
Antecedents and Outcomes of Work Engagement among Psychiatric Nurses in Japan


1
Hyogo Prefectural Hyogo Mental Health Center, Kobe 651-1242, Japan
2
Department of Nursing, Graduate School of Health Sciences, Kobe University, Kobe 654-0142, Japan
3
Faculty of Policy Management, Keio University, Kanagawa 252-0882, Japan
4
Department of Nursing, Osaka Psychiatric Medical Center, Osaka 541-8567, Japan
*
Author to whom correspondence should be addressed.
Healthcare 2023, 11(3), 295; https://doi.org/10.3390/healthcare11030295
Submission received: 26 December 2022
/
Revised: 12 January 2023
/
Accepted: 14 January 2023
/
Published: 18 January 2023
Abstract
:While previous studies have examined antecedents and outcomes of work engagement among general nurses, studies among psychiatric nurses remain limited. This study aimed to explore the antecedents (i.e., job crafting and nursing practice environment) and outcomes (i.e., strength-oriented care attitudes, mental health, and turnover intention) of work engagement among psychiatric nurses in Japan. This cross-sectional study included 309 nurses from three psychiatric hospitals in Japan (valid response rate: 60.4%). Data collection using the self-administered questionnaire took place from July to August 2021. We performed Structural Equation Modeling to examine the directional relationships among variables. Job crafting (β = 0.57, p < 0.01) and nursing practice environment (β = 0.23, p = 0.01) exhibited positive effects on work engagement. Work engagement had positive effects on strength-oriented care attitudes (β = 0.15, p = 0.04) and mental health (β = 0.37, p < 0.01) as well as negative effects on intention to resign from their profession as a nurse (β = −0.17, p = 0.01). Job crafting and a healthier nursing practice environment could help enhance work engagement. Higher work engagement could contribute to improving strength-oriented care attitudes, mental health, and intention to resign from their profession as a nurse.
1. Introduction
The increased prevalence of mental illness has resulted in the growing demand for high-quality mental health care for patients of all ages [1]. Psychiatric nurses comprise the largest workforce among mental health professionals and provide close care to patients and their family members. Their job performance is directly related to quality of care in mental health services. However, they can often experience higher levels of emotional exhaustion and lower levels of personal accomplishment due to work-related stressors, such as physical, psychological, or verbal violence from patients, difficulties in nurse–patient relationships, and excessive workload [2,3,4]. These stressors experienced by psychiatric nurses could deteriorate job performance as well as mental health and turnover intention, leading to poor quality of care [5,6].
Work engagement, defined as “a positive, fulfilling, and work-related state of mind that is composed of (a) vigor, (b) dedication, and (c) absorption [7]”, has received attention in the fields of nursing [8]. Vigor means high levels of energy and mental resilience during work. Dedication refers to a sense of significance, enthusiasm, and pride. Absorption means complete concentration in one’s work [7]. In general, engaged employees have high levels of energy and better mental health [9]. While some empirical studies in general nurses showed higher work engagement could lead to high-quality care for patients [10,11,12,13,14], studies including psychiatric nurses remain limited [15,16]. Compared to general nurses, psychiatric nurses can often experience stressful situations more frequently, such as violence from patients, stress related to patient–nurse interpersonal relationships, and encountering suicidal attempts and self-harm [3]. According to past studies, such job characteristics may result in some differences in antecedents and outcomes of work engagement between psychiatric nurses and general nurses [4,5]. Further investigation is needed to explore the related factors of work engagement in psychiatric nurses.
Mental health care in recent years places importance on supporting the utilization and development of mentally ill patients’ preferences, abilities, hopes, and experiences, as well as the available resources and opportunities in their environments, which are considered “strengths” [17]. The strength-oriented care leads to many benefits for patients with mental illness, such as reduced length of hospitalization and improved adherence to medication as well as improved quality of life and life satisfaction [18,19]. However, no research examined the relationship between work engagement and strength-oriented care to date. Exploring this association among psychiatric nurses may provide great insights into the strategies for enhancing strength-oriented care attitudes, leading to high-quality mental health care.
Job crafting, defined as “the cognitive and physical change that individuals make in the task or relational boundaries of their work [20],” is proactive behaviors and cognitions that enhance their own resources. It consists of three components: changing the cognitive task boundaries (cognitive crafting), changing the job’s boundaries (task crafting), and changing the relational boundaries (relational crafting) [20]. These three components are theoretically responsible for helping employees have a positive attitude toward their work, enhancing work engagement [21,22]. However, no previous studies have empirically clarified the relationship between job crafting and work engagement among psychiatric nurses.
Nursing practice environment is defined as “the organizational characteristics of work settings that promote or inhibit nursing practice [23].” It is composed of (a) nurse participation in hospital affairs, (b) supervisors’ leadership and supports, (c) staffing and resource adequacy, (d) collegial nurse–physician relationship, and (e) nursing foundations for quality of care [23,24]. A supportive work environment for nursing practice could contribute to fostering nurses’ willingness to dedicate more effort into their work, leading to higher levels of work engagement through enhancing extrinsic motivation [15]. However, few studies have examined the relationship between nursing practice environment and work engagement among psychiatric nurses.
Past studies investigating outcomes of work engagement have reported that highly engaged nurses could tend to have better mental health [25] and lower turnover intention [11,26]. However, these studies did not include psychiatric nurses. It remains unclear whether work engagement could contribute to the improvement of these work-related outcomes among psychiatric nurses.
1.1. Aim
This study aimed to examine the antecedents and outcomes of work engagement among psychiatric nurses in Japan.
1.2. Conceptual Framework and Hypotheses in This Study
The Job Demands–Resources model (JD-R model) has routinely been adopted as a theoretical framework to delineate the antecedents and outcomes of work engagement [21]. Previous studies have also suggested that the JD-R model can be used to comprehensively understand work engagement and related factors among nurses [27,28]. According to this model, job resources (e.g., nursing practice environment) positively stimulate work engagement and improve work-related outcomes (e.g., job performance, mental health, and turnover intention) through a motivational process [21]. Job resources mean “physical, psychosocial, or organizational resources in the workplace for achieving personal work goals, reducing job stress, or facilitating personal growth and development [21]”. In addition, job crafting theoretically acts to improve job resources and then enhances work engagement in this model [21].
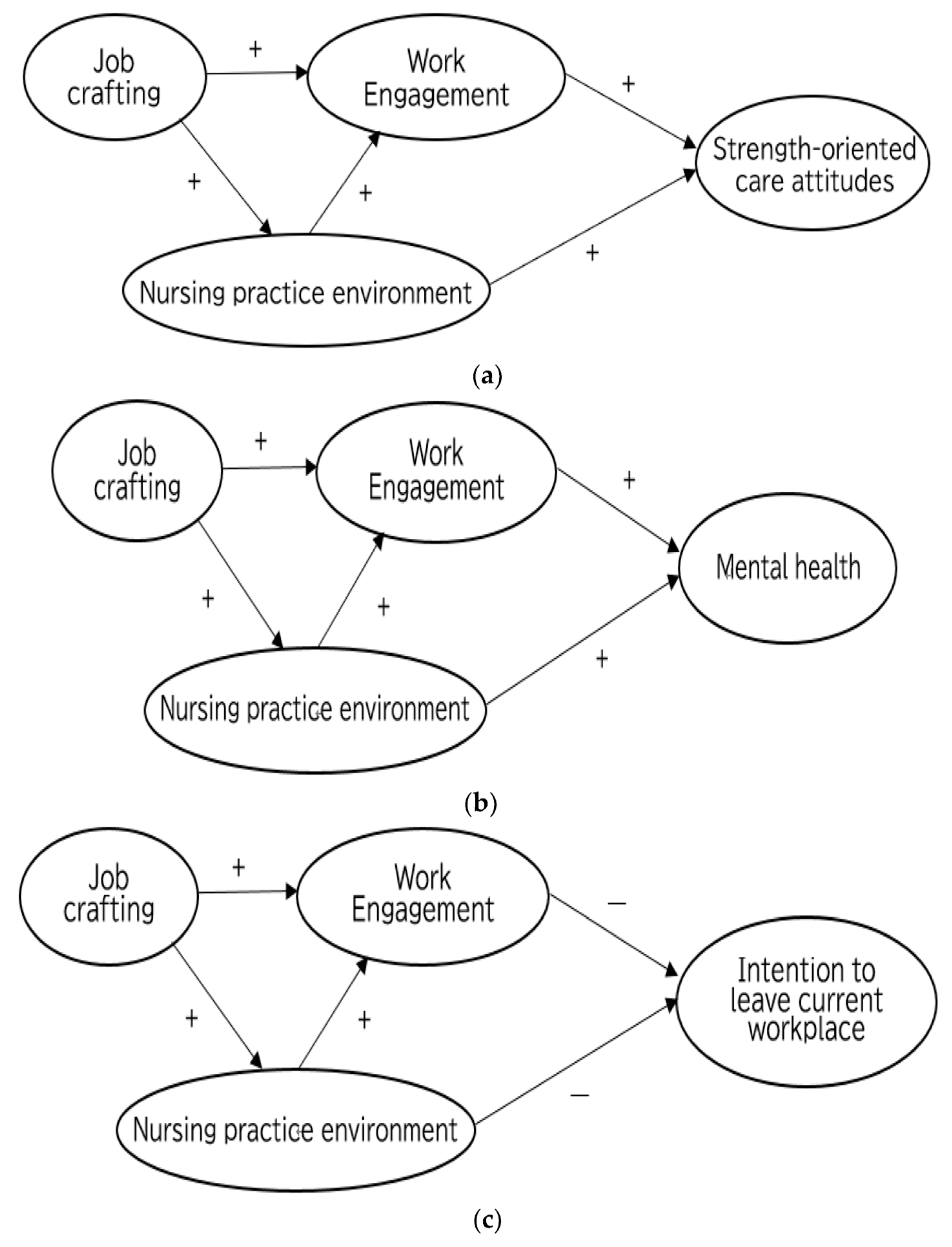
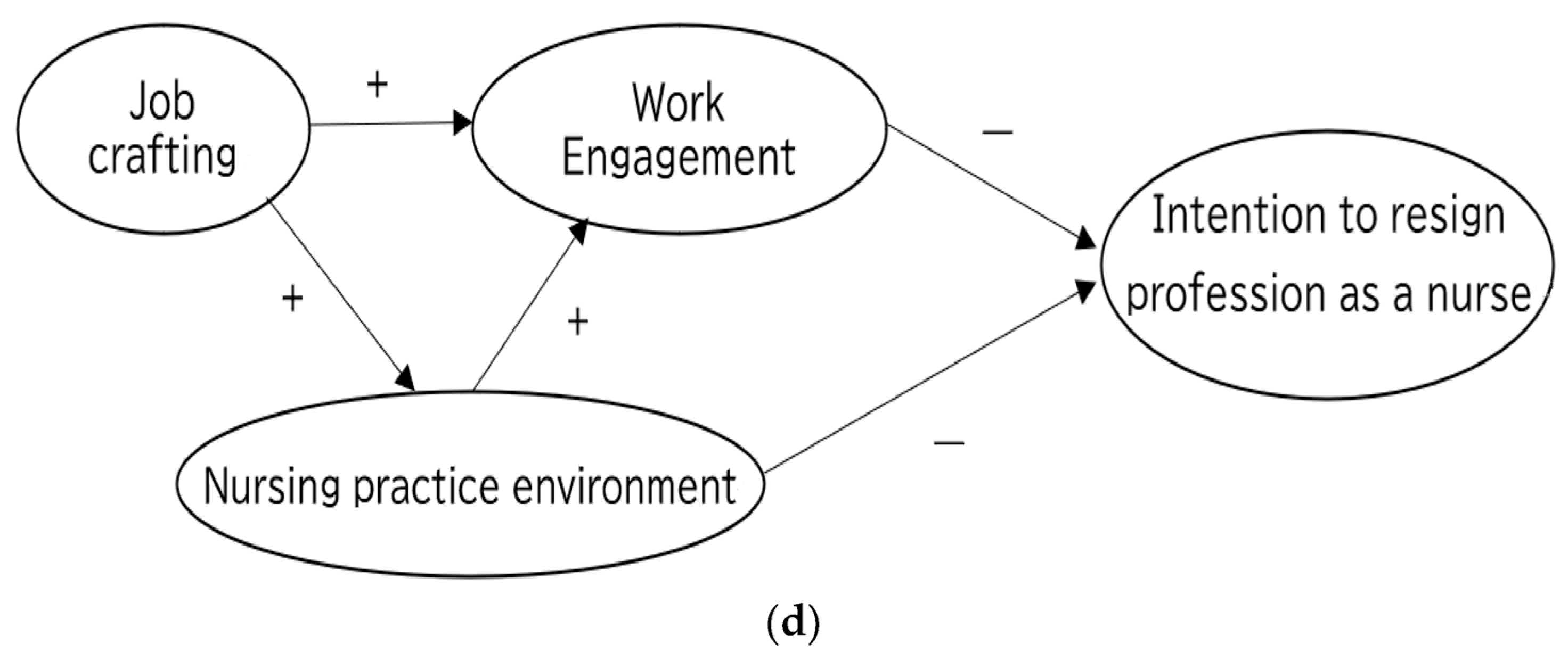
In this study, job crafting and nursing practice environment were considered as antecedents of work engagement. Strength-oriented care attitudes, mental health, and turnover intention (intention to leave current workplace and intention to resign from their profession as a nurse) were considered as outcomes of work engagement. Thus, we set the following hypotheses (Figure 1a–d), based on the JD-R model.
1.2.1. Antecedents of Work Engagement
Hypothesis 1.1.
Job crafting has a direct and positive effect on work engagement.
Hypothesis 1.2.
Job crafting has an indirect and positive effect on work engagement mediated by job resource (i.e., nursing practice environment).
Hypothesis 2.
Nursing practice environment has a direct and positive effect on work engagement.
1.2.2. Outcomes of Work Engagement
Hypothesis 3.1.
Work engagement has a direct and positive effect on strength-oriented care attitudes (Figure 1a).
Hypothesis 3.2.
Work engagement has a direct and positive effect on mental health (Figure 1b).
Hypothesis 3.3.
Work engagement has a direct and negative association with intention to leave current workplace (Figure 1c).
Hypothesis 3.4.
Work engagement has a direct and negative association with intention to resign from their profession as a nurse (Figure 1d).
1.2.3. Mediating Effects of Work Engagement
In the JD-R model [21], work engagement theoretically plays a role in mediating the relationships between job resources and work-related outcomes. Thus, we set the following hypotheses to explore the mediation effects of work engagement:
Hypothesis 4.1.
Work engagement mediates the association between nursing practice environment and strength-oriented care attitudes (Figure 1a).
Hypothesis 4.2.
Work engagement mediates the association between nursing practice environment and mental health (Figure 1b).
Hypothesis 4.3.
Work engagement mediates the association between nursing practice environment and intention to leave current workplace (Figure 1c).
Hypothesis 4.4.
Work engagement mediates the association between nursing practice environment and intention to resign from their profession as a nurse (Figure 1d).
2. Materials and Methods
2.1. Design
The current study was a cross-sectional study with quantitative analysis including hypotheses testing.
2.2. Participants and Settings
Participants consisted of psychiatric nurses from three psychiatric hospitals in the Kinki and Kyushu region of Japan, which were selected through convenience sampling. The inclusion criteria for psychiatric nurses were as follows: (a) registered or licensed practical nurses, (b) nurses directly engaged in psychiatric patient care, and (c) nurses working in wards or community care departments such as outpatient, home-visiting nursing stations, and psychiatric daycare. The nursing director and nursing deputy director were excluded because they mainly engaged in hospital management. This study had no restrictions on the participants by sociodemographic status (e.g., age, gender, or years of experience).
2.3. Procedures
After obtaining permission from the nursing directors, the investigators explained the purpose of this study, research methods, the principle of anonymity, and voluntary participation to all nursing directors and head nurses. Anonymous self-administered questionnaires and research description documents were subsequently distributed to all eligible nurses (n = 512) through head nurses at each department. When we distributed the questionnaires to the participants, we asked the head nurses to inform the participants that their cooperation in this study should be of their own free will. It took 20 to 30 min to complete the questionnaire forms, which was clearly stated in the description document. Completed questionnaires were placed into envelopes, sealed, and posted to a collection box located at the departments. Data collection took place from July to August 2021, which was during the COVID-19 pandemic.
2.4. Measurement
2.4.1. Work Engagement
Work engagement was assessed using the 9-item short version of the Utrecht Work Engagement Scale (UWES-9) [29,30]. This scale is composed of three subscales measuring: vigor (three items; e.g., “At my work, I feel like I am bursting with energy”), dedication (three items; e.g., “My job inspires me”), and absorption (three items; e.g., “I feel happy when I am working intensely”). It is a 7-point Likert scale ranging from 0 (never) to 6 (always), with higher scores indicating higher work engagement. The average scores of UWES-9 are calculated as an index of work engagement. The Japanese version of the UWES-9 was developed through the process of forward and back translation [30]. It showed good reliability, i.e., good internal consistency (Cronbach α = 0.92) and the test–retest reliability as well as good construct validity [30].
2.4.2. Job Crafting
Job crafting was assessed using Job Crafting Scale developed by Sekiguchi and his colleagues (2017) based on the conceptualization by Wrzesniewski and Dutton (2001) [20,31]. This scale was developed by dual-panel translation methods [31]. It comprises nine items assessing three subscales: task crafting (three items; e.g., “Adding or reducing tasks so that my job can be performed more smoothly”), relational crafting (three items; e.g., “Actively interacting with people through my job”), and cognitive crafting (three items; e.g., “Reframing my job as significant and meaningful”). It is a 7-point Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree). Each subscale score is calculated by dividing the sum of item scores by the number of the items, with higher scores indicating more job crafting behaviors. This scale was found to have acceptable internal consistency (Cronbach α = 0.67–0.80) and good construct validity [31].
2.4.3. Nursing Practice Environment
Nursing practice environment was assessed using the Japanese version of the Practice Environment Scale of the Nursing Work Index with a 4-point Likert scale ranging from 1 (strongly disagree) to 4 (strongly agree) [23,32]. A higher score indicates a more positive nursing practice environment. It consists of the following five subscales: (a) nurse participation in hospital affairs (nine items; e.g., “Opportunity for staff nurses to participate in policy decisions”), (b) manager’s ability, leadership, and support (five items; e.g., “A nurse manager who is a good manager and leader”), (c) staffing and resource adequacy (four items; e.g., “Enough registered nurses to provide quality patient care”), (d) collegial nurse–physician relations (three items; e.g., “Physicians and nurses have good working relationships”), and I nursing foundation for quality of care (ten items; e.g., “Active staff development or continuing education programs for nurses”). The average scores of each subscale are calculated as an index of each component of the nursing practice environment. This scale was developed through the process of forward and back translation procedure [32]. Each subscale was found to have acceptable reliability (Cronbach α = 0.76–0.86 and correlation coefficients based on the test–retest method = 0.65–0.83). Additionally, this scale showed acceptable validity and convergent validity [32].
2.4.4. Strength-Oriented Care Attitudes
Strength-oriented care attitudes were assessed using a scale developed in Japan by Niekawa and his colleagues (2012) [33]. It comprises eleven items, which are composed of three subcomponents measuring the person-centered approach (three items; e.g., “I actively have conversations with patients about their characters and values as well as their illnesses and symptoms”), shared decision making (three items; e.g., “Patients are involved in the conferences regarding goal setting and care planning”), and strength approach (three items; e.g., “I try to discover patient’s personal and environmental strengths through dialogue and involvement”). A higher score means higher strength-oriented care attitudes. All items are measured on a 4-point Likert scale ranging from 0 (rarely do) to 3 (do), and the average scores of this scale are calculated as an index of strength-oriented care attitudes. This scale was confirmed to have generally good convergent validity (Pearson’s correlation coefficient with the Recovery Attitude scale = 0.12–0.23, p < 0.05), test–retest reliability (ICC: 0.76–0.84), and internal consistency (Cronbach’s alpha coefficient: 0.65–0.87) [33].
2.4.5. Mental Health of Psychiatric Nurses
Mental health was assessed using the Japanese version of the 5-item World Health Organization Well-Being Index (WHO-5-J). The scale is among the most widely used questionnaires assessing mental health [34,35]. All items are measured on a 6-point Likert scale ranging from 0 (At no time) to 5 (All of the time). The total scores of WHO-5-J are calculated as an index of mental health. Higher scores indicate better mental health, and the total scores below 13 indicate low mental health status. The WHO-5-J was developed through forward and back translation procedures. It showed good reliability (Cronbach α = 0.89) and good construct validity [36,37].
2.4.6. Turnover Intention
Turnover intention was asked by two questions: “intention to leave current workplace” and “intention to resign [from their] profession as a nurse”, with reference to previous research [38,39]. Participants referred to the last 6 months when they responded to each question without considering the influence of the COVID-19 pandemic. Each item was rated on a 5-point Likert scale ranging from 1 (Not at all) to 5 (Very strongly). Higher scores indicated stronger turnover intention.
2.4.7. Demographic Variables
Demographic variables included age, gender, years of nursing experience, years of work tenure in psychiatric or mental health services, qualification, job position, employment status, educational level, and settings.
2.5. Statistical Analysis
We conducted a descriptive analysis of the study variables by using the software SPSS version 25 for Windows (IBM Corp., Armonk, NY, USA). Student’s t-test was performed to compare mean work engagement scores between subgroups of discrete variables. Pearson’s correlation coefficients were calculated to determine correlations between continuous variables.
We conducted structural equation modeling (SEM) to test our hypothetical model using the Amos version 26.0. software (IBM Corp., Armonk, NY, USA). In order to avoid overly complex models, SEM was performed for each of the four outcome variables: strength-oriented care attitudes (Model 1), mental health (Model 2), intention to leave current workplace (Model 3), and intention to resign from their profession as a nurse (Model 4). Bootstrap resampling with 1000 bootstrap samples was also performed to estimate confidence intervals. The bias-corrected confidence intervals were reported in this study. Latent constructs were identified by the observed indicators using parcels, as suggested by earlier studies [40,41]. Work engagement, job crafting, nursing practice environment, and strength-oriented care attitudes were parceled into each subcomponent (e.g., work engagement was parceled into its three factors (vigor, dedication, and absorption). Mental health was parceled into two elements through the division of odd and even numbered items of WHO-5-J. Moreover, each turnover intention variable (i.e., intention to leave current workplace and intention to resign from their profession as a nurse) was set with a path coefficient of 1 and an error variance value of 0.5.
Alongside the chi-square (χ2) statistic, we used the following fit indices to evaluate the model: the goodness-of-fit index (GFI), the adjusted goodness-of-fit index (AGFI), the Comparative Fit Index (CFI), the normed fit index (NFI), and the root mean square error of approximation index (RMSEA). A satisfying model needs to meet the following criteria: GFI > 0.90, AGFI > 0.90, CFI > 0.90, NFI > 0.90, and RMSEA < 0.05 [42]. Nevertheless, RMSEA < 0.08 was also acceptable, which has been recognized by researchers [43]. p values of less than 0.05 were considered statistically significant. All the tests were two-tailed.
2.6. Ethical Considerations
Participants received a written explanation of the aims, methods, voluntary nature of the study, and the protection of anonymity. Only those who agreed to participate in the study answered the questionnaire. The aims and procedures of this study were approved by the Institutional Review Board of the Graduate School of Health Science, Kobe University (No. 1009).
3. Results
Among 512 psychiatric nurses who received questionnaires, 325 returned the questionnaires (response rate: 63.5 %). However, 16 nurses were excluded due to missing responses regarding one or more items of the variables used in the main analysis. We used data from the remaining 309 participants to conduct the analyses in this study (valid response rate: 60.4%).
3.1. Participants’ Characteristics
Table 1 shows the characteristics of the participants. The mean age of the participants was 43.3 years (range: 20–65 years; SD = 10.7), and 54.7% were female. The average years of nursing experiences was 17.8 years (range: 0.3–44.3 years; SD = 10.6). Most of the psychiatric nurses were full-time (n = 295; 95.5%), registered nurses (n = 304; 98.4%), staff nurses (n = 239, 77.4%), and worked in inpatient psychiatric wards (n = 251; 81.2%).
3.2. Scores of Each Scale and Correlations between Scores for Each Scale
Table 2 shows the means, standard deviations, Cronbach’s α coefficients, and correlations of all scales included in this study. A mean score of work engagement among the total participants was 2.58 (SD = 1.01). The mean score of WHO-5-J in this study was 11.85 (SD = 5.25). No significant differences in work engagement were observed by study variables except for settings (i.e., wards/community care settings). Student’s t-test showed that the work engagement score of nurses in wards (M = 2.52, SD = 1.03) was significantly lower than those in community care settings (M = 2.85, SD = 0.92; t = −2.22, p = 0.03).
Cognitive crafting had a stronger positive relationship with work engagement than other variables (r = 0.59, p < 0.01) (Table 2).
3.3. Hypothesis Testing
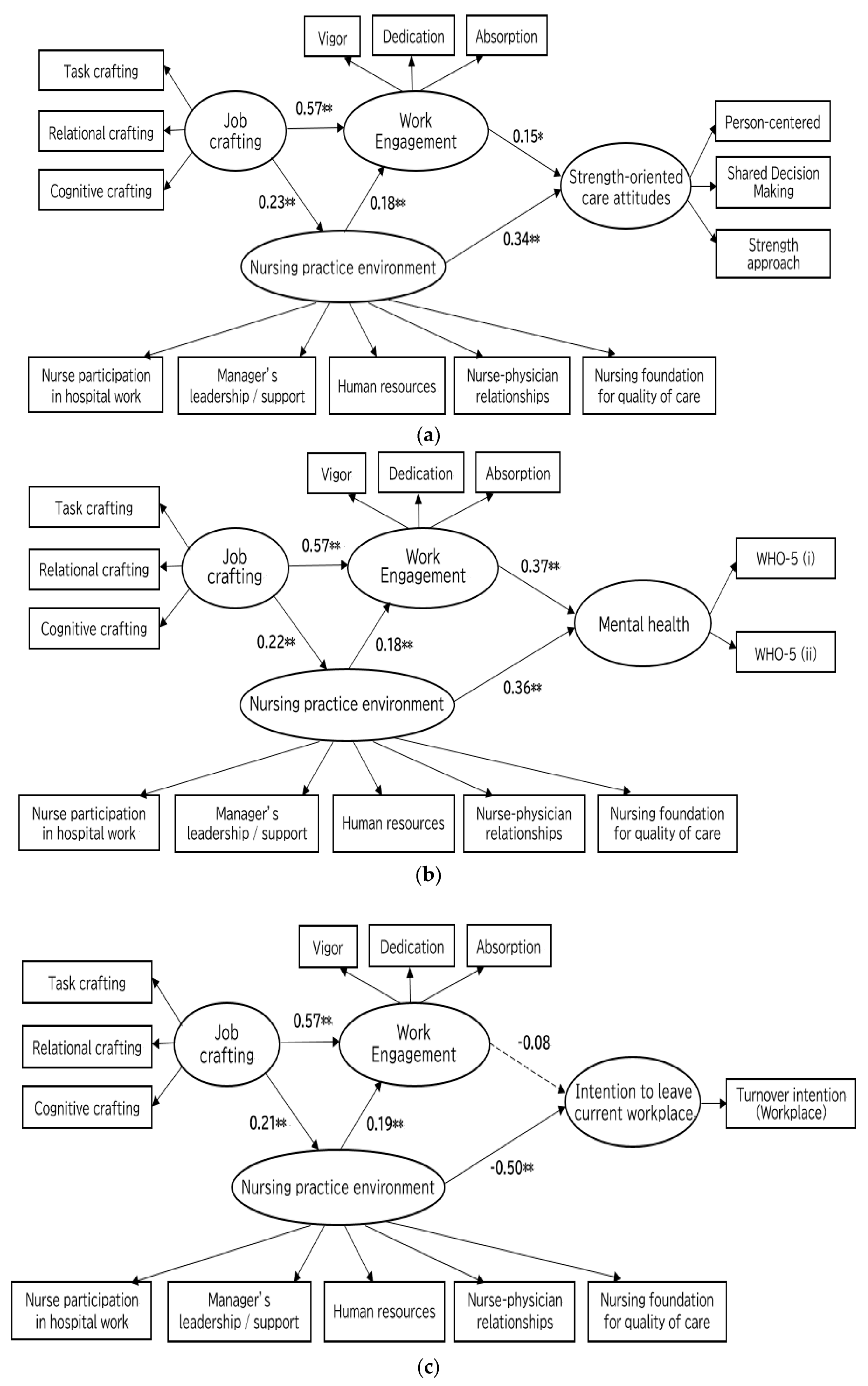
The results of the tests of hypothesized models regarding the antecedents and outcomes of work engagement among psychiatric nurses are shown in Figure 2a–d. Acceptable model fits were shown in all four models (Table 3). Additional analyses were completed by controlling for gender, job position, and settings (ward settings or community care settings) as potential confounders. The path coefficients remained virtually the same as those of all models in Figure 2, while the model fit was slightly lower (e.g., Model 1 with control variables had the following model fit indices; χ2 = 245.56, df = 108, GFI: 0.91, AGFI: 0.88, CFI: 0.94, NFI: 0.90, RMSEA: 0.07). The impact of the control variables on the model was weak. None of the control variables significantly affected the structural paths in the model (p’s > 0.05).
3.3.1. Antecedents of Work Engagement
The results of structural equation modeling for all four models showed that job crafting (e.g., in Model 1; β = 0.57, 95%CI; [0.44–0.69], p < 0.01) and nursing practice environment (e.g., in Model 1; β = 0.23, 95%CI; [0.07–0.36], p = 0.01) had direct and positive effects on work engagement (Figure 2). Moreover, job crafting had an indirect and positive effect on work engagement mediated by nursing practice environment (e.g., in Model 1; indirect effect = 0.04, 95%CI [0.02, 0.08], p = 0.01). Figure 2a–d showed the results regarding the direct and indirect effects of antecedents on work engagement for each model. Thereby, H1-a, H1-b, and H2 were supported.
3.3.2. Outcomes of Work Engagement
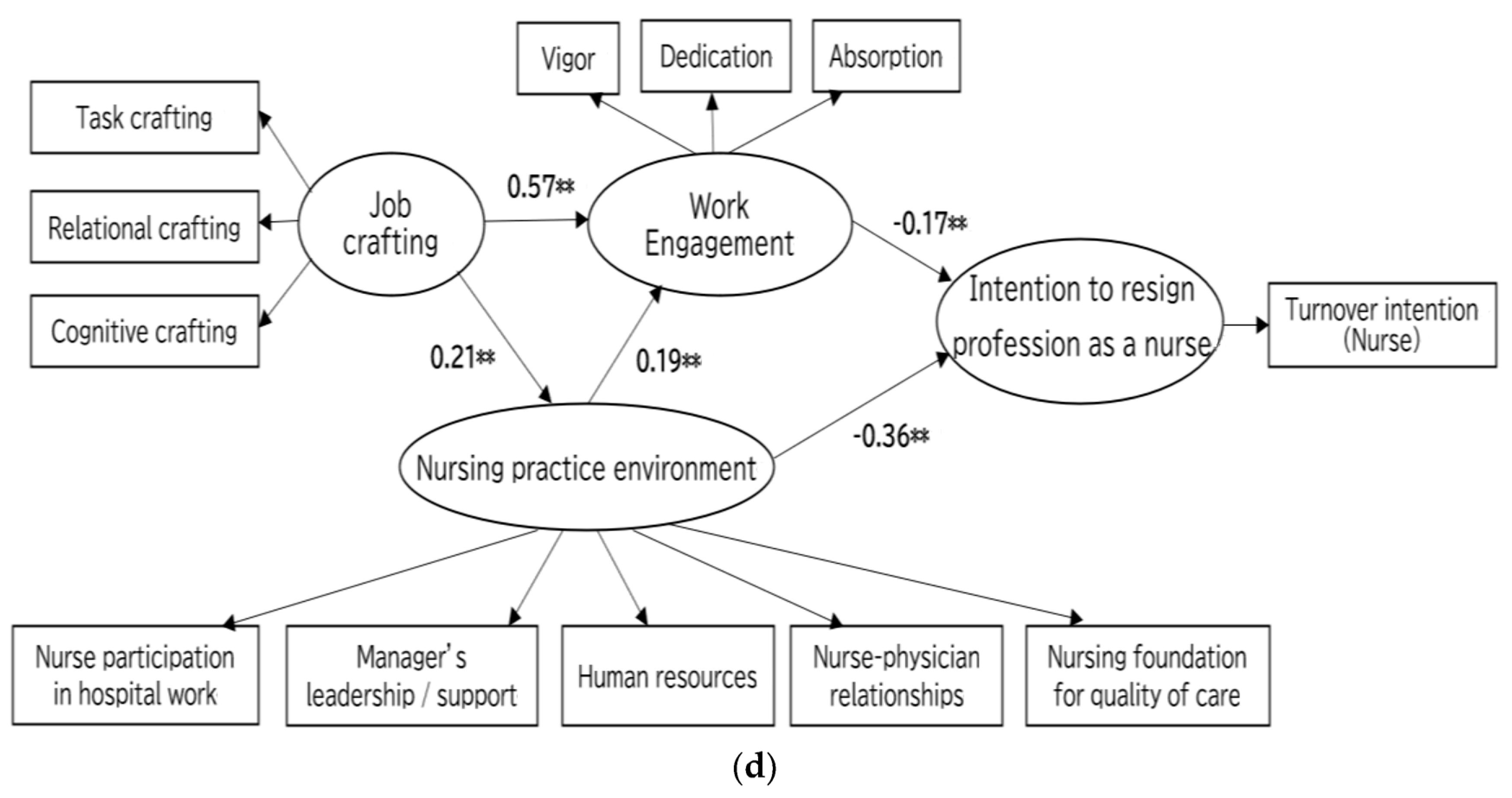
Work engagement had direct and positive effects on strength-oriented care attitudes (β = 0.15, 95%CI; [0.01, 0.29], p = 0.04) and mental health (β = 0.37, 95%CI; [0.23, 0.47], p < 0.01). Work engagement also had a direct and negative association with intention to resign from their profession as a nurse (β = −0.17, 95%CI; [−0.31, −0.04], p = 0.01), while it did not have a direct and significant association with intention to leave current workplace (β = −0.08, 95%CI; [−0.2, 0.07], p = 0.30). Thus, H3-a, H3-b, and H3-d were supported, but H3-c was not supported.
In addition, the nursing practice environment had direct and significant effects on strength-oriented care attitudes (β = 0.34, 95% CI; [0.21, 0.46], p < 0.01), mental health (β = 0.36, 95% CI; [0.24, 0.48], p < 0.01), intention to leave current workplace (β = −0.50, 95% CI; [−0.65, −0.36], p < 0.01), and intention to resign from their profession as a nurse (β = −0.36, 95% CI; [−0.52, −0.19], p < 0.01).
3.3.3. Mediating Effects of Work Engagement on Outcome Variables
Work engagement partly mediated the effects of nursing practice environment on strength-oriented care attitudes (0.03, 95%CI; [0.003, 0.07], p = 0.02), mental health (0.07, 95%CI; [0.03, 0.12], p < 0.01), and intention to resign from their profession as a nurse (−0.03, 95%CI; [−0.08, −0.01], p = 0.01), while it did not mediate the relationship between nursing practice environment and intention to leave current workplace (−0.01, 95%CI; [−0.05, 0.01], p = 0.2). Thus, H4-a, H4-b, and H4-d were supported, but H4-c was not supported.
4. Discussion
This study highlighted the possible antecedents (i.e., job crafting and nursing practice environment) and outcomes (i.e., strength-oriented care attitudes, mental health, and turnover intention) of work engagement among psychiatric nurses. Notably, job crafting and nursing practice environment had direct/indirect and positive effects on work engagement. Especially, job crafting had a greater impact on work engagement. Work engagement also had positive associations with strength-oriented care attitudes and mental health, while the effect of work engagement on strength-oriented care attitudes was small. In addition, work engagement had a negative relationship with intention to resign their profession as a nurse, while work engagement had no significant relationship with intention to leave their current workplace.
Regarding outcomes of work engagement, our study is the first to demonstrate the significant effects of work engagement on strength-oriented care attitudes, although the correlation was quite weak. Highly engaged nurses usually exhibit more energy and experience positive emotions at work [27]. Positive feelings toward patients can let nurses focus on patients’ strengths and potential rather than on their problems and shortcomings. Consequently, it would lead to a positive outlook toward patients’ recovery as well as better strengths-oriented care attitudes. These in turn might contribute to high-quality mental health care [8,44], including discharge support and care for realizing community life patients want [33]. Therefore, work engagement might be an important psychological driver for practicing strength-oriented care in the field of psychiatric nursing, where nurses sometimes have difficulty in having positive feelings due to negative experiences such as violence from patients. As this study was conducted during the COVID-19 pandemic, some difficulties might arise, due to the restrictions in patient involvement and discharge support in terms of infection prevention [45,46]. Since it may be difficult for psychiatric nurses to implement care plans based on strength orientation under these circumstances, the association between strength-oriented care attitudes and work engagement may have been weakened in this study.
Work engagement also had a positive impact on mental health among psychiatric nurses, which is consistent with the findings of previous studies among general nurses [25,47]. Highly engaged nurses may tend to have good mental health by fulfilling their needs for self-actualization through their work. This is a result of nurses easily having positive work-related emotions, despite sometimes facing difficulties at work. Additionally, COVID-19 causes nurses psychological distress and exacerbates depressive symptoms [46]. In fact, many participants in this study were in poor mental health conditions, as the average WHO-5-J scores were below 13. The psychological distress caused by the COVID-19 pandemic might weaken the association between work engagement and mental health. However, given our findings that showed the positive relationship between two variables even under these circumstances, work engagement may help psychiatric nurses maintain and improve their mental health.
The results in this study also suggested that work engagement could contribute to lower intention to resign their profession as a nurse. However, work engagement did not show a significant relationship with intention to leave their current workplace. Several previous studies have reported a negative association between work engagement and turnover intention [15,48]. However, these studies analyzed turnover intention as a single concept without distinguishing between intention to resign from their profession as a nurse and intention to leave their current workplace. The results of our study suggest that work engagement may have different effects on two types of turnover intention, respectively. Future research distinguishing these two types of turnover intentions and examining their relationship to work engagement may provide useful suggestions for preventive measures against nursing shortages and turnover from workplace.
Among antecedents of work engagement, job crafting had a direct/indirect and positive effect on psychiatric nurses’ work engagement. This was consistent with the findings of previous studies for general nurses [49,50,51]. Among three job-crafting components, cognitive crafting had the strongest correlation with work engagement. Cognitive crafting is related to higher self-efficacy by reframing one’s work as meaningful or redefining the purpose and the meaning of their work [21]. As the self-efficacy of psychiatric nurses tends to be low due to difficulties in mental care and work-related stressors [52], cognitive crafting can play a significant role to enhance psychiatric nurses’ self-efficacy, resulting in facilitating work engagement.
Nursing practice environment also had a direct and positive effect on work engagement. In addition, nursing practice environment was directly and positively associated with strength-oriented care attitudes and mental health as well as directly and negatively related with turnover intention (i.e., intention to resign from their profession as a nurse and intention to leave current workplace). In mental health care, psychiatric nurses carefully observe patients’ conditions including psychiatric symptoms to notice any changes and empower them to draw on their inner resources (e.g., their hopes and strength) through a positive therapeutic relationship [53,54]. A healthier nursing practice environment including collaborative relationships with physicians, plenty of support from supervisors, rich educational opportunities, and abundant human resources will help psychiatric nurses efficiently perform these professional tasks. Additionally, such a healthy nursing practice environment may contribute to not only the enhancement of their ability as psychiatric nurses but also the improvement in the difficulties they face regarding nurse–patient relationships. These work-related positive experiences may encourage them to engage in psychiatric nursing, ensuing the improvement of work-related outcomes. Given that the findings of this Japanese study were consistent with past studies in Western countries and other Asian countries [15,16,55], healthier nursing practice environment may be a key predictor for work engagement globally.
The results of this study should be interpreted with caution due to limitations. First, participants were selected from three psychiatric hospitals through convenience sampling, and psychiatric nurses at clinics or general hospitals were not included. Moreover, the majority of the participants were from wards. Since the work engagement score of nurses in wards was significantly lower than those in community care settings, generalizability should be confined. Second, since we used a cross-sectional design, causal relationships between work engagement and related factors were not confirmed. Future studies with longitudinal design among psychiatric nurses in various settings, including more community care settings, are needed. As this study was conducted during the COVID-19 pandemic with a specific stressful situation, further studies may reveal whether the result in this study is replicable after the pandemic.
Implications for Practice
This study suggested that work engagement is important for psychiatric nurses and nursing managers to improve work-related outcomes (i.e., strength-oriented care attitudes, mental health, and turnover intention). To enhance work engagement among psychiatric nurses, it may be important to incorporate job crafting (especially, cognitive crafting) into clinical practice and to improve nursing practice environment such as increasing supervisor’s support, making harmonious relationships with physicians and improving the nursing foundations for quality of care. One strategy to introduce cognitive crafting into practice may be to set educational opportunities for psychiatric nurses to re-think and reflect on the benefit and value of their work.
5. Conclusions
Job crafting and healthier nursing practice environment could enhance work engagement among psychiatric nurses. Higher work engagement as well as healthier nursing practice environment could help to improve work-related outcomes (i.e., strength-oriented care attitudes, mental health, and turnover intention), which may secondarily improve quality of mental health care.
Author Contributions
All of us have been sufficiently involved in this work as follows: Conceptualization/design: Y.K., R.C., Y.H., A.S. and T.S.; Data collection: Y.K. and T.S.; Writing—Original draft preparation: Y.K.; Writing—Review and editing: Y.K., R.C., Y.H., A.S. and T.S.; supervision: R.C., Y.H. and A.S.; analysis: Y.K., R.C., Y.H. and A.S. We take public responsibility for its validity and presentation as an original publication. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by the FRANCE BED MEDICAL HOME CARE RESEARCH SUBSIDY PUBLIC INTEREST INCORPORATED FOUNDATIONS 2021 [grant numbers 029]; JSPS KA-KENHI [grant number 19K10923].
Institutional Review Board Statement
This study received ethical approval by the Institutional Review Board of the Graduate School of Health Science, Kobe University (No. 1009).
Informed Consent Statement
All participants received full explanations in writing about the purpose and methods as well as the data storage and privacy protection methods employed. Those who agreed to participate in the study answered the questionnaire. Personal information and other data were handled and analyzed with appropriate precautions.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, R.C., upon reasonable request.
Acknowledgments
We would like to express our gratitude to the psychiatric nurses who responded to the questionnaire in the midst of the COVID-19 pandemic.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/mental-health-strengthening-our-response (accessed on 19 December 2022).
- Fallahi-Khoshknab, M.; Ghavidel, F.; Molavynejad, S.; Zarea, K. The role of organizational factors in nurse burnout: Experiences from Iranian nurses working in psychiatric wards. J. Fam. Med. Prim. Care 2019, 8, 3893–3899. [Google Scholar] [CrossRef] [PubMed]
- Rn, I.M.L.; Gómez-Urquiza, J.L.; Cañadas, G.R.; De La Fuente, E.I.; Albendín-García, L.; la Fuente, G.A.C. Prevalence of burnout in mental health nurses and related factors: A systematic review and meta-analysis. Int. J. Ment. Health Nurs. 2019, 28, 1035–1044. [Google Scholar] [CrossRef]
- Mukaihata, T.; Fujimoto, H.; Greiner, C. Factors influencing work engagement among psychiatric nurses in Japan. J. Nurs. Manag. 2020, 28, 306–316. [Google Scholar] [CrossRef]
- Curran, M.-J.; Rivera, R.R.; Knaplund, C.; Espinosa, L.; Cato, K.D. Engagement among psychiatric nurses: Is it different? How and why? Nurs. Manag. 2020, 51, 20–26. [Google Scholar] [CrossRef]
- Yoshizawa, K.; Sugawara, N.; Yasui-Furukori, N.; Danjo, K.; Furukori, H.; Sato, Y.; Tomita, T.; Fujii, A.; Nakagam, T.; Sasaki, M.; et al. Relationship between occupational stress and depression among psychiatric nurses in Japan. Arch. Environ. Occup. Health 2016, 71, 10–15. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Bakker, A.B. Job demands, job resources, and their relationship with burnout and engagement: A multi-sample study. J. Organ. Behav. 2004, 25, 293–315. [Google Scholar] [CrossRef] [Green Version]
- Keyko, K.; Cummings, G.G.; Yonge, O.; Wong, C.A. Work engagement in professional nursing practice: A systematic review. Int. J. Nurs. Stud. 2016, 61, 142–164. [Google Scholar] [CrossRef]
- Bakker, A.B.; Demerouti, E. Towards a model of work engagement. Career Dev. Int. 2008, 13, 209–223. [Google Scholar] [CrossRef] [Green Version]
- Abdelhadi, N.; Drach-Zahavy, A. Promoting patient care: Work engagement as a mediator between ward service climate and patient-centred care. J. Adv. Nurs. 2012, 68, 1276–1287. [Google Scholar] [CrossRef]
- Cao, T.; Huang, X.; Wang, L.; Li, B.; Dong, X.; Lu, H.; Wan, Q.; Shang, S. Effects of organisational justice, work engagement and nurses’ perception of care quality on turnover intention among newly licensed registered nurses: A structural equation modelling approach. J. Clin. Nurs. 2020, 29, 2626–2637. [Google Scholar] [CrossRef]
- Dong, X.; Lu, H.; Wang, L.; Zhang, Y.; Chen, J.; Li, B.; Huang, X.; Wan, Q.; Dong, S.; Shang, S. The effects of job characteristics, organizational justice and work engagement on nursing care quality in China: A mediated effects analysis. J. Nurs. Manag. 2020, 28, 559–566. [Google Scholar] [CrossRef]
- Freeney, Y.; Fellenz, M.R. Work engagement as a key driver of quality of care: A study with midwives. J. Health Organ. Manag. 2013, 27, 330–349. [Google Scholar] [CrossRef]
- Wong, C.A.; Laschinger, H.K.S.; Rn, G.G.C. Authentic leadership and nurses’ voice behaviour and perceptions of care quality. J. Nurs. Manag. 2010, 18, 889–900. [Google Scholar] [CrossRef]
- Huang, X.; Wang, L.; Dong, X.; Li, B.; Wan, Q. Effects of nursing work environment on work-related outcomes among psychiatric nurses: A mediating model. J. Psychiatr. Ment. Health Nurs. 2021, 28, 186–196. [Google Scholar] [CrossRef]
- Van Bogaert, P.; Clarke, S.; Willems, R.; Mondelaers, M. Staff engagement as a target for managing work environments in psychiatric hospitals: Implications for workforce stability and quality of care. J. Clin. Nurs. 2013, 22, 1717–1728. [Google Scholar] [CrossRef]
- Rapp, C.A.; Hisanaga, H. The philosophy and science of strengths model case management. Jpn. J. Psychiatr. Rehabil. 2010, 14, 6–16. [Google Scholar]
- Gottlieb, L.N.; Gottlieb, B.; Shamian, J. Principles of strengths-based nursing leadership for strengths-based nursing care: A new paradigm for nursing and healthcare for the 21st century. Nurs. Leadersh. 2012, 25, 38–50. [Google Scholar] [CrossRef] [PubMed]
- Tse, S.; Tsoi, E.W.; Hamilton, B.; O’Hagan, M.; Shepherd, G.; Slade, M.; Whitley, R.; Petrakis, M. Uses of strength-based interventions for people with serious mental illness: A critical review. Int. J. Soc. Psychiatry 2016, 62, 281–291. [Google Scholar] [CrossRef] [PubMed]
- Wrzesniewski, A.; Dutton, J.E. Crafting a Job: Revisioning Employees as Active Crafters of Their Work. Acad. Manag. Rev. 2001, 26, 179–201. [Google Scholar] [CrossRef]
- Bakker, A.B.; Demerouti, E. Job demands–resources theory: Taking stock and looking forward. J. Occup. Health Psychol. 2017, 22, 273–285. [Google Scholar] [CrossRef] [PubMed]
- Sakuraya, A.; Shimazu, A.; Imamura, K.; Kawakami, N. Effects of a Job Crafting Intervention Program on Work Engagement Among Japanese Employees: A Randomized Controlled Trial. Front. Psychol. 2020, 11, 235. [Google Scholar] [CrossRef]
- Lake, E.T. Development of the practice environment scale of the nursing work index. Res. Nurs. Health 2002, 25, 176–188. [Google Scholar] [CrossRef] [PubMed]
- Lake, E.T.; Hallowell, S.G.; Kutney-Lee, A.; Hatfield, L.A.; Del Guidice, M.; Boxer, B.A.; Ellis, L.N.; Verica, L.; Aiken, L.H. Higher Quality of Care and Patient Safety Associated With Better NICU Work Environments. J. Nurs. Care Qual. 2016, 31, 24–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kunie, K.; Kawakami, N.; Shimazu, A.; Yonekura, Y.; Miyamoto, Y. The relationship between work engagement and psychological distress of hospital nurses and the perceived communication behaviors of their nurse managers: A cross-sectional survey. Int. J. Nurs. Stud. 2017, 71, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Li, Z.; Wan, Q. Effects of work practice environment, work engagement and work pressure on turnover intention among community health nurses: Mediated moderation model. J. Adv. Nurs. 2019, 75, 3485–3494. [Google Scholar] [CrossRef]
- Bakker, A.B. An Evidence-Based Model of Work Engagement. Curr. Dir. Psychol. Sci. 2011, 20, 265–269. [Google Scholar] [CrossRef] [Green Version]
- Kato, Y.; Chiba, R.; Shimazu, A. Work Engagement and the Validity of Job Demands–Resources Model Among Nurses in Japan: A Literature Review. Work. Health Saf. 2021, 69, 323–342. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Bakker, A.B.; Salanova, M. The measurement of work engagement with a short questionnaire a cross-national study. Educ. Psychol. Meas. 2006, 66, 701–716. [Google Scholar] [CrossRef]
- Shimazu, A.; Schaufeli, W.; Kosugi, S.; Suzuki, A.; Nashiwa, H.; Kato, A.; Sakamoto, M.; Irimajiri, H.; Amano, S.; Hirohata, K.; et al. Work Engagement in Japan: Validation of the Japanese Version of the Utrecht Work Engagement Scale. Appl. Psychol. 2008, 57, 510–523. [Google Scholar] [CrossRef]
- Sekiguchi, T.; Li, J.; Hosomi, M. Predicting Job Crafting From the Socially Embedded Perspective: The Interactive Effect of Job Autonomy, Social Skill, and Employee Status. J. Appl. Behav. Sci. 2017, 53, 470–497. [Google Scholar] [CrossRef] [Green Version]
- Ogata, Y.; Nagano, M.; Nishioka, M. Preliminary study of the reliability and validity on the Practice Environment Scale of the Nursing Work Index, PES-NWI (Japanese version). J. Jpn. Soc. Healthc. Adm. 2010, 47, 69–80. [Google Scholar] [CrossRef]
- Niekawa, N.; Maeda, K.; Yamaguchi, S. The development of a scale for strength-oriented care attitudes among staff in community mental health care. In Research Report on Creating a Community-Based Psychiatric Medical Model and Its Effect Verification to Facilitate “Community-centered Life”; National Center of Neurology and Psychiatry: Tokyo, Japan, 2012; pp. 117–148. (In Japanese) [Google Scholar]
- Gao, J.; Weaver, S.R.; Dai, J.; Jia, Y.; Liu, X.; Jin, K.; Fu, H. Workplace Social Capital and Mental Health among Chinese Employees: A Multi-Level (2012), Cross-Sectional Study. PLoS ONE 2014, 9, e85005. [Google Scholar] [CrossRef]
- Kuehner, C.; Schultz, K.; Gass, P.; Meyer-Lindenberg, A.; Dreßing, H. Mental Health Status in the Community During the COVID-19-Pandemic. Psychiatr. Prax. 2020, 47, 361–369. [Google Scholar] [CrossRef]
- Awata, S.; Bech, P.; Koizumi, Y.; Seki, T.; Kuriyama, S.; Hozawa, A.; Ohmori, K.; Nakaya, N.; Matsuoka, H.; Tsuji, I. Validity and utility of the Japanese version of the WHO-Five Well-Being Index in the context of detecting suicidal ideation in elderly community residents. Int. Psychogeriatrics 2007, 19, 77–88. [Google Scholar] [CrossRef]
- Awata, S.; Bech, P.; Yoshida, S.; Hirai, M.; Suzuki, S.; Yamashita, M.; Ohara, A.; Hinokio, Y.; Matsuoka, H.; Oka, Y. Reliability and validity of the Japanese version of the World Health Organization-Five Well-Being Index in the context of detecting depression in diabetic patients. Psychiatry Clin. Neurosci. 2007, 61, 112–119. [Google Scholar] [CrossRef]
- Labrague, L.J.; Nwafor, C.E.; Tsaras, K. Influence of toxic and transformational leadership practices on nurses’ job satisfaction, job stress, absenteeism and turnover intention: A cross-sectional study. J. Nurs. Manag. 2020, 28, 1104–1113. [Google Scholar] [CrossRef]
- Nantsupawat, A.; Kunaviktikul, W.; Nantsupawat, R.; Wichaikhum, O.-A.; Thienthong, H.; Poghosyan, L. Effects of nurse work environment on job dissatisfaction, burnout, intention to leave. Int. Nurs. Rev. 2017, 64, 91–98. [Google Scholar] [CrossRef]
- Little, T.D.; Rhemtulla, M.; Gibson, K.; Schoemann, A.M. Why the items versus parcels controversy needn’t be one. Psychol. Methods 2013, 18, 285–300. [Google Scholar] [CrossRef] [Green Version]
- Matsunaga, M. Item Parceling in Structural Equation Modeling: A Primer. Commun. Methods Meas. 2008, 2, 260–293. [Google Scholar] [CrossRef]
- Wu, M.L. The Structural Equation Model: AMOS Operation and Application; Chongqing University Press: Chongqing, China, 2010; pp. 236–237. [Google Scholar]
- Schermelleh-Engel, K.; Moosbrugger, H.; Müller, H. Evaluating the Fit of Structural Equation Models: Tests of Significance and Descriptive Goodness-of-Fit Measures. Methods Psychol. Res. 2003, 8, 23–74. [Google Scholar]
- Bakker, A.B. Strategic and proactive approaches to work engagement. Organ. Dyn. 2017, 46, 67–75. [Google Scholar] [CrossRef]
- Bhandari, M.; Yadav, U.; Dahal, T.; Karki, A. Depression, Anxiety and Stress among Nurses Providing Care to the COVID-19 Patients: A Descriptive Cross-sectional Study. J. Nepal Med. Assoc. 2022, 60, 151–154. [Google Scholar] [CrossRef]
- Inamata, Y.; Furuya, I.; Oozeki, H.; Miyabayashi, I. Impact and current status of visitation restrictions caused by COVID-19 -Using Riessman’s thematic analysis. Seisen Jogakuin Coll. J. Nurs. 2022, 2, 41–56. [Google Scholar]
- García-Iglesias, J.J.; Gómez-Salgado, J.; Ortega-Moreno, M.; Navarro-Abal, Y. Relationship Between Work Engagement, Psychosocial Risks, and Mental Health Among Spanish Nurses: A Cross-Sectional Study. Front. Public Health 2021, 8, 627472. [Google Scholar] [CrossRef]
- Kiky, S.; Daniel, L. Work Engagement and Turnover Intention: The Moderating Effect of Organizational Justice. Adv. Soc. Sci. Educ. Humanit. Res. 2021, 570, 58–65. [Google Scholar] [CrossRef]
- Baghdadi, N.A.; Aliem, S.M.F.A.; Alsayed, S.K. The relationship between nurses’ job crafting behaviours and their work engagement. J. Nurs. Manag. 2021, 29, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Deetz, J.M.; Davidson, J.E.; Daugherty, J.; Graham, P.; Carroll, D.M. Exploring correlation of nurse manager meaning and joy in work with employee engagement. Appl. Nurs. Res. 2020, 55, 151297. [Google Scholar] [CrossRef]
- Jutengren, G.; Jaldestad, E.; Dellve, L.; Eriksson, A. The Potential Importance of Social Capital and Job Crafting for Work Engagement and Job Satisfaction among Health-Care Employees. Int. J. Environ. Res. Public Health 2020, 17, 4272. [Google Scholar] [CrossRef]
- Yada, H.; Abe, H.; Odachi, R.; Adachi, K. Exploration of the factors related to self-efficacy among psychiatric nurses. PLoS ONE 2020, 15, e0230740. [Google Scholar] [CrossRef]
- Berg, A.; Hallberg, I.R. Psychiatric nurses’ lived experiences of working with inpatient care on a general team psychiatric ward. J. Psychiatr. Ment. Health Nurs. 2000, 7, 323–333. [Google Scholar] [CrossRef]
- Delaney, K.R.; Johnson, M.E. Metasynthesis of Research on the Role of Psychiatric Inpatient Nurses: What is important to staff? J. Am. Psychiatr. Nurses Assoc. 2014, 20, 125–137. [Google Scholar] [CrossRef] [PubMed]
- Gillet, N.; Le Gouge, A.; Pierre, R.; Bongro, J.; Méplaux, V.; Brunault, P.; Guyetant, S.; Fremont, C.; Camus, V.; Colombat, P.; et al. Managerial style and well-being among psychiatric nurses: A prospective study. J. Psychiatr. Ment. Health Nurs. 2019, 26, 265–273. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
(a): Hypothesized model (Model 1) for antecedents and outcome (strength-oriented care attitudes) of work engagement among psychiatric nurses. (b): Hypothesized model (Model 2) for antecedents and outcome (mental health) of work engagement among psychiatric nurses. (c): Hypothesized model (Model 3) for antecedents and outcome (intention to leave current workplace) of work engagement among psychiatric nurses. (d): Hypothesized model (Model 4) for antecedents and outcome (intention to resign from their profession as a nurse) of work engagement among psychiatric nurses. Note: + means the hypothesized relationship is positive, − means the hypothesized relationship is negative.
Figure 1.
(a): Hypothesized model (Model 1) for antecedents and outcome (strength-oriented care attitudes) of work engagement among psychiatric nurses. (b): Hypothesized model (Model 2) for antecedents and outcome (mental health) of work engagement among psychiatric nurses. (c): Hypothesized model (Model 3) for antecedents and outcome (intention to leave current workplace) of work engagement among psychiatric nurses. (d): Hypothesized model (Model 4) for antecedents and outcome (intention to resign from their profession as a nurse) of work engagement among psychiatric nurses. Note: + means the hypothesized relationship is positive, − means the hypothesized relationship is negative.


Figure 2.
(a). The result of Model 1 regarding antecedents and outcome (strength-oriented care attitudes) of work engagement among psychiatric nurses. Note: * p < 0.05, ** p < 0.01. Indirect effect of job crafting on work engagement mediated by nursing practice environment; 0.04, 95%CI [0.02, 0.08], p = 0.01. (b). The result of Model 2 regarding antecedents and outcome (mental health) of work engagement among psychiatric nurses. Note: * p < 0.05, ** p < 0.01. WHO-5 (i) means the total score of the odd-numbered items (i.e., items 1, 3, and 5) on the WHO-5-J. WHO-5 (ii) means the total score of the even-numbered items (i.e., items 2 and 4) on the WHO-5-J. Indirect effect of job crafting on work engagement mediated by nursing practice environment; 0.04, 95%CI [0.01, 0.08], p = 0.01. (c). The result of Model 3 regarding antecedents and outcome (intention to leave current workplace) of work engagement among psychiatric nurses. Note: * p < 0.05, ** p < 0.01. Dotted line represents nonsignificant path (p > 0.05). Indirect effect of job crafting on work engagement mediated by nursing practice environment; 0.04, 95%CI [0.01, 0.08], p = 0.01. (d). The result of Model 4 regarding antecedents and outcome (intention to resign from their profession as a nurse) of work engagement among psychiatric nurses. Note: * p < 0.05, ** p < 0.01. Indirect effect of job crafting on work engagement mediated by nursing practice environment; 0.04, 95%CI [0.01, 0.08], p = 0.01.
Figure 2.
(a). The result of Model 1 regarding antecedents and outcome (strength-oriented care attitudes) of work engagement among psychiatric nurses. Note: * p < 0.05, ** p < 0.01. Indirect effect of job crafting on work engagement mediated by nursing practice environment; 0.04, 95%CI [0.02, 0.08], p = 0.01. (b). The result of Model 2 regarding antecedents and outcome (mental health) of work engagement among psychiatric nurses. Note: * p < 0.05, ** p < 0.01. WHO-5 (i) means the total score of the odd-numbered items (i.e., items 1, 3, and 5) on the WHO-5-J. WHO-5 (ii) means the total score of the even-numbered items (i.e., items 2 and 4) on the WHO-5-J. Indirect effect of job crafting on work engagement mediated by nursing practice environment; 0.04, 95%CI [0.01, 0.08], p = 0.01. (c). The result of Model 3 regarding antecedents and outcome (intention to leave current workplace) of work engagement among psychiatric nurses. Note: * p < 0.05, ** p < 0.01. Dotted line represents nonsignificant path (p > 0.05). Indirect effect of job crafting on work engagement mediated by nursing practice environment; 0.04, 95%CI [0.01, 0.08], p = 0.01. (d). The result of Model 4 regarding antecedents and outcome (intention to resign from their profession as a nurse) of work engagement among psychiatric nurses. Note: * p < 0.05, ** p < 0.01. Indirect effect of job crafting on work engagement mediated by nursing practice environment; 0.04, 95%CI [0.01, 0.08], p = 0.01.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Demographics of the participants (n = 309).
| Sociodemographic Variables | Mean ± SD [Range] or Number (%) |
|---|---|
| Age | 43.3 ± 10.7 [20–65] |
| Gender | |
| Male | 133 (43.0) |
| Female | 169 (54.7) |
| Unknown | 7 (2.3) |
| Years of nursing experiences | 17.8 ± 10.6 [0.3–44.3] |
| Years of work tenure in psychiatric or mental health services | 13.7 ± 9.9 [0.2–44.3] |
| Qualification | |
| Registered nurses | 304 (98.4) |
| Licensed practical nurses | 3 (1.0) |
| Unknown | 2 (0.6) |
| Job Position | |
| Head nurse | 22 (7.1) |
| Deputy head | 13 (4.2) |
| Chief nurse | 35 (11.3) |
| Staff nurse | 239 (77.4) |
| Employment status | |
| Full-time | 295 (95.5) |
| Part-time | 12 (3.9) |
| Unknown | 2 (0.6) |
| Education level | |
| Four-year college degree or above | 68 (22.0) |
| Lower than college degree | 233 (75.5) |
| Unknown | 8 (2.5) |
| Settings | |
| Ward settings | 251 (81.2) |
| Acute psychiatric ward | 106 (34.4) |
| Chronic psychiatric ward | 107 (34.5) |
| Medical treatment and supervision ward | 21 (6.8) |
| Child adolescent psychiatric ward | 12 (3.9) |
| COVID-19-related ward | 5 (1.6) |
| Community care settings | 57 (18.5) |
| Outpatient | 15 (4.9) |
| Home-visit nursing station | 29 (9.4) |
| Psychiatric daycare | 13 (4.2) |
| Unknown | 1 (0.3) |
Note: SD; Standard Deviation.
Table 2.
Pearson’s correlations coefficients, means, and standard deviations of the variables in this study (n = 309).
Table 2.
Pearson’s correlations coefficients, means, and standard deviations of the variables in this study (n = 309).
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 Task crafting §1 | 1 | ||||||||||||
| 2 Relational crafting §1 | 0.58 ** | 1 | |||||||||||
| 3 Cognitive crafting §1 | 0.47 ** | 0.60 ** | 1 | ||||||||||
| 4 Participation opportunity in work §2 | 0.15* | 0.15 ** | 0.25 ** | 1 | |||||||||
| 5 Supervisors’ leadership and support §2 | 0.04 | 0.10 | 0.18 ** | 0.52 ** | 1 | ||||||||
| 6 Human resources §2 | 0.06 | 0.08 | 0.07 | 0.46 ** | 0.38 ** | 1 | |||||||
| 7 Nurse–physician collaborations §2 | 0.08 | 0.13 * | 0.24 ** | 0.39 ** | 0.35 ** | 0.40 ** | 1 | ||||||
| 8 Foundation for quality of care §2 | 0.02 | 0.07 | 0.13 * | 0.63 ** | 0.50 ** | 0.61 ** | 0.46 ** | 1 | |||||
| 9 Strength-oriented care attitudes §3 | 0.32 ** | 0.30 ** | 0.29 ** | 0.29 ** | 0.16 ** | 0.28 ** | 0.13 * | 0.32 ** | 1 | ||||
| 10 Mental health §4 | 0.20 ** | 0.34 ** | 0.32 ** | 0.30 ** | 0.31 ** | 0.34 ** | 0.32 ** | 0.36 ** | 0.28 ** | 1 | |||
| 11 Intention to leave current workplace | −0.04 | −0.13 * | −0.11 * | −0.31 ** | −0.28 ** | −0.37 ** | −0.25 ** | −0.34 ** | −0.09 | −0.32 ** | 1 | ||
| 12 Intention to resign from their profession as a nurse | −0.10 | −0.13 * | −0.12 * | −0.25 ** | −0.21 ** | −0.28 ** | −0.23 ** | −0.24 ** | −0.08 | −0.39 ** | 0.76 ** | 1 | |
| 13 Work engagement §5 | 0.30 ** | 0.47 ** | 0.59 ** | 0.32 ** | 0.18 ** | 0.14 * | 0.16 ** | 0.18 ** | 0.23 ** | 0.42 ** | −0.17 ** | −0.21 ** | 1 |
| [Min, Max] | [1, 7] | [1, 7] | [1, 7] | [1, 4] | [1, 4] | [1, 4] | [1, 4] | [1.1, 4] | [0, 3] | [0, 25] | [1, 5] | [1, 5] | [0, 5.56] |
| Mean | 4.67 | 4.60 | 4.53 | 2.45 | 2.91 | 2.40 | 2.80 | 2.62 | 1.69 | 11.85 | 2.25 | 1.27 | 2.58 |
| SD | 1.05 | 1.03 | 1.14 | 0.51 | 0.62 | 0.66 | 0.51 | 0.51 | 0.50 | 5.25 | 2.02 | 1.20 | 1.01 |
| Cronbach’s α coefficient in this study | 0.81 | 0.83 | 0.87 | 0.84 | 0.92 | 0.87 | 0.85 | 0.88 | 0.88 | 0.93 | - | - | 0.93 |
Note: §1: Job Crafting Scale, §2: Practice Environment Scale of the Nursing Work Index, §3: The scale for strength-oriented care attitudes, §4: The Japanese version of the 5-item World Health Organization Well-Being Index, §5: The 9-item short version of the Utrecht Work Engagement Scale. * p < 0.05, ** p < 0.01. SD; Standard Deviation. Cronbach’s α coefficients for intention to leave current workplace and intention to resign from their profession as a nurse were not calculated due to single items.
Table 3.
Fit indices for all hypothetical models.
| Models | χ2 | df | GFI | AGFI | CFI | NFI | RMSEA |
|---|---|---|---|---|---|---|---|
| Model 1 | 176.38 | 72 | 0.93 | 0.89 | 0.95 | 0.93 | 0.07 |
| Model 2 | 156.59 | 60 | 0.93 | 0.89 | 0.96 | 0.93 | 0.07 |
| Model 3 | 120.73 | 50 | 0.94 | 0.90 | 0.96 | 0.94 | 0.07 |
| Model 4 | 125.09 | 50 | 0.94 | 0.90 | 0.96 | 0.93 | 0.07 |
Note: Models 1–4 tested the relationships among antecedents, work engagement, and outcomes. Strength-oriented care attitudes (Model 1); mental health (Model 2); intention to leave current workplace (Model 3); and intention to resign from their profession as a nurse (Model 4).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Kato, Y.; Chiba, R.; Shimazu, A.; Hayashi, Y.; Sakamoto, T. Antecedents and Outcomes of Work Engagement among Psychiatric Nurses in Japan. Healthcare 2023, 11, 295. https://doi.org/10.3390/healthcare11030295
AMA Style
Kato Y, Chiba R, Shimazu A, Hayashi Y, Sakamoto T. Antecedents and Outcomes of Work Engagement among Psychiatric Nurses in Japan. Healthcare. 2023; 11(3):295. https://doi.org/10.3390/healthcare11030295
Chicago/Turabian StyleKato, Yuichi, Rie Chiba, Akihito Shimazu, Yuta Hayashi, and Takuya Sakamoto. 2023. "Antecedents and Outcomes of Work Engagement among Psychiatric Nurses in Japan" Healthcare 11, no. 3: 295. https://doi.org/10.3390/healthcare11030295
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.