
Complex/cryptic EWSR1::FLI1/ERG Gene Fusions and 1q Jumping Translocation in Pediatric Ewing Sarcomas
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Summary of the Patient Cohort in This Study
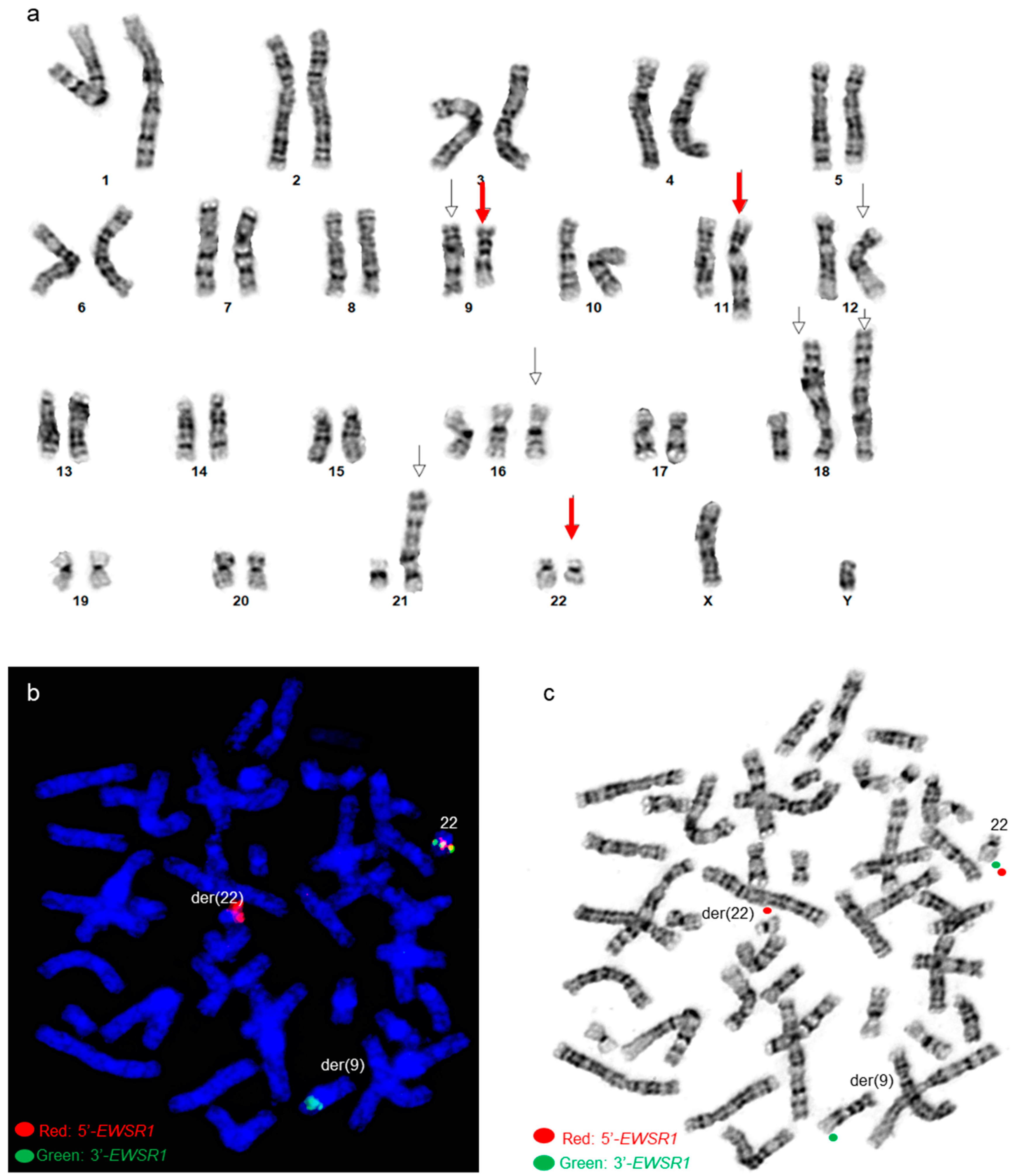
3.2. Patient 3
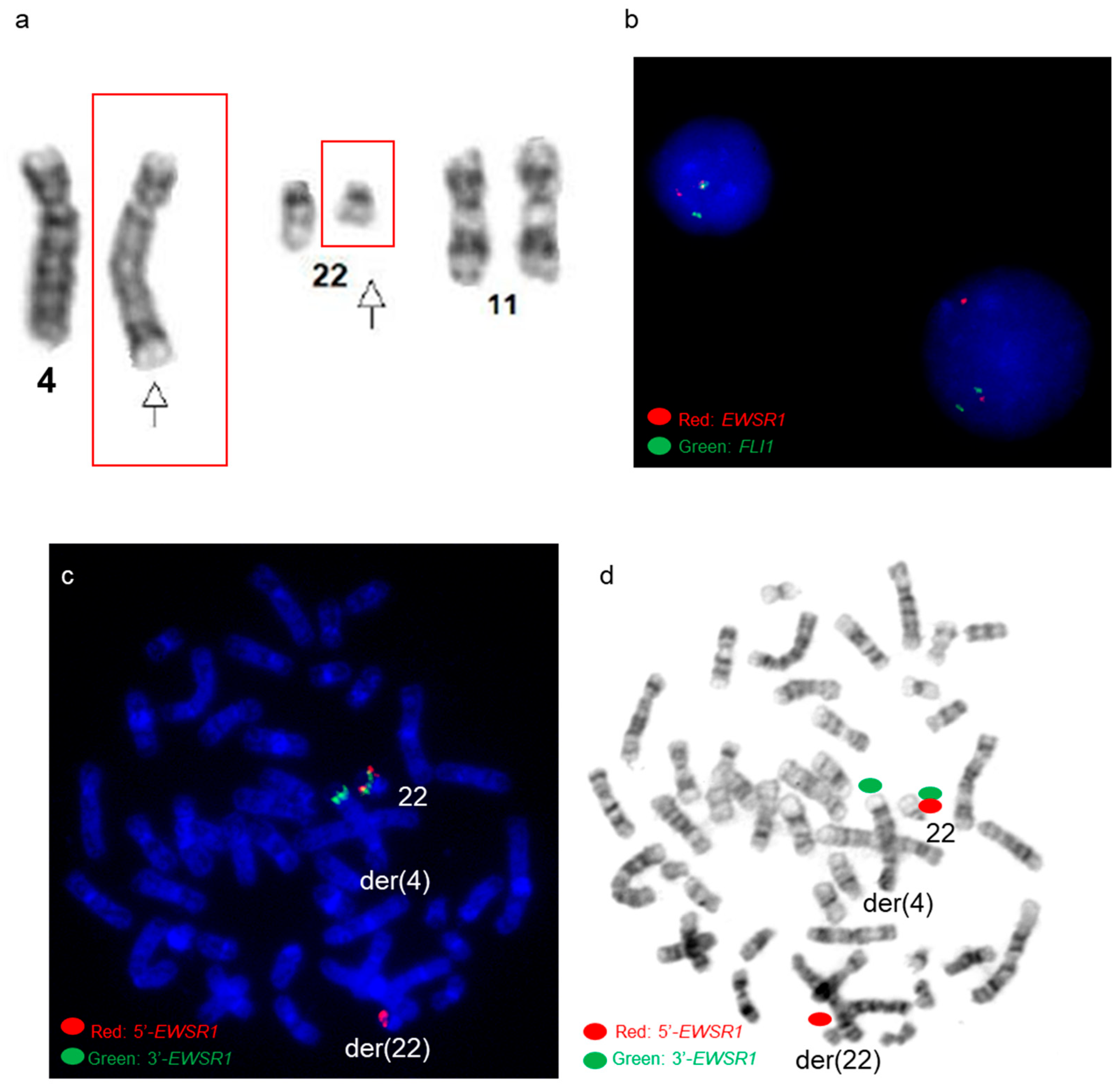
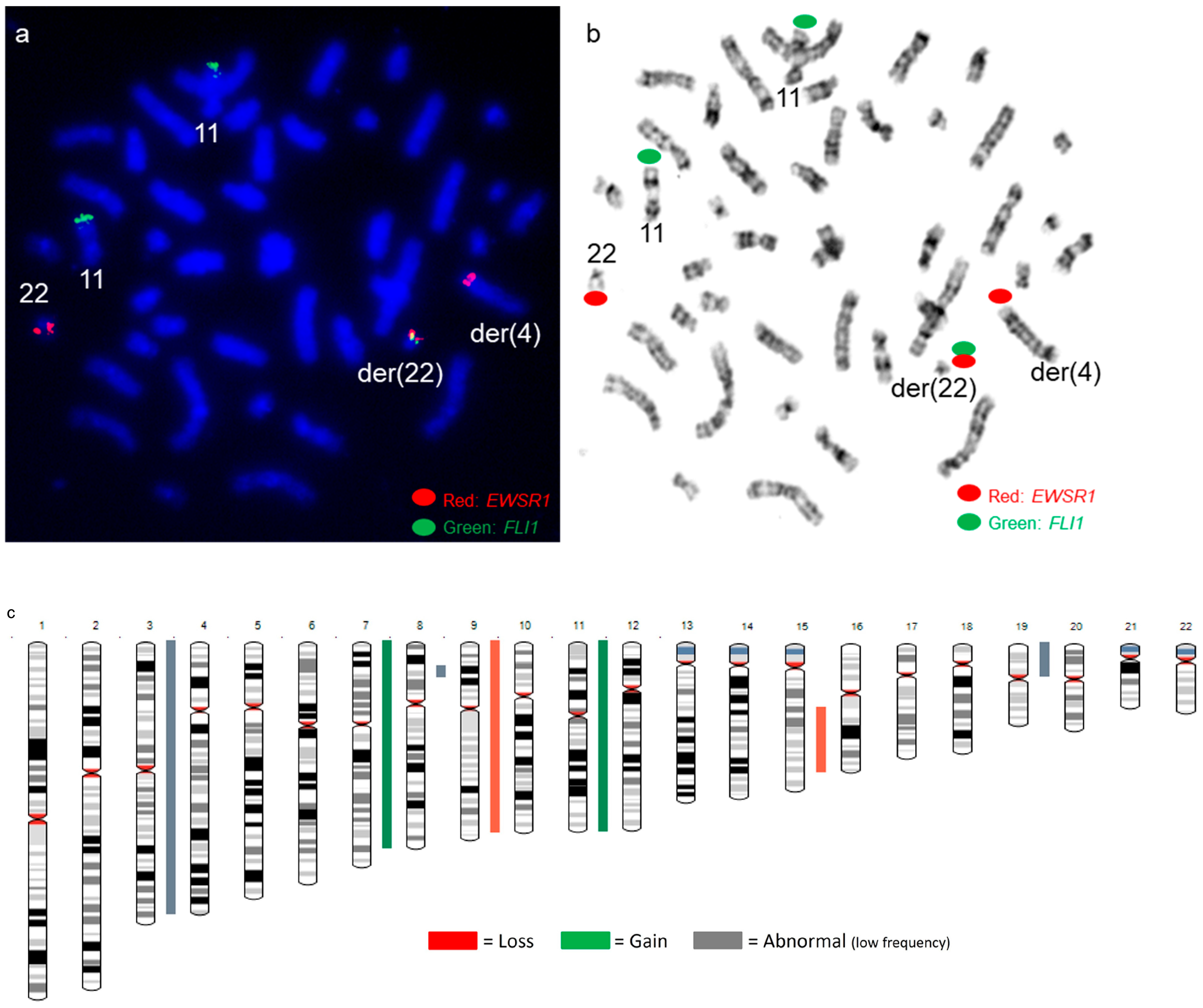
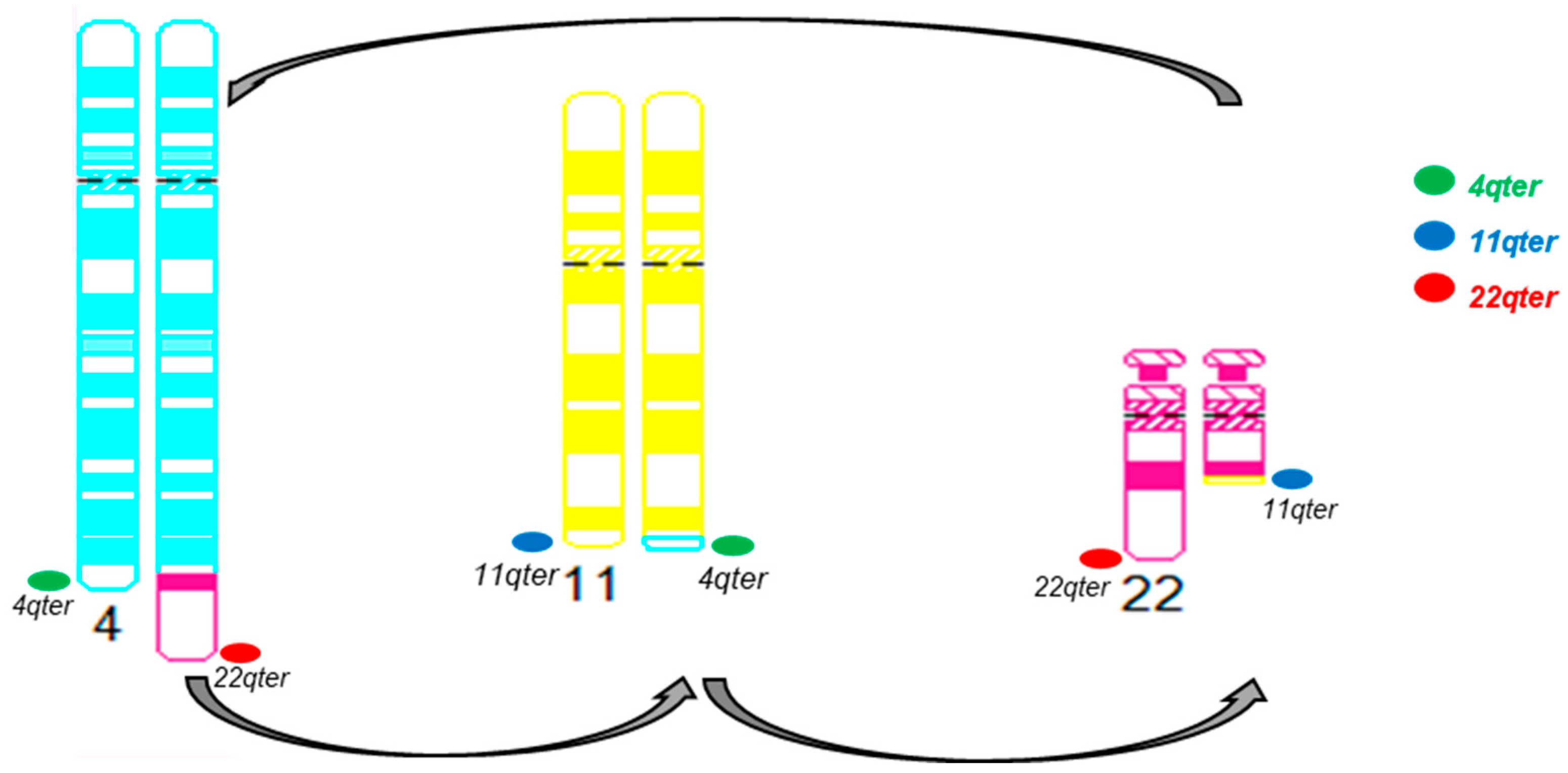
3.3. Patient 4
- NanoString gene fusion panel revealed an EWSR1::FLI1 fusion involving exon 10 of EWSR1 and exon 5 of FLI1 (Figure 9).
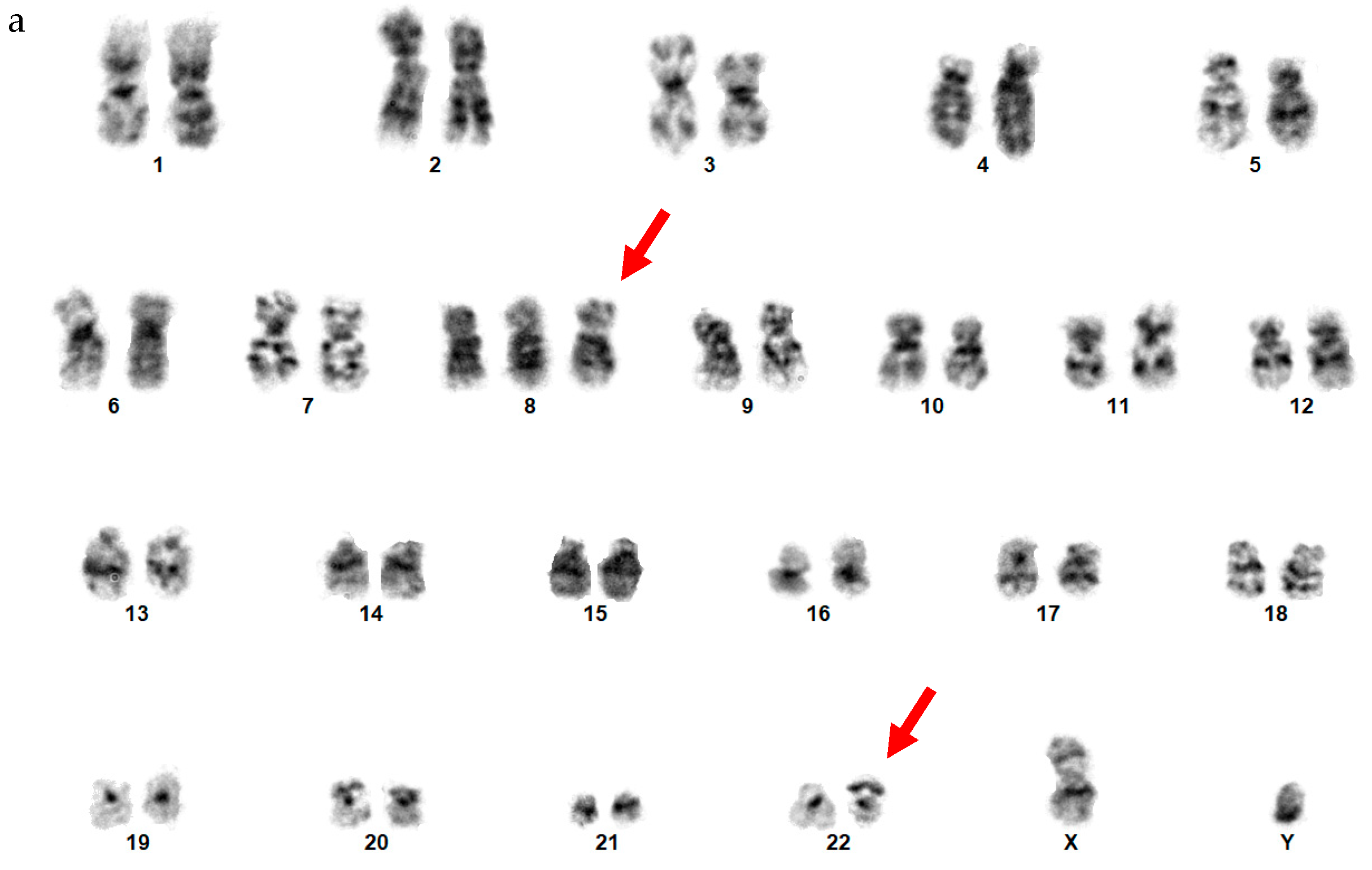
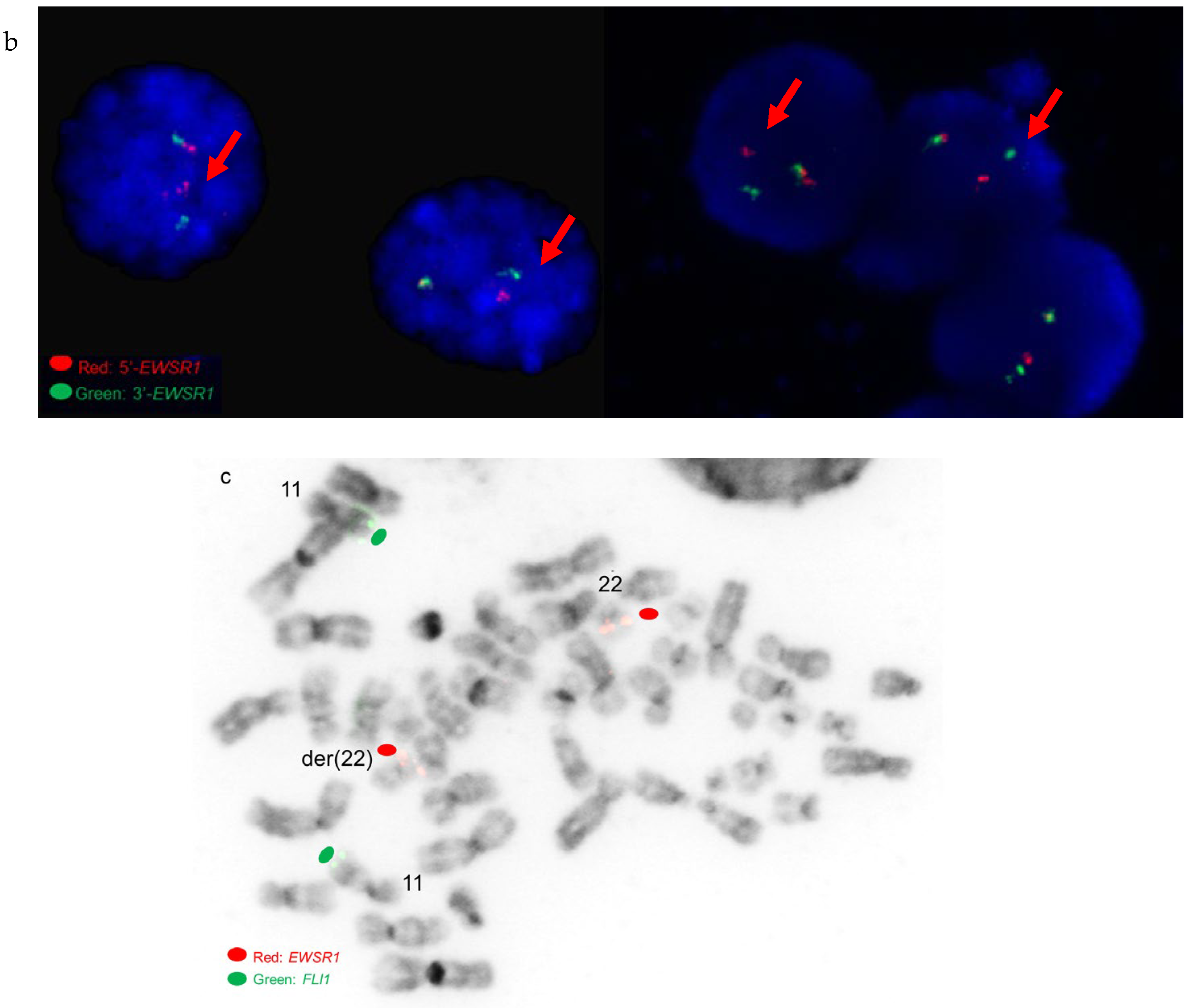
3.4. Patient 8
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The WHO Classification of Tumours Editorial Board. WHO Classification of Tumours Soft Tissue and Bone Tumours, 5th ed.; IARC Press: Lyon, France, 2020. [Google Scholar]
- Sandberg, A.A.; Bridge, J.A. The Cytogenetics of Bone and Soft Tissue Tumors; R.G.: Austin, TX, USA; Landes, France, 1994; p. 469. [Google Scholar]
- Turc-Carel, C.; Aurias, A.; Mugneret, F.; Lizard, S.; Sidaner, I.; Volk, C.; Thiery, J.P.; Olschwang, S.; Philip, I.; Berger, M.P.; et al. Chromosomes in Ewing’s sarcoma. I. An evaluation of 85 cases of remarkable consistency of t(11;22)(q24;q12). Cancer Genet. Cytogenet. 1988, 32, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Delattre, O.; Zucman, J.; Melot, T.; Garau, X.S.; Zucker, J.-M.; Lenoir, G.M.; Ambros, P.F.; Sheer, D.; Turc-Carel, C.; Triche, T.J.; et al. The Ewing Family of Tumors—A Subgroup of Small-Round-Cell Tumors Defined by Specific Chimeric Transcripts. N. Engl. J. Med. 1994, 331, 294–299. [Google Scholar] [CrossRef] [PubMed]
- Ohno, T.; Rao, V.N.; Reddy, E.S. EWS/Fli-1 chimeric protein is a transcriptional activator. Cancer Res. 1993, 53, 5859–5863. [Google Scholar] [PubMed]
- May, W.A.; Lessnick, S.L.; Braun, B.S.; Klemsz, M.; Lewis, B.C.; Lunsford, L.B.; Hromas, R.; Denny, C.T. The Ewing’s sarcoma EWS/FLI-1 fusion gene encodes a more potent transcriptional activator and is a more powerful transforming gene than FLI-1. Mol. Cell. Biol. 1993, 13, 7393–7398. [Google Scholar] [PubMed]
- Miller, H.E.; Gorthi, A.; Bassani, N.; Lawrence, L.A.; Iskra, B.S.; Bishop, A.J.R. Reconstruction of Ewing Sarcoma Developmental Context from Mass-Scale Transcriptomics Reveals Characteristics of EWSR1-FLI1 Permissibility. Cancers 2020, 12, 948. [Google Scholar] [CrossRef]
- Sandberg, A.A.; Bridge, J.A. Updates on cytogenetics and molecular genetics of bone and soft tissue tumors: Ewing sarcoma and peripheral primitive neuroectodermal tumors. Cancer Genet. Cytogenet. 2000, 123, 1–26. [Google Scholar] [CrossRef]
- Newby, R.; Rowe, D.; Paterson, L.; Farquharson, M.A.; MacDuff, E.; Coupe, A.; Hale, J.; Dildey, P.; Bown, N. Cryptic EWSR1-FLI1 fusions in Ewing sarcoma: Potential pitfalls in the diagnostic use of fluorescence in situ hybridization probes. Cancer Genet. Cytogenet. 2010, 200, 60–64. [Google Scholar] [CrossRef]
- Rekhi, B.; Vogel, U.; Basak, R.; Desai, S.B.; Jambhekar, N.A. Clinicopathological and Molecular Spectrum of Ewing Sarcomas/PNETs, Including Validation of EWSR1 Rearrangement by Conventional and Array FISH Technique in Certain Cases. Pathol. Oncol. Res. 2013, 20, 503–516. [Google Scholar] [CrossRef]
- Haley, L.; Parimi, V.; Jiang, L.; Pallavajjala, A.; Hardy, M.; Yonescu, R.; Morsberger, L.; Stinnett, V.; Long, P.; Zou, Y.S.; et al. Diagnostic Utility of Gene Fusion Panel to Detect Gene Fusions in Fresh and Formalin-Fixed, Paraffin-Embedded Cancer Specimens. J. Mol. Diagn. 2021, 23, 1343–1358. [Google Scholar] [CrossRef]
- Rivera, C.M.; Faquin, W.C.; Thierauf, J.; Afrogheh, A.H.; Jaquinet, A.; Iafrate, A.J.; Rivera, M.N.; Troulis, M.J. Detection of EWSR1 fusions in CCOC by targeted RNA-seq. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2021, 134, 240–244. [Google Scholar] [CrossRef]
- Kallen, M.E.; Hornick, J.L. From the ashes of “Ewing-like” sarcoma: A contemporary update of the classification, immunohistochemistry, and molecular genetics of round cell sarcomas. Semin. Diagn. Pathol. 2022, 39, 29–37. [Google Scholar] [CrossRef]
- Kallen, M.E.; Hornick, J.L. The 2020 WHO Classification: What’s New in Soft Tissue Tumor Pathology? Am. J. Surg. Pathol. 2021, 45, e1–e23. [Google Scholar] [CrossRef]
- Jiang, L.; Pallavajjala, A.; Huang, J.; Haley, L.; Morsberger, L.; Stinnett, V.; Hardy, M.; Park, R.; Ament, C.; Finch, A.; et al. Clinical Utility of Targeted Next-Generation Sequencing Assay to Detect Copy Number Variants Associated with Myelodysplastic Syndrome in Myeloid Malignancies. J. Mol. Diagn. 2021, 23, 467–483. [Google Scholar] [CrossRef]
- Roberts, P.; Burchill, S.A.; Brownhill, S.; Cullinane, C.J.; Johnston, C.; Griffiths, M.J.; McMullan, D.J.; Bown, N.P.; Morris, S.P.; Lewis, I.J. Ploidy and karyotype complexity are powerful prognostic indicators in the Ewing’s sarcoma family of tumors: A study by the United Kingdom Cancer Cytogenetics and the Children’s Cancer and Leukaemia Group. Genes Chromosom. Cancer 2007, 47, 207–220. [Google Scholar] [CrossRef]
- Llombart-Bosch, A.; Carda, C.; Peydro-Olaya, A.; Noguera, R.; Perez-Bacete, M.; Pellin, A.; Boix, J. Soft tissue Ewing’s sarcoma. Characterization in established cultures and xenografts with evidence of a neuroectodermic phenotype. Cancer 1990, 66, 2589–2601. [Google Scholar] [CrossRef]
- Abdelmoula, N.B.; Landman-Parker, J.; Tourniaire, B.; Josset, P.; Boccon-Gibod, L.; Peter, M.; Delattre, O. An aggressive Ewing sarcoma associated with a new variant translocation, t(4;11;22)(q25;q24;q12), hyperdiploid karyotype, and tetrasomy 8. Cancer Genet. Cytogenet. 2005, 163, 186–188. [Google Scholar] [CrossRef]
- Squire, J.; Zielenska, M.; Thorner, P.; Tennyson, S.; Weitzman, S.; Pai, K.M.; Yeger, H.; Ng, Y.-K.; Weksberg, R. Variant translocations of chromosome 22 in Ewing’s sarcoma. Genes Chromosom. Cancer 1993, 8, 190–194. [Google Scholar] [CrossRef]
- Nagaraj, P.; Srinivas, C.H.; Rao, R.; Manohar, S. Extra skeletal Soft Tissue Ewing’s Sarcoma with Variant Translocation of Chromosome t (4; 22) (q35; q12)-A Case Report. J. Orthop. Case Rep. 2013, 3, 12–15. [Google Scholar]
- Sirvent, N.; Trassard, M.; Ebran, N.; Attias, R.; Pedeutour, F. Fusion of EWSR1 with the DUX4 facioscapulohumeral muscular dystrophy region resulting from t(4;22)(q35;q12) in a case of embryonal rhabdomyosarcoma. Cancer Genet. Cytogenet. 2009, 195, 12–18. [Google Scholar] [CrossRef]
- Maire, G.; Brown, C.W.; Bayani, J.; Pereira, C.; Gravel, D.H.; Bell, J.C.; Zielenska, M.; Squire, J.A. Complex rearrangement of chromosomes 19, 21, and 22 in Ewing sarcoma involving a novel reciprocal inversion-insertion mechanism of EWS-ERG fusion gene formation: A case analysis and literature review. Cancer Genet. Cytogenet. 2008, 181, 81–92. [Google Scholar] [CrossRef]
- Kaneko, Y.; Kobayashi, H.; Handa, M.; Satake, N.; Maseki, N. EWS-ERG fusion transcript produced by chromosomal insertion in a Ewing sarcoma. Genes Chromosom. Cancer 1997, 18, 228–231. [Google Scholar] [CrossRef]
- Jinawath, N.; Morsberger, L.; Norris-Kirby, A.; Williams, L.M.; Yonescu, R.; Argani, P.; Griffin, C.A.; Murphy, K.M. Complex rearrangement of chromosomes 1, 7, 21, 22 in Ewing sarcoma. Cancer Genet. Cytogenet. 2010, 201, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Berger, R.; Bernard, O.A. Jumping translocations. Genes Chromosom. Cancer 2007, 46, 717–723. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, J.R.; Tian, E.; Walker, B.A.; Wardell, C.; Lukacs, J.L.; Sammartino, G.; Bailey, C.; Schinke, C.D.; Thanendrarajan, S.; Davies, F.E.; et al. An acquired high-risk chromosome instability phenotype in multiple myeloma: Jumping 1q Syndrome. Blood Cancer J. 2019, 9, 62. [Google Scholar] [CrossRef]
- Lee, I.; Gudipati, M.A.; Waters, E.; Duong, V.H.; Baer, M.R.; Zou, Y. Jumping translocations of chromosome 1q occurring by a multi-stage process in an acute myeloid leukemia progressed from myelodysplastic syndrome with a TET2 mutation. Mol. Cytogenet. 2019, 12, 47. [Google Scholar] [CrossRef]
- Najfeld, V.; Hauschildt, B.; Scalise, A.; Gattani, A.; Patel, R.; Ambinder, E.P.; Silverman, L.R. Jumping translocations in leukemia. Leukemia 1995, 9, 634–639. [Google Scholar]
- Hattinger, C.M.; Pötschger, U.; Tarkkanen, M.; Squire, J.; Zielenska, M.; Kiuru-Kuhlefelt, S.; Kager, L.; Thorner, P.; Knuutila, S.; Niggli, F.K.; et al. Prognostic impact of chromosomal aberrations in Ewing tumours. Br. J. Cancer 2002, 86, 1763–1769. [Google Scholar] [CrossRef]
- Mackintosh, C.; Ordonez, J.L.; Garcia-Dominguez, D.J.; Sevillano, V.; Llombart-Bosch, A.; Szuhai, K.; Scotlandi, K.; Alberghini, M.; Sciot, R.; Sinnaeve, F.; et al. 1q gain and CDT2 overexpression underlie an aggressive and highly proliferative form of Ewing sarcoma. Oncogene 2012, 31, 1287–1298. [Google Scholar] [CrossRef]
- Sawyer, J.R.; Tian, E.; Thomas, E.; Koller, M.; Stangeby, C.; Sammartino, G.; Goosen, L.; Swanson, C.; Binz, R.L.; Barlogie, B.; et al. Evidence for a novel mechanism for gene amplification in multiple myeloma: 1q12 pericentromeric heterochromatin mediates breakage-fusion-bridge cycles of a 1q12 approximately 23 amplicon. Br. J. Haematol. 2009, 147, 484–494. [Google Scholar] [CrossRef]
- Barki-Celli, L.; Lefebvre, C.; Le Baccon, P.; Nadeau, G.; Bonnefoix, T.; Usson, Y.; Vourc, C.; Khochbin, S.; Leroux, D.; Callanan, M. Differences in nuclear positioning of 1q12 pericentric heterochromatin in normal and tumor B lymphocytes with 1q rearrangements. Genes Chromosom. Cancer 2005, 43, 339–349. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | Ewing Sarcoma (Location) | Conventional Chromosome Analysis (Karyotype of Abnormal Clones) | FISH (Positive for) | Gene Fusion |
|---|---|---|---|---|
| 1 | L. chest wall | 49,XX,+4,+8,t(11;22)(q24;q12),+20/96-99,slx2 | EWSR1 | EWSR1::FLI |
| 2 | R. iliac crest | 49,XX,+5,+8,+8,t(11;22)(q24;q12) | EWSR1 | EWSR1::FLI |
| 3 | R. humerus & metastatic lung | 48,XY,del(9)(q34),t(9;11;22)(q22;q24;q12),add(12)(q24.1),+16, +18,der(18)t(1;18)(q11;p11.3)x2,der(21)t(1;21)(q11;p11.2)/ 49,sl,+13/50,sdl,+20 | EWSR1 & EWSR1::FLI1 | EWSR1::FLI |
| 4 | R. femur | 46,XY,t(4;22)(q35;q12),+8,-10,+12,-16/50,sl,+4,+8,+10,+16 | EWSR1 & EWSR1::FLI1 | EWSR1::FLI |
| 5 | L. pubic bone | 96-104,XXXX,add(1)(p12),i(1)(q10),+2,+2,+4,+4,+8,+8,+8,+8,+9, t(11;22)(q24;q12)x2,der(16)t(12;16)(q13;q24)x2,+20,+20 | EWSR1 | EWSR1::FLI |
| 6 | R. lung & metastatic lymph node | 47,XX,+1,+1,der(1;15)(q10;q10)x2,add(2)(q35),del(5)(q31),t(11;22)(q24;q12), +15 | EWSR1 | EWSR1::FLI |
| 7 | L. femur | 51,XX,+2,+5,+7,+8,t(11;22)(q24;q12),+20 at diagnosis | EWSR1 | EWSR1::FLI |
| 51,XX,+2,+5,+7,+8,del(10)(q24q25),t(11;22)(q24;q12),+20 at follow-up | EWSR1 | EWSR1::FLI | ||
| 8 | L. chest wall | 47,XY,+8,der(22)add(22)(p11.2)del(22)(q12) | EWSR1 * | EWSR1::ERG |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zou, Y.S.; Morsberger, L.; Hardy, M.; Ghabrial, J.; Stinnett, V.; Murry, J.B.; Long, P.; Kim, A.; Pratilas, C.A.; Llosa, N.J.; et al. Complex/cryptic EWSR1::FLI1/ERG Gene Fusions and 1q Jumping Translocation in Pediatric Ewing Sarcomas. Genes 2023, 14, 1139. https://doi.org/10.3390/genes14061139
Zou YS, Morsberger L, Hardy M, Ghabrial J, Stinnett V, Murry JB, Long P, Kim A, Pratilas CA, Llosa NJ, et al. Complex/cryptic EWSR1::FLI1/ERG Gene Fusions and 1q Jumping Translocation in Pediatric Ewing Sarcomas. Genes. 2023; 14(6):1139. https://doi.org/10.3390/genes14061139
Chicago/Turabian StyleZou, Ying S., Laura Morsberger, Melanie Hardy, Jen Ghabrial, Victoria Stinnett, Jaclyn B. Murry, Patty Long, Andrew Kim, Christine A. Pratilas, Nicolas J. Llosa, and et al. 2023. "Complex/cryptic EWSR1::FLI1/ERG Gene Fusions and 1q Jumping Translocation in Pediatric Ewing Sarcomas" Genes 14, no. 6: 1139. https://doi.org/10.3390/genes14061139