This section discusses in detail the testing of the respiratory sensor and oximeter sensor. This test involved healthy subjects, both adults and children. For the adults, sessions were conducted on how to hold their breath for a certain period. Holding one’s breath is expected to result in an oxygen saturation value below 95% and is used to test the accuracy of the sensor at more varied oxygen saturation levels. The test results for each sensor are described in the following sub-sections.
3.2.1. Testing of Respiration Rate Sensor
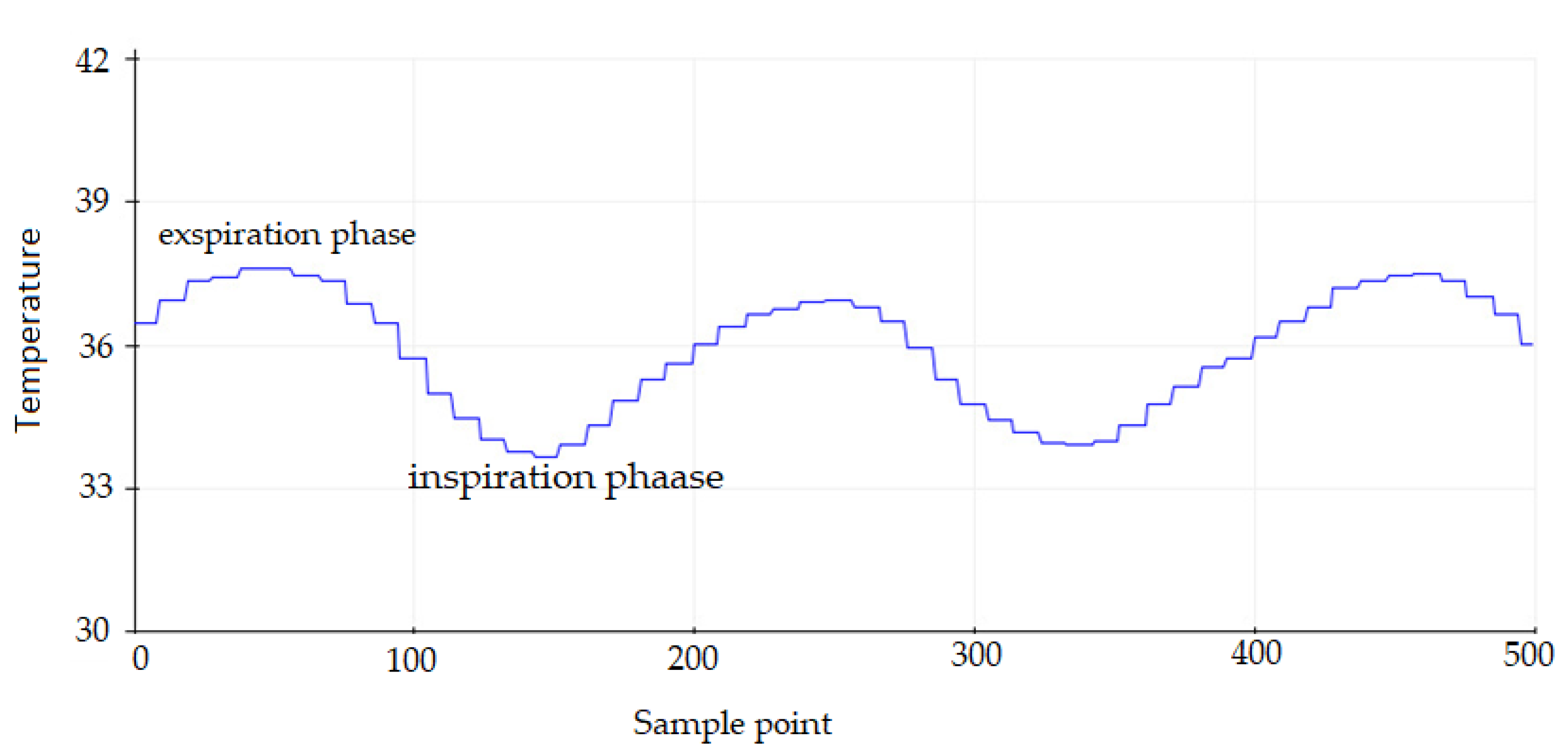
In the breathing sensor testing, an oxygen mask is placed over the mouth and nose. The subject is relaxed and sitting in a chair. The subjects were asked to breathe normally; there was no emphasis on either the inspiratory or expiratory phases. The MLX90614 sensor will detect changes in temperature flowing in the oxygen mask due to the inspiration and expiration phases as shown in
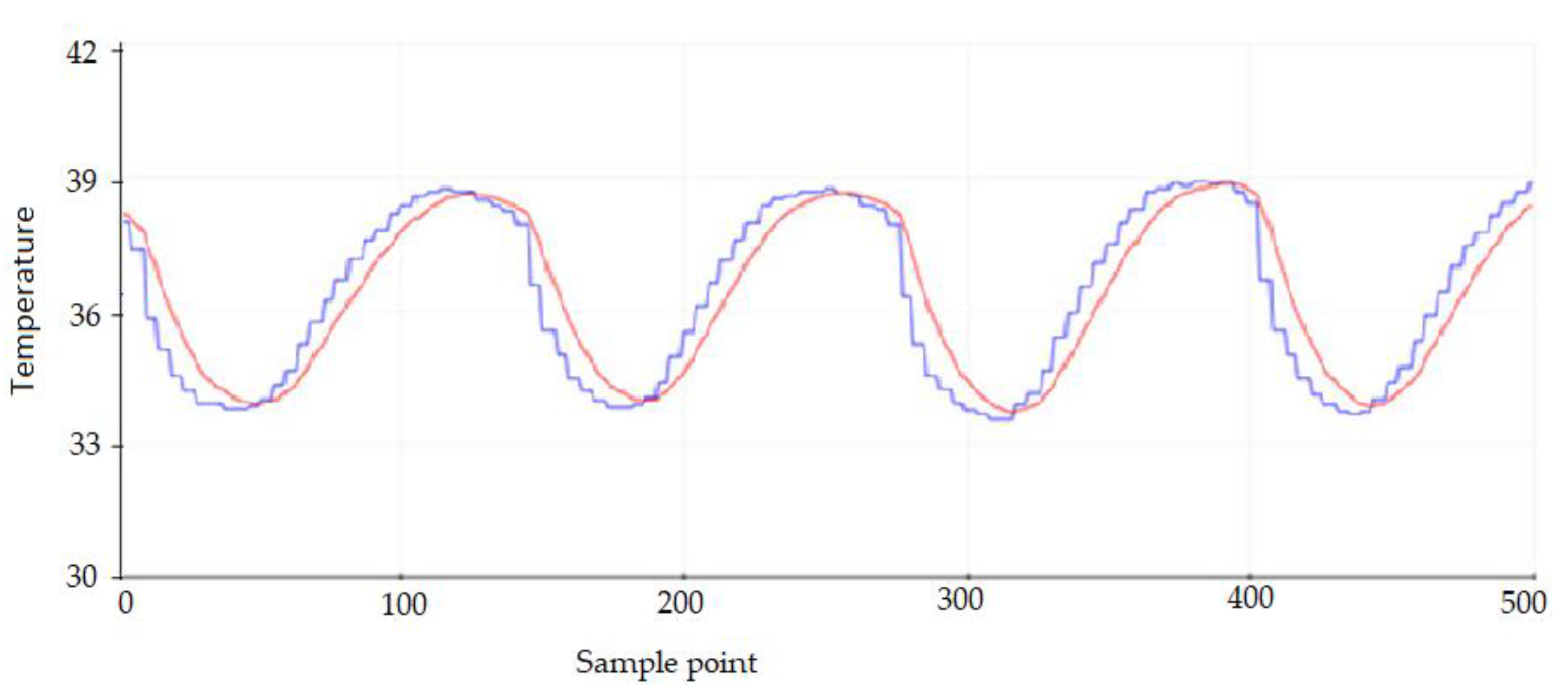
Figure 15. The expiratory phase shows a higher temperature than the inspiratory phase. One respiratory cycle includes these two phases which are then estimated every 15 s to obtain the respiration rate per minute. Since the raw signal from the sensor contains a small number of ripples with a high frequency as shown in
Figure 16, a digital low-pass filter with a cut-off frequency of 10 Hz is designed to reject the ripples. The filtered signal is shown in
Figure 16. A red line indicates that the respiratory signal is not contaminated with high-frequency noise.
The results of the calculation of the respiratory rate by the main controller unit based on sensor readings are then compared with the manual calculations with palpation techniques for one minute. The tests for adults and children were carried out 15 times each. The test results are presented in
Table 4. The test results show that the calculation of the respiratory rate using the sensor produces an accuracy of up to 100% with a delta error of ±1–2 rate/min both over and under estimation. This delta error could be caused by the calculation of breathing by the system for 15 s, which is then multiplied by four to obtain the respiratory rate per minute. Thus, the respiratory rate estimated by the device is a multiple of four. Therefore, it is possible to generate a delta error compared to the actual respiratory rate.
To test the reliability of the performance of the breathing sensor, another test scenario was also carried out with very fast breathing in the range of 30–70 breaths per minute. Adult subjects were asked to breathe faster as if experiencing shortness of breath. The results of testing this scenario are presented in
Table 5. In this scenario, the device is able to achieve 100% accuracy even though in some experiments there is a delta error of ±2–6 rate/min. In the respiratory scenario greater than 30 rate/min., the resulting delta error also tends to be linear.
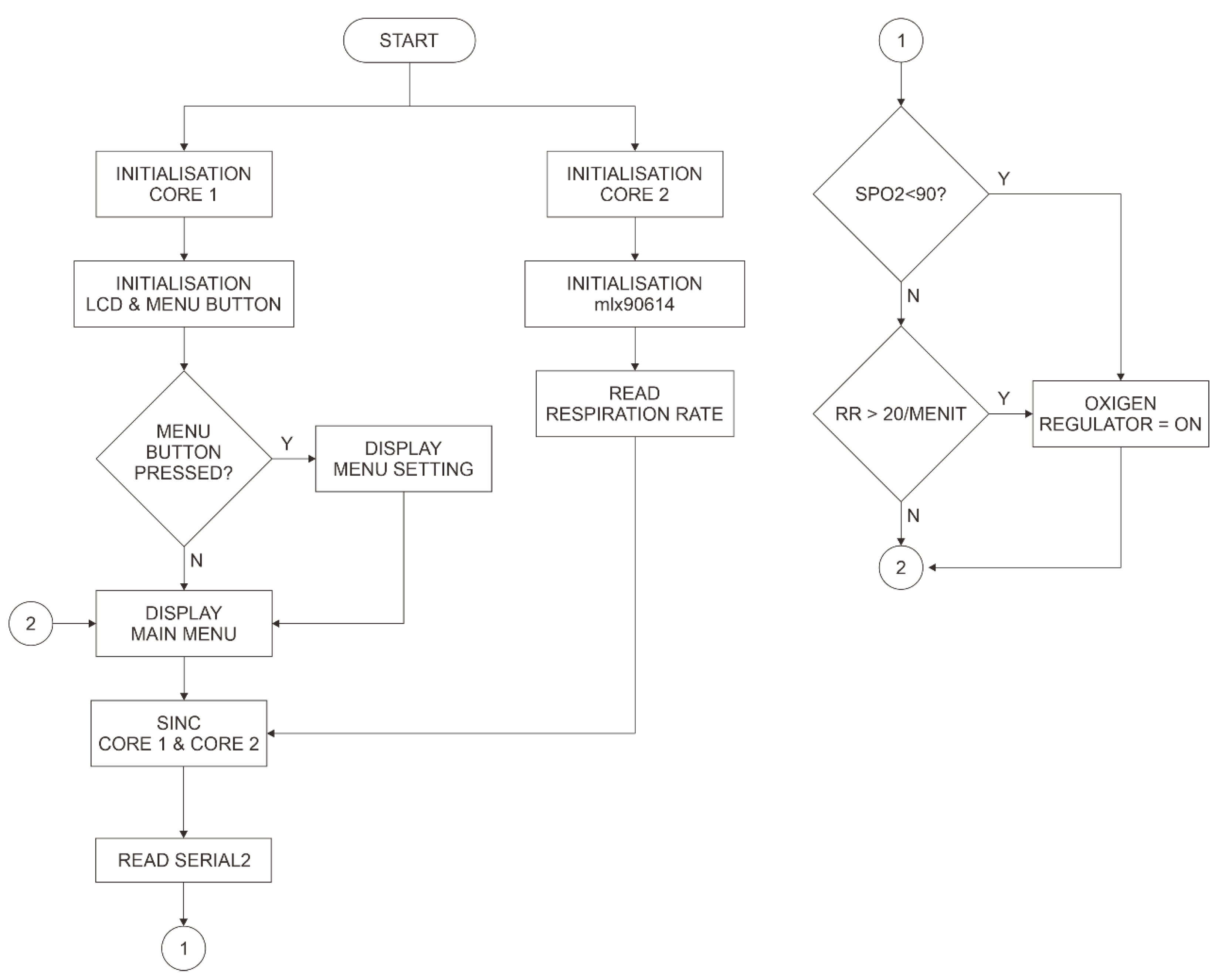
3.2.3. Testing of the Automatic Regulator
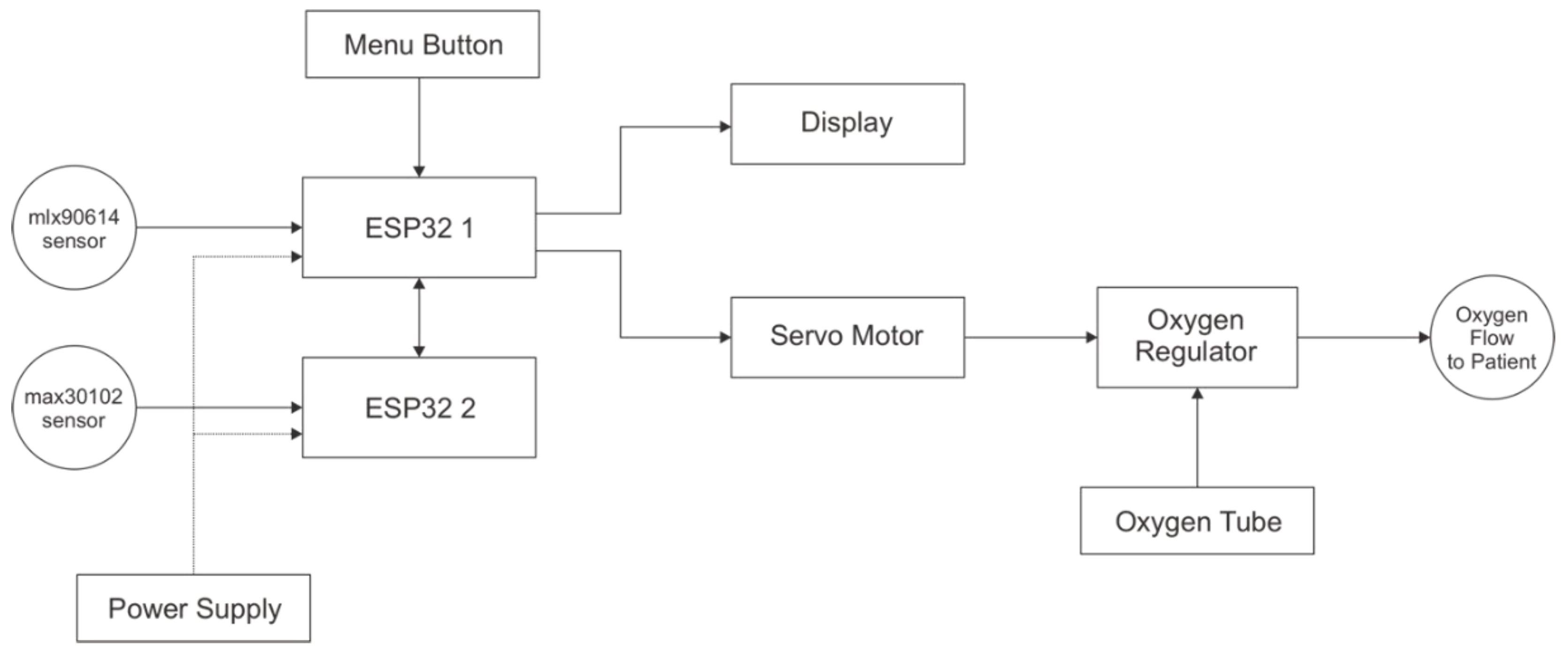
The proposed system supports both semi-automatic and fully-automatic control applications. Semi-automatic means that the user can set the MV manually through the device interface and the processor will then send commands to the actuator to adjust the oxygen rate through the servo motor. In this mode, the control of the regulator does not refer to body weight, respiration rate, or oxygen saturation. In fully-automatic mode, the system will adjust the oxygen rate in the regulator based on the body weight, respiration rate, and oxygen saturation data that are read by the sensor. Tests of the performance of the system in controlling the oxygen rate were carried out in fully-automatic mode, which also represents the test in semi-automatic mode.
This performance test only involved adult subjects. Subjects were asked to breathe at various rates, which was necessary to test the response of the actuator when receiving a low-to-high flow-control instruction or vice versa. The variations in the weight values are also set manually to make testing easier. The respiration rate is conditioned to greater than 20 rate/min, which is an abnormal condition for adults, so that the automatic mode works. There are four variations of respiration rate for each weight value.
The test results of the proposed system in automatic mode are presented in
Table 7. The results of the MV calculation by the device are rounded up/down so there are differences from the manual calculations. This is intended to simplify the step of regulating the oxygen flow, but with small deviations of about 0.5–1 L/min.
The test results of the variation of the oxygen flow value from high to low and vice versa do not affect the performance of the actuator. In other words, the actuator remains accurate in responding to changes in the oxygen flow according to the commands given by the main control unit.
A performance evaluation was also carried out by comparing the performance of the proposed system with a previous study by Puspitasari et al. [
17]. In the previous study, the maximum controllable oxygen flow was 8 L/min. Meanwhile, the currently proposed device is capable of delivering oxygen up to 14 L/min. In some conditions, for example, patients with a higher body weight and respiratory rate, more oxygen supply is required.
This proposed system can be used by patients who require continuous oxygen therapy during the medical treatment period. This system is able to control the flow of oxygen based on the needs of the human body with reference to body weight, oxygen saturation, and respiration rate. This system is expected to provide efficiency in the use of oxygen during the COVID-19 pandemic.


 ,
, 

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}