
Mechanical Factors Implicated in Zirconia Implant Fracture Placed within the Anterior Region—A Systematic Review

 ,
,  , , , and
, , , and 
Abstract
:1. Introduction
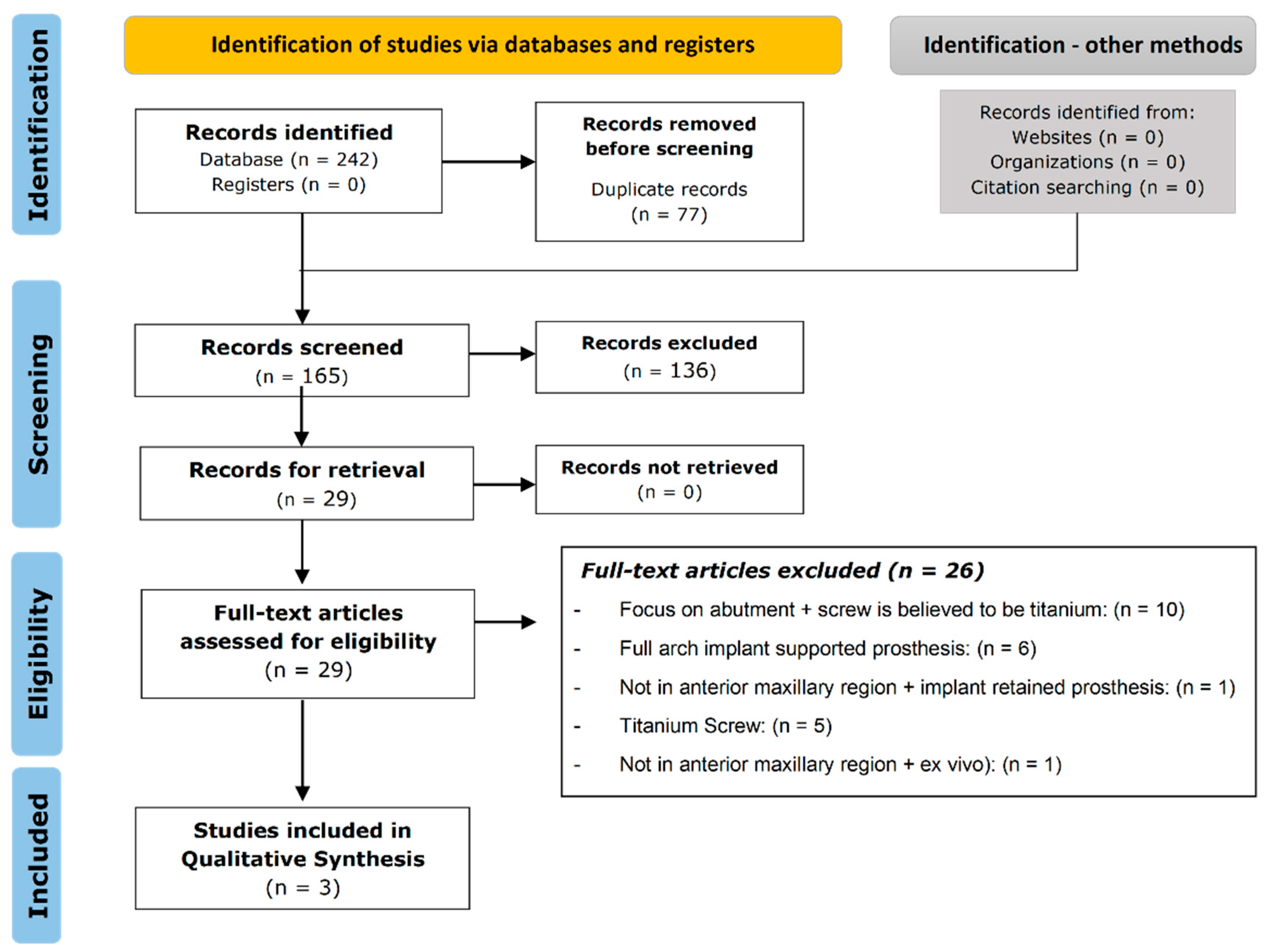
2. Methods
3. Results
3.1. Quality Assessment of Included Studies
3.2. Study Characteristics
3.3. Risk of Bias Assessment

{kind=link}
| Citation | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Roehling et al. (2016) [21] | Y | Y | Y | N | N/A | Y | N | Y | Y | N/A | Y |
| Scherrer et al. (2019) [22] | N/A | N/A | Y | N/A | N/A | N/A | Y | N/A | N/A | N/A | N/A |
| Percentage (%) | 50 | 50 | 100 | 0 | 0 | 50 | 50 | 50 | 50 | 0 | 50 |
| Citation | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | Q12 | Q13 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Paolantoni et al. (2016) [20] | U | N | Y | U | U | U | N | Y | Y | N/A | N/A | Y | U |
| Percentage (%) | 0 | 0 | 100 | 0 | 0 | 0 | 0 | 100 | 100 | 0 | 0 | 100 | 0 |
| Study | Country | Setting/Context | Participant Characteristics | Groups | Outcomes Measured | Description of Main Results |
|---|---|---|---|---|---|---|
| Paolantoni et al. 2016 [20] | Italy | University of Naples | Patients—65 Females—44 Males—21 74 missing maxillary teeth Mean age 53 ± 4 years. | Treatment group 1 received standard zirconia anchorage with a layer of lithium disilicate (pressed) and an all-ceramic luted crown (two piece). Group 1—Single implant-51 patients; Two single nonadjacent implants prosthetic restorations—9 patients 51 fixtures (68.9%) were placed with a one-stage procedure with a healing period of 12 months; 23 fixtures (31.1%) were inserted with a two-stage procedure and a healing period of 6 months. Group 2 (n = 45) received one-piece restoration with the porcelain facing fire-pressed onto custom zirconia anchorage. | Mechanical outcomes: Fracture failure of abutment, restoration and porcelain facing, loss of retention of the abutment due to screw loosening, or restoration fracture. Biological outcomes: Implant Mobility, Plaque Index (PI), Bleeding Index (BI), and marginal bone loss (MBL). |
|
| Study | Country | Setting/Context | Participant Characteristics | Groups | Outcomes Measured | Description of Main Results |
|---|---|---|---|---|---|---|
| Scherrer et al. 2019 [22] | Switzerland | Study design: Retrospective Cohort Study. Funding source: Not specified. | Broken first generation monotype zirconia implant parts, upper portion with the crown cemented. | Number of teeth: 15. Axis Biodental Implants (10), Z-Systems Implants (3), Straumann Implants (1), Swiss Dental Solutions Implants (1). | Details of Intervention: Fractographic failure analysis to identify origin of failure and characteristics of surface cracks. Measured/Treatment Outcomes: A mathematical model spreadsheet was utilized to compute bending and torsion moments on a total load of 500 N distributed over identified occlusal contacts. Follow-up Period: Not specified. |
|
| Roehling. et al. 2016 [21] | Germany | Study design: Retrospective Funding Source: Not specified. | 85 participants (47 female, 38 male) who received a first generation monotype zirconia implant between the dates of Oct 2004 and Nov 2009. Mean age 54.86; 161 implants assessed, 7 smokers (11 implants), 21 patients had bruxism (57 implants). | Only 1 group measured at initial placement and at/near 7 years. | Details of intervention: Data collected-number, diameter, length and position of implants, age, gender, risk factors, and bone quality and intra-oral image. Outcome measured: Subjective complaints, recurrent peri-implantitis with suppuration, implant mobility, gingival Index (GI), modified plaque index (PI) probing depth (PD), modified sulcus bleeding Index (mBI), distance from the implant shoulder to the mucosal margin (DIM). Success was measured by a criteria formulated by Buser and colleagues. Follow-up period: Mean follow-up period of 5.94 +/− 0.09 years |
|
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| Database | MeSH Terms and Search Strategy |
|---|---|
| Scopus | (“fract* resistan*” OR “fract* analys*” OR “fract* behavio*r” OR “fract* strength” OR fract* OR “fract* dimension” OR “fract* tough*” OR “fract* model” OR fragment* OR break* OR crack* OR fissure* OR split*) AND (“two-piece zirconia” OR “two piece zirconia” OR “2 piece zirconia” OR “2-piece zirconia” OR “zirconia implant*” OR “zirconia screw” OR “zirconia abutment*”) AND TITLE-ABS-KEY (anterior OR “anterior area” OR “anterior zone” OR “anterior section” OR “anterior region” OR “anterior segment” OR maxil* OR “*esthetic zone” OR “*esthetic region” OR “*esthetic area” OR “*esthetic section” OR “*esthetic segment”) AND TITLE-ABS-KEY (implant* OR abut*)) |
| Ovid |
|
| PubMed | (maxilla OR maxil* OR anterior OR “anterior area” OR “anterior region” OR “anterior zone” OR “anterior section” OR “aesthetic zone” OR “aesthetic area” OR “esthetic zone” OR “esthetic area”) AND (fract* OR “fracture resistance” OR “fractal behaviour” OR “fracture behaviour” OR “fracture strength” OR “fractal dimension” OR “fracture toughness” OR “fracture model” OR “fractal model” OR break* OR crack* OR fissure* OR split*) AND (“two piece zirconia” OR “two-piece zirconia” OR “2-piece zirconia” OR “2 piece zirconia” OR “zirconia abutment” OR “zirconia implant” OR zirconia implants”) |
| Cochrane Library | (“fract* resistan*” OR “fract* analysis” OR fracture OR fractures OR “fract* behaviour” OR “fracture strength” OR “fract* dimension” OR “fractal toughness” OR “fracture toughness” OR “fractal model” OR “fracture model” OR fragment* OR break* OR crack* OR fissure* OR split*) AND (“two-piece zirconia” OR “two piece zirconia” OR “2 piece zirconia” OR “2-piece zirconia” OR “zirconia abutment*” OR “zirconia screw” OR “zirconia implant*”) AND (anterior OR “anterior area” OR “anterior zone” OR “anterior section” OR “anterior region” OR “anterior segment” OR maxil* OR “aesthetic zone” OR “esthetic zone” OR “aesthetic region” OR “*esthetic region” OR “aesthetic area” OR “*esthetic area” OR “aesthetic section” OR “*esthetic section” OR “aesthetic segment” OR “*esthetic segment”) |
Appendix B
| A. JBI Critical Appraisal Checklist for Randomized Controlled Trials [23]. | |||||
| Criteria | Yes | No | Unclear | Not Applicable | |
| 1 | Was true randomization used for assignment of participants to treatment groups? | ||||
| 2 | Was allocation to treatment groups concealed? | ||||
| 3 | Were treatment groups similar at the baseline? | ||||
| 4 | Were participants blind to treatment assignment? | ||||
| 5 | Were those delivering treatment blind to treatment assignment? | ||||
| 6 | Were outcomes assessors blind to treatment assignment? | ||||
| 7 | Were treatment groups treated identically other than the intervention of interest? | ||||
| 8 | Was follow-up complete and if not, were differences between groups in terms of their follow-up adequately described and analyzed? | ||||
| 9 | Were participants analyzed in the groups to which they were randomized? | ||||
| 10 | Were outcomes measured in the same way for treatment groups? | ||||
| 11 | Were outcomes measured in a reliable way? | ||||
| 12 | Was appropriate statistical analysis used? | ||||
| 13 | Was the trial design appropriate, and any deviations from the standard RCT design (individual randomization, parallel groups) accounted for in the conduct and analysis of the trial? | ||||
| Overall appraisal: Include/Exclude/Seek further info | |||||
| B. JBI Critical Appraisal Checklist for Cohort Studies [23]. | |||||
| Criteria | Yes | No | Unclear | Not Applicable | |
| 1 | Were the two groups similar and recruited from the same population? | ||||
| 2 | Were the exposures measured similarly to assign people to both exposed and unexposed groups? | ||||
| 3 | Was the exposure measured in a valid and reliable way? | ||||
| 4 | Were confounding factors identified? | ||||
| 5 | Were strategies to deal with confounding factors stated? | ||||
| 6 | Were the groups/participants free of the outcome at the start of the study (or at the moment of exposure)? | ||||
| 7 | Were the outcomes measured in a valid and reliable way? | ||||
| 8 | Was the follow-up time reported and sufficient to be long enough for outcomes to occur? | ||||
| 9 | Was follow-up complete, and if not, were the reasons for lack of follow-up described and explored? | ||||
| 10 | Were strategies to address incomplete follow-up utilized? | ||||
| 11 | Was appropriate statistical analysis used? | ||||
| Overall appraisal: Include/Exclude/Seek further info | |||||
References
- Bethke, A.; Pieralli, S.; Kohal, R.J.; Burkhardt, F.; von Stein-Lausnitz, M.; Vach, K.; Spies, B.C. Fracture resistance of zirconia oral implants in vitro: A systematic review and meta-analysis. Materials 2020, 13, 562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kunrath, M.F.; Gupta, S.; Lorusso, F.; Scarano, A.; Noumbissi, S. Oral tissue interactions and cellular response to zirconia implant-prosthetic components: A critical review. Materials 2021, 14, 2825. [Google Scholar] [CrossRef] [PubMed]
- Comisso, I.; Arias-Herrera, S.; Gupta, S. Zirconium dioxide implants as an alternative to titanium: A systematic review. J. Clin. Exp. Dent. 2021, 13, e511–e519. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.T.; Eo, M.Y.; Nguyen, T.T.H.; Kim, S.M. General review of titanium toxicity. Int. J. Implant Dent. 2019, 5, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katsoulis, J.; Fierz, J.; Iizuka, T.; Mericske-Stern, R. Prosthetic rehabilitation, implant survival and quality of life 2 to 5 years after resection of oral tumors. Clin. Implant. Dent. Relat. Res. 2013, 15, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Javed, F.; Al-Hezaimi, K.; Al-Rasheed, A.; Almas, K.; Romanos, G.E. Implant survival rate after oral cancer therapy: A review. Oral Oncol. 2010, 46, 854–859. [Google Scholar] [CrossRef] [PubMed]
- Hessling, S.A.; Wehrhan, F.; Schmitt, C.M.; Weber, M.; Schlittenbauer, T.; Scheer, M. Implant-based rehabilitation in oncology patients can be performed with high long-term success. J. Oral Maxillofac. Surg. 2015, 73, 889–896. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, T.; Sasaki, A.; Saito, I.; Arimoto, S.; Yatagai, N.; Hiraoka, Y.; Takeda, D.; Kakei, Y.; Akashi, M. Success of dental implants in patients with large bone defect and analysis of risk factors for implant failure: A non-randomized retrospective cohort study. Clin. Oral Investig. 2021. [Google Scholar] [CrossRef] [PubMed]
- Munro, T.; Miller, C.M.; Antunes, E.; Sharma, D. Interactions of osteoprogenitor cells with a novel zirconia implant surface. J. Funct. Biomater. 2020, 11, 50. [Google Scholar] [CrossRef]
- Hadyaoui, D.; Daouahi, N.; Nouira, Z.; Cherif, M. Gingival harmony in anterior aesthetic restorations. Dent. J. 2014, 2, 155–162. [Google Scholar] [CrossRef] [Green Version]
- Agustin-Panadero, R.; Serra-Pastor, B.; Fons-Font, A.; Sola-Ruiz, M.F. Prospective clinical study of zirconia full-coverage restorations on teeth prepared with biologically oriented preparation technique on gingival health: Results after two-year follow-up. Oper. Dent. 2018, 43, 482–487. [Google Scholar] [CrossRef] [PubMed]
- Kohal, R.-J.; Dennison, D.K. Clinical longevity of zirconia implants with the focus on biomechanical and biological outcome. Curr. Oral Health Rep. 2020, 7, 344–351. [Google Scholar] [CrossRef]
- Riemer, L.K.R. Ceramic implant systems and the influence of artificial hydrothermal aging on their breaking strength—An in vitro study. Dent. Prosthet. Clin. 2018. [Google Scholar] [CrossRef]
- Spies, B.C.; Fross, A.; Adolfsson, E.; Bagegni, A.; Doerken, S.; Kohal, R.J. Stability and aging resistance of a zirconia oral implant using a carbon fiber-reinforced screw for implant-abutment connection. Dent. Mater. 2018, 34, 1585–1595. [Google Scholar] [CrossRef]
- Garcia-Hammaker, S.; Saglik, B.; Sierraalta, M.; Razzoog, M. Influence of screw channel angulation on the fracture resistance of zirconia abutments: An in vitro study. J. Prosthodont. 2021, 30, 329–334. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. PLoS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K.; et al. Systematic reviews of etiology and risk. In Joanna Briggs Institute Reviewer’s Manual; Aromataris, E., Munn, Z., Eds.; The Joanna Briggs Institute: Adeleide, Australia, 2017; Chapter 7. [Google Scholar]
- Tufanaru, C.; Munn, Z.; Aromataris, E.; Campbell, J.; Hopp, L. Systematic reviews of effectiveness. In Joanna Briggs Institute Reviewer’s Manual; Aromataris, E., Munn, Z., Eds.; The Joanna Briggs Institute: Adeleide, Australia, 2017; Chapter 3. [Google Scholar]
- J.B. Institute. Joanna Briggs Institute (JBI) SUMARI. 2019. Available online: https://sumari.jbi.global/ (accessed on 7 January 2022).
- Paolantoni, G.; Marenzi, G.; Blasi, A.; Mignogna, J.; Sammartino, G. Findings of a four-year randomized controlled clinical trial comparing two-piece and one-piece zirconia abutments supporting single prosthetic restorations in maxillary anterior region. Biomed. Res. Int. 2016, 2016, 8767845. [Google Scholar] [CrossRef] [Green Version]
- Roehling, S.; Woelfler, H.; Hicklin, S.; Kniha, H.; Gahlert, M. A Retrospective clinical study with regard to survival and success rates of zirconia implants up to and after 7 years of loading. Clin. Implant. Dent. Relat. Res. 2016, 18, 545–558. [Google Scholar] [CrossRef]
- Scherrer, S.S.; Mekki, M.; Crottaz, C.; Gahlert, M.; Romelli, E.; Marger, L.; Durual, S.; Vittecoq, E. Translational research on clinically failed zirconia implants. Dent. Mater. 2019, 35, 368–388. [Google Scholar] [CrossRef]
- Joanna Briggs Institute. Critical Appraisal Tools; Joanna Briggs Institute: Adeleide, Australia, 2018. [Google Scholar]
- Liaw, K.; Delfini, R.H.; Abrahams, J.J. Dental implant complications. Semin. Ultrasound. CT MRI 2015, 36, 427–433. [Google Scholar] [CrossRef]
- Dutta, S.R.; Passi, D.; Singh, P.; Atri, M.; Mohan, S.; Sharma, A. Risks and complications associated with dental implant failure: Critical update. Natl. J. Maxillofac. Surg. 2020, 11, 14–19. [Google Scholar]
- Do, T.A.; Le, H.S.; Shen, Y.W.; Huang, H.L.; Fuh, L.J. Risk factors related to late failure of dental implant—A systematic review of recent studies. Int. J. Environ. Res. Public Health 2020, 17, 3931. [Google Scholar] [CrossRef] [PubMed]
- Castellanos-Cosano, L.; Rodriguez-Perez, A.; Spinato, S.; Wainwright, M.; Machuca-Portillo, G.; Serrera-Figallo, M.A.; Torres-Lagares, D. Descriptive retrospective study analyzing relevant factors related to dental implant failure. Med. Oral Patol. Oral Cir. Bucal 2019, 24, e726–e738. [Google Scholar] [CrossRef] [PubMed]
- Bosshardt, D.D.; Chappuis, V.; Buser, D. Osseointegration of titanium, titanium alloy and zirconia dental implants: Current knowledge and open questions. Periodontol. 2000 2017, 73, 22–40. [Google Scholar] [CrossRef] [PubMed]
- Afrashtehfar, K.I.; del Fabbro, M. Clinical performance of zirconia implants: A meta-review. J. Prosthet. Dent. 2020, 123, 419–426. [Google Scholar] [CrossRef]
- Osman, R.B.; van der Veen, A.J.; Huiberts, D.; Wismeijer, D.; Alharbi, N. 3D-printing zirconia implants; a dream or a reality? An in-vitro study evaluating the dimensional accuracy, surface topography and mechanical properties of printed zirconia implant and discs. J. Mech. Behav. Biomed. Mater. 2017, 75, 521–528. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Attard, L.; Lee, V.; Le, J.; Lowe, C.; Singh, V.; Zhao, J.; Sharma, D. Mechanical Factors Implicated in Zirconia Implant Fracture Placed within the Anterior Region—A Systematic Review. Dent. J. 2022, 10, 22. https://doi.org/10.3390/dj10020022
Attard L, Lee V, Le J, Lowe C, Singh V, Zhao J, Sharma D. Mechanical Factors Implicated in Zirconia Implant Fracture Placed within the Anterior Region—A Systematic Review. Dentistry Journal. 2022; 10(2):22. https://doi.org/10.3390/dj10020022
Chicago/Turabian StyleAttard, Lauryn, Victoria Lee, Jennifer Le, Chloe Lowe, Vipra Singh, Jacky Zhao, and Dileep Sharma. 2022. "Mechanical Factors Implicated in Zirconia Implant Fracture Placed within the Anterior Region—A Systematic Review" Dentistry Journal 10, no. 2: 22. https://doi.org/10.3390/dj10020022