
From Genotype to Phenotype—A Review of Kabuki Syndrome †
by
 ,
,
Kelly K. Barry
1 ,
,
Michaelangelo Tsaparlis
2,
Deborah Hoffman
3,
Deborah Hartman
4,
Margaret P. Adam
5,
Christina Hung
2 and
Olaf A. Bodamer
2,6,*
1
Tufts University School of Medicine, Boston, MA 02111, USA
2
Division of Genetics and Genomics, Boston Children’s Hospital, Boston, MA 02115, USA
3
Takeda Pharmaceuticals, Cambridge, MA 02139, USA
4
Orexia Therapeutics, Boston, MA 02115, USA
5
Division of Genetic Medicine, Department of Pediatrics, University of Washington, Seattle, WA 98195, USA
6
Broad Institute of MIT and Harvard University, Cambridge, MA 02142, USA
*
Author to whom correspondence should be addressed.
†
This article is dedicated to Professor Dr. Norio Niikawa (1942–2022).
Genes 2022, 13(10), 1761; https://doi.org/10.3390/genes13101761
Submission received: 6 September 2022
/
Revised: 23 September 2022
/
Accepted: 24 September 2022
/
Published: 29 September 2022
(This article belongs to the Special Issue Feature Papers in Human Genomics and Genetic Diseases)
Abstract
:Kabuki syndrome (KS) is a rare neuro-developmental disorder caused by variants in genes of histone modification, including KMT2D and KDM6A. This review assesses our current understanding of KS, which was originally named Niikawa–Kuroki syndrome, and aims to guide surveillance and medical care of affected individuals as well as identify gaps in knowledge and unmet patient needs. Ovid MEDLINE and EMBASE databases were searched from 1981 to 2021 to identify reports related to genotype and systems-based phenotype characterization of KS. A total of 2418 articles were retrieved, and 152 were included in this review, representing a total of 1369 individuals with KS. Genotype, phenotype, and the developmental and behavioral profile of KS are reviewed. There is a continuous clinical phenotype spectrum associated with KS with notable variability between affected individuals and an emerging genotype–phenotype correlation. The observed clinical variability may be attributable to differences in genotypes and/or unknown genetic and epigenetic factors. Clinical management is symptom oriented, fragmented, and lacks established clinical care standards. Additional research should focus on enhancing understanding of the burden of illness, the impact on quality of life, the adult phenotype, life expectancy and development of standard-of-care guidelines.
1. Introduction
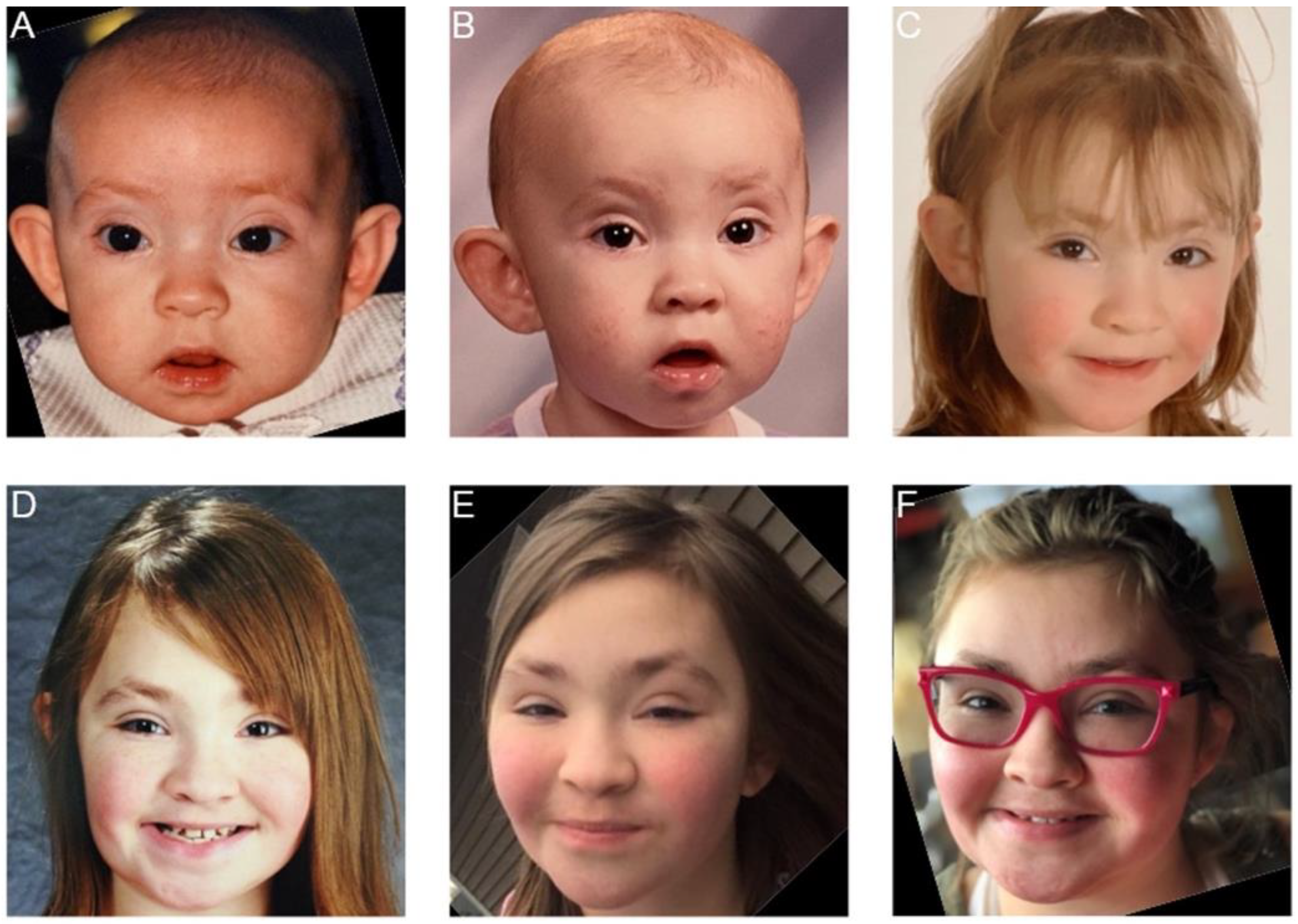
Kabuki syndrome (KS) (Niikawa–Kuroki syndrome) is a rare, congenital disorder that was first recognized as a distinct entity by two independent groups of clinicians in 1981 [1,2]. KS has been reported across all ethnicities [3,4] at an estimated frequency of 1:32,000 to 1:86,000 [5,6]. Five main cardinal features are reported to be most prevalent: (1) characteristic facial gestalt (e.g., arched eyebrows with lateral sparsening, eversion of the lateral third of the lower eye lid, long palpebral fissures, hypoplastic columella, prominent ears, cleft lip and/or palate) (Figure 1); (2) skeletal abnormalities; (3) dermatoglyphic abnormalities; (4) mild-to-moderate intellectual disability; (5) postnatal growth deficiency [5].
We now recognize that the clinical phenotype of KS follows a highly variable and continuous spectrum that additionally includes cardiac, renal, genitourinary and/or inner ear structural defects, dental anomalies, developmental delays, hypotonia, feeding difficulties, hearing loss, as well as involvement of the immune, neurologic, ophthalmologic, gastrointestinal, and endocrine systems [4,5,7]. Aspects of the clinical phenotype in KS may be accentuated in different ethnicities, as recently reported from Italy, China and Korea [8,9,10].
Updated international consensus diagnostic criteria were recently published [8]. Historically, the diagnosis of KS depended on the recognition of the characteristic facial gestalt. These features evolve over time and may make a clinical diagnosis of KS more challenging in older individuals (Figure 1).
The identification of the molecular basis of KS [9,10] allows for targeted genetic testing of individuals who may exhibit the classic phenotype of KS and for next generation sequencing (NGS) (e.g., gene panel, exome or genome) of individuals who may demonstrate certain aspects of KS. Heterozygous pathogenic variants in KMT2D are associated with autosomal dominant KS type 1 (KS1, MIM #147920) whereas heterozygous or hemizygous variants in KDM6A are associated with X-linked dominant KS type 2 (KS2, MIM #300867).
The vast majority of individuals (>80%) with a clinical diagnosis of KS harbor pathogenic variants in the coding regions of KMT2D, whereas a much smaller number (6–10%) harbor pathogenic variants in the coding regions of KDM6A [10,11,12,13]. Pathogenic variants in deep intronic or regulatory sequences of either gene have, to our knowledge, not been reported. Additional genes have been implicated in the etiology of KS-like phenotypes including RAP1A/RAP1B, HNRNPK and ZMZ1 [14,15,16]. Likely, other genes associated with a KS-like phenotype do exist.
The majority of pathogenic variants in both KMT2D and KDM6A are, de novo, either associated with loss-of-function (nonsense, frameshift, splice site) resulting in haploinsufficiency or with missense variants, which may pose a challenge for variant classification [9,10]. Mosaicism and familial variants have been reported in a few affected individuals with KS [17,18,19,20,21,22,23,24,25]. Widespread use of NGS has led to the identification of additional KMT2D-related disorders in addition to KS: Individuals with missense variants in a highly conserved region of 54 amino acids in exons 38 or 39 of KMT2D present with a unique clinical phenotype that includes choanal atresia, athelia, thyroid abnormalities, abnormal pubertal development, and short stature [26,27]. KMT2D variants may also be associated with isolated alobar holoprosencephaly [28,29]
KMT2D encodes a lysine-specific methyltransferase, responsible for post-translational histone 3 lysine 4 (H3K4) mono-, di- and tri-methylation, which is exclusively associated with actively transcribed genes [4,30]. KDM6A encodes an X-linked H3K27 demethylase that removes repressive epigenetic marks and interacts with KMT2D in regulating gene expression in the activating signal cointegrator-2 -containing complex (ASCOM) complex [31]. Transcriptional regulation is a highly specialized and temporally orchestrated process during early embryogenesis and development, ensuring the correct time and location of gene expression. This temporal and spatial coordination of transcription determines cell fate, cell-cycle progression, stem cell function, and ultimately normal embryogenesis. The complexity and importance of perfectly concerted transcriptional control necessitate a number of regulatory mechanisms, including chromatin and histone modifications. While histone modifications are conserved and broadly used mechanisms in transcriptional regulation, many of these enzymes act very specifically on their target substrates in mammals.
This review aims to appraise our current knowledge of Kabuki syndrome with specific attention to clinical presentation and associated genotypes to identify gaps in knowledge and unmet patient needs.
2. Materials and Methods
A literature search was conducted using EMBASE and Ovid MEDLINE databases by two independent individuals (KB and MT). Search terms and inclusion and exclusion criteria are detailed in Table 1. Search dates were from 1981 to April 2021. All search terms were combined using the operator “OR” (e.g., “Kabuki syndrome” OR “Niikawa–Kuroki syndrome”).
3. Results
3.1. Literature Search
A total of 2418 citations matching the search terms were identified (EMBASE 1270; Ovid MEDLINE 1148). After removal of duplicates and evaluation of abstracts for exclusion and inclusion criteria (Table 1), 152 citations were included in the final analysis.
3.2. Demographics
A total of 1369 individuals with KS were identified in the published literature. When gender was reported (n = 582), 43% were male, and 57% were female. The average age at the time of publication was 9.97 years (median 9 years, range 0–45 years). Reported ethnicity (n = 475) was as follows: Scandinavian (18%), US-American (14%), British (14%), Italian (10%), Chinese (8%), Brazilian (5%), Korean (4%), Australian (4%), Turkish (4%), French (3%), German (3%), Japanese (3%), Canadian (2%), Czech (2%), Thai (2%), Welch (1%). Case reports from Taiwan, Spain, Ireland, Palestine, Iran, Morocco, Egypt, Columbia, and Ecuador were also identified.
3.3. Genotype
A total of 1174 individuals with pathogenic or likely pathogenic variants in KMT2D were identified. The remaining 195 individuals carried a clinical diagnosis of KS without molecular confirmation. The majority of KMT2D variants were truncating (nonsense: n = 241 or frameshift: n = 137), followed by missense (n = 163), small deletions (n = 95), and splice site variants (n = 66). When recorded (n = 718), the relative frequency of variants correlated with the size of the exon and was the highest for exons 39 (20% of variants), 48 (15%), 31 (11%), 34 (7%), 11 (5%), and 10 (5%) of KMT2D. Five mosaic KMT2D cases were identified with reported levels of mosaicism of 68%, 40%, 32% and 37% in blood [17,24,25]. One study did not specify the level of mosacism [17].
A total of 89 individuals with pathogenic or likely pathogenic variants in KDM6A were identified. When described (n = 56), the majority of KDM6A variants were truncating (nonsense: n = 15, or frameshift: n = 10), followed by splice site (n = 11), missense (n = 10), large deletions (n = 3), small insertions (n = 3), indel (n = 2), and small deletions (n = 2). In a recent study which evaluated 61 pathogenic KDM6A variants in patients with KS type 2, truncating variants were distributed across the entire gene whereas missense variants were primarily clustered in the TRP2, TRP3, TRP 7, and Jmj-C domains [23]. One mosaic KDM6A case was identified; the level of mosaicism was not reported [18]
In total, 19 cases of inherited pathogenic variants from affected parents were identified including 14 inherited KDM6A variants (13 maternally inherited, 1 paternally inherited) and 5 inherited KMT2D variants (5 maternally inherited) [19,20,21,22,23,25,32]. Additional clinically diagnosed familial cases were reported [33,34,35,36]. A sex-specific pattern was observed across inherited cases of KS2, with affected mothers and daughters exhibiting a milder phenotype and affected sons displaying a more severe or “classic” phenotype. In mothers, typical facial features were less apparent and intellectual disability was generally mild or absent [19,20,21]. In the paternally inherited case of KS2, the father and daughter were similarly affected [37]. Prenatal and antenatal history is sparse for most of these cases. A complex congenital heart defect was identified antenatally in one maternally inherited case of KS2 [21]. Additionally, one family had co-inheritance of generalized epilepsy with febrile seizures plus (GEFS+) and KS2 [22]. In familial KS1, there is marked clinical heterogeneity within families without obvious sex-specific differences.
3.4. Facial Gestalt
The cardinal facial features associated with KS include long palpebral fissures; eversion of the lateral third of the lower eyelid; arched and broad eyebrows with a sparse lateral third; a broad/depressed nasal tip with short columella; and large, prominent, or cupped ears [11]. Dysmorphic facial features are most apparent in early childhood (between 3 and 12 years) [8], and to less extent in neonates, infants, and adults [13,38] (Figure 1). Though facial dysmorphism is considered a cardinal feature of KS, patients with KS2 may be less likely than patients with KS1 to have typical facial features [23].
3.5. Congenital Heart Defects
The reported frequency of congenital heart defects in KS varies, ranging between 28 and 80%; most are diagnosed prenatally or at an early age [7,39] and primarily involve the left ventricular outflow tract, including the atrial and ventricular septa [7,24]. In descending order of prevalence, ventricular septal defects, coarctation of the aorta, atrial septal defects, bicuspid aortic valve, patent ductus arteriosus, and hypoplastic left heart syndrome were most commonly reported [7,10,40,41,42,43]. The prevalence of cardiovascular anomalies may be higher in KS2 compared with KS1 [23].
3.6. Immunologic Profile
Immune deficiency and autoimmune disorders manifest in 60–73% of KS patients. Hypogammaglobulinemia occurs in up to 58% and IgA deficiency in up to 80% [44,45,46,47,48,49,50]. Like common variable immunodeficiency (CVID), immunoglobulin levels may be normal in childhood but later become abnormal [51], and autoimmune manifestations may increase with age [52]. In a large KS registry, the prevalence of infection, hypogammaglobulinemia, immune thrombocytopenia, autoimmune hemolytic anemia, thyroiditis, and vitiligo were similar between children (<9 years), teens (9–18 years), and adults (>18 years); however, the prevalence of autoimmune disease was statistically significantly higher in adults compared to children and teens [52]. Chronic otitis media, a sequela of childhood immunodeficiency, is common in children with KS, occurring in up to 40% of individuals. In rare cases, severe otitis media can result in deafness [53]
Autoimmune disorders typically manifest in late childhood between 4 and 13 years [54]. The most frequent autoimmune manifestations include immune thrombocytopenic purpura (with or without concurrent hemolytic anemia or autoimmune neutropenia) [54,55], vitiligo [56], autoimmune thyroiditis [57], type 1 diabetes [6,58,59,60], and type 3 membranous glomerulonephritis [61]. Interestingly, selective IgA deficiency (common in KS), may be causally related to the development of type I diabetes [59,62,63]. Inflammatory bowel disease has also been reported [64].
Rare cases of premature death have been reported in severely immunologically impaired patients [46,51,52,58,65]. In one study, three of the five deaths were secondary to immunopathological complications including acute bronchitis (n = 2) and acute hemolysis secondary to chronic Evans syndrome (n = 1) at <1, 2, and 24 years of age, respectively [52].
3.7. Brain and Neurologic Manifestations
Congenital central nervous system malformations and functional neurological abnormalities are common. Muscular hypotonia is highly prevalent (51–98%) and may lead to long-term sequelae including developmental delays and oromotor dysfunction [66]. Emerging evidence suggests that hypotonia may be due to a primary defect in skeletal muscle [67]. Dysarthria is not uncommon (10–26%) and may be underestimated [68]. Vestibular dysfunction also contributes to gross motor delay [69]. The estimated prevalence of epilepsy is 17%, with the age of onset ranging from infancy to adolescence [70,71,72]. Partial seizures involving the frontal and temporal regions manifesting with focal motor deficits are well-described [71,73,74,75,76,77]. No relationship between epileptogenic zone and polymicrogyria has been established [74,75,78].
Structural central nervous system anomalies may have an ethnic association; most cases of cortical dysplasia were reported in Caucasian individuals, although reporting biases cannot be excluded [78]. The reported spectrum of congenital brain abnormalities continues to expand. Recently, a case of lobar holoprosencephaly was described [79].
3.8. Cancer
The incidence of cancer and whether individuals with KS have an increased predisposition for malignancy is unknown. Somatic mutations in the histone methyltransferase KMT2D are frequently implicated in tumorigenesis and depending on the biologic context, this methyltransferase may exert either tumor suppressive or promoting functions [80,81]. It has been proposed that patients with germline variants in KMT2D may be at an increased risk for developing cancer due to somatic second hit mutations [81]. Despite this, less than twenty patients with Kabuki syndrome and malignancies, mostly affecting soft tissues or the hematological system, have been reported. Solid and soft tissue neoplasms reported in KS and age at diagnosis include: Wilms tumor, 3 years [82]; neuroblastoma, 6 months [83]; low-grade fibromyxoid sarcoma, 11 years [84]; synovial sarcoma, 16 years [85]; aggressive desmoid fibromatosis, 10 years [81]; hepatoblastoma, 6 years [83]; hepatocellular carcinoma, 15 years [86]; giant cell fibroblastoma, 12 years [87]; spinal ependymoma, 23 years [88]. Hematologic malignancies and age at diagnosis include Hodgkin lymphoma, 34 years [89]; acute lymphocytic leukemia, 1 year [90]; Burkitt lymphoma, 3 and 5 years, respectively [91,92]. Notably, Epstein-Barr virus (EBV)-positive Burkitt’s lymphoma is more commonly seen in immunocompromised patients, perhaps explaining its relationship with KS [93,94]. Pilomatrixomas, a benign tumor of the hair cell matrix, are also infrequently reported [95,96].
3.9. Endocrinopathies
Endocrine dysfunction is common in KS. Postnatal growth restriction occurs in 35–85% of individuals and is far more common than growth hormone deficiency [5,97,98,99]. Recent attention has focused on persistent hyperinsulinemic hypoglycemia, which is likely underdiagnosed or underreported in KS [18,100]. If untreated, hyperinsulinemic hypoglycemia can lead to developmental delay and permanent neurologic damage [18]. Persistent hypoglycemia in infancy is attributed to pituitary hormone deficiency, growth hormone deficiency, adrenal insufficiency, and, more notably, dysregulated insulin secretion by the pancreatic β-cells. Persistent hypoglycemia may be more common in KS2, suggesting a possible genotype–phenotype correlation [12]. Supporting this, inhibition of KDM6A increased the release of insulin from pancreatic islet cells in murine models [101].
Two cases of isolated central diabetes insipidus (DI) are described in the literature [102,103]. Although congenital brain malformations can cause central DI, most cases are idiopathic [103]. Of these case reports, one patient had an abnormal pituitary gland and stalk on MRI.
In KS, the risk for diabetes mellitus type II may be as high as 20% in early adulthood [104]. In such cases, type II diabetes is usually comorbid with obesity.
3.10. Genitourinary Anomalies
In total, 30–40% of individuals with KS have a genitourinary anomaly [66]. Both renal and urogenital anomalies are common; the most common renal malformations are horseshoe kidneys and renal hypoplasia [105]. In males, cryptorchidism and hypospadias are the most prevalent urogenital anomalies [13,106,107]. Rare cases of other anomalies including ureteric and renal duplication, ectopic kidneys, renal agenesis, hypoplastic labia are reported [40,87,108,109]. Renal dysfunction and failure are rare, occurring in a few isolated cases [97,106,110,111,112]. Most cases of severe renal insufficiency are secondary to congenital renal dysplasia. Renal anomalies can increase susceptibility to urinary tract infections and, less frequently, renal calculi. Interestingly, patients with KS2 may have a higher prevalence of genitourinary anomalies than those with KS1 overall but a lower prevalence of kidney and renal tract anomalies [23].
3.11. Ophthalmologic Abnormalities
Ocular abnormalities occur in 38–72% of KS patients [113,114]. In addition to cardinal features (e.g., long palpebral fissures, lower eyelid eversion, and epicanthus), ptosis, epiblepharon, and centurion eyelid syndrome with consecutive epiphora are observed in 10–20% of individuals [115]. Refractive errors, notably astigmatism, may occur in up to 90% of patients [115]. Microphthalmia, anophthalmia, and coloboma (MAC) spectrum is the third most common manifestation in about 3.2% of cases [88]. In a large cohort of patients with KS2, nystagmus was reported in 11% of patients [23].
3.12. Gastrointestinal Involvement
3.13. Reproductive Health
There is a paucity of information regarding fertility and reproductive health pertaining to KS. Familial transmission of KS both to and from affected males and females has been reported [19,20,21,22,37]. Endocrine dysregulation can interfere with fertility, but the extent and implication of this are not adequately discussed in the existing literature [116]. Both patients and clinicians would benefit from further research in this area.
3.14. Prenatal and Perinatal History
There is a paucity of data concerning prenatal and perinatal complications of KS. One study reported abnormal second and third trimester ultrasounds and quad screens in 69% and 44% of cases, respectively [117]. Polyhydramnios is reported in 25–41% of pregnancies [117,118,119] compared to 0.5–2% in the general population [120,121]. It is plausible that craniofacial anomalies or functional impairment in swallowing, both well-described features of KS, contribute to this finding [117].
3.15. Growth and Feeding
Postnatal growth restriction (60–83%) and short stature (31–81%) [5,97] are common in KS. Birth parameters are typically normal, but failure to thrive and growth restriction become apparent in infancy, likely secondary to feeding problems and hypotonia, resulting in poorly coordinated sucking and swallowing [40,97]. Severe feeding difficulty in infancy necessitates nasogastric tube or gastrostomy tube placement in 65–74% of infants [40,113]. Premature birth, growth hormone deficiency, delayed bone age, aspiration pneumonia, congenital heart defects, and palatal anomalies [122] also contribute to delayed or abnormal growth but do not entirely explain the growth restriction [105]. In KS2, sex-specific differences in growth parameters have been described; in one study, males had shorter birth lengths and significantly shorter stature at last examination compared to their female counterparts [23]. There is limited research evaluating the impact of recombinant human growth hormone (rh-GH) therapy in children with KS. Several small studies have shown promising results, demonstrating statistically significant increases in linear growth following at least one year of rh-GH therapy, without negatively impacting cardiovascular health [123,124,125]. Without growth hormone therapy, adult height may fall anywhere from −5.57 SD and −1.08 SD below the mean for healthy controls, with females more severely affected than males [126].
The natural history of KS is poorly characterized. In one Japanese study, childhood height ranged from −2.1 to −5 SD below the mean for healthy controls; 27% of children had height within the normal range; none were greater than +0.5 SD above the mean [5]. In another study, the average birth length was −0.14 SD and −0.11 SD below the mean for males and females, respectively. Growth restriction became more apparent by one year of age and was maintained into adulthood [122]. KS1-specific growth charts were recently developed to establish normative growth parameters [127].
Interestingly, up to 50% of individuals with KS will become overweight or obese in late childhood or adolescence [6,23,40,97,127]. In one study, BMI was in the overweight to obese range in 57% of patients over 5 years old [6]; 75% of these children failed to thrive in infancy. Unsurprisingly, obesity in adolescence is associated with significant comorbidities and can exacerbate pre-existing medical issues, such as patellar dislocation [128], which is more common in older children with KS, particularly females with hypermobile knee joints. Patients with KS may also have an inherent predisposition for developing hypertension, even in the absence of other metabolic risk factors, due to premature atherosclerosis [129] and growth hormone deficiency, which is associated with endothelial dysfunction, increased intimal thickness, and reduced aortic elasticity [7].
3.16. Language and Development
Developmental milestones are often delayed in children with KS. Cognitive impairment, hypotonia, skeletal anomalies, congenital heart defects, hearing loss, and gastrointestinal anomalies can cause delays in speech and language development, feeding and swallowing, walking, sitting upright, and toilet training [25,119,130,131,132,133]. Conductive and sensorineural hearing loss, in particular, are associated with poor verbal outcomes [119].
In one study, the average age of acquisition of developmental milestones was as follows [119]: sitting unassisted, 11 months; walking without assistance, 20 months; single word utterance, 21 months. Language development was uniformly delayed; only one patient acquired their first word at a developmentally appropriate time.
Language acquisition varies in KS [134,135]. Although most children will eventually speak in complete sentences, isolated case reports describe children without a single word or simple sentence development until upwards of 10 years [133,136]. Patients may be nonverbal at the extreme end of the spectrum [134,137]. Motor and language development do not always correlate; some individuals may have significant motor impairment with relatively strong language skills and vice versa.
No clear pattern of psychomotor development has emerged, and data are limited to sporadic case reports [1,2,36,134,138,139]; however, some genotype–phenotype hypotheses have emerged. Haploinsufficiency of KDM6A is similarly associated with more severe psychomotor developmental delays [134]. In KS2, males may exhibit more severe neurodevelopmental issues, whereas females with KS2 display a more variable neurodevelopmental profile, possibly due to differences in X-chromosome inactivation [23]. Patients with protein-truncating mutations in KDM6A versus protein-altering variants may also display more severe intellectual disability [23].
3.17. Cognitive Profile
Intellectual disability (ID) is one of the cardinal features of KS, presenting in up to 90% of cases [98,99]. ID is generally designated with intelligence quotient (IQ) scores of less than 70, which falls into the “very low range of functioning” (bottom 2%) of age-matched individuals [140]. In KS, intellectual disability is typically mild to moderate; average IQ is in the upper-50s or low-to-mid 60s [25,141,142] with a range of 25–109 [17]. Up to 92% of individuals with KS will have an IQ of 80 or less [143]. IQ scores in the low 40s represent the lower bound of performance [17,57,141,144,145].
Severe ID is rare and only described in a few cases [12,17,76,146]. Individuals with KS typically possess relative strengths in verbal reasoning and working memory with excellent long-term memory of faces, music, lyrics, events, and dates [6]. Age-appropriate planning, cognitive flexibility, and social cognition are also observed [147]. Conversely, relative deficiencies in visual-spatial skills, processing speed, and nonverbal reasoning are described [17,25,130,147]. Further insight into difficult cognitive tasks reported in KS by parents include reading a map, following directions to a location, and math problems [148].
3.18. Communication, Speech, and Language
A variable pattern of oromotor, speech, and language deficits reflects neurologic, orofacial, structural, hearing, and cognitive impairment.
Receptive and expressive language delays present across multiple language sub-domains (e.g., semantics, syntax, morphology, and pragmatics) [68,119]; however, a deficit in one language domain does not predict disordered development in another [149]. Articulation and resonance can also be affected [68,150]; speech is often described as “thick, slurred, and indistinct” [133] and resonance as “hyper-nasal” [68,151], likely secondary to poor oromotor coordination and hypotonia [149,150]. Dysarthria, characterized by imprecise consonants, harsh vocal quality, hypernasality, and slowed rate of speech, is common. Children with otherwise normal cognition and appropriate expressive/receptive vocabulary may use phonological processes to simplify words or demonstrate poor morphosyntactic (e.g., ‘word endings’ such as -ing, plural -s) abilities [132].
Some studies report improvements in speech, language, and oromotor function with age; however, others conclude the opposite, noting worsening language impairment over time [74,152]. Regardless, most individuals with KS will have communication deficits persisting into early childhood or adolescence [68].
3.19. Behavioral Phenotype
Autistic-like behavior, hyperactivity, inattention, impulsivity, self-mutilation, sleep disturbances, multiple phobias, emotional dysregulation, impairment of adaptive skills, difficulty with communication and peer interactions, poor eye contact, and anxiety disorders are among the diverse behavioral phenotypes associated with KS [6,10,11,12,56,58,138,153,154,155]. Though children may exhibit autistic-like behaviors, diagnostic criteria for autism are met in a minority of cases [11,138].
Severe behavioral phenotypes (e.g., aggression, oppositional behavior) are rare, occurring only in patients with severe cognitive deficits [130]. Children with KS generally behave as expected for their chronological age and demonstrate age-appropriate maladaptive behavior [130].
More consistently, children with KS are socially outgoing, talkative, and affectionate, with good socialization skills and affable nature [6,130]. A small survey of adolescents with KS reported a range of emotional impacts that included anxiety, sadness, frustration, and feeling different from other people [89].
4. Conclusions
A broad and continuous spectrum of clinical phenotypes is associated with KS, with notable variability between affected individuals. Advancements in genetic sequencing improve our understanding of this disease and elucidate the role of KMT2D and KDM6A in transcriptional regulation, growth, and development. Current literature lacks consistent clinical characterization of KS, posing challenges in drawing meaningful genotype–phenotype correlations. Limited long-term follow-up similarly restricts our understanding of the natural history of the disease. Unfortunately, clinical management is fragmented and remains largely symptom oriented.
This review holistically examines KS and details the natural history as described in current literature to guide the surveillance and expectant management of KS (Table 2, Table 3 and Table 4). Clinicians, caregivers, and affected individuals would benefit from an improved understanding of the disease burden and impact on quality of life, the adult phenotype, and the development of standard-of-care guidelines.
Author Contributions
Conceptualization, K.K.B., D.H. (Deborah Hartman) and O.A.B.; methodology, K.K.B., O.A.B.; data curation, K.K.B., M.T., C.H.; writing—original draft preparation, K.K.B.; writing—review and editing, K.K.B., M.T., M.P.A., C.H., O.A.B., D.H. (Deborah Hartman), D.H. (Deborah Hoffman); supervision, D.H., O.A.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Written informed consent was obtained from the patient to publish their photographs in this paper.
Data Availability Statement
Not applicable.
Acknowledgments
We would like to thank our patient and her family for their willingness to provide photographs for this study.
Conflicts of Interest
Kelly Barry and Deborah Hoffman were employed at Takeda Pharmaceuticals at the time this study was initiated. Takeda Pharmaceuticals had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results. All other authors have no conflicts of interest to disclose.
References
- Niikawa, N.; Matsuura, N.; Fukushima, Y.; Ohsawa, T.; Kajii, T. Kabuki make-up syndrome: A syndrome of mental retardation, unusual facies, large and protruding ears, and postnatal growth deficiency. J. Pediatr. 1981, 99, 565–569. [Google Scholar] [CrossRef]
- Kuroki, Y.; Suzuki, Y.; Chyo, H. A new malformation syndrome of long palpebral fissures, large ears, depressed nasal tip, and skeletal anomalies associated with postnatal dwarfism and mental retardation. J. Pediatr. 1981, 99, 570–573. [Google Scholar] [CrossRef]
- Adam, M.P.; Hudgins, L. Kabuki syndrome: A review. Clin. Genet. 2005, 67, 209–219. [Google Scholar] [CrossRef]
- Bogershausen, N.; Gatinois, V.; Riehmer, V.; Kayserili, H.; Becker, J.; Thoenes, M.; Simsek-Kiper, P.O.; Barat-Houari, M.; Elcioglu, N.H.; Wieczorek, D.; et al. Mutation Update for Kabuki Syndrome Genes KMT2D and KDM6A and Further Delineation of X-Linked Kabuki Syndrome Subtype 2. Hum. Mutat. 2016, 37, 847–864. [Google Scholar] [CrossRef] [PubMed]
- Niikawa, N.; Kuroki, Y.; Kajii, T.; Matsuura, N.; Ishikiriyama, S.; Tonoki, H.; Ishikawa, N.; Yamada, Y.; Fujita, M.; Umemoto, H.; et al. Kabuki make-up (Niikawa-Kuroki) syndrome: A study of 62 patients. Am. J. Med. Genet. 1988, 31, 565–589. [Google Scholar] [CrossRef]
- White, S.M.; Thompson, E.M.; Kidd, A.; Savarirayan, R.; Turner, A.; Amor, D.; Delatycki, M.B.; Fahey, M.; Baxendale, A.; White, S.; et al. Growth, behavior, and clinical findings in 27 patients with Kabuki (Niikawa-Kuroki) syndrome. Am. J. Med. Genet. Part A 2004, 127A, 118–127. [Google Scholar] [CrossRef] [PubMed]
- Digilio, M.C.; Gnazzo, M.; Lepri, F.; Dentici, M.L.; Pisaneschi, E.; Baban, A.; Passarelli, C.; Capolino, R.; Angioni, A.; Novelli, A.; et al. Congenital heart defects in molecularly proven Kabuki syndrome patients. Am. J. Med. Genet. Part A 2017, 173, 2912–2922. [Google Scholar] [CrossRef] [PubMed]
- Adam, M.P.; Banka, S.; Bjornsson, H.T.; Bodamer, O.; Chudley, A.E.; Harris, J.; Kawame, H.; Lanpher, B.C.; Lindsley, A.W.; Merla, G.; et al. Kabuki syndrome: International consensus diagnostic criteria. J. Med. Genet. 2019, 56, 89–95. [Google Scholar] [CrossRef]
- Ng, S.B.; Bigham, A.W.; Buckingham, K.J.; Hannibal, M.C.; McMillin, M.J.; Gildersleeve, H.I.; Beck, A.E.; Tabor, H.K.; Cooper, G.M.; Mefford, H.C.; et al. Exome sequencing identifies MLL2 mutations as a cause of Kabuki syndrome. Nat Genet. 2010, 42, 790–793. [Google Scholar] [CrossRef]
- Lederer, D.; Grisart, B.; Digilio, M.C.; Benoit, V.; Crespin, M.; Ghariani, S.C.; Maystadt, I.; Dallapiccola, B.; Verellen-Dumoulin, C. Deletion of KDM6A, a histone demethylase interacting with MLL2, in three patients with kabuki syndrome. Am. J. Hum. Genet. 2012, 90, 119–124. [Google Scholar] [CrossRef] [Green Version]
- Paděrová, J.; Holubová, A.; Simandlová, M.; Puchmajerová, A.; Vlčková, M.; Malíková, M.; Pourová, R.; Vejvalková, S.; Havlovicová, M.; Šenkeříková, M.; et al. Molecular genetic analysis in 14 Czech Kabuki syndrome patients is confirming the utility of phenotypic scoring. Clin. Genet. 2016, 90, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Banka, S.; Lederer, D.; Benoit, V.; Jenkins, E.; Howard, E.; Bunstone, S.; Kerr, B.; McKee, S.; Lloyd, I.C.; Shears, D.; et al. Novel KDM6A (UTX) mutations and a clinical and molecular review of the X-linked Kabuki syndrome (KS2). Clin. Genet. 2015, 87, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Bögershausen, N.; Wollnik, B. Unmasking Kabuki syndrome. Clin. Genet. 2013, 83, 201–211. [Google Scholar] [CrossRef] [PubMed]
- Lange, L.; Pagnamenta, A.T.; Lise, S.; Clasper, S.; Stewart, H.; Akha, E.S.; Quaghebeur, G.; Knight, S.J.L.; Keays, D.A.; Taylor, J.C.; et al. A de novo frameshift in HNRNPK causing a Kabuki-like syndrome with nodular heterotopia. Clin. Genet. 2016, 90, 258–262. [Google Scholar] [CrossRef]
- Bögershausen, N.; Tsai, I.C.; Pohl, E.; Simsek Kiper, P.Ö.; Beleggia, F.; Percin, F.E.; Keupp, K.; Matchan, A.; Milz, E.; Alanay, Y.; et al. Spotlight on the pathogenesis of Kabuki syndrome. Med. Genet. 2015, 27, 84. [Google Scholar]
- Carapito, R.; Ivanova, E.L.; Morlon, A.; Meng, L.; Molitor, A.; Erdmann, E.; Kieffer, B.; Pichot, A.; Naegely, L.; Kolmer, A.; et al. ZMIZ1 Variants Cause a Syndromic Neurodevelopmental Disorder. Am. J. Hum. Genet. 2019, 104, 319–330. [Google Scholar] [CrossRef]
- Caciolo, C.; Alfieri, P.; Piccini, G.; Digilio, M.C.; Lepri, F.R.; Tartaglia, M.; Menghini, D.; Vicari, S. Neurobehavioral features in individuals with Kabuki syndrome. Mol. Genet. Genomic Med. 2018, 6, 322–331. [Google Scholar] [CrossRef]
- Yap, K.L.; Johnson, A.E.K.; Fischer, D.; Kandikatla, P.; Deml, J.; Nelakuditi, V.; Halbach, S.; Jeha, G.S.; Burrage, L.C.; Bodamer, O.; et al. Congenital hyperinsulinism as the presenting feature of Kabuki syndrome: Clinical and molecular characterization of 10 affected individuals. Gen. Med. 2019, 21, 233–242. [Google Scholar] [CrossRef]
- Margot, H.; Geneviève, D.; Gatinois, V.; Arveiler, B.; Moutton, S.; Touitou, I.; Lacombe, D. Typical facial gestalt in X-linked Kabuki syndrome. Am. J. Med. Genet. Part A 2016, 170, 3363–3364. [Google Scholar] [CrossRef]
- Hannibal, M.C.; Buckingham, K.J.; Ng, S.B.; Ming, J.E.; Beck, A.E.; McMillin, M.J.; Gildersleeve, H.I.; Bigham, A.W.; Tabor, H.K.; Mefford, H.C.; et al. Spectrum of MLL2 (ALR) mutations in 110 cases of Kabuki syndrome. Am. J. Med. Genet. Part A 2011, 155, 1511–1516. [Google Scholar] [CrossRef]
- Lederer, D.; Shears, D.; Benoit, V.; Verellen-Dumoulin, C.; Maystadt, I. A three generation X-linked family with Kabuki syndrome phenotype and a frameshift mutation in KDM6A. Am. J. Med. Genet. Part A 2014, 164, 1289–1292. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Lee, C.G. Coinheritance of novel mutations in SCN1A causing gefs+ and in KDM6A causing kabuki syndrome in a family. Ann. Clin. Lab. Sci. 2017, 47, 229–235. [Google Scholar] [PubMed]
- Faundes, V.; Goh, S.; Akilapa, R.; Bezuidenhout, H.; Bjornsson, H.T.; Bradley, L.; Brady, A.F.; Brischoux-Boucher, E.; Brunner, H.; Bulk, S.; et al. Clinical delineation, sex differences, and genotype–phenotype correlation in pathogenic KDM6A variants causing X-linked Kabuki syndrome type 2. Gen. Med. 2021, 23, 1202–1210. [Google Scholar] [CrossRef] [PubMed]
- Murakami, H.; Tsurusaki, Y.; Enomoto, K.; Kuroda, Y.; Yokoi, T.; Furuya, N.; Yoshihashi, H.; Minatogawa, M.; Abe-Hatano, C.; Ohashi, I.; et al. Update of the genotype and phenotype of KMT2D and KDM6A by genetic screening of 100 patients with clinically suspected Kabuki syndrome. Am. J. Med. Genet. Part A 2020, 182, 2333–2344. [Google Scholar] [CrossRef] [PubMed]
- Lepri, F.R.; Cocciadiferro, D.; Augello, B.; Alfieri, P.; Pes, V.; Vancini, A.; Caciolo, C.; Squeo, G.M.; Malerba, N.; Adipietro, I.; et al. Clinical and neurobehavioral features of three novel kabuki syndrome patients with mosaic KMT2D mutations and a review of literature. Int. J. Mol. Sci. 2018, 19, 82. [Google Scholar] [CrossRef]
- Cuvertino, S.; Hartill, V.; Colyer, A.; Garner, T.; Nair, N.; Al-Gazali, L.; Canham, N.; Faundes, V.; Flinter, F.; Hertecant, J.; et al. A restricted spectrum of missense KMT2D variants cause a multiple malformations disorder distinct from Kabuki syndrome. Gen. Med. 2020, 22, 867–877. [Google Scholar] [CrossRef]
- Baldridge, D.; Spillmann, R.C.; Wegner, D.J.; Wambach, J.A.; White, F.V.; Sisco, K.; Toler, T.L.; Dickson, P.I.; Cole, F.S.; Shashi, V.; et al. Phenotypic expansion of KMT2D-related disorder: Beyond Kabuki syndrome. Am. J. Med. Genet. Part A 2020, 182, 1053–1065. [Google Scholar] [CrossRef]
- Tekendo-Ngongang, C.; Kruszka, P.; Martinez, A.F.; Muenke, M. Novel heterozygous variants in KMT2D associated with holoprosencephaly. Clin Genet. 2019, 96, 266–270. [Google Scholar] [CrossRef]
- Sakaria, R.P.; Zaveri, P.G.; Holtrop, S.; Zhang, J.; Brown, C.W.; Pivnick, E.K. Case Report: An Infant With Kabuki Syndrome, Alobar Holoprosencephaly and Truncus Arteriosus: A Case for Whole Exome Sequencing in Neonates With Congenital Anomalies. Front Genet. 2021, 12, 766316. [Google Scholar] [CrossRef]
- Froimchuk, E.; Jang, Y.; Ge, K. Histone H3 lysine 4 methyltransferase KMT2D. Gene 2017, 627, 337–342. [Google Scholar] [CrossRef]
- Aref-Eshghi, E.; Schenkel, L.C.; Lin, H.; Skinner, C.; Ainsworth, P.; Pare, G.; Rodenhiser, D.; Schwartz, C.; Sadikovic, B. The defining DNA methylation signature of Kabuki syndrome enables functional assessment of genetic variants of unknown clinical significance. Epigenetics 2017, 12, 923–933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kokitsu-Nakata, N.M.; Petrin, A.L.; Heard, J.P.; Vendramini-Pittoli, S.; Henkle, L.E.; dos Santos, D.V.C.; Murray, J.C.; Richieri-Costa, A. Analysis of MLL2 gene in the first Brazilian family with Kabuki syndrome. Am. J. Med. Genet. Part A 2012, 158A, 2003–2008. [Google Scholar] [CrossRef] [PubMed]
- Halal, F.; Gledhill, R.; Dudkiewicz, A. Autosomal dominant inheritance of the Kabuki make-up (Niikawa-Kuroki) syndrome. Am. J. Med. Genet. 1989, 33, 376–381. [Google Scholar] [CrossRef]
- Galan-Gomez, E.; Cardesa-Garcia, J.J.; Campo-Sampedro, F.M.; Salamanca-Maesso, C.; Martinez-Frias, M.L.; Frias, J.L. Kabuki make-up (Niikawa-Kuroki) syndrome in five Spanish children. Am. J. Med. Genet. 1995, 59, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Frediani, T.; Lucarelli, S.; Bruni, L. Niikawa-Kuroki (Kabuki) syndrome in two siblings. Minerva Pediatr. 2001, 53, 43–48. [Google Scholar]
- Shotelersuk, V.; Punyashthiti, R.; Srivuthana, S.; Wacharasindhu, S. Kabuki syndrome: Report of six Thai children and further phenotypic and genetic delineation. Am. J. Med. Genet. 2002, 110, 384–390. [Google Scholar] [CrossRef]
- Faundes, V.; Malone, G.; Newman, W.G.; Banka, S. A comparative analysis of KMT2D missense variants in Kabuki syndrome, cancers and the general population. J. Hum. Genet. 2018, 64, 161–170. [Google Scholar] [CrossRef]
- Banka, S.; Veeramachaneni, R.; Reardon, W.; Howard, E.; Bunstone, S.; Ragge, N.; Parker, M.J.; Crow, Y.J.; Kerr, B.; Kingston, H.; et al. How genetically heterogeneous is Kabuki syndrome: MLL2 testing in 116 patients, review and analyses of mutation and phenotypic spectrum. Eur. J. Hum. Genet. 2012, 20, 381–388. [Google Scholar] [CrossRef]
- Yuan, S.M. Congenital heart defects in Kabuki syndrome. Cardiol. J. 2013, 20, 121–124. [Google Scholar] [CrossRef]
- Cheon, C.K.; Ko, J.M. Kabuki syndrome: Clinical and molecular characteristics. Korean J. Pediatr. 2015, 58, 317–324. [Google Scholar] [CrossRef]
- Hughes, H.E.; Davies, S.J. Coarctation of the aorta in kabuki syndrome. Arch. Dis. Child. 1994, 70, 512–514. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.K.; Ahn, K.J.; Kwon, B.S.; Kim, G.B.; Bae, E.J.; Noh, C.I.; Ko, J.M. The strong association of left-side heart anomalies with Kabuki syndrome. Korean J. Pediatr. 2015, 58, 256–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Digilio, M.C.; Baban, A.; Marino, B.; Dallapiccola, B. Hypoplastic left heart syndrome in patients with kabuki syndrome. Pediatr. Cardiol. 2010, 31, 1111–1113. [Google Scholar] [CrossRef] [PubMed]
- Adam, M. Insights into the molecular genetics of Kabuki syndrome. Adv. Genom. Genet. 2015, 5, 121–129. [Google Scholar] [CrossRef]
- Frenk, N.E.; Kim, C.A.; Carneiro-Sampaio, M.; Orii, N.M.; de Moraes Vasconcelos, D. Basic Evaluation of the immunocompetence of Brazilian patients with Kabuki syndrome. Pediatria 2009, 31, 170–177. [Google Scholar]
- Stagi, S.; Gulino, A.V.; Lapi, E.; Rigante, D. Epigenetic control of the immune system: A lesson from Kabuki syndrome. Immunol. Res. 2016, 64, 345–359. [Google Scholar] [CrossRef]
- Hostoffer, R.W.; Bay, C.A.; Wagner, K.; Venglarcik, I.J.; Sahara, H.; Omair, E.; Clark, H.T. Kabuki make-up syndrome associated with an acquired hypogammaglobulinemia and anti-IgA antibodies. Clin. Pediatr. 1996, 35, 273–276. [Google Scholar] [CrossRef]
- Lindsley, A.W.; Saal, H.M.; Burrow, T.A.; Hopkin, R.J.; Shchelochkov, O.; Khandelwal, P.; Xie, C.; Bleesing, J.; Filipovich, L.; Risma, K.; et al. Defects of B-cell terminal differentiation in patients with type-1 Kabuki syndrome. J. Allergy Clin. Immunol. 2016, 137, 179–187.e10. [Google Scholar] [CrossRef] [PubMed]
- Brackmann, F.; Krumbholz, M.; Langer, T.; Rascher, W.; Holter, W.; Metzler, M. Novel MLL2 mutation in Kabuki syndrome with hypogammaglobulinemia and severe chronic thrombopenia. J. Pediatr. Hematol. Oncol. 2013, 35, e314–e316. [Google Scholar] [CrossRef]
- Pham, M.N.; Byun, M.; Cunningham-Rundles, C. Kabuki syndrome another player on the immunodeficiency stage. J. Clin. Immunol. 2018, 38, 379–380. [Google Scholar] [CrossRef]
- Hoffman, J.D.; Ciprero, K.L.; Sullivan, K.E.; Kaplan, P.B.; McDonald-McGinn, D.M.; Zackai, E.H.; Ming, J.E. Immune abnormalities are a frequent manifestation of Kabuki syndrome. Am. J. Med. Genet. 2005, 135A, 278–281. [Google Scholar] [CrossRef] [PubMed]
- Margot, H.; Boursier, G.; Duflos, C.; Sanchez, E.; Amiel, J.; Andrau, J.C.; Arpin, S.; Brischoux-Boucher, E.; Boute, O.; Burglen, L.; et al. Immunopathological manifestations in Kabuki syndrome: A registry study of 177 individuals. Genet. Med. 2020, 22, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Tekin, M.; Fitoz, S.; Arici, S.; Cetinkaya, E.; Incesulu, A. Niikawa-Kuroki (Kabuki) syndrome with congenital sensorineural deafness: Evidence for a wide spectrum of inner ear abnormalities. Int. J. Pediatr. Otorhinolaryngol. 2006, 70, 885–889. [Google Scholar] [CrossRef] [PubMed]
- Ming, J.E.; Russell, K.L.; McDonald-McGinn, D.M.; Zackai, E.H. Autoimmune disorders in Kabuki syndrome. Am. J. Med. Genet. 2005, 132A, 260–262. [Google Scholar] [CrossRef]
- Almecija, A.C.; Perez, V.; Baro, M.; Guerra-Garcia, P.; Vivanco, J.L. Atypical Autoimmune Hematologic Disorders in a Patient With Kabuki Syndrome. J. Pediatr. Hematol. Oncol. 2019, 41, e114–e115. [Google Scholar] [CrossRef]
- Zannolli, R.; Buoni, S.; Macucci, F.; Scarinci, R.; Viviano, M.; Orsi, A.; de Aloe, G.; Fimiani, M.; Volterrani, L.; de Santi, M.M.; et al. Kabuki syndrome with trichrome vitiligo, ectodermal defect and hypogammaglobulinemia A and G. Brain Dev. 2007, 29, 373–376. [Google Scholar] [CrossRef]
- Gurbuz, F.; Ozalp Yuregir, O.; Ceylaner, S.; Topaloglu, A.K.; Yuksel, B. Coexistence of Kabuki Syndrome and Autoimmune Thyroiditis. J. Clin. Res. Pediatr. Endocrinol. 2016, 8, 105–106. [Google Scholar] [CrossRef]
- Wilson, G.N. Thirteen cases of Niikawa-Kuroki syndrome: Report and review with emphasis on medical complications and preventive management. Am. J. Med. Genet. 1998, 79, 112–120. [Google Scholar] [CrossRef]
- Fujishiro, M.; Ogihara, T.; Tsukuda, K.; Shojima, N.; Fukushima, Y.; Kimura, S.; Oka, Y.; Asano, T. A case showing an association between type 1 diabetes mellitus and Kabuki syndrome. Diabetes Res. Clin. Pract. 2003, 60, 25–31. [Google Scholar] [CrossRef]
- Dunn, N.; Katial, R.; Stitt, J. A patient with kabuki (niikawa-kuroki) syndrome, common variable immunodeficiency and immune-mediated neutropenia found to have a novel mutation in the KTM2D Gene. J. Allergy Clin. Immunol. 2016, 137, AB117. [Google Scholar] [CrossRef]
- Nishizaki, N.; Fujinaga, S.; Hirano, D.; Murakami, H.; Kamei, K.; Ohtomo, Y.; Shimizu, T.; Kaneko, K. Membranoproliferative glomerulonephritis Type 3 associated with Kabuki syndrome. Clin. Nephrol. 2014, 81, 369–373. [Google Scholar] [CrossRef]
- Liblau, R.S.; Caillat-Zucman, S.; Fischer, A.M.; Bach, J.F.; Boitard, C. The prevalence of selective IgA deficiency in type 1 diabetes mellitus. J. Pathol. Microbiol. Immunol. 1992, 100, 709–712. [Google Scholar] [CrossRef]
- Smith, W.I., Jr.; Rabin, B.S.; Huellmantel, A.; Thiel, D.H.V.; Drash, A. Immunopathology of juvenile-onset diabetes mellitus: IgA deficiency and juvenile diabetes. Diabetes 1978, 27, 1092–1097. [Google Scholar] [CrossRef] [PubMed]
- Ho, J.; Fox, D.; Innes, A.M.; McLeod, R.; Butzner, D.; Johnson, N.; Trevenen, C.; Kendrick, V.; Cole, D.E.C. Kabuki syndrome and Crohn disease in a child with familial hypocalciuric hypercalcemia. J. Pediatr. Endocrinol. Metab. 2010, 23, 975–979. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.; Bogucki, B.; Mavers, M.; deMello, D.E.; Knutsen, A. Cardiac conduction abnormalities and congenital immunodeficiency in a child with Kabuki syndrome: Case report. BMC Med. Genet. 2005, 6, 28. [Google Scholar] [CrossRef]
- Dentici, M.; Barresi, S.; Niceta, M.; Pantaleoni, F.; Pizzi, S.; Dallapiccola, B.; Tartaglia, M.; Digilio, M. Clinical spectrum of Kabuki-like syndrome caused by HNRNPK haploinsufficiency. Case report and literature review. Eur. J. Hum. Genet. 2019, 26, 477. [Google Scholar] [CrossRef]
- Wright, A.; Hall, A.; Daly, T.; Fontelonga, T.; Potter, S.; Schafer, C.; Lindsley, A.; Hung, C.; Bodamer, O.; Gussoni, E. Lysine methyltransferase 2D regulates muscle fiber size and muscle cell differentiation. FASEB J. 2021, 35, e21955. [Google Scholar] [CrossRef] [PubMed]
- Morgan, A.T.; Mei, C.; Da Costa, A.; Fifer, J.; Lederer, D.; Benoit, V.; McMillin, M.J.; Buckingham, K.J.; Bamshad, M.J.; Pope, K.; et al. Speech and language in a genotyped cohort of individuals with Kabuki syndrome. Am. J. Med. Genet. Part A 2015, 167, 1483–1492. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Raynor, E.M.; Lee, J.W.; Smith, S.L.; Heet, H.; Garrison, D.; Wrigley, J.; Kaylie, D.M.; Riska, K.M. Vestibular dysfunction and gross motor milestone acquisition in children with hearing loss: A systemic review. Otolaryngol.-Head Neck Surg. 2021, 165, 493–506. [Google Scholar] [CrossRef]
- Kurahashi, N.; Miyake, N.; Mizuno, S.; Koshimizu, E.; Kurahashi, H.; Yamada, K.; Natsume, J.; Aoki, Y.; Nakamura, M.; Taniai, H.; et al. Characteristics of epilepsy in patients with Kabuki syndrome with KMT2D mutations. Brain Dev. 2017, 39, 672–677. [Google Scholar] [CrossRef]
- Verrotti, A.; Agostinelli, S.; Cirillo, C.; D’Egidio, C.; Mohn, A.; Boncimino, A.; Coppola, G.; Spalice, A.; Nicita, F.; Pavone, P.; et al. Long-term outcome of epilepsy in Kabuki syndrome. Seizure 2011, 20, 650–654. [Google Scholar] [CrossRef]
- Anzai, M.; Terashima, H.; Kumagai, T.; Takenaka, S.; Kasai, M.; Watanabe, S.; Kubota, M.; Kozaki, R. A Kabuki syndrome patient with late onset West syndrome and intractable epilepsy. No To Hattatsu 2015, 47, S392. (In Japanese) [Google Scholar]
- Grunseich, C.; Fishbein, T.M.; Berkowitz, F.; Shamim, E.A. Tremor and Deep Brain Nuclei Hyperintensities in Kabuki Syndrome. Pediatr. Neurol. 2010, 43, 148–150. [Google Scholar] [CrossRef]
- Di Gennaro, G.; Condoluci, C.; Casali, C.; Ciccarelli, O.; Albertini, G. Epilepsy and polymicrogyria in Kabuki make-up (Niikawa-Kuroki) syndrome. Pediatr. Neurol. 1999, 21, 566–568. [Google Scholar] [CrossRef]
- Yoshioka, S.; Takano, T.; Matsuwake, K.; Sokoda, T.; Takeuchi, Y. A Japanese patient with Kabuki syndrome and unilateral perisylvian cortical dysplasia. Brain Dev. 2011, 33, 174–176. [Google Scholar] [CrossRef]
- Lodi, M.; Chifari, R.; Parazzini, C.; Viri, M.; Beccaria, F.; Lorenzetti, M.E.; Meloni, M.; Capovilla, G.; Romeo, A. Seizures and EEG pattern in Kabuki syndrome. Brain Dev. 2010, 32, 829–834. [Google Scholar] [CrossRef]
- Oksanen, V.E.; Arvio, M.A.; Peippo, M.M.; Valanne, L.K.; Sainio, K.O. Temporo-occipital spikes: A typical EEG finding in Kabuki syndrome. Pediatr. Neurol. 2004, 30, 67–70. [Google Scholar] [CrossRef]
- Topcu, Y.; Bayram, E.; Karaoglu, P.; Yis, U.; Kurul, S.H. Kabuki syndrome and perisylvian cortical dysplasia in a Turkish girl. J. Pediatr. Neurosci. 2013, 8, 259–260. [Google Scholar] [CrossRef] [PubMed]
- Daly, T.; Roberts, A.; Yang, E.; Mochida, G.H.; Bodamer, O. Holoprosencephaly in Kabuki syndrome. Am. J. Med. Genet. Part A 2020, 182, 441–445. [Google Scholar] [CrossRef]
- Dhar, S.S.; Lee, M.G. Cancer-epigenetic function of the histone methyltransferase KMT2D and therapeutic opportunities for the treatment of KMT2D-deficient tumors. Oncotarget 2021, 12, 1296–1308. [Google Scholar] [CrossRef]
- Scala, M.; Morana, G.; Sementa, A.R.; Merla, G.; Piatelli, G.; Capra, V.; Pavanello, M. Aggressive desmoid fibromatosis in Kabuki syndrome: Expanding the tumor spectrum. Pediatr. Blood Cancer 2019, 66, e27831. [Google Scholar] [CrossRef]
- Teranishi, H.; Koga, Y.; Nakashima, K.; Morihana, E.; Ishii, K.; Sakai, Y.; Taguchi, T.; Oda, Y.; Miyake, N.; Matsumoto, N.; et al. Cancer Management in Kabuki Syndrome: The First Case of Wilms Tumor and a Literature Review. J. Pediatr. Hematol. Oncol. 2018, 40, 391–394. [Google Scholar] [CrossRef]
- Tumino, M.; Licciardello, M.; Sorge, G.; Cutrupi, M.C.; Di Benedetto, F.; Amoroso, L.; Catania, R.; Pennisi, M.; D’Amico, S.; Di Cataldo, A. Kabuki syndrome and cancer in two patients. Am. J. Med. Genet. Part A 2010, 152A, 1536–1539. [Google Scholar] [CrossRef] [PubMed]
- Shahdadpuri, R.; O’Meara, A.; O’Sullivan, M.; Reardon, W. Low-grade fibromyxoid sarcoma: Yet another malignancy associated with Kabuki syndrome. Clin. Dysmorphol. 2008, 17, 199–202. [Google Scholar] [CrossRef] [PubMed]
- Casanova, M.; Selicorni, A.; Ferrari, A. Cancer predisposition in children with Kabuki syndrome. Am. J. Med. Genet. Part A 2011, 155, 1504. [Google Scholar] [CrossRef] [PubMed]
- Timothy, L.D.; Lehrke, H.D.; Chandan, V.S.; Kolbe, A.B.; Furuya, K.N. Diffuse Adenomatosis and Hepatocellular Carcinoma Treated with Liver Transplantation in an Adolescent Female with Kabuki Syndrome with a Novel KMT2D Gene Mutation. Case Rep. Pediatr. 2019, 2019, 7983824. [Google Scholar] [CrossRef]
- Karagianni, P.; Lambropoulos, V.; Stergidou, D.; Fryssira, H.; Chatziioannidis, I.; Spyridakis, I. Recurrent giant cell fibroblastoma: Malignancy predisposition in Kabuki syndrome revisited. Am. J. Med. Genet. Part A 2016, 170, 1333–1338. [Google Scholar] [CrossRef]
- Roma, D.; Palma, P.; Capolino, R.; Figà-Talamanca, L.; Diomedi-Camassei, F.; Lepri, F.R.; Digilio, M.C.; Marras, C.E.; Messina, R.; Carai, A.; et al. Spinal ependymoma in a patient with Kabuki syndrome: A case report. BMC Med. Genet. 2015, 16, 80. [Google Scholar] [CrossRef]
- Kaiwar, C.; Kruisselbrink, T.M.; Kudva, Y.C.; Klee, E.W.; Pichurin, P. Exome sequencing confirms diagnosis of kabuki syndrome in an-adult with hodgkin lymphoma and unusually severe multisystem phenotype. Clin. Immunol. 2019, 207, 55–57. [Google Scholar] [CrossRef]
- Scherer, S.; Theile, U.; Beyer, V.; Ferrari, R.; Kreck, C.; Rister, M. Patient with Kabuki syndrome and acute leukemia. Am. J. Med. Genet. 2003, 122A, 76–79. [Google Scholar] [CrossRef]
- Ijichi, O.; Kawakami, K.; Matsuda, Y.; Ikarimoto, N.; Miyata, K.; Takamatsu, H.; Tokunaga, M. A case of kabuki make-up syndrome with EBV + Burkitt’s lymphoma. Acta Paediatr. Jpn. Overs. Ed. 1996, 38, 66–68. [Google Scholar] [CrossRef]
- de Billy, E.; Strocchio, L.; Cacchione, A.; Agolini, E.; Gnazzo, M.; Novelli, A.; De Vito, R.; Capolino, R.; Digilio, M.C.; Caruso, R.; et al. Burkitt lymphoma in a patient with Kabuki syndrome carrying a novel KMT2D mutation. Am. J. Med. Genet. Part A 2019, 179, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Berger, F.; Delecluse, H.J. Lymphomas in immunocompromised hosts. Rev Prat 1993, 43, 1661–1664. [Google Scholar]
- Chrzanowska, K.H.; Krajewska-Walasek, M.; Kuś, J.; Michałkiewicz, J.; Maziarka, D.; Wolski, J.K.; Brecevic, L.; Madaliński, K. Kabuki (Niikawa-Kuroki) syndrome associated with immunodeficiency. Clin. Genet. 1998, 53, 308–312. [Google Scholar] [CrossRef]
- Hamahata, A.; Kamei, W.; Ishikawa, M.; Konoeda, H.; Yamaki, T.; Sakurai, H. Multiple pilomatricomas in Kabuki syndrome. Pediatr. Dermatol. 2013, 30, 253–255. [Google Scholar] [CrossRef]
- Bernier, F.-E.; Schreiber, A.; Coulombe, J.; Hatami, A.; Marcoux, D. Pilomatricoma Associated with Kabuki Syndrome. Pediatr. Dermatol. 2017, 34, e26–e27. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, L.; El Moneim, A.A.; Aleck, K.; Aughton, D.J.; Baumann, C.; Braddock, S.R.; Gillessen-Kaesbach, G.; Graham, J.M., Jr.; Grebe, T.A.; Gripp, K.W.; et al. Further delineation of Kabuki syndrome in 48 well-defined new individuals. Am. J. Med. Genet. 2005, 132A, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Schrander-Stumpel, C.T.R.M.; Spruyt, L.; Curfs, L.M.G.; Defloor, T.; Schrander, J.J.P. Kabuki syndrome: Clinical data in 20 patients, literature review, and further guidelines for preventive management. Am. J. Med. Genet. 2005, 132A, 234–243. [Google Scholar] [CrossRef]
- Kawame, H.; Hannibal, M.C.; Hudgins, L.; Pagon, R.A. Phenotypic spectrum and management issues in Kabuki syndrome. J. Pediatr. 1999, 134, 480–485. [Google Scholar] [CrossRef]
- Gole, H.; Chuk, R.; Coman, D. Persistent hyperinsulinism in kabuki syndrome 2: Case report and literature review. Clin. Pract. 2016, 6, 68–70. [Google Scholar] [CrossRef]
- Gibson, C.E.; Boodhansingh, K.E.; Li, C.; Conlin, L.; Chen, P.; Becker, S.A.; Bhatti, T.; Bamba, V.; Adzick, N.S.; De Leon, D.D.; et al. Congenital Hyperinsulinism in Infants with Turner Syndrome: Possible Association with Monosomy X and KDM6A Haploinsufficiency. Horm. Res. Paediatr. 2018, 89, 413–422. [Google Scholar] [CrossRef]
- Tawa, R.; Kaino, Y.; Ito, T.; Goto, Y.; Kida, K.; Matsuda, H. A case of Kabuki make-up syndrome with central diabetes insipidus and growth hormone neurosecretory dysfunction. Acta Paediatr. Jpn. Overseas Ed. 1994, 36, 412–415. [Google Scholar] [CrossRef] [PubMed]
- Ito, N.; Ihara, K.; Tsutsumi, Y.; Miyake, N.; Matsumoto, N.; Hara, T. Hypothalamic pituitary complications in Kabuki syndrome. Pituitary 2013, 16, 133–138. [Google Scholar] [CrossRef] [PubMed]
- So, P.L.; Luk, H.M.; Yu, K.P.T.; Cheng, S.S.W.; Hau, E.W.L.; Ho, S.K.L.; Lam, S.T.S.; Lo, I.F.M. Clinical and molecular characterization study of Chinese Kabuki syndrome in Hong Kong. Am. J. Med. Genet. Part A 2020, 185, 675–686. [Google Scholar] [CrossRef]
- Banka, S.; Howard, E.; Bunstone, S.; Chandler, K.E.; Kerr, B.; Lachlan, K.; McKee, S.; Mehta, S.G.; Tavares, A.L.T.; Tolmie, J.; et al. MLL2 mosaic mutations and intragenic deletion-duplications in patients with Kabuki syndrome. Clin. Genet. 2013, 83, 467–471. [Google Scholar] [CrossRef]
- Courcet, J.B.; Faivre, L.; Michot, C.; Burguet, A.; Perez-Martin, S.; Alix, E.; Amiel, J.; Baumann, C.; Cordier, M.P.; Cormier-Daire, V.; et al. Clinical and molecular spectrum of renal malformations in kabuki syndrome. J. Pediatr. 2013, 163, 742–746. [Google Scholar] [CrossRef]
- Çetinkaya, E.; Misirhoǧlu, E.D.; Vidinlisan, S.; Baydar, Z.; Özhan, Z.R. Hypospadias in a patient with Kabuki make-up (Niikawa-Kuroki) syndrome. J. Pediatr. Endocrinol. Metab. 2001, 14, 803–805. [Google Scholar] [CrossRef]
- Shawky, R.M.; Gamal, R.; Mostafa, N. Kabuki make-up syndrome with genitourinary anomalies, ophthalmologic features and hyperpigmentation in an Egyptian child. Egypt. J. Med. Hum. Genet. 2017, 18, 87–92. [Google Scholar] [CrossRef]
- Wang, L.C.; Chiu, I.S.; Wang, P.J.; Wu, M.H.; Wang, J.K.; Hung, Y.B.; Lin, S.J. Kabuki make-up syndrome associated with congenital heart disease. Zhonghua Min Guo Xiao Er Ke Yi Xue Hui Za Zhi 1994, 35, 63–69. [Google Scholar] [PubMed]
- Kerr, B.; Murphy, P.; Quinn, J. Refractory ITP in a patient with Kabuki syndrome: Response to low-dose rituximab. Int. J. Hematol. 2017, 105, 702–703. [Google Scholar] [CrossRef]
- Ewart-Toland, A.; Enns, G.M.; Cox, V.A.; Mohan, G.C.; Rosenthal, P.; Golabi, M. Severe congenital anomalies requiring transplantation in children with Kabuki syndrome. Am. J. Med. Genet. 1998, 80, 362–367. [Google Scholar] [CrossRef]
- Hamdi Kamel, M.; Gilmartin, B.; Mohan, P.; Hickey, D.P. Successful long-term outcome of kidney transplantation in a child with Kabuki syndrome. Pediatr. Transplant. 2006, 10, 105–107. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Bögershausen, N.; Alanay, Y.; Simsek Kiper, P.O.; Plume, N.; Keupp, K.; Pohl, E.; Pawlik, B.; Rachwalski, M.; Milz, E.; et al. A mutation screen in patients with Kabuki syndrome. Hum. Genet. 2011, 130, 715–724. [Google Scholar] [CrossRef] [PubMed]
- Kluijt, I.; Van Dorp, D.B.; Kwee, M.L.; Toutain, A.; Keppler-Noreuil, K.; Warburg, M.; Bitoun, P. Kabuki syndrome—Report of six cases and review of the literature with emphasis on ocular features. Ophthalmic Genet. 2000, 21, 51–61. [Google Scholar] [CrossRef]
- Cheon, C.K.; Choi, H.Y.; Park, S.H.; Jung, J.H.; Kim, S.J. Ocular manifestations in kabuki syndrome: A report of 10 cases and literature review. Ophthalmic Genet. 2020, 42, 101–104. [Google Scholar] [CrossRef]
- Wessels, M.W.; Brooks, A.S.; Hoogeboom, J.; Niermeijer, M.F.; Willems, P.J. Kabuki syndrome: A review study of three hundred patients. Clin. Dysmorph. 2002, 11, 95–102. [Google Scholar] [CrossRef]
- Rosenberg, C.E.; Daly, T.; Hung, C.; Hsueh, I.; Lindsley, A.W.; Bodamer, O. Prenatal and perinatal history in Kabuki Syndrome. Am. J. Med. Genet. Part A 2020, 182, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Dentici, M.L.; Di Pede, A.; Lepri, F.R.; Gnazzo, M.; Lombardi, M.H.; Auriti, C.; Petrocchi, S.; Pisaneschi, E.; Bellacchio, E.; Capolino, R.; et al. Kabuki syndrome: Clinical and molecular diagnosis in the first year of life. Arch. Dis. Child. 2015, 100, 158–164. [Google Scholar] [CrossRef]
- Vaux, K.K.; Jones, K.L.; Jones, M.C.; Schelley, S.; Hudgins, L. Developmental outcome in Kabuki syndrome. Am. J. Med. Genet. 2005, 132A, 263–264. [Google Scholar] [CrossRef] [PubMed]
- Dorleijn, D.M.; Cohen-Overbeek, T.E.; Groenendaal, F.; Bruinse, H.W.; Stoutenbeek, P. Idiopathic polyhdranmios and postnatal findings. J. Matern. Fetal. Neonatal. Med. 2009, 22, 315–320. [Google Scholar] [CrossRef]
- Magann, E.F.; Chauhan, S.P.; Doherty, D.A.; Lutgendorf, M.A.; Magann, M.I.; Morrison, J.C. A review of idiopathic hydramnios and pregnancy outcomes. Obstet. Gynecol. Surv. 2007, 62, 795–802. [Google Scholar] [CrossRef] [PubMed]
- Schott, D.A.; Blok, M.J.; Gerver, W.J.M.; Devriendt, K.; Zimmermann, L.J.I.; Stumpel, C.T.R.M. Growth pattern in Kabuki syndrome with a KMT2D mutation. Am. J. Med. Genet. Part A 2016, 170, 3172–3179. [Google Scholar] [CrossRef] [PubMed]
- Schott, D.A.; Gerver, W.J.M.; Stumpel, C.T.R.M. Growth Hormone Therapy in Children with Kabuki Syndrome: 1-year Treatment Results. Horm. Res. Paediatr. 2017, 88, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Schott, D.A.; Stumpel, C.T.R.M.; Klaassens, M. Hypermobility in individuals with Kabuki syndrome: The effect of growth hormone treatment. Am. J. Med. Genet. Part A 2019, 179, 219–223. [Google Scholar] [CrossRef] [PubMed]
- van Montfort, L.; Gerver, W.J.M.; Kooger, B.L.S.; Plat, J.; Bierau, J.; Stumpel, C.; Schott, D.A. Follow-Up Study of Growth Hormone Therapy in Children with Kabuki Syndrome: Two-Year Treatment Results. Horm. Res. Paediatr. 2021, 94, 285–296. [Google Scholar] [CrossRef]
- Schott, D.A.; Gerver, W.J.M.; Stumpel, C.T.R.M. Growth Hormone Stimulation Tests in Children with Kabuki Syndrome. Horm. Res. Paediatr. 2016, 86, 319–324. [Google Scholar] [CrossRef] [PubMed]
- Ruault, V.; Corsini, C.; Duflos, C.; Akouete, S.; Georgescu, V.; Abaji, M.; Alembick, Y.; Alix, E.; Amiel, J.; Amouroux, C.; et al. Growth charts in Kabuki syndrome 1. Am. J. Med. Genet. Part A 2020, 182, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Kurosawa, K.; Kawame, H.; Ochiai, Y.; Nakashima, M.; Tohma, T.; Ohashi, H. Patellar dislocation in Kabuki syndrome. Am. J. Med. Genet. 2002, 108, 160–163. [Google Scholar] [CrossRef] [PubMed]
- Weir, R.A.; Alston, A.F.; Ali, M.A. Acute myocardial infarction in Kabuki syndrome: Chance occurrence or a novel risk factor for premature atherosclerosis? Int. J. Cardiol. 2014, 176, e26–e28. [Google Scholar] [CrossRef] [PubMed]
- Mervis, C.B.; Becerra, A.M.; Rowe, M.L.; Hersh, J.H.; Morris, C.A. Intellectual abilities and adaptive behavior of children and adolescents with Kabuki syndrome: A preliminary study. Am. J. Med. Genet. 2005, 132A, 248–255. [Google Scholar] [CrossRef]
- Toutain, A.; Plée, Y.; Ployet, M.J.; Benoit, S.; Perrot, A.; Sembely, C.; Barthez, M.A.; Moraine, C. Deafness and Mondini dysplasia in Kabuki (Niikawa-Kuroki) Syndrome. Report of a case and review of the literature. Genet. Couns. 1997, 8, 99–105. [Google Scholar] [PubMed]
- Van Lierde, K.M.; Van Borsel, J.; Van Cauwenberge, P. Speech patterns in Kabuki make-up syndrome: A case report. J. Commun. Disord. 2000, 33, 447–462. [Google Scholar] [CrossRef]
- Burke, L.W.; Jones, M.C. Kabuki syndrome: Underdiagnosed recognizable pattern in cleft palate patients. Cleft Palate-Craniofac. J. 1995, 32, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Lindgren, A.M.; Hoyos, T.; Talkowski, M.E.; Hanscom, C.; Blumenthal, I.; Chiang, C.; Ernst, C.; Pereira, S.; Ordulu, Z.; Clericuzio, C.; et al. Haploinsufficiency of KDM6A is associated with severe psychomotor retardation, global growth restriction, seizures and cleft palate. Hum. Genet. 2013, 132, 537–552. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Mo, G.; Ling, Y.; Ji, L. A novel KMT2D mutation resulting in Kabuki syndrome: A case report. Mol. Med. Rep. 2016, 14, 3641–3645. [Google Scholar] [CrossRef] [Green Version]
- Petzold, D.; Kratzsch, E.; Opitz, C.; Tinschert, S. The Kabuki syndrome: Four patients with oral abnormalities. Eur. J. Orthod. 2003, 25, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Miyake, N.; Mizuno, S.; Okamoto, N.; Ohashi, H.; Shiina, M.; Ogata, K.; Tsurusaki, Y.; Nakashima, M.; Saitsu, H.; Niikawa, N.; et al. KDM6A Point Mutations Cause Kabuki Syndrome. Hum. Mutat. 2013, 34, 108–110. [Google Scholar] [CrossRef] [PubMed]
- Ho, H.H.; Eaves, L.C. Kabuki make-up (Niikawa-Kuroki) syndrome: Cognitive abilities and autistic features. Dev. Med. Child Neurol. 1997, 39, 487–490. [Google Scholar] [CrossRef] [PubMed]
- Bayar Muluk, N.; Yalçinkaya, F.; Budak, B.; Gündüz, S.; Ayas, K. Evaluation for language and speech development in Kabuki make-up syndrome: A case report. Int. J. Pediatr. Otorhinolaryngol. 2009, 73, 1837–1840. [Google Scholar] [CrossRef]
- Association, A.P. Diagnostic and Statistical Manual of Mental Health Disorders, 5th ed.; American Psychologial Association: Washington, DC, USA, 2013; pp. 33–41. [Google Scholar]
- Lehman, N.; Mazery, A.C.; Visier, A.; Baumann, C.; Lachesnais, D.; Capri, Y.; Toutain, A.; Odent, S.; Mikaty, M.; Goizet, C.; et al. Molecular, clinical and neuropsychological study in 31 patients with Kabuki syndrome and KMT2D mutations. Clin. Genet. 2017, 92, 298–305. [Google Scholar] [CrossRef]
- Paulussen, A.D.C.; Stegmann, A.P.A.; Blok, M.J.; Tserpelis, D.; Posma-Velter, C.; Detisch, Y.; Smeets, E.E.J.G.L.; Wagemans, A.; Schrander, J.J.P.; Van Den Boogaard, M.J.H.; et al. MLL2 mutation spectrum in 45 patients with Kabuki syndrome. Hum. Mutat. 2011, 32, E2018–E2025. [Google Scholar] [CrossRef] [PubMed]
- Kasdon, B.D.; Fox, J.E. Kabuki syndrome: Diagnostic and treatment considerations. Ment. Health Fam. Med. 2012, 9, 171–179. [Google Scholar] [PubMed]
- Porntaveetus, T.; Abid, M.F.; Theerapanon, T.; Srichomthong, C.; Ohazama, A.; Kawasaki, K.; Kawasaki, M.; Suphapeetiporn, K.; Sharpe, P.T.; Shotelersuk, V. Expanding the oro-dental and mutational spectra of Kabuki Syndrome with expression of KMT2D and KDM6A in human tooth germs. Int. J. Biol. Sci. 2018, 14, 381–389. [Google Scholar] [CrossRef]
- Xin, C.; Wang, C.; Wang, Y.; Zhao, J.; Wang, L.; Li, R.; Liu, J. Identification of novel KMT2D mutations in two Chinese children with Kabuki syndrome: A case report and systematic literature review. BMC Med. Genet. 2018, 19, 31. [Google Scholar] [CrossRef] [PubMed]
- Miyake, N.; Koshimizu, E.; Okamoto, N.; Mizuno, S.; Ogata, T.; Nagai, T.; Kosho, T.; Ohashi, H.; Kato, M.; Sasaki, G.; et al. MLL2 and KDM6A mutations in patients with Kabuki syndrome. Am. J. Med. Genet. Part A 2013, 161, 2234–2243. [Google Scholar] [CrossRef]
- van Dongen, L.C.M.; Wingbermuhle, P.A.M.; van der Veld, W.M.; Stumpel, C.; Kleefstra, T.; Egger, J.I.M. Exploring the cognitive phenotype of Kabuki (Niikawa-Kuroki) syndrome. J. Intellect. Disabil. Res. JIDR 2019, 63, 498–506. [Google Scholar] [CrossRef]
- Theodore-Oklota, C.; Hartman, D.S.; Hoffman, D.L.; Björnsson, H.T. A Qualitative Study to Characterize the Humanistic Burden of Kabuki Syndrome in the United States and Canada. Adv. Ther. 2022, 39, 619–631. [Google Scholar] [CrossRef]
- Malik, P.; Sharma, A.; Sakhuja, S.; Munjal, S.; Panda, N.K. Speech and language characteristics in Kabuki Syndrome. Internet J. Allied Health Sci. Pract. 2010, 8, 12. [Google Scholar] [CrossRef]
- Upton, S.; Stadter, C.S.; Landis, P.; Wulfsberg, E.A. Speech characteristics in the Kabuki syndrome. Am. J. Med. Genet. 2003, 116A, 338–341. [Google Scholar] [CrossRef]
- Ilyina, H.; Lurie, I.; Naumtchik, I.; Amoashy, D.; Stephanenko, G.; Fedotov, V.; Kostjuk, A. Kabuki make-up (Niikawa-Kuroki) syndrome in the Byelorussian register of congenital malformations: Ten new observations. Am. J. Med. Genet. 1995, 56, 127–131. [Google Scholar] [CrossRef]
- Defloor, T.; Van Borsel, J.; Schrander-Stumpel, C.T.R.M.; Curfs, L.M.G. Expressive language in children with Kabuki syndrome. Am. J. Med. Genet. 2005, 132A, 256–259. [Google Scholar] [CrossRef]
- Sertçelik, M.; Uğur, Ç.; Şahin Aközel, A.; Gürkan, C.K. A child with kabuki syndrome and autism spectrum disorder. Noropsikiyatr. Ars. 2016, 53, 280–282. [Google Scholar] [CrossRef] [PubMed]
- Lai, K.V.; Nussbaum, E.; Do, P.; Chen, J.; Randhawa, I.S.; Chin, T. Congenital lung anomalies in kabuki syndrome. J. Pediatr. Cong. Disord. 2014, 104, 1–5. [Google Scholar]
- Matsumoto, N.; Niikawa, N. Kabuki make-up syndrome: A review. Am. J. Med. Genet. Semin. Med. Genet. 2003, 117C, 57–65. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Evolution of facial features of a patient with a pathogenic variant in KMT2D at 6 months (A), 12 months (B), 3 years (C), 5 years (D), 10 years (E), and 19 years (F). (Photos shown with permission of the patient and parents).
Figure 1.
Evolution of facial features of a patient with a pathogenic variant in KMT2D at 6 months (A), 12 months (B), 3 years (C), 5 years (D), 10 years (E), and 19 years (F). (Photos shown with permission of the patient and parents).


{kind=link}
Table 1.
Search terms, inclusion, and exclusion criteria.
| Search Terms | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
|
|
|
KS = Kabuki syndrome.
Table 2.
Recommended initial evaluation by organ system.
| System 1 | Evaluation | Comment |
|---|---|---|
| Growth | Measurement of height, weight, and head circumference | While infants may have FTT, adolescents and adults may have obesity. KS-specific growth charts available |
| Ophthalmologic | Ophthalmology evaluation | For assessment of strabismus, refractive error, ptosis, and corneal abnormalities |
| Hearing | Baseline audiology evaluation | To assess for conductive and/or sensorineural hearing loss |
| Mouth | Directed evaluation of the palate for palatal anomalies | Consider referral to a craniofacial specialist if palatal anomalies are suspected |
| Consider dental evaluation for those over 3 years of age | ||
| Cardiac | Echocardiogram with visualization of the aortic arch | To assess for congenital heart defects, including coarctation of the aorta |
| Consider EKG | If arrhythmia is suspected | |
| Respiratory | Consider chest radiographs to assess for diaphragmatic eventuation | In those with respiratory issues, chronic cough, or recurrent pneumonia |
| Gastrointestinal/Feeding | Asses nutritional status, feeding, GERD | Consider assessment by a feeding team and/or a VFSS for those with suspected dysphagia |
| Genitourinary | Baseline renal ultrasound | To evaluate for renal anomalies and hydronephrosis |
| Physical examination for hypospadias and/or cryptorchidism in males | ||
| Musculoskeletal | Consider radiographs of the spine in those with scoliosis | To assess for vertebral anomalies |
| Endocrinologic | Assessment for hyperinsulinism | In neonates and infants with persistent hypoglycemia |
| Assessment for hypothyroidism and growth hormone deficiency | In those with an abnormal growth velocity | |
| Immunologic | T cell count, T cell subsets, and serum immunoglobulin levels at the time of diagnosis or at age one year (whichever comes later) | Referral to immunology if immunological studies are abnormal or there is a history of recurrent infections |
| Neurologic | EEG | In those with suspected seizures |
| Brain MRI | To evaluate for a structural brain malformation in those with seizures | |
| To evaluate for Chiari I malformation in those with suggestive symptoms | ||
| Psychiatric/behavioral | Neuropsychiatric evaluation | To include screening for the presence of behavioral problems, including sleep disturbances, ADHD, anxiety, and/or traits suggestive of ASD for individuals age >12 months |
| Miscellaneous/Other | Developmental assessment | To include motor, speech/language evaluation, general cognitive, and vocational skills |
| Consultation with a clinical geneticist and/or genetic counselor | Medical home, care coordination, molecular diagnosis and counseling |
1 Adapted with permission from GeneReviews®; Adam MP, Hudgins L, Hannibal M. Kabuki Syndrome. 1 September 2011 [Updated 15 July 2021]. In: Adam MP, Ardinger HH, Pagon RA et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK62111/ (accessed on 29 April 2022). KS = Kabuki syndrome; FTT = failure to thrive; EKG = electrocardiogram; GERD = gastroesophageal reflux disease; VFSS = videofluoroscopic swallow study; EEG = electroencephalogram; MRI = magnetic resonance imaging; ADHD = attention-deficit/hyperactivity disorder; ASD = autism spectrum disorder.
Table 3.
Health surveillance by organ system.
| System 1 | Evaluation | Frequency |
|---|---|---|
| Growth | Measurement of at least height and weight | At each appointment |
| Ophthalmologic | Ophthalmology or optometry to assess vision | At least annually |
| Hearing | Hearing assessment | At least annually |
| Musculoskeletal | Clinical evaluation for scoliosis | At each appointment until skeletal maturity |
| Endocrinologic | Thyroid function tests | Every 2–3 years |
| Immunologic | Assessment of complete blood count, immunoglobulin levels, flow cytometry? | Every 2–3 years |
| Miscellaneous/Other | Monitor developmental progress and educational needs | At each visit during childhood and adolescence |
1 Adapted with permission from GeneReviews®; Adam MP, Hudgins L, Hannibal M. Kabuki Syndrome. 1 September 2011 [Updated 15 July 2021]. In: Adam MP, Ardinger HH, Pagon RA et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK62111/ (accessed on 29 April 2022).
Table 4.
Treatment of manifestations by indication.
| Manifestation 1 | Treatment | Considerations/Other |
|---|---|---|
| Strabismus, refractive error, ptosis, lagophthalmos | Standard treatment per Ophthalmology | |
| Hearing loss | Consideration of pressure equalizing tubes in those with conductive hearing loss | Referral to an ENT specialist and audiologist |
| Hearing aids may be considered for those with sensorineural hearing loss | ||
| Cleft lip and/or palate | Standard treatment | Management through a specialized Craniofacial clinic is ideal |
| The palate may be shorter, which can lead to velopharyngeal insufficiency after typical cleft repair | ||
| Dental anomalies | Orthodontic referral if hypodontia or significant malocclusion are noted | |
| Congenital heart defects and/or arrhythmia | Standard treatment per Cardiology | It is unclear whether there is an increased risk for aortic aneurysm; however, if catheterization or angioplasty is being considered, a potential increased risk of aortic aneurysm should be communicated to the treating team |
| Feeding difficulties/GERD | Standard treatment, which may include thickening feeds and appropriate positioning after meals in infants and toddlers | Pharmacologic treatment for GERD may be considered |
| Consideration of gastrostomy tube | In those with severe feeding difficulties and/or poorly coordinated suck and swallow | |
| Chronic diarrhea | Referral to a Gastroenterology specialist | Consider evaluation for malabsorption and/or celiac disease |
| Hypospadias/cryptorchidism | Standard treatment per Urology | |
| Hyperinsulinism and hypothyroidism | Standard treatment per Endocrinology | |
| Short stature | Consideration of growth hormone therapy | |
| Recurrent infections | Intravenous immunoglobulin (IVIG) therapy may be considered in those this documented immunoglobulin deficiency | Referral to Immunology |
| Seizure disorder | Standard antiepileptic treatment per Neurology | |
| Premature thelarche | No treatment is warranted if there are no other signs of premature puberty | |
| Need for anesthesia | Care in positioning during intubation due to joint laxity, which can affect the cervical spine | Education regarding potential structural airway anomalies that could make intubation difficult |
1 Adapted with permission from GeneReviews®; Adam MP, Hudgins L, Hannibal M. Kabuki Syndrome. 1 September 2011 [Updated 15 July 2021]. In: Adam MP, Ardinger HH, Pagon RA et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK62111/ (accessed on 1 September 2022).
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Barry, K.K.; Tsaparlis, M.; Hoffman, D.; Hartman, D.; Adam, M.P.; Hung, C.; Bodamer, O.A. From Genotype to Phenotype—A Review of Kabuki Syndrome. Genes 2022, 13, 1761. https://doi.org/10.3390/genes13101761
AMA Style
Barry KK, Tsaparlis M, Hoffman D, Hartman D, Adam MP, Hung C, Bodamer OA. From Genotype to Phenotype—A Review of Kabuki Syndrome. Genes. 2022; 13(10):1761. https://doi.org/10.3390/genes13101761
Chicago/Turabian StyleBarry, Kelly K., Michaelangelo Tsaparlis, Deborah Hoffman, Deborah Hartman, Margaret P. Adam, Christina Hung, and Olaf A. Bodamer. 2022. "From Genotype to Phenotype—A Review of Kabuki Syndrome" Genes 13, no. 10: 1761. https://doi.org/10.3390/genes13101761
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.