


Effectiveness of Photodynamic Therapy as Antiseptic Measure for Oral Cavity and Pharynx: A Systematic Review

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Sources of Information
2.3. Search Strategy
- Randomized clinical trials;
- Participants are older 18 years and younger 80 years with the indication for oral surgery with/or inflammatory diseases of oral cavity and pharynx;
- Use of photodynamic therapy as antiseptic method before operations in oral cavity or the part of management of inflammatory diseases of oral cavity and pharynx.
- Other types of research;
- Participants are younger than 18 years or older than 80 years old;
- Antibiotics taking for last month, anti-inflammatory drugs or pain-killers taking for last 5 days;
- Severe comorbidity proof;
- Pregnancy or lactation;
- Fungal infection;
- Acute viral or bacterial infections of other localization;
- Other conditions that are contraindications for laser use.
2.4. Selection of Studies
2.5. Data Collection Process and Items
2.6. Study Risk of Bias Assessment
- The randomization process;
- Deviations from intended interventions;
- Missing outcome data;
- Measurement of the outcome; and
- Selection of the reported result.
3. Results
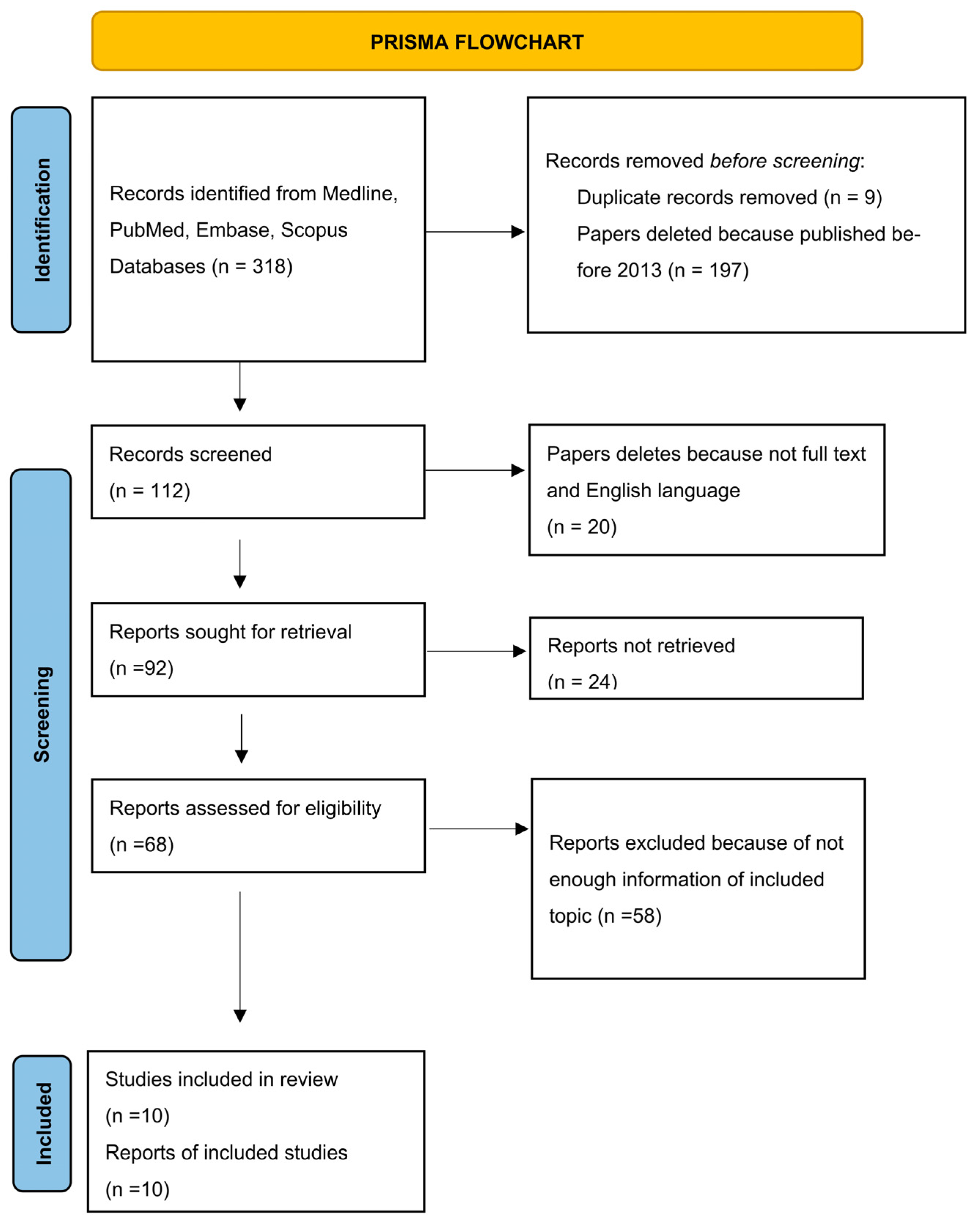
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias within Studies
4. Discussion
4.1. Review Study Discussion
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cheng, Y.; Chen, J.W.; Ge, M.K.; Zhou, Z.Y.; Yin, X.; Zou, S.J. Efficacy of Adjunctive Laser in Non-Surgical Periodontal Treatment: A Systematic Review and Meta-Analysis. Lasers Med. Sci. 2016, 31, 151–163. [Google Scholar] [CrossRef]
- Arsić, Z.; Jovanović, R.; Djordjević, A.; Šehalić, M.; Marjanović, D.; Mikić, M.; Vlahović, Z.; Raša, M. Clinical and Microbiological Effects of Photodynamic Therapy Applied in Non-Surgical Treatment of Periodontitis. Vojnosanit. Pregl. 2022, 79, 17–24. [Google Scholar] [CrossRef]
- Prazmo, E.J.; Kwaśny, M.; Łapiński, M.; Mielczarek, A. Photodynamic Therapy As a Promising Method Used in the Treatment of Oral Diseases. Adv. Clin. Exp. Med. 2016, 25, 799–807. [Google Scholar] [CrossRef] [Green Version]
- Katsikanis, F.; Strakas, D.; Vouros, I. The Application of Antimicrobial Photodynamic Therapy (APDT, 670 Nm) and Diode Laser (940 Nm) as Adjunctive Approach in the Conventional Cause-Related Treatment of Chronic Periodontal Disease: A Randomized Controlled Split-Mouth Clinical Trial. Clin. Oral Investig. 2020, 24, 1821–1827. [Google Scholar] [CrossRef]
- Raghavendra, M.; Koregol, A.; Bhola, S. Photodynamic Therapy: A Targeted Therapy in Periodontics. Aust. Dent. J. 2009, 54, S102–S109. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Yang, D.; Lei, S.; Liu, J.; Song, Y.; Zhao, H.; Zeng, X.; Dan, H.; Chen, Q. Photodynamic Therapy-a Promising Treatment of Oral Mucosal Infections. Photodiagn. Photodyn. Ther. 2022, 39, 103010. [Google Scholar] [CrossRef] [PubMed]
- Romanova, N.A.; Brovko, L.Y.; Moore, L.; Pometun, E.; Savitsky, A.P.; Ugarova, N.N.; Griffiths, M.W. Assessment of Photodynamic Destruction of Escherichia Coli O157:H7 and Listeria Monocytogenes by Using ATP Bioluminescence. Appl. Environ. Microbiol. 2003, 69, 6393–6398. [Google Scholar] [CrossRef] [Green Version]
- Warrier, A.; Mazumder, N.; Prabhu, S.; Satyamoorthy, K.; Murali, T.S. Photodynamic Therapy to Control Microbial Biofilms. Photodiagn. Photodyn. Ther. 2021, 33, 102090. [Google Scholar] [CrossRef]
- Takasaki, A.A.; Aoki, A.; Mizutani, K.; Schwarz, F.; Sculean, A.; Wang, C.Y.; Koshy, G.; Romanos, G.; Ishikawa, I.; Izumi, Y. Application of Antimicrobial Photodynamic Therapy in Periodontal and Peri-Implant Diseases. Periodontol. 2000 2009, 51, 109–140. [Google Scholar] [CrossRef]
- Kim, M.M.; Darafsheh, A. Light Sources and Dosimetry Techniques for Photodynamic Therapy. Photochem. Photobiol. 2020, 96, 280–294. [Google Scholar] [CrossRef] [Green Version]
- Habashneh, R.A.; Asa’ad, F.A.; Khader, Y. Photodynamic Therapy in Periodontal and Peri-Implant Diseases. Quintessence Int. 2015, 46, 677–690. [Google Scholar] [CrossRef]
- Passanezi, E.; Damante, C.A.; de Rezende, M.L.R.; Greghi, S.L.A. Lasers in Periodontal Therapy. Periodontol 2000 2015, 67, 268–291. [Google Scholar] [CrossRef] [PubMed]
- Soukos, N.S.; Goodson, J.M. Photodynamic Therapy in the Control of Oral Biofilms. Periodontol 2000 2011, 55, 143–166. [Google Scholar] [CrossRef] [PubMed]
- Ferrisse, T.M.; Dias, L.M.; de Oliveira, A.B.; Jordão, C.C.; de Oliveira Mima, E.G.; Pavarina, A.C. Efficacy of Curcumin-Mediated Antibacterial Photodynamic Therapy for Oral Antisepsis: A Systematic Review and Network Meta-Analysis of Randomized Clinical Trials. Photodiagn. Photodyn. Ther. 2022, 39, 102876. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Pu, R.; Qian, Y.; Shi, J.; Si, M. Antimicrobial Photodynamic Therapy versus Antibiotics as an Adjunct in the Treatment of Periodontitis and Peri-Implantitis: A Systematic Review and Meta-Analysis. Photodiagn. Photodyn. Ther. 2021, 34, 102231. [Google Scholar] [CrossRef]
- Qi, M.; Chi, M.; Sun, X.; Xie, X.; Weir, M.D.; Oates, T.W.; Zhou, Y.; Wang, L.; Bai, Y.; Xu, H.H.K. Novel Nanomaterial-Based Antibacterial Photodynamic Therapies to Combat Oral Bacterial Biofilms and Infectious Diseases. Int. J. Nanomedicine. 2019, 14, 6937–6956. [Google Scholar] [CrossRef] [Green Version]
- Nunes, L.P.; Nunes, G.P.; Ferrisse, T.M.; Strazzi-Sahyon, H.B.; Cintra, L.T.Â.; dos Santos, P.H.; Sivieri-Araujo, G. Antimicrobial Photodynamic Therapy in Endodontic Reintervention: A Systematic Review and Meta-Analysis. Photodiagn. Photodyn. Ther. 2022, 39, 103014. [Google Scholar] [CrossRef]
- Trindade, A.C.; De Figueiredo, J.A.P.; Steier, L.; Weber, J.B.B. Photodynamic Therapy in Endodontics: A Literature Review. Photomed. Laser Surg. 2015, 33, 175–182. [Google Scholar] [CrossRef]
- de Araújo, L.P.; de Oliveira da Rosa, W.L.; Gobbo, L.B.; da Silva, T.A.; de Almeida, J.F.A.; Ferraz, C.C.R. Global Research Trends on Photodynamic Therapy in Endodontics: A Bibliometric Analysis. Photodiagn. Photodyn. Ther. 2022, 40, 103039. [Google Scholar] [CrossRef]
- Bordea, I.R.; Hanna, R.; Chiniforush, N.; Grădinaru, E.; Câmpian, R.S.; Sîrbu, A.; Amaroli, A.; Benedicenti, S. Evaluation of the Outcome of Various Laser Therapy Applications in Root Canal Disinfection: A Systematic Review. Photodiagn. Photodyn. Ther. 2020, 29, 101611. [Google Scholar] [CrossRef]
- Plotino, G.; Grande, N.M.; Mercade, M. Photodynamic Therapy in Endodontics. Int. Endod. J. 2019, 52, 760–774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chrepa, V.; Kotsakis, G.A.; Pagonis, T.C.; Hargreaves, K.M. The Effect of Photodynamic Therapy in Root Canal Disinfection: A Systematic Review. J. Endod. 2014, 40, 891–898. [Google Scholar] [CrossRef]
- Siddiqui, S.H.; Awan, K.H.; Javed, F. Bactericidal Efficacy of Photodynamic Therapy against Enterococcus Faecalis in Infected Root Canals: A Systematic Literature Review. Photodiagn. Photodyn. Ther. 2013, 10, 632–643. [Google Scholar] [CrossRef]
- Pourhajibagher, M.; Bahador, A. Adjunctive Antimicrobial Photodynamic Therapy to Conventional Chemo-Mechanical Debridement of Infected Root Canal Systems: A Systematic Review and Meta-Analysis. Photodiagn. Photodyn. Ther. 2019, 26, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Baghani, Z.; Shabestari, S.B.; Karrabi, M. Clinical Attachment Loss in the Use of Adjunctive Antimicrobial Photodynamic Therapy in Stages II-IV Grade C Molar-Incisor Periodontitis: A Systematic Review and Meta-Analysis. Bosn. J. Basic Med. Sci. 2022, 22, 843–861. [Google Scholar] [CrossRef]
- Wang, N.; Hao, S.; Zhang, J.; Yang, J. Clinical Efficacy of Photodynamic Therapy on Halitosis: A Systematic Review and Meta-Analysis. Lasers Med. Sci. 2022, 38, 29. [Google Scholar] [CrossRef] [PubMed]
- Pacheco, J.A.; Molena, K.F.; Martins, C.R.O.G.; Corona, S.A.M.; Borsatto, M.C. Photobiomodulation (PBMT) and Antimicrobial Photodynamic Therapy (APDT) in Oral Manifestations of Patients Infected by Sars-CoV-2: Systematic Review and Meta-Analysis. Bull. Natl. Res. Cent. 2022, 46, 140. [Google Scholar] [CrossRef] [PubMed]
- Manresa, C.; Sanz-Miralles, E.C.; Twigg, J.; Bravo, M. Supportive Periodontal Therapy (SPT) for Maintaining the Dentition in Adults Treated for Periodontitis. Cochrane Database Syst. Rev. 2018, 1, CD009376. [Google Scholar] [CrossRef] [PubMed]
- Salvi, G.E.; Stähli, A.; Schmidt, J.C.; Ramseier, C.A.; Sculean, A.; Walter, C. Adjunctive Laser or Antimicrobial Photodynamic Therapy to Non-Surgical Mechanical Instrumentation in Patients with Untreated Periodontitis: A Systematic Review and Meta-Analysis. J. Clin. Periodontol. 2020, 47 (Suppl. S22), 176–198. [Google Scholar] [CrossRef] [Green Version]
- Azaripour, A.; Dittrich, S.; Van Noorden, C.J.F.; Willershausen, B. Efficacy of Photodynamic Therapy as Adjunct Treatment of Chronic Periodontitis: A Systematic Review and Meta-Analysis. Lasers Med. Sci. 2018, 33, 407–423. [Google Scholar] [CrossRef]
- Albaker, A.M.; ArRejaie, A.S.; Alrabiah, M.; Abduljabbar, T. Effect of Photodynamic and Laser Therapy in the Treatment of Peri-Implant Mucositis: A Systematic Review. Photodiagn. Photodyn. Ther. 2018, 21, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Sgolastra, F.; Petrucci, A.; Gatto, R.; Marzo, G.; Monaco, A. Photodynamic Therapy in the Treatment of Chronic Periodontitis: A Systematic Review and Meta-Analysis. Lasers Med. Sci. 2013, 28, 669–682. [Google Scholar] [CrossRef]
- Sgolastra, F.; Petrucci, A.; Severino, M.; Graziani, F.; Gatto, R.; Monaco, A. Adjunctive Photodynamic Therapy to Non-Surgical Treatment of Chronic Periodontitis: A Systematic Review and Meta-Analysis. J. Clin. Periodontol. 2013, 40, 514–526. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. PLoS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef] [PubMed]
- Cochrane Handbook for Systematic Reviews of Interventions | Cochrane Training. Available online: https://training.cochrane.org/handbook (accessed on 12 February 2022).
- Annunziata, M.; Donnarumma, G.; Guida, A.; Nastri, L.; Persico, G.; Fusco, A.; Sanz-Sánchez, I.; Guida, L. Clinical and Microbiological Efficacy of Indocyanine Green-Based Antimicrobial Photodynamic Therapy as an Adjunct to Non-Surgical Treatment of Periodontitis: A Randomized Controlled Clinical Trial. Clin. Oral. Investig. 2023, 27, 2385–2394. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, K.; Pavaskar, R.; Cappetta, E.; Drew, H. Effectiveness of Adjunctive Use of Low-Level Laser Therapy and Photodynamic Therapy After Scaling and Root Planing in Patients with Chronic Periodontitis. Int. J. Periodontics Restor. Dent. 2019, 39, 837–843. [Google Scholar] [CrossRef]
- Martins, S.H.L.; Novaes, A.B.; Taba, M.; Palioto, D.B.; Messora, M.R.; Reino, D.M.; Souza, S.L.S. Effect of Surgical Periodontal Treatment Associated to Antimicrobial Photodynamic Therapy on Chronic Periodontitis: A Randomized Controlled Clinical Trial. J. Clin. Periodontol. 2017, 44, 717–728. [Google Scholar] [CrossRef]
- Soundarajan, S.; Rajasekar, A. Comparative Evaluation of Combined Efficacy of Methylene Blue Mediated Antimicrobial Photodynamic Therapy (a-PDT) Using 660 Nm Diode Laser versus Erbium-Chromium-Yttrium-Scandium-Gallium-Garnet (Er, Cr: YSGG) Laser as an Adjunct to Scaling and Root Planin. Photodiagn. Photodyn. Ther. 2022, 39, 102971. [Google Scholar] [CrossRef]
- Hill, G.; Dehn, C.; Hinze, A.V.; Frentzen, M.; Meister, J. Indocyanine Green-Based Adjunctive Antimicrobial Photodynamic Therapy for Treating Chronic Periodontitis: A Randomized Clinical Trial. Photodiagn. Photodyn. Ther. 2019, 26, 29–35. [Google Scholar] [CrossRef]
- Betsy, J.; Prasanth, C.S.; Baiju, K.V.; Prasanthila, J.; Subhash, N. Efficacy of Antimicrobial Photodynamic Therapy in the Management of Chronic Periodontitis: A Randomized Controlled Clinical Trial. J. Clin. Periodontol. 2014, 41, 573–581. [Google Scholar] [CrossRef]
- Ichinose-Tsuno, A.; Aoki, A.; Takeuchi, Y.; Kirikae, T.; Shimbo, T.; Lee, M.-C.-I.; Yoshino, F.; Maruoka, Y.; Itoh, T.; Ishikawa, I.; et al. Antimicrobial Photodynamic Therapy Suppresses Dental Plaque Formation in Healthy Adults: A Randomized Controlled Clinical Trial. BMC Oral Health 2014, 14, 152. [Google Scholar] [CrossRef]
- Albaker, A.M.; ArRejaie, A.S.; Alrabiah, M.; Al-Aali, K.A.; Mokeem, S.; Alasqah, M.N.; Vohra, F.; Abduljabbar, T. Effect of Antimicrobial Photodynamic Therapy in Open Flap Debridement in the Treatment of Peri-Implantitis: A Randomized Controlled Trial. Photodiagn. Photodyn. Ther. 2018, 23, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, T.; Sezgin, G.P.; Sönmez Kaplan, S. Effect of a 980-Nm Diode Laser on Post-Operative Pain after Endodontic Treatment in Teeth with Apical Periodontitis: A Randomized Clinical Trial. BMC Oral Health 2021, 21, 41. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Chen, B.; Huang, H.; He, Z.; Sun, J.; Wang, G.; Gu, X.; Tang, B.Z. AIE-Active Photosensitizers: Manipulation of Reactive Oxygen Species Generation and Applications in Photodynamic Therapy. Biosensors 2022, 12, 348. [Google Scholar] [CrossRef]
- Verger, A.; Brandhonneur, N.; Molard, Y.; Cordier, S.; Kowouvi, K.; Amela-Cortes, M.; Dollo, G. From Molecules to Nanovectors: Current State of the Art and Applications of Photosensitizers in Photodynamic Therapy. Int. J. Pharm. 2021, 604, 120763. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.; Herrera, D.; Kebschull, M.; Chapple, I.; Jepsen, S.; Beglundh, T.; Sculean, A.; Tonetti, M.S.; Merete Aass, A.; Aimetti, M.; et al. Treatment of Stage I–III Periodontitis—The EFP S3 Level Clinical Practice Guideline. J. Clin. Periodontol. 2020, 47, 4–60. [Google Scholar] [CrossRef] [PubMed]
- Tapashetti, R.; Bhagat, M. Photodynamic Therapy in Periodontics. Galore Int. J. Health Sci. Res. 2020, 5, 14. [Google Scholar]
- de Oliveira, R.R.; Schwartz-Filho, H.O.; Novaes, A.B.; Taba, M. Antimicrobial Photodynamic Therapy in the Non-Surgical Treatment of Aggressive Periodontitis: A Preliminary Randomized Controlled Clinical Study. J. Periodontol. 2007, 78, 965–973. [Google Scholar] [CrossRef]
- Braun, A.; Dehn, C.; Krause, F.; Jepsen, S. Short-Term Clinical Effects of Adjunctive Antimicrobial Photodynamic Therapy in Periodontal Treatment: A Randomized Clinical Trial. J. Clin. Periodontol. 2008, 35, 877–884. [Google Scholar] [CrossRef]
- Xue, D.; Tang, L.; Bai, Y.; Ding, Q.; Wang, P.; Zhao, Y. Clinical Efficacy of Photodynamic Therapy Adjunctive to Scaling and Root Planing in the Treatment of Chronic Periodontitis: A Systematic Review and Meta-Analysis. Photodiagn. Photodyn. Ther. 2017, 18, 119–127. [Google Scholar] [CrossRef]
- Carvalho, L.H.; D’Avila, G.B.; Leão, A.; Haffajee, A.D.; Socransky, S.S.; Feres, M. Scaling and Root Planing, Systemic Metronidazole and Professional Plaque Removal in the Treatment of Chronic Periodontitis in a Brazilian Population: I. Clinical Results. J. Clin. Periodontol. 2004, 31, 1070–1076. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, Y.; Mae, M.; Oohira, M.; Ozaki, Y.; Ohba, S.; Asahina, I.; Yoshimura, A. Clinical Efficacy and Safety of Antimicrobial Photodynamic Therapy in Residual Periodontal Pockets during the Maintenance Phase. Pharmaceuticals 2022, 15, 924. [Google Scholar] [CrossRef]
- Gilbert, A.; Baggott. Photochemistry. J. Essent. Mol. Photochem. 1991, 743–789. [Google Scholar] [CrossRef]
- Chambrone, L.; Wang, H.L.; Romanos, G.E. Antimicrobial Photodynamic Therapy for the Treatment of Periodontitis and Peri-Implantitis: An American Academy of Periodontology Best Evidence Review. J. Periodontol. 2018, 89, 783–803. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Yan, Q.; Wu, X.; Hua, F.; Shi, B. The Benefit of Antimicrobial Photodynamic Therapy to Mechanical Debridement in the Treatment of Smokers with Peri-Implant Diseases: A Systematic Review and Meta-Analysis. Lasers Med. Sci. 2022, 37, 3051–3066. [Google Scholar] [CrossRef] [PubMed]
- Zhao, T.; Song, J.; Ping, Y.; Li, M. The Application of Antimicrobial Photodynamic Therapy (APDT) in the Treatment of Peri-Implantitis. Comput. Math. Methods Med. 2022, 2022, 3547398. [Google Scholar] [CrossRef]
- Rahman, B.; Acharya, A.B.; Siddiqui, R.; Verron, E.; Badran, Z.; Rahman, B.; Acharya, A.B.; Siddiqui, R.; Verron, E.; Badran, Z. Photodynamic Therapy for Peri-Implant Diseases. Antibiotics 2022, 11, 918. [Google Scholar] [CrossRef]
- Sperandio, F.; Huang, Y.-Y.; Hamblin, M. Antimicrobial Photodynamic Therapy to Kill Gram-Negative Bacteria. Recent Pat. Anti-Infect. Drug Discov. 2013, 8, 108–120. [Google Scholar] [CrossRef] [Green Version]
- Couto, A.C.F.; de Carvalho, R.V.H.; Brancini, G.T.P.; Martins, F.G.; Sorgi, C.A.; da Silva, R.A.B.; Nelson-Filho, P.; Paula-Silva, F.W.G.; Borsatto, M.C.; Braga, G.Ú.L.; et al. Photosensitizers Attenuate LPS-Induced Inflammation: Implications in Dentistry and General Health. Lasers Med. Sci. 2020, 36, 913–926. [Google Scholar] [CrossRef]
- Nesi-Reis, V.; Lera-Nonose, D.S.S.L.; Oyama, J.; Silva-Lalucci, M.P.P.; Demarchi, I.G.; Aristides, S.M.A.; Teixeira, J.J.V.; Silveira, T.G.V.; Lonardoni, M.V.C. Contribution of Photodynamic Therapy in Wound Healing: A Systematic Review. Photodiagn. Photodyn. Ther. 2018, 21, 294–305. [Google Scholar] [CrossRef]


{kind=link}
| Author (Name, Last Name), Year | N of Patients (Total, in Each Group) | Patients Age (Mean, Median) | Assessment Criterion | The Intervention Group (Test Group) | The Control Group | Laser Treatment (Mode), Photosensitizer | Location Use/Disease | Results | |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Marco Annunziata, 2023 [36] | 24: 12 + 12 | 18–80, 25 |
| ICG-aPDT with an 810 nm diode laser (ICG-indocyanine green photosensitizer) | Irrigating the pockets with the photosensitizer solution and carrying inside the optical fibre with the laser kept it turned off mode |
| Periodontitis | In the Test group: at 6 months for a higher PD reduction in initial deep pockets (PD ≥ 6 mm) and a higher percentage of closed pockets (PD ≤ 4 mm/no bleeding on probing).
|
| 2 | Kaveri Kranti Gandhi, 2019 [37] | 30 | 30–60 |
| Test group1: (Scaling and root planning (SRP) + PDT) Test group2 (SRP + low level laser therapy (LLLT)) | Scaling and root planning (SRP) alone |
100 MW 810 nm
| Chronic periodontitis | The test groups showed significantly higher reductions in Gingival Index, probing depth, and clinical attachment level |
| 3 | Sérgio H. L. Martins, 2017 [38] | 40 | ≥35 years |
| Patients with severe chronic periodontitis (SCP) were treated with aPDT + ST (surgical periodontal treatment) | Patients with severe chronic periodontitis treated only with ST (surgical periodontal treatment) | Red Laser 70 mW of power, and a power density of 28 mW/cm2
| Severe chronic periodontitis |
|
| 4 | Zoran Arsić 2022 [2] | 25 | 30–70 |
| The test group was treated by NSPT (non-surgical periodontal treatment) combined with aPDT | The control group was treated by NSPT (non-surgical periodontal treatment) applied alone |
| Periodontitis | NSPT combined with aPDT led to a statistically significant improvement of both clinical parameters and microbiological status compared to NSPT applied on its own |
| 5 | Subasree Soundarajan 2022 [39] | 36 | 18–70 |
| Group III—SRP (scaling and root planning) followed by antimicrobial Photodynamic therapy using diode laser | Group I—Scaling and root planing (SRP) alone Group II—SRP followed by application of Er, Cr: YSGG laser |
| chronic periodontitis | PI, GI PD, and CAL significantly improved at 3 months follow up compared to baseline in Group II and Group III with p < 0.05 |
| 6 | Fotios Katsikanis, 2019 [4] | 21 | 48.2 ± 8.2 | periodontal pocket depth | Diode group-SRP with diode laser Photodynamic group- SRP with photodynamic therapy | The control group: SRP (scaling and root planning) alone |
| severe periodontal disease pocket depth (PPD) of ≥5 mm |
|
| 7 | Greta Hill, 2019 [40] | 20 | 61.1 |
| ICG-based aPDT with a Diode laser | Patients were treated with scaling and root planning of the affected teeth |
at 2 kHz
| chronic periodontitis |
|
| 8 | Betsy Joseph, 2014 [41] | 88 | Control group 38.4 ± 9.6 years Test group 40.8 ± 8.3 years |
| SRP with aPDT | SRP alone |
| Chronic periodontitis |
|
| 9 | Akiko Ichinose-Tsuno, 2014 [42] | 11 | 28.0 ± 2.3 years |
| The right or left mandibular premolars were randomly assigned to the treatment (with aPDT) | The right or left mandibular premolars were randomly assigned to the treatment (without aPDT) | A combination of 500 or 1000 μg/mL toluidine blue O (TBO) and LED irradiation for 20 s
| Health of oral cavity |
|
| 10 | Abdulaziz M Albaker [43] | 24 | aPDT + OFD group 58.4 ± 8.0; OFD group 61.5 ± 9.9 |
|
|
| A diode laser of 670 nanometers at 150 milliwatts with optic fibre diameter 0.06 mm. | Peri-implantitis | At 6 months, aPDT and OFD significantly reduced peri-implant PI, BOP, PD and MBL. |
| Study | The Randomization Process | Deviations from the Intended Interventions | Missing Outcome Date | Measurement of Outcome Data | Selection of the Reported Result |
|---|---|---|---|---|---|
| Seérgio H. L. Martins et al., 2017 [38] | Low risk | Low risk | Low risk | Low risk | Low risk |
| Tuna Kaplan et al., 2021 [44] | Low risk | High risk | Low risk | Low risk | Low risk |
| Fotios Katsikanis et al., 2019 [4] | Some concern | Some concern | Low risk | Low risk | Low risk |
| Subasree Soundarajan 2022 [39] | Low risk | Low risk | Low risk | Low risk | Low risk |
| Zoran Arsic et al., 2022 [2] | Some concern | Some concern | Low risk | Low risk | Low risk |
| Greta Hill et al., 2019 [40] | Low risk | Low risk | Low risk | Low risk | Low risk |
| Betsy Joseph et al., 2014 [41] | Low risk | Some concern | Low risk | Low risk | Low risk |
| Akiko Ichinose-Tsuno et al., 2014 [42] | Low risk | Low risk | Low risk | Low risk | Some concern |
| Marco Annunziata et al., 2023 [36] | Low risk | High risk | High risk | High risk | Some concern |
| Abdulaziz M Albaker 2018 [43] | Low risk | Low risk | Low risk | Low risk | Low risk |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sologova, D.; Petukhova, M.; Podoplelova, P.; Davletshin, D.; Firsova, A.; Grishin, A.; Grin, M.; Suvorov, N.; Vasil’ev, Y.; Dydykin, S.; et al. Effectiveness of Photodynamic Therapy as Antiseptic Measure for Oral Cavity and Pharynx: A Systematic Review. Dent. J. 2023, 11, 192. https://doi.org/10.3390/dj11080192
Sologova D, Petukhova M, Podoplelova P, Davletshin D, Firsova A, Grishin A, Grin M, Suvorov N, Vasil’ev Y, Dydykin S, et al. Effectiveness of Photodynamic Therapy as Antiseptic Measure for Oral Cavity and Pharynx: A Systematic Review. Dentistry Journal. 2023; 11(8):192. https://doi.org/10.3390/dj11080192
Chicago/Turabian StyleSologova, Diana, Marina Petukhova, Polina Podoplelova, Dinislam Davletshin, Anna Firsova, Andrey Grishin, Mikhail Grin, Nikita Suvorov, Yuriy Vasil’ev, Sergey Dydykin, and et al. 2023. "Effectiveness of Photodynamic Therapy as Antiseptic Measure for Oral Cavity and Pharynx: A Systematic Review" Dentistry Journal 11, no. 8: 192. https://doi.org/10.3390/dj11080192