
Psychological Health in Intensive Care Unit Health Care Workers after the COVID-19 Pandemic

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Psychometric Tools
2.3. Open-Ended Questions
- “In your opinion, what positive and negative aspects did the experience of providing health care to patients admitted to the COVID-19 intensive care unit during the first phase of the emergency leave you with?”
- “In your experience, are there differences between how you experienced the care of COVID patients during the first phase of the emergency and today? Since the reopening of the COVID wards after the summer, do you feel that you approach the work and the relationship with patients and colleagues in the same way or differently than in the first phase?”
2.4. Statistics
3. Results
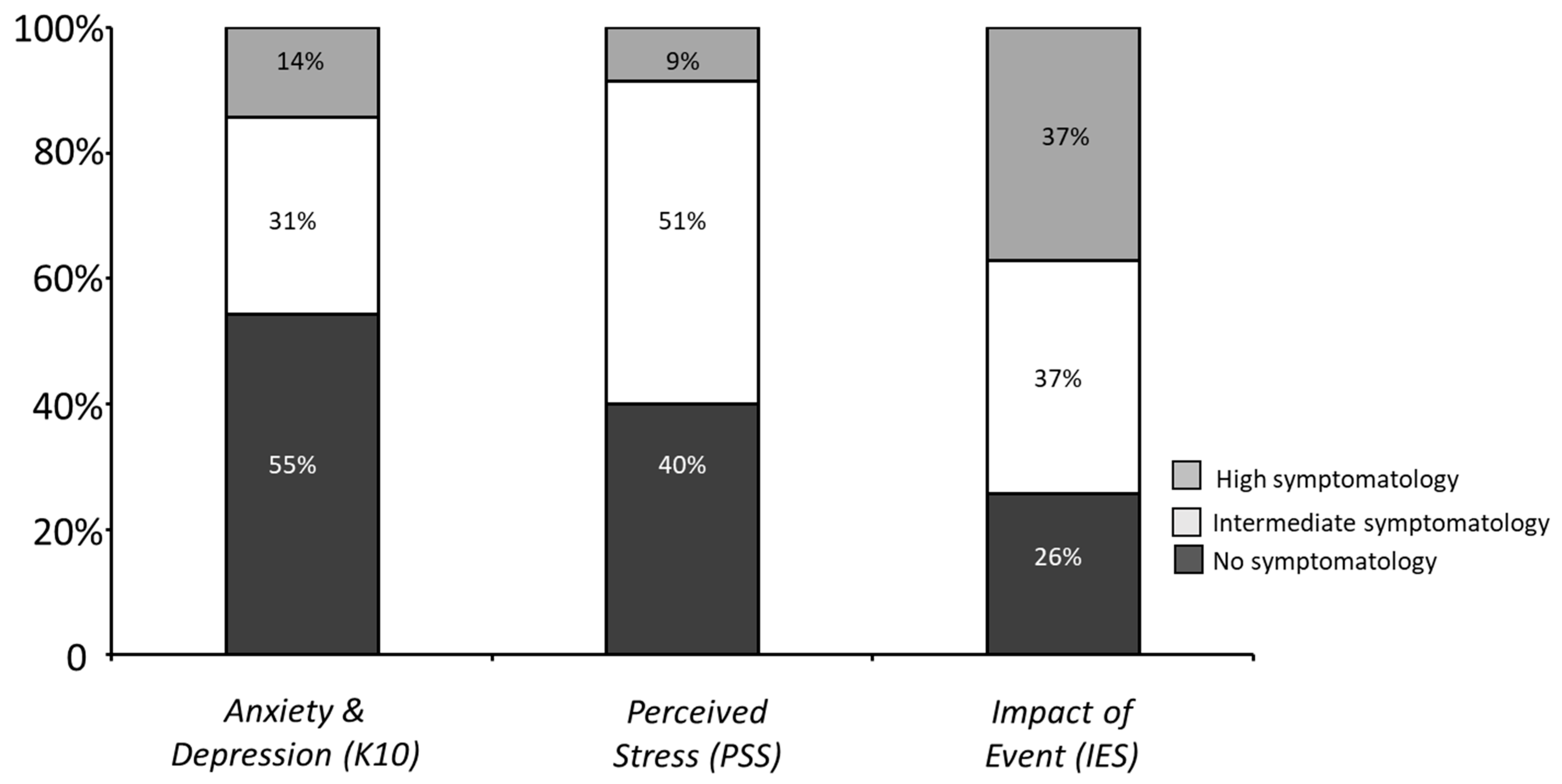
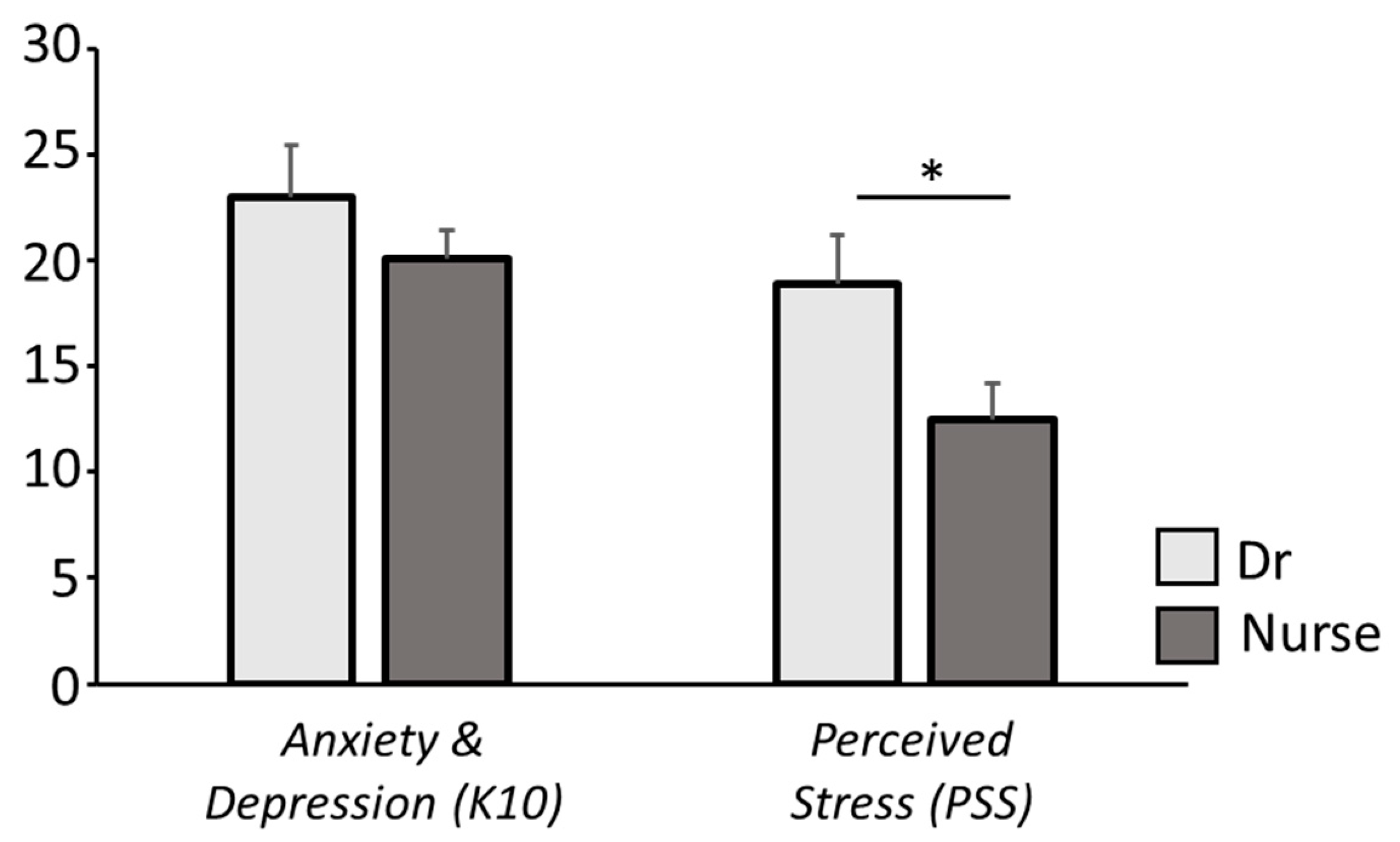
3.1. Evaluation of Anxious/Depressive Symptoms and Perceived Stress Levels
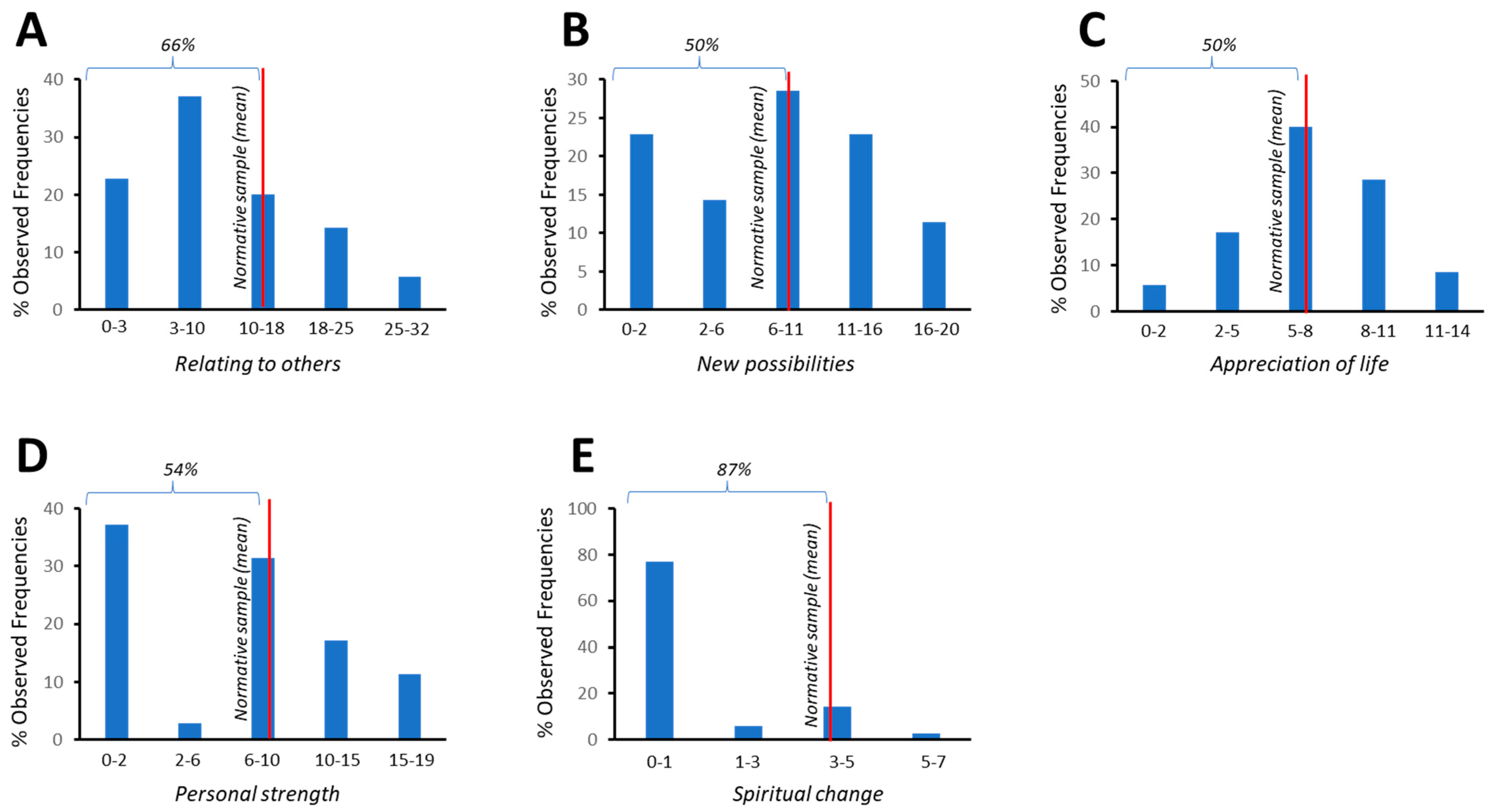
3.2. Presence of PTSD Symptoms and Long-Term Post-Traumatic Growth
3.3. Qualitative Analysis—Open-Ended Questions
- Quality of relationships in the workplace, understood as the level of cooperation and support perceived within the team.
- Sense of emotional-relational competence, considered as the perception of being able to relate to and understand the mental states of oneself, patients, and colleagues.
- Sense of clinical-technical competence, defined as the perception of sufficient technical preparation to deal with clinical emergencies in patients,
3.3.1. Quality of Relations in the Workplace:
3.3.2. Sense of Emotional-Relational Competence:
3.3.3. Sense of Clinical-Technical Competence:
4. Discussion
4.1. Limitations
4.2. Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviation
References
- Istituto Superiore di Sanità (ISS). Cosa Sono i Coronavirus. Available online: https://www.epicentro.iss.it/coronavirus/cosa-sono (accessed on 29 May 2022).
- Iodice, F.; Cassano, V.; Rossini, P.M. Direct and indirect neurological, cognitive, and behavioral effects of COVID-19 on the healthy elderly, mild-cognitive-impairment, and Alzheimer’s disease populations. Neurol. Sci. 2021, 42, 455–465. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Mazza, M.G.; De Lorenzo, R.; Conte, C.; Poletti, S.; Vai, B.; Bollettini, I.; Melloni, E.M.T.; Furlan, R.; Ciceri, F.; Rovere-Querini, P.; et al. Anxiety and depression in COVID-19 survivors: Role of inflammatory and clinical predictors. Brain Behav. Immun. 2020, 89, 594–600. [Google Scholar] [CrossRef]
- Kaseda, E.T.; Levine, A.J. Post-traumatic stress disorder: A differential diagnostic consideration for COVID-19 survivors. Clin. Neuropsychol. 2020, 34, 7–8. [Google Scholar] [CrossRef]
- World Health Organization (WHO). WHO Coronavirus (COVID-19) Dashboard Overview Data Table. 2021. Available online: https://covid19.who.int/ (accessed on 29 May 2022).
- Istituto Superiore di Sanità (ISS). Epidemia COVID-19. Aggiornamento Nazionale 28 Dicembre 2021–Ore 12:00. Available online: https://www.epicentro.iss.it/coronavirus/bollettino/Bollettino-sorveglianza-integrata-COVID-19_28-dicembre-2021.pdf (accessed on 29 May 2022).
- Serafini, G.; Parmigiani, B.; Amerio, A.; Aguglia, A.; Sher, L.; Amore, M. The psychological impact of COVID-19 on the mental health in the general population. QJM 2020, 113, 531–537. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; McIntyre, R.S.; Choo, F.N.; Tran, B.; Ho, R.; Sharma, V.K.; et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav. Immun. 2020, 87, 40–48. [Google Scholar] [CrossRef]
- Bonati, M.; Campi, R.; Segre, G. Psychological impact of the quarantine during the COVID-19 pandemic on the general European adult population: A systematic review of the evidence. Epidemiol. Psychiatr. Sci. 2022, 31, e27. [Google Scholar] [CrossRef]
- Talevi, D.; Socci, V.; Carai, M.; Carnaghi, G.; Faleri, S.; Trebbi, E.; di Bernardo, A.; Capelli, F.; Pacitti, F. Mental health outcomes of the COVID-19 pandemic. Riv. Psichiatr. 2020, 55, 137–144. [Google Scholar] [CrossRef]
- Preti, E.; Di Mattei, V.; Perego, G.; Ferrari, F.; Mazzetti, M.; Taranto, P.; Di Pierro, R.; Madeddu, F.; Calati, R. The Psychological Impact of Epidemic and Pandemic Outbreaks on Healthcare Workers: Rapid Review of the Evidence. Curr. Psychiatry Rep. 2020, 22, 43. [Google Scholar] [CrossRef]
- Zaka, A.; Shamloo, S.E.; Fiorente, P.; Tafuri, A. COVID-19 pandemic as a watershed moment: A call for systematic psychological health care for frontline medical staff. J. Health Psychol. 2020, 25, 883–887. [Google Scholar] [CrossRef]
- Gillen, P.; Neill, R.D.; Manthorpe, J.; Mallett, J.; Schroder, H.; Nicholl, P.; Currie, D.; Moriarty, J.; Ravalier, J.; McGrory, S.; et al. Decreasing Wellbeing and Increasing Use of Negative Coping Strategies: The Effect of the COVID-19 Pandemic on the UK Health and Social Care Workforce. Epidemiologia 2022, 3, 26–39. [Google Scholar] [CrossRef]
- Veronese, G.; Mahamid, F.A.; Bdier, D. Subjective well-being, sense of coherence, and posttraumatic growth mediate the association between COVID-19 stress, trauma, and burnout among Palestinian health-care providers. Am. J. Orthopsychiatry 2022, 92, 291–301. [Google Scholar] [CrossRef]
- Proserpio, P.; Zambrelli, E.; Lanza, A.; Dominese, A.; Di Giacomo, R.; Quintas, R.; Tramacere, I.; Rubino, A.; Turner, K.; Colosio, C.; et al. Sleep disorders and mental health in hospital workers during the COVID-19 pandemic: A cross-sectional multicenter study in Northern Italy. Neurol. Sci. 2022, 43, 2241–2251. [Google Scholar] [CrossRef]
- Danet Danet, A. Psychological impact of COVID-19 pandemic in Western frontline healthcare professionals. A systematic review. Med. Clin. 2021, 156, 449–458. [Google Scholar] [CrossRef]
- Giusti, E.M.; Pedroli, E.; D’Aniello, G.E.; Stramba Badiale, C.; Pietrabissa, G.; Manna, C.; Stramba Badiale, M.; Riva, G.; Castelnuovo, G.; Molinari, E. The Psychological Impact of the COVID-19 Outbreak on Health Professionals: A Cross-Sectional Study. Front. Psychol. 2020, 11, 1684. [Google Scholar] [CrossRef]
- Rossi, R.; Socci, V.; Jannini, T.B.; Pacitti, F.; Siracusano, A.; Rossi, A.; Di Lorenzo, G. Mental Health Outcomes among Italian Health Care Workers during the COVID-19 Pandemic. JAMA Netw. Open 2021, 4, e2136143. [Google Scholar] [CrossRef]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Zhang, W.R.; Wang, K.; Yin, L.; Zhao, W.F.; Xue, Q.; Peng, M.; Min, B.Q.; Tian, Q.; Leng, H.X.; Du, J.L.; et al. Mental health and psychosocial problems of medical health workers during the COVID-19 epidemic in China. Psychother. Psychosom. 2020, 89, 242–250. [Google Scholar] [CrossRef]
- Zeng, N.; Zhao, Y.M.; Yan, W.; Li, C.; Lu, Q.D.; Liu, L.; Ni, S.Y.; Mei, H.; Yuan, K.; Shi, L.; et al. A systematic review and meta-analysis of long term physical and mental sequelae of COVID-19 pandemic: Call for research priority and action. Mol. Psychiatry 2022, 1, 11. [Google Scholar] [CrossRef]
- Kalaitzaki, A.; Tamiolaki, A.; Tsouvelas, G. From secondary traumatic stress to vicarious posttraumatic growth amid COVID-19 lockdown in Greece: The role of health care workers’ coping strategies. Psychol. Trauma 2022, 14, 273–280. [Google Scholar] [CrossRef]
- Hong, S.; Kim, H.; Park, M.K. Impact of COVID-19 on post-traumatic stress symptoms in the general population: An integrative review. Int. J. Ment. Health Nurs. 2021, 30, 834–846. [Google Scholar] [CrossRef]
- Vagni, M.; Maiorano, T.; Giostra, V.; Pajardi, D. Coping with COVID-19: Emergency Stress, Secondary Trauma and Self-Efficacy in Healthcare and Emergency Workers in Italy. Front. Psychol. 2020, 11, 566912. [Google Scholar] [CrossRef]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef]
- Liu, X.; Zhu, M.; Zhang, R.; Zhang, J.; Zhang, C.; Liu, P.; Feng, Z.; Chen, Z. Public mental health problems during COVID-19 pandemic: A large-scale meta-analysis of the evidence. Transl. Psychiatry 2021, 11, 384. [Google Scholar] [CrossRef]
- Yunitri, N.; Chu, H.; Kang, X.L.; Jen, H.J.; Pien, L.C.; Tsai, H.T.; Kamil, A.R.; Chou, K.R. Global prevalence and associated risk factors of posttraumatic stress disorder during COVID-19 pandemic: A meta-analysis. Int. J. Nurs. Stud. 2022, 126, 104136. [Google Scholar] [CrossRef]
- Şanlıtürk, D. Perceived and sources of occupational stress in intensive care nurses during the COVID-19 pandemic. Intensive Crit. Care Nurs. 2021, 67, 103107. [Google Scholar] [CrossRef]
- Kashtanov, A.; Molotok, E.; Yavorovskiy, A.; Boyarkov, A.; Vasil’ev, Y.; Alsaegh, A.; Dydykin, S.; Kytko, O.; Meylanova, R.; Enina, Y.; et al. A Comparative Cross-Sectional Study Assessing the Psycho-Emotional State of Intensive Care Units’ Physicians and Nurses of COVID-19 Hospitals of a Russian Metropolis. Int. J. Environ. Res. Public Health 2022, 19, 1828. [Google Scholar] [CrossRef]
- Yamane, D.; Zarabian, K.; Devine, K.; Benjenk, I.; Farrar, K.; Park, O.L.; Kim, J.; Davison, D.; Heinz, E. Hospital-Based Healthcare Worker Perceptions of Personal Risk Related to COVID-19: One Year Follow-Up. J. Am. Board Fam. Med. 2022, 35, 284–294. [Google Scholar] [CrossRef]
- Azoulay, E.; Pochard, F.; Reignier, J.; Argaud, L.; Bruneel, F.; Courbon, P.; Cariou, A.; Klouche, K.; Labbé, V.; Barbier, F.; et al. Symptoms of Mental Health Disorders in Critical Care Physicians Facing the Second COVID-19 Wave: A Cross-Sectional Study. Chest 2021, 160, 944–955. [Google Scholar] [CrossRef]
- Pan, L.; Xu, Q.; Kuang, X.; Zhang, X.; Fang, F.; Gui, L.; Li, M.; Tefsen, B.; Zha, L.; Liu, H. Prevalence and factors associated with post-traumatic stress disorder in healthcare workers exposed to COVID-19 in Wuhan, China: A cross-sectional survey. BMC Psychiatry 2021, 21, 572. [Google Scholar] [CrossRef]
- Tedeschi, R.G.; Calhoun, L.G. Posttraumatic growth: Conceptual foundations and empirical evidence. Psychol. Inq. 2004, 15, 1–18. [Google Scholar] [CrossRef]
- Feingold, J.H.; Hurtado, A.; Feder, A.; Peccoralo, L.; Southwick, S.M.; Ripp, J.; Pietrzak, R.H. Posttraumatic growth among health care workers on the frontlines of the COVID-19 pandemic. J. Affect Disord. 2022, 296, 35–40. [Google Scholar] [CrossRef]
- Kalaitzaki, A.; Rovithis, M. Secondary traumatic stress and vicarious posttraumatic growth in healthcare workers during the first COVID-19 lockdown in Greece: The role of resilience and coping strategies. Psychiatriki 2021, 32, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Barker, P.R.; Colpe, L.J.; Epstein, J.F.; Gfroerer, J.C.; Hiripi, E.; Howes, M.J.; Normand, S.-L.T.; Manderscheid, R.W.; Walters, E.E.; et al. Screening for serious mental illness in the general population. Arch. Gen. Psychiatry 2003, 60, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Carrà, G.; Sciarini, P.; Segagni-Lusignani, G.; Clerici, M.; Montomoli, C.; Kessler, R.C. Do they actually work across borders? Evaluation of two measures of psychological distress as screening instruments in a non Ango-Saxon country. Eur. Psychiatry 2010, 26, 122–127. [Google Scholar] [CrossRef]
- Yan, S.; Yang, J.; Ye, M.; Chen, S.; Xie, C.; Huang, J.; Liu, H. Post-traumatic Growth and Related Influencing Factors in Discharged COVID-19 Patients: A Cross-Sectional Study. Front. Psychol. 2021, 12, 658307. [Google Scholar] [CrossRef]
- Cohen, S.; Williamson, G. Perceived stress in a probability sample of the United States. In The Social Psychology of Health; Spacapan, S., Oskamp, S., Eds.; Sage Publications, Inc.: Thousand Oaks, CA, USA, 1988; pp. 31–67. ISBN1 080393162X. ISBN2 9780803931626. [Google Scholar]
- Tedeschi, R.G.; Calhoun, L.G. The posttraumatic growth inventory: Measuring the positive legacy of trauma. J. Trauma Stress 1996, 9, 455–471. [Google Scholar] [CrossRef]
- Prati, G.; Pietrantoni, L. Italian Adaptation and Confirmatory Factor Analysis of the Full and the Short Form of the Posttraumatic Growth Inventory. J. Loss Trauma 2014, 19, 12–22. [Google Scholar] [CrossRef]
- Weiss, D.S. The impact of Event Scale: Revised. In Cross-Cultural Assessment of Psychological Trauma and PTSD; International and Cultural Psychology Series; Springer: Boston, MA, USA, 2007; pp. 219–238. ISBN 978-0-387-70990-1. [Google Scholar]
- Giannantonio, M. Psicotraumatologia e Psicologia Dell’Emergenza; Ecomind: Salerno, Italy, 2003; ISBN 8887795169. [Google Scholar]
- Da Silva, B.; Santos Vitti, L.; Faro, A. Kessler Psychological Distress Scale: Internal Structure and Relation to Other Variables. Psico-USF 2021, 26, 91–101. [Google Scholar] [CrossRef]
- Greenberg, N.; Weston, D.; Hall, C.; Caulfield, T.; Williamson, V.; Fong, K. Mental health of staff working in intensive care during COVID-19. Occup. Med. 2021, 71, 62–67. [Google Scholar] [CrossRef]
- Ezzat, A.; Li, Y.; Holt, J.; Komorowski, M. The global mental health burden of COVID-19 on critical care staff. Br. J. Nurs. 2021, 30, 634–642. [Google Scholar] [CrossRef] [PubMed]
- Phiri, P.; Ramakrishnan, R.; Rathod, S.; Elliot, K.; Thayanandan, T.; Sandle, N.; Haque, N.; Chau, S.W.; Wong, O.W.; Chan, S.S.; et al. An evaluation of the mental health impact of SARS-CoV-2 on patients, general public and healthcare professionals: A systematic review and meta-analysis. EClinicalMedicine 2021, 34, 100806. [Google Scholar] [CrossRef] [PubMed]
- Rossi, R.; Socci, V.; Pacitti, F.; Di Lorenzo, G.; Di Marco, A.; Siracusano, A.; Rossi, A. Mental Health Outcomes Among Frontline and Second-Line Health Care Workers During the Coronavirus Disease 2019 (COVID-19) Pandemic in Italy. JAMA Netw. Open 2020, 3, e2010185. [Google Scholar] [CrossRef] [PubMed]
- Elbay, R.Y.; Kurtulmuş, A.; Arpacıoğlu, S.; Karadere, E. Depression, anxiety, stress levels of physicians and associated factors in COVID-19 pandemics. Psychiatry Res. 2020, 290, 113130. [Google Scholar] [CrossRef] [PubMed]
- Cipolotti, L.; Chan, E.; Murphy, P.; van Harskamp, N.; Foley, J.A. Factors contributing to the distress, concerns, and needs of UK Neuroscience health care workers during the COVID-19 pandemic. Psychol. Psychother. 2021, 94 (Suppl. S2), 536–543. [Google Scholar] [CrossRef] [PubMed]
- Laurent, A.; Fournier, A.; Lheureux, F.; Louis, G.; Nseir, S.; Jacq, G.; Goulenok, C.; Muller, G.; Badie, J.; Bouhemad, B.; et al. Mental health and stress among ICU healthcare professionals in France according to intensity of the COVID-19 epidemic. Ann. Intensive Care 2021, 11, 90. [Google Scholar] [CrossRef]
- Lasalvia, A.; Bonetto, C.; Porru, S.; Carta, A.; Tardivo, S.; Bovo, C.; Ruggeri, M.; Amaddeo, F. Psychological impact of COVID-19 pandemic on healthcare workers in a highly burdened area of north-east Italy. Epidemiol. Psychiatr. Sci. 2020, 30, E1. [Google Scholar] [CrossRef]
- Shechter, A.; Diaz, F.; Moise, N.; Anstey, D.E.; Ye, S.; Agarwal, S.; Birk, J.L.; Brodie, D.; Cannone, D.E.; Chang, B.; et al. Psychological distress, coping behaviors, and preferences for support among New York healthcare workers during the COVID-19 pandemic. Gen. Hosp. Psychiatry 2020, 66, 1–8. [Google Scholar] [CrossRef]
- Sünnetçi Silistre, E.; Hatipoğlu, H.U.; Yeşilbaş, O.; Gürbüz, F.Ş.; Ozturk, E.; Yalcinkaya, A. Investigating the psychological impact of COVID-19 on healthcare workers in the intensive care unit. JOSAM 2022, 6, 29–35. [Google Scholar] [CrossRef]
- Chahley, E.R.; Reel, R.M.; Taylor, S. The lived experience of healthcare professionals working frontline during the 2003 SARS epidemic, 2009 H1N1 pandemic, 2012 MERS outbreak, and 2014 EVD epidemic: A qualitative systematic review. SSM Qual. Res. Health 2021, 1, 100026. [Google Scholar] [CrossRef]
- Guo, W.P.; Min, Q.; Gu, W.W.; Yu, L.; Xiao, X.; Yi, W.B.; Li, H.L.; Huang, B.; Li, J.L.; Dai, Y.J.; et al. Prevalence of mental health problems in frontline healthcare workers after the first outbreak of COVID-19 in China: A cross-sectional study. Health Qual. Life Outcomes 2021, 19, 103. [Google Scholar] [CrossRef] [PubMed]
- Carmassi, C.; Foghi, C.; Dell’Oste, V.; Cordone, A.; Bertelloni, C.A.; Bui, E.; Dell’Osso, L. PTSD symptoms in healthcare workers facing the three coronavirus outbreaks: What can we expect after the COVID-19 pandemic. Psychiatry Res. 2020, 292, 113312. [Google Scholar] [CrossRef] [PubMed]
- Carmassi, C.; Malacarne, P.; Dell’oste, V.; Bertelloni, C.A.; Cordone, A.; Foghi, C.; Dell’osso, L. Post-traumatic stress disorder, burnout and their impact on global functioning in Italian emergency healthcare workers. Minerva Anestesiol. 2021, 87, 556–566. [Google Scholar] [CrossRef] [PubMed]
- Caillet, A.; Coste, C.; Sanchez, R.; Allaouchiche, B. Psychological Impact of COVID-19 on ICU Caregivers. Anaesth. Crit. Care Pain Med. 2020, 39, 717–722. [Google Scholar] [CrossRef]
- Laurent, A.; Fournier, A.; Lheureux, F.; Poujol, A.L.; Deltour, V.; Ecarnot, F.; Meunier-Beillard, N.; Loiseau, M.; Binquet, C.; Quenot, J.P. Risk and protective factors for the possible development of post-traumatic stress disorder among intensive care professionals in France during the first peak of the COVID-19 epidemic. Eur. J. Psychotraumatol. 2022, 13, 2011603. [Google Scholar] [CrossRef]
- Altmayer, V.; Weiss, N.; Cao, A.; Marois, C.; Demeret, S.; Rohaut, B.; Le Guennec, L.; Réa-Neuro-Pitié-Salpêtriere study group. Coronavirus disease 2019 crisis in Paris: A differential psychological impact between regular intensive care unit staff members and reinforcement workers. Aust. Crit. Care 2021, 34, 142–145. [Google Scholar] [CrossRef]
- Dobson, H.; Malpas, C.B.; Burrell, A.J.; Gurvich, C.; Chen, L.; Kulkarni, J.; Winton-Brown, T. Burnout and psychological distress amongst Australian healthcare workers during the COVID-19 pandemic. Australas. Psychiatry 2021, 29, 26–30. [Google Scholar] [CrossRef]
- Crowe, S.; Howard, A.F.; Vanderspank-Wright, B.; Gillis, P.; McLeod, F.; Penner, C.; Haljan, G. The effect of COVID-19 pandemic on the mental health of Canadian critical care nurses providing patient care during the early phase pandemic: A mixed method study. Intensive Crit. Care Nurs. 2021, 63, 102999. [Google Scholar] [CrossRef]
- Leng, M.; Wei, L.; Shi, X.; Cao, G.; Wei, Y.; Xu, H.; Zhang, X.; Zhang, W.; Xing, S.; Wei, H. Mental distress and influencing factors in nurses caring for patients with COVID-19. Nurs. Crit. Care 2021, 26, 94–101. [Google Scholar] [CrossRef]
- Jung, H.; Jung, S.Y.; Lee, M.H.; Kim, M.S. Assessing the Presence of Post-Traumatic Stress and Turnover Intention Among Nurses Post-Middle East Respiratory Syndrome Outbreak: The Importance of Supervisor Support. Workplace Health Saf. 2020, 68, 337–345. [Google Scholar] [CrossRef] [Green Version]
- Chen, W.C.; Teckie, S.; Somerstein, G.; Adair, N.; Potters, L. Guidelines to Reduce Hospitalization Rates for Patients Receiving Curative-Intent Radiation Therapy During the COVID-19 Pandemic: Report from a Multicenter New York Area Institution. Adv. Radiat. Oncol. 2020, 5, 621–627. [Google Scholar] [CrossRef] [PubMed]
- Mancini, A.D. Heterogeneous mental health consequences of COVID-19: Costs and benefits. Psychol. Trauma 2020, 12, S15–S16. [Google Scholar] [CrossRef] [PubMed]
- Huecker, M.; Shreffler, J.; Danzl, D. COVID-19: Optimizing healthcare provider wellness and posttraumatic growth. Am. J. Emerg. Med. 2021, 46, 693–694. [Google Scholar] [CrossRef] [PubMed]
- Shakespeare-Finch, J.; Bowen-Salter, H.; Cashin, M.; Badawi, A.; Wells, R.; Rosenbaum, S.; Steel, Z. COVID-19: An Australian Perspective. J. Loss Trauma 2020, 25, 662–672. [Google Scholar] [CrossRef]
- Aggar, C.; Samios, C.; Penman, O.; Whiteing, N.; Massey, D.; Rafferty, R.; Bowen, K.; Stephens, A. The impact of COVID-19 pandemic-related stress experienced by Australian nurses. Int. J. Ment. Health Nurs. 2022, 31, 91–103. [Google Scholar] [CrossRef]
- Zhang, X.T.; Shi, S.S.; Qin Ren, Y.; Wang, L. The Traumatic Experience of Clinical Nurses During the COVID-19 Pandemic: Which Factors are Related to Post-Traumatic Growth? Risk Manag. Healthc. Policy 2021, 14, 2145–2151. [Google Scholar] [CrossRef]
- Kapur, A.; Rudin, B.; Potters, L. Posttraumatic Growth in Radiation Medicine During the COVID-19 Outbreak. Adv. Radiat. Oncol. 2022, 7, 100975. [Google Scholar] [CrossRef]
- Kalaitzaki, A.E.; Tamiolaki, A.; Rovithis, M. The healthcare professionals amidst COVID-19 pandemic: A perspective of resilience and posttraumatic growth. Asian J. Psychiatr. 2020, 52, 102172. [Google Scholar] [CrossRef]
- Gibbons, S.; Murphy, D.; Joseph, S. Countertransference and positive growth in social workers. J. Soc. Work Pract. 2011, 25, 17–30. [Google Scholar] [CrossRef]
- Kjellenberg, E.; Nilsson, F.; Daukantaite, D.; Cardena, E. Transformative narratives: The impact of working with war and torture survivors. Psychol. Trauma 2014, 6, 120–128. [Google Scholar] [CrossRef]
- Shakespeare-Finch, J.; Lurie-Beck, J. A meta-analytic clarification of the relationship between posttraumatic growth and symptoms of posttraumatic distress disorder. J. Anxiety Disord. 2014, 28, 223–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manning-Jones, S.; de Terte, I.; Stephens, C. The Relationship Between Vicarious Posttraumatic Growth and Secondary Traumatic Stress Among Health Professionals. J. Loss Trauma 2017, 22, 256–270. [Google Scholar] [CrossRef]
- Boerner, M.; Joseph, S.; Murphy, D. Is the association between posttraumatic stress and posttraumatic growth moderated by defense styles? Traumatology 2020. [Google Scholar] [CrossRef]
- Park, Y.S.; Park, K.H.; Lee, J. Validation of the Korean Version of Impact of Event Scale-Revised (IES-R) in Korean Nurses during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 28, 11311. [Google Scholar] [CrossRef] [PubMed]
- Palmborg, Å.; Lötvall, R.; Cardeña, E. Acute Stress among Nurses in Sweden during the COVID-19 Pandemic. J. Trauma Dissociation 2022, 6, 100283. [Google Scholar] [CrossRef]
- Carola, V.; Vincenzo, C.; Morale, C.; Pelli, M.; Rocco, M.; Nicolais, G. Psychological health in COVID-19 patients after discharge from an intensive care unit. Front. Public Health 2022, 10, 951136. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Measure | M | SD |
|---|---|---|
| PTGI—Relating to others | 10.60 | 8.50 |
| PTGI—New possibilities | 8.46 | 5.85 |
| PTGI—Personal Strength | 7.11 | 5.74 |
| PTGI—Spiritual Change | 1.03 | 1.89 |
| PTGI—Appreciation of Life | 7.31 | 3.48 |
| IES—Avoidance | 1.25 | 0.85 |
| IES—Intrusiveness | 1.53 | 0.85 |
| IES—Iperarousal | 1.19 | 0.88 |
| K10 | PSS | IES | PTGI | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AV | IN | IP | TS | RO | NP | PS | SC | AL | ||||
| K10 | 1.00 | |||||||||||
| PSS | 0.76 | 1.00 | ||||||||||
| IES | Avoidance (AV) | 0.47 | 0.23 | 1.00 | ||||||||
| Intrusiveness (IN) | 0.55 | 0.33 | 0.75 | 1.00 | ||||||||
| Iperarousal (IP) | 0.73 | 0.57 | 0.65 | 0.75 | 1.00 | |||||||
| Total Score (TS) | 0.63 | 0.38 | 0.89 | 0.93 | 0.87 | 1.00 | ||||||
| PTGI | Relating to others (RO) | 0.14 | −0.18 | 0.12 | 0.22 | 0.01 | 0.15 | 1.00 | ||||
| New possibilities (NP) | 0.18 | 0.04 | 0.43 | 0.51 | 0.40 | 0.51 | 0.78 | 1.00 | ||||
| Personal Strength (PS) | 0.12 | 0.03 | 0.31 | 0.47 | 0.27 | 0.40 | 0.82 | 0.87 | 1.00 | |||
| Spiritual Change (SC) | 0.30 | −0.06 | 0.25 | 0.27 | 0.22 | 0.29 | 0.33 | 0.42 | 0.31 | 1.00 | ||
| Appreciation of Life (AL) | 0.18 | 0.06 | 0.31 | 0.51 | 0.37 | 0.45 | 0.61 | 0.75 | 0.70 | 0.42 | 1.00 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carola, V.; Vincenzo, C.; Morale, C.; Cecchi, V.; Rocco, M.; Nicolais, G. Psychological Health in Intensive Care Unit Health Care Workers after the COVID-19 Pandemic. Healthcare 2022, 10, 2201. https://doi.org/10.3390/healthcare10112201
Carola V, Vincenzo C, Morale C, Cecchi V, Rocco M, Nicolais G. Psychological Health in Intensive Care Unit Health Care Workers after the COVID-19 Pandemic. Healthcare. 2022; 10(11):2201. https://doi.org/10.3390/healthcare10112201
Chicago/Turabian StyleCarola, Valeria, Cristina Vincenzo, Chiara Morale, Valentina Cecchi, Monica Rocco, and Giampaolo Nicolais. 2022. "Psychological Health in Intensive Care Unit Health Care Workers after the COVID-19 Pandemic" Healthcare 10, no. 11: 2201. https://doi.org/10.3390/healthcare10112201