
Sexual Quality of Life-Female (SQoL-F): Cultural Adaptation and Validation of European Portuguese Version

 ,
,  ,
,  ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
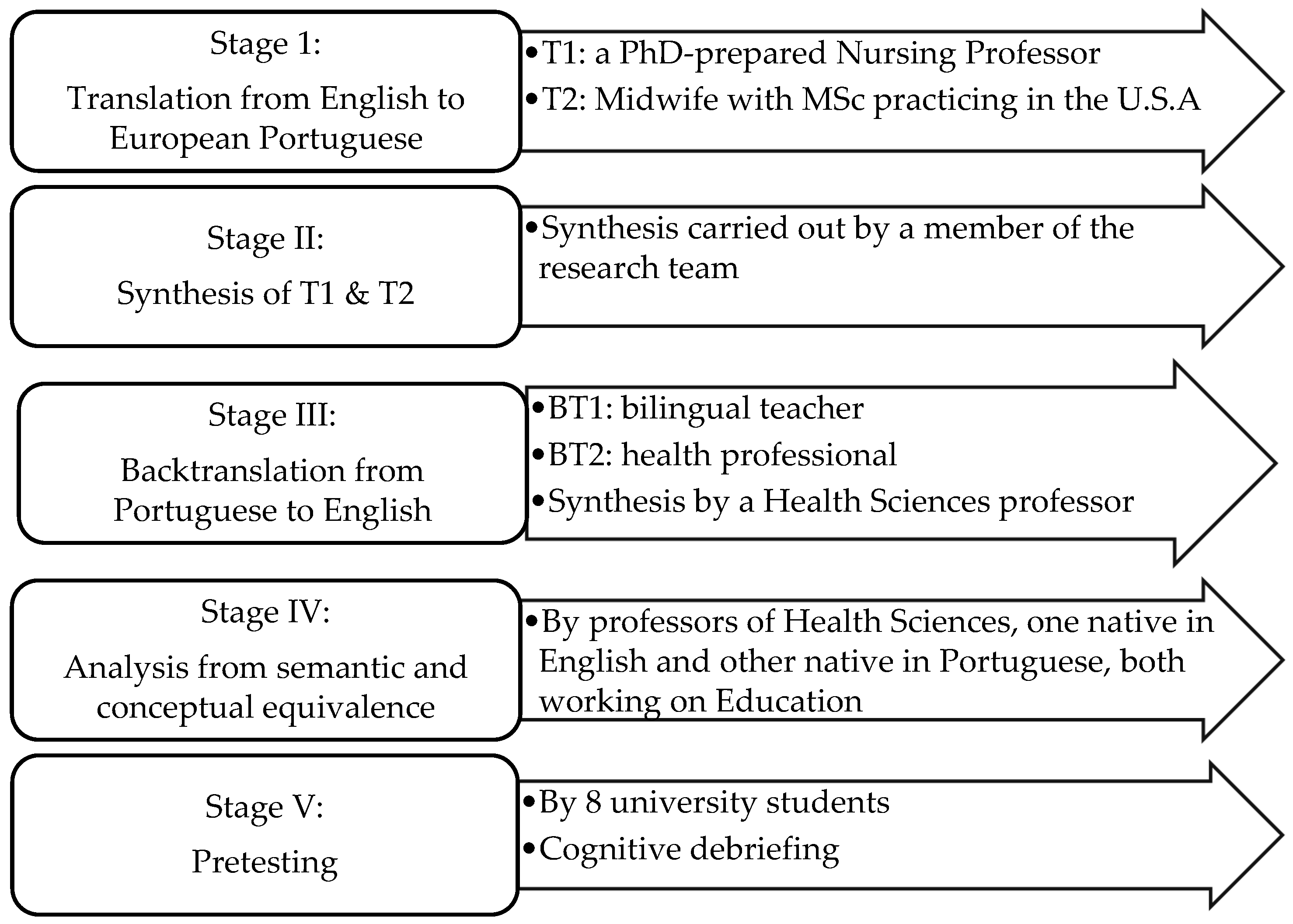
2.2. Translation, Cultural Perspective of Semantics and Validation
2.3. Participants and Setting
2.4. Data Collection Procedure
2.5. Data Analysis
2.5.1. Reliability
2.5.2. Validity
2.6. Ethical Procedures
3. Results
3.1. Characteristics of Participants
3.2. Reliability
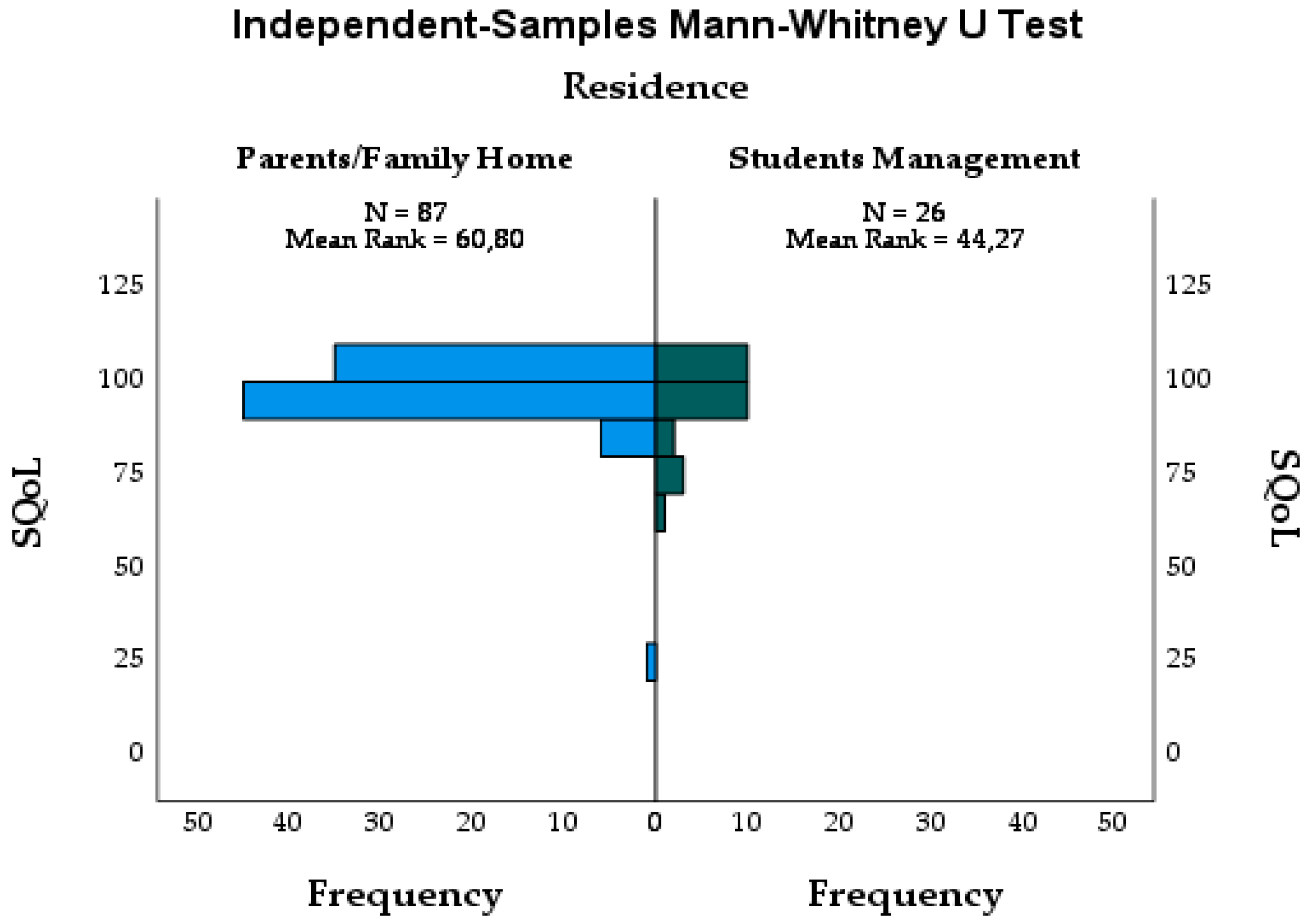
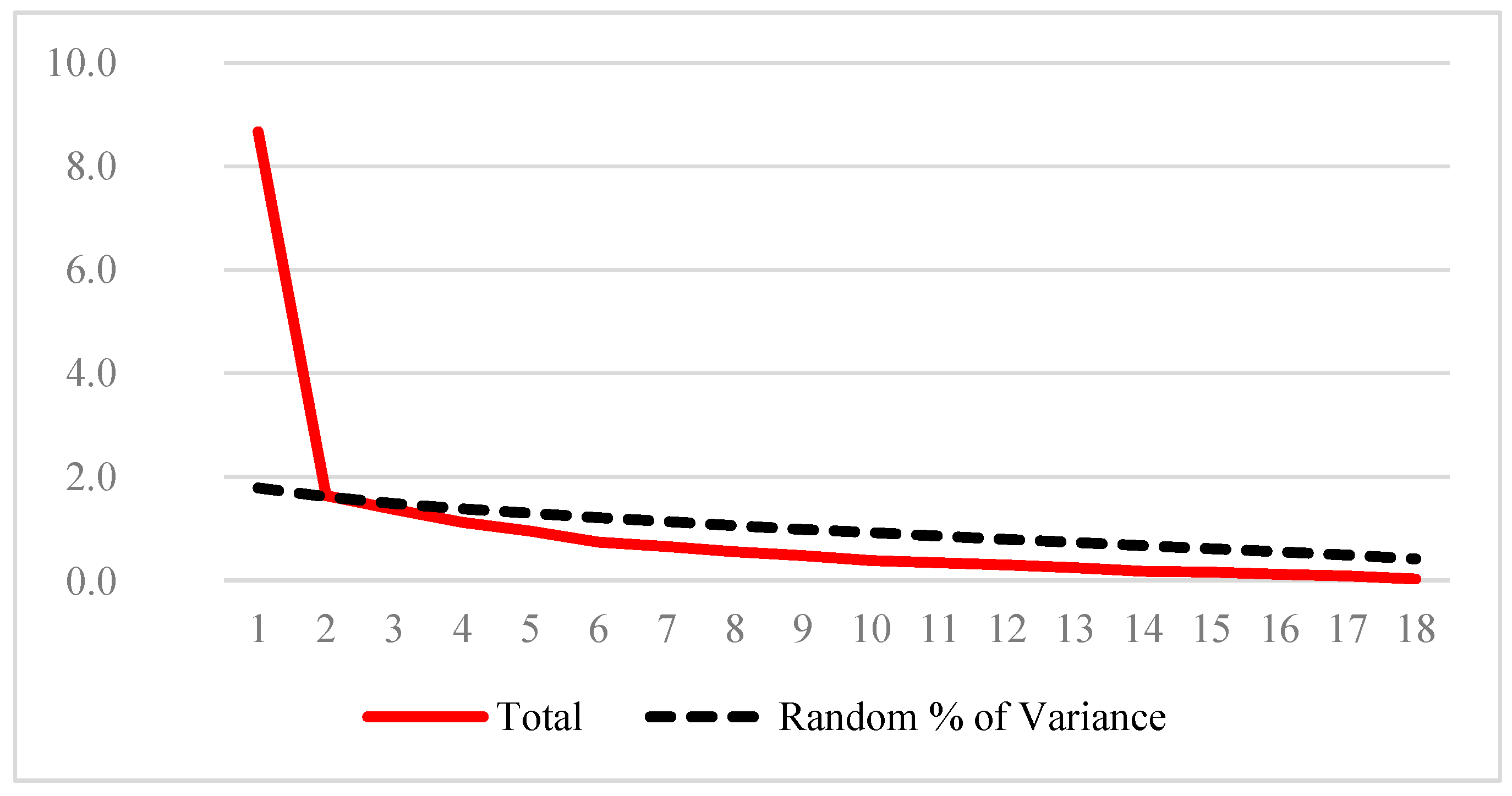
3.3. Construct Validity
4. Discussion
4.1. Reliability
4.2. Validity
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Rao, T.S.S.; Nagaraj, A.K.M. Female sexuality. Indian J. Psychiatry 2015, 57 (Suppl. S2), S296. [Google Scholar] [PubMed]
- Kingsberg, S.A.; Schaffir, J.; Faught, B.M.; Pinkerton, J.V.; Parish, S.J.; Iglesia, C.B.; Gudeman, J.; Krop, J.; Simon, J.A. Female sexual health: Barriers to optimal outcomes and a roadmap for improved patient–clinician communications. J. Women’s Health 2019, 28, 432–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Symonds, T.; Boolell, M.; Quirk, F. Development of a questionnaire on sexual quality of life in women. J. Sex Marital. Ther. 2005, 31, 385–397. [Google Scholar] [CrossRef] [PubMed]
- Cantarino, S.G.; Pinto, J.M.d.M.; Fabião, J.A.d.S.A.d.O.; García, A.M.C.; Abellán, M.V.; Rodrigues, M.A. The importance of religiosity/spirituality in the sexuality of pregnant and postpartum women. PLoS ONE 2016, 11, e0156809. [Google Scholar] [CrossRef] [Green Version]
- Mollaioli, D.; Ciocca, G.; Limoncin, E.; Di Sante, S.; Gravina, G.L.; Carosa, E.; Lenzi, A.; Jannini, E.A.F. Lifestyles and sexuality in men and women: The gender perspective in sexual medicine. Reprod. Biol. Endocrinol. 2020, 18, 10. [Google Scholar] [CrossRef]
- Milhausen, R.R.; Sakaluk, J.K.; Fisher, T.D.; Davis, C.M.; Yarber, W.L. Handbook of Sexuality-Related Measures; Routledge: London, UK, 2019. [Google Scholar]
- Lawrance, K.-a.; Byers, E.S. Development of the interpersonal exchange model of sexual satisfaction in long term relationships. Can. J. Hum. Sex. 1992, 1, 123–128. [Google Scholar]
- Pengpid, S.; Peltzer, K. Associations of physical partner violence and sexual violence victimization on health risk behaviours and mental health among university students from 25 countries. BMC Public Health 2020, 20, 937. [Google Scholar] [CrossRef]
- McClelland, S.I. Measuring sexual quality of life: Ten recommendations for health psychologists. In Handbook of Health Psychology; Psychology Press: New York, NY, USA, 2012. [Google Scholar]
- Flynn, K.E.; Lin, L.; Cyranowski, J.M.; Reeve, B.B.; Reese, J.B.; Jeffery, D.D.; Smith, A.W.; Porter, L.S.; Dombeck, C.B.; Bruner, D.W. Development of the NIH PROMIS® Sexual Function and Satisfaction measures in patients with cancer. J. Sex. Med. 2013, 10, 43–52. [Google Scholar] [CrossRef] [Green Version]
- Merghati-Khoei, E.; Emami-Razavi, S.H.; Bakhtiyari, M.; Hajmirzaei, S.; Haghighi, S.T.-t.; Korte, J.E.; Maasoumi, R. Spinal cord injury and women’s sexual life: Case–control study. Spinal Cord 2017, 55, 269–273. [Google Scholar] [CrossRef]
- Cybulski, M.; Cybulski, L.; Krajewska-Kulak, E.; Orzechowska, M.; Cwalina, U.; Jasinski, M. Sexual quality of life, sexual knowledge, and attitudes of older adults on the example of inhabitants over 60s of Bialystok, Poland. Front. Psychol. 2018, 9, 483. [Google Scholar] [CrossRef] [Green Version]
- Dias, E.N.; Pais-Ribeiro, J.L. O modelo de coping de Folkman e Lazarus: Aspectos históricos e conceituais. Rev. Psicol. E Saúde 2019, 11, 55–66. [Google Scholar] [CrossRef]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almeida, L.; Freire, T. Metodología de Investigação em Psicología e Educação; Edições Psiquilibrios: Coimbra, Portugal, 2017. [Google Scholar]
- Todendi, P.F.; Valim, A.R.; Reuter, C.P.; Mello, E.D.; Gaya, A.R.; Burgos, M.S. Metabolic risk in schoolchildren is associated with low levels of cardiorespiratory fitness, obesity, and parents’ nutritional profile. J. Pediatr. 2016, 92, 388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Damásio, B.F. Uso da análise fatorial exploratória em psicologia. Aval. Psicol. Interam. J. Psychol. Assess. 2012, 11, 213–228. [Google Scholar]
- Field, A. Discovering Statistics Using SPSS; Sage Publications: Sussex, UK, 2009. [Google Scholar]
- Moreira, J.M. Questionários: Teoria e Prática. Coimbra: Almedina. Moskos, C. (1977). From Institution to Occupation: Trends in Military Organizations. Armed Forces Soc. 2004, 4, 41–50. [Google Scholar]
- Polit, D.F.; Beck, C.T. Essential of Nursing Research: Appraising Evidence for Nursing Practice (4. Uppl); Lippincott Williams & Wilkins: New York, NY, USA, 2020. [Google Scholar]
- Souza, A.C.; Alexandre, N.M.C.; Guirardello, E.d.B. Propriedades psicométricas na avaliação de instrumentos: Avaliação da confiabilidade e da validade. Epidemiol. E Serviços De Saúde 2017, 26, 649–659. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Maasoumi, R.; Mokarami, H.; Nazifi, M.; Stallones, L.; Taban, A.; Yazdani Aval, M.; Samimi, K. Psychometric properties of the Persian translation of the sexual quality of life–male questionnaire. Am. J. Men’s Health 2017, 11, 564–572. [Google Scholar] [CrossRef]
- Draugalis, J.R.; Coons, S.J.; Plaza, C.M. Best practices for survey research reports: A synopsis for authors and reviewers. Am. J. Pharm. Educ. 2008, 72, 11. [Google Scholar] [CrossRef]
- Machado, M.H. Perfil da enfermagem no Brasil: Relatório final; FIOCRUZ/COFEN: Rio de Janeiro, Brasil, 2017; p. 750. [Google Scholar]
- Moreno, A.B.; Faerstein, E.; Werneck, G.L.; Lopes, C.S.; Chor, D. Propriedades psicométricas do instrumento abreviado de avaliação de qualidade de vida da Organização Mundial da Saúde no estudo pró-saúde. Cad. De Saúde Pública 2006, 22, 2585–2597. [Google Scholar] [CrossRef] [Green Version]
- Hays, R.D.; Weech-Maldonado, R.; Teresi, J.A.; Wallace, S.P.; Stewart, A.L. Commentary: Copyright restrictions versus open access to survey instruments. Med. Care 2018, 56, 107. [Google Scholar] [CrossRef] [PubMed]
- Frey, B.B. The SAGE Encyclopedia of Educational Research, Measurement, and Evaluation; Sage Publications: London, UK, 2018. [Google Scholar]
- de Carvalho, C.P.; do Rosário, M.; Pinheiro, M.; Gouveia, J.A.; Vilar, D.G.R. Questionário de atitudes e crenças sobre sexualidade e educação sexual (QACSES) para adolescentes: Estudos de validação psicométrica. Rev. De Psicol. Da Criança E Do Adolesc. 2016, 7, 345–363. [Google Scholar]
- Curtis, T.J.; Field, N.; Clifton, S.; Mercer, C.H. Household structure and its association with sexual risk behaviours and sexual health outcomes: Evidence from a British probability sample survey. BMJ Open 2018, 8, e024255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- González-Pascual, J.L.; Esteban-Gonzalo, L.; Rodríguez-García, M.; Gómez-Cantarino, S.; Moreno-Preciado, M. The Effect of Stereotypes and Prejudices Regarding Gender Roles on the Relation between Nurses and "Muslim Fathers" in Health Institutions within the Community of Madrid (Spain). Nurs. Inq. 2017, 24, e12194. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.A.; Mullinax, M.; Trussell, J.; Davidson Sr, J.K.; Moore, N.B. Sexual satisfaction and sexual health among university students in the United States. Am. J. Public Health 2011, 101, 1643–1654. [Google Scholar] [CrossRef] [PubMed]
- Mehta, S.D.; Nordgren, R.K.; Agingu, W.; Otieno, F.; Odongo, W.; Odhiambo, F.; Bailey, R.C. Sexual quality of life and association with HIV and sexually transmitted infections among a cohort of heterosexual couples in Kenya. J. Sex. Med. 2018, 15, 1446–1455. [Google Scholar] [CrossRef] [Green Version]
- Yáñez-Araque, B.; Gómez-Cantarino, S.; Gutiérrez-Broncano, S.; López-Ruiz, V.R. Examining the Determinants of Healthcare Workers’ Performance: A Configurational Analysis during COVID-19 Times. Int. J. Environ. Res. Public Health 2021, 18, 5671. [Google Scholar] [CrossRef]
- Cattell, R.B. The scree test for the number of factors. Multivar. Behav. Res. 1966, 1, 245–276. [Google Scholar] [CrossRef]
- DeVellis, R.F. Chapter Guidelines in scale development. Scale Dev. Theory Appl. 2017, 26, 145. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Participants n (%) | Chi-Squared | |
|---|---|---|---|
| Age | ≤20 years | 44 (38.9) | = 3.204; p = 0.202 |
| 21–22 years | 40 (35.4) | ||
| >23 years | 29 (25.7) | ||
| Year of Study | 1st year | 34 (30.1) | = 2.009; p = 0.571 |
| 2nd year | 29 (25.7) | ||
| 3rd year | 24 (21.2) | ||
| 4th year | 26 (23.0) | ||
| Residence | Parents house | 52 (46.0) | = 58.106; p < 0.001 |
| University housing | 8 (7.1) | ||
| Rented room | 27 (23.9) | ||
| Rented house with roommates | 9 (8.0) | ||
| Other | 17 (15.0) | ||
| Total | 113 (100) | - | |
| Item | Mean | Std. Deviation | Corrected Item-Total Correlation | Cronbach’s Alpha If Item Deleted |
|---|---|---|---|---|
| * SQoL-F1 | 5.62 | 0.672 | 0.716 | 0.831 |
| SQoL-F2 | 5.72 | 0.785 | 0.748 | 0.828 |
| SQoL-F3 | 5.83 | 0.625 | 0.878 | 0.827 |
| SQoL-F4 | 5.82 | 0.697 | 0.838 | 0.826 |
| * SQoL-F5 | 5.49 | 0.888 | 0.672 | 0.829 |
| SQoL-F6 | 5.78 | 0.765 | 0.684 | 0.831 |
| SQoL-F7 | 5.39 | 1.097 | 0.534 | 0.834 |
| SQoL-F8 | 5.89 | 0.541 | 0.835 | 0.831 |
| * SQoL-F9 | 5.34 | 0.786 | 0.658 | 0.831 |
| SQoL-10 | 2.68 | 1.670 | −0.154 | 0.887 |
| SQoL-F11 | 5.84 | 0.591 | 0.617 | 0.836 |
| SQoL-F12 | 5.51 | 0.974 | 0.493 | 0.836 |
| * SQoL-F13 | 5.62 | 0.899 | 0.747 | 0.826 |
| SQoL-F14 | 5.63 | 1.028 | 0.416 | 0.840 |
| SQoL-F15 | 5.73 | 0.845 | 0.628 | 0.831 |
| * SQoL-F16 | 3.46 | 1.866 | −0.059 | 0.888 |
| SQoL-F17 | 5.81 | 0.774 | 0.646 | 0.832 |
| * SQoL-F18 | 4.94 | 1.325 | 0.434 | 0.841 |
| Item | English Description and Portuguese Description |
|---|---|
| * SQoL-F1 | 1. When I think about my sex life I feel, I think that generally it is a pleasant part of my life * 1. Quando penso na minha vida sexual, acho que em geral, é uma parte agradável da minha vida * |
| SQoL-F2 | 2. When I think about my sex life I feel frustrated 2. Quando penso na minha vida sexual, sinto-me frustrada |
| SQoL-F3 | 3. When I think about my sex life I feel depressed 3. Quando penso na minha vida sexual, sinto-me deprimida |
| SQoL-F4 | 4. When I think about my sex life I feel less of a woman 4. Quando penso na minha vida sexual, sinto-me menos mulher. |
| * SQoL-F5 | 5. When I think about my sex life I feel good with myself * 5. Quando penso na minha vida sexual, sinto bem comigo mesma * |
| SQoL-F6 | 6. I lost confidence in myself as a sexual partner 6. Perdi a confiança em mim como parceira sexual. |
| SQoL-F7 | 7. When I think about my sex life I feel anxious 7. Quando penso sobre a minha vida sexual, sinto-me ansiosa. |
| SQoL-F8 | 8. When I think about my sex life I feel rage 8. Quando penso sobre a minha vida sexual, sinto raiva |
| * SQoL-F9 | 9. When I think about my sex life I feel closer to my partner * 9. Quando penso na minha vida sexual, sinto-me mais próxima do meu parceiro * |
| SQoL-10 | 10. I worry about the future of my sex life 10. Preocupo-me com o futuro da minha vida sexual |
| SQoL-F11 | 11. I lost pleasure in sexual intercourse 11. Perdi o prazer na atividade sexual |
| SQoL-F12 | 12. When I think about my sex life I feel embarrassed 12. Quando penso na minha vida sexual, fico embaraçada |
| * SQoL-F13 | 13. When I think about my sex life I feel I can speak to my partner about sexual matters * 13. Quando penso acerca da minha vida sexual, sinto que posso falar com o meu parceiro sobre questões de índole sexual * |
| SQoL-F14 | 14. I try to avoid sexual intercourse 14. Eu tento evitar ter atividade sexual |
| SQoL-F15 | 15. When I think about my sex life I feel guilty 15. Quando penso acerca da minha vida sexual, sinto-me culpada |
| * SQoL-F16 | 16. When I think about my sex life I am scared that my partner will feel hurt or rejected * 16. Quando eu penso na minha vida sexual, preocupo-me se o meu parceiro se sente magoado ou rejeitado * |
| SQoL-F17 | 17. When I think about my sex life I feel as if I have lost something 17. Quando penso na minha sexual, sinto-me como que tenha perdido algo |
| * SQoL-F18 | 18. When I think about my sex life I am satisfied the frequency of sexual intercourse * 18. Quando eu penso sobre a minha vida sexual, estou satisfeita com a frequência da atividade sexual * |
| Component | Component | ||||||
|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 1 | 2 | 3 | |
| SQoL3F | 0.945 | −0.551 | 0.883 | 0.555 | |||
| SQoL4F | 0.926 | −0.460 | 0.846 | 0.530 | |||
| SQoL8F | 0.892 | −0.570 | 0.831 | 0.605 | |||
| SQoL17F | 0.802 | 0.676 | 0.477 | ||||
| SQoL6F | 0.789 | −0.406 | −0.447 | 0.614 | 0.758 | ||
| SQoL15F | 0.767 | −0.460 | 0.556 | 0.806 | |||
| SQoL2F | 0.757 | −0.561 | 0.804 | 0.404 | |||
| SQoL13F | −0.737 | 0.554 | −0.785 | ||||
| SQoL1F | −0.673 | 0.629 | −0.774 | −0.410 | |||
| SQoL11F | 0.669 | −0.491 | −0.578 | 0.576 | 0.727 | ||
| SQoL14F | 0.637 | −0.598 | 0.884 | ||||
| SQoL5F | −0.631 | 0.483 | 0.534 | −0.768 | |||
| SQoL16F | 0.704 | 0.727 | |||||
| SQoL18F | 0.544 | 0.454 | −0.620 | ||||
| SQoL10F | 0.856 | 0.708 | |||||
| SQoL7F | 0.448 | −0.825 | 0.603 | ||||
| SQoL12F | 0.437 | −0.801 | 0.535 | ||||
| SQoL9F | −0.509 | 0.552 | 0.676 | −0.760 | |||
| Matrix | ||
|---|---|---|
| Empirical | Randomized | |
| 1 | 8.669 | 1.788 |
| 2 | 1.638 | 1.613 |
| 3 | 1.371 | 1.482 |
| 4 | 1.121 | 1.382 |
| 5 | 0.953 | 1.296 |
| 6 | 0.740 | 1.212 |
| 7 | 0.655 | 1.138 |
| 8 | 0.552 | 1.059 |
| 9 | 0.478 | 0.985 |
| 10 | 0.381 | 0.923 |
| 11 | 0.338 | 0.855 |
| 12 | 0.296 | 0.793 |
| 13 | 0.242 | 0.731 |
| 14 | 0.175 | 0.667 |
| 15 | 0.157 | 0.613 |
| 16 | 0.118 | 0.552 |
| 17 | 0.085 | 0.489 |
| 18 | 0.029 | 0.417 |
| Total | 18.00 | 18.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sim-Sim, M.; Aaberg, V.; Gómez-Cantarino, S.; Dias, H.; Caldeira, E.; Soto-Fernandez, I.; Gradellini, C. Sexual Quality of Life-Female (SQoL-F): Cultural Adaptation and Validation of European Portuguese Version. Healthcare 2022, 10, 255. https://doi.org/10.3390/healthcare10020255
Sim-Sim M, Aaberg V, Gómez-Cantarino S, Dias H, Caldeira E, Soto-Fernandez I, Gradellini C. Sexual Quality of Life-Female (SQoL-F): Cultural Adaptation and Validation of European Portuguese Version. Healthcare. 2022; 10(2):255. https://doi.org/10.3390/healthcare10020255
Chicago/Turabian StyleSim-Sim, Margarida, Vicki Aaberg, Sagrario Gómez-Cantarino, Hélia Dias, Ermelinda Caldeira, Irene Soto-Fernandez, and Cinzia Gradellini. 2022. "Sexual Quality of Life-Female (SQoL-F): Cultural Adaptation and Validation of European Portuguese Version" Healthcare 10, no. 2: 255. https://doi.org/10.3390/healthcare10020255