
The Role of ACE, ACE2, and AGTR2 Polymorphisms in COVID-19 Severity and the Presence of COVID-19-Related Retinopathy

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patient Selection, Inclusion, and Exclusion Criteria
2.3. Study Protocol
2.4. Image Analysis
2.5. Genotyping
2.6. Statistical Analysis
3. Results
3.1. Demographics and Clinical Characteristics
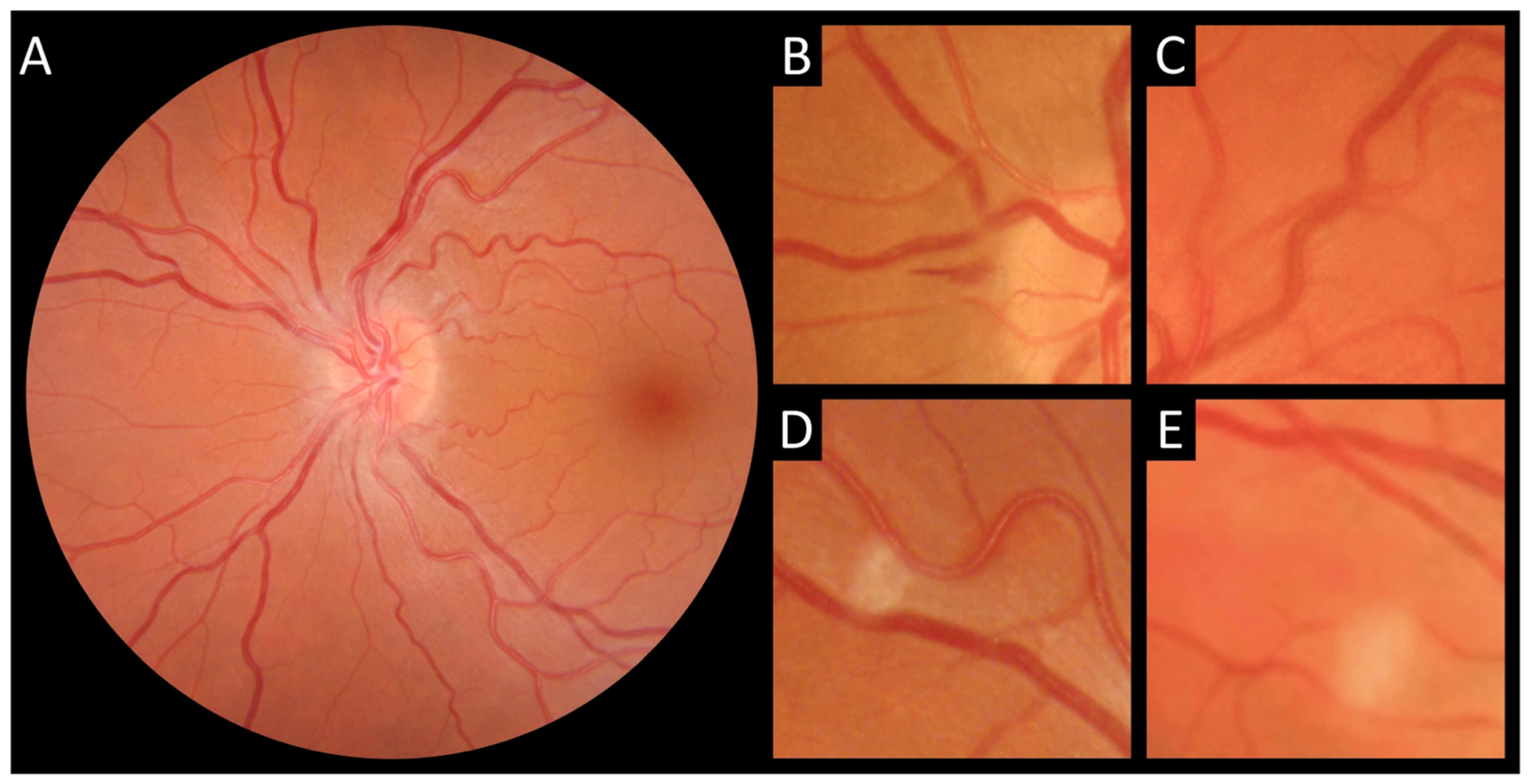
3.2. COVID-19 Retinopathy
3.3. Genotyping
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guan, W.-J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- de Figueiredo, C.S.; Raony, Í.; Giestal-de-Araujo, E. SARS-CoV-2 Targeting the Retina: Host–virus Interaction and Possible Mechanisms of Viral Tropism. Ocul. Immunol. Inflamm. 2020, 28, 1301–1304. [Google Scholar] [CrossRef] [PubMed]
- Collin, J.; Queen, R.; Zerti, D.; Dorgau, B.; Georgiou, M.; Djidrovski, I.; Hussain, R.; Coxhead, J.M.; Joseph, A.; Rooney, P.; et al. Co-expression of SARS-CoV-2 entry genes in the superficial adult human conjunctival, limbal and corneal epithelium suggests an additional route of entry via the ocular surface. Ocul. Surf. 2020, 19, 190–200. [Google Scholar] [CrossRef]
- Choudhary, R.; Kapoor, M.S.; Singh, A.; Bodakhe, S.H. Therapeutic targets of renin-angiotensin system in ocular disorders. J. Curr. Ophthalmol. 2017, 29, 7–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Almeida-Pititto, B.; Dualib, P.M.; Zajdenverg, L.; Dantas, J.R.; De Souza, F.D.; Rodacki, M.; Bertoluci, M.C. Severity and mortality of COVID 19 in patients with diabetes, hypertension and cardiovascular disease: A meta-analysis. Diabetol. Metab. Syndr. 2020, 12, 75. [Google Scholar] [CrossRef]
- Apicella, M.; Campopiano, M.C.; Mantuano, M.; Mazoni, L.; Coppelli, A.; Del Prato, S. COVID-19 in people with diabetes: Understanding the reasons for worse outcomes. Lancet Diabetes Endocrinol. 2020, 8, 782–792. [Google Scholar] [CrossRef]
- Callender, L.A.; Curran, M.; Bates, S.M.; Mairesse, M.; Weigandt, J.; Betts, C.J. The Impact of Pre-existing Comorbidities and Therapeutic Interventions on COVID-19. Front. Immunol. 2020, 11, 1991. [Google Scholar] [CrossRef]
- Cui, C.; Huang, C.; Zhou, W.; Ji, X.; Zhang, F.; Wang, L.; Zhou, Y.; Cui, Q. AGTR2, One Possible Novel Key Gene for the Entry of SARS-CoV-2 Into Human Cells. IEEE/ACM Trans. Comput. Biol. Bioinform. 2021, 18, 1230–1233. [Google Scholar] [CrossRef]
- Jevnikar, K.; Jaki Mekjavic, P.; Vidovic Valentincic, N.; Petrovski, G.; Globocnik Petrovic, M. An Update on COVID-19 Related Ophthalmic Manifestations. Ocul. Immunol. Inflamm. 2021, 29, 684–689. [Google Scholar] [CrossRef]
- Teo, K.Y.; Invernizzi, A.; Staurenghi, G.; Cheung, C.M.G. COVID-19 related retinal micro-vasculopathy—A review of current evidence: COVID-19 related retinal micro-vasculopathy. Am. J. Ophthalmol. 2022, 235, 98–110. [Google Scholar] [CrossRef] [PubMed]
- Wong, T.Y.; Islam, F.A.; Klein, R.; Klein, B.E.; Cotch, M.F.; Castro, C.; Sharrett, A.R.; Shahar, E. Retinal vascular caliber, cardiovascular risk factors, and inflammation: The multi-ethnic study of atherosclerosis (MESA). Investig. Ophthalmol. Vis. Sci. 2006, 47, 2341–2350. [Google Scholar] [CrossRef] [PubMed]
- Jaki Mekjavic, P.; Lenassi, E.; Eiken, O.; Mekjavic, I.B. Effect of acute hypercapnia during 10-day hypoxic bed rest on posterior eye structures. J. Appl. Physiol. 2016, 120, 1241–1248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, K.; Kim, E.S.; Yu, S.Y. Optical coherence tomography angiography analysis of foveal microvascular changes and inner retinal layer thinning in patients with diabetes. Br. J. Ophthalmol. 2018, 102, 1226–1231. [Google Scholar] [CrossRef]
- Matsushita, K.; Ding, N.; Kou, M.; Hu, X.; Chen, M.; Gao, Y.; Honda, Y.; Zhao, D.; Dowdy, D.; Mok, Y.; et al. The Relationship of COVID-19 Severity with Cardiovascular Disease and Its Traditional Risk Factors: A Systematic Review and Meta-Analysis. Glob. Heart 2020, 15, 64. [Google Scholar] [CrossRef]
- Bae, S.; Kim, S.R.; Kim, M.N.; Shim, W.J.; Park, S.M. Impact of cardiovascular disease and risk factors on fatal outcomes in patients with COVID-19 according to age: A systematic review and meta-analysis. Heart 2021, 107, 373–380. [Google Scholar] [CrossRef]
- Karakaş Çelik, S.; Çakmak Genç, G.; Pişkin, N.; Açikgöz, B.; Altinsoy, B.; Kurucu İşsiz, B.; Dursun, A. Polymorphisms of ACE (I/D) and ACE2 receptor gene (Rs2106809, Rs2285666) are not related to the clinical course of COVID-19: A case study. J. Med. Virol. 2021, 93, 5947–5952. [Google Scholar] [CrossRef]
- Zmorzynski, S.; Szudy-Szczyrek, A.; Popek-Marciniec, S.; Korszen-Pilecka, I.; Wojcierowska-Litwin, M.; Luterek, M.; Chocholska, S.; Styk, W.; Swiderska-Kołacz, G.; Januszewska, J.; et al. ACE Insertion/Deletion Polymorphism (rs4646994) Is Associated with the Increased Risk of Multiple Myeloma. Front. Oncol. 2019, 9, 44. [Google Scholar] [CrossRef] [Green Version]
- Calabrese, C.; Annunziata, A.; Coppola, A.; Pafundi, P.C.; Guarino, S.; Di Spirito, V.; Maddaloni, V.; Pepe, N.; Fiorentino, G. ACE Gene I/D Polymorphism and Acute Pulmonary Embolism in COVID19 Pneumonia: A Potential Predisposing Role. Front. Med. 2020, 7, 631148. [Google Scholar] [CrossRef]
- Möhlendick, B.; Schönfelder, K.; Breuckmann, K.; Elsner, C.; Babel, N.; Balfanz, P.; Dahl, E.; Dreher, M.; Fistera, D.; Herbstreit, F.; et al. ACE2 polymorphism and susceptibility for SARS-CoV-2 infection and severity of COVID-19. Pharm. Genom. 2021, 31, 165–171. [Google Scholar] [CrossRef]
- Mahmood, Z.S.; Fadhil, H.Y.; Hussein, T.A.A.; Ad’hiah, A.H. Severity of coronavirus disease 19: Profile of inflammatory markers and ACE (rs4646994) and ACE2 (rs2285666) gene polymorphisms in Iraqi patients. Meta Gene 2022, 31, 101014. [Google Scholar] [CrossRef] [PubMed]
- Gómez, J.; Albaiceta, G.M.; García-Clemente, M.; López-Larrea, C.; Amado-Rodríguez, L.; Lopez-Alonso, I.; Hermida, T.; Enriquez, A.I.; Herrero, P.; Melón, S.; et al. Angiotensin-converting enzymes (ACE, ACE2) gene variants and COVID-19 outcome. Gene 2020, 762, 145102. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.P.; Kuznetsova, T.; Thijs, L.; Jin, Y.; Schmitz, B.; Brand, S.M.; Brand, E.; Manunta, P.; Bianchi, G.; Struijker-Boudier, H.; et al. Are retinal microvascular phenotypes associated with the 1675G/A polymorphism in the angiotensin II type-2 receptor gene? Am. J. Hypertens. 2011, 24, 1300–1305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warnecke, C.; Mugrauer, P.; Sürder, D.; Erdmann, J.; Schubert, C.; Regitz-Zagrosek, V. Intronic ANG II type 2 receptor gene polymorphism 1675 G/A modulates receptor protein expression but not mRNA splicing. Am. J. Physiol-Regul. Integr. Comp. Physiol. 2005, 289, R1729–R1735. [Google Scholar] [CrossRef]
- Panel, C.-T.G. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. 2021. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 31 August 2021).
- Invernizzi, A.; Torre, A.; Parrulli, S.; Zicarelli, F.; Schiuma, M.; Colombo, V.; Giacomelli, A.; Cigada, M.; Milazzo, L.; Ridolfo, A.; et al. Retinal findings in patients with COVID-19: Results from the SERPICO-19 study. EClinicalMedicine 2020, 27, 100550. [Google Scholar] [CrossRef]
- Yamamoto, N.; Ariumi, Y.; Nishida, N.; Yamamoto, R.; Bauer, G.; Gojobori, T.; Shimotohno, K.; Mizokami, M. SARS-CoV-2 infections and COVID-19 mortalities strongly correlate with ACE1 I/D genotype. Gene 2020, 758, 144944. [Google Scholar] [CrossRef]
- Zheng, H.; Cao, J.J. Angiotensin-Converting Enzyme Gene Polymorphism and Severe Lung Injury in Patients with Coronavirus Disease 2019. Am. J. Pathol. 2020, 190, 2013–2017. [Google Scholar] [CrossRef]
- Totomoch-Serra, A.; Domínguez-Cruz, M.G.; Manterola, C.; de Lourdes Muñoz, M. Variants in AGTR2 gene in Maya people with COVID-19. Gene 2021, 795, 145794. [Google Scholar] [CrossRef]
- Chlamydas, S.; Papavassiliou, A.G.; Piperi, C. Epigenetic mechanisms regulating COVID-19 infection. Epigenetics 2021, 16, 263–270. [Google Scholar] [CrossRef]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Takahashi, T.; Ellingson, M.K.; Wong, P.; Israelow, B.; Lucas, C.; Klein, J.; Silva, J.; Mao, T.; Oh, J.E.; Tokuyama, M.; et al. Sex differences in immune responses that underlie COVID-19 disease outcomes. Nature 2020, 588, 315–320. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| COVID-19 | p | Controls (n = 96) | p | ||
|---|---|---|---|---|---|
| Mild (n = 12) | Severe (n = 57) | ||||
| Age, years | 56 (49–60) | 58 (50–62) | 0.49 | 53 (41–60) | 0.06 |
| Sex (male) | 7 (58%) | 38 (67%) | 0.58 | 18 (19%) | <0.001 |
| Systolic pressure | 125 (114–153) | 120 (108–132) | 0.14 | 115 (105, 123) | <0.001 |
| Diastolic pressure | 76 (68–83) | 72 (69–81) | 0.76 | 79 (75–84) | 0.01 |
| COVID-19 clinical characteristics | |||||
| Duration of symptoms, days | 3.5 (1–4.5) | 10 (8–13) | <0.001 | - | - |
| Chest pain | 1 (8%) | 18 (32%) | 0.07 | - | - |
| Cough | 1 (8%) | 55 (96%) | <0.001 | - | - |
| Anosmia/ageusia | 0 (0%) | 6 (11%) | 0.12 | - | - |
| Dyspnoea | 2 (17%) | 42 (74%) | <0.001 | - | - |
| Diarrhea | 0 (0%) | 8 (14%) | 0.07 | - | - |
| Headache | 1 (8%) | 10 (18%) | 0.40 | - | - |
| DVT/PE | 0 (0%) | 3 (5%) | 0.28 | - | - |
| ICU admission | 0 (0%) | 6 (11%) | 0.12 | - | - |
| Laboratory parameters | |||||
| HbA1c | 5.5 (5.2–5.8) | 5.6 (5.4–5.9) | 0.18 | 5.4 (5.1–5.7) | <0.001 |
| LDH (μkat/L) | 3.2 (2.4–4.1) | 5.0 (4.2–5.8) | <0.001 | 2.8 (2.5–3.3) | <0.001 |
| Ferritin (μg/L) | 196 (110–375) | 843 (456–1501) | 0.001 | 53 (27–98) | <0.001 |
| CRP (mg/L) | 21 (11–45) | 34 (21–57) | 0.17 | ? | |
| White blood cells (×109/L) | 7.7 (5.3–8.5) | 6.9 (4.7–8.5) | 0.43 | 7 (5–8.1) | 0.58 |
| RDW (%) | 14.3 (14.0–15.1) | 13.9 (13.3–14.3) | 0.06 | 13 (12–14) | <0.001 |
| Platelets (×109/L) | 200 (175–278) | 263 (188–331) | 0.23 | 247 (194–317) | 0.87 |
| Lymphocytes (×109/L) | 1.8 (1.1–1.9) | 1.2 (0.8–1.7) | 0.09 | 2.1 (1.7–2.9) | <0.001 |
| D-dimer (μg/L) | 742 (427–1117) | 711 (513–1388) | 0.68 | 86 (58–251) | <0.001 |
| Treatment | |||||
| Dexamethasone | 0 (0%) | 50 (88%) | <0.001 | - | - |
| Remdesivir | 0 (0%) | 25 (44%) | 0.003 | - | - |
| Antibiotic | 1 (8%) | 8 (14%) | 1.00 | - | - |
| Oxygen | 0 (0%) | 50 (88%) | <0.001 | - | - |
| COVID-19 Retinopathy | p | ||
|---|---|---|---|
| NO (n = 19) | YES (n = 50) | ||
| Age, years | 57 (47–60) | 58 (50–63) | 0.31 |
| Sex (male) | 12 (63%) | 33 (66%) | 0.83 |
| Systolic pressure | 120 (111–130) | 121 (108–135) | 0.86 |
| Diastolic pressure | 74 (68–81) | 72 (67–83) | 0.93 |
| COVID-19 clinical characteristics | |||
| Duration of symptoms, days | 11.0 (6.5–15.0) | 9.0 (6.0–12.8) | 0.28 |
| Chest pain | 3 (16%) | 16 (32%) | 0.18 |
| Cough | 14 (74%) | 42 (84%) | 0.33 |
| Anosmia/ageusia | 1 (5%) | 5 (10%) | 1.00 |
| Dyspnoea | 11 (58%) | 33 (66%) | 0.53 |
| Diarrhea | 2 (11%) | 6 (12%) | 1.00 |
| Headache | 3 (16%) | 8 (16%) | 0.98 |
| DVT/PE | 0 (0%) | 3 (6%) | 0.56 |
| ICU admission | 3 (16%) | 3 (6%) | 0.22 |
| Laboratory parameters | |||
| HbA1c | 5.50 (5.25–5.85) | 5.60 (5.40–5.90) | 0.31 |
| LDH (μkat/L) | 4.40 (3.08–5.18) | 4.80 (3.83–5.29) | 0.35 |
| Ferritin (μg/L) | 816 (310–1434) | 684 (374–1447) | 0.65 |
| CRP (mg/L) | 15 (5–27) | 38 (25–64) | <0.001 |
| White blood cells (×109/L) | 8.10 (7.20–10.30) | 6.60 (4.48–7.97) | 0.01 |
| RDW (%) | 13.90 (13.45–14.20) | 14.05 (13.55–14.55) | 0.64 |
| Platelets (×109/L) | 289 (215–314) | 228 (165–347) | 0.30 |
| Lymphocytes (×109/L) | 1.67 (1.07–2.03) | 1.15 (0.78–1.46) | 0.03 |
| D-dimer (μg/L) | 590 (474–932) | 746 (530–1438) | 0.21 |
| Treatment | |||
| Dexamethasone | 13 (68%) | 37 (74%) | 0.64 |
| Remdesivir | 10 (53%) | 15 (30%) | 0.08 |
| Antibiotic | 3 (16%) | 6 (12%) | 0.70 |
| Oxygen | 12 (63%) | 38 (76%) | 0.29 |
| Polymorphism | Genotype | n | COVID-19 (n = 69) | Controls (n = 96) | p | p adj.a | n | COVID-19 Retinopathy | p | p adj.a | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| NO (n = 19) | YES (n = 50) | ||||||||||
| ACE (rs4646994) | |||||||||||
| Female and male | II | 163 | 11 (16%) | 20 (21%) | 0.54 | 1.00 | 67 | 3 (17%) | 8 (16%) | 0.71 | 0.89 |
| ID | 32 (48%) | 49 (51%) | 10 (56%) | 22 (45%) | |||||||
| DD | 24 (36%) | 27 (28%) | 5 (28%) | 19 (39%) | |||||||
| HWE (p) | 0.95 | 0.78 | 0.56 | 0.7 | |||||||
| ACE2 (rs2285666) | |||||||||||
| Female | AA | 101 | 1 (4%) | 3 (4%) | 0.83 | 1.00 | 23 | 0 (0%) | 1 (6%) | 0.18 | 0.29 |
| GA | 5 (22%) | 22 (28%) | 0 (0%) | 5 (31%) | |||||||
| GG | 17 (74%) | 53 (68%) | 7 (100%) | 10 (63%) | |||||||
| Male | AA | 63 | 13 (29%) | 6 (33%) | 0.97 | 1.00 | 45 | 3 (25%) | 10 (30%) | 1.00 | 1.00 |
| GG | 32 (71%) | 12 (67%) | 9 (75%) | 23 (70%) | |||||||
| HWE (p) | 0.26 | 0.31 | 0.23 | 0.64 | |||||||
| AGTR2 (rs1403543) | |||||||||||
| Female | GG | 101 | 7 (30%) | 22 (28%) | 0.06 | 0.31 | 23 | 0 (0%) | 7 (44%) | 0.07 | 0.18 |
| AG | 14 (61%) | 32 (41%) | 6 (86%) | 8 (50%) | |||||||
| AA | 2 (9%) | 24 (31%) | 1 (14%) | 1 (6%) | |||||||
| Male | GG | 63 | 23 (51%) | 9 (50%) | 1.00 | 1.00 | 45 | 9 (75%) | 14 (42%) | 0.05 | 0.18 |
| AA | 22 (49%) | 9 (50%) | 3 (25%) | 19 (58%) | |||||||
| HWE (p) | 0.18 | 0.11 | 0.58 | 0.67 | |||||||
| Polymorphism | Genotype | Veins Diameter | Arteries Diameter | ||
|---|---|---|---|---|---|
| Estimate (95% CI) | p | Estimate (95% CI) | p | ||
| ACE a | II | 1.96 (−9.18–13.09) | 0.73 | 1.75 (−7.57–11.08) | 0.71 |
| ID | −0.64 (−8.38–7.10) | 0.87 | 0.89 (−5.80–7.58) | 0.79 | |
| DD | Ref. | Ref. | |||
| Femaleb | |||||
| ACE2 | AA | −9.6 (−44.05–24.85) | 0.58 | −3.11 (−26.88–20.65) | 0.80 |
| GA | 14.21 (−14.29–42.71) | 0.32 | 10.94 (−10.52–32.41) | 0.31 | |
| GG | Ref. | Ref. | |||
| AGTR2 | AA | −2.43 (−26.30–21.44) | 0.84 | 13.16 (−4.54–30.86) | 0.14 |
| AG | 7.85 (−8.41–24.11) | 0.34 | 11.03 (−1.21–23.28) | 0.08 | |
| GG | Ref. | Ref. | |||
| Maleb | |||||
| ACE2 | AA | 1.14 (−8.87–11.15) | 0.82 | −0.67 (−9.43–8.09) | 0.88 |
| GG | Ref. | Ref. | |||
| AGTR2 | AA | −3.55 (−11.99–4.88) | 0.41 | −6.41 (−13.69–0.87) | 0.08 |
| GG | Ref. | Ref. | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jevnikar, K.; Lapajne, L.; Petrovič, D.; Meglič, A.; Logar, M.; Vidovič Valentinčič, N.; Globočnik Petrovič, M.; Cilenšek, I.; Mekjavić, P.J. The Role of ACE, ACE2, and AGTR2 Polymorphisms in COVID-19 Severity and the Presence of COVID-19-Related Retinopathy. Genes 2022, 13, 1111. https://doi.org/10.3390/genes13071111
Jevnikar K, Lapajne L, Petrovič D, Meglič A, Logar M, Vidovič Valentinčič N, Globočnik Petrovič M, Cilenšek I, Mekjavić PJ. The Role of ACE, ACE2, and AGTR2 Polymorphisms in COVID-19 Severity and the Presence of COVID-19-Related Retinopathy. Genes. 2022; 13(7):1111. https://doi.org/10.3390/genes13071111
Chicago/Turabian StyleJevnikar, Kristina, Luka Lapajne, Daniel Petrovič, Andrej Meglič, Mateja Logar, Nataša Vidovič Valentinčič, Mojca Globočnik Petrovič, Ines Cilenšek, and Polona Jaki Mekjavić. 2022. "The Role of ACE, ACE2, and AGTR2 Polymorphisms in COVID-19 Severity and the Presence of COVID-19-Related Retinopathy" Genes 13, no. 7: 1111. https://doi.org/10.3390/genes13071111