
Potential Effects of Oral Isotretinoin on Growth Plate and Height

1
Pediatric Endocrinology Unit, Department of Pediatrics, Hospital de Clínicas, Universidade Federal do Paraná, Curitiba 80060-240, PR, Brazil
2
Department of Internal Medicine, Endocrine Division (SEMPR), Hospital de Clínicas, Universidade Federal do Paraná, Curitiba 80030-110, PR, Brazil
3
Department of Pediatrics, Universidade Federal do Paraná, Curitiba 80030-110, PR, Brazil
*
Authors to whom correspondence should be addressed.
Endocrines 2023, 4(2), 281-292; https://doi.org/10.3390/endocrines4020023
Submission received: 20 November 2022
/
Revised: 13 March 2023
/
Accepted: 31 March 2023
/
Published: 7 April 2023
(This article belongs to the Special Issue Growth and Growth Disorders)
Abstract
:Longitudinal growth and puberty are the result of a complex interaction of genetic, hormonal, nutritional, and environmental factors. Acne vulgaris is a chronic disease of the pilosebaceous unit that affects 85% of adolescents worldwide. Isotretinoin is a synthetic vitamin A derivative drug effective and is widely employed for the treatment of moderate and severe acne vulgaris. Premature epiphyseal closure has been reported in patients with neuroblastoma treated with high doses of isotretinoin as well as in patients with acne receiving lower doses. Although the mechanisms for these effects are not clear, it has been suggested that isotretinoin may have a negative impact on the GH-IGF-I axis, leading to a reduction in IGF-I and IGFBP3 serum levels. Although many of the isotretinoin adverse effects in pediatric patients are transient, premature epiphyseal closure and bone abnormalities can lead to transient abnormalities and permanent deformities with a negative impact on longitudinal growth and final height. The aim of this study was to review the potential effects of oral isotretinoin on the growth plate and growth during childhood and adolescence.
1. Introduction
Acne vulgaris is a multifactorial, chronic, immune-mediated, inflammatory primary disease of the pilosebaceous unit [1]. It affects 85% of adolescents worldwide and can persist into adulthood [2]. There are four main factors in acne pathogenesis: follicular epidermal hyperproliferation, increased sebum production, inflammation, and Cutibacterium acnes (formerly Propionibacterim acnes) presence and activity [3]. A combination of topical and systemic drugs, such as antibiotics, benzoyl peroxide, retinoids, and hormonal-based therapies (oral contraceptives with antiandrogenic effects), are recommended therapies to cope with the various stages of the acne pathogenic process [2].
Hyperseborrhea has been considered the major etiopathogenetic factor of acne. With puberty onset, androgens stimulate sebaceous glands and increase sebum production [4]. Other hormones may be implicated in sebum production, such as estrogens, insulin, growth hormone (GH), insulin-like growth factor I (IGF-I), corticotropin-releasing hormone (CRH), adrenocorticotropic hormone (ACTH), melanocyte-stimulating hormone (MSH), and glucocorticoids [5]. GH and IGF-I are known stimulators of cell proliferation and apoptosis inhibitors [6]. Recently, some reports have suggested that IGF-I plays a role in acne pathogenesis by stimulating sebocyte growth, the lipogenesis of sebaceous glands, and androgen synthesis, like dihydrotestosterone and dehydroepiandrosterone sulfate [7,8,9]. Smith et al. found that IGF-I transmits its lipogenic signal in sebocytes via activation of the phosphoinositide-3-kinase–protein kinase B/Akt (PI3K-PKB/Akt) signaling pathway, which is involved in many aspects of cell growth, survival, and apoptosis [10]. IGF-I also stimulates keratinocyte proliferation by activating the IGF-I receptor (IGF-IR). A growth spurt during adolescence occurs due to increased GH secretion and higher concentrations of IGF-I, which is typical of puberty, whereas these high IGF-I levels might also be associated with the most severe course of acne at this age [8]. The development of hyperandrogenism and acne in patients with Laron syndrome during high-dose IGF-I treatment supports the role of IGF-I in acne pathogenesis [11,12].
Retinoids are both natural and synthetic vitamin A derivatives, with multiple actions and important roles in the regulation of cell proliferation, differentiation, morphogenesis, and apoptosis. They also inhibit malignant cell growth and tumor progression, exert immuno-modulatory actions, and alter cellular cohesiveness [13]. Isotretinoin, a 13-cis-retinoic acid, is an aromatic retinoid-like vitamin A used in the treatment of moderate or severe acne that is refractory to topical treatment and systemic antibiotics, ichthyotic skin disease, and psoriasis [1,14,15]. Isotretinoin is also recommended for the treatment of high-risk neuroblastoma and pediatric medulloblastoma, but in these cases, higher doses are used compared to those used for dermatological diseases [15,16].
Retinoids are oxidized to all-trans-retinaldehyde and subsequently converted to all-trans-retinoic acid (ATRA), the biologically active form of vitamin A. The effects of retinoids are mediated by their binding and activation of the nuclear retinoic acid (RAR) and retinoid X (RXR) receptors, which regulate the transcription of genes involved in normal growth and differentiation [13,15,17]. It is estimated that isotretinoin affects over 500 genes, of which 300 are upregulated and 200 are downregulated [15]. The effects of ATRA are also mediated by non-genomic signaling pathways, such as mitogen-activated protein kinase (MAPK) and protein kinase A (PKA).
Isotretinoin exerts its action by isomerization to ATRA, which then interacts with the retinoid receptors. Isotretinoin has a higher affinity for RXR, but the affinity is low for both RAR and RXR [13,17]. These nuclear receptors can be expressed in different amounts in hippocampal neurons, neural crest cells, epidermal keratinocytes, mucosa cells, hair follicle cells, intestinal epithelial cells, skeletal muscle cells, granulosa cells, the growth plate, the cardiovascular system, and the liver [17,18]. However, the relative lack of receptor specificity explains the wide spectrum of possible adverse effects of the drug, such as an increase in serum aminotransferase levels, dry skin, ocular and nasal mucosa xerosis, nose bleeds, conjunctivitis, headache, and hair loss. The use of isotretinoin has also been associated with moderate increases in serum triglycerides levels, pancreatitis, arthralgia, myalgia, vision and hearing loss, pseudotumor cerebri, teratogenicity, insomnia, irritability, depression, and suicide [1,17]. Apoptosis is the underlying and unifying mechanism of the adverse effects of isotretinoin [18]. Teratogenicity is the most severe adverse effect, and preventing fetal exposure to isotretinoin is mandatory. The most frequent abnormalities are microtia, anotia, micrognathia, heart and aortic arch defects, thymic ectopia or aplasia, cerebellar vermis agenesis, and various neuronal migration anomalies. ATRA leads to large-scale reprogramming of cranial neural crest gene expression, which results in increased apoptosis [18]. The common and less severe adverse effects related to oral isotretinoin comprise dryness of the skin and mucosae membranes, which is caused by sebocyte apoptosis and cell cycle arrest [18]. The retinoids are metabolized by the hepatic system, and ATRA and isotretinoin induce hepatocyte apoptosis. Moderate increases in alanine aminotransferase, aspartate aminotransferase, and triglycerides are often associated with oral isotretinoin treatment [17,18].
Isotretinoin is the only drug that acts on all the etiopathogenic factors of acne vulgaris and is the only monotherapy that provides prolonged remission or cure in up to 80% of patients [1]. The indications for isotretinoin are severe acne (conglobate or nodular-cystic) and moderate acne (nodular-cystic or papular-pustular), refractory to initial treatments, a tendency to scarring, significant emotional impairment, or impaired social functions [1,2]. The dose used in these conditions is 0.5–1.0 mg/kg/day for 16–24 weeks to a cumulative dose of 120–140 mg/kg or until complete regression of the lesions. An alternative approach with lower daily doses, such as 0.1–0.5 mg/day (up to 5 mg), has been proposed for 18 months or up to 1–2 months after lesion resolution, as this schedule seems to be associated with less adverse events, better tolerability, and recurrence rates similar to those observed with the conventional dose [1,15].
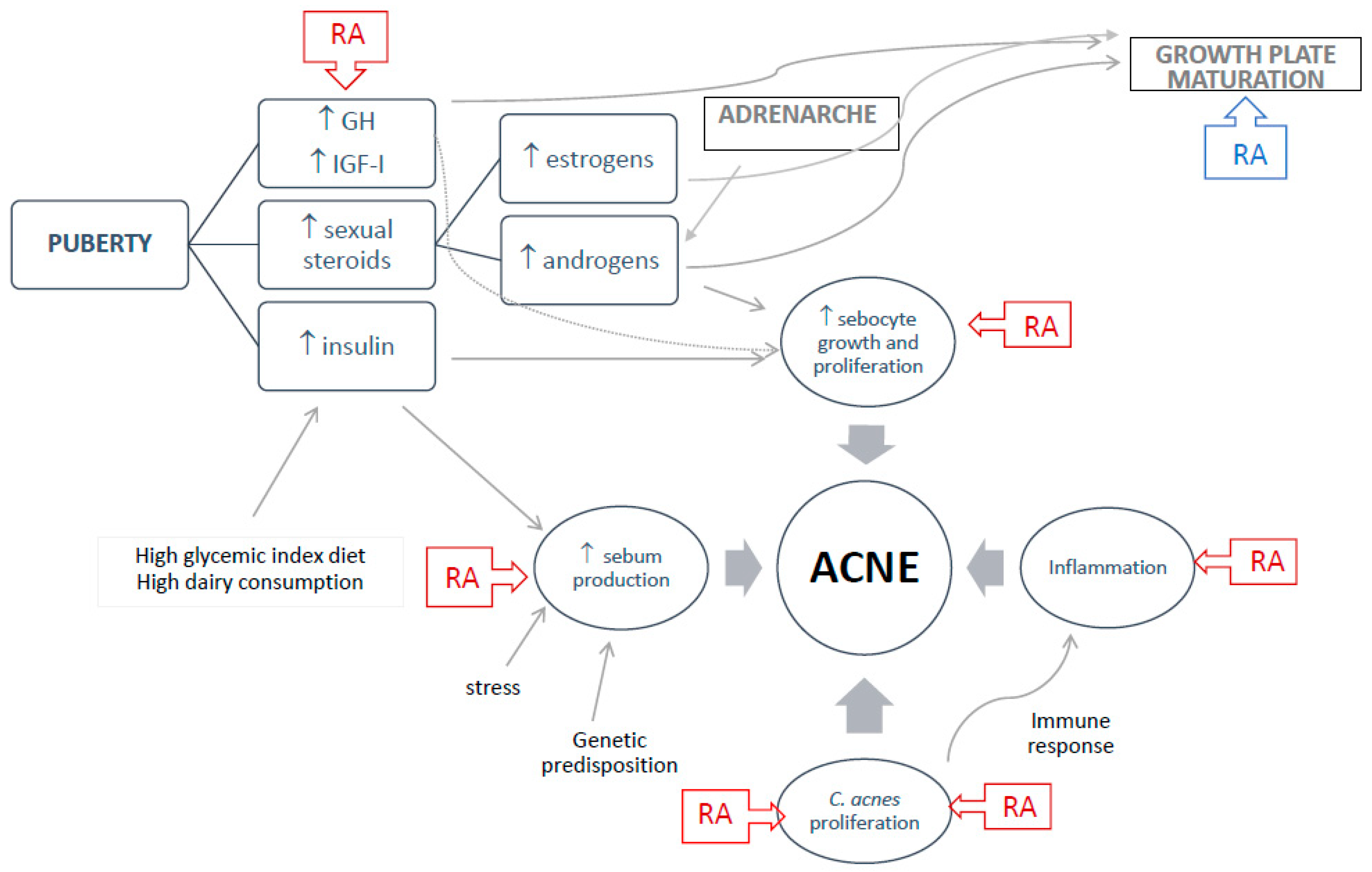
GH physiologically increases pancreatic insulin secretion and circulating insulin, which, in turn, induces hepatic IGF-I secretion. Both IGF-I and insulin levels increase during puberty and are influenced by high glycemic index diets and dairy protein consumption [2]. It was proposed that higher cumulative isotretinoin doses could influence acne pathogenesis through a reduction in IGF-I levels [19]. In a case-control prospective study, it was demonstrated that IGF-I levels and acne severity were significantly higher in patients younger than 21 years when compared to those older than 21 years, while IGF-I, insulin, and glucose levels were not different between the patients and controls [9]. Therefore, it has been suggested that drugs that act to reduce IGF-I and insulin levels could be effective in the treatment of acne vulgaris. Figure 1 summarizes the pathogenesis of acne vulgaris and the action of oral isotretinoin.
Although many of the adverse effects of isotretinoin in pediatric patients are transient, its actions on the GH-IGF-I axis and proapoptotic effects have the potential to promote premature epiphyseal closure with a negative impact on linear growth and final adult height [20,21,22,23,24]. In this narrative review, we have summarized the main studies evaluating the effects of oral isotretinoin therapy on the growth plate, GH-IGF-I axis, and other hormones during childhood and adolescence.
2. Methods
A comprehensive and non-systematic search was carried out in the PubMed, LILACS, and SciELO databases up to December 2022, using the terms retinoid, retinoic acid, isotretinoin, acne vulgaris, growth plate, growth, and epiphyseal closure. The publications were critically selected by the authors.
3. Normal Growth, Adrenarche, and Puberty
Normal human growth is a very dynamic process with partly overlapping phases that include fetal growth, the infancy phase, childhood, and puberty [25]. The amount of GH and IGF-I secreted changes throughout each of these periods. Fetal growth is very fast during the first trimester of gestation, but GH is not essential for fetal growth, as evidenced by the normal or slightly reduced size at birth of children with GH deficiency or GH resistance [26,27]. The IGFs and insulin are, indeed, the major determinants of intense fetal growth, with insulin controlling hepatic IGF-I production in response to nutritional status.
The infancy phase, considered a continuation of fetal growth and mainly dependent on nutrition, ends at about 3–4 years of age. After a normal full-term birth, growth during the first year of life is extremely rapid, leading to a 50% increase in body length. This impressive growth velocity declines to one-third by 10 months of age and continues to decline until 3–4 years of life. Full GH-dependence of IGF-I production does not occur until the second year of postnatal life [28,29,30,31].
The beginning of the childhood period is marked by the resumption of significant GH action, promoting a new phase of growth acceleration [30]. During the prepubertal period, GH secretion rates are similar in boys and girls and a slow deceleration of growth is observed [32]. Puberty is characterized by an increase in growth velocity and the pubertal growth spurt, which is then followed by deceleration until growth stops completely with the closing of the epiphyseal growth plates. GH and IGF-I are fundamental regulators of longitudinal bone growth and have interdependent roles in the regulation of growth and skeletal function. A marked increase in the GH secretion rate, GH pulse amplitudes, and sensitivity to GH occur during puberty in a gender-specific way [32,33], followed by an increase in IGF-I serum concentrations [34,35]. After puberty, GH and IGF-I levels fall with increasing age [34].
Puberty is a complex physiological process of developmental changes regulated by multiple genetic and hormonal pathways. During puberty, adolescents reach sexual maturity and become capable of reproduction [36]. Luteinizing hormone (LH) and follicular stimulating hormone (FSH) are released from the pituitary gland in a pulsatile manner in response to hypothalamic gonadotrophin-releasing hormone (GnRH) stimulation. The number and amplitude of pulses increase at puberty, and there is an augmentation in the production of sex steroid hormones, primarily estrogens in girls and androgens in boys [36]. Puberty onset usually occurs after 8 years of age (range 8–13 years) in girls, and the development of breast tissue (Tanner staging B2) is its clinical marker. In boys, a testicular volume greater than 4 mL is the marker of puberty onset, between 9 and 14 years of age [36]. The pubertal spurt commonly starts at B2 in girls and at a testicular volume of around 10 mL in boys [36].
Many of the growth events during puberty are mediated by estrogens produced both by the ovaries and the peripheral conversion of androgens by aromatase. Estrogen is primarily responsible for the increase in GH secretion by the pituitary at puberty, mainly by increasing the GH pulse amplitude. In both girls and boys, growth acceleration correlates with a rise in circulating estrogen levels. However, rising testosterone levels have also been shown to directly increase GH secretion [36], and it is thought that testosterone itself may also contribute to bone formation via a direct effect on chondrocytes [37].
Around 6 to 8 years of age, a process known as adrenarche occurs: the zona reticularis of the adrenal cortex develops, and the ACTH-dependent production of weak androgen starts, specifically dehydroepiandrosterone (DHEA) and its sulphate (DHEAS) and androstenedione [38,39]. These androgens contribute to sebaceous and apocrine gland development. Signs of adrenarche are the development of body odor, greasy hair, mild acne, axillary, and pubic hair [36,38,39]. These weak androgens stimulate longitudinal epiphyseal growth and appear to stimulate osteoblast proliferation by interleukin-6 inhibition and IGF-I stimulation, in contrast to estrogens, which accelerate epiphyseal chondrocyte maturation and senescence leading to epiphyseal fusion [37,39]. Adrenal androgens are presumably involved in bone maturation before pubertal onset [36,38,39].
4. Growth Plate Regulation
Longitudinal growth is determined by the elongation of the long bones through the growth plates. The growth plate, or physis, is a highly organized cartilaginous portion at the ends of the long bones and is responsible for longitudinal bone growth during development driven by a process of chondrocyte proliferation, hypertrophy, and subsequent matrix deposition [40]. At skeletal maturity, the growth plates are replaced by bone.
The growth plate is organized into distinct zones, each zone with a unique morphology and function and under the regulatory control of local and systemic factors, such as extracellular matrix (ECM) proteins, GH, IGF-I, parathyroid hormone-related protein (PTHrP), thyroid hormone, glucocorticoids, androgens, and estrogens [40,41]. The chondrocytes produce ECM and enzymes that control the mineralization and migration of osteoblasts and osteoclasts, coordinating their own death. Bone formation starts with prechondrogenic mesenchymal cells, which differentiate into proliferative chondrocytes and metabolically active hypertrophic chondrocytes. The ECM is mainly composed of type-II collagen and aggrecan, a large proteoglycan. It is replaced by type-X collagen when proliferative chondrocytes differentiate into hypertrophic chondrocytes [37,41,42].
Retinoic acid is important in growth plate homeostasis, controlling signaling pathways such as fibroblast growth factors (FGF), the wingless/int-1 (Wnt)/β-catenin signaling pathway, bone morphogenic proteins (BMP), and sonic hedgehog protein (Shh). Retinoic acid binds to RAR and RXR and downregulates the transcription of genes that inhibit cartilage growth and differentiation, skeletal growth, matrix homeostasis, and growth plate function in postnatal mice. RARγ was demonstrated to be expressed specifically in the growth plate, from the proliferative zone to the hypertrophic zone [42,43]. Its activation downregulates type-II collagen and aggrecan synthesis. Retinoic acid also suppresses the secretion of FGF23 by osteoblasts and osteocytes, leading to an increase in calcitriol synthesis, which in turn reduces chondrocyte proliferation [44].
The activation of FGF-receptor 3 (FGFR3) by FGF9 and FGF18 inhibits chondrocyte proliferation and limits the lengthening of the long bones. FGFR3 induces premature exit of proliferating chondrocytes into hypertrophy and enhances bone formation [41]. Cellular communication network factor 2 (CCN2) has a significant role in matrix remodeling, osteoclastogenesis, and angiogenesis during development and is particularly sensitive to retinoic acid signaling [42].
A recent clinical case report has given support for the hypothesis that elevated retinoic acid concentrations accelerate bone and dental maturation in humans [45]. The patient was a 10-year-old prepubertal boy with retinal scarring, photophobia, autism spectrum disease, markedly advanced bone age, and accelerated dental development. He was born full term after an uncomplicated pregnancy and delivery, with a birth weight of 2.98 kg [−1.3 standard deviation score (SDS)] and birth length of 46 cm (−2.3 SDS). At the physical exam, he had pubic hair Tanner II, a testicular size of 3–4 mL bilaterally, and no gynecomastia. He presented with low serum vitamin A and elevated total and 13-cis-retinoc acid concentrations and a 3-year advance in bone age, which was advanced in relation to the chronological age without elevated estrogen levels. This syndrome was associated with a deletion on chromosome 10q23, which included the genes of the major retinoic acid-metabolizing enzymes [45].
5. Isotretinoin Effects on Bone and Growth Plate
The skeletal effects of oral retinoid therapy have been described, including hyperostotic changes or tendon and ligament calcification, reduced bone density, osteoporosis, and premature epiphyseal closure [46,47], with susceptibility to adverse effects associated with the retinoid dose, duration of therapy, and age of exposure. Although children and adolescents are obviously the populations at risk for premature growth plate closure, they appear to be relatively free from hyperostosis [48]. Table 1 summarizes the main studies evaluating the effects of retinoids on bone and growth.
Physiologic growth plate closure occurs at different ages among boys and girls during pubertal development. Magnetic resonance imaging showed that 50% of girls had fused growth plates at 14–17 years, and 90% of them fused at 15–18 years. For the boys, 50% and 90% had fused growth plates by 15–18 and 17–20 years, respectively [61]. Thus, chronological age is not a reliable criterion to define the end of longitudinal growth, and adolescents with open growth plates might be susceptible to premature closure related to isotretinoin. Premature epiphysiodesis is a labeled side effect of isotretinoin, related to the dose, age of exposure, and treatment duration, with more pronounced effects in young individuals exposed to higher doses [46].
Premature epiphysiodesis was previously reported during treatment with high doses of isotretinoin for pediatric neuroblastoma [16,48], though premature epiphyseal closure was also reported in young patients treated with oral isotretinoin for acne [16]. The first case report was a 14-year-old boy treated with a 6-month single course of isotretinoin (0.75 mg/kg/day) for cystic acne. He reported bilateral knee pain during isotretinoin use, and 12 months after, he presented pain and valgus deformity of his right knee. An X-ray confirmed the valgus deformity and closure of the lateral femoral physis [53]. The second case was a 16-year-old boy with knee pain and a previous 6-month single course of isotretinoin (0.5 mg/kg/day) for acne refractory to topical treatments. The knee X-ray was normal, but magnetic resonance imaging (MRI) revealed acute epiphysiodesis lesions with irregular epiphyseal cartilage associated with a marked metaphyseal-epiphyseal oedema, which was more severe on the left knee. The treatment was stopped, and the pain disappeared over two months [55]. Both authors did not report the growth velocity, height, or pubertal staging of the patients.
More recently, Delgado et al. published a study of 20 survivors of high-risk neuroblastoma (9.46–16.03 years) in complete remission and 20 matched, healthy controls (10.36–14.11 years), with 7 females and 13 males in each group. Isotretinoin was a standard treatment for high-risk neuroblastoma (mean cumulative dose: 8540 mg). In the high-risk neuroblastoma group, 10 patients were prepubertal, 11 (55%) received GH therapy due to GH deficiency, of which 6 were considered good responders. The height and weight z-scores were markedly lower in the high-risk neuroblastoma survivors, whereas the body mass index z-scores did not differ significantly. Three high-risk neuroblastoma boys had bony bridges involving less than 25% of the physis, and nine high-risk neuroblastoma participants had femoral metaphyseal tongues on MRI. Diffusion tensor imaging (DTI), used to evaluate physeal and metaphyseal structure and function, revealed physeal abnormalities correlated with short stature in the patients [62]. It is important to note that other factors, such as radiotherapy used in the treatment of these patients, may also be involved with these findings.
Retinoic acid may impact the growth plate with histological changes, through the enhancement of cartilage matrix degradation, a loss of chondrocytes in the epiphyseal cartilage, and invasion by osteoclasts, followed by apoptosis and endochondral ossification [16,63]. On the other hand, recently, a histopathological study revealed a loss of columnar organization in the growth plate with scattered cells, without signs of apoptosis, suggesting that retinoids might affect the growth plate cartilage and induce epiphyseal closure without apoptosis [22]. Other skeletal events have been associated with isotretinoin. Arthralgia is a common complaint, and the knee seems to be the most affected joint, both the tibial and femoral epiphysis. Effects on the elbow and ankle were also described [50]. Patients may experience asymmetric epiphyseal growth plate arrest with a valgus deformity, suggesting that the pathophysiology of the arrest favors the lateral aspect of the growth plate [55]. Calcium, phosphorus, and alkaline phosphatase serum levels are normal during premature epiphysiodesis and are not good parameters to evaluate the effects of treatment on bone health [49].
Interestingly, despite the closure of the growth plate in the lower extremity bones, a radiograph of the hand and the wrist for bone age assessment might be normal for chronological age, indicating that conventional methods of determining bone age are inadequate when evaluating growth in patients treated with retinoids [16,57]. This is an important clinical problem because bone age is, traditionally, a marker of bone maturation that indicates the stage of endochondral maturation at the epiphysis and growth assessed by radiography of the hands and wrists. In this setting, radiographic bone age can give a false idea that growth is not being compromised. Therefore, X-ray follow-up is not recommended for children and adolescents taking retinoids for acne treatment. If growth velocity reduction and poor longitudinal growth occur, a detailed examination of the patient’s medical history and magnetic resonance scans to diagnose partial fusion of the epiphyseal cartilage are needed. Withdrawal of the drug should alleviate the pain and allow normal growth in cases where the growth plate is not totally closed [55]. Surprisingly, despite all these reports and considerations and knowing that acne vulgaris occurs more frequently in teenagers during puberty, growth assessment is not usually recommended as part of the clinical evaluation of adolescents on isotretinoin therapy for acne [1,15,17].
6. Isotretinoin Effects on GH-IGF-I Axis and Pituitary Hormones
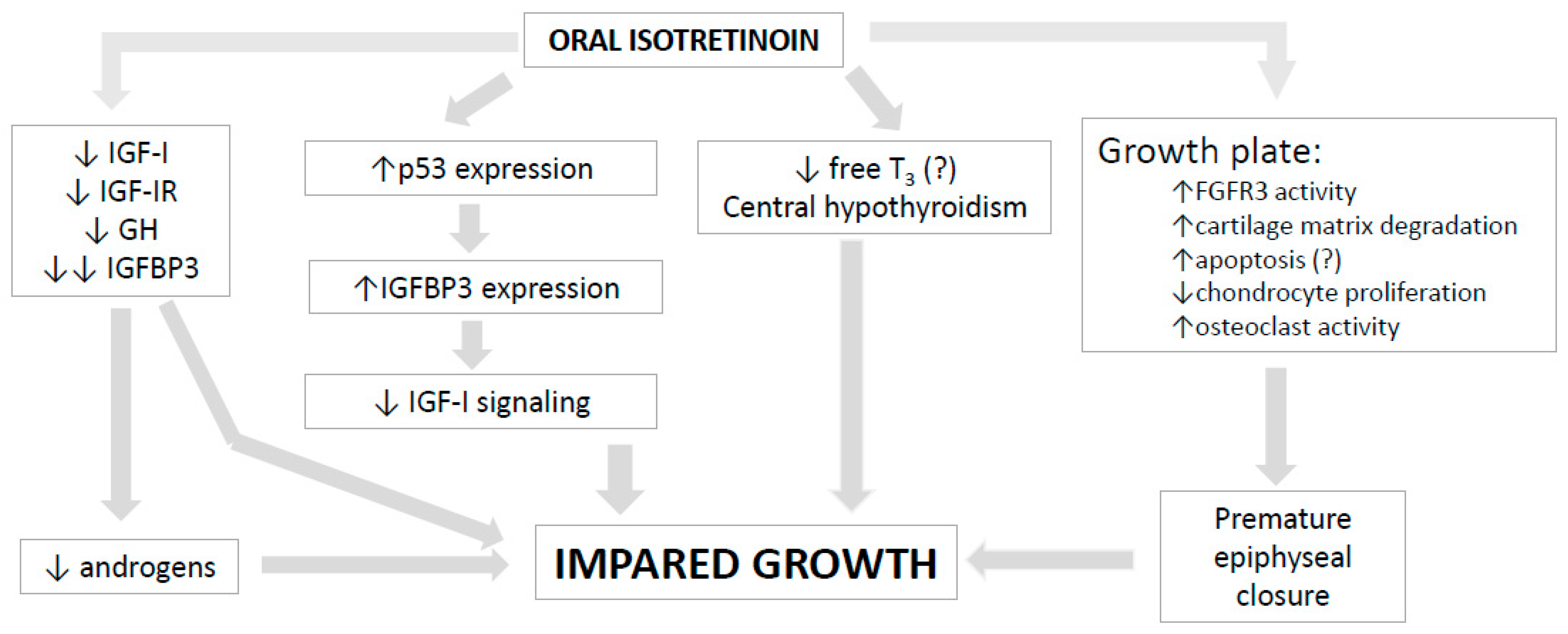
Therapy with oral isotretinoin may interfere with GH physiology, but the data are scarce. Oral isotretinoin upregulates the expression of p53, which inhibits the expression of androgen receptors and IGF-IR and induces the expression of IGF-binding protein 3 (IGFBP3). It is well known that GH and IGF-I stimulate cell proliferation and inhibit apoptosis, while in contrast, IGFBP3 and some proteases exert antiproliferative and proapoptotic effects [6]. IGFBP3 binds to RXRα and leads to the modulation of its transcriptional activity, which is essential for mediating the effects of IGFBP3 on apoptosis [7,64]. The p53-mediated induction of IGFBP3 gene expression inhibits mitogenic IGF-I signaling [64].
Twenty 3-week-old male rats were randomly divided into a control group and an experimental group (n = 10). The experimental rats were treated by gavage with high-dose ATRA for 10 days. After this period, the experimental rats exhibited a lower body weight and shorter nasal-tail and radial tibial length than the controls. CYP26B1 enzyme activity in the liver was elevated, and histopathological staining revealed a narrowed cartilaginous epiphyseal plate, a sparse medullary cavity of trabecular bone, fewer trabecular bones, and advanced bone marrow mineralization. The circulating GH, IGF-I, and IGFBP3 levels decreased. The authors concluded that high-dose ATRA intake over a brief period reduces GH, IGF-I, and IGFBP3 levels, affects cartilage and bone homeostasis, and inhibits bone growth in developing animals [65].
Karadag et al. studied the effect of isotretinoin on the GH-IGF-I axis in 47 patients (15–40 years) with acne. The therapy was initiated at a dose of 0.5–0.75 mg/kg/day and adjusted to 0.88 mg/kg/day as a maintenance dosage after 1 month. After 3 months of treatment, the IGF-I and IGFBP3 levels significantly decreased, while the mean basal GH levels did not change [19]. In another study of the same group of researchers including 105 patients with acne (14–42 years), the participants were divided into three groups based on the isotretinoin dose: 0.5–1.0 mg/kg/day (high dose—group 1), 0.2–0.5 mg/kg/day (low dose—group 2), and an intermittent 0.5–1.0 mg/kg/day only one week per month (intermittent dose—group 3). After 3 months of therapy, the isotretinoin significantly reduced the IGF-I and random GH levels in groups 1 and 2, and these effects were more pronounced in the high-dose group. The IGFBP3 levels were significantly reduced in all three groups, and the weakest effect was seen in the intermittent-dose group [66]. The total testosterone and cortisol levels decreased, and the sex hormone-binding globulin (SHBG) levels increased significantly in the three groups after therapy. Moreover, significant reductions in the LH, prolactin, ACTH, cortisol, and free triiodothyronine (fT3) levels were also observed in the low- and high-dose groups but not in the intermittent group, while the FSH and TSH did not change [66]. On the other hand, Rodighiero et al. did not show a significant reduction in the IGF-I levels in a group of 10 patients (14–30 years) with severe acne treated with progressive doses of oral isotretinoin up to a cumulative dose of 120 mg/kg after 3 months [67]. In this study, the other 36 patients with acne vulgaris received other therapies following the European Dermatology Forum guidelines, and in the whole group, the IGF-I levels were higher in the patients than in the controls but with no significant variation after treatment [67]. Similar findings of the association between acne severity and IGF-I levels were also reported by other investigators in smaller studies with a brief period of observation including patients within a wide range of ages [68,69,70].
Bexarotene, a synthetic RXR-selective retinoid, causes central hypothyroidism, and high doses of levothyroxine are required for its treatment. This synthetic retinoid seems to suppress TSH production and increase thyroid hormone degradation by a non-deiodinase-mediated pathway [71]. Decreases in fT3 levels may be caused by the RXR-mediated suppression of TSH gene expression, and reversible hypothyroidism was previously shown [3,71,72]. A decrease in fT3 can lead to impaired growth during puberty, but more studies are needed to prove these effects of isotretinoin on the hypothalamic–pituitary–thyroid axis.
The mechanisms of the possible actions of oral isotretinoin on growth and final height are shown in Figure 2.
7. Conclusions
Isotretinoin might cause growth impairment by inducing premature fusion of the growth plates, which seems to be associated with younger age, incremental doses, and the duration of the therapy, beyond individual susceptibility. The GH-IGF-I axis and other hormones may be affected during treatment, but further research is necessary to determine the magnitude and consequences of this effect and the participation of the different players. Moderate and severe acne, skeletal deformities, reduced longitudinal growth, and impaired final adult height may cause psychological and self-esteem problems in adolescents and young adults. Since the effects of the selected doses of isotretinoin for the treatment of acne on the growth plate and longitudinal growth are not clear yet, we recommend careful discussion of the negative effects and benefits of this treatment with patients and parents. If there is any concern about adult height, the use of isotretinoin should be avoided during childhood and adolescence as much as possible to preserve the height potential.
Author Contributions
Conceptualization, A.A.C.-D., C.L.B. and M.C.S.B.; acquisition, analysis, or interpretation of the data, M.C.S.B. and A.A.C.-D.; writing—original draft preparation, A.A.C.-D.; writing—review and editing, A.A.C.-D., C.L.B. and M.C.S.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
No new data were created in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bagatin, E.; Costa, C.S.; Rocha, M.; Picosse, F.R.; Kamamoto, C.S.L.; Pirmez, R.; Ianhez, M.; Miot, H.A. Consensus on the use of oral isotretinoin in dermatology-Brazilian Society of Dermatology. An. Bras. Dermatol. 2020, 95 (Suppl. 1), 19–38. [Google Scholar] [CrossRef] [PubMed]
- Habeshian, K.A.; Cohen, B.A. Current Issues in the Treatment of Acne Vulgaris. Pediatrics 2020, 145 (Suppl. 2), S225–S230. [Google Scholar] [CrossRef] [PubMed]
- Karadag, A.S.; Ertugrul, D.T.; Tutal, E.; Akin, K.O. Isotretinoin influences pituitary hormone levels in acne patients. Acta Derm. Venereol. 2011, 91, 31–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- George, R.; Clarke, S.; Thiboutot, D. Hormonal therapy for acne. Semin. Cutan. Med. Surg. 2008, 27, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Lolis, M.S.; Bowe, W.P.; Shalita, A.R. Acne and systemic disease. Med. Clin. N. Am. 2009, 93, 1161–1181. [Google Scholar] [CrossRef]
- Boguszewski, C.L.; Boguszewski, M. Growth Hormone’s Links to Cancer. Endocr. Rev. 2019, 40, 558–574. [Google Scholar] [CrossRef]
- Feily, A.; Namazi, M.R. Decrease of insulin growth factor-1 as a novel mechanism for anti-androgen effect of isotretinoin and its reported association with depression in some cases. J. Drugs Dermatol. 2011, 10, 793–794. [Google Scholar]
- Zouboulis, C.C.; Jourdan, E.; Picardo, M. Acne is an inflammatory disease and alterations of sebum composition initiate acne lesions. J. Eur. Acad. Dermatol. Venereol. 2014, 28, 527–532. [Google Scholar] [CrossRef]
- Kara, Y.A. Evaluation of serum insulin-like growth factor-1, insulin, glucose levels in patients with adolescent and post-adolescent acne. J. Cosmet. Dermatol. 2022, 21, 1292–1296. [Google Scholar] [CrossRef]
- Smith, T.M.; Gilliland, K.; Clawson, G.A.; Thiboutot, D. IGF-1 induces SREBP-1 expression and lipogenesis in SEB-1 sebocytes via activation of the phosphoinositide 3-kinase/Akt pathway. J. Investig. Dermatol. 2008, 128, 1286–1293. [Google Scholar] [CrossRef] [Green Version]
- Ben-Amitai, D.; Laron, Z. Effect of insulin-like growth factor-1 deficiency or administration on the occurrence of acne. J. Eur. Acad. Dermatol. Venereol. 2011, 25, 950–954. [Google Scholar] [CrossRef] [PubMed]
- Klinger, B.; Anin, S.; Silbergeld, A.; Eshet, R.; Laron, Z. Development of hyperandrogenism during treatment with insulin-like growth factor-I (IGF-I) in female patients with Laron syndrome. Clin. Endocrinol. 1998, 48, 81–87. [Google Scholar] [CrossRef]
- Berbis, P. Retinoids: Mechanisms of action. Ann. Dermatol. Venereol. 2010, 137 (Suppl. 3), S97–S103. [Google Scholar] [CrossRef]
- Zaenglein, A.L.; Levy, M.L.; Stefanko, N.S.; Benjamin, L.T.; Bruckner, A.L.; Choate, K.; Craiglow, B.G.; DiGiovanna, J.J.; Eichenfield, L.F.; Elias, P.; et al. Consensus recommendations for the use of retinoids in ichthyosis and other disorders of cornification in children and adolescents. Pediatr. Dermatol. 2021, 38, 164–180. [Google Scholar] [CrossRef] [PubMed]
- Rademaker, M. Isotretinoin: Dose, duration and relapse. What does 30 years of usage tell us? Australas. J. Dermatol. 2013, 54, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Alazawi, S.; Hendriksz, T. Analysis of the effects of isotretinoin on the premature epiphyseal closure in pediatric populations: A literature review. J. Osteopath Med. 2022, 122, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Bagatin, E.; Costa, C.S. The use of isotretinoin for acne-an update on optimal dosing, surveillance, and adverse effects. Expert Rev. Clin. Pharmacol. 2020, 13, 885–897. [Google Scholar] [CrossRef]
- Melnik, B.C. Apoptosis May Explain the Pharmacological Mode of Action and Adverse Effects of Isotretinoin, Including Teratogenicity. Acta Derm. Venereol. 2017, 97, 173–181. [Google Scholar] [CrossRef] [Green Version]
- Karadag, A.S.; Ertugrul, D.T.; Tutal, E.; Akin, K.O. Short-term isotretinoin treatment decreases insulin-like growth factor-1 and insulin-like growth factor binding protein-3 levels: Does isotretinoin affect growth hormone physiology? Br. J. Dermatol. 2010, 162, 798–802. [Google Scholar] [CrossRef]
- Pease, C.N. Focal retardation and arrestment of growth of bones due to vitamin A intoxication. JAMA 1962, 182, 980–985. [Google Scholar] [CrossRef]
- Kodaka, T.; Takaki, H.; Soeta, S.; Mori, R.; Naito, Y. Local disappearance of epiphyseal growth plates in rats with hypervitaminosis A. J. Vet. Med. Sci. 1998, 60, 815–821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuoka, M.; Onodera, T.; Majima, T.; Iwasaki, K.; Takahashi, D.; Kondo, E.; Iwasaki, N. Correction osteotomy for bilateral varus knee deformity caused by premature epiphyseal closure induced by hypervitaminosis A: A case report. BMC Musculoskelet. Disord. 2019, 20, 287. [Google Scholar] [CrossRef] [Green Version]
- Carroll Woodard, J.; Donovan, A.G.; Eckhoff, C. Vitamin (A and D)-induced premature physeal closure (hyena disease) in calves. J. Comp. Pathol. 1997, 116, 353–366. [Google Scholar] [CrossRef] [PubMed]
- Woodard, J.C.; Donovan, G.A.; Fisher, L.W. Pathogenesis of vitamin (A and D)-induced premature growth-plate closure in calves. Bone 1997, 21, 171–182. [Google Scholar] [CrossRef] [PubMed]
- Karlberg, J. On the modelling of human growth. Stat. Med. 1987, 6, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Aguiar-Oliveira, M.H.; Souza, A.H.O.; Oliveira, C.R.P.; Campos, V.C.; Oliveira-Neto, L.A.; Salvatori, R. Mechanisms in Endocrinology: The multiple facets of GHRH/GH/IGF-I axis: Lessons from lifetime, untreated, isolated GH deficiency due to a GHRH receptor gene mutation. Eur. J. Endocrinol. 2017, 177, R85–R97. [Google Scholar] [CrossRef] [Green Version]
- Laron, Z. Lessons from 50 Years of Study of Laron Syndrome. Endocr. Pract. 2015, 21, 1395–1402. [Google Scholar] [CrossRef]
- Bernardini, S.; Spadoni, G.L.; Povoa, G.; Boscherini, B.; Hall, K. Plasma levels of insulin-like growth factor binding protein-1, and growth hormone binding protein activity from birth to the third month of life. Acta Endocrinol. 1992, 127, 313–318. [Google Scholar] [CrossRef]
- Bozzola, M.; Tettoni, K.; Locatelli, F.; Radetti, G.; Belloni, C.; Autelli, M.; Zecca, M.; Valentini, R.; Severi, F.; Tato, L. Postnatal variations of growth hormone bioactivity and of growth hormone-dependent factors. Arch. Pediatr. Adolesc. Med. 1996, 150, 1068–1071. [Google Scholar] [CrossRef]
- Low, L.C.; Tam, S.Y.; Kwan, E.Y.; Tsang, A.M.; Karlberg, J. Onset of significant GH dependence of serum IGF-I and IGF-binding protein 3 concentrations in early life. Pediatr. Res. 2001, 50, 737–742. [Google Scholar] [CrossRef] [Green Version]
- Ong, K.; Kratzsch, J.; Kiess, W.; Dunger, D.; Team, A.S. Circulating IGF-I levels in childhood are related to both current body composition and early postnatal growth rate. J. Clin. Endocrinol. Metab. 2002, 87, 1041–1044. [Google Scholar] [CrossRef] [PubMed]
- Albertsson-Wikland, K.; Rosberg, S.; Karlberg, J.; Groth, T. Analysis of 24-hour growth hormone profiles in healthy boys and girls of normal stature: Relation to puberty. J. Clin. Endocrinol. Metab. 1994, 78, 1195–1201. [Google Scholar] [CrossRef] [PubMed]
- Coutant, R.; de Casson, F.B.; Rouleau, S.; Douay, O.; Mathieu, E.; Gatelais, F.; Bouhours-Nouet, N.; Voinot, C.; Audran, M.; Limal, J.M. Divergent effect of endogenous and exogenous sex steroids on the insulin-like growth factor I response to growth hormone in short normal adolescents. J. Clin. Endocrinol. Metab. 2004, 89, 6185–6192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juul, A.; Bang, P.; Hertel, N.T.; Main, K.; Dalgaard, P.; Jorgensen, K.; Muller, J.; Hall, K.; Skakkebaek, N.E. Serum insulin-like growth factor-I in 1030 healthy children, adolescents, and adults: Relation to age, sex, stage of puberty, testicular size, and body mass index. J. Clin. Endocrinol. Metab. 1994, 78, 744–752. [Google Scholar] [CrossRef]
- Lofqvist, C.; Andersson, E.; Gelander, L.; Rosberg, S.; Blum, W.F.; Albertsson Wikland, K. Reference values for IGF-I throughout childhood and adolescence: A model that accounts simultaneously for the effect of gender, age, and puberty. J. Clin. Endocrinol. Metab. 2001, 86, 5870–5876. [Google Scholar] [CrossRef] [Green Version]
- Wood, C.L.; Lane, L.C.; Cheetham, T. Puberty: Normal physiology (brief overview). Best. Pract. Res. Clin. Endocrinol. Metab. 2019, 33, 101265. [Google Scholar] [CrossRef]
- Nilsson, O.; Marino, R.; De Luca, F.; Phillip, M.; Baron, J. Endocrine regulation of the growth plate. Horm. Res. 2005, 64, 157–165. [Google Scholar] [CrossRef]
- Biro, F.M.; Pinney, S.M.; Huang, B.; Baker, E.R.; Walt Chandler, D.; Dorn, L.D. Hormone changes in peripubertal girls. J. Clin. Endocrinol. Metab. 2014, 99, 3829–3835. [Google Scholar] [CrossRef] [Green Version]
- Rosenfield, R.L. Normal and Premature Adrenarche. Endocr. Rev 2021, 42, 783–814. [Google Scholar] [CrossRef]
- D’Andrea, C.R.; Alfraihat, A.; Singh, A.; Anari, J.B.; Cahill, P.J.; Schaer, T.; Snyder, B.D.; Elliott, D.; Balasubramanian, S. Part 1. Review and meta-analysis of studies on modulation of longitudinal bone growth and growth plate activity: A macro-scale perspective. J. Orthop. Res. 2021, 39, 907–918. [Google Scholar] [CrossRef]
- Agirdil, Y. The growth plate: A physiologic overview. EFORT Open Rev. 2020, 5, 498–507. [Google Scholar] [CrossRef]
- Shimo, T.; Koyama, E.; Okui, T.; Masui, M.; Kunisada, Y.; Ibaragi, S.; Yoshioka, N.; Kurio, N.; Yoshida, S.; Sasaki, A.; et al. Retinoic Receptor Signaling Regulates Hypertrophic Chondrocyte-specific Gene Expression. Vivo 2019, 33, 85–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Luca, F.; Uyeda, J.A.; Mericq, V.; Mancilla, E.E.; Yanovski, J.A.; Barnes, K.M.; Zile, M.H.; Baron, J. Retinoic acid is a potent regulator of growth plate chondrogenesis. Endocrinology 2000, 141, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Rausch, S.; Barholz, M.; Foller, M.; Feger, M. Vitamin A regulates fibroblast growth factor 23 (FGF23). Nutrition 2020, 79–80, 110988. [Google Scholar] [CrossRef]
- Nilsson, O.; Isoherranen, N.; Guo, M.H.; Lui, J.C.; Jee, Y.H.; Guttmann-Bauman, I.; Acerini, C.; Lee, W.; Allikmets, R.; Yanovski, J.A.; et al. Accelerated Skeletal Maturation in Disorders of Retinoic Acid Metabolism: A Case Report and Focused Review of the Literature. Horm. Metab. Res. 2016, 48, 737–744. [Google Scholar] [CrossRef] [Green Version]
- DiGiovanna, J.J. Isotretinoin effects on bone. J. Am. Acad. Dermatol. 2001, 45, S176–S182. [Google Scholar] [CrossRef] [PubMed]
- DiGiovanna, J.J.; Langman, C.B.; Tschen, E.H.; Jones, T.; Menter, A.; Lowe, N.J.; Eichenfield, L.; Hebert, A.A.; Pariser, D.; Savin, R.P.; et al. Effect of a single course of isotretinoin therapy on bone mineral density in adolescent patients with severe, recalcitrant, nodular acne. J. Am. Acad. Dermatol. 2004, 51, 709–717. [Google Scholar] [CrossRef]
- Duvalyan, A.; Cha, A.; Goodarzian, F.; Arkader, A.; Villablanca, J.G.; Marachelian, A. Premature epiphyseal growth plate arrest after isotretinoin therapy for high-risk neuroblastoma: A case series and review of the literature. Pediatr. Blood Cancer 2020, 67, e28236. [Google Scholar] [CrossRef]
- Milstone, L.M.; McGuire, J.; Ablow, R.C. Premature epiphyseal closure in a child receiving oral 13-cis-retinoic acid. J. Am. Acad. Dermatol. 1982, 7, 663–666. [Google Scholar] [CrossRef]
- Prendiville, J.; Bingham, E.A.; Burrows, D. Premature epiphyseal closure–a complication of etretinate therapy in children. J. Am. Acad. Dermatol. 1986, 15, 1259–1262. [Google Scholar] [CrossRef]
- Marini, J.C.; Hill, S.; Zasloff, M.A. Dense metaphyseal bands and growth arrest associated with isotretinoin therapy. Am. J. Dis. Child. 1988, 142, 316–318. [Google Scholar] [CrossRef]
- Standeven, A.M.; Davies, P.J.; Chandraratna, R.A.; Mader, D.R.; Johnson, A.T.; Thomazy, V.A. Retinoid-induced epiphyseal plate closure in guinea pigs. Fundam. Appl. Toxicol. 1996, 34, 91–98. [Google Scholar] [CrossRef]
- Steele, R.G.; Lugg, P.; Richardson, M. Premature epiphyseal closure secondary to single-course vitamin A therapy. Aust. N. Z. J. Surg. 1999, 69, 825–827. [Google Scholar] [CrossRef] [PubMed]
- Hobbie, W.L.; Mostoufi, S.M.; Carlson, C.A.; Gruccio, D.; Ginsberg, J.P. Prevalence of advanced bone age in a cohort of patients who received cis-retinoic acid for high-risk neuroblastoma. Pediatr. Blood Cancer 2011, 56, 474–476. [Google Scholar] [CrossRef]
- Luthi, F.; Eggel, Y.; Theumann, N. Premature epiphyseal closure in an adolescent treated by retinoids for acne: An unusual cause of anterior knee pain. Joint. Bone Spine 2012, 79, 314–316. [Google Scholar] [CrossRef]
- Zhao, S.; Goodson, N.J. Diffuse idiopathic skeletal hyperostosis and isotretinoin in cystic acne. BMJ Case Rep. 2015, 2015, bcr2015209775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noyes, J.J.; Levine, M.A.; Belasco, J.B.; Mostoufi-Moab, S. Premature Epiphyseal Closure of the Lower Extremities Contributing to Short Stature after cis-Retinoic Acid Therapy in Medulloblastoma: A Case Report. Horm. Res. Paediatr. 2016, 85, 69–73. [Google Scholar] [CrossRef] [Green Version]
- Steineck, A.; MacKenzie, J.D.; Twist, C.J. Premature physeal closure following 13-cis-retinoic acid and prolonged fenretinide administration in neuroblastoma. Pediatr. Blood Cancer 2016, 63, 2050–2053. [Google Scholar] [CrossRef] [PubMed]
- Park, W.K.; Choi, H.S.; Chung, C.Y.; Park, M.S.; Sung, K.H. Genu varum deformity due to premature epiphyseal closure after treatment with isotretinoin for neuroblastoma: A case report. J. Orthop. Surg. 2020, 28, 2309499020924483. [Google Scholar] [CrossRef]
- Koh, K.N.; Jeon, J.Y.; Park, S.S.; Im, H.J.; Kim, H.; Kang, M.S. Physeal Abnormalities in Children With High-risk Neuroblastoma Intensively Treated With/Without 13-Cis-Retinoic Acid. J. Pediatr. Orthop. 2021, 41, e841–e848. [Google Scholar] [CrossRef]
- Kvist, O.; Luiza Dallora, A.; Nilsson, O.; Anderberg, P.; Sanmartin Berglund, J.; Flodmark, C.E.; Diaz, S. A cross-sectional magnetic resonance imaging study of factors influencing growth plate closure in adolescents and young adults. Acta Paediatr. 2021, 110, 1249–1256. [Google Scholar] [CrossRef]
- Delgado, J.; Jaramillo, D.; Chauvin, N.A.; Guo, M.; Stratton, M.S.; Sweeney, H.E.; Barrera, C.A.; Mostoufi-Moab, S. Evaluating growth failure with diffusion tensor imaging in pediatric survivors of high-risk neuroblastoma treated with high-dose cis-retinoic acid. Pediatr. Radiol. 2019, 49, 1056–1065. [Google Scholar] [CrossRef] [PubMed]
- Horton, W.E.; Yamada, Y.; Hassell, J.R. Retinoic acid rapidly reduces cartilage matrix synthesis by altering gene transcription in chondrocytes. Dev. Biol. 1987, 123, 508–516. [Google Scholar] [CrossRef] [PubMed]
- Melnik, B.C. p53: Key conductor of all anti-acne therapies. J. Transl. Med. 2017, 15, 195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, Q.; Wang, X.; Bai, H.; Tan, X.; Liu, X. Effects of high-dose all-trans retinoic acid on longitudinal bone growth of young rats. Growth Horm. IGF Res. 2022, 62, 101446. [Google Scholar] [CrossRef]
- Karadag, A.S.; Takci, Z.; Ertugrul, D.T.; Bilgili, S.G.; Balahoroglu, R.; Takir, M. The effect of different doses of isotretinoin on pituitary hormones. Dermatology 2015, 230, 354–359. [Google Scholar] [CrossRef]
- Rodighiero, E.; Bertolani, M.; Saleri, R.; Pedrazzi, G.; Lotti, T.; Feliciani, C.; Satolli, F. Do acne treatments affect insulin-like growth factor-1 serum levels? A clinical and laboratory study on patients with acne vulgaris. Dermatol. Ther. 2020, 33, e13439. [Google Scholar] [CrossRef] [PubMed]
- Kaymak, Y.; Adisen, E.; Ilter, N.; Bideci, A.; Gurler, D.; Celik, B. Dietary glycemic index and glucose, insulin, insulin-like growth factor-I, insulin-like growth factor binding protein 3, and leptin levels in patients with acne. J. Am. Acad. Dermatol. 2007, 57, 819–823. [Google Scholar] [CrossRef]
- Smith, T.M.; Cong, Z.; Gilliland, K.L.; Clawson, G.A.; Thiboutot, D.M. Insulin-like growth factor-1 induces lipid production in human SEB-1 sebocytes via sterol response element-binding protein-1. J. Investig. Dermatol. 2006, 126, 1226–1232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahaman, S.M.A.; De, D.; Handa, S.; Pal, A.; Sachdeva, N.; Ghosh, T.; Kamboj, P. Association of insulin-like growth factor (IGF)-1 gene polymorphisms with plasma levels of IGF-1 and acne severity. J. Am. Acad. Dermatol. 2016, 75, 768–773. [Google Scholar] [CrossRef]
- Sherman, S.I. Etiology, diagnosis, and treatment recommendations for central hypothyroidism associated with bexarotene therapy for cutaneous T-cell lymphoma. Clin. Lymphoma 2003, 3, 249–252. [Google Scholar] [CrossRef] [PubMed]
- Masood, M.Q.; Hakeem, H. Isotretinoin associated reversible hypothyroidism. Thyroid 2011, 21, 1039–1040. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Etiopathogenic factors of acne vulgaris and possible action of oral isotretinoin. Notes: IGF-I, insulin-like growth factor I; GH, growth hormone; RA, retinoic acid. Red = inhibition; Blue = acceleration.
Figure 1.
Etiopathogenic factors of acne vulgaris and possible action of oral isotretinoin. Notes: IGF-I, insulin-like growth factor I; GH, growth hormone; RA, retinoic acid. Red = inhibition; Blue = acceleration.

Figure 2.
Potential mechanisms of the actions of oral isotretinoin on growth. Notes: IGF-I, insulin-like growth factor I; IGF-IR, insulin-like growth factor I receptor; GH, growth hormone; IGFBP3, insulin-like growth factor-binding protein 3; T3, triiodothyronine; FGFR3, fibroblast growth factor receptor 3.
Figure 2.
Potential mechanisms of the actions of oral isotretinoin on growth. Notes: IGF-I, insulin-like growth factor I; IGF-IR, insulin-like growth factor I receptor; GH, growth hormone; IGFBP3, insulin-like growth factor-binding protein 3; T3, triiodothyronine; FGFR3, fibroblast growth factor receptor 3.


{kind=link}
{kind=link}
Table 1.
Summary of main studies evaluating the retinoid effects on bone and growth.
| Authors | Study Type | Reason for Retinoid Use | Dose and Duration of Therapy | Main Findings |
|---|---|---|---|---|
| Milstone et al., 1982 [49] | Case report 10-year-old boy | Epidermolytic hyperkeratosis | Oral isotretinoin: 0.5–4.5 mg/kg/day, cycles of 6 months followed by 2- to 4-week periods off drug; total of 4 years | Right knee pain; radiographic evidence of partial closure of the proximal epiphysis of the right tibia |
| Prendiville et al., 1986 [50] | Case reports: Case 1: 8.5-year-old boy Case 2: 11-year-old girl | Case 1: nonbullous ichthyosiform erythroderma Case 2: systematized verrucous nevi | Case 1: etretinate (0.5–2.5 mg/kg/day for 6.3 years) Case 2: etretinate (1 mg/kg/day for 5.4 years) | Case 1: premature growth plate closure of the right distal tibial epiphysis; shortness of stature, thinning of long bones, and traumatic fractures Case 2: bilateral fusion of both elbow epiphyses and precocious narrowing of the upper and lower femoral epiphyses |
| Marini et al., 1988 [51] | Case report: 13-year-old boy | Fibrodysplasia ossificans progressiva | Oral isotretinoin: 4–5 mg/kg/day, for 5 months | Striking growth arrest lines on long bones, metaphysis of upper and lower extremities. 5–9 months after discontinuance: gradual decrease of metaphyseal bands and resumption of clinical growth |
| Standeven et al., 1996 [52] | Animal study: guinea pigs | Experimental study | Intraperitoneal isotretinoin: 21 mg/kg/day for 7 days via osmotic pump | Irreversible histological features of epiphyseal closure |
| Woodard et al., 1997 [24] | Animal study: calves (6 treated and 6 controls) | Experimental study | Intramuscular vitamin A (2,000,000 IU) + vitamin D (300,000 IU) on the first day after birth, and oral vitamin A (10,000 IU/kg/day per 8 weeks), and after oral vitamin A (30,000 IU/kg/day per 8 weeks) | Premature closure of growth plate (proximal and distal tibia, radius, hind, and fore limbs) by microscopical examination in treated animals. After 1 week, bone growth of the proximal tibia of a control animal was 136 μg/day; in the treated animal it was 25 μg/day |
| Kodaka et al., 1998 [21] | Animal study: 5 rats treated and 5 controls | Experimental study | Oral vitamin A: 50,000, 100,000, and 150,000 IU/100 g/day for 5 days from 4 weeks after birth | Premature growth plate disappearance; eosinophilic cartilage bands in higher dose groups |
| Steele et al., 1999 [53] | Case report: 14-year-old boy | Cystic acne | Oral isotretinoin: 75 mg/kg/day for 6 months | Bilateral knee pain, genu valgum; closure of lateral femoral physis |
| Hobbie et al., 2011 [54] | Retrospective review: 32 children (13 girls), 7.4–16.4-year-old | Neuroblastoma | Oral isotretinoin: Group 1 (24 patients): 6 cycles 160 mg/m2/day (2 weeks on, 2 weeks off) Group 2 (8 patients): did not receive isotretinoin | Group 1: advanced bone age in 7 children, 9.5 years (6–10.5) from diagnosis-younger median age at neuroblastoma diagnosis |
| Luthi et al., 2012 [55] | Case report: 16-year-old boy | Acne refractory to topical treatments | Oral isotretinoin: 0.5 mg/kg/day for 7 months | Bilateral knee pain. Knee RM: acute epiphysiodesis lesions with irregular epiphyseal cartilage, and marked metaphyseal-epiphyseal oedema |
| Zhao et al., 2015 [56] | Case report: 35-year-old man | Cystic acne | Oral isotretinoin: 4 cycles of 500 mg/kg/day for 6 months and a final long-term course gradually down-titrated to 20 mg/day from 15-year-old | Thoracic back pain, diffuse idiopathic skeletal hyperostosis |
| Noyes et al., 2016 [57] | Case report: 9-year-old girl | Medulloblastoma | Oral isotretinoin: 11 cycles of 180 mg/m2/day (14-day cycles) for 13 months | Bilateral premature closure of distal femur and proximal tibia growth plates; normal bone age in the hand and wrist |
| Steineck et al., 2016 [58] | Case series: Case A: 6-year-old girl (at diagnosis) Case B: 5-year-old boy (at diagnosis) | Neuroblastoma | Oral fenretide: Case A and B: 2475 mg/m2/day, delivered as 800 mg orally three times daily for 7 days, repeated every 21 days, 70 courses over 5 years (cumulative dose 1212,750 mg/m2) | Premature epiphyseal closure Case A: left knee pain; arm and leg length discrepancy, short adult stature (21-year-old): 154 cm (8th percentile), mid-parental height 172.7 cm (90th percentile). Case B: genu varum; short adult stature (20-year-old): 165 cm (5th percentile), mid-parental height unavailable. |
| Matsuoka et al., 2019 [22] | Case report: 10-year-old girl | Neuroblastoma | Oral isotretinoin: initial dose of 20 mg/day and maintenance dose of 40 mg/day for a total period of 9.8 years from 1 year- old. | Knee pain, bilateral varus knee deformity due to premature epiphyseal closure; polar irregularity of chondrocytes and decreased cartilage matrix without apoptosis by histopathological examination of the growth plate |
| Duvalyan et al., 2019 [48] | Case series: Case A: 9-year-old girl Case B: 11-year-old boy Case C: 10-year-old boy | Neuroblastoma | Oral isotretinoin Case A: 160 mg/m2/day, 2 weeks on, 2 weeks off (cumulative dose: 19,200 mg/m2) Case B and C: 160 mg/m2/day, 2 weeks on, 2 weeks off (cumulative dose: 13,440 mg/m2) | Bilateral knees plate closure Case A: right leg deformity and length discrepancy. Height at the 2.5 percentile (17-year-old) Case B: progressive genu valgum. Height at the 0.06 percentile (14-year-old) Case C: leg length discrepancy. Height at the 4.3 percentile (13-year-old) |
| Park et al., 2020 [59] | Case report: 10-year-old boy | Neuroblastoma | Oral isotretinoin (72.3 mg/m2/day) for 1 year | Genu varum; premature epiphyseal closure |
| Koh et al., 2021 [60] | Case-control study: 15 patients (8 girls): 4.9±1.7 years 12 controls (7 girls): 4.9 ± 1.9 years | Neuroblastoma | Oral isotretinoin (13 patients): 6 cycles of 160 mg/m2/day, 2 weeks on, 2 weeks off | 6/13: physeal abnormalities; asymmetric genu valgum deformity-higher risk of deformity if a child was above 5 years. No significant growth differences in height during follow-up |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Cardoso-Demartini, A.A.; Boguszewski, C.L.; Boguszewski, M.C.S. Potential Effects of Oral Isotretinoin on Growth Plate and Height. Endocrines 2023, 4, 281-292. https://doi.org/10.3390/endocrines4020023
AMA Style
Cardoso-Demartini AA, Boguszewski CL, Boguszewski MCS. Potential Effects of Oral Isotretinoin on Growth Plate and Height. Endocrines. 2023; 4(2):281-292. https://doi.org/10.3390/endocrines4020023
Chicago/Turabian StyleCardoso-Demartini, Adriane A., Cesar Luiz Boguszewski, and Margaret C. S. Boguszewski. 2023. "Potential Effects of Oral Isotretinoin on Growth Plate and Height" Endocrines 4, no. 2: 281-292. https://doi.org/10.3390/endocrines4020023