
Reduced Retinal Blood Vessel Densities Measured by Optical Coherence Tomography Angiography in Keratoconus Patients Are Negatively Correlated with Keratoconus Severity
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Optical Coherence Tomography Angiography
2.2. Scheimpflug Corneal Topography
2.3. Statistics
3. Results
3.1. Demographic Data and Ocular Data
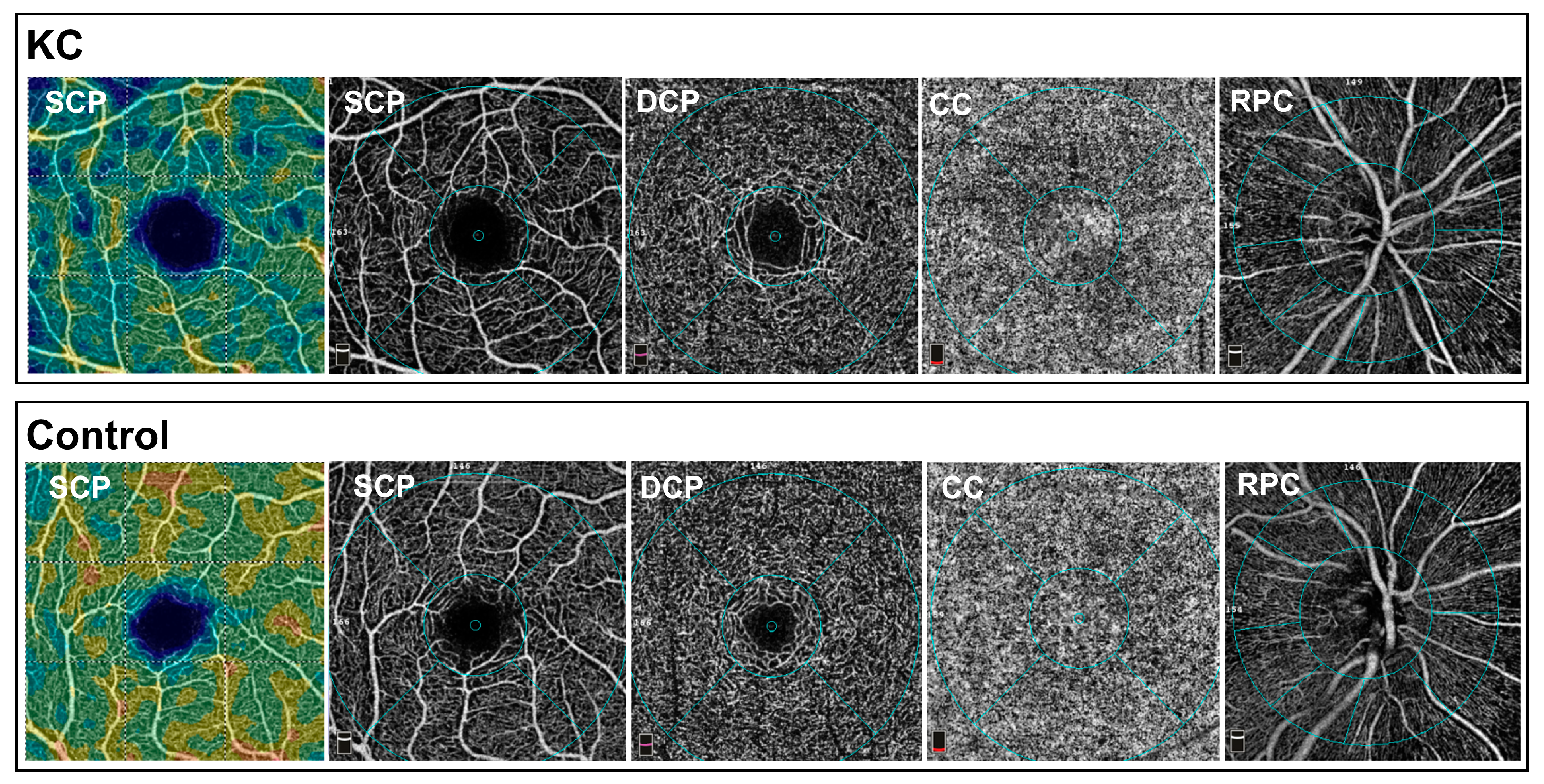
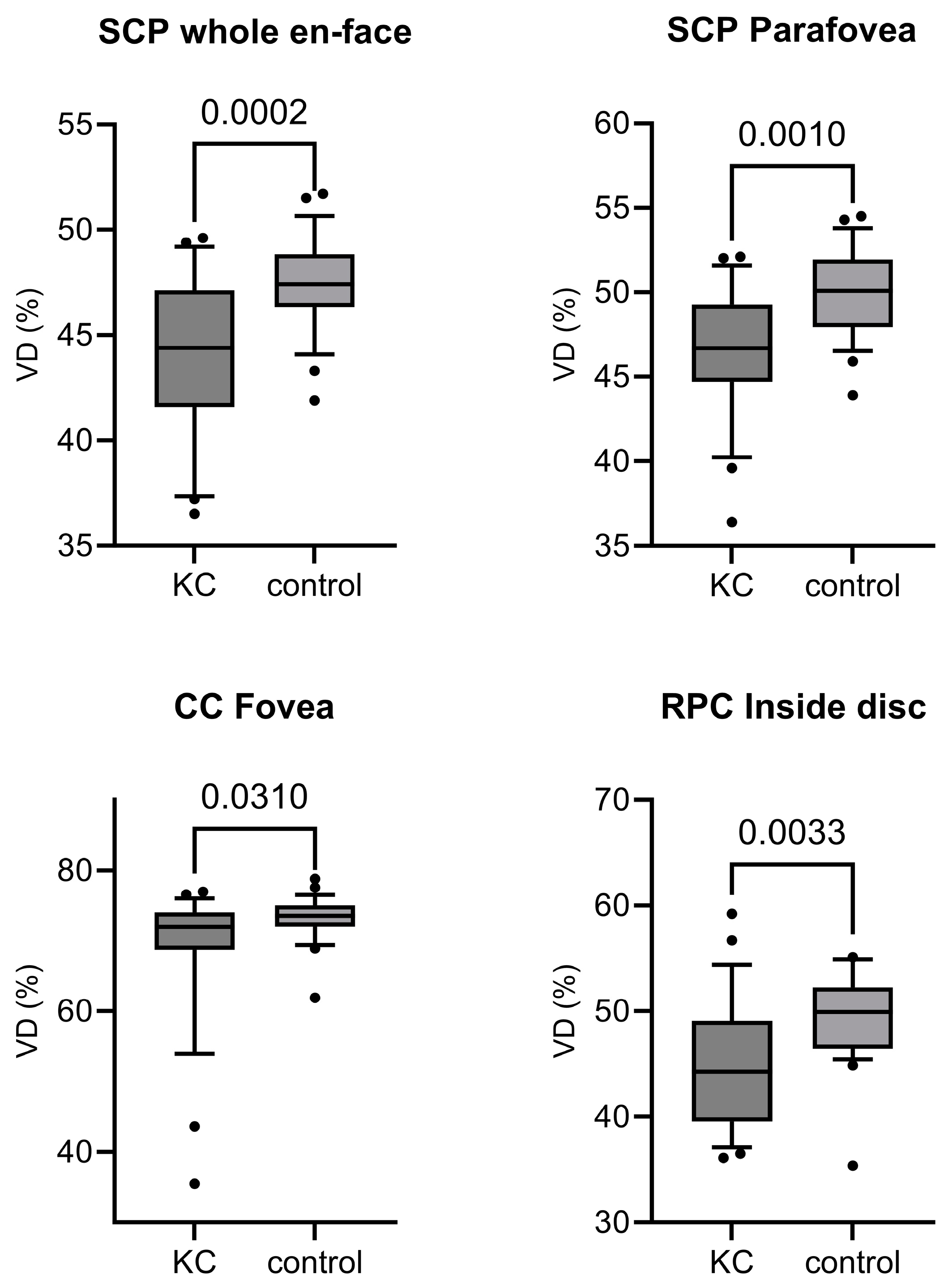
3.2. Optical Coherence Tomography Angiography Data
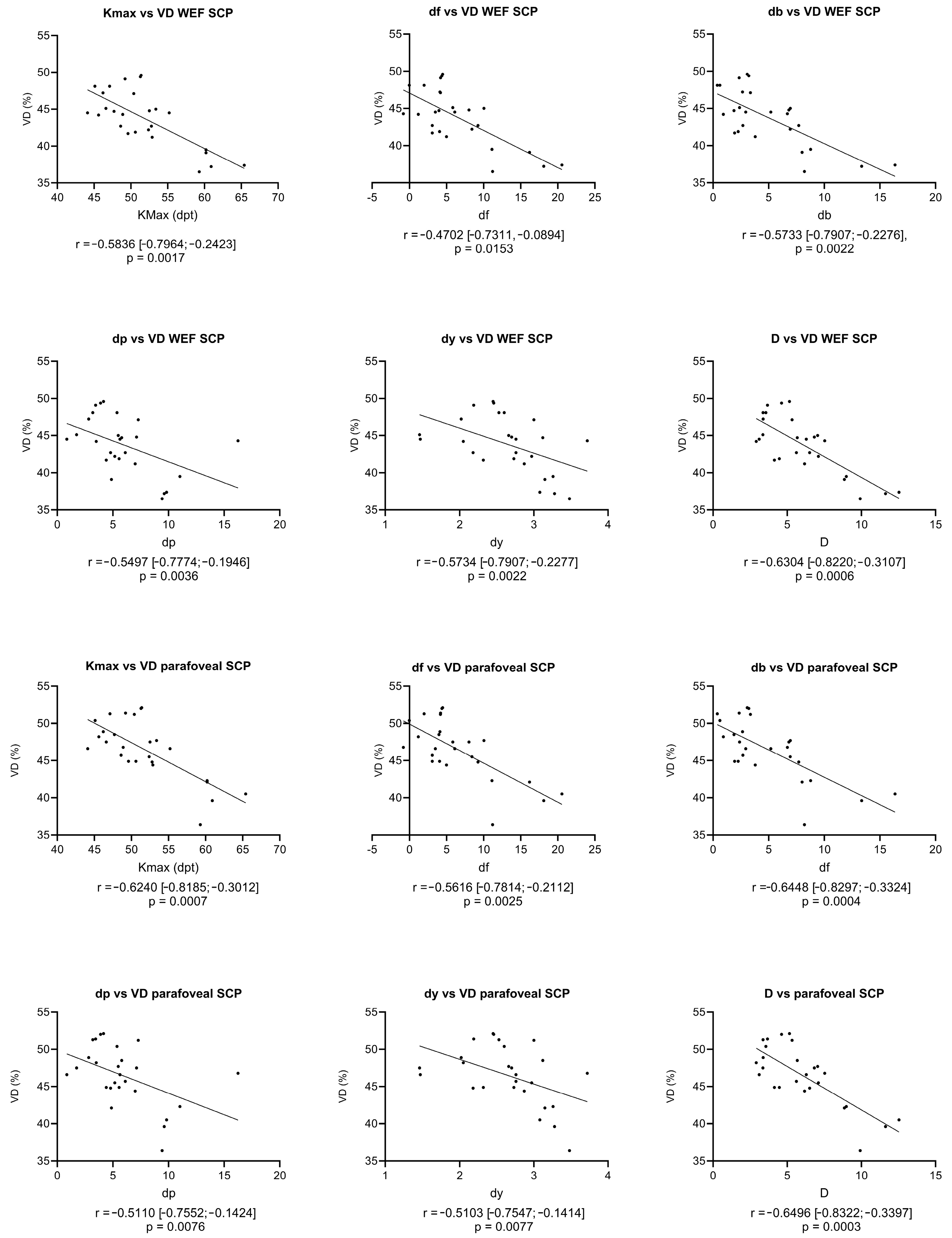
3.3. Correlation Analysis
3.4. Summary of the Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Deshmukh, R.; Ong, Z.Z.; Rampat, R.; Alió del Barrio, J.L.; Barua, A.; Ang, M.; Mehta, J.S.; Said, D.G.; Dua, H.S.; Ambrósio, R.; et al. Management of Keratoconus: An Updated Review. Front. Med. 2023, 10, 1212314. [Google Scholar] [CrossRef] [PubMed]
- Godefrooij, D.A.; de Wit, G.A.; Uiterwaal, C.S.; Imhof, S.M.; Wisse, R.P.L. Age-Specific Incidence and Prevalence of Keratoconus: A Nationwide Registration Study. Am. J. Ophthalmol. 2017, 175, 169–172. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, G.; Rama, P. The Keratoconus Enigma: A Review with Emphasis on Pathogenesis. Ocul. Surf. 2020, 18, 363–373. [Google Scholar] [CrossRef] [PubMed]
- Davidson, A.E.; Hayes, S.; Hardcastle, A.J.; Tuft, S.J. The Pathogenesis of Keratoconus. Eye 2014, 28, 189–195. [Google Scholar] [CrossRef]
- Panahi, Y.; Azimi, A.; Naderi, M.; Jadidi, K.; Sahebkar, A. An Analytical Enrichment-Based Review of Structural Genetic Studies on Keratoconus. J. Cell. Biochem. 2019, 120, 4748–4756. [Google Scholar] [CrossRef] [PubMed]
- Shetty, R.; Sathyanarayanamoorthy, A.; Ramachandra, R.A.; Arora, V.; Ghosh, A.; Srivatsa, P.R.; Pahuja, N.; Nuijts, R.M.M.A.; Sinha-Roy, A.; Mohan, R.R.; et al. Attenuation of Lysyl Oxidase and Collagen Gene Expression in Keratoconus Patient Corneal Epithelium Corresponds to Disease Severity. Mol. Vis. 2015, 21, 12–25. [Google Scholar]
- Unni, P.; Lee, H.J. Systemic Associations with Keratoconus. Life 2023, 13, 1363. [Google Scholar] [CrossRef] [PubMed]
- McMahon, T.T.; Szczotka-Flynn, L.; Barr, J.T.; Anderson, R.J.; Slaughter, M.E.; Lass, J.H.; Iyengar, S.K.; CLEK Study Group. A New Method for Grading the Severity of Keratoconus: The Keratoconus Severity Score (KSS). Cornea 2006, 25, 794. [Google Scholar] [CrossRef] [PubMed]
- Alió, J.L.; Shabayek, M.H. Corneal Higher Order Aberrations: A Method to Grade Keratoconus. J. Refract. Surg. 2006, 22, 539–545. [Google Scholar] [CrossRef]
- Belin, M.W.; Ambrósio, R. Scheimpflug Imaging for Keratoconus and Ectatic Disease. Indian J. Ophthalmol. 2013, 61, 401–406. [Google Scholar] [CrossRef]
- Motlagh, M.N.; Moshirfar, M.; Murri, M.S.; Skanchy, D.F.; Momeni-Moghaddam, H.; Ronquillo, Y.C.; Hoopes, P.C. Pentacam® Corneal Tomography for Screening of Refractive Surgery Candidates: A Review of the Literature, Part I. Med. Hypothesis Discov. Innov. Ophthalmol. 2019, 8, 177–203. [Google Scholar] [PubMed]
- Bae, G.H.; Kim, J.R.; Kim, C.H.; Lim, D.H.; Chung, E.S.; Chung, T.-Y. Corneal Topographic and Tomographic Analysis of Fellow Eyes in Unilateral Keratoconus Patients Using Pentacam. Am. J. Ophthalmol. 2014, 157, 103–109.e1. [Google Scholar] [CrossRef] [PubMed]
- Aghazadeh Amiri, M.; Hashemi, H.; Ramin, S.; Yekta, A.; Taheri, A.; Nabovati, P.; Khabazkhoob, M. Corneal Thickness Measurements with Scheimpflug and Slit Scanning Imaging Techniques in Keratoconus. J. Curr. Ophthalmol. 2017, 29, 23–27. [Google Scholar] [CrossRef]
- Song, Y.; Feng, Y.; Qu, M.; Ma, Q.; Tian, H.; Li, D.; He, R. Analysis of the Diagnostic Accuracy of Belin/Ambrósio Enhanced Ectasia and Corvis ST Parameters for Subclinical Keratoconus. Int. Ophthalmol. 2023, 43, 1465–1475. [Google Scholar] [CrossRef] [PubMed]
- Hashemi, H.; Beiranvand, A.; Yekta, A.; Maleki, A.; Yazdani, N.; Khabazkhoob, M. Pentacam Top Indices for Diagnosing Subclinical and Definite Keratoconus. J. Curr. Ophthalmol. 2016, 28, 21–26. [Google Scholar] [CrossRef]
- Bamdad, S.; Sedaghat, M.R.; Yasemi, M.; Vahedi, A. Sensitivity and Specificity of Belin Ambrosio Enhanced Ectasia Display in Early Diagnosis of Keratoconus. J. Ophthalmol. 2020, 2020, 7625659. [Google Scholar] [CrossRef]
- Santodomingo-Rubido, J.; Carracedo, G.; Suzaki, A.; Villa-Collar, C.; Vincent, S.J.; Wolffsohn, J.S. Keratoconus: An Updated Review. Contact Lens Anterior Eye 2022, 45, 101559. [Google Scholar] [CrossRef]
- Shi, Y. Strategies for Improving the Early Diagnosis of Keratoconus. Clin Optom 2016, 8, 13–21. [Google Scholar] [CrossRef]
- Cao, K.; Verspoor, K.; Sahebjada, S.; Baird, P.N. Evaluating the Performance of Various Machine Learning Algorithms to Detect Subclinical Keratoconus. Transl. Vis. Sci. Technol. 2020, 9, 24. [Google Scholar] [CrossRef]
- Venkateswaran, N.; Galor, A.; Wang, J.; Karp, C.L. Optical Coherence Tomography for Ocular Surface and Corneal Diseases: A Review. Eye Vis. 2018, 5, 13. [Google Scholar] [CrossRef]
- Lahme, L.; Storp, J.J.; Diener, R.; Eter, N.; Hansen, U.; Leclaire, M.D.; Alnawaiseh, M. Corneal Epithelial Thickness in Keratoconus Patients Compared to Healthy Controls. Ophthalmologie 2022, 119, 952–957. [Google Scholar] [CrossRef]
- Reinstein, D.Z.; Archer, T.J.; Gobbe, M. Corneal Epithelial Thickness Profile in the Diagnosis of Keratoconus. J. Refract. Surg. 2009, 25, 604–610. [Google Scholar] [CrossRef] [PubMed]
- Spaide, R.F.; Fujimoto, J.G.; Waheed, N.K.; Sadda, S.R.; Staurenghi, G. Optical Coherence Tomography Angiography. Prog. Retin. Eye Res. 2018, 64, 1–55. [Google Scholar] [CrossRef]
- Lauermann, J.L.; Eter, N.; Alten, F. Optical Coherence Tomography Angiography Offers New Insights into Choriocapillaris Perfusion. Ophthalmologica 2018, 239, 74–84. [Google Scholar] [CrossRef]
- de Carlo, T.E.; Romano, A.; Waheed, N.K.; Duker, J.S. A Review of Optical Coherence Tomography Angiography (OCTA). Int. J. Retin. Vitr. 2015, 1, 5. [Google Scholar] [CrossRef]
- Kashani, A.H.; Chen, C.-L.; Gahm, J.K.; Zheng, F.; Richter, G.M.; Rosenfeld, P.J.; Shi, Y.; Wang, R.K. Optical Coherence Tomography Angiography: A Comprehensive Review of Current Methods and Clinical Applications. Prog. Retin. Eye Res. 2017, 60, 66–100. [Google Scholar] [CrossRef]
- Jia, Y.; Bailey, S.T.; Hwang, T.S.; McClintic, S.M.; Gao, S.S.; Pennesi, M.E.; Flaxel, C.J.; Lauer, A.K.; Wilson, D.J.; Hornegger, J.; et al. Quantitative Optical Coherence Tomography Angiography of Vascular Abnormalities in the Living Human Eye. Proc. Natl. Acad. Sci. USA 2015, 112, E2395–E2402. [Google Scholar] [CrossRef] [PubMed]
- Mendis, K.R.; Balaratnasingam, C.; Yu, P.; Barry, C.J.; McAllister, I.L.; Cringle, S.J.; Yu, D.-Y. Correlation of Histologic and Clinical Images to Determine the Diagnostic Value of Fluorescein Angiography for Studying Retinal Capillary Detail. Investig. Ophthalmol. Vis. Sci. 2010, 51, 5864–5869. [Google Scholar] [CrossRef] [PubMed]
- Spaide, R.F.; Klancnik, J.M.; Cooney, M.J. Retinal Vascular Layers Imaged by Fluorescein Angiography and Optical Coherence Tomography Angiography. JAMA Ophthalmol. 2015, 133, 45–50. [Google Scholar] [CrossRef]
- Leclaire, M.D.; Clemens, C.R.; Eter, N.; Mihailovic, N. Choroidal neovascularization due to a punctate inner choroidopathy visualized by optical coherence tomography angiography. Ophthalmologe 2021, 118, 842–846. [Google Scholar] [CrossRef]
- Fukushima, A.; Maruko, I.; Chujo, K.; Hasegawa, T.; Arakawa, H.; Iida, T. Characteristics of Treatment-Naïve Quiescent Choroidal Neovascularization Detected by Optical Coherence Tomography Angiography in Patients with Age-Related Macular Degeneration. Graefe’s Arch. Clin. Exp. Ophthalmol. 2021, 259, 2671–2677. [Google Scholar] [CrossRef] [PubMed]
- Inoue, M.; Jung, J.J.; Balaratnasingam, C.; Dansingani, K.K.; Dhrami-Gavazi, E.; Suzuki, M.; de Carlo, T.E.; Shahlaee, A.; Klufas, M.A.; El Maftouhi, A.; et al. A Comparison Between Optical Coherence Tomography Angiography and Fluorescein Angiography for the Imaging of Type 1 Neovascularization. Investig. Ophthalmol. Vis. Sci. 2016, 57, OCT314–OCT323. [Google Scholar] [CrossRef] [PubMed]
- Mihailovic, N.; Eter, N.; Alnawaiseh, M. Foveale avaskuläre Zone und OCT-Angiographie. Eine Übersicht aktueller Erkenntnisse. Ophthalmologe 2019, 116, 610–616. [Google Scholar] [CrossRef] [PubMed]
- Brücher, V.C.; Storp, J.J.; Eter, N.; Alnawaiseh, M. Optical Coherence Tomography Angiography-Derived Flow Density: A Review of the Influencing Factors. Graefe’s Arch. Clin. Exp. Ophthalmol. 2020, 258, 701–710. [Google Scholar] [CrossRef]
- Diener, R.; Leclaire, M.D.; Eckardt, F.; Lauermann, J.L.; Alnawaiseh, M.; Eter, N.; Treder, M. Cilioretinal Arteries Influence Optic Nerve Head, Peripapillary, and Macular Vessel Densities In Healthy Eyes: An Optical Coherence Tomography Angiography Study. Retina 2021, 41, 2399–2406. [Google Scholar] [CrossRef] [PubMed]
- Leclaire, M.D.; Eter, N.; Alnawaiseh, M. Die optische Kohärenztomographie-Angiographie und Erkrankungen des kardiovaskulären Spektrums. Ein Überblick über die aktuelle Studienlage. Ophthalmologe 2021, 118, 1119–1127. [Google Scholar] [CrossRef]
- Sampson, D.M.; Gong, P.; An, D.; Menghini, M.; Hansen, A.; Mackey, D.A.; Sampson, D.D.; Chen, F.K. Axial Length Variation Impacts on Superficial Retinal Vessel Density and Foveal Avascular Zone Area Measurements Using Optical Coherence Tomography Angiography. Investig. Ophthalmol. Vis. Sci. 2017, 58, 3065–3072. [Google Scholar] [CrossRef] [PubMed]
- Alshehri, O.; Abdelaal, A.M.; Abudawood, G.; Khan, M.A.; Alsharif, S.; Hijazi, H.; AlQassimi, A. Normative Values for Corneal Tomography and Comparison of Both Eyes in Young Saudi Males with 20/20 Vision Using Pentacam-HR Scheimpflug Imaging. Clin. Ophthalmol. 2022, 16, 2631–2637. [Google Scholar] [CrossRef] [PubMed]
- Viswanathan, D.; Kumar, N.L.; Males, J.J.; Graham, S.L. Comparative Analysis of Corneal Measurements Obtained from a Scheimpflug Camera and an Integrated Placido-Optical Coherence Tomography Device in Normal and Keratoconic Eyes. Acta Ophthalmol. 2015, 93, e488–e494. [Google Scholar] [CrossRef]
- Finis, D.; Ralla, B.; Karbe, M.; Borrelli, M.; Schrader, S.; Geerling, G. Comparison of Two Different Scheimpflug Devices in the Detection of Keratoconus, Regular Astigmatism, and Healthy Corneas. J. Ophthalmol. 2015, 2015, e315281. [Google Scholar] [CrossRef]
- Chua, J.; Sim, R.; Tan, B.; Wong, D.; Yao, X.; Liu, X.; Ting, D.S.W.; Schmidl, D.; Ang, M.; Garhöfer, G.; et al. Optical Coherence Tomography Angiography in Diabetes and Diabetic Retinopathy. J. Clin. Med. 2020, 9, 1723. [Google Scholar] [CrossRef] [PubMed]
- Mihailovic, N.; Leclaire, M.D.; Eter, N.; Brücher, V.C. Altered Microvascular Density in Patients with Systemic Lupus Erythematosus Treated with Hydroxychloroquine—An Optical Coherence Tomography Angiography Study. Graefe’s Arch. Clin. Exp. Ophthalmol. 2020, 258, 2263–2269. [Google Scholar] [CrossRef] [PubMed]
- Esser, E.L.; Zimmermann, J.A.; Storp, J.J.; Eter, N.; Mihailovic, N. Retinal Microvascular Density Analysis in Patients with Rheumatoid Arthritis Treated with Hydroxychloroquine. Graefe’s Arch. Clin. Exp. Ophthalmol. 2023, 261, 1433–1442. [Google Scholar] [CrossRef] [PubMed]
- Hormel, T.T.; Hwang, T.S.; Bailey, S.T.; Wilson, D.J.; Huang, D.; Jia, Y. Artificial Intelligence in OCT Angiography. Progress. Retin. Eye Res. 2021, 85, 100965. [Google Scholar] [CrossRef]
- Spaide, R.F.; Fujimoto, J.G.; Waheed, N.K. Image Artifacts In Optical Coherence Tomography Angiography. Retina 2015, 35, 2163–2180. [Google Scholar] [CrossRef] [PubMed]
- Enders, C.; Lang, G.E.; Dreyhaupt, J.; Loidl, M.; Lang, G.K.; Werner, J.U. Quantity and Quality of Image Artifacts in Optical Coherence Tomography Angiography. PLoS ONE 2019, 14, e0210505. [Google Scholar] [CrossRef]
- Al-Sheikh, M.; Ghasemi Falavarjani, K.; Akil, H.; Sadda, S.R. Impact of Image Quality on OCT Angiography Based Quantitative Measurements. Int. J. Retin. Vitr. 2017, 3, 13. [Google Scholar] [CrossRef] [PubMed]
- Storp, J.J.; Leclaire, M.D.; Zimmermann, J.A.; Englmaier, V.A.; Albert, F.; Eter, N.; Al-Nawaiseh, S. Further Evidence Against Bilateral Manifestation of Coats Disease In Optical Coherence Tomography Angiography of The Macula. Retina 2023, 43, 1525–1533. [Google Scholar] [CrossRef]
- Tomlinson, A.; Hasan, B.; Lujan, B.J. Importance of Focus in OCT Angiography. Ophthalmol. Retin. 2018, 2, 748–749. [Google Scholar] [CrossRef]
- Jung, J.J.; Soh, Y.Q.; Sha, P.; Yu, S.; Durbin, M.K.; Hoang, Q.V. Effects of Induced Astigmatism on Spectral Domain-OCT Angiography Quantitative Metrics. Am. J. Ophthalmol. 2020, 219, 49–58. [Google Scholar] [CrossRef]
- VIDAL OLIVER, L.; Gallego Pinazo, R.; Dolz-Marco, R. Astigmatism Effect and Its Correction on Quantitative Metrics Using Optical Coherence Tomography Angiography. Investig. Ophthalmol. Vis. Sci. 2022, 63, 2941–F0094. [Google Scholar]
- Vidal-Oliver, L.; Gallego-Pinazo, R.; Dolz-Marco, R. Astigmatism Influences Quantitative and Qualitative Analysis in Optical Coherence Tomography Angiography Imaging. Transl. Vis. Sci. Technol. 2024, 13, 10. [Google Scholar] [CrossRef] [PubMed]
- Wylęgała, A.; Szkodny, D.; Fiolka, R.; Wylęgała, E. Assessment of the Retinal Vessels in Keratoconus: An OCT Angiography Study. J. Clin. Med. 2022, 11, 2960. [Google Scholar] [CrossRef] [PubMed]
- Dogan, B.; Bozdogan, Y.C.; Gedik, B.; Erol, M.K.; Bulut, M.; Duman, F. Optic Disc and Retinal Vessel Densities Assessment by Optical Coherence Tomography Angiography in Patients with Keratoconus. Photodiagnosis Photodyn. Ther. 2023, 41, 103218. [Google Scholar] [CrossRef] [PubMed]
- Hsu, R.-H.; Chien, Y.-H.; Hwu, W.-L.; Lee, N.-C. Diversity in Heritable Disorders of Connective Tissue at a Single Center. Connect. Tissue Res. 2021, 62, 580–585. [Google Scholar] [CrossRef] [PubMed]
- Hirata, K.; Triposkiadis, F.; Sparks, E.; Bowen, J.; Wooley, C.F.; Boudoulas, H. The Marfan Syndrome: Abnormal Aortic Elastic Properties. J. Am. Coll. Cardiol. 1991, 18, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.J.; Schubart, J.R.; Sheehan, T.; Bascom, R.; Francomano, C.A. Arterial Elasticity in Ehlers-Danlos Syndromes. Genes 2020, 11, 55. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.S.; Follis, F.M.; Shively, B.K.; Wernly, J.A. Osteogenesis Imperfecta and Cardiovascular Diseases. Ann. Thorac. Surg. 1995, 60, 1439–1443. [Google Scholar] [CrossRef]
- Callewaert, B.; Malfait, F.; Loeys, B.; De Paepe, A. Ehlers-Danlos Syndromes and Marfan Syndrome. Best. Pract. Res. Clin. Rheumatol. 2008, 22, 165–189. [Google Scholar] [CrossRef]
- Malfait, F.; Coucke, P.; Symoens, S.; Loeys, B.; Nuytinck, L.; De Paepe, A. The Molecular Basis of Classic Ehlers-Danlos Syndrome: A Comprehensive Study of Biochemical and Molecular Findings in 48 Unrelated Patients. Hum. Mutat. 2005, 25, 28–37. [Google Scholar] [CrossRef]
- Robertson, I. Keratoconus and the Ehlers-Danlos Syndrome: A New Aspect of Keratoconus. Med. J. Aust. 1975, 1, 571–573. [Google Scholar] [CrossRef]
- Woodward, E.G.; Morris, M.T. Joint Hypermobility in Keratoconus. Ophthalmic Physiol. Opt. 1990, 10, 360–362. [Google Scholar] [CrossRef] [PubMed]
- Esfandiari, H.; Ansari, S.; Mohammad-Rabei, H.; Mets, M.B. Management Strategies of Ocular Abnormalities in Patients with Marfan Syndrome: Current Perspective. J. Ophthalmic Vis. Res. 2019, 14, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Marini, J.C.; Forlino, A.; Bächinger, H.P.; Bishop, N.J.; Byers, P.H.; Paepe, A.D.; Fassier, F.; Fratzl-Zelman, N.; Kozloff, K.M.; Krakow, D.; et al. Osteogenesis imperfecta. Nat. Rev. Dis. Primers 2017, 3, 17052. [Google Scholar] [CrossRef] [PubMed]
- Zeri, F.; Swann, P.G.; Naroo, S. Osteogenesis imperfecta and Keratoconus in an Italian Family. Clin. Exp. Optom. 2018, 101, 400–403. [Google Scholar] [CrossRef] [PubMed]
- Chou, C.-C.; Shih, P.-J.; Jou, T.-S.; Hsu, M.-Y.; Chen, J.-P.; Hsu, R.-H.; Lee, N.-C.; Chien, Y.-H.; Hwu, W.-L.; Wang, I.-J. Corneal Biomechanical Characteristics in Osteogenesis Imperfecta With Collagen Defect. Transl. Vis. Sci. Technol. 2023, 12, 14. [Google Scholar] [CrossRef] [PubMed]
- Evereklioglu, C.; Madenci, E.; Bayazit, Y.A.; Yilmaz, K.; Balat, A.; Bekir, N.A. Central Corneal Thickness is Lower in Osteogenesis Imperfecta and Negatively Correlates with the Presence of Blue Sclera. Ophthalmic Physiol. Opt. 2002, 22, 511–515. [Google Scholar] [CrossRef] [PubMed]
- Robati, R.M.; Einollahi, B.; Einollahi, H.; Younespour, S.; Fadaifard, S. Skin Biophysical Characteristics in Patients with Keratoconus: A Controlled Study. Scientifica 2016, 2016, 6789081. [Google Scholar] [CrossRef] [PubMed]
- Rezar-Dreindl, S.; Eibenberger, K.; Told, R.; Unterluggauer, V.; Sacu, S.; Schmidt-Erfurth, U.; Stifter, E. Microvascular Retinal Changes in Patients with Marfan Syndrome. Curr. Eye Res. 2022, 47, 1186–1192. [Google Scholar] [CrossRef]
- Chen, H.; Ng, K.Y.; Li, S.; Jin, G.; Cao, Q.; Lian, Z.; Luo, X.; Ding, X.; Zheng, D. Characteristics of The Foveal Microvasculature In Children with Marfan Syndrome. Retina 2022, 42, 138–151. [Google Scholar] [CrossRef]
- Shetty, R.; Ghosh, A.; Lim, R.R.; Subramani, M.; Mihir, K.; Ranganath, A.; Nagaraj, S.; Nuijts, R.M.M.A.; Beuerman, R.; Shetty, R.; et al. Elevated Expression of Matrix Metalloproteinase-9 and Inflammatory Cytokines in Keratoconus Patients Is Inhibited by Cyclosporine A. Investig. Ophthalmol. Vis. Sci. 2015, 56, 738–750. [Google Scholar] [CrossRef] [PubMed]
- Galvis, V.; Sherwin, T.; Tello, A.; Merayo, J.; Barrera, R.; Acera, A. Keratoconus: An Inflammatory Disorder? Eye 2015, 29, 843–859. [Google Scholar] [CrossRef] [PubMed]
- Chaerkady, R.; Shao, H.; Scott, S.-G.; Pandey, A.; Jun, A.S.; Chakravarti, S. The Keratoconus Corneal Proteome: Loss of Epithelial Integrity and Stromal Degeneration. J. Proteom. 2013, 87, 122–131. [Google Scholar] [CrossRef]
- Xu, J.; Shi, G.-P. Vascular Wall Extracellular Matrix Proteins and Vascular Diseases. Biochim. Biophys. Acta 2014, 1842, 2106–2119. [Google Scholar] [CrossRef] [PubMed]
- Siordia, J.A.; Franco, J.C. The Association Between Keratoconus and Mitral Valve Prolapse: A Meta-Analysis. Curr. Cardiol. Rev. 2020, 16, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Akıncı, B. Evaluating Corneal Changes in Patients with Aort Aneurysm. Med. J. Haydarpaşa Numune Train. Res. Hosp. 2018, 59, 136–141. [Google Scholar] [CrossRef]
- Pierro, L.; Bianco, L.; Bertuzzi, F.; Arrigo, A.; Saladino, A.; Distefano, A.; Berni, A.; Knutsson, K.A.; Rama, P.; Bandello, F. New Findings in Early-Stage Keratoconus: Lamina Cribrosa Curvature, Retinal Nerve Fiber Layer Thickness, and Vascular Perfusion. Am. J. Ophthalmol. 2023, 246, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Zırtıloğlu, S.; Alikma, M.S.; Acar, O.P.A.; Furuncuoglu, U.; Guven, F. Evaluation of the Optic Nerve Head and Macular Vessel Density in Keratoconus Patients Using Optical Coherence Tomography Angiography—A Cross-Sectional Study. Eur. J. Ophthalmol. 2022, 33, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Falavarjani, K.G.; Shenazandi, H.; Naseri, D.; Anvari, P.; Kazemi, P.; Aghamohammadi, F.; Alissmail, F.; Alemzadeh, S.A. Foveal Avascular Zone and Vessel Density in Healthy Subjects: An Optical Coherence Tomography Angiography Study. J. Ophthalmic Vis. Res. 2018, 13, 260–265. [Google Scholar] [CrossRef]
- Yang, S.; Zhou, M.; Lu, B.; Zhang, P.; Zhao, J.; Kang, M.; Wang, R.; Wang, F.; Sun, X. Quantification of Macular Vascular Density Using Optical Coherence Tomography Angiography and Its Relationship with Retinal Thickness in Myopic Eyes of Young Adults. J. Ophthalmol. 2017, 2017, e1397179. [Google Scholar] [CrossRef]
- You, Q.S.; Chan, J.C.H.; Ng, A.L.K.; Choy, B.K.N.; Shih, K.C.; Cheung, J.J.C.; Wong, J.K.W.; Shum, J.W.H.; Ni, M.Y.; Lai, J.S.M.; et al. Macular Vessel Density Measured With Optical Coherence Tomography Angiography and Its Associations in a Large Population-Based Study. Investig. Ophthalmol. Vis. Sci. 2019, 60, 4830–4837. [Google Scholar] [CrossRef] [PubMed]
- Lavia, C.; Bonnin, S.; Maule, M.; Erginay, A.; Tadayoni, R.; Gaudric, A. Vessel Density of Superficial, Intermediate, and Deep Capillary Plexuses Using Optical Coherence Tomography Angiography. Retina 2019, 39, 247–258. [Google Scholar] [CrossRef]
- Yu, J.; Gu, R.; Zong, Y.; Xu, H.; Wang, X.; Sun, X.; Jiang, C.; Xie, B.; Jia, Y.; Huang, D. Relationship Between Retinal Perfusion and Retinal Thickness in Healthy Subjects: An Optical Coherence Tomography Angiography Study. Investig. Ophthalmol. Vis. Sci. 2016, 57, OCT204–OCT210. [Google Scholar] [CrossRef] [PubMed]
- Dimitrova, G.; Chihara, E.; Takahashi, H.; Amano, H.; Okazaki, K. Quantitative Retinal Optical Coherence Tomography Angiography in Patients With Diabetes Without Diabetic Retinopathy. Investig. Ophthalmol. Vis. Sci. 2017, 58, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Venkatesh, R.; Sinha, S.; Gangadharaiah, D.; Gadde, S.G.K.; Mohan, A.; Shetty, R.; Yadav, N.K. Retinal Structural-Vascular-Functional Relationship Using Optical Coherence Tomography and Optical Coherence Tomography—Angiography in Myopia. Eye Vis. 2019, 6, 8. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Zhao, Q.; Tao, R.; Lu, H.; Xiao, Z.; Zheng, L.; Ding, D.; Ding, S.; Ma, Y.; Lu, Z.; et al. Decreased Retinal Vascular Density in Alzheimer’s Disease (AD) and Mild Cognitive Impairment (MCI): An Optical Coherence Tomography Angiography (OCTA) Study. Front. Aging Neurosci. 2021, 12, 572484. [Google Scholar] [CrossRef] [PubMed]
- Milani, P.; Montesano, G.; Rossetti, L.; Bergamini, F.; Pece, A. Vessel Density, Retinal Thickness, and Choriocapillaris Vascular flow in Myopic Eyes on OCT Angiography. Graefe’s Arch. Clin. Exp. Ophthalmol. 2018, 256, 1419–1427. [Google Scholar] [CrossRef] [PubMed]
- Hou, H.; Moghimi, S.; Zangwill, L.M.; Shoji, T.; Ghahari, E.; Penteado, R.C.; Akagi, T.; Manalastas, P.I.C.; Weinreb, R.N. Macula Vessel Density and Thickness in Early Primary Open-Angle Glaucoma. Am. J. Ophthalmol. 2019, 199, 120–132. [Google Scholar] [CrossRef] [PubMed]
- Brautaset, R.L.; Rosén, R.; Cerviño, A.; Miller, W.L.; Bergmanson, J.; Nilsson, M. Comparison of Macular Thickness in Patients with Keratoconus and Control Subjects Using the Cirrus HD-OCT. Biomed. Res. Int. 2015, 2015, 832863. [Google Scholar] [CrossRef]
- Deonarain, S.; Motala, A.; Mthembu, T.; Nxele, N.; Phakathi, T.; Thwala, N.; Rampersad, N. Macular Thicknesses in Patients with Keratoconus: An Optical Coherence Tomography Study. Afr. Vision. Eye Health 2019, 78, 8. [Google Scholar] [CrossRef]
- Uzunel, U.D.; Küsbeci, T.; Yüksel, B. Does the Stage of Keratoconus Affect Optical Coherence Tomography Measurements? Semin. Ophthalmol. 2017, 32, 676–681. [Google Scholar] [CrossRef] [PubMed]
- Aydemir, G.A.; Kocabaş, D.O.; Bilen, A.; Aydemir, E.; Bayat, A.H.; Oren, B.; Kiziltoprak, H. Evaluation of Retinal Layer Thicknesses in Patients with Keratoconus Using Retinal Layer Segmentation Analysis. Klin. Monbl Augenheilkd. 2023, 240, 1199–1206. [Google Scholar] [CrossRef] [PubMed]
- Fard, A.M.; Patel, S.P.; Sorkhabi, R.D.; Salekzamani, S.; Pezzino, E.; Nader, N.D. Posterior Pole Retinal Thickness Distribution Pattern in Keratoconus. Int. Ophthalmol. 2020, 40, 2807–2816. [Google Scholar] [CrossRef] [PubMed]
- Sahebjada, S.; Amirul Islam, F.M.; Wickremasinghe, S.; Daniell, M.; Baird, P.N. Assessment of Macular Parameter Changes in Patients with Keratoconus Using Optical Coherence Tomography. J. Ophthalmol. 2015, 2015, e245953. [Google Scholar] [CrossRef] [PubMed]
- Özsaygılı, C.; Yıldırım, Y. The Relationship Between Keratoconus Stage and the Thickness of the Retinal Layers. Turk. J. Ophthalmol. 2021, 51, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Hashemi, H.; Heirani, M.; Ambrósio, R.; Hafezi, F.; Naroo, S.A.; Khorrami-Nejad, M. THE link between Keratoconus and Posterior Segment Parameters: An Updated, Comprehensive Review. Ocul. Surf. 2022, 23, 116–122. [Google Scholar] [CrossRef]
- Fernández-Vigo, J.I.; Moreno-Morillo, F.J.; López-Varela, E.; Novo-Bujan, J.; Ortega-Hortas, M.; Burgos-Blasco, B.; López-Guajardo, L.; Donate-López, J. Repeatability of Choriocapillaris Flow Voids by Optical Coherence Tomography Angiography in Central Serous Chorioretinopathy. PLoS ONE 2022, 17, e0279243. [Google Scholar] [CrossRef]
- Fernández-Vigo, J.I.; Kudsieh, B.; Macarro-Merino, A.; Arriola-Villalobos, P.; Martínez-de-la-Casa, J.M.; García-Feijóo, J.; Fernández-Vigo, J.Á. Reproducibility of Macular and Optic Nerve Head Vessel Density Measurements by Swept-Source Optical Coherence Tomography Angiography. Eur. J. Ophthalmol. 2020, 30, 756–763. [Google Scholar] [CrossRef] [PubMed]
- Manalastas, P.I.C.; Zangwill, L.M.; Saunders, L.J.; Mansouri, K.; Belghith, A.; Suh, M.H.; Yarmohammadi, A.; Penteado, R.C.; Akagi, T.; Shoji, T.; et al. Reproducibility of Optical Coherence Tomography Angiography Macular and Optic Nerve Head Vascular Density in Glaucoma and Healthy Eyes. J. Glaucoma 2017, 26, 851–859. [Google Scholar] [CrossRef]
- Mastropasqua, R.; D’Aloisio, R.; Agnifili, L.; Zuppardi, E.; Di Marzio, G.; Di Nicola, M.; Porreca, A.; Guarini, D.; Totta, M.; Brescia, L.; et al. Functional and Structural Reliability of Optic Nerve Head Measurements in Healthy Eyes by Means of Optical Coherence Tomography Angiography. Medicina 2020, 56, 44. [Google Scholar] [CrossRef]
- Lauermann, J.L.; Heiduschka, P.; Nelis, P.; Treder, M.; Alnawaiseh, M.; Clemens, C.R.; Eter, N.; Alten, F. Comparison of Choriocapillaris Flow Measurements between Two Optical Coherence Tomography Angiography Devices. Ophthalmologica 2017, 237, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Li, X.-X.; Wu, W.; Zhou, H.; Deng, J.-J.; Zhao, M.-Y.; Qian, T.-W.; Yan, C.; Xu, X.; Yu, S.-Q. A Quantitative Comparison of Five Optical Coherence Tomography Angiography Systems in Clinical Performance. Int. J. Ophthalmol. 2018, 11, 1784–1795. [Google Scholar] [CrossRef] [PubMed]
- Magrath, G.N.; Say, E.A.T.; Sioufi, K.; Ferenczy, S.; Samara, W.A.; Shields, C.L. Variability In Foveal Avascular Zone and Capillary Density Using Optical Coherence Tomography Angiography Machines In Healthy Eyes. Retina 2017, 37, 2102–2111. [Google Scholar] [CrossRef] [PubMed]
- Mihailovic, N.; Brand, C.; Lahme, L.; Schubert, F.; Bormann, E.; Eter, N.; Alnawaiseh, M. Repeatability, Reproducibility and Agreement of Foveal Avascular Zone Measurements Using Three Different Optical Coherence Tomography Angiography Devices. PLoS ONE 2018, 13, e0206045. [Google Scholar] [CrossRef] [PubMed]
- Coscas, F.; Sellam, A.; Glacet-Bernard, A.; Jung, C.; Goudot, M.; Miere, A.; Souied, E.H. Normative Data for Vascular Density in Superficial and Deep Capillary Plexuses of Healthy Adults Assessed by Optical Coherence Tomography Angiography. Investig. Ophthalmol. Vis. Sci. 2016, 57, OCT211–OCT223. [Google Scholar] [CrossRef] [PubMed]
- Ye, J.; Wang, M.; Shen, M.; Huang, S.; Xue, A.; Lin, J.; Fan, Y.; Wang, J.; Lu, F.; Shao, Y. Deep Retinal Capillary Plexus Decreasing Correlated With the Outer Retinal Layer Alteration and Visual Acuity Impairment in Pathological Myopia. Investig. Ophthalmol. Vis. Sci. 2020, 61, 45. [Google Scholar] [CrossRef]
- Nelis, P.; Kleffner, I.; Burg, M.C.; Clemens, C.R.; Alnawaiseh, M.; Motte, J.; Marziniak, M.; Eter, N.; Alten, F. OCT-Angiography Reveals Reduced Vessel Density in the Deep Retinal Plexus of CADASIL Patients. Sci. Rep. 2018, 8, 8148. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| KC (n = 26) | Controls (n = 26) | p | |
|---|---|---|---|
| n | 26 | 26 | n.a. |
| gender | 4/22 | 4/22 | n.a. |
| age (y) | 25.48 [20.48, 34.78] | 26.05 [23.68, 29.83] | 0.8382 |
| axial lengths (mm) | 23.81 [23.30, 24.14] | 24.04 [23.54, 24.22] | 0.3465 |
| corneal astigmatism (dpt) | 2.00 [1.35; 3.90] | 0.8 [0.60; 0.98] | <0.0001 |
| thinnest spot corneal pachymetry (µm) | 482.00 [467.00, 505.30] | 538.50 [523.30, 558.00] | <0.0001 |
| Kmax (dpt) | 50.95 [47.55; 53.85] | 43.60 [42.50, 44.43] | <0.0001 |
| df | 4.42 [3.39; 9.44] | 0.42 [−0.25; 0.86] | <0.0001 |
| db | 3.29 [2.33; 7.14] | −0.29 [−0.67; −0.08] | <0.0001 |
| dp | 5.43 [3.79; 7.17] | 0.83 [0.25; 1.13] | <0.0001 |
| dt | 1.75 [1.07; 2.34] | −0.07 [−0.79; 0.42] | <0.0001 |
| dy | 2.72 [2.29; 3.09] | 0.56 [0.35; 0.99] | <0.0001 |
| D | 5.65 [3.64; 7.21] | 0.99 [0.40; 1.31] | <0.0001 |
| KC (n = 26) | Controls (n = 26) | p | |
|---|---|---|---|
| SCP (VD) | |||
| whole en face | 44.40 [41.58; 47.13] | 47.40 [46.33; 48.83] | 0.0002 |
| Fovea | 17.35 [14.00; 26.15] | 21.75 [20.25; 25.30] | 0.0719 |
| Parafoveal | 46.70 [44.70; 49.28] | 50.10 [47.95; 51.93] | 0.0010 |
| DCP (VD) | |||
| whole en face | 50.60 [46.55; 54.25] | 50.70 [48.20; 53.40] | 0.5871 |
| Fovea | 36.10 [31.55; 42.53] | 38.35 [34.73; 42.58] | 0.3016 |
| Parafoveal | 53.35 [48.85; 55.75] | 52.60 [50.20; 54.65] | 0.9819 |
| CC (VD) | |||
| whole en face | 73.73 [71.41; 75.21] | 73.15 [71.74; 74.70] | 0.7682 |
| Fovea | 71.97 [68.72; 74.02] | 73.55 [72.01; 75.03] | 0.0310 |
| Parafoveal | 73.79 [71.27; 76.10] | 72.67 [71.51; 74.62] | 0.2245 |
| RPC (VD) | |||
| whole en face | 47.70 [46.00; 50.90] | 47.65 [46.00; 50.10] | 0.6359 |
| inside disc | 44.30 [39.55; 49.10] | 49.90 [46.45; 52.28] | 0.0033 |
| Peripapillary | 51.10 [49.35; 53.80] | 50.45 [48.88; 53.15] | 0.4571 |
| CRT (µm) | 264.00 [248.50; 276.30] | 264.5 [254.00; 270.30] | 0.7889 |
| FAZ (mm2) | 0.23 [0.14; 0.30] | 0.20 [0.14; 0.25] | 0.2590 |
| AI | 0.13 [0.11; 0.16] | 0.12 [0.11; 0.16] | 0.6388 |
| RT: all layers (µm) | |||
| whole en face | 334.80 [320,10; 339.50] | 332.70 [323.20; 343.20] | 0.4593 |
| Fovea | 273.60 [255.30; 288.90] | 275.60 [266.60; 281.10] | 0.7039 |
| Parafoveal | 343.40 [330.50; 349.20] | 341.30 [332.70; 352.80] | 0.9442 |
| RT: inner layers (µm) | |||
| whole en face | 172.60 [167.90; 181.00] | 175.60 [170.90; 183.30] | 0.9283 |
| Fovea | 89.10 [76.40; 106.90] | 94.40 [91.30; 106.40] | 0.7490 |
| Parafoveal | 183.50 [177.90; 191.20] | 184.90 [180.70; 191.50] | 0.7642 |
| RT: outer layers (µm) | |||
| whole en face | 157.10 [152.20; 162.90] | 156.60 [150.90; 160.80] | 0.6384 |
| Fovea | 180.30 [174.50; 189.00] | 182.30 [170.80; 186.70] | 0.6672 |
| Parafoveal | 157.60 [152.10; 163.40] | 156.20 [149.80; 161.40] | 0.7279 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leclaire, M.D.; Storp, J.J.; Lahme, L.; Esser, E.L.; Eter, N.; Alnawaiseh, M. Reduced Retinal Blood Vessel Densities Measured by Optical Coherence Tomography Angiography in Keratoconus Patients Are Negatively Correlated with Keratoconus Severity. Diagnostics 2024, 14, 707. https://doi.org/10.3390/diagnostics14070707
Leclaire MD, Storp JJ, Lahme L, Esser EL, Eter N, Alnawaiseh M. Reduced Retinal Blood Vessel Densities Measured by Optical Coherence Tomography Angiography in Keratoconus Patients Are Negatively Correlated with Keratoconus Severity. Diagnostics. 2024; 14(7):707. https://doi.org/10.3390/diagnostics14070707
Chicago/Turabian StyleLeclaire, Martin Dominik, Jens Julian Storp, Larissa Lahme, Eliane Luisa Esser, Nicole Eter, and Maged Alnawaiseh. 2024. "Reduced Retinal Blood Vessel Densities Measured by Optical Coherence Tomography Angiography in Keratoconus Patients Are Negatively Correlated with Keratoconus Severity" Diagnostics 14, no. 7: 707. https://doi.org/10.3390/diagnostics14070707