
Reaching the Diagnosis of Checkpoint Inhibitor-Induced Diabetes Mellitus in Different Clinical Scenarios: A Real-World Application of Updated Diagnostic Criteria
 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
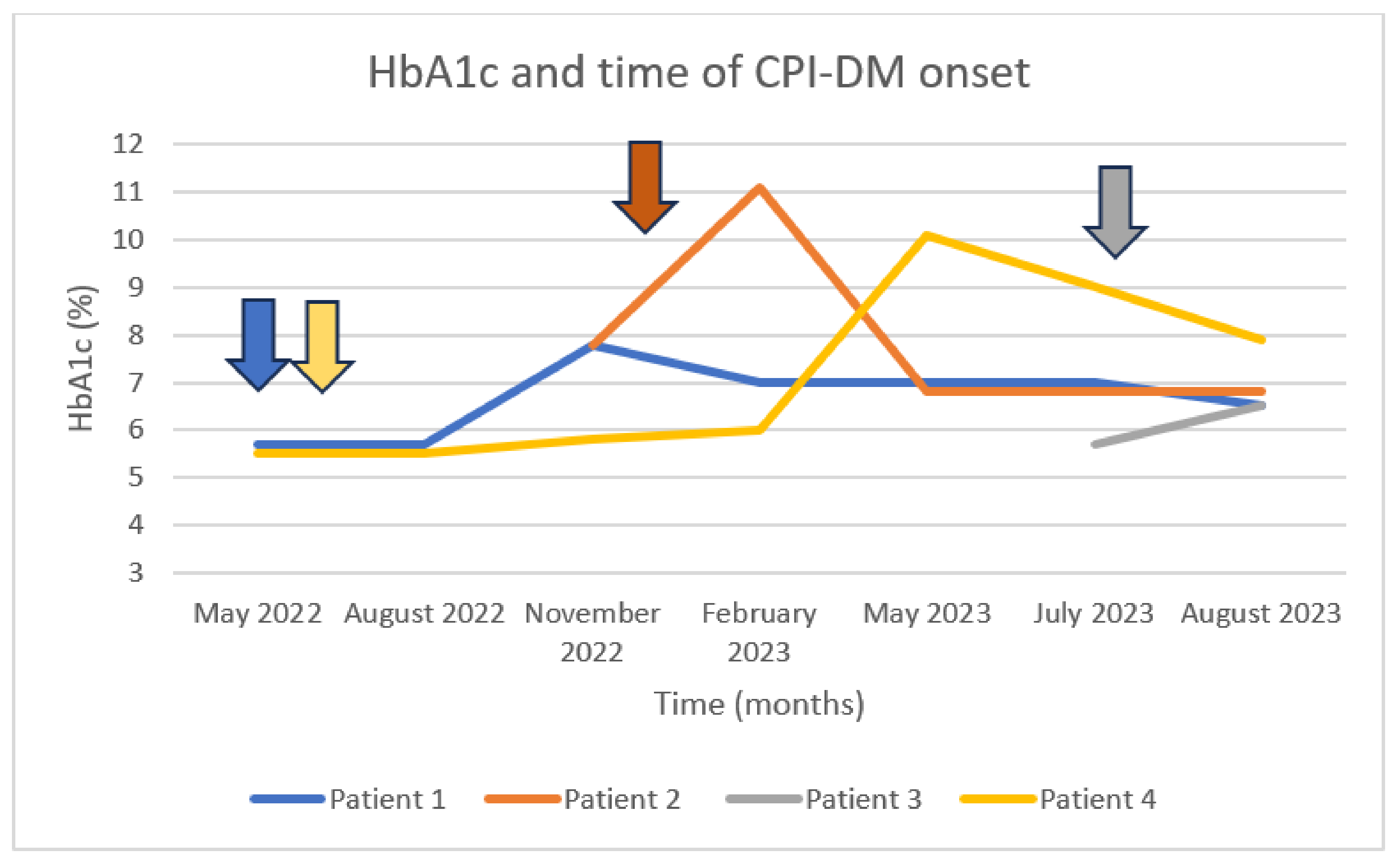
3.1. Clinical Scenario 1: Anti-IA2 Positivity
3.2. Clinical Scenario 2: Anti-GAD Positivity
3.3. Clinical Scenario 3: DKA Manifestation with Positive Anti-GAD, Anti-IA2, and Anti-ZnT8
3.4. Clinical Scenario 4: DKA Manifestation with No Antibody-Based Confirmation of CPI-DM
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pardoll, D.M. The blockade of immune checkpoints in cancer immunotherapy. Nat. Rev. Cancer 2012, 12, 252–264. [Google Scholar] [CrossRef]
- Postow, M.A.; Sidlow, R.; Hellmann, M.D. Immune-Related Adverse Events Associated with Immune Checkpoint Blockade. N. Engl. J. Med. 2018, 378, 158–168. [Google Scholar] [CrossRef] [PubMed]
- Cosio, T.; Coniglione, F.; Flaminio, V.; Gaziano, R.; Coletta, D.; Petruccelli, R.; Dika, E.; Bianchi, L.; Campione, E. Pyodermitis during Nivolumab Treatment for Non-Small Cell Lung Cancer: A Case Report and Review of the Literature. Int. J. Mol. Sci. 2023, 24, 4580. [Google Scholar] [CrossRef]
- Wright, J.J.; Powers, A.C.; Johnson, D.B. Endocrine toxicities of immune checkpoint inhibitors. Nat. Rev. Endocrinol. 2021, 17, 389–399. [Google Scholar] [CrossRef]
- Husebye, E.S.; Castinetti, F.; Criseno, S.; Curigliano, G.; Decallonne, B.; Fleseriu, M.; Higham, C.E.; Lupi, I.; Paschou, S.A.; Toth, M.; et al. Endocrine-related adverse conditions in patients receiving immune checkpoint inhibition: An ESE clinical practice guideline. Eur. J. Endocrinol. 2022, 187, G1–G21. [Google Scholar] [CrossRef] [PubMed]
- Mytareli, C.; Ziogas, D.C.; Karampela, A.; Papalexis, P.; Siampanopoulou, V.; Lafioniatis, A.; Benopoulou, O.; Gogas, H.; Angelousi, A. The Uncharted Landscape of Rare Endocrine Immune-Related Adverse Events. Cancers 2023, 15, 2016. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Tsang, V.; Menzies, A.M.; Sasson, S.C.; Carlino, M.S.; Brown, D.A.; Clifton-Bligh, R.; Gunton, J.E. Risk Factors and Characteristics of Checkpoint Inhibitor-Associated Autoimmune Diabetes Mellitus (CIADM): A Systematic Review and Delineation From Type 1 Diabetes. Diabetes Care 2023, 46, 1292–1299. [Google Scholar] [CrossRef]
- Wu, L.; Tsang, V.H.M.; Sasson, S.C.; Menzies, A.M.; Carlino, M.S.; Brown, D.A.; Clifton-Bligh, R.; Gunton, J.E. Unravelling Checkpoint Inhibitor Associated Autoimmune Diabetes: From Bench to Bedside. Front. Endocrinol. 2021, 12, 764138. [Google Scholar] [CrossRef]
- Kotwal, A.; Haddox, C.; Block, M.; Kudva, Y.C. Immune checkpoint inhibitors: An emerging cause of insulin-dependent diabetes. BMJ Open Diabetes Res. Care 2019, 7, e000591. [Google Scholar] [CrossRef]
- Stamatouli, A.M.; Quandt, Z.; Perdigoto, A.L.; Clark, P.L.; Kluger, H.; Weiss, S.A.; Gettinger, S.; Sznol, M.; Young, A.; Rushakoff, R.; et al. Collateral Damage: Insulin-Dependent Diabetes Induced With Checkpoint Inhibitors. Diabetes 2018, 67, 1471–1480. [Google Scholar] [CrossRef]
- Barroso-Sousa, R.; Barry, W.T.; Garrido-Castro, A.C.; Hodi, F.S.; Min, L.; Krop, I.E.; Tolaney, S.M. Incidence of Endocrine Dysfunction Following the Use of Different Immune Checkpoint Inhibitor Regimens: A Systematic Review and Meta-analysis. JAMA Oncol. 2018, 4, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Tsang, V.H.M.; McGrath, R.T.; Clifton-Bligh, R.J.; Scolyer, R.A.; Jakrot, V.; Guminski, A.D.; Long, G.V.; Menzies, A.M. Checkpoint Inhibitor-Associated Autoimmune Diabetes Is Distinct From Type 1 Diabetes. J. Clin. Endocrinol. Metab. 2019, 104, 5499–5506. [Google Scholar] [CrossRef] [PubMed]
- De Filette, J.M.K.; Pen, J.J.; Decoster, L.; Vissers, T.; Bravenboer, B.; Van der Auwera, B.J.; Gorus, F.K.; Roep, B.O.; Aspeslagh, S.; Neyns, B.; et al. Immune checkpoint inhibitors and type 1 diabetes mellitus: A case report and systematic review. Eur. J. Endocrinol. 2019, 181, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Zhou, H.; Zhang, Y.; Fang, W.; Yang, Y.; Huang, Y.; Zhang, L. Reporting of Immune Checkpoint Inhibitor Therapy-Associated Diabetes, 2015–2019. Diabetes Care 2020, 43, e79–e80. [Google Scholar] [CrossRef]
- Chen, X.; Affinati, A.H.; Lee, Y.; Turcu, A.F.; Henry, N.L.; Schiopu, E.; Qin, A.; Othus, M.; Clauw, D.; Ramnath, N.; et al. Immune Checkpoint Inhibitors and Risk of Type 1 Diabetes. Diabetes Care 2022, 45, 1170–1176. [Google Scholar] [CrossRef] [PubMed]
- Byun, D.J.; Braunstein, R.; Flynn, J.; Zheng, J.; Lefkowitz, R.A.; Kanbour, S.; Girotra, M. Immune Checkpoint Inhibitor-Associated Diabetes: A Single-Institution Experience. Diabetes Care 2020, 43, 3106–3109. [Google Scholar] [CrossRef]
- Shen, M.; Chen, D.; Zhao, R.; Zheng, X.; Gu, Y.; Yang, T.; Shi, Y. Real-world adherence to toxicity management guidelines for immune checkpoint inhibitor-induced diabetes mellitus. Front. Endocrinol. 2023, 14, 1213225. [Google Scholar] [CrossRef]
- ElSayed, N.A.; Aleppo, G.; Aroda, V.R.; Bannuru, R.R.; Brown, F.M.; Bruemmer, D.; Collins, B.S.; Hilliard, M.E.; Isaacs, D.; Johnson, E.L.; et al. 2. Classification and Diagnosis of Diabetes: Standards of Care in Diabetes-2023. Diabetes Care 2023, 46, S19–S40. [Google Scholar] [CrossRef]
- Kitabchi, A.E.; Umpierrez, G.E.; Miles, J.M.; Fisher, J.N. Hyperglycemic crises in adult patients with diabetes. Diabetes Care 2009, 32, 1335–1343. [Google Scholar] [CrossRef] [PubMed]
- Profili, N.I.; Castelli, R.; Gidaro, A.; Merella, A.; Manetti, R.; Palmieri, G.; Maioli, M.; Delitala, A.P. Endocrine Side Effects in Patients Treated with Immune Checkpoint Inhibitors: A Narrative Review. J. Clin. Med. 2023, 12, 5161. [Google Scholar] [CrossRef] [PubMed]
- Shalit, A.; Sarantis, P.; Koustas, E.; Trifylli, E.M.; Matthaios, D.; Karamouzis, M.V. Predictive Biomarkers for Immune-Related Endocrinopathies following Immune Checkpoint Inhibitors Treatment. Cancers 2023, 15, 375. [Google Scholar] [CrossRef]
- Lo Preiato, V.; Salvagni, S.; Ricci, C.; Ardizzoni, A.; Pagotto, U.; Pelusi, C. Diabetes mellitus induced by immune checkpoint inhibitors: Type 1 diabetes variant or new clinical entity? Review of the literature. Rev. Endocr. Metab. Disord. 2021, 22, 337–349. [Google Scholar] [CrossRef]
- Marchand, L.; Thivolet, A.; Dalle, S.; Chikh, K.; Reffet, S.; Vouillarmet, J.; Fabien, N.; Cugnet-Anceau, C.; Thivolet, C. Diabetes mellitus induced by PD-1 and PD-L1 inhibitors: Description of pancreatic endocrine and exocrine phenotype. Acta Diabetol. 2019, 56, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Cheema, A.; Makadia, B.; Karwadia, T.; Bajwa, R.; Hossain, M. Autoimmune Diabetes Associated With Pembrolizumab: A Review of Published Case Reports. World J. Oncol. 2018, 9, 1–4. [Google Scholar] [CrossRef]
- Kedzior, S.K.; Jacknin, G.; Hudler, A.; Mueller, S.W.; Kiser, T.H. A Severe Case of Diabetic Ketoacidosis and New-Onset Type 1 Diabetes Mellitus Associated with Anti-Glutamic Acid Decarboxylase Antibodies Following Immunotherapy with Pembrolizumab. Am. J. Case Rep. 2021, 22, e931702. [Google Scholar] [CrossRef] [PubMed]
- Kapke, J.; Shaheen, Z.; Kilari, D.; Knudson, P.; Wong, S. Immune Checkpoint Inhibitor-Associated Type 1 Diabetes Mellitus: Case Series, Review of the Literature, and Optimal Management. Case Rep. Oncol. 2017, 10, 897–909. [Google Scholar] [CrossRef] [PubMed]
- Gauci, M.L.; Laly, P.; Vidal-Trecan, T.; Baroudjian, B.; Gottlieb, J.; Madjlessi-Ezra, N.; Da Meda, L.; Madelaine-Chambrin, I.; Bagot, M.; Basset-Seguin, N.; et al. Autoimmune diabetes induced by PD-1 inhibitor-retrospective analysis and pathogenesis: A case report and literature review. Cancer Immunol. Immunother. 2017, 66, 1399–1410. [Google Scholar] [CrossRef] [PubMed]
- Grimmelmann, I.; Momma, M.; Zimmer, L.; Hassel, J.C.; Heinzerling, L.; Pfohler, C.; Loquai, C.; Ruini, C.; Utikal, J.; Thoms, K.M.; et al. Lipase elevation and type 1 diabetes mellitus related to immune checkpoint inhibitor therapy—A multicentre study of 90 patients from the German Dermatooncology Group. Eur. J. Cancer 2021, 149, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Basak, E.A.; de Joode, K.; Uyl, T.J.J.; van der Wal, R.; Schreurs, M.W.J.; van den Berg, S.A.A.; Oomen-de Hoop, E.; van der Leest, C.H.; Chaker, L.; Feelders, R.A.; et al. The course of C-peptide levels in patients developing diabetes during anti-PD-1 therapy. Biomed. Pharmacother. 2022, 156, 113839. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.; Marshall, J.L.; He, A.R. Workup and Management of Immune-Mediated Hepatobiliary Pancreatic Toxicities That Develop During Immune Checkpoint Inhibitor Treatment. Oncologist 2020, 25, 105–111. [Google Scholar] [CrossRef]
- Kawata, S.; Kozawa, J.; Yoneda, S.; Fujita, Y.; Kashiwagi-Takayama, R.; Kimura, T.; Hosokawa, Y.; Baden, M.Y.; Uno, S.; Uenaka, R.; et al. Inflammatory Cell Infiltration Into Islets without PD-L1 Expression Is Associated with the Development of Immune Checkpoint Inhibitor-Related Type 1 Diabetes in Genetically Susceptible Patients. Diabetes 2023, 72, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Hughes, J.; Vudattu, N.; Sznol, M.; Gettinger, S.; Kluger, H.; Lupsa, B.; Herold, K.C. Precipitation of autoimmune diabetes with anti-PD-1 immunotherapy. Diabetes Care 2015, 38, e55–e57. [Google Scholar] [CrossRef] [PubMed]
- Inaba, H.; Kaido, Y.; Ito, S.; Hirobata, T.; Inoue, G.; Sugita, T.; Yamamoto, Y.; Jinnin, M.; Kimura, H.; Kobayashi, T.; et al. Human Leukocyte Antigens and Biomarkers in Type 1 Diabetes Mellitus Induced by Immune-Checkpoint Inhibitors. Endocrinol. Metab. 2022, 37, 84–95. [Google Scholar] [CrossRef]
- Okamoto, M.; Okamoto, M.; Gotoh, K.; Masaki, T.; Ozeki, Y.; Ando, H.; Anai, M.; Sato, A.; Yoshida, Y.; Ueda, S.; et al. Fulminant type 1 diabetes mellitus with anti-programmed cell death-1 therapy. J. Diabetes Investig. 2016, 7, 915–918. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, K.; Shono-Saito, T.; Yamate, T.; Kai, Y.; Sakai, T.; Shimizu, F.; Yamada, Y.; Mori, H.; Noso, S.; Ikegami, H.; et al. A case of fulminant type 1 diabetes mellitus, with a precipitous decrease in pancreatic volume, induced by nivolumab for malignant melanoma: Analysis of HLA and CTLA-4 polymorphisms. Eur. J. Dermatol. 2017, 27, 184–185. [Google Scholar] [CrossRef]
- Usui, Y.; Udagawa, H.; Matsumoto, S.; Imai, K.; Ohashi, K.; Ishibashi, M.; Kirita, K.; Umemura, S.; Yoh, K.; Niho, S.; et al. Association of Serum Anti-GAD Antibody and HLA Haplotypes with Type 1 Diabetes Mellitus Triggered by Nivolumab in Patients with Non-Small Cell Lung Cancer. J. Thorac. Oncol. 2017, 12, e41–e43. [Google Scholar] [CrossRef]
- Ishi, A.; Tanaka, I.; Iwama, S.; Sakakibara, T.; Mastui, T.; Kobayashi, T.; Hase, T.; Morise, M.; Sato, M.; Arima, H.; et al. Efficacies of programmed cell death 1 ligand 1 blockade in non-small cell lung cancer patients with acquired resistance to prior programmed cell death 1 inhibitor and development of diabetic ketoacidosis caused by two different etiologies: A retrospective case series. Endocr. J. 2021, 68, 613–620. [Google Scholar] [CrossRef]
- Caulfield, J.I.; Aizenbud, L.; Perdigoto, A.L.; Meffre, E.; Jilaveanu, L.; Michalek, D.A.; Rich, S.S.; Aizenbud, Y.; Adeniran, A.; Herold, K.C.; et al. Germline genetic variants are associated with development of insulin-dependent diabetes in cancer patients treated with immune checkpoint inhibitors. J. Immunother. Cancer 2023, 11, e006570. [Google Scholar] [CrossRef]
- Okubo, M.; Hataya, Y.; Fujimoto, K.; Iwakura, T.; Matsuoka, N. Recovery from insulin dependence in immune checkpoint inhibitor-associated diabetes mellitus: A case report. J. Diabetes Investig. 2023, 14, 147–150. [Google Scholar] [CrossRef]


{kind=link}
| Case 1 | Case 2 | Case 3 | Case 4 | |
|---|---|---|---|---|
| Age (years)/gender (F/M) | 75/F | 57/M | 54/F | 69/M |
| Underlying cancer | Metastatic melanoma | Melanoma | Metastatic CRC | Renal cancer |
| Type of CPI | Nivolumab + ipilimumab | Pembrolizumab | Nivolumab plus + OV | Pembrolizumab |
| Previous history of DM | Yes | Yes | No | No |
| Family history of DM | Yes | Yes | Yes | No |
| BMI (kg/m2) | 32.2 | 29.1 | 23.4 | 27.7 |
| Onset of autoimmune DM presentation | 5 months | 1 month | 1 month | 12 months |
| DKA | No | No | Yes | Yes |
| Baseline glucose levels (mg/dL) | >200 | >300 | >300 | >300 |
| HbA1c (%) | 7.8 | 11.1 | 6.4 | 9.7 |
| C-peptide (0.7–5.19 ng/mL) | 3.15 | 0.31 | 0.72 | 0.93 |
| Islet autoantibodies | (+) Anti-IA2 | (+) Anti-GAD | (+) Anti-IA2, (+) anti-GAD, (+) anti-ZnT8 | Negative |
| Amylase (28–100 U/L) | 135 | 49 | 68 | 36 |
| Triglycerides (50–150 ng/dL) | 110 | 156 | 249 | 73 |
| Concurrent ir endocrinopathies | No | Hypophysitis (corticotrope axis deficiency) | Subacute thyroiditis | No |
| Follow-up since CPI-DM presentation (months) | 6 months | 3 months | 1 month | 1 month |
| Outcome | Insulin therapy–glycemic control HbA1c = 7% | Insulin therapy–glycemic control HbA1c = 6.8% | Insulin therapy–glycemic control HbA1c = 6.2% | Insulin therapy–glycemic control Hb1Ac = 9.3% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Angelousi, A.; Ziogas, D.C.; Siampanopoulou, V.; Mytareli, C.; Anastasopoulou, A.; Lyrarakis, G.; Gogas, H. Reaching the Diagnosis of Checkpoint Inhibitor-Induced Diabetes Mellitus in Different Clinical Scenarios: A Real-World Application of Updated Diagnostic Criteria. Diseases 2024, 12, 40. https://doi.org/10.3390/diseases12020040
Angelousi A, Ziogas DC, Siampanopoulou V, Mytareli C, Anastasopoulou A, Lyrarakis G, Gogas H. Reaching the Diagnosis of Checkpoint Inhibitor-Induced Diabetes Mellitus in Different Clinical Scenarios: A Real-World Application of Updated Diagnostic Criteria. Diseases. 2024; 12(2):40. https://doi.org/10.3390/diseases12020040
Chicago/Turabian StyleAngelousi, Anna, Dimitrios C. Ziogas, Vasiliki Siampanopoulou, Chrysoula Mytareli, Amalia Anastasopoulou, George Lyrarakis, and Helen Gogas. 2024. "Reaching the Diagnosis of Checkpoint Inhibitor-Induced Diabetes Mellitus in Different Clinical Scenarios: A Real-World Application of Updated Diagnostic Criteria" Diseases 12, no. 2: 40. https://doi.org/10.3390/diseases12020040