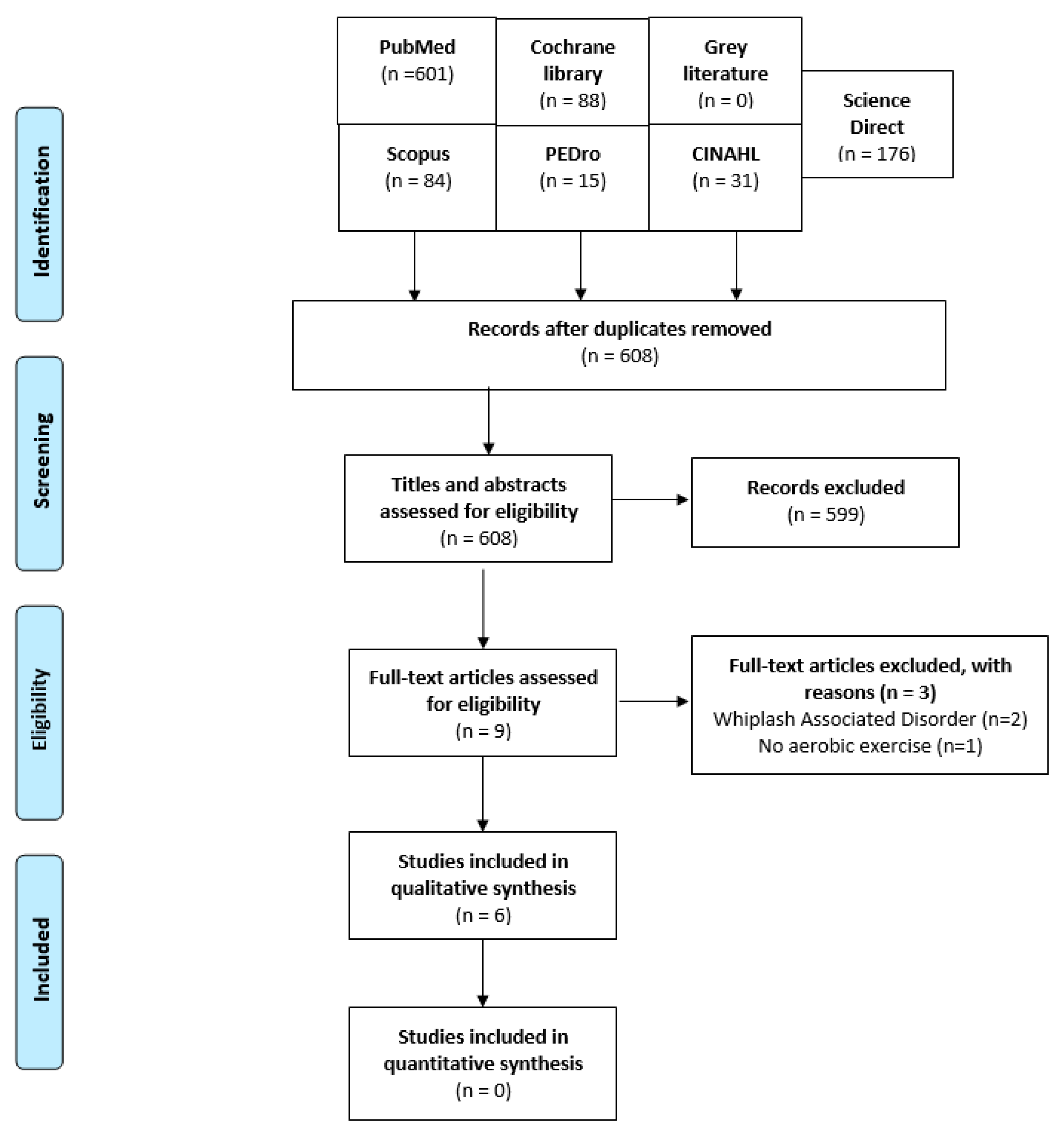
2.2. Study Selection
2.3. Eligibility Criteria Based on the PICOS Framework
2.3.1. Participants
2.3.2. Intervention
2.3.3. Comparison Groups
2.3.4. Outcome Measures
2.3.5. Study Design
2.4. Methodological Quality Assessment
2.5. Data Extraction
2.6. Evidence Synthesis
3. Results
3.1. Participants
3.2. Interventions
3.3. Outcome Measures
3.4. Methodological Quality
3.5. Program Variable Analysis
4. Discussion
4.1. Recommendations
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fejer, R.; Kyvik, K.O.; Hartvigsen, J. The prevalence of neck pain in the world population: A systematic critical review of the literature. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 2006, 15, 834–848. [Google Scholar] [CrossRef] [Green Version]
- Safiri, S.; Kolahi, A.-A.; Hoy, D.; Buchbinder, R.; Mansournia, M.A.; Bettampadi, D.; Ashrafi-Asgarabad, A.; Almasi-Hashiani, A.; Smith, E.; Sepidarkish, M.; et al. Global, regional, and national burden of neck pain in the general population, 1990-2017: Systematic analysis of the Global Burden of Disease Study 2017. BMJ 2020, 368, m791. [Google Scholar] [CrossRef] [Green Version]
- Manchikanti, L.; Singh, V.; Datta, S.; Cohen, S.P.; Hirsch, J.A. Comprehensive review of epidemiology, scope, and impact of spinal pain. Pain Physician 2009, 12, E35. [Google Scholar] [CrossRef]
- Haldeman, S.; Carroll, L.; Cassidy, J.D. Findings from the bone and joint decade 2000 to 2010 task force on neck pain and its associated disorders. J. Occup. Environ. Med. 2010, 52, 424–427. [Google Scholar] [CrossRef] [PubMed]
- Hurwitz, E.L.; Randhawa, K.; Yu, H.; Côté, P.; Haldeman, S. The Global Spine Care Initiative: A summary of the global burden of low back and neck pain studies. Eur. Spine J. 2018, 27, 796–801. [Google Scholar] [CrossRef]
- Hage, R.; Detrembleur, C.; Dierick, F.; Brismée, J.-M.; Roussel, N.; Pitance, L. Sensorimotor performance in acute-subacute non-specific neck pain: A non-randomized prospective clinical trial with intervention. BMC Musculoskelet. Disord. 2021, 22, 1017. [Google Scholar] [CrossRef]
- Price, J.; Rushton, A.; Tyros, V.; Heneghan, N.R. Expert consensus on the important chronic non-specific neck pain motor control and segmental exercise and dosage variables: An international e-Delphi study. PLoS ONE 2021, 16, e0253523. [Google Scholar] [CrossRef]
- Nikander, R.; Mälkiä, E.; Parkkari, J.; Heinonen, A.; Starck, H.; Ylinen, J. Dose-response relationship of specific training to reduce chronic neck pain and disability. Med. Sci. Sports Exerc. 2006, 38, 2068–2074. [Google Scholar] [CrossRef]
- Krøll, L.S.; Hammarlund, C.S.; Linde, M.; Gard, G.; Jensen, R.H. The effects of aerobic exercise for persons with migraine and co-existing tension-type headache and neck pain. A randomized, controlled, clinical trial. Cephalalgia 2018, 38, 1805–1816. [Google Scholar] [CrossRef]
- De Zoete, R.M.; Armfield, N.R.; McAuley, J.H.; Chen, K.; Sterling, M. Comparative effectiveness of physical exercise interventions for chronic non-specific neck pain: A systematic review with network meta-analysis of 40 randomised controlled trials. Br. J. Sports Med. 2021, 55, 730–742. [Google Scholar] [CrossRef]
- Sculco, A.D.; Paup, D.C.; Fernhall, B.; Sculco, M.J. Effects of aerobic exercise on low back pain patients in treatment. Spine J. 2001, 1, 95–101. [Google Scholar] [CrossRef]
- Thomas, E.N.; Blotman, F. Aerobic exercise in fibromyalgia: A practical review. Rheumatol. Int. 2010, 30, 1143–1150. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.; Khattab, S.; Haddad, C.; Babineau, J.; Furlan, A.; Kumbhare, D. Effect of aerobic exercise in the treatment of myofascial pain: A systematic review. J. Exerc. Rehabil. 2018, 14, 902. [Google Scholar] [CrossRef]
- Hoffman, M.D.; Hoffman, D.R. Does aerobic exercise improve pain perception and mood? A review of the evidence related to healthy and chronic pain subjects. Curr. Pain Headache Rep. 2007, 11, 93–97. [Google Scholar] [CrossRef]
- Laudisio, A.; Giovannini, S.; Finamore, P.; Loreti, C.; Vannetti, F.; Coraci, D.; Incalzi, R.A.; Zuccal, G.; Macchi, C.; Padua, L.; et al. Muscle strength is related to mental and physical quality of life in the oldest old. Arch. Gerontol. Geriatr. 2020, 89, 104109. [Google Scholar] [CrossRef]
- Giovannini, S.; Macchi, C.; Liperoti, R.; Laudisio, A.; Coraci, D.; Loreti, C.; Vannetti, F.; Onder, G.; Padua, L. Association of body fat with health-related quality of life and depression in nonagenarians: The Mugello Study. J. Am. Med. Dir. Assoc. 2019, 20, 564–568. [Google Scholar] [CrossRef]
- O’Riordan, C.; Clifford, A.; Van De Ven, P.; Nelson, J. Chronic neck pain and exercise interventions: Frequency, intensity, time, and type principle. Arch. Phys. Med. Rehabil. 2014, 95, 770–783. [Google Scholar] [CrossRef]
- Krøll, L.; Sjödahl Hammarlund, C.; Gard, G.; Jensen, R.H.; Bendtsen, L. Has aerobic exercise effect on pain perception in persons with migraine and coexisting tension-type headache and neck pain? A randomized, controlled, clinical trial. Eur. J. Pain 2018, 22, 1399–1408. [Google Scholar] [CrossRef]
- Daher, A.; Dar, G.; Carel, R. Effectiveness of combined aerobic exercise and neck-specific exercise compared to neck-specific exercise alone on work ability in neck pain patients: A secondary analysis of data from a randomized controlled trial. Int. Arch. Occup. Environ. Health 2021, 94, 1739–1750. [Google Scholar] [CrossRef]
- Daher, A.; Carel, R.S.; Tzipi, K.; Esther, H.; Dar, G. The effectiveness of an aerobic exercise training on patients with neck pain during a short- and long-term follow-up: A prospective double-blind randomized controlled trial. Clin. Rehabil. 2020, 34, 617–629. [Google Scholar] [CrossRef]
- Burnet, K.; Kelsch, E.; Zieff, G.; Moore, J.B.; Stoner, L. How fitting is FITT?: A perspective on a transition from the sole use of frequency, intensity, time, and type in exercise prescription. Physiol. Behav. 2019, 199, 33–34. [Google Scholar] [CrossRef] [PubMed]
- de Morton, N.A. The PEDro scale is a valid measure of the methodological quality of clinical trials: A demographic study. Aust. J. Physiother. 2009, 55, 129–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Popay, J.; Roberts, H.; Sowden, A.; Petticrew, M.; Arai, L.; Rodgers, M.; Britten, N.; Roen, K.; Duffy, S. Guidance on the conduct of narrative synthesis in systematic reviews. Prod. ESRC Methods Programme Version 2006, 1, b92. [Google Scholar]
- Özden, F.; Tümtürk, İ.; Yuvakgil, Z.; Sarı, L. The effectiveness of physical exercise in patients with lumbar spinal stenosis: A systematic review. Sport Sci. Health 2022, 18, 1129–1140. [Google Scholar] [CrossRef]
- Brage, K.; Ris, I.; Falla, D.; Søgaard, K.; Juul-Kristensen, B. Pain education combined with neck-and aerobic training is more effective at relieving chronic neck pain than pain education alone–A preliminary randomized controlled trial. Man. Ther. 2015, 20, 686–693. [Google Scholar] [CrossRef]
- Korshøj, M.; Jørgensen, M.B.; Lidegaard, M.; Mortensen, O.S.; Krustrup, P.; Holtermann, A.; Søgaard, K. Decrease in musculoskeletal pain after 4 and 12 months of an aerobic exercise intervention: A worksite RCT among cleaners. Scand. J. Public Health 2018, 46, 846–853. [Google Scholar] [CrossRef]
- Muyor, J.M. Exercise Intensity and Validity of the Ratings of Perceived Exertion (Borg and OMNI Scales) in an Indoor Cycling Session. J. Hum. Kinet. 2013, 39, 93–101. [Google Scholar] [CrossRef] [Green Version]
- Stefani, L.; Galanti, G.; Klika, R. Clinical implementation of exercise guidelines for cancer patients: Adaptation of ACSM’s guidelines to the Italian model. J. Funct. Morphol. Kinesiol. 2017, 2, 4. [Google Scholar] [CrossRef] [Green Version]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; LaMonte, M.J.; Lee, I.-M.; Nieman, D.C.; Swain, D.P. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef]
- Tan, L.; Cicuttini, F.M.; Fairley, J.; Romero, L.; Estee, M.; Hussain, S.M.; Urquhart, D.M. Does aerobic exercise effect pain sensitisation in individuals with musculoskeletal pain? A systematic review. BMC Musculoskelet. Disord. 2022, 23, 113. [Google Scholar] [CrossRef]
- Osthoff, A.K.R.; Niedermann, K.; Braun, J.; Adams, J.; Brodin, N.; Dagfinrud, H.; Duruoz, T.; Esbensen, B.A.; Günther, K.-P.; Hurkmans, E.; et al. 2018 EULAR recommendations for physical activity in people with inflammatory arthritis and osteoarthritis. Ann. Rheum. Dis. 2018, 77, 1251–1260. [Google Scholar] [CrossRef] [Green Version]
- Hordern, M.D.; Dunstan, D.; Prins, J.; Baker, M.; Singh, M.A.F.; Coombes, J. Exercise prescription for patients with type 2 diabetes and pre-diabetes: A position statement from Exercise and Sport Science Australia. J. Sci. Med. Sport 2012, 15, 25–31. [Google Scholar] [CrossRef]
- Stanton, R.; Happell, B. A Systematic Review of the Aerobic Exercise Program Variables for People with Schizophrenia. Curr. Sport. Med. Rep. 2014, 13, 260–266. [Google Scholar] [CrossRef] [PubMed]
- Dunbar, C.C.; Goris, C.; Michielli, D.W.; Kalinski, M.I. Accuracy and Reproducibility of an Exercise Prescription Based on Ratings of Perceived Exertion for Treadmill and Cycle Ergometer Exercise. Percept. Mot. Ski. 1994, 78, 1335–1344. [Google Scholar] [CrossRef] [PubMed]
- Kressler, J.; Cowan, R.; Ginnity, K.; Nash, M.S. Subjective measures of exercise intensity to gauge substrate partitioning in persons with paraplegia. Top. Spinal Cord Inj. Rehabil. 2012, 18, 205–211. [Google Scholar] [CrossRef] [Green Version]
- Smart, N.; Marwick, T.H. Exercise training for patients with heart failure: A systematic review of factors that improve mortality and morbidity. Am. J. Med. 2004, 116, 693–706. [Google Scholar] [CrossRef]
- Booth, J.; Moseley, L.; Schiltenwolf, M.; Cashin, A.; Davies, M.; Hübscher, M. Exercise for chronic musculoskeletal pain: A biopsychosocial approach. Musculoskelet. Care 2017, 15, 413–421. [Google Scholar] [CrossRef]
- Wewege, M.A.; Booth, J.; Parmenter, B.J. Aerobic vs. resistance exercise for chronic non-specific low back pain: A systematic review and meta-analysis. J. Back Musculoskelet. Rehabil. 2018, 31, 889–899. [Google Scholar] [CrossRef] [PubMed]
- Kanamori, S.; Takamiya, T.; Inoue, S.; Kai, Y.; Kawachi, I.; Kondo, K. Exercising alone versus with others and associations with subjective health status in older Japanese: The JAGES Cohort Study. Sci. Rep. 2016, 6, 39151. [Google Scholar] [CrossRef] [Green Version]
- Farrance, C.; Tsofliou, F.; Clark, C. Adherence to community based group exercise interventions for older people: A mixed-methods systematic review. Prev. Med. 2016, 87, 155–166. [Google Scholar] [CrossRef] [Green Version]
- Stanton, R.; Reaburn, P. Exercise and the treatment of depression: A review of the exercise program variables. J. Sci. Med. Sport 2014, 17, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Callaghan, P.; Khalil, E.; Morres, I.; Carter, T. Pragmatic randomised controlled trial of preferred intensity exercise in women living with depression. BMC Public Health 2011, 11, 465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perraton, L.G.; Kumar, S.; Machotka, Z. Exercise parameters in the treatment of clinical depression: A systematic review of randomized controlled trials. J. Eval. Clin. Pract. 2010, 16, 597–604. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Studies | Characteristics of the Sample | Characteristics of the Intervention | Outcome Measures | Aerobic Exercise Intensity/Duration/ Type/Supervision | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Sample/ Diagnosis/Women/Study Design | Dropout | Mean Age ± SD (yo) | Interventions | Number of Sessions | Frequency (Times/wk) | Period (wk) | Long Term Follow-Up (Months) | |||
| Daher et al., 2021 | N = 139; ΝΝP; Female: 106 Randomized trial | 0 | (A) 55 ± 10.4 (B) 54.1 ± 10.7 | (A) Aerobic Exercise group: neck-specific exercise PLUS moderate cycling exercise (60% of the age-predicted maximum heartrate) for 20 min during the first week, 30 min during the second week, and 45 min during the third to sixth weeks (N = 69) | 12 | 2 | 6 | 3 and 6 months | Work Ability Index (WAI), Global Rating of Change (GROC) | Moderate (60% of the age-predicted maximum heartrate)/20 min during the first week, 30 min during the second week and 45 min during the third week and the remaining six weeks/cycling exercise/Physiotherapists supervised all exercise programs. |
| (B) Neck exercises: supervised neck-specific exercise (N = 70) | 12 | 2 | 6 | |||||||
| Daher et al., 2020 | N = 139/NNP/Female: 106 (cont.) Randomized trial | 17 | (A) 55.0 ± 10.4 (B) 54.1 ± 10.7 | (A) Aerobic Exercise group: cycling exercise (60% of the age-predicted maximum heartrate) for 20 min during the first week, 30 min during the second week and 45 min during the third week and the remaining six weeks PLUS supervised neck-specific exercise (N = 62) | 12 | 2 | 6 | 3 and 6 months | Visual Analogue Scale (VAS), Neck Disability Index (NDI), Fear Avoidance Beliefs Questionnaire (FABQ) and cervicogenic headache | Moderate (60% of the age-predicted maximum heartrate)/20 min during the first week, 30 min during the second week and 45 min during the third week and the remaining six weeks/cycling exercise/physiotherapists supervised all exercise programs. |
| (B) Conventional group: supervised neck-specific exercise (N = 60) | 12 | 2 | 6 | |||||||
| Krøll et al., 2018 (a) | N= 70/Migraine and co-existing tension-type headache and neck pain/Female: 62 Randomized trial (cont.) | 18 | (A) 42 ± 10.9 (B) 36 ± 10.1 | (A) Aerobic Exercise group: 45 min of bike or cycling or brisk walking at a moderate intensity (14–16 RPE). (N = 26) | 36 | 3 | 12 | 6 months | The number of days with TTH and NP, pain intensity, pain duration, area under the curve of duration * pain intensity for migraine, TTH and NP, physical fitness, level of physical activity, psychological well-being, and perceived ability to perform daily activities. | Moderate to high. The exercise period was divided into 10 min of warm-up (corresponding to 11–13 RPE), 30 min of endurance training (corresponding to 14–16 RPE), and 5 min of cool-down (corresponding to 11–13 RPE)/45 min/Bike or brisk walking/physiotherapist supervised 1/3 of the program. |
| (B) Control group: did not receive any type of pain-modulating treatment. (N = 26) | - | - | 12 | |||||||
| Krøll et al., 2018 (b) | N = 70/Migraine and co-existing tension-type headache and neck pain/Female: 62 Randomized trial | 18 | (A) 42 ± 10.9 (B) 36 ± 10.1 | (A) Aerobic Exercise group: 45 min of bike or cycling or brisk walking at a moderate intensity (14–16 RPE). (N = 26) | 36 | 3 | 12 | 6 months | Pericranial tenderness, pain thresholds, supra-thresholds, and temporal summation | Moderate to high. The exercise period was divided into 10 min of warm-up (corresponding to 11–13 RPE), 30 min of endurance training (corresponding to 14–16 RPE), and 5 min of cool-down (corresponding to 11–13 RPE)/45 min/Bike or brisk walking/physiotherapist supervised 1/3 of the program |
| (B) Control group: did not receive any type of pain-modulating treatment. (N = 26) | - | - | 12 | |||||||
| Korshøj et al., 2017 | N = 116; NNP; Female: 88 (cont.) | 11 | (A) 44.9 ± 9.2 (B) 45.7 ± 8.1 | (A) Aerobic exercise group: Aerobic exercise ≥60% maximal oxygen consumption VO2 max with the following: aerobics, biking on a stationary bike, treadmill running, and circuit training for 30 min. (N = 57) | 40 | 2 | 16 and 48 | 4 and 12 months | Standardized Nordic Questionnaire for the Analyses of Musculoskeletal Symptoms for the following areas: neck, shoulders, arms/wrists, upper back, lower back, hip, knees, and feet/ankles. | Moderate. Heartrate reserve of 67%/30 min/aerobics, biking on a stationary bike, treadmill running, and circuit training/supervised (not reporting who). |
| (B) Reference group: lectures in health promotion (N = 59) | 2 | 2 h | - | |||||||
| Brage et al., 2015 | N = 15; NNP; Female: 15 Randomized trial | 0 | (A) 42.14 ± 10.8 (B) 40.7 ± 13.6 | (A) Pain education and exercise group: pain education (90 min) and specific training (neck-shoulder exercises, balance and aerobic training). Aerobic exercise included walking, jogging, swimming, cycling (N = 7) | 4 Pain education 8 for exercise | - | 8 | No follow-up | Neck pain, function and Global Perceived Effect (GPE), Surface electromyography (EMG) from neck flexor and extensor muscles during performance of the Cranio-Cervical Flexion Test (CCFT) and three postural control tests (two-legged: eyes open and closed, one-legged: eyes open) | Moderate; 11 and 14 on a Borg scale/The starting duration was set to 20% below the patient indication and progressed weekly by increasing the duration of training by 20% (up to a maximum of 30 min)/walking, swimming, cycling, jogging, or stick walking/no supervision |
| (B) Pain education group: Pain education only (90 min) (N = 8) | 4 Pain education | 8 | ||||||||
| Studies | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Y | Y | Y | Y | N | N | N | Y | Y | Y | Y | 7 |
| Y | Y | Y | Y | N | N | Y | Y | Y | Y | Y | 8 |
| Y | Y | Y | Y | N | N | N | N | N | Y | Y | 5 |
| Y | Y | Y | Y | N | N | N | N | N | Y | Y | 5 |
| Y | Y | N | Y | N | N | N | N | Y | Y | Y | 5 |
| Y | Y | Y | Y | N | N | Y | N | Y | Y | Y | 7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paraskevopoulos, E.; Koumantakis, G.A.; Papandreou, M. A Systematic Review of the Aerobic Exercise Program Variables for Patients with Non-Specific Neck Pain: Effectiveness and Clinical Applications. Healthcare 2023, 11, 339. https://doi.org/10.3390/healthcare11030339
Paraskevopoulos E, Koumantakis GA, Papandreou M. A Systematic Review of the Aerobic Exercise Program Variables for Patients with Non-Specific Neck Pain: Effectiveness and Clinical Applications. Healthcare. 2023; 11(3):339. https://doi.org/10.3390/healthcare11030339
Chicago/Turabian StyleParaskevopoulos, Eleftherios, George A. Koumantakis, and Maria Papandreou. 2023. "A Systematic Review of the Aerobic Exercise Program Variables for Patients with Non-Specific Neck Pain: Effectiveness and Clinical Applications" Healthcare 11, no. 3: 339. https://doi.org/10.3390/healthcare11030339