
Personalised External Aortic Root Support (PEARS) Compared with Alternatives for People with Life-Threatening Genetically Determined Aneurysms of the Aortic Root



Abstract
:1. Introduction
1.1. Clinical Niche
1.2. Existing Surgical Practice
1.2.1. Total Root Replacement (TRR)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Statement |
|---|
| 1. Marfan Syndrome has been estimated at 1:9800 [9] † |
| 2. The UK population is 63.2 million |
| 3. There are about 6500 people with Marfan syndrome in the UK |
| 4. The average Marfan life expectancy is now >50 years and the Marfan Foundation (USA PPI view) say people with Marfan can live a normal life expectancy into their 70’s |
| 5. The number of people becoming eligible for a root operation is estimated to be about 110 per year |
| 6. About 85% of MFS patients might have an aortic intervention |
| 7. About 110 aortic root operations are needed per year in the UK * |
| TRR (972) * | VSRR (413) * | PEARS (30) ** | |
|---|---|---|---|
| Patients | |||
| Mean age (years) | 35 | 33 | 28 (IQR 20–44) |
| Mean pre-op Ao. root size (mm) | 61 | 52 | 46 (IQR 43–48) |
| Follow up events per decade | |||
| Re-intervention on aortic valve | 3% | 13% | None to date |
| Thrombo-embolic events | 7% | 3% | None to date |
| Composite valve events | 13% | 19% | None to date |
1.2.2. Valve Sparing Root Replacement (VSRR)
1.3. What Patients Value
1.3.1. Avoidance of Anticoagulation Has a High Priority for Young Patients, Allowing Pregnancy, Active Sports and Normal Lifestyle
1.3.2. Anticoagulation with Coumadin/Warfarin Is Regarded by Some as a Small Price to Pay
2. Experimental Section
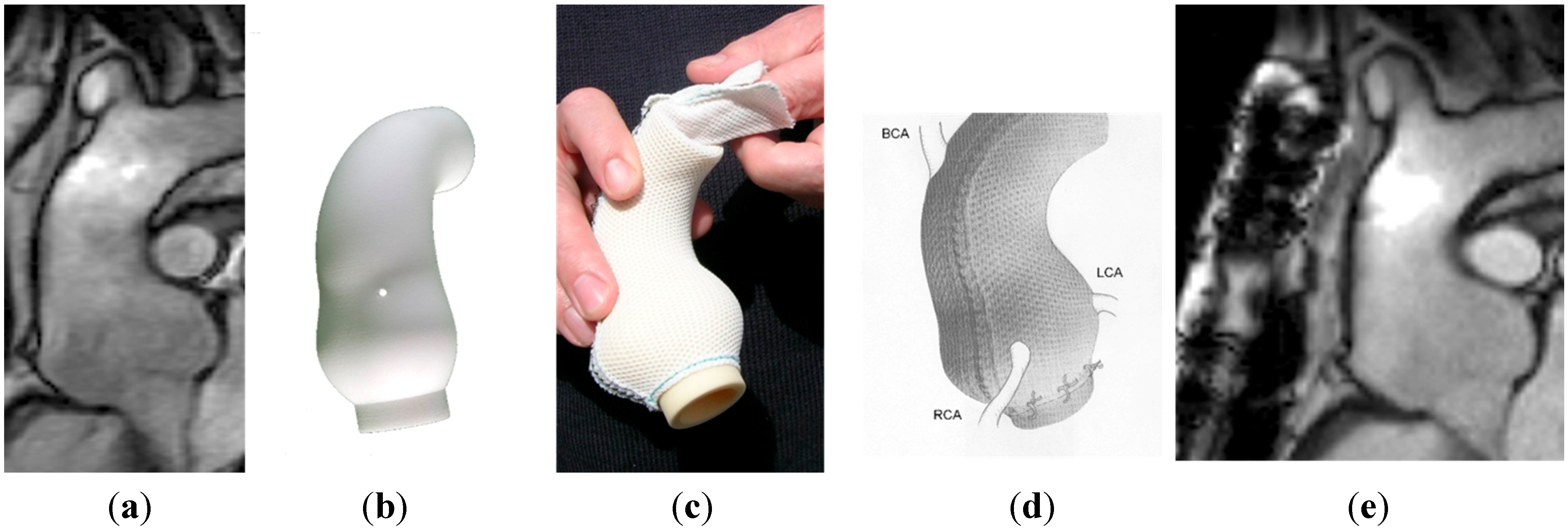
What External Support (PEARS) Entails

| VSRR * (N = 239) | IQR | PEARS (N = 30) | IQR | |
|---|---|---|---|---|
| Operation time minutes, median (IQR) | 340 | 275–441 | 145 | 136–165 |
| Bypass time minutes, median (IQR) | 194 | 248–270 | 0 | One patient |
| Myocardial ischaemia median (IQR) | 156 | 117–221 | 0 | 0–0 |
| Circulatory arrest | 48 (20%) | 0 | 0 | |
| Transfusion | Usual | 1 (3%) | ||
| Coagulation aid (FFP, platelets) | Common | 1 (3%) |
3. Results and Discussion
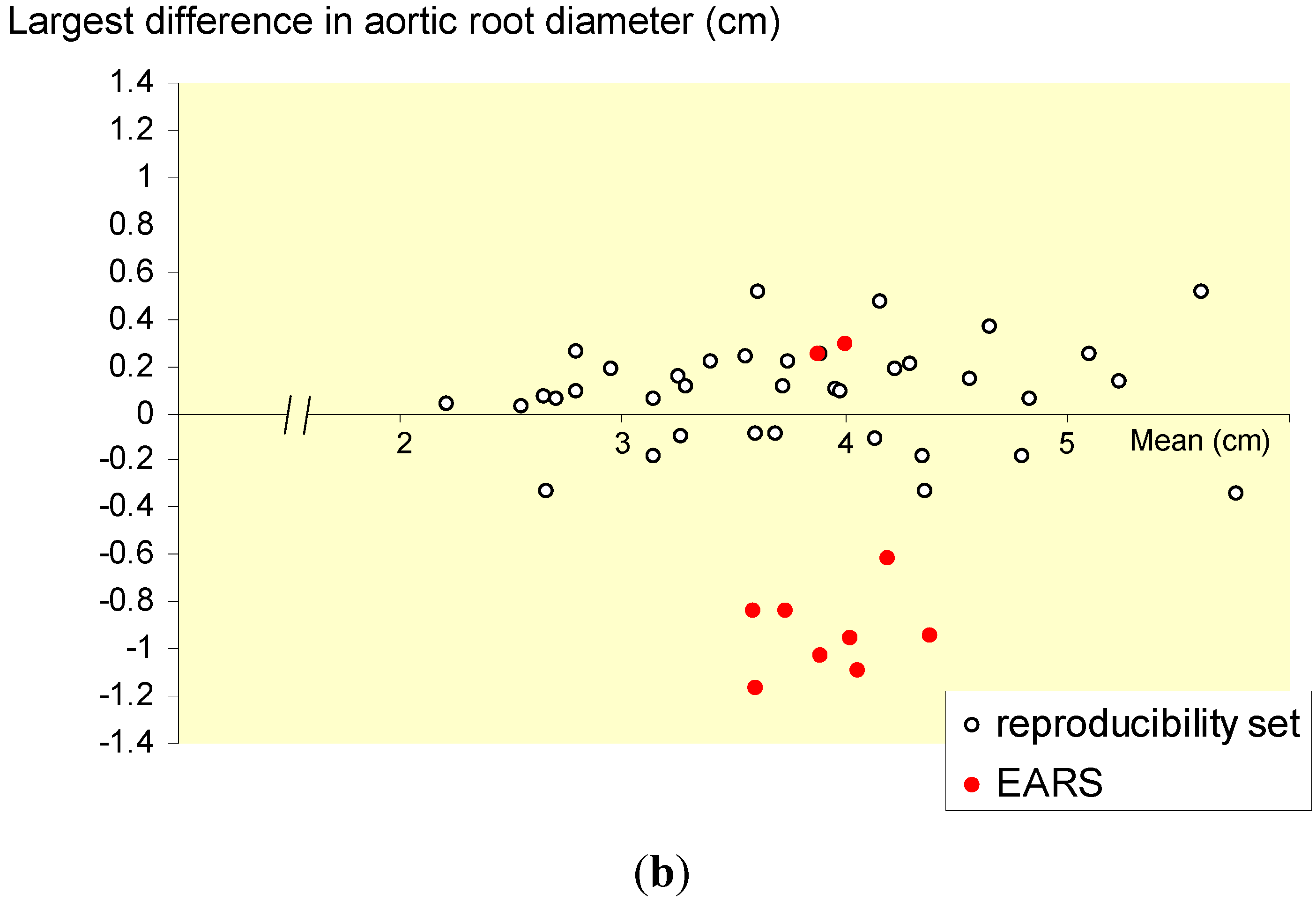
3.1. What External Support (PEARS) Offers


| Mean of diameters N = 24 | Before | Latest after |
|---|---|---|
| Aortic annulus (mm) | 29 | 29 |
| Sinus Valsalva largest diameter (mm) | 45 | 44 * |
| Ascending aorta (mm) | 32 | 33 |
| Arch (mm) | 24 | 24 |
| Descending aorta (mm) | 23 | 24 |
3.2. Cost Implications

4. Conclusions
Acknowledgments
Author contributions
Conflicts of Interest
References
- Treasure, T.; Pepper, J.; Golesworthy, T.; Mohiaddin, R.; Anderson, R.H. External aortic root support: NICE guidance. Heart 2012, 98, 65–68. [Google Scholar] [CrossRef] [PubMed]
- Golesworthy, T.; Lamperth, M.; Mohiaddin, R.; Pepper, J.; Thornton, W.; Treasure, T. A jacket for the Marfan’s aorta. Lancet 2004, 364, 1582. [Google Scholar] [CrossRef] [PubMed]
- Barkun, J.S.; Aronson, J.K.; Feldman, L.S.; Maddern, G.J.; Strasberg, S.M.; Altman, D.G.; Barkun, J.S.; Blazeby, J.M.; Boutron, I.C.; Campbell, W.B.; et al. Evaluation and stages of surgical innovations. Lancet 2009, 374, 1089–1096. [Google Scholar] [CrossRef] [PubMed]
- Ergina, P.L.; Cook, J.A.; Blazeby, J.M.; Boutron, I.; Clavien, P.A.; Reeves, B.C.; Seiler, C.M.; Altman, D.G.; Aronson, J.K.; Barkun, J.S.; et al. Challenges in evaluating surgical innovation. Lancet 2009, 374, 1097–1104. [Google Scholar] [CrossRef] [PubMed]
- McCulloch, P.; Altman, D.G.; Campbell, W.B.; Flum, D.R.; Glasziou, P.; Marshall, J.C.; Nicholl, J.; Aronson, J.K.; Barkun, J.S.; Blazeby, J.M.; et al. No surgical innovation without evaluation: the IDEAL recommendations. Lancet 2009, 374, 1105–1112. [Google Scholar] [CrossRef]
- Cook, J.A.; McCulloch, P.; Blazeby, J.M.; Beard, D.J.; Marinac-Dabic, D.; Sedrakyan, A. IDEAL framework for surgical innovation 3: Randomised controlled trials in the assessment stage and evaluations in the long term study stage. BMJ 2013, 346, f2820. [Google Scholar] [CrossRef] [PubMed]
- Ergina, P.L.; Barkun, J.S.; McCulloch, P.; Cook, J.A.; Altman, D.G. IDEAL framework for surgical innovation 2: observational studies in the exploration and assessment stages. BMJ 2013, 346, f3011. [Google Scholar] [CrossRef] [PubMed]
- McCulloch, P.; Cook, J.A.; Altman, D.G.; Heneghan, C.; Diener, M.K. IDEAL framework for surgical innovation 1: The idea and development stages. BMJ 2013, 346, f3012. [Google Scholar] [CrossRef] [PubMed]
- Gray, J.R.; Bridges, A.B.; Faed, M.J.; Pringle, T.; Baines, P.; Dean, J.; Boxer, M. Ascertainment and severity of Marfan syndrome in a Scottish population. J. Med. Genet. 1994, 31, 51–54. [Google Scholar] [CrossRef] [PubMed]
- Chiu, H.H.; Wu, M.H.; Chen, H.C.; Kao, F.Y.; Huang, S.K. Epidemiological profile of Marfan syndrome in a general population: a national database study. Mayo Clin. Proc. 2014, 89, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Murdoch, J.L.; Walker, B.A.; Halpern, B.L.; Kuzma, J.W.; McKusick, V.A. Life expectancy and causes of death in the Marfan syndrome. N. Engl. J. Med. 1972, 286, 804–808. [Google Scholar] [CrossRef] [PubMed]
- Judge, D.P.; Dietz, H.C. Marfan's syndrome. Lancet 2005, 366, 1965–1976. [Google Scholar] [CrossRef] [PubMed]
- Silverman, D.I.; Burton, K.J.; Gray, J.; Bosner, M.S.; Kouchoukos, N.T.; Roman, M.J.; Boxer, M.; Devereux, R.B.; Tsipouras, P. Life expectancy in the Marfan syndrome. Am. J. Cardiol. 1995, 75, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Vahanian, A.; Alfieri, O.; Andreotti, F.; Antunes, M.J.; Baron-Esquivias, G.; Baumgartner, H.; Borger, M.A.; Carrel, T.P.; De, B.M.; Evangelista, A.; et al. Guidelines on the management of valvular heart disease (version 2012). Eur. Heart J. 2012, 33, 2451–2496. [Google Scholar] [CrossRef] [PubMed]
- Treasure, T.; Waller, D.; Tan, C.; Entwisle, J.; O’Brien, M.; O’Byrne, K.; Thomas, G.; Snee, M.; Spicer, J.; Landau, D.; et al. The Mesothelioma and Radical surgery randomized controlled trial: the Mars feasibility study. J. Thorac. Oncol. 2009, 4, 1254–1258. [Google Scholar] [CrossRef] [PubMed]
- Treasure, T.; Fallowfield, L.; Lees, B.; Farewell, V. Pulmonary metastasectomy in colorectal cancer: the PulMiCC trial. Thorax 2012, 67, 185–187. [Google Scholar] [CrossRef] [PubMed]
- Treasure, T.; Takkenberg, J.J.; Pepper, J. Surgical management of aortic root disease in Marfan syndrome and other congenital disorders associated with aortic root aneurysms. Heart 2014. [Google Scholar] [CrossRef] [Green Version]
- Bentall, H.; De Bono, A. A technique for complete replacement of the ascending aorta. Thorax 1968, 23, 338–339. [Google Scholar] [CrossRef] [PubMed]
- Treasure, T. The evolution of aortic root surgery for Marfan syndrome. Interact. Cardiovasc. Thorac. Surg. 2010, 10, 353–355. [Google Scholar] [CrossRef] [PubMed]
- Benedetto, U.; Melina, G.; Takkenberg, J.J.; Roscitano, A.; Angeloni, E.; Sinatra, R. Surgical management of aortic root disease in Marfan syndrome: A systematic review and meta-analysis. Heart 2011, 97, 955–958. [Google Scholar] [CrossRef] [PubMed]
- Treasure, T.; Takkenberg, J.J.; Golesworthy, T.; Rega, F.; Petrou, M.; Rosendahl, U.; Mohiaddin, R.; Rubens, M.; Thornton, W.; Lees, B.; et al. Personalised external aortic root support (PEARS) in Marfan syndrome: analysis of 1-9 year outcomes by intention-to-treat in a cohort of the first 30 consecutive patients to receive a novel tissue and valve-conserving procedure, compared with the published results of aortic root replacement. Heart 2014, 100, 969–975. [Google Scholar] [CrossRef] [Green Version]
- McDonald, G.R.; Schaff, H.V.; Pyeritz, R.E.; McKusick, V.A.; Gott, V.L. Surgical management of patients with the Marfan syndrome and dilatation of the ascending aorta. J. Thorac. Cardiovasc. Surg. 1981, 81, 180–186. [Google Scholar]
- Gott, V.L.; Pyeritz, R.E.; Magovern, G.J., Jr.; Cameron, D.E.; McKusick, V.A. Surgical treatment of aneurysms of the ascending aorta in the Marfan syndrome. Results of composite-graft repair in 50 patients. N. Engl. J. Med. 1986, 314, 1070–1074. [Google Scholar] [CrossRef] [PubMed]
- Fagan, A.; Pillai, R.; Radley-Smith, R.; Yacoub, M. Results of new valve conserving operation for treatment of aneurysms or acute dissection of aortic root. (Abstract). Br. Heart J. 1983, 49, 302. [Google Scholar]
- Yacoub, M.H.; Gehle, P.; Chandrasekaran, V.; Birks, E.J.; Child, A.; Radley-Smith, R. Late results of a valve-preserving operation in patients with aneurysms of the ascending aorta and root. J. Thorac. Cardiovasc. Surg. 1998, 115, 1080–1090. [Google Scholar] [CrossRef] [PubMed]
- Birks, E.J.; Webb, C.; Child, A.; Radley-Smith, R.; Yacoub, M.H. Early and long-term results of a valve-sparing operation for Marfan syndrome. Circulation 1999, 100 (Suppl. 19), II29–II35. [Google Scholar] [CrossRef] [PubMed]
- David, T.E.; Armstrong, S.; Ivanov, J.; Feindel, C.M.; Omran, A.; Webb, G. Results of aortic valve-sparing operations. J. Thorac. Cardiovasc. Surg. 2001, 122, 39–46. [Google Scholar] [CrossRef] [PubMed]
- David, T.E. For everything there is a season. J. Thorac. Cardiovasc. Surg. 2005, 130, 961–965. [Google Scholar] [CrossRef] [PubMed]
- David, T.E.; Armstrong, S.; Maganti, M.; Colman, J.; Bradley, T.J. Long-term results of aortic valve-sparing operations in patients with Marfan syndrome. J. Thorac. Cardiovasc. Surg. 2009, 138, 859–864. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, M.; Baraki, H.; Maeding, I.; Fitzner, S.; Sarikouch, S.; Khaladj, N.; Hagl, C.; Haverich, A. Long-term results after aortic valve-sparing operation (David I). Eur. J. Cardiothorac. Surg. 2012, 41, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Coselli, J.S.; Volguina, I.V.; Lemaire, S.A.; Sundt, T.M.; Connolly, H.M.; Stephens, E.H.; Schaff, H.V.; Milewicz, D.M.; Vricella, L.A.; Dietz, H.C.; et al. Early and 1-year outcomes of aortic root surgery in patients with Marfan syndrome: A prospective, multicenter, comparative study. J. Thorac. Cardiovasc. Surg. 2014, 147, 1758–1767. [Google Scholar] [CrossRef] [PubMed]
- Fosbraey, J. The psychosocial impact of personalised external aortic root support surgery in Marfan syndrome. Masters Dissertation; Health Psychology: King’s College London, 2014. Available from: http://www.marfanaorticrootsupport.org/images/downloads/The_psychosocial_impact_of_personalised_external_aortic_root_support_surgery_in_Marfan_syndrome.pdf (accessed on 3 January 2015).
- Van Geldorp, M.W.; Eric Jamieson, W.R.; Kappetein, A.P.; Ye, J.; Fradet, G.J.; Eijkemans, M.J.; Grunkemeier, G.L.; Bogers, A.J.; Takkenberg, J.J. Patient outcome after aortic valve replacement with a mechanical or biological prosthesis: Weighing lifetime anticoagulant-related event risk against reoperation risk. J. Thorac. Cardiovasc. Surg. 2009, 137, 881–885. [Google Scholar] [CrossRef] [PubMed]
- Mokhles, M.M.; Kortke, H.; Stierle, U.; Wagner, O.; Charitos, E.I.; Bogers, A.J.; Gummert, J.; Sievers, H.H.; Takkenberg, J.J. Survival comparison of the Ross procedure and mechanical valve replacement with optimal self-management anticoagulation therapy: Propensity-matched cohort study. Circulation 2011, 123, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Pepper, J.; Petrou, M.; Rega, F.; Rosendahl, U.; Golesworthy, T.; Treasure, T. Implantation of an individually computer-designed and manufactured external support for the Marfan aortic root. Multimedia Manual Cardio-Thoracic Surg. 2013. [Google Scholar] [CrossRef]
- Coselli, J.S.; Volguina, I.V.; Lemaire, S.A.; Sundt, T.M.; Connolly, H.M.; Stephens, E.H.; Schaff, H.V.; Milewicz, D.M.; Vricella, L.A.; Dietz, H.C.; et al. Early and 1-year outcomes of aortic root surgery in patients with Marfan syndrome: A prospective, multicenter, comparative study. J. Thorac. Cardiovasc. Surg. 2014, 147, 1758–1767. [Google Scholar] [CrossRef] [PubMed]
- Pepper, J.; Golesworthy, T.; Utley, M.; Chan, J.; Ganeshalingam, S.; Lamperth, M.; Mohiaddin, R.; Treasure, T. Manufacturing and placing a bespoke support for the Marfan aortic root: Description of the method and technical results and status at one year for the first ten patients. Interact. Cardiovasc. Thorac. Surg. 2010, 10, 360–365. [Google Scholar] [CrossRef] [PubMed]
- Treasure, T.; Crowe, S.; Chan, K.M.; Ranasinghe, A.; Attia, R.; Lees, B.; Utley, M.; Golesworthy, T.; Pepper, J. A method for early evaluation of a recently introduced technology by deriving a comparative group from existing clinical data: A case study in external support of the Marfan aortic root. BMJ Open 2012, 2, e000725. [Google Scholar] [PubMed]
- Allen, C.; Pepper, J. External aortic support for people with Marfan's syndrome. BMJ 2010, 340, c1692. [Google Scholar] [CrossRef] [PubMed]
- Cohen, O.; Odim, J.; De la, Z.D.; Ukatu, C.; Vyas, R.; Vyas, N.; Palatnik, K.; Laks, H. Long-term experience of girdling the ascending aorta with Dacron mesh as definitive treatment for aneurysmal dilation. Ann. Thorac. Surg. 2007, 83, S780–S784. [Google Scholar] [CrossRef] [PubMed]
- Verbrugghe, P.; Verbeken, E.; Pepper, J.; Treasure, T.; Meyns, B.; Meuris, B.; Herijgers, P.; Rega, F. External aortic root support: A histological and mechanical study in sheep. Interact. Cardiovasc. Thorac. Surg. 2013, 17, 334–339. [Google Scholar] [CrossRef] [PubMed]
- Pepper, J.; Goddard, M.; Mohiaddin, R.; Treasure, T. Histology of a Marfan aorta 4.5 years after personalized external aortic root support. Eur. J. Cardio-Thoracic Surg. 2014. [Google Scholar] [CrossRef]
- Treasure, T.; Golesworthy, T.; Pepper, J.; Ruiz, F.; Gallivan, S. Prophylactic surgery of the aortic root in Marfan Syndrome: Reconsieration of the ddecision making process in the era of customised external aortic root support. Ital. J. Vasc. Endovasc. Surg. 2011, 18, 215–223. [Google Scholar]
- Coselli, J.S.; Volguina, I.V.; Lemaire, S.A.; Sundt, T.M.; Connolly, H.M.; Stephens, E.H.; Schaff, H.V.; Milewicz, D.M.; Vricella, L.A.; Dietz, H.C.; et al. Early and 1-year outcomes of aortic root surgery in patients with Marfan syndrome: A prospective, multicenter, comparative study. J. Thorac. Cardiovasc. Surg. 2014, 147, 1758–1767. [Google Scholar] [CrossRef] [PubMed]
- Treasure, T.; Morton, D. GRIST: Growing recruitment in interventional and surgical trials. J R. Soc. Med. 2012, 105, 140–141. [Google Scholar] [CrossRef] [PubMed]
- Fiorentino, F.; Treasure, T. Pulmonary metastasectomy for colorectal cancer: Making the case for a randomized controlled trial in the zone of uncertainty. J. Thorac. Cardiovasc. Surg. 2013, 146, 748–752. [Google Scholar] [CrossRef] [PubMed]
- Fiorentino, F.; Treasure, T. Pulmonary metastasectomy: Are observational studies sufficient evidence for effectiveness? Ann. Thorac. Surg. 2013, 96, 1129–1131. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Treasure, T.; Pepper, J. Personalised External Aortic Root Support (PEARS) Compared with Alternatives for People with Life-Threatening Genetically Determined Aneurysms of the Aortic Root. Diseases 2015, 3, 2-14. https://doi.org/10.3390/diseases3010002
Treasure T, Pepper J. Personalised External Aortic Root Support (PEARS) Compared with Alternatives for People with Life-Threatening Genetically Determined Aneurysms of the Aortic Root. Diseases. 2015; 3(1):2-14. https://doi.org/10.3390/diseases3010002
Chicago/Turabian StyleTreasure, Tom, and John Pepper. 2015. "Personalised External Aortic Root Support (PEARS) Compared with Alternatives for People with Life-Threatening Genetically Determined Aneurysms of the Aortic Root" Diseases 3, no. 1: 2-14. https://doi.org/10.3390/diseases3010002