
Clinical, Epidemiological, Morphological, and Immunohistochemical Aspects of Nasopharyngeal Carcinoma—4-Year Retrospective Study in the Western Part of Romania

 , and
, and
Abstract
:1. Introduction
2. Aim of the Study
3. Patients, Materials, and Methods
4. Results
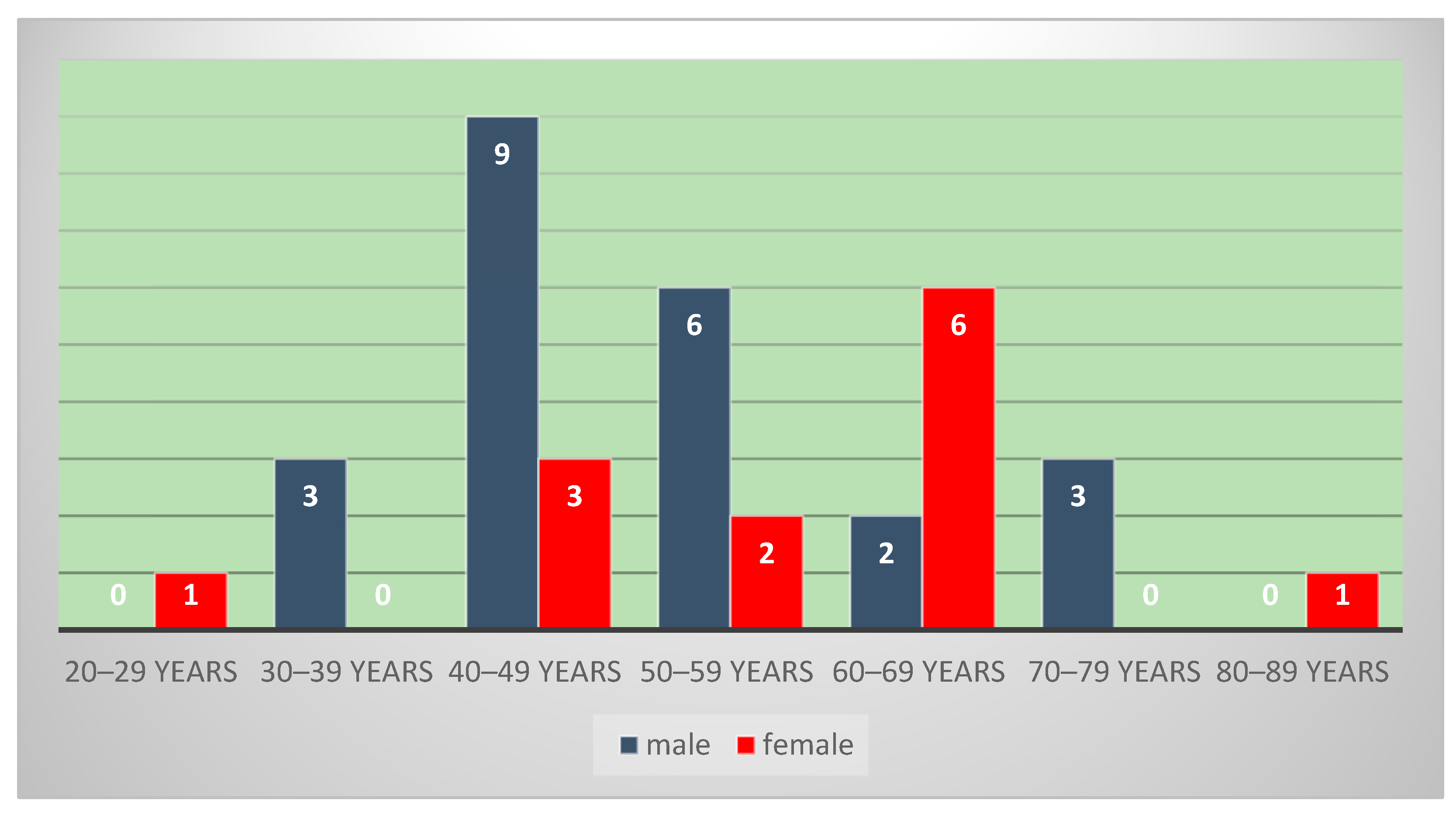
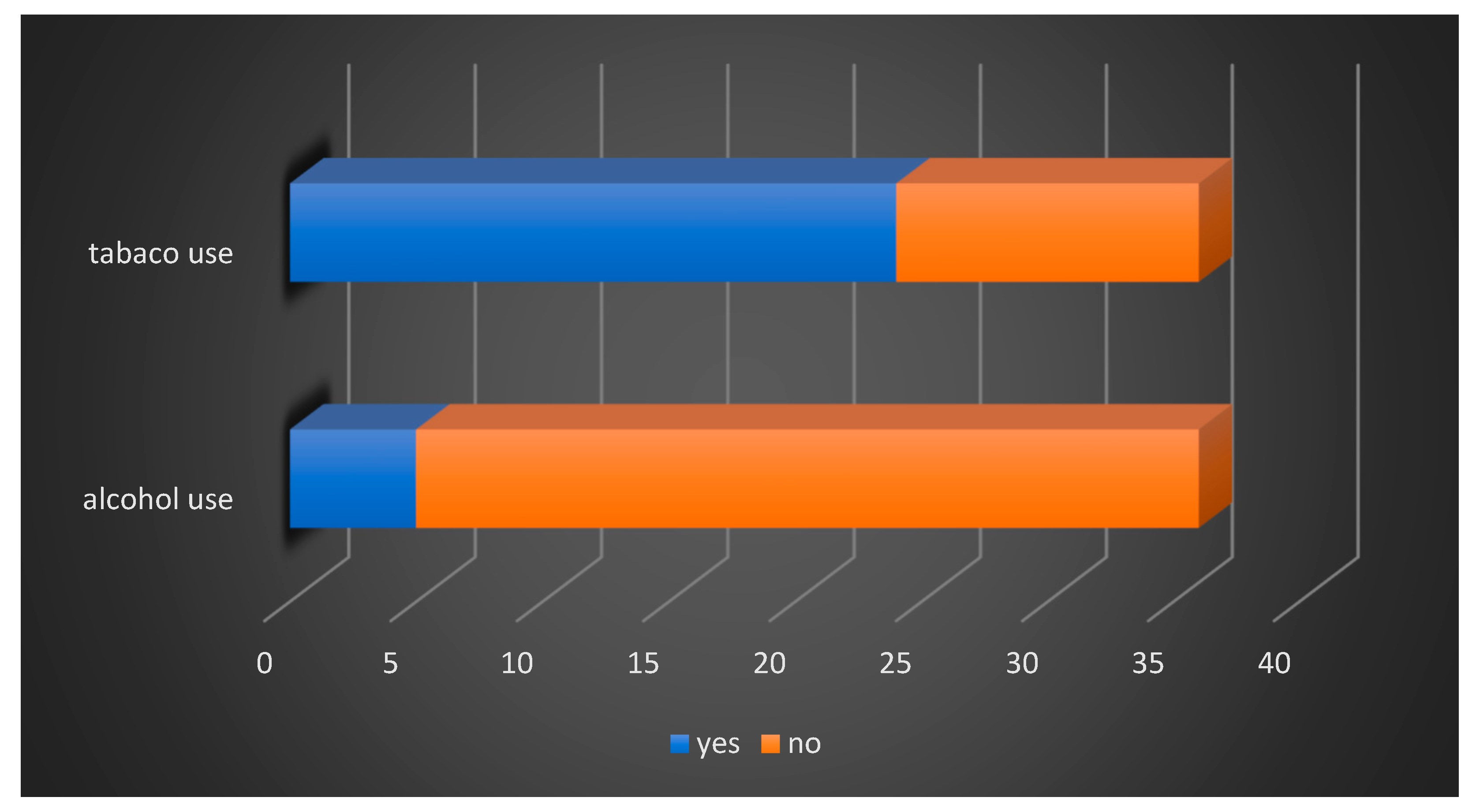
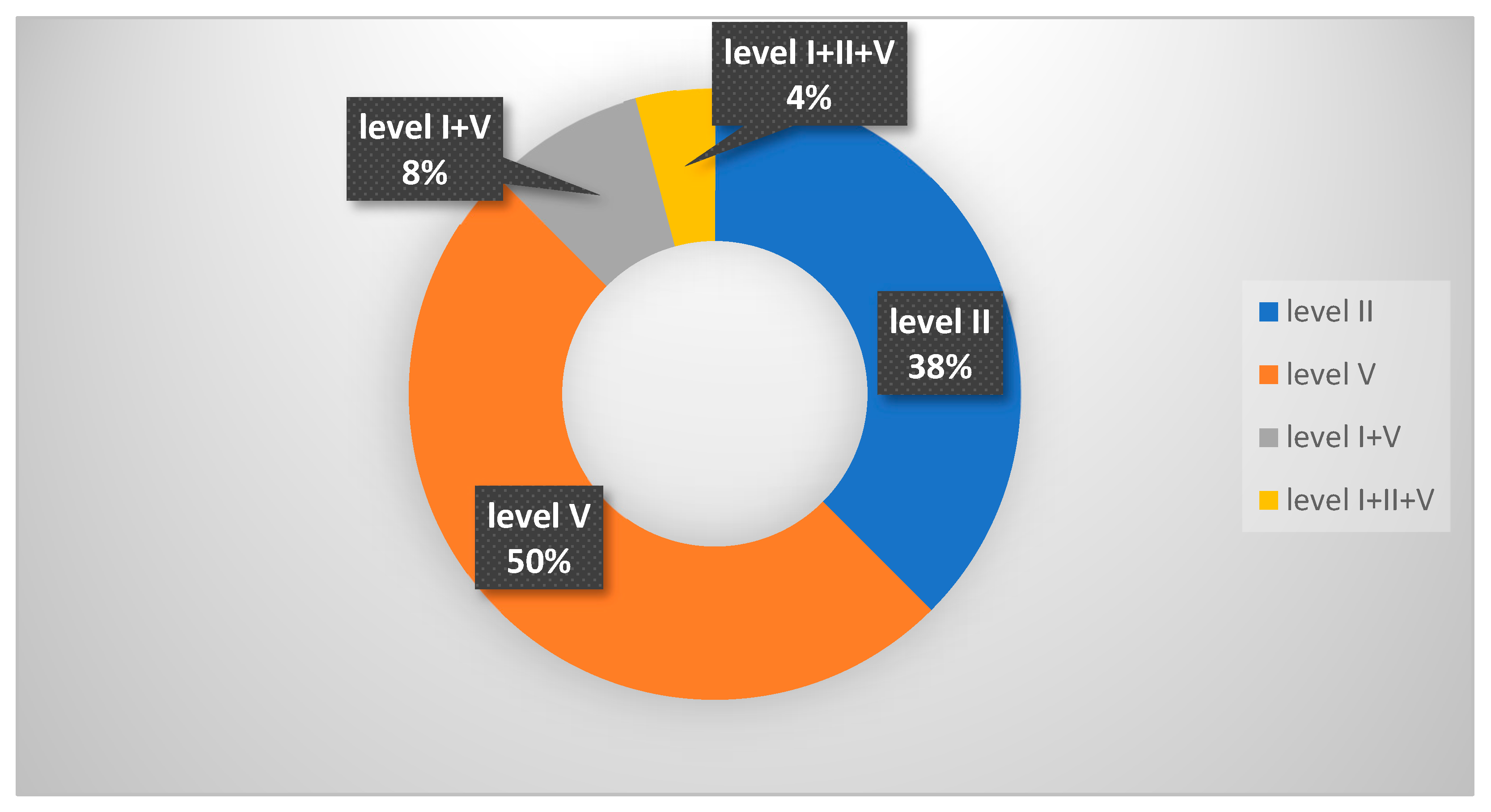
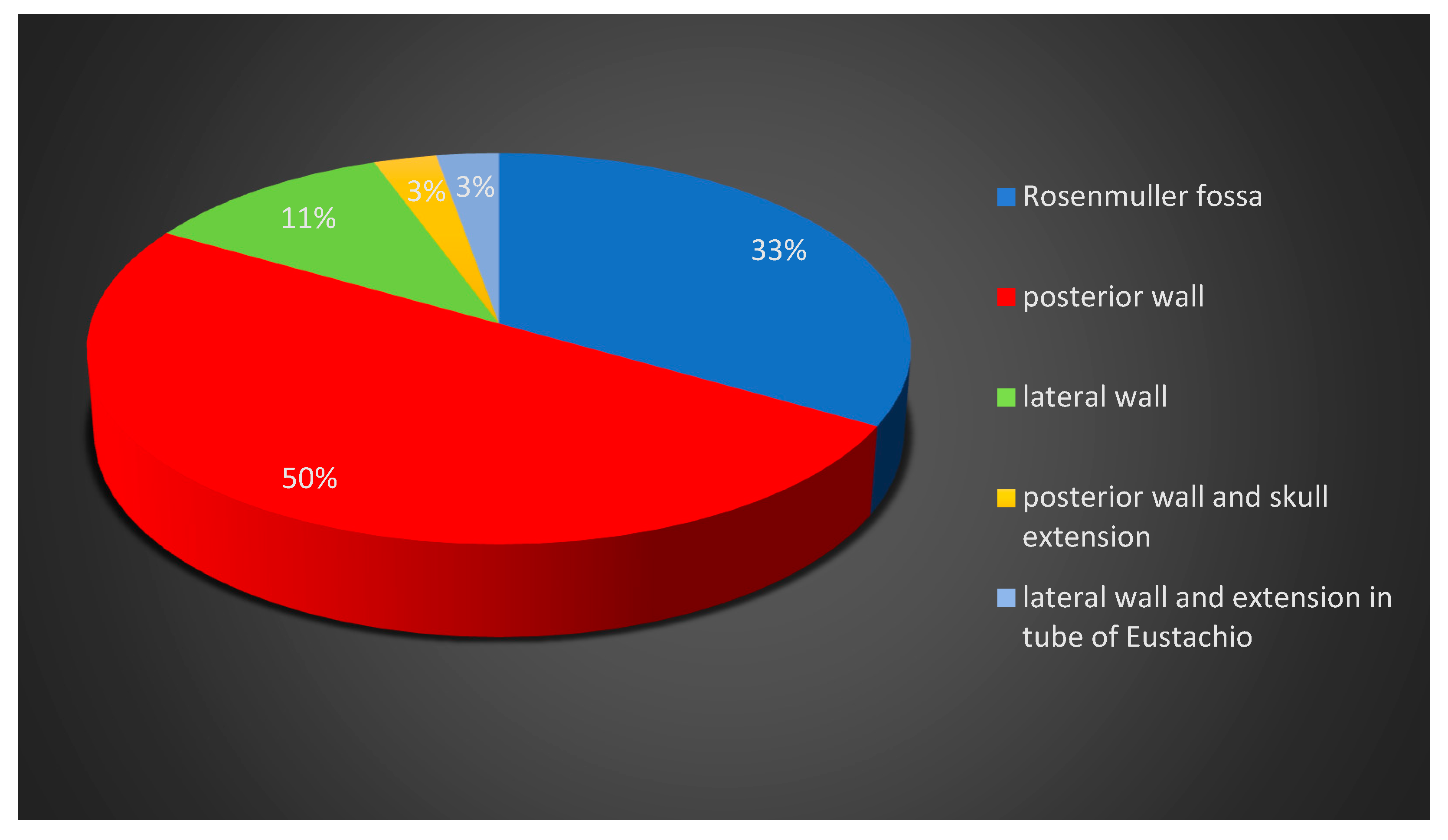
4.1. Clinical–Epidemiological Findings
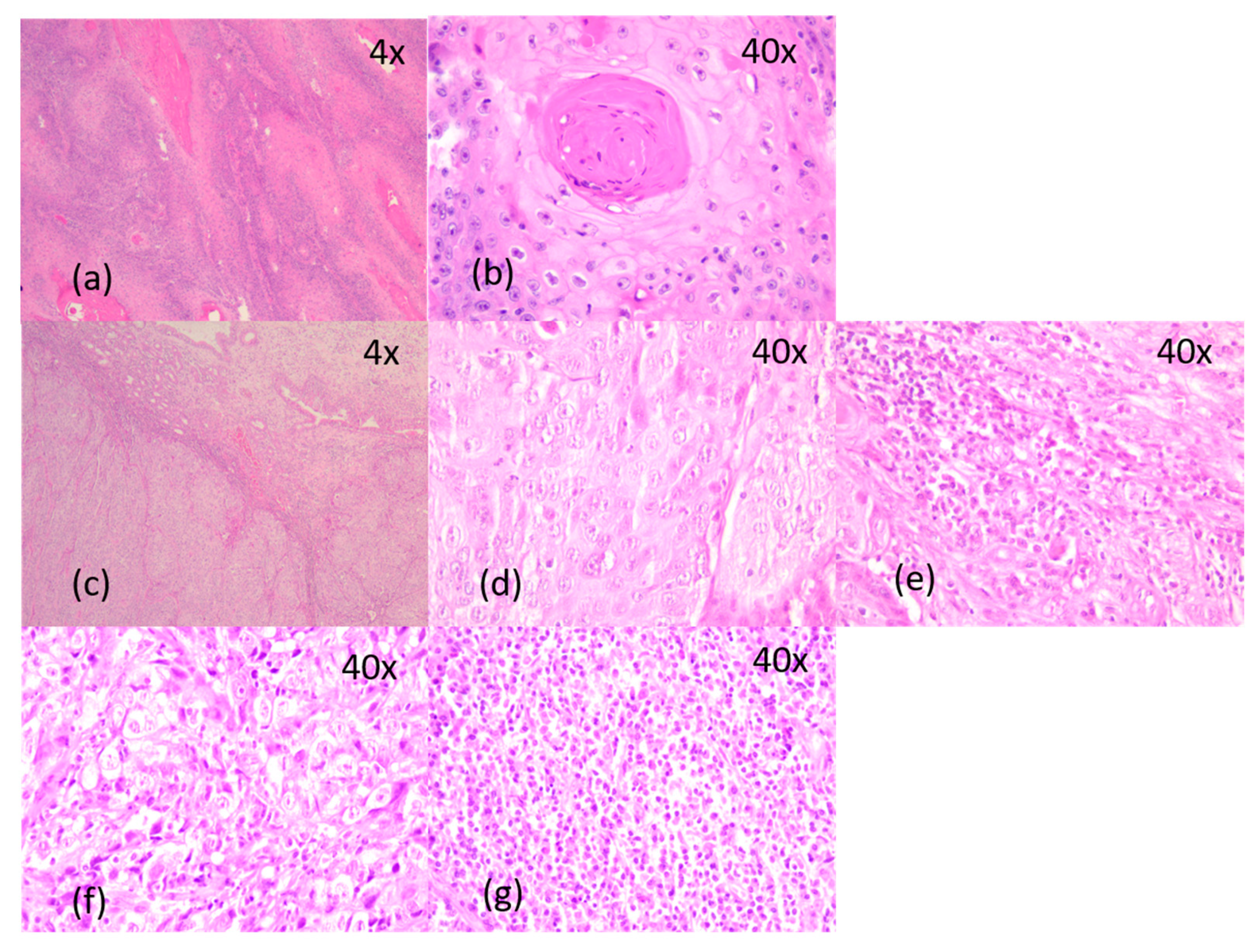
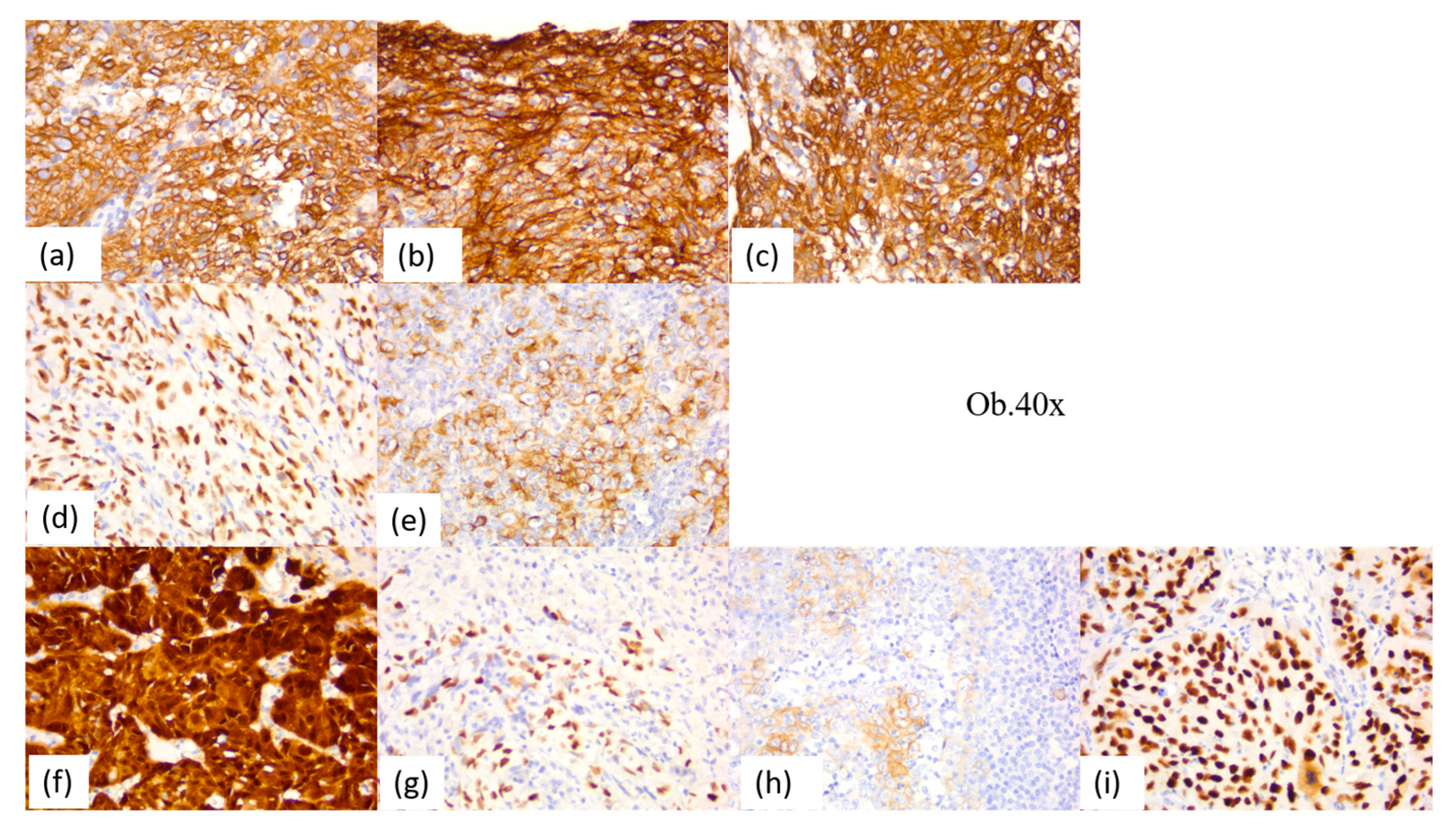
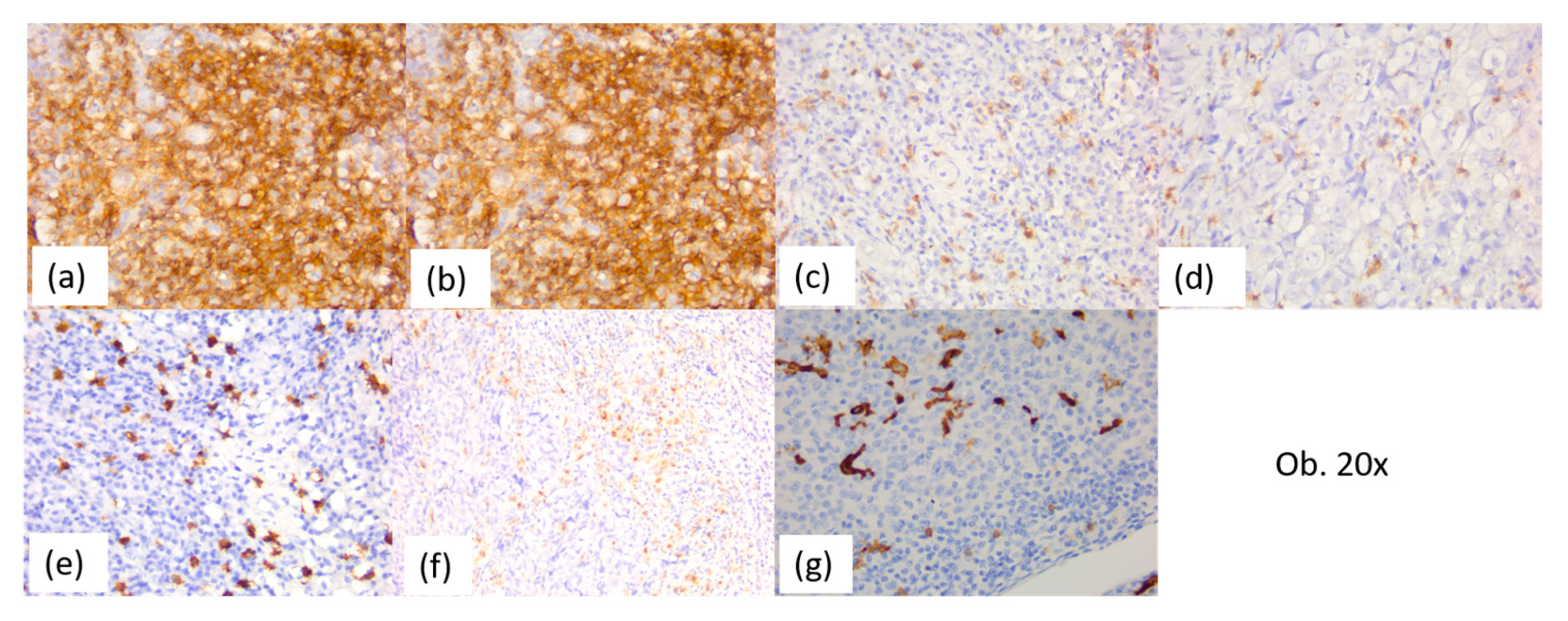
4.2. Histopathological Findings
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chen, Y.; Chan, A.T.C.; Le, Q.-T.; Blanchard, P.; Sun, Y.; Ma, J. Nasopharyngeal carcinoma. Lancet 2019, 394, 64–80. [Google Scholar] [CrossRef]
- Spano, J.-P.; Busson, P.; Atlan, D.; Bourhis, J.; Pignon, J.-P.; Esteban, C.; Armand, J.-P. Nasopharyngeal carcinomas: An update. Eur. J. Cancer 2003, 39, 2121–2135. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Cho, W.C. Nasopharyngeal carcinoma: Molecular biomarker discovery and progress. Mol. Cancer 2007, 6, 1. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Zheng, R.; Baade, P.D.; Zhang, S.; Zeng, H.; Bray, F.; Jemal, A.; Yu, X.Q.; He, J. Cancer statistics in China, 2015. CA Cancer J. Clin. 2016, 66, 115–132. [Google Scholar] [CrossRef] [PubMed]
- Young, L.S.; Dawson, C.W. Epstein-Barr virus and nasopharyngeal carcinoma. Chin. J. Cancer. 2014, 33, 581–590. [Google Scholar] [CrossRef]
- Wu, L.; Li, C.; Pan, L. Nasopharyngeal carcinoma: A review of current updates. Exp. Ther. Med. 2018, 15, 3687–3692. [Google Scholar] [CrossRef] [PubMed]
- Ear, E.N.S.; Irekeola, A.A.; Yean Yean, C. Diagnostic and Prognostic Indications of Nasopharyngeal Carcinoma. Diagnostics 2020, 10, 611. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.H.; Austin, S.A.; Chen, S.H.; Sonne, D.C.; Gurushanthaiah, D. Nasopharyngeal Carcinoma Diagnostic Challenge in a Nonendemic Setting: Our Experience with 101 Patients. Perm. J. 2017, 21, 16–180. [Google Scholar] [CrossRef] [PubMed]
- WHO Classification of Tumours Editorial Board. Head and Neck Tumours, 5th ed.; International Agency for Research on Cancer: Lyon, France, 2022. [Google Scholar]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef]
- Chua, D.T.; Sham, J.S.; Kwong, D.L.; Au, G.K. Treatment outcome after radiotherapy alone for patients with Stage I-II nasopharyngeal carcinoma. Cancer 2003, 98, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Islam, K.A.; Chow, L.K.-Y.; Kam, N.W.; Wang, Y.; Chiang, C.L.; Choi, H.C.-W.; Xia, Y.-F.; Lee, A.W.-M.; Ng, W.T.; Dai, W. Prognostic Biomarkers for Survival in Nasopharyngeal Carcinoma: A Systematic Review of the Literature. Cancers 2022, 14, 2122. [Google Scholar] [CrossRef] [PubMed]
- Ng, W.T.; Chow, J.C.H.; Beitler, J.J.; Corry, J.; Mendenhall, W.; Lee, A.W.M.; Robbins, K.T.; Nuyts, S.; Saba, N.F.; Smee, R.; et al. Current Radiotherapy Considerations for Nasopharyngeal Carcinoma. Cancers 2022, 14, 5773. [Google Scholar] [CrossRef]
- Wong, K.C.W.; Hui, E.P.; Lo, K.-W.; Lam, W.K.J.; Johnson, D.; Li, L.; Tao, Q.; Chan, K.C.A.; To, K.-F.; King, A.D.; et al. Nasopharyngeal carcinoma: An evolving paradigm. Nat. Rev. Clin. Oncol. 2021, 18, 679–695. [Google Scholar] [CrossRef]
- Taylor, G.S.; Jia, H.; Harrington, K.; Lee, L.W.; Turner, J.; Ladell, K.; Price, D.A.; Tanday, M.; Matthews, J.; Roberts, C.; et al. A recombinant modified vaccinia ankara vaccine encoding Epstein-Barr virus (EBV) target antigens: A phase I trial in UK patients with EBV-positive cancer. Clin. Cancer Res. 2014, 20, 5009–5022. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.C.; Hung, E.C.; Woo, J.K.; Chan, P.K.; Leung, S.F.; Lai, F.P.; Cheng, A.S.; Yeung, S.W.; Chan, Y.W.; Tsui, T.K.; et al. Early detection of naso-pharyngeal carcinoma by plasma Epstein-Barr virus DNA analysis in a surveillance program. Cancer 2013, 119, 1838–1844. [Google Scholar] [CrossRef]
- Gong, L.; Kwong, D.L.-W.; Dai, W.; Wu, P.; Wang, Y.; Lee, A.W.-M.; Guan, X.-Y. The stromal and immune landscape of nasopharyngeal carcinoma and its implications for precision medicine targeting the tumor microenvironment. Front. Oncol. 2021, 11, 744889. [Google Scholar] [CrossRef] [PubMed]
- Alexa, A.; Baderca, F.; Lighezan, R.; Izvernariu, D. Myofibroblasts reaction in urothelial carcinomas. Rom. J. Morphol. Embryol. 2009, 50, 639–643. [Google Scholar] [PubMed]
- Alexa, A.; Baderca, F.; Zăhoi, D.E.; Lighezan, R.; Izvernariu, D.; Raica, M. Clinical significance of Her2/neu overexpression in urothelial carcinomas. Rom. J. Morphol. Embryol. 2010, 51, 277–282. [Google Scholar] [PubMed]
- Salemme, V.; Centonze, G.; Cavallo, F.; Defilippi, P.; Conti, L. The crosstalk between tumor cells and the immune microenvironment in breast cancer: Implications for immunotherapy. Front. Oncol. 2021, 11, 610303. [Google Scholar] [CrossRef] [PubMed]
- Forder, A.; Stewart, G.L.; Telkar, N.; Lam, W.L.; Garnis, C. New insights into the tumour immune microenvironment of nasopharyngeal carcinoma. Curr. Res. Immunol. 2022, 3, 222–227. [Google Scholar] [CrossRef]
- Chen, Y.P.; Yin, J.H.; Li, W.F.; Li, H.J.; Chen, D.P.; Zhang, C.J.; Lv, J.W.; Wang, Y.Q.; Li, X.M.; Li, J.Y.; et al. Single-cell transcriptomics reveals regulators underlying immune cell diversity and immune subtypes associated with prognosis in nasopharyngeal carcinoma. Cell Res. 2020, 30, 1024–1042. [Google Scholar] [CrossRef]
- Sobti, A.; Sakellariou, C.; Nilsson, J.S.; Askmyr, D.; Greiff, L.; Lindstedt, M. Exploring Spatial Heterogeneity of Immune Cells in Nasopharyngeal Cancer. Cancers 2023, 15, 2165. [Google Scholar] [CrossRef] [PubMed]
- Pardoll, D.M. The blockade of immune checkpoints in cancer immunotherapy. Nat. Rev. Cancer 2012, 12, 252–264. [Google Scholar] [CrossRef] [PubMed]
- Masterson, L.; Howard, J.; Gonzalez-Cruz, J.; Jackson, C.; Barnett, C.; Overton, L.; Liu, H.; Ladwa, R.; Simpson, F.; McGrath, M.; et al. Immune checkpoint inhibitors in advanced nasopharyngeal carcinoma: Beyond an era of chemoradiation? Int. J. Cancer 2020, 146, 2305–2314. [Google Scholar] [CrossRef] [PubMed]
- Dasari, V.; Sinha, D.; Neller, M.A.; Smith, C.; Khanna, R. Prophylactic and therapeutic strategies for Epstein-Barr virus-associated diseases: Emerging strategies for clinical development. Expert. Rev. Vaccines 2019, 18, 457–474. [Google Scholar] [CrossRef] [PubMed]
- Cui, X.; Snapper, C.M. Epstein Barr Virus: Development of Vaccines and Immune Cell Therapy for EBV-Associated Diseases. Front. Immunol. 2021, 12, 734471. [Google Scholar] [CrossRef] [PubMed]
- Renaud, S.; Lefebvre, A.; Mordon, S.; Moralès, O.; Delhem, N. Novel Therapies Boosting T Cell Immunity in Epstein Barr Virus-Associated Nasopharyngeal Carcinoma. Int. J. Mol. Sci. 2020, 21, 4292. [Google Scholar] [CrossRef] [PubMed]
- Yoshizaki, T.; Kondo, S.; Dochi, H.; Kobayashi, E.; Mizokami, H.; Komura, S.; Endo, K. Immune Microenvironment of Nasopharyngeal Carcinoma and Epstein-Barr Virus. Encyclopedia. Available online: https://encyclopedia.pub/entry/53156 (accessed on 13 March 2024).
- Wang, Y.Q.; Chen, Y.P.; Zhang, Y.; Jiang, W.; Liu, N.; Yun, J.P.; Sun, Y.; He, Q.M.; Tang, X.R.; Wen, X.; et al. Prognostic significance of tumor-infiltrating lymphocytes in nondisseminated nasopharyngeal carcinoma: A large-scale cohort study. Int. J. Cancer 2018, 142, 2558–2566. [Google Scholar] [PubMed]
- Almangush, A.; Ruuskanen, M.; Hagström, J.; Hirvikoski, P.; Tommola, S.; Kosma, V.M.; Nieminen, P.; Mäkitie, A.; Leivo, I. Tumor-infiltrating lymphocytes associate with outcome in nonendemic nasopharyngeal carcinoma: A multicenter study. Hum. Pathol. 2018, 81, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Berele, B.A.; Cai, Y.; Yang, G. Prognostic Value of Tumor Infiltrating Lymphocytes in Nasopharyngeal Carcinoma Patients: Meta-Analysis. Technol. Cancer Res. Treat. 2021, 20, 15330338211034265. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Chen, G.; Zhang, C.; Liao, X.; Xie, J.; Liang, T.; Liao, W.; Song, L.; Zhang, X. Prognostic significance of tumor-infiltrating lymphocytes and macrophages in nasopharyngeal carcinoma: A systematic review and meta-analysis. Eur. Arch. Otorhinolaryngol. 2022, 279, 25–35. [Google Scholar] [CrossRef]
- Zheng, X.; Huang, Y.; Li, K.; Luo, R.; Cai, M.; Yun, J. Immunosuppressive Tumor Microenvironment and Immunotherapy of Epstein–Barr Virus-Associated Malignancies. Viruses 2022, 14, 1017. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, J.S.; Sobti, A.; Swoboda, S.; Erjefält, J.S.; Forslund, O.; Lindstedt, M.; Greiff, L. Immune Phenotypes of Nasopharyngeal Cancer. Cancers 2020, 12, 3428. [Google Scholar] [CrossRef]
- Lu, J.; Chen, X.M.; Huang, H.R.; Zhao, F.P.; Wang, F.; Liu, X.; Li, X.P. Detailed analysis of inflammatory cell infiltration and the prognostic impact on nasopharyngeal carcinoma. Head. Neck. 2018, 40, 1245–1253. [Google Scholar] [CrossRef]
- Nilsson, J.S.; Abolhalaj, M.; Lundberg, K.; Lindstedt, M.; Greiff, L. Dendritic cell subpopulations in nasopharyngeal cancer. Oncol. Lett. 2019, 17, 2557–2561. [Google Scholar] [CrossRef] [PubMed]
- Sabado, R.L.; Balan, S.; Bhardwaj, N. Dendritic cell-based immunotherapy. Cell Res. 2017, 27, 74–95. [Google Scholar] [CrossRef] [PubMed]
- Sulistya, A.B.; Haifa, R.; Facicilia, G.; Marbun, K.T.; Kirana, M.N.; Dewi, Y.A.; Sartika, C.R.; Wijaya, A.; Dandan, K.L. Dendritic Cell as Potential Immunotherapy for Nasopharyngeal Cancer: A Review. Indones. Biomed. J. 2023, 15, 269–277. [Google Scholar] [CrossRef]
- Su, Z.Y.; Siak, P.Y.; Leong, C.O.; Cheah, S.C. Nasopharyngeal Carcinoma and Its Microenvironment: Past, Current, and Future Perspectives. Front. Oncol. 2022, 12, 840467. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Ying, H. Revealing the crosstalk between nasopharyngeal carcinoma and immune cells in the tumor microenvironment. J. Exp. Clin. Cancer Res. 2022, 41, 244. [Google Scholar] [CrossRef]
- Jin, S.; Li, R.; Chen, M.-Y.; Yu, C.; Tang, L.-Q.; Liu, Y.-M.; Li, J.-P.; Liu, Y.-N.; Luo, Y.-L.; Zhao, Y.; et al. Single-cell transcriptomic analysis defines the interplay between tumor cells, viral infection, and the microenvironment in nasopharyngeal carcinoma. Cell Res. 2020, 30, 950–965. [Google Scholar] [CrossRef] [PubMed]
- Bruce, J.P.; To, K.-F.; Lui, V.W.Y.; Chung, G.T.Y.; Chan, Y.-Y.; Tsang, C.M.; Yip, K.Y.; Ma, B.B.Y.; Woo, J.K.S.; Hui, E.P.; et al. Whole-genome profiling of nasopharyngeal carcinoma reveals viral-host co-operation in inflammatory NF-κB activation and immune escape. Nat. Commun. 2021, 12, 4193. [Google Scholar] [CrossRef] [PubMed]
- Lo, A.K.; Dawson, C.W.; Lung, H.L.; Wong, K.L.; Young, L.S. The role of EBV-encoded LMP1 in the NPC tumor microenvironment: From function to therapy. Front. Oncol. 2021, 11, 640207. [Google Scholar] [CrossRef]
- Ooft, M.L.; van Ipenburg, J.A.; Sanders, M.E.; Kranendonk, M.; Hofland, I.; de Bree, R.; Koljenović, S.; Willems, S.M. Prognostic role of tumour-associated macrophages and regulatory T cells in EBV-positive and EBV-negative nasopharyngeal carcinoma. J. Clin. Pathol. 2018, 71, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Guo, C.; Xiong, F.; Yu, J.; Ge, J.; Wang, H.; Liao, Q.; Zhou, Y.; Gong, Q.; Xiang, B.; et al. Single cell RNA-seq reveals the landscape of tumor and infiltrating immune cells in nasopharyngeal carcinoma. Cancer Lett. 2020, 477, 131–143. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antibody | Substrate | Clone | Dilution |
|---|---|---|---|
| CK AE1/AE3 1 | Mouse, Monoclonal | AE1/AE3 | 1:100 |
| CK5 2 | Mouse, Monoclonal | XM26 | 1:100 |
| p63 | Mouse, Monoclonal | 7JUL | 1:25 |
| CK7 3 | Mouse, Monoclonal | 307M-94 | 1:100 |
| CK20 4 | Mouse, Monoclonal | L26 | 1:150 |
| 34βE12 5 | Mouse, Monoclonal | 34βE12 | RTU 6 |
| EMA 7 | Mouse, Monoclonal | GP1.4 | 1:300 |
| p53 | Mouse, Monoclonal | DO-7 | 1:800 |
| p16 | Mouse, Monoclonal | CS1 | 1:150 |
| EBV 8 | Mouse, Monoclonal | CS1-4 | RTU 6 |
| LCA 9 | Mouse, Monoclonal | X16/99 | 1:40 |
| CD20 10 | Mouse, Monoclonal | L26 | 1:250 |
| CD4 11 | Mouse, Monoclonal | 4B12 | 1:100 |
| CD8 12 | Mouse, Monoclonal | 4B11 | 1:50 |
| CD68 13 | Mouse, Monoclonal | 514H12 | 1:100 |
| CD1a 14 | Mouse, Monoclonal | MTB1 | RTU 6 |
| CD117 15 | Mouse, Monoclonal | T595 | 1:20 |
| Symptoms Due to the Presence of Nasopharynx Mass | Eustachian Tube Dysfunction | Skull Base and Cranial Nerves Involvement |
|---|---|---|
| Left nasal obstruction, oral respiration | Left mixed hearing loss | No |
| Bilateral nasal obstruction, oral respiration, hyposmia, snoring | Sensorineural bilateral hearing loss | Headache |
| Left nasal obstruction | Left conductive hearing loss, tinnitus | No |
| Left nasal obstruction, epistaxis | Left sensorineural hearing loss | No |
| No | No | No |
| Left nasal obstruction | Left sensorineural hearing loss | No |
| Left nasal obstruction | No | No |
| No | Right conductive hearing loss | No |
| Bilateral nasal obstruction | No | No |
| No | No | No |
| Bilateral nasal obstruction, oral respiration | No | Headache |
| Bilateral nasal obstruction | Left sensorineural hearing loss | Headache, diplopia |
| No | No | No |
| No | No | No |
| Bilateral nasal obstruction, oral respiration | Serous otitis media | No |
| Left nasal obstruction | Left mixed hearing loss | Headache |
| Right epistaxis | No | No |
| Bilateral nasal obstruction, snoring, dysphonia, cough | No | No |
| Right epistaxis | No | No |
| Left nasal obstruction, oral respiration | left conductive hearing loss, tinnitus | Headache |
| No | No | Headache |
| Bilateral nasal obstruction | Right conductive hearing loss | No |
| Left nasal obstruction, mucopurulent nasal discharge | No | Headache |
| Bilateral nasal obstruction, epistaxis | No | No |
| Bilateral nasal obstruction | Right conductive hearing loss | No |
| Bilateral nasal obstruction | No | Numbness, paresthesia |
| No | Left otalgia | No |
| Bilateral nasal obstruction, epistaxis | No | No |
| Left nasal obstruction, oral respiration | No | No |
| Bilateral nasal obstruction, oral respiration | No | No |
| No | No | No |
| Bilateral nasal obstruction, oral respiration, dysphonia | No | Nerve II paresis, deviation of the right eyeball |
| Left nasal obstruction, oral respiration | No | Headache |
| No | No | No |
| Bilateral nasal obstruction, oral respiration | Right otalgia, bilateral conductive hearing loss | No |
| Bilateral nasal obstruction, epistaxis | No | Headache |
| Antibody | Reaction Intensity | Malignant Squamous Component | Inflammatory Cellular Component | Cases/Rate of Positive Cases | Observations |
|---|---|---|---|---|---|
| AE1/AE3 | +++ 1 | 100% | N/A 5 | 26/100% | Diffuse reaction |
| CK5 | +++ | 100% | N/A | 26/100% | Diffuse reaction |
| p63 | +++ | 80–100% | N/A | 26/100% | Diffuse reaction |
| 34βE12 | ++ 2/+++ | 80–100% | N/A | 25/96% | Diffuse reaction |
| EMA | ++ | 10–80% | N/A | 24/92% | Focal reaction |
| CK7 | − 3 | 0% | N/A | 0/0% | Positive intern control present |
| CK20 | − | 0% | N/A | 0/0% | |
| p53 | ++/+++ | 80–100% | N/A | 26/100% | Diffuse reaction |
| EBV | ++/+++ | 80–100% | 15% | 2/8% | Diffuse reaction |
| p16 | +++ | 100% | N/A | 1/4% | Nuclear and cytoplasmic, intense, and diffuse reaction |
| CD117 | + 4/++ | 60–80% | 0% | 10/38% | Heterogeneous reaction, in malignant component, positive internal control present on mast cells |
| CD117 | +++ | 0% | 1–15% | 20/80% | |
| LCA | +++ | N/A | 60–90% | 26/100% | Peri- and intratumor |
| CD20 | ++/+++ | N/A | 70–85% | 26/100% | Peri- and intratumor |
| CD4 | ++/+++ | N/A | 10–20% of lymphocytes | 26/100% | Predominantly peritumoral |
| CD8 | ++/+++ | N/A | 5–10% of lymphocytes | 26/100% | Predominantly peritumoral, CD4:CD8=1:1 in 75% of cases and 2:1 in 25% of cases |
| CD68 | ++ | N/A | 6–15% | 23/88% | Macrophage and dendritic cells |
| CD1a | ++ | N/A | 5–15% | 23/88% | Predominantly intratumor dendritic cells, also CD68-positive |
| Antibody | Reaction Intensity | Malignant Squamous Component | Inflammatory Cellular Component | Cases/Rate of Positive Cases | Observations |
|---|---|---|---|---|---|
| CK AE1/AE3 | +++ 1 | 100% | N/A 2 | 10/100% | Diffuse reaction |
| CK5 | +++ | 100% | N/A | 10/100% | Diffuse reaction |
| p63 | +++ | 90–100% | N/A | 10/100% | Diffuse reaction |
| 34βE12 | + 3/++ 4 | 20–90% | N/A | 10/100% | Focal/diffuse reaction |
| EMA | +/++ | 10–70% | N/A | 10/100% | Focal/diffuse reaction |
| CK7 | − 5 | 0% | N/A | 0/0% | Positive intern control present |
| CK20 | − | 0% | N/A | 0/0% | |
| p53 | +/++ | 30–100% | N/A | 10/100% | Focal/diffuse reaction |
| EBV | − | 0% | N/A | 0/0% | |
| p16 | +++ | 90% | N/A | 1/10% | Nuclear and cytoplasmic, intense and diffuse reaction |
| CD117 | − | 0% | 0% | 0/0% | Negative reaction in malignant component, positive internal control present on mast cells |
| CD117 | +++ | 0% | 1–10% | 10/100% | Positive reaction on mast cells |
| LCA | +++ | N/A | 80–85% | 10/100% | Peritumoral |
| CD20 | ++/+++ | N/A | 70–85% | 26/100% | Peritumoral |
| CD4 | ++ | N/A | 10–20% of lymphocytes | 10/100% | Peritumoral |
| CD8 | ++/+++ | N/A | 1–10% of lymphocytes | 10/100% | CD4:CD8=1:1 in 90% of cases and 2:1 in 10% of cases |
| CD68 | ++ | N/A | 5–15% | 10/100% | Dendritic cells, rare macrophages |
| CD1a | +++ | N/A | 5–15% | 10/100% | CD68-positive dendritic cells |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marin, M.A.; Closca, R.-M.; Marin, A.; Rakitovan, M.; Nicoara, A.; Poenaru, M.; Militaru, M.; Baderca, F. Clinical, Epidemiological, Morphological, and Immunohistochemical Aspects of Nasopharyngeal Carcinoma—4-Year Retrospective Study in the Western Part of Romania. Diagnostics 2024, 14, 722. https://doi.org/10.3390/diagnostics14070722
Marin MA, Closca R-M, Marin A, Rakitovan M, Nicoara A, Poenaru M, Militaru M, Baderca F. Clinical, Epidemiological, Morphological, and Immunohistochemical Aspects of Nasopharyngeal Carcinoma—4-Year Retrospective Study in the Western Part of Romania. Diagnostics. 2024; 14(7):722. https://doi.org/10.3390/diagnostics14070722
Chicago/Turabian StyleMarin, Maria Alina, Raluca-Maria Closca, Aurel Marin, Marina Rakitovan, Adrian Nicoara, Marioara Poenaru, Marius Militaru, and Flavia Baderca. 2024. "Clinical, Epidemiological, Morphological, and Immunohistochemical Aspects of Nasopharyngeal Carcinoma—4-Year Retrospective Study in the Western Part of Romania" Diagnostics 14, no. 7: 722. https://doi.org/10.3390/diagnostics14070722