
The Reproducibility and Usefulness of Estimated Average Glucose for Hyperglycemia Management during Health Checkups: A Retrospective Cross-Sectional Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Laboratory Measurements
2.3. Statistical Analyses
3. Results
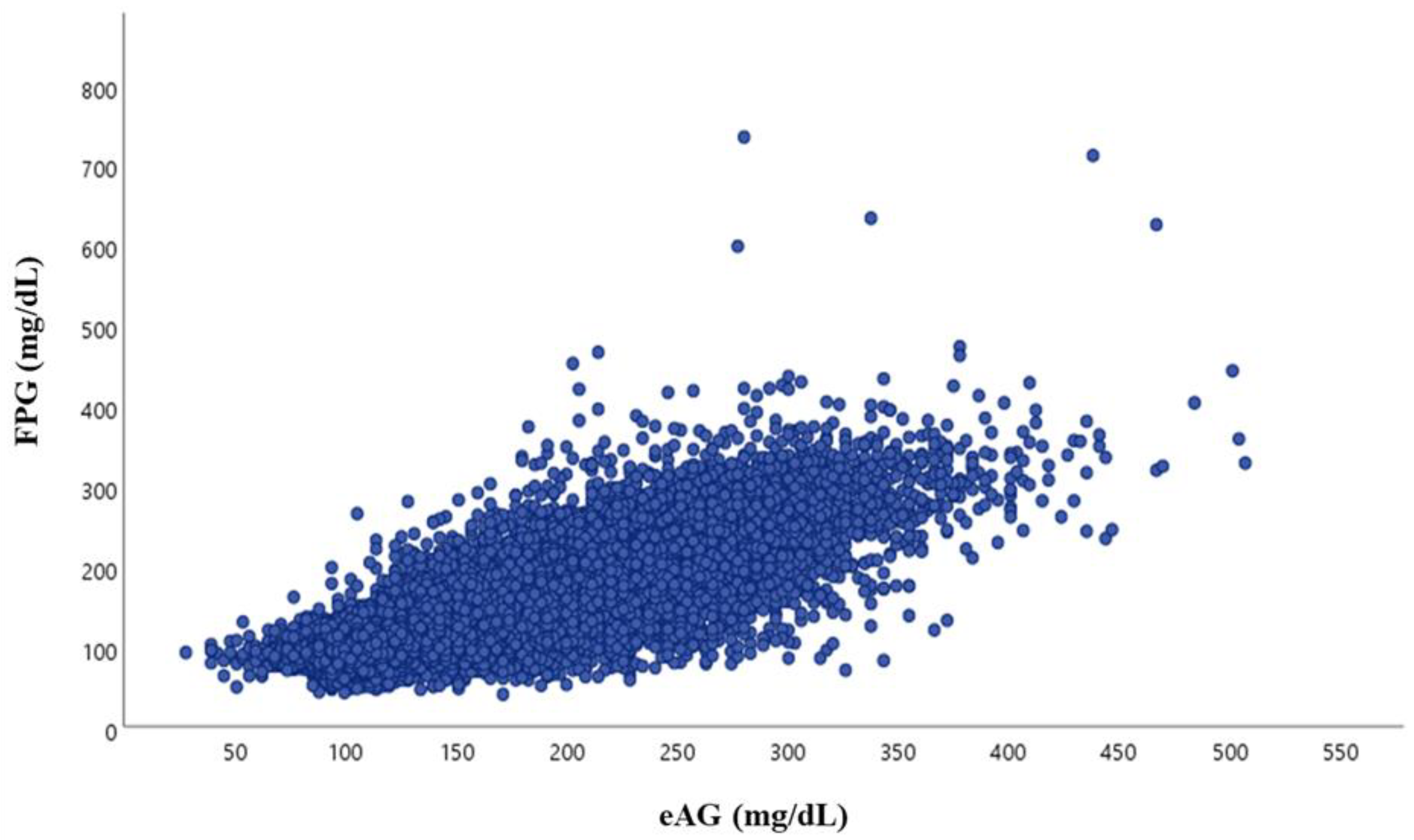
3.1. Characteristics of Study Subjects and the Correlation between FPG and eAG According to FPG Group
3.2. Mean Glucose Levels for Specified HbA1c Levels
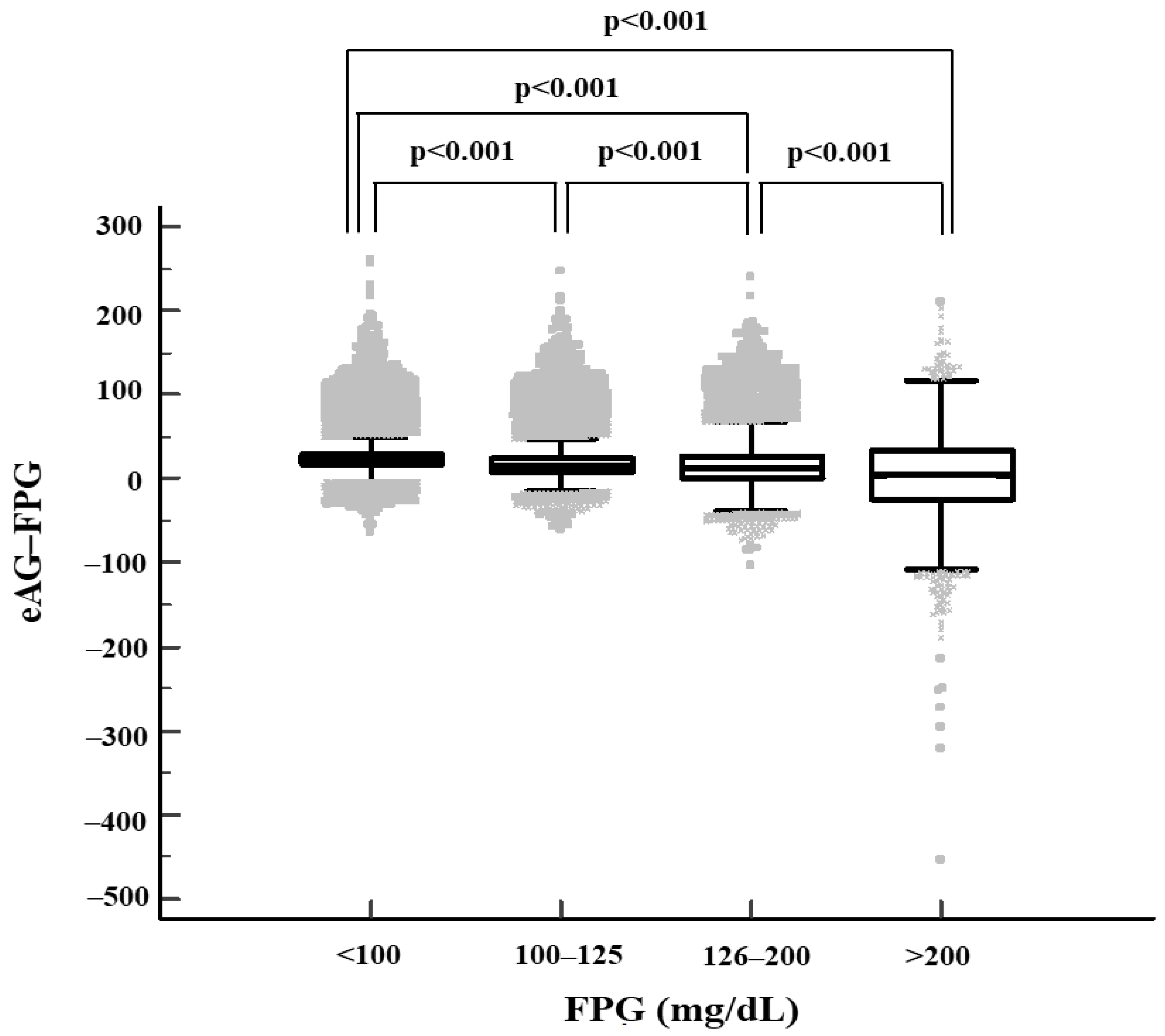
3.3. Difference between eAG and FPG Values
3.4. Factors Associated with eAG
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Diabetes Control and Complications Trial Research Group; Nathan, D.M.; Genuth, S.; Lachin, J.; Cleary, P.; Crofford, O.; Davis, M.; Rand, L.; Siebert, C. The Effect of Intensive Treatment of Diabetes on the Development and Progression of Long-Term Complications in Insulin-Dependent Diabetes Mellitus. N. Engl. J. Med. 1993, 329, 977–986. [Google Scholar] [CrossRef]
- Inzucchi, S.E.; Bergenstal, R.M.; Buse, J.B.; Diamant, M.; Ferrannini, E.; Nauck, M.; Peters, A.L.; Tsapas, A.; Wender, R.; Matthews, D.R.; et al. Management of hyperglycemia in type 2 diabetes: A patient-centered approach: Position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2012, 35, 1364–1379. [Google Scholar] [CrossRef] [Green Version]
- Consensus Committee. Consensus statement on the worldwide standardization of the hemoglobin A1c measurement: The American Diabetes Association, European Association for the Study of Diabetes, International Federation of Clinical Chemistry and Laboratory Medicine, and the International Diabetes Federation. Diabetes Care 2007, 30, 2399–2400. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 2010, 33, S62–S69. [Google Scholar] [CrossRef] [Green Version]
- Laiteerapong, N.; Ham, S.A.; Gao, Y.; Moffet, H.H.; Liu, J.Y.; Huang, E.S.; Karter, A.J. The Legacy Effect in Type 2 Diabetes: Impact of Early Glycemic Control on Future Complications (The Diabetes & Aging Study). Diabetes Care 2019, 42, 416–426. [Google Scholar] [CrossRef] [Green Version]
- Stratton, I.M.; Adler, A.I.; Neil, H.A.; Matthews, D.R.; Manley, S.E.; Cull, C.A.; Hadden, D.; Turner, R.C.; Holman, R.R. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): Prospective observational study. BMJ 2000, 321, 405–412. [Google Scholar] [CrossRef] [Green Version]
- Little, R.R.; Rohlfing, C.L.; Sacks, D.B.; National Glycohemoglobin Standardization Program (NGSP) Steering Committee. Status of Hemoglobin A1c Measurement and Goals for Improvement: From Chaos to Order for Improving Diabetes Care. Clin. Chem. 2011, 57, 205–214. [Google Scholar] [CrossRef]
- Nathan, D.M.; Kuenen, J.; Borg, R.; Zheng, H.; Schoenfeld, D.; Heine, R.J.; for the A1c-Derived Average Glucose (ADAG) Study Group. Translating the A1C Assay Into Estimated Average Glucose Values. Diabetes Care 2008, 31, 1473–1478. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. 5. Glycemic Targets. Diabetes Care 2016, 39, S39–S46. [Google Scholar] [CrossRef] [Green Version]
- DeVries, J.H. Glucose Variability: Where It Is Important and How to Measure It. Diabetes 2013, 62, 1405–1408. [Google Scholar] [CrossRef] [Green Version]
- Lu, J.; Ma, X.; Zhou, J.; Zhang, L.; Mo, Y.; Ying, L.; Lu, W.; Zhu, W.; Bao, Y.; Vigersky, R.A.; et al. Association of Time in Range, as Assessed by Continuous Glucose Monitoring, With Diabetic Retinopathy in Type 2 Diabetes. Diabetes Care 2018, 41, 2370–2376. [Google Scholar] [CrossRef] [Green Version]
- Picconi, F.; Parravano, M.; Ylli, D.; Pasqualetti, P.; Coluzzi, S.; Giordani, I.; Malandrucco, I.; Lauro, D.; Scarinci, F.; Giorno, P.; et al. Retinal neurodegeneration in patients with type 1 diabetes mellitus: The role of glycemic variability. Acta Diabetol. 2017, 54, 489–497. [Google Scholar] [CrossRef]
- Zinman, B.; Marso, S.P.; Poulter, N.R.; Emerson, S.S.; Pieber, T.R.; Pratley, R.E.; Lange, M.; Brown-Frandsen, K.; Moses, A.; Ocampo Francisco, A.M.; et al. Day-to-day fasting glycaemic variability in DEVOTE: Associations with severe hypoglycaemia and cardiovascular outcomes (DEVOTE 2). Diabetologia 2018, 61, 48–57. [Google Scholar] [CrossRef] [Green Version]
- Frontoni, S.; Di Bartolo, P.; Avogaro, A.; Bosi, E.; Paolisso, G.; Ceriello, A. Glucose variability: An emerging target for the treatment of diabetes mellitus. Diabetes Res. Clin. Pract. 2013, 102, 86–95. [Google Scholar] [CrossRef]
- Suh, S.; Kim, J.H. Glycemic Variability: How Do We Measure It and Why Is It Important? Diabetes Metab. J. 2015, 39, 273–282. [Google Scholar] [CrossRef]
- Bozkaya, G.; Ozgu, E.; Karaca, B. The association between estimated average glucose levels and fasting plasma glucose levels. Clinics 2010, 65, 1077–1080. [Google Scholar] [CrossRef] [Green Version]
- Mahato, R.V.; Nepal, A.K.; Gelal, B.; Poudel, B.; Kumar Yadav, B.; Rajendra, K.C.; Gyawali, P.; Regmi, P.; Atreya, P. Association of estimated average glucose with fasting, post-prandial and average of fasting and pp serum glucose levels. JNAMLS 2012, 11, 14–18. [Google Scholar]
- Kim, H.-Y.; Lee, S.-Y.; Suh, S.; Kim, J.H.; Lee, M.K.; Park, H.-D. The relationship between estimated average glucose and fasting plasma glucose. Clin. Chem. Lab. Med. 2013, 51, 2195–2200. [Google Scholar] [CrossRef]
- Jia, K.-K.; Zhang, J. Evaluation of five routine glucose methods on an Olympus AU5400 analyzer using the CDC hexokinase reference method. Clin. Chem. Lab. Med. 2010, 48, 361–364. [Google Scholar] [CrossRef]
- Juvenile Diabetes Research Foundation Continuous Glucose Monitoring Study Group Hemoglobin A1c and Mean Glucose in Patients With Type 1 Diabetes: Analysis of data from the Juvenile Diabetes Research Foundation continuous glucose monitoring randomized trial. Diabetes Care 2011, 34, 540–544. [CrossRef] [Green Version]
- American Diabetes Association. 6. Glycemic Targets: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021, 44, S73–S84. [Google Scholar] [CrossRef]
- Rybicka, M.; Krysiak, R.; Okopień, B. The dawn phenomenon and the Somogyi effect—Two phenomena of morning hyper-glycaemia. Endokrynol. Pol. 2011, 62, 276–284. [Google Scholar]
- Li, C.; Ma, X.; Yin, J.; Mo, Y.; Zhang, L.; Lu, J.; Lu, W.; Bao, Y.; Vigersky, R.A.; Zhou, J.; et al. The dawn phenomenon across the glycemic continuum: Implications for defining dysglycemia. Diabetes Res. Clin. Pract. 2020, 166, 108308. [Google Scholar] [CrossRef]
- Monnier, L.; Colette, C.; Dejager, S.; Owens, D. The dawn phenomenon in type 2 diabetes: How to assess it in clinical practice? Diabetes Metab. 2015, 41, 132–137. [Google Scholar] [CrossRef] [Green Version]
- Hempe, J.M.; Soros, A.A.; Chalew, S.A. Estimated Average Glucose and Self-Monitored Mean Blood Glucose Are Discordant Estimates of Glycemic Control. Diabetes Care 2010, 33, 1449–1451. [Google Scholar] [CrossRef] [Green Version]
- Munshi, M.N.; Segal, A.R.; Slyne, C.; Samur, A.A.; Brooks, K.M.; Horton, E.S. Shortfalls of the use of HbA1C-derived eAG in older adults with diabetes. Diabetes Res. Clin. Pract. 2015, 110, 60–65. [Google Scholar] [CrossRef] [Green Version]
- Wei, N.; Zheng, H.; Nathan, D.M. Empirically Establishing Blood Glucose Targets to Achieve HbA1c Goals. Diabetes Care 2014, 37, 1048–1051. [Google Scholar] [CrossRef] [Green Version]
- Chao, G.; Zhu, Y.; Chen, L. Role and Risk Factors of Glycosylated Hemoglobin Levels in Early Disease Screening. J. Diabetes Res. 2021, 2021, 6626587. [Google Scholar] [CrossRef]
- Peng, X.; Ge, J.; Wang, C.; Sun, H.; Ma, Q.; Xu, Y.; Ma, Y. Longitudinal Average Glucose Levels and Variance and Risk of Stroke: A Chinese Cohort Study. Int. J. Hypertens. 2020, 2020, 895305. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| All | FPG | p Value | Post-Hoc | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| <100 mg/dL a | 100–125 mg/dL b | 126–200 mg/dL c | >200 mg/dL d | |||||||||
| Total | ||||||||||||
| Subj., N | 328,035 | 182,848 | 109,555 | 31,875 | 3757 | |||||||
| Age, year | 52± | 13 | 49± | 13 | 56± | 12 | 58± | 11 | 53± | 12 | <0.001 | a < d < b < c |
| Hb, g/dL | 14.3± | 1.5 | 14.1± | 1.6 | 14.5± | 1.5 | 14.7± | 1.5 | 15.3± | 1.6 | <0.001 | a < b < c < d |
| FPG, mg/dL | 104± | 25 | 90± | 6 | 109± | 7 | 145± | 18 | 250± | 44 | <0.001 | a < b < c < d |
| HbA1c, % | 5.9± | 0.9 | 5.6± | 0.4 | 6.0± | 0.6 | 7.2± | 1 | 10.5± | 1.8 | <0.001 | a < b < c < d |
| eAG, mg/dL | 123.81± | 25.74 | 113.49± | 10.91 | 125.72± | 15.95 | 161.07± | 30.03 | 254.60± | 52.97 | <0.001 | a < b < c < d |
| Corr.coeff.(r) | 0.811 | 0.21 | 0.413 | 0.573 | 0.524 | |||||||
| eAG–FPG | 20.24± | 15.57 | 23.31± | 11.44 | 16.97± | 14.53 | 15.78± | 24.62 | 4.14± | 47.96 | <0.001 | d < c < b < a |
| Male | ||||||||||||
| Subj., N | 172,095 | 83,791 | 64,422 | 21,272 | 2610 | |||||||
| Age, year | 52± | 13 | 48± | 13 | 54± | 12 | 57± | 10 | 52± | 11 | <0.001 | a < d < b < c |
| Hb, g/dL | 15.3± | 1.2 | 15.3± | 1.1 | 15.3± | 1.2 | 15.3± | 1.3 | 15.8± | 1.3 | <0.001 | a,b,c < d |
| FPG, mg/dL | 107± | 27 | 91± | 6 | 109± | 7 | 146± | 18 | 250± | 45 | <0.001 | a < b < c < d |
| HbA1c, % | 6.0± | 1 | 5.6± | 0.4 | 6.0± | 0.6 | 7.2± | 1 | 10.4± | 1.8 | <0.001 | a < b < c < d |
| eAG, mg/dL | 125.68± | 27.76 | 113.65± | 10.97 | 124.78± | 15.99 | 160.24± | 29.99 | 252.52± | 53.09 | <0.001 | a < b < c < d |
| eAG–FPG | 18.80± | 16.6 | 22.75± | 11.8 | 15.75± | 14.57 | 14.43± | 24.7 | 2.73± | 48.56 | <0.001 | d < c < b < a |
| Corr.coeff.(r) | 0.817 | 0.142 | 0.413 | 0.568 | 0.52 | |||||||
| Female | ||||||||||||
| Subj., N | 155,940 | 99,057 | 45,133 | 10,603 | 1147 | |||||||
| Age, year | 53± | 13 | 49± | 13 | 58± | 11 | 60± | 10 | 54± | 12 | <0.001 | a < d < b < c |
| Hb, g/dL | 13.2± | 1.1 | 13.1± | 1.1 | 13.4± | 1.1 | 13.5± | 1.2 | 14.0± | 1.4 | <0.001 | a < b < c < d |
| FPG, mg/dL | 100± | 22 | 90± | 7 | 108± | 7 | 144± | 17 | 252± | 42 | <0.001 | a < b < c < d |
| HbA1c, % | 5.9± | 0.8 | 5.6± | 0.4 | 6.1± | 0.6 | 7.3± | 1 | 10.7± | 1.8 | <0.001 | a < b < c < d |
| eAG, mg/dL | 121.75± | 23.13 | 113.35± | 10.85 | 127.05± | 15.8 | 162.73± | 30.04 | 259.34± | 52.43 | <0.001 | a < b < c < d |
| Corr.coeff.(r) | 0.801 | 0.264 | 0.425 | 0.591 | 0.535 | |||||||
| eAG–FPG | 21.84± | 14.17 | 23.78± | 11.1 | 18.72± | 14.3 | 18.48± | 24.24 | 7.35± | 46.43 | <0.001 | d < b,c < a |
| HbA1C | Estimated Mean Glucose Concentration | Estimated Mean FPG | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ADAG Study * | Present Study | Reanalyzed ADAG Data ** | Present Study | |||||||||||||||||||
| (%) | mg/dL | mmol/L | mg/dL | mmol/L | mg/dL | mmol/L | mg/dL | mmol/L | ||||||||||||||
| ≤5.6 | 107.4± | 6.2 | 5.9± | 0.3 | 92.6± | 9.4 | 5.1± | 0.5 | ||||||||||||||
| 6.0 | 126 | (100–152) | 7.0 | (5.5–8.5) | ||||||||||||||||||
| 5.7–<6.5 | 124.1± | 6.0 | 6.9± | 0.3 | 122 | (117–127) | 6.8 | (6.5–7.0) | 101.4± | 12.7 | 5.6± | 0.7 | ||||||||||
| 6.5–<7.0 | 144.7± | 4.0 | 8.0± | 0.2 | 142 | (135–150) | 7.9 | (7.5–8.3) | 120.8± | 17.3 | 6.7± | 1.0 | ||||||||||
| 7.0 | 154 | (123–185) | 8.6 | (6.8–10.3) | ||||||||||||||||||
| 7.0–<7.5 | 159.2± | 4.0 | 8.8± | 0.2 | 152 | (143–162) | 8.4 | (7.9–9.0) | 132.8± | 21.2 | 7.4± | 1.2 | ||||||||||
| 7.5–<8.0 | 173.6± | 4.0 | 9.6± | 0.2 | 167 | (157–177) | 9.3 | (8.7–9.8) | 143.8± | 26.1 | 8.0± | 1.4 | ||||||||||
| 8.0 | 183 | (147–217) | 10.2 | (8.1–12.1) | ||||||||||||||||||
| 8.0–8.5 | 189.3± | 4.9 | 10.5± | 0.3 | 178 | (164–192) | 9.9 | (9.1–10.7) | 156.1± | 32.7 | 8.7± | 1.8 | ||||||||||
| 9.0 | 212 | (170–249) | 11.8 | (9.4–13.9) | ||||||||||||||||||
| 10.0 | 240 | (193–282) | 13.4 | (10.7–15.7) | ||||||||||||||||||
| 11.0 | 269 | (217–314) | 14.9 | (12.0–17.5) | ||||||||||||||||||
| 12.0 | 298 | (240–347) | 16.5 | (13.3–19.3) | ||||||||||||||||||
| FPG | p Value | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| <100 mg/dL | 100–125 mg/dL | 126–200 mg/dL | >200 mg/dL | |||||||
| eAG–FPG * | Negative, N (%) | 2681 | (1.5) | 10,582 | (9.7) | 8234 | (25.8) | 1740 | (46.3) | <0.001 |
| Positive, N (%) | 180,167 | (98.5) | 98,973 | (90.3) | 23,641 | (74.2) | 2017 | (53.7) | ||
| Coefficient | (SE) | Standard Coefficient | p Value | |
|---|---|---|---|---|
| Age | 0.256 | (0.036) | 0.119 | <0.001 |
| Sex (ref. male) | 4.168 | (1.401) | 0.078 | 0.003 |
| WC | −0.017 | (0.048) | −0.006 | 0.727 |
| Hb | 0.003 | (0.352) | 0.000 | 0.993 |
| FPG | 0.906 | (0.018) | 0.817 | <0.001 |
| Creatinine | 1.292 | (3.228) | 0.011 | 0.689 |
| HDL-C | −0.072 | (0.033) | −0.036 | 0.031 |
| LDL-C | 0.015 | (0.011) | 0.020 | 0.170 |
| TG | −0.010 | (0.003) | −0.046 | 0.003 |
| e-GFR | 0.055 | (0.044) | 0.030 | 0.213 |
| HOMA-IR | 0.173 | (0.224) | 0.012 | 0.440 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nah, E.-H.; Cho, S.; Park, H.; Noh, D.; Kwon, E.; Cho, H.-I. The Reproducibility and Usefulness of Estimated Average Glucose for Hyperglycemia Management during Health Checkups: A Retrospective Cross-Sectional Study. Healthcare 2022, 10, 824. https://doi.org/10.3390/healthcare10050824
Nah E-H, Cho S, Park H, Noh D, Kwon E, Cho H-I. The Reproducibility and Usefulness of Estimated Average Glucose for Hyperglycemia Management during Health Checkups: A Retrospective Cross-Sectional Study. Healthcare. 2022; 10(5):824. https://doi.org/10.3390/healthcare10050824
Chicago/Turabian StyleNah, Eun-Hee, Seon Cho, Hyeran Park, Dongwon Noh, Eunjoo Kwon, and Han-Ik Cho. 2022. "The Reproducibility and Usefulness of Estimated Average Glucose for Hyperglycemia Management during Health Checkups: A Retrospective Cross-Sectional Study" Healthcare 10, no. 5: 824. https://doi.org/10.3390/healthcare10050824