
Evaluation of RT-qPCR and Loop-Mediated Isothermal Amplification (LAMP) Assays for the Detection of SARS-CoV-2 in Argentina

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
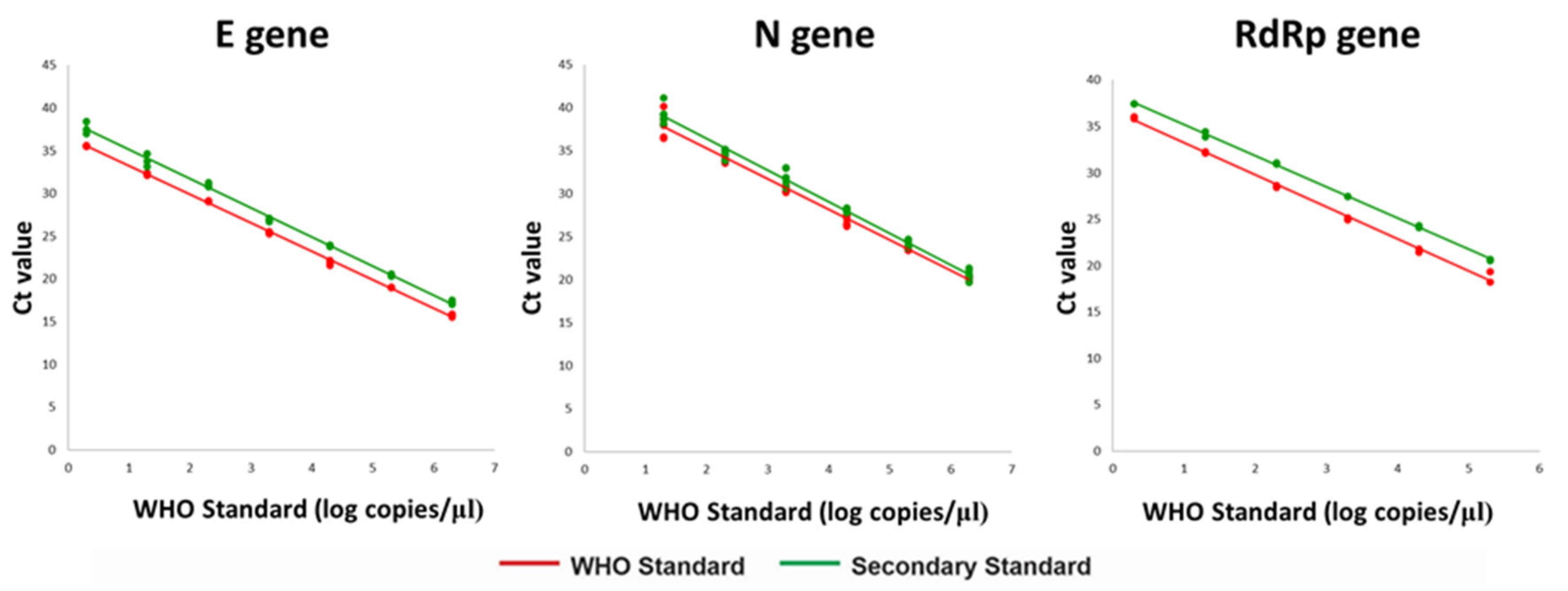
2.2. Preparation and Calibration of a Secondary Standard
2.3. Panel of Positive and Negative SARS-CoV-2 Contrived Samples
2.4. SARS-CoV-2 RNA Detection Kits
2.5. Comparison of Methods and Statistical Analyses
3. Results
3.1. Calibration of the Secondary Standard
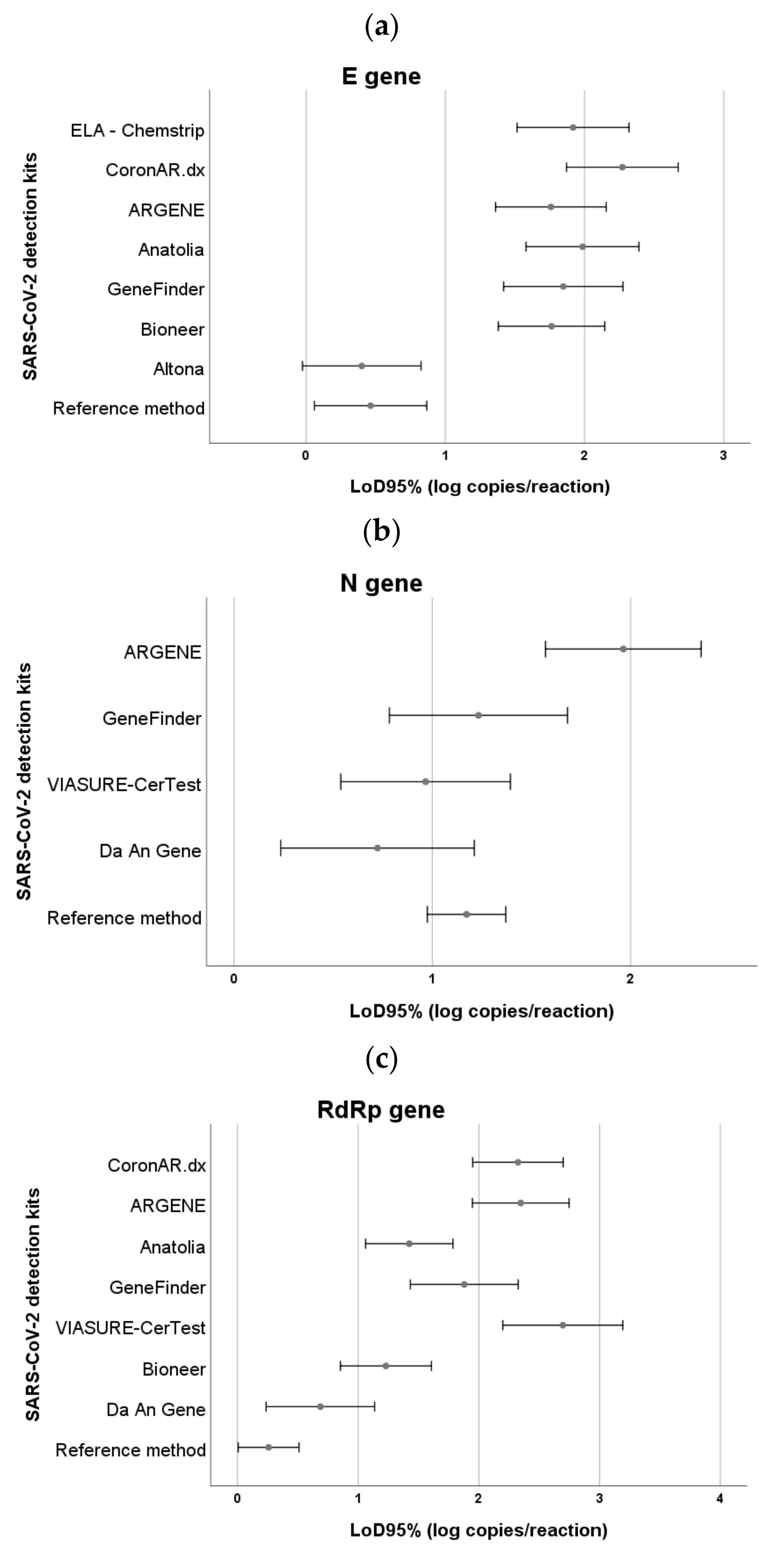
3.2. Differences in the Limit of Detection of Commercial Kits
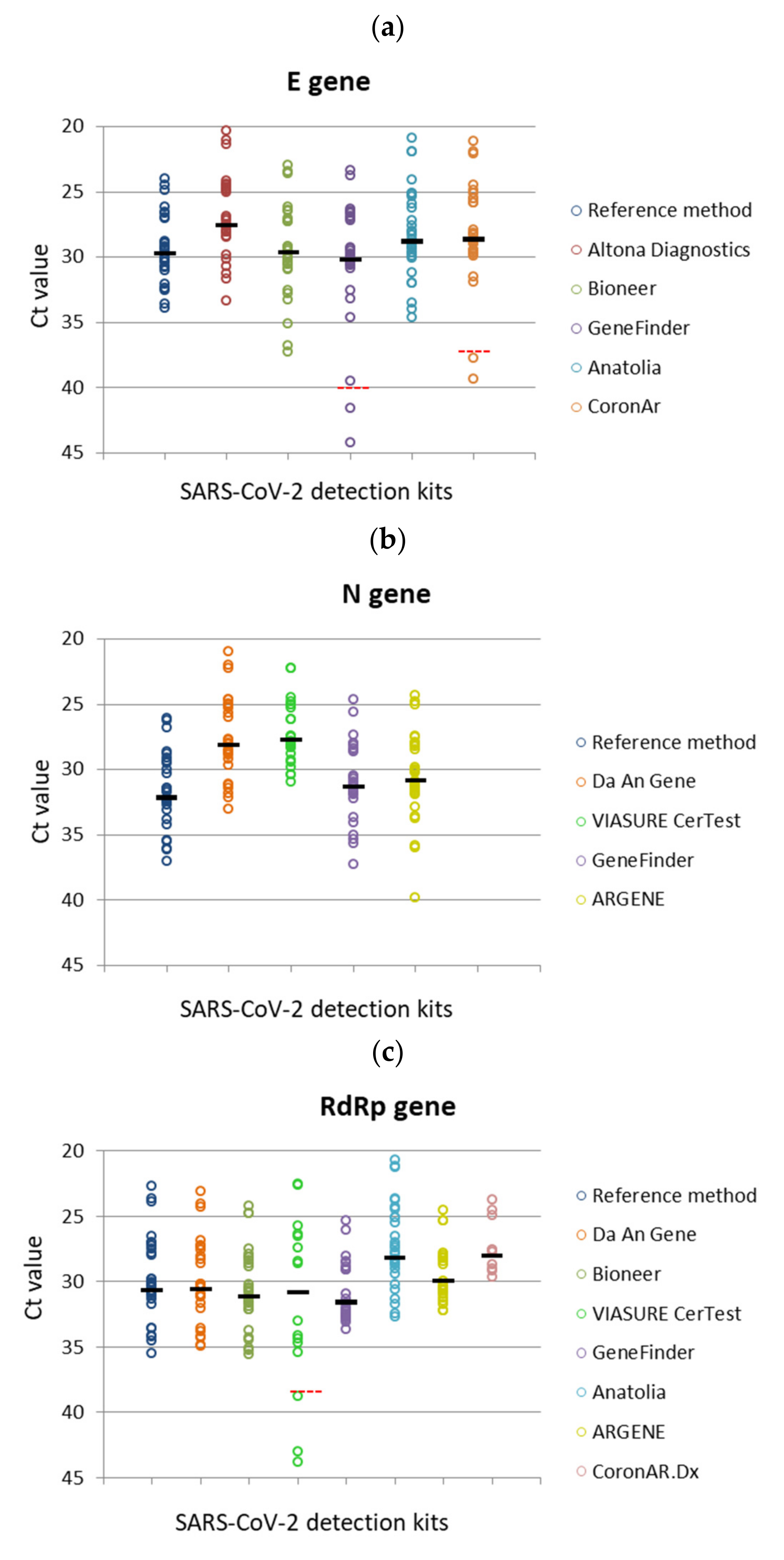
3.3. Variations in the Clinical Performance of the Commercial Kits
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chan, J.F.W.; Yuan, S.; Kok, K.-H.; Chu, H.; Yang, J.; Xing, F.; Yip, C.; Cai, J.-P.; Chan, K.-H.; Tsoi, H.-W.; et al. A Familial Cluster of Pneumonia Associated with the 2019 Novel Coronavirus Indicating Person-to-Person Transmission: A Study of a Family Cluster. Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef] [Green Version]
- WHO. Laboratory Testing for Coronavirus Disease (COVID-19) in Suspected Human Cases: Interim Guidance, 19 March 2020; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Chaouch, M. Loop-mediated isothermal amplification (LAMP): An effective molecular point-of-care technique for the rapid diagnosis of coronavirus SARS-CoV-2. Rev. Med. Virol. 2021, e2215. [Google Scholar] [CrossRef]
- Dudley, D.M.; Newman, C.M.; Weiler, A.M.; Ramuta, M.D.; Shortreed, C.G.; Heffron, A.S.; Accola, M.A.; Rehrauer, W.M.; Friedrich, T.C.; O’Connor, D.H. Optimizing direct RT-LAMP to detect transmissible SARS-CoV-2 from primary nasopharyngeal swab samples. PLoS ONE 2020, 15, e0244882. [Google Scholar] [CrossRef]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.W.; Bleicker, T.; Brünink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Eurosurveillance 2020, 25, 2000045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilrich, C.; Wilrich, P.T. Estimation of the POD function and the LOD of a qualitative microbiological measurement method. J. AOAC Int. 2009, 92, 1763–1772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Manual for Preparation of Secondary Reference Materials for in Vitro Diagnostic Assays Designed for Infectious Disease Nucleic Acid or Antigen Detection: Calibration to WHO International Standards; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Van Kasteren, P.B.; van der Veer, B.; van den Brink, S.; Wijsman, L.; de Jonge, J.; van den Brandt, A.; Molenkamp, R.; Reusken, C.B.E.M.; Meijer, A. Comparison of seven commercial RT-PCR diagnostic kits for COVID-19. J. Clin. Virol. 2020, 128, 104412. [Google Scholar] [CrossRef] [PubMed]
- Igloi, Z.; Leven, M.; Abou-Nouar, Z.A.-K.; Weller, B.; Matheeussen, V.; Coppens, J.; Koopmans, M.; Molenkamp, R. Comparison of commercial realtime reverse transcription PCR assays for the detection of SARS-CoV-2. J. Clin. Virol. 2020, 129, 104510. [Google Scholar] [CrossRef] [PubMed]
- LeBlanc, J.J.; Gubbay, J.B.; Li, Y.; Needle, R.; Arneson, S.R.; Marcino, D.; Charest, H.; Desnoyers, G.; Dust, K.; Fattouh, R.; et al. Real-time PCR-based SARS-CoV-2 detection in Canadian laboratories. J. Clin. Virol. 2020, 128, 104433. [Google Scholar] [CrossRef] [PubMed]
- Ji, T.; Liu, Z.; Wang, G.Q.; Guo, X.; Khan, S.A.; Lai, C.; Chen, H.; Huang, S.; Xia, S.; Chen, B.; et al. Detection of COVID-19: A review of the current literature and future perspectives. Biosens. Bioelectron. 2020, 166, 112455. [Google Scholar] [CrossRef]
- Kashir, J.; Yaqinuddin, A. Loop mediated isothermal amplification (LAMP) assays as a rapid diagnostic for COVID-19. Med. Hypotheses 2020, 141, 109786. [Google Scholar] [CrossRef]
- Alekseenko, A.; Barrett, D.; Pareja-Sanchez, Y.; Howard, R.J.; Strandback, E.; Ampah-Korsah, H.; Rovšnik, U.; Zuniga-Veliz, S.; Klenov, A.; Malloo, J.; et al. Direct detection of SARS-CoV-2 using non-commercial RT-LAMP reagents on heat-inactivated samples. Sci. Rep. 2021, 11, 1820. [Google Scholar] [CrossRef] [PubMed]
- Schermer, B.; Fabretti, F.; Damagnez, M.; Di Cristanziano, V.; Heger, E.; Arjune, S.; Tanner, N.A.; Imhof, T.; Koch, M.; Ladha, A.; et al. Rapid SARS-CoV-2 testing in primary material based on a novel multiplex RT-LAMP assay. PLoS ONE 2020, 15, e0238612. [Google Scholar] [CrossRef]
- Mautner, L.; Baillie, C.-K.; Herold, H.M.; Volkwein, W.; Guertler, P.; Eberle, U.; Ackermann, N.; Sing, A.; Pavlovic, M.; Goerlich, O.; et al. Rapid point-of-care detection of SARS-CoV-2 using reverse transcription loop-mediated isothermal amplification (RT-LAMP). Virol. J. 2020, 17, 160. [Google Scholar] [CrossRef]
- WHO. Diagnostic Testing for SARS-CoV-2: Interim Guidance, 11 September 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Zhu, X.; Wang, X.; Han, L.; Chen, T.; Wang, L.; Li, H.; Li, S.; He, L.; Fu, X.; Chen, S.; et al. Multiplex reverse transcription loop-mediated isothermal amplification combined with nanoparticle-based lateral flow biosensor for the diagnosis of COVID-19. Biosens. Bioelectron. 2020, 166, 112437. [Google Scholar] [CrossRef]
- Baek, Y.H.; Um, J.; Antigua, K.J.C.; Park, J.-H.; Kim, Y.; Oh, S.; Kim, Y.; Choi, W.-S.; Kim, S.G.; Jeong, J.H.; et al. Development of a reverse transcription-loop-mediated isothermal amplification as a rapid early-detection method for novel SARS-CoV-2. Emerg. Microbes Infect. 2020, 9, 998–1007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, G.-S.; Ku, K.; Baek, S.-H.; Kim, S.-J.; Kim, S.; Kim, B.-T.; Maeng, J.-S. Development of Reverse Transcription Loop-Mediated Isothermal Amplification Assays Targeting Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). J. Mol. Diagn. 2020, 22, 729–735. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.E.; Lim, B.; Hsu, C.-C.; Xiong, D.; Wu, W.; Yu, Y.; Jia, H.; Wang, Y.; Zeng, Y.; Ji, M.; et al. RT-LAMP for rapid diagnosis of coronavirus SARS-CoV-2. Microb. Biotechnol. 2020, 13, 950–961. [Google Scholar] [CrossRef] [Green Version]
- Lu, Y.; Li, L.; Ren, S.; Liu, X.; Zhang, L.; Li, W.; Yu, H. Comparison of the diagnostic efficacy between two PCR test kits for SARS-CoV-2 nucleic acid detection. J. Clin. Lab. Anal. 2020, 34, e23554. [Google Scholar] [CrossRef]
- Yan, C.; Cui, J.; Huang, L.; Du, B.; Chen, L.; Xue, G.; Li, S.; Zhang, W.; Zhao, L.; Sun, Y.; et al. Rapid and visual detection of 2019 novel coronavirus (SARS-CoV-2) by a reverse transcription loop-mediated isothermal amplification assay. Clin. Microbiol. Infect. 2020, 26, 773–779. [Google Scholar] [CrossRef]
- Nalla, A.K.; Casto, A.M.; Huang, M.-L.W.; Perchetti, G.A.; Sampoleo, R.; Shrestha, L.; Wei, Y.; Zhu, H.; Jerome, K.R.; Greninger, A.L. Comparative Performance of SARS-CoV-2 Detection Assays Using Seven Different Primer-Probe Sets and One Assay Kit. J. Clin. Microbiol. 2020, 58. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Pei, F.; Ji, M.; Wang, L.; Zhao, H.; Li, H.; Yang, W.; Wang, Q.; Zhao, Q.; Wang, Y. Sensitivity evaluation of 2019 novel coronavirus (SARS-CoV-2) RT-PCR detection kits and strategy to reduce false negative. PLoS ONE 2020, 15, e0241469. [Google Scholar] [CrossRef] [PubMed]
- Chu, D.K.W.; Pan, Y.; Cheng, S.M.S.; Hui, K.P.Y.; Krishnan, P.; Liu, Y.; Ng, D.Y.M.; Wan, C.K.C.; Yang, P.; Wang, Q.; et al. Molecular Diagnosis of a Novel Coronavirus (2019-nCoV) Causing an Outbreak of Pneumonia. Clin. Chem. 2020, 66, 549–555. [Google Scholar] [CrossRef] [Green Version]
- Mustafa Hellou, M.; Górska, A.; Mazzaferri, F.; Cremonini, E.; Gentilotti, E.; De Nardo, P.; Poran, I.; Leeflang, M.M.; Tacconelli, E.; Paul, M. Nucleic acid amplification tests on respiratory samples for the diagnosis of coronavirus infections: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2020, 27, 341–351. [Google Scholar] [CrossRef] [PubMed]
- Subsoontorn, P.; Lohitnavy, M.; Kongkaew, C. The diagnostic accuracy of isothermal nucleic acid point-of-care tests for human coronaviruses: A systematic review and meta-analysis. Sci. Rep. 2020, 10, 22349. [Google Scholar] [CrossRef]
- Dao Thi, V.L.; Herbst, K.; Boerner, K.; Meurer, M.; Kremer, L.P.M.; Kirrmaier, D.; Freistaedter, A.; Papagiannidis, D.; Galmozzi, C.; Stanifer, M.L.; et al. A colorimetric RT-LAMP assay and LAMP-sequencing for detecting SARS-CoV-2 RNA in clinical samples. Sci. Transl. Med. 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Shirato, K.; Yano, T.; Senba, S.; Akachi, S.; Kobayashi, T.; Nishinaka, T.; Notomi, T.; Matsuyama, S. Detection of Middle East respiratory syndrome coronavirus using reverse transcription loop-mediated isothermal amplification (RT-LAMP). Virol. J. 2014, 11, 139. [Google Scholar] [CrossRef] [Green Version]
- Shirato, K.; Semba, S.; El-Kafrawy, S.A.; Hassan, A.M.; Tolah, A.M.; Takayama, I.; Kageyama, T.; Notomi, T.; Kamitani, W.; Matsuyama, S.; et al. Development of fluorescent reverse transcription loop-mediated isothermal amplification (RT-LAMP) using quenching probes for the detection of the Middle East respiratory syndrome coronavirus. J. Virol. Methods 2018, 258, 41–48. [Google Scholar] [CrossRef]
- Schrader, C.; Schielke, A.; Ellerbroek, L.; Johne, R. PCR inhibitors—Occurrence, properties and removal. J. Appl. Microbiol. 2012, 113, 1014–1026. [Google Scholar] [CrossRef] [PubMed]
- Huggett, J.; Dheda, K.; Bustin, S.; Zumla, A. Real-time RT-PCR normalisation; strategies and considerations. Genes. Immun. 2005, 6, 279–284. [Google Scholar] [CrossRef] [Green Version]
- Alvarez-Diaz, D.A.; Muñoz, C.F.; Laiton-Donato, K.; Usme-Ciro, J.A.; Franco-Sierra, N.D.; Flórez-Sánchez, A.C.; Gómez-Rangel, S.; Rodríguez-Calderon, L.D.; Barbosa-Ramirez, J.; Ospitia-Baez, E.; et al. Molecular analysis of several in-house rRT-PCR protocols for SARS-CoV-2 detection in the context of genetic variability of the virus in Colombia. Infect. Genet. Evol. 2020, 84, 104390. [Google Scholar] [CrossRef]
- Artesi, M.; Bontems, S.; Göbbels, P.; Franckh, M.; Maes, P.; Boreux, R.; Meex, C.; Melin, P.; Hayette, M.-P.; Bours, V.; et al. A Recurrent Mutation at Position 26340 of SARS-CoV-2 Is Associated with Failure of the E Gene Quantitative Reverse Transcription-PCR Utilized in a Commercial Dual-Target Diagnostic Assay. J. Clin. Microbiol. 2020, 58. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, K.; Steininger, P.; Ziegler, R.; Steinmann, J.; Korn, K.; Ensser, A. SARS-CoV-2 samples may escape detection because of a single point mutation in the N gene. Eurosurveillance 2020, 25, 2001650. [Google Scholar] [CrossRef] [PubMed]
- Bal, A.; Destras, G.; Gaymard, A.; Stefic, K.; Marlet, J.; Eymieux, S.; Regue, H.; Semanas, Q.; d’Aubarede, C.; Billaud, G.; et al. Two-step strategy for the identification of SARS-CoV-2 variant of concern 202012/01 and other variants with spike deletion H69-V70, France, August to December 2020. Eurosurveillance 2021, 26, 2100008. [Google Scholar] [CrossRef]
- Osorio, N.S.; Correia-Neves, M. Implication of SARS-CoV-2 evolution in the sensitivity of RT-qPCR diagnostic assays. Lancet Infect. Dis. 2021, 21, 166–167. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Kit | Methodology | Regulation Status | Country of Origin | Internal Control | No. PCRs (Target Genes) 1 | Equipment | Ct 2 Cut-Off |
|---|---|---|---|---|---|---|---|
| WHO protocol- Charité assay (https://www.who.int/docs/default-source/coronaviruse/protocol-v2-1) (accessed on: 1 February 2020) | RT-qPCR | LDT 3 | Germany | An endogenous human gene detection was used in an independent reaction | Three single PCRs (E,N,RdRp) | ABI 7500 | Not indicated. Any signal is considered positive |
| RealStar SARS-CoV-2 RT-PCR Kit 1.0 (Altona Diagnostics) | RT-qPCR | CE-IVD 4 | Germany | Heterologous. Spiked into sample or PCR mix. | One multiplex PCR (E,S,IC 5) | ABI 7500 | Not indicated. Any signal is considered positive |
| Detection kit for 2019Novel coronavirus (2019-nCoV) RNA-Da An Gene Ltd. (Sun-Yat University) | RT-qPCR | CE-IVD | China | Pseudovirus containing human endogenous internal standard | One multiplex PCR (N, ORF1ab, IC) | ABI 7500 | ≤40 |
| AccuPower SARS-CoV-2 Realtime RT PCR Kit (Bioneer Corporation) | RT-qPCR | CE-IVD | Korea | Heterologous. Included in PCR mix | Two multiplex PCRs (PCR1: E, IC PCR2: RdRP, IC) | CFX96 | ≤38 |
| VIASURE SARS CoV-2 Real time PCR Detection Kit (CerTest Biotec SL) | RT-qPCR | CE-IVD | Spain | Heterologous. Included in PCR mix | One multiplex PCR (N,ORF1ab, IC) | CFX96 | <38 |
| GeneFinder COVID-19 Plus RealAmp kit (Osang Healthcare Co., Ltd.) | RT-qPCR | CE-IVD | Korea | Endogenous human IC | One multiplex PCR (E, N, RdRP, IC) | ABI 7500 | ≤43 |
| Bosphore Novel Coronavirus (2019-nCoV) detection kit v2 (Anatolia Geneworks) | RT-qPCR | CE-IVD | Turkey | Heterologous. Spiked into sample or PCR mix | One multiplex PCR (E, ORF1ab, IC) | ABI 7500 | Not indicated |
| ARGENE SARS-COV-2 R-GENE® (Biomerieux) | RT-qPCR | CE-IVD | France | Two types: IC spiked into sample and cellular control | Two multiplex PCRs (PCR1: N, RdRp, IC PCR2: E, IC, Chuman) | CFX96 | Not indicated |
| CoronAR.dx (Argenomics- ZEV-Biotech) | RT-qPCR | IVD | Argentina | Synthetic DNA corresponding to the RPP30 gene | Three single PCRs (E, RdRP, IC) | ABI 7500 | ≤37 ≤ 40 ≤ 35 |
| WGene SARS-CoV-2 RT detection kit (Wiener lab) | RT-qPCR | CE-IVD | Argentina | Endogenous IC corresponding to RNAsaP | One multiplex PCR (N + RdRp), IC | ABI 7500 | |
| iAMP COVID-19 Detection Kit (ATILA Biosystems) | Real time IA 6 | IVD | China | Includes an IC to validate the extraction procedure | One multiplex IA (N + ORF1ab), IC | ABI 7500 | Any signal is considered positive |
| Covid-19 NEOKIT Tecnoami (NEOKIT SAS) | Colorimetric IA | IVD-ANMaT 7 | Argentina | Not included | One multiplex IA (E + N+ORF1Aa + ORF1ab) | Thermal block | NA 8 |
| ELA CHEMSTRIP Covid-19 (Chemtest Argentina SA) | IA plus immune- chromatographic detection | ANMaT | Argentina | Endogenous IC corresponding to RNAsaP | Two single IA (E, IC) | Thermal block | NA |
| Kits | Target Genes 1 | Kappa Index (CI 95%) | Clinical Sensitivity (%) (CI 95%) | Clinical Specificity (%) (CI 95%) |
|---|---|---|---|---|
| Altona Diagnostics | E | 0.97 (0.85–1) | 100 (89.3–100) | 96.7 (0.79–0.98) |
| S | 1.00 (1.00–1.00) | 100 (89.3–100) | 100 (88.6–100) | |
| E + S | 1.00 (1.00–1.00) | 100 (89.3–100) | 100(88.6–100) | |
| DaAn Gene | N | 1.00 (1.00–1.00) | 100 (89.3–100) | 100 (88.6–100) |
| ORF1ab | 1.00 (1.00–1.00) | 100 (89.3–100) | 100 (88.6–100) | |
| N + ORF1ab | 1.00 (1.00–1.00) | 100 (89.3–100) | 100 (88.6–100) | |
| Bioneer | E | 1.00 (1.00–1.00) | 100 (89.3–100) | 100 (89.0–100) |
| RdRp | 1.00 (1.00–1.00) | 100 (89.3–100) | 100 (89.0–100) | |
| E + RdRp | 1.00 (1.00–1.00) | 100 (89.3–100) | 100 (89.0–100) | |
| VIASURE-CerTest | N | 1.00 (0.85–1.00) | 100 (89.0 –100) | 100 (79.3– 98.2) |
| ORF1ab | 0.42 (0.24–0.60) | 42 (26.4–59.2) | 100 (89.0–100) | |
| N + ORF1ab | 0.42 (0.24–0.60) | 42 (26.4–59.2) | 100 (89.0–100) | |
| GeneFinder | E | 0.97 (0.91–1.00) | 96.8 (83.8 –99.4) | 100 (89.0–100) |
| N | 1.00 (1.00–1.00) | 100 (89.0–100) | 100 (89.0–100) | |
| RdRp | 0.81 (0.66–0.95) | 80.6 (63.7–90.8) | 100 (89.0–100) | |
| E + N + RdRp | 1.00 (1.00–1.00) | 100 (89.0–100) | 100 (89.0–100) | |
| Anatolia | E | 1.00 (1.00–1.00) | 100 (89.3–100) | 100 (89.0–100) |
| ORF1ab | 1.00 (1.00–1.00) | 100 (89.3–100) | 100 (89.0–100) | |
| E + ORF1ab | 1.00 (1.00–1.00) | 100 (89.3–100) | 100 (89.0–100) | |
| ARGENE | N | 0.97 (0.91–1.00) | 100 (89.3–100) | 96.8 (83.8–99.4) |
| RdRp | 0.81 (0.67–0.95) | 81.3 (64.7–91.1) | 100 (89.0–100) | |
| E | Use for resolution of equivocal samples | |||
| N + RdRp + (E) | 1.00 (0.91–1.00) | 100 (89.3–100) | 100 (83.8–99.4) | |
| CoronArDx | E | 0.94 (0.69 –1.00) | 93.8(79.9–98.3) | 100 (88.6–100) |
| RdRp | 0.31 (0.13–0.48) | 31.3 (18.0–48.6) | 100 (88.6–100) | |
| E + RdRp | 0.94 (0.69–1.00) | 93.8 (79.9–98.3) | 100 (88.6–100) | |
| Wiener lab | N + RdRp | 0.97 (0.91–1.00) | 96.9 (84.3 –99.4) | 100 (89.0–100) |
| iAMP COVID-19 Detection Kit | N + ORF1ab | 0.93 (0.67–1.00) | 92.6 (83.0–100) | 100.0 (89.0–100) |
| NEOKIT | E + N + ORF1aa + ORF1ab | 0.75 (0.59–0.91) | 75.0 (57.9–86.7) | 100.0 (0.89–100) |
| ELA-CHEMSTRIP | E | 0.84 (0.71–0.97) | 100 (89.3–100) | 83.9 (67.4–92.9) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fellner, M.D.; Bonaventura, R.; Basiletti, J.; Avaro, M.; Benedetti, E.; Campos, A.; Dattero, M.E.; Russo, M.; Vladmirsky, S.; Molina, V.; et al. Evaluation of RT-qPCR and Loop-Mediated Isothermal Amplification (LAMP) Assays for the Detection of SARS-CoV-2 in Argentina. Genes 2021, 12, 659. https://doi.org/10.3390/genes12050659
Fellner MD, Bonaventura R, Basiletti J, Avaro M, Benedetti E, Campos A, Dattero ME, Russo M, Vladmirsky S, Molina V, et al. Evaluation of RT-qPCR and Loop-Mediated Isothermal Amplification (LAMP) Assays for the Detection of SARS-CoV-2 in Argentina. Genes. 2021; 12(5):659. https://doi.org/10.3390/genes12050659
Chicago/Turabian StyleFellner, María Dolores, Romina Bonaventura, Jorge Basiletti, Martín Avaro, Estefanía Benedetti, Ana Campos, María Elena Dattero, Mara Russo, Sara Vladmirsky, Viviana Molina, and et al. 2021. "Evaluation of RT-qPCR and Loop-Mediated Isothermal Amplification (LAMP) Assays for the Detection of SARS-CoV-2 in Argentina" Genes 12, no. 5: 659. https://doi.org/10.3390/genes12050659