
The Performance of Pulmonary Function Tests in Predicting Systemic Sclerosis—Interstitial Lung Disease in the European Scleroderma Trial and Research Database
 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Patients and Methods
Statistical Analysis
3. Results
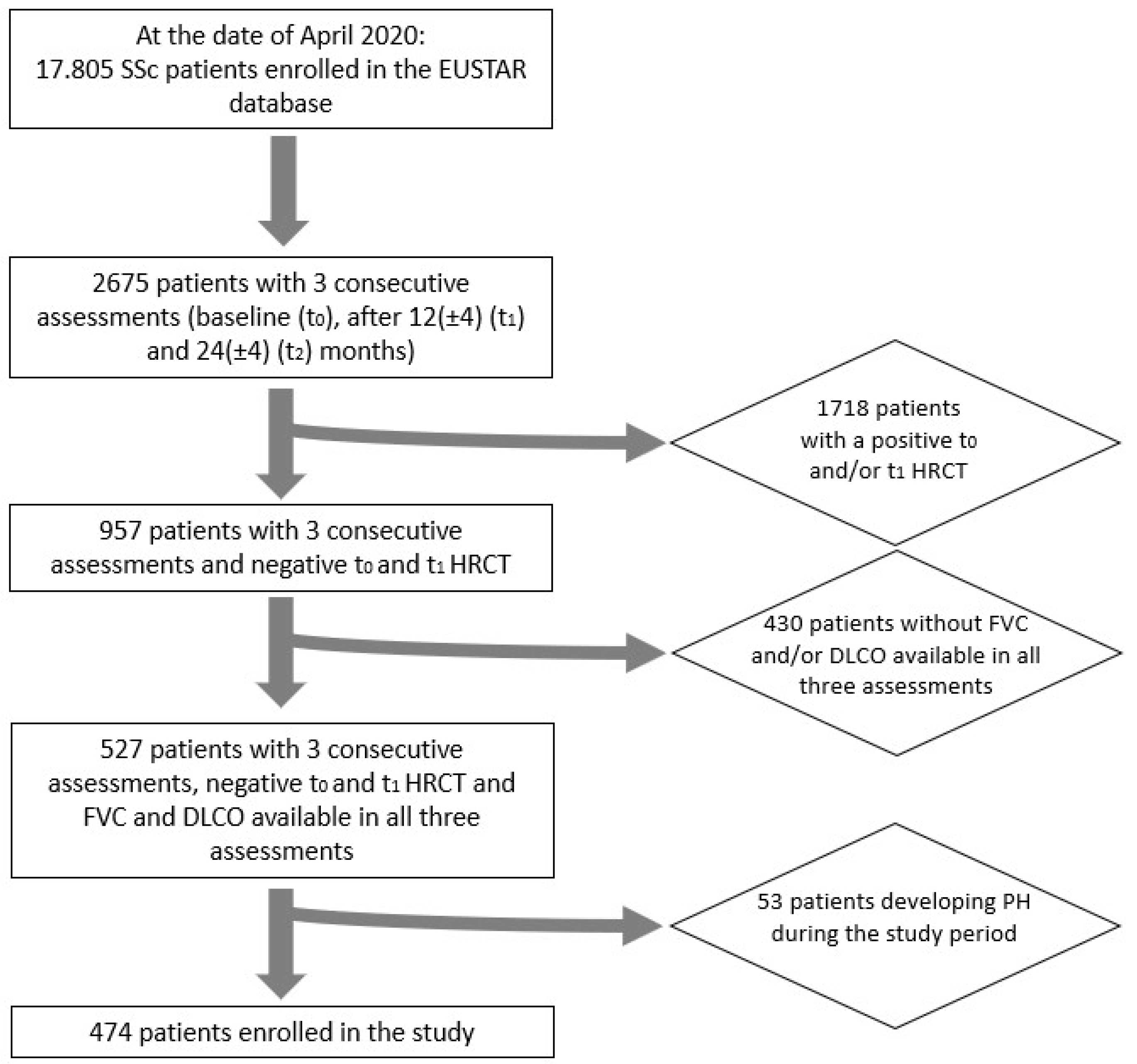
3.1. Study Population
3.2. Pulmonary Function Trends
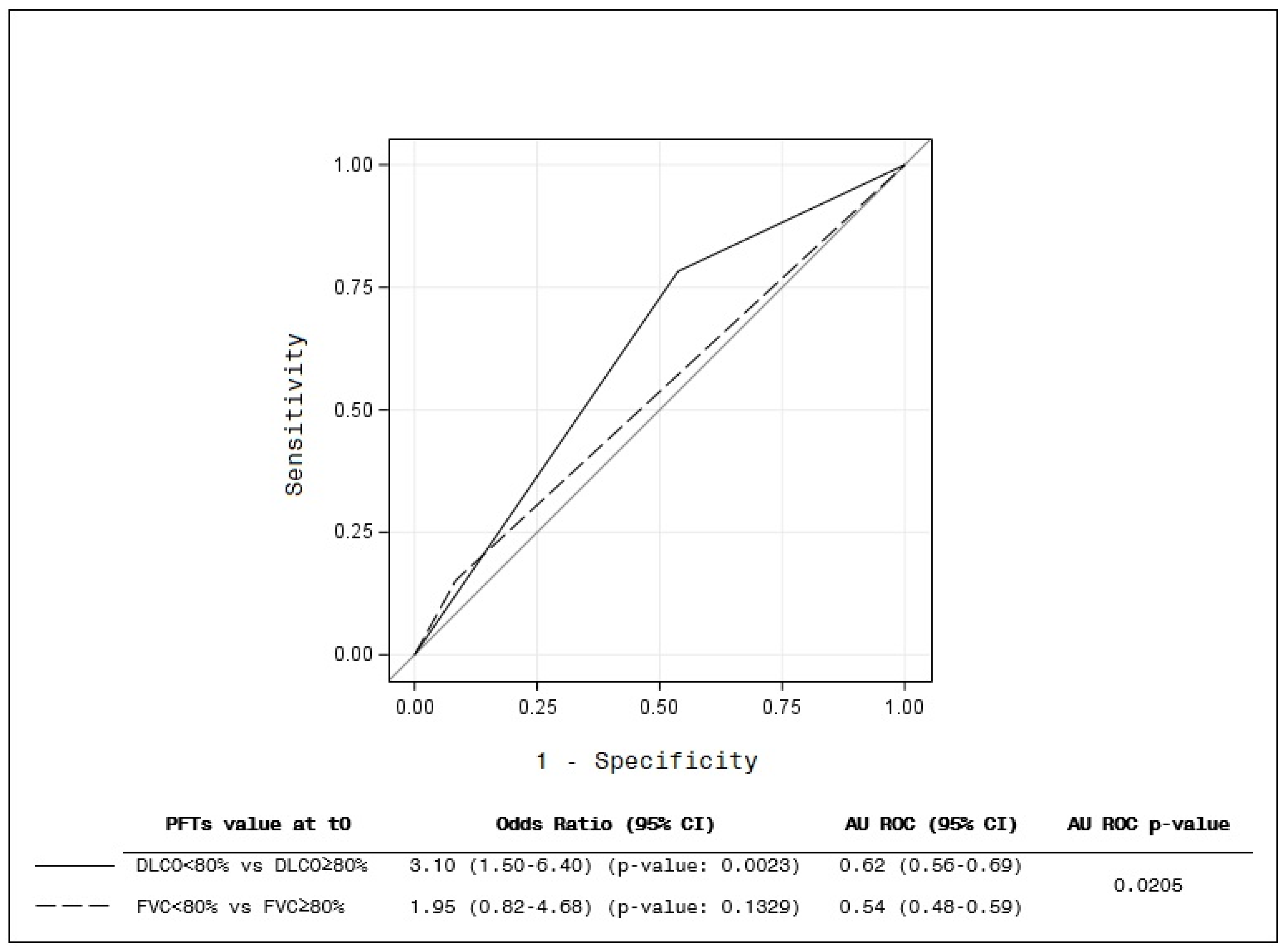
3.3. Primary End Point
3.4. Secondary End Point
- 161 patients maintained a normal DLCO;
- 47 moved from a normal to a reduced DLCO;
- 38 patients presented a reduced DLCO at t0 and recovered beyond normality at t1;
- 228 patients had a reduced DLCO both at t0 and at t1.
- 415 patients maintained a normal FVC;
- 16 patients moved from a normal to a reduced FVC;
- 11 patients presented a reduced FVC at t0 and recovered beyond a normality of ≥80% at t1;
- 32 patients had a reduced FVC both at t0 and at t1.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| SSc | Systemic sclerosis |
| ILD | Interstitial lung disease |
| HRCT | High-resolution computed tomography |
| PFTs | Pulmonary function tests |
| DLCO | Diffusion of the lung for carbon oxide |
| FVC | Forced vital capacity |
| EUSTAR | European Scleroderma Trial and Research |
| dcSSc | Diffuse cutaneous subset of SSc |
| lcSSc | Limited cutaneous subset of SSc |
| ACA | Anticentromere antibodies |
| Topo-I | Anti-topoisomerase I |
| RNA-Pol III | Anti-RNA polymerase III antibodies |
Appendix A
- -
- Basel (Switzerland) Ulrich Walker, Dr. Bettina Bannert (002);
- -
- Bari (Italy) Florenzo Iannone, Fabio Cacciapaglia [email protected] (004);
- -
- Genova (Italy) Maurizio Cutolo, Sabrina Paolino [email protected] (011);
- -
- Pavia (Italy), Carlomaurizio Montecucco, Roberto Caporali [email protected] (019);
- -
- Madrid (Spain), Patricia Carreira, Beatriz E. Joven (023);
- -
- Padova (Italy), Andrea Doria, Elisabetta Zanatta (031);
- -
- Paris (France), Dominique Farge Bancel, Adrian Hij [email protected] (035);
- -
- Torino (Italy), Raffaele Pellerito, Torino, Italy (049);
- -
- Tübingen (Germany), Jörg Henes, Ann-Christian Pecher [email protected] (056);
- -
- Niska Banja (Serbia and Montenegro), Bojana Stamenkovic, Aleksandra Stankovic [email protected] (073);
- -
- Moscow (Russia), Lidia P.Ananieva, Ludmila Garzanova [email protected] (078);
- -
- Bad Nauheim (Germany), Ulf Müller-Ladner (081);
- -
- Lille (France), David Launay (093);
- -
- Bucharest (Romania), Ruxandra Maria Ionescu, Daniela Opris [email protected] (096);
- -
- Bucharest (Romania), Ana Maria Gheorghiu, Mihai Bojinca (100);
- -
- Erlangen (Germany), Jörg Distler (106);
- -
- Milan (Italy); Francesca Ingegnoli (110);
- -
- Gent (Belgium), Vanessa Smith (113);
- -
- Foggia (Italy), Francesco Paolo Cantatore, Addolorata Corrado [email protected] (115);
- -
- Copenhagen (Denmark), Susanne Ullman (116);
- -
- Brussels (Belgium), Marie Vanthuyne, Houssiau frédéric [email protected] (122);
- -
- Beijing (China), Mengtao Li (154);
- -
- Alexandria (Egypt), Walid Ahmed Abdel Atty Mohamed (155);
- -
- Roma (Italy), Edoardo Rosato, Antonietta Gigante (158);
- -
- Madrid (Spain), Paloma García de la Peña Lefebvre, Dr. Jorge Juan Gonzalez Martin (169);
- -
- Buenos Aires (Argentina), Eduardo Kerzberg, Fabiana Montoya [email protected] (178);
- -
- Barcelona (Spain), Ivan Castellví, Milena Millan (180);
- -
- New Brunswick, USA, Vivien M. Hsu (188);
- -
- Lubeck (Germany), Gabriela Riemekasten, Sabine Sommerlatte (199).
References
- Varga, J.; Trojanowska, M.; Kuwana, M. Pathogenesis of systemic sclerosis: Recent insights of molecular and cellular mechanisms and therapeutic opportunities. J. Scleroderma Relat. Disord. 2017, 2, 137–152. [Google Scholar] [CrossRef]
- Volkmann, E.R.; Fischer, A. Update on morbidity and mortality in systemic sclerosis–related interstitial lung disease. J. Scleroderma Relat. Disord. 2020, 6, 11–20. [Google Scholar] [CrossRef]
- Steen, V.D.; Medsger, T.A. Changes in causes of death in systemic sclerosis, 1972–2002. Ann. Rheum. Dis. 2007, 66, 940–944. [Google Scholar] [CrossRef]
- Perelas, A.; Silver, R.M.; Arrossi, A.V.; Highland, K.B. Systemic sclerosis-associated interstitial lung disease. Lancet Respir. Med. 2020, 8, 304–320. [Google Scholar] [CrossRef]
- Walker, U.A.; Tyndall, A.; Czirjak, L.; Denton, C.; Farge-Bancel, D.; Kowal-Bielecka, O.; Muller-Ladner, U.; Bocelli-Tyndall, C.; Matucci-Cerinic, M. Clinical risk assessment of organ manifestations in systemic sclerosis: A report from the EULAR scleroderma trials and research group database. Ann. Rheum. Dis. 2007, 66, 754–763. [Google Scholar] [CrossRef]
- Zanatta, E.; Moccaldi, B.; Szucs, G.; Spagnolo, P. Should we use nintedanib as early therapy in patients with SSc-ILD? Autoimmun. Rev. 2023, in press. [Google Scholar] [CrossRef] [PubMed]
- Panagopoulos, P.K.; Goules, A.V.; Georgakopoulou, V.E.; Kallianos, A.; Chatzinikita, E.; Pezoulas, V.C.; Malagari, K.; Fotiadis, D.I.; Vlachoyiannopoulos, P.; Vassilakopoulos, T.; et al. Small airways dysfunction in patients with systemic sclerosis and interstitial lung disease. Front. Med. 2022, 9, 1016898. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann-Vold, A.M.; Fretheim, H.; Halse, A.K.; Seip, M.; Bitter, H.; Wallenius, M.; Garen, T.; Salberg, A.; Brunborg, C.; Midtvedt, Ø.; et al. Tracking Impact of Interstitial Lung Disease in Systemic Sclerosis in a Complete Nationwide Cohort. Am. J. Respir. Crit. Care Med. 2019, 200, 1258–1266. [Google Scholar] [CrossRef] [PubMed]
- Cottin, V.; Brown, K.K. Interstitial lung disease associated with systemic sclerosis (SSc-ILD). Respir. Res. 2019, 20, 13. [Google Scholar] [CrossRef] [PubMed]
- Man, A.; Davidyock, T.; Ferguson, L.T.; Ieong, M.; Zhang, Y.; Simms, R.W. Changes in forced vital capacity over time in systemic sclerosis: Application of group-based trajectory modelling. Rheumatology 2015, 54, 1464–1471. [Google Scholar] [CrossRef]
- Assassi, S.; Sharif, R.; Lasky, R.E.; McNearney, T.A.; Estrada-Y-Martin, R.M.; Draeger, H.; Nair, D.N.; Fritzler, M.J.; Reveille, J.D.; Arnett, F.C.; et al. Predictors of interstitial lung dis-ease in early systemic sclerosis: A prospective longitudinal study of the GENISOS cohort. Arthr Res. Ther. 2010, 12, R166. [Google Scholar] [CrossRef] [PubMed]
- Distler, O.; Volkmann, E.R.; Hoffmann-Vold, A.M.; Maher, T.M. Current and future perspectives on management of systemic scle-rosis-associated interstitial lung disease. Expert. Rev. Clin. Immunol. 2010, 15, 1009–1017. [Google Scholar] [CrossRef] [PubMed]
- Ruaro, B.; Baratella, E.; Confalonieri, P.; Confalonieri, M.; Vassallo, F.G.; Wade, B.; Geri, P.; Pozzan, R.; Caforio, G.; Marrocchio, C.; et al. High-Resolution Computed Tomography and Lung Ultrasound in Patients with Systemic Sclerosis: Which One to Choose? Diagnostics 2021, 11, 2293. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann-Vold, A.M.; Maher, T.M.; Philpot, E.E.; Ashrafdazadeh, A.; Barake, R.; Barsotti, S.; Bruni, C.; Carducci, P.; Carreira, P.E.; Castellvi, I.; et al. The identification and man-agement of interstitial lung disease in systemic sclerosis: Evidence-based European consensus statements. Lancet Rheumatol. 2020, 2, e71–e83. [Google Scholar] [CrossRef] [PubMed]
- Plastiras, S.C.; Karadimitrakis, S.P.; Ziakas, P.D.; Vlachoyiannopoulos, P.G.; Moutsopoulos, H.M.; Tzelepis, G.E. Scleroderma lung: Initial forced vital capacity as predictor of pulmonary function decline. Arthritis Rheumatol. 2006, 55, 598–602. [Google Scholar] [CrossRef]
- Hoffman, A.M.; Aaløkken, T.M.; Brit, L.M.; Garen, T.; Midtvedt, O.; Brunborg, C.; Tore, G.J.; Molberg, Ø. Predictive value of serial high-resolution computed tomography analyses and concurrent lung function tests in systemic sclerosis. Arthritis Rheumatol. 2015, 67, 2205–2212. [Google Scholar] [CrossRef]
- Caron, M.; Hoa, S.; Hudson, M.; Schwartzman, K.; Steele, R. Pulmonary function tests as outcomes for systemic sclerosis interstitial lung disease. Eur. Respir. Rev. 2018, 27, 170102. [Google Scholar] [CrossRef]
- Raghu, G.; Remy-Jardin, M.; Richeldi, L.; Thomson, C.C.; Inoue, Y.; Johkoh, T.; Kreuter, M.; Lynch, D.A.; Maher, T.M.; Martinez, F.J.; et al. Idiopathic Pulmonary Fibrosis (an Update) and Progressive Pulmonary Fibrosis in Adults: An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2022, 205, e18–e47. [Google Scholar] [CrossRef]
- Kaenmuang, P.; Navasakulpong, A. Short-Term Lung Function Changes and Predictors of Progressive Systemic Sclerosis–Related Interstitial Lung Disease. Tuberc. Respir. Dis. 2020, 83, 312–320. [Google Scholar] [CrossRef]
- Goh, N.S.; Desai, S.R.; Veeraraghavan, S.; Hansell, D.M.; Copley, S.J.; Maher, T.B.; Corte, T.J.; Sander, C.R.; Ratoff, J.; Devaraj, J.; et al. Interstitial lung disease in systemic sclerosis: A simple staging system. Am. J. Respir. Crit. Care Med. 2008, 177, 1248–1254. [Google Scholar] [CrossRef]
- Goh, N.S.; Hoyles, R.K.; Denton, C.P.; Hansell, D.M.; Renzoni, E.A.; Maher, T.M.; Nicholson, A.G.; Wells, A.U. Short-Term Pulmonary Function Trends Are Predictive of Mortality in Interstitial Lung Disease Associated With Systemic Sclerosis. Arthritis Rheumatol. 2017, 69, 1670–1678. [Google Scholar] [CrossRef] [PubMed]
- Naidu, G.S.R.S.N.K.; Sharma, S.K.; Adarsh, M.B.; Dhir, V.; Sinha, A.; Dhooria, S.; Jain, S. Effect of mycophenolate mofetil (MMF) on sys-temic sclerosis-related interstitial lung disease with mildly impaired lung function: A double-blind, placebo-controlled, ran-domized trial. Rheumatol. Int. 2020, 40, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Showalter, K.; Hoffmann, A.; Rouleau, G.; Aaby, D.; Lee, J.; Richardson, C.; Dematte, J.; Agrawal, R.; Chang, R.W.; Hinchcliff, M. Performance of Forced Vital Capacity and Lung Diffusion Cutpoints for Associated Radiographic Interstitial Lung Disease in Systemic Sclerosis. J. Rheumatol. 2018, 45, 1572–1576. [Google Scholar] [CrossRef] [PubMed]
- Khanna, D.; Seibold, J.R.; Wells, A.; Distler, O.; Allanore, Y.; Denton, C.; Furst, D.E. Systemic sclerosis-associated interstitial lung disease: Lessons from clinical trials, outcome measures, and future study design. Curr. Rheumatol. Rev. 2010, 6, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, E.J.; Jaafar, S.; Assassi, S.; Domsic, R.T.; Frech, T.M.; Gordon, J.K.; Broderick, R.J.; Hant, F.N.; Hinchcliff, M.E.; Shah, A.A.; et al. PFTs alone are an inadequate screening tool for the diagnosis of ILD in patients with early dcSSc. Arthritis Rheumatol. 2020, 72, 1892–1896. [Google Scholar] [CrossRef] [PubMed]
- Khanna, S.A.; Nance, J.W.; Suliman, S.A. Detection and Monitoring of Interstitial Lung Disease in Patients with Systemic Sclerosis. Curr. Rheumatol. Rep. 2022, 24, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Van den Hoogen, F.; Khanna, D.; Fransen, J.; Johnson, S.R.; Baron, M.; Tyndall, A.; Matucci-Cerinic, M.; Naden, R.P.; Medsger, T.A., Jr.; Carreira, P.E.; et al. 2013 classification criteria for systemic sclerosis: An American college of rheumatology/European league against rheumatism collaborative initiative. Arthritis Rheum. Dis. 2013, 72, 1747–1755. [Google Scholar] [CrossRef]
- Subcommittee for Scleroderma Criteria of the American Rheumatism Association Diagnostic and Therapeutic Criteria Com-mittee. Preliminary criteria for the classification of systemic sclerosis (scleroderma). Arthritis Rheum. 1980, 23, 581–590. [Google Scholar] [CrossRef]
- Owens, G.R.; Fino, G.J.; Herbert, D.L.; Steen, V.D.; Medsger Jr, T.A.; Pennock, B.E.; Cottrell, J.J.; Rodnan, G.P.; Rogers, R.M. Pulmonary function in progressive systemic sclerosis. Comparison of CREST syndrome variant with diffuse scleroderma. Chest 1983, 84, 546–550. [Google Scholar] [CrossRef]
- Morisset, J.; Vittinghoff, E.; Elicker, B.M.; Hu, X.; Le, S.; Ryu, J.H.; Jones, K.D.; Haemel, A.; Golden, J.A.; Boin, F.; et al. Mortality Risk Prediction in Scleroderma-Related Interstitial Lung Disease: The SADL Model. Chest 2017, 152, 999–1007. [Google Scholar] [CrossRef]
- Herzog, E.L.; Mathur, A.; Tager, A.M.; Feghali-Bostwick, C.; Schenider, F.; Varga, J. Review: Interstitial lung disease associated with systemic sclerosis and idiopathic pulmonary fibrosis: How similar and distinct? Arthritis Rheumatol. 2014, 66, 1967–1978. [Google Scholar] [CrossRef]
- Knarborg, M.; Hyldgaard, C.; Bendstrup, E.; Davidsen, J.R.; Løkke, A.; Shaker, S.B.; Hilberg, O. Incidence, prevalence and regional distribution of systemic sclerosis and related interstitial lung Disease: A nationwide retrospective cohort study. Chronic Respir. Dis. 2022, 19, 14799731221125559. [Google Scholar] [CrossRef]
- George, P.M.; Wells, A.U. Disease staging and sub setting of interstitial lung disease associated with systemic sclerosis: Impact on therapy. Expert. Rev. Clin. Immunol. 2018, 14, 127–135. [Google Scholar] [CrossRef]
- Tashkin, D.P.; Volkmann, E.R.; Tseng, C.-H.; Kim, H.J.; Goldin, J.; Clements, P.; Furst, D.; Khanna, D.; Kleerup, E.; Roth, M.D.; et al. Relationship between quantitative radiographic assessments of interstitial lung disease and physiological and clinical features of systemic sclerosis. Ann. Rheum. Dis. 2016, 75, 374–381. [Google Scholar] [CrossRef]
- Nagy, T.; Toth, N.M.; Palmer, E.; Polivka, L.; Csoma, B.; Nagy, A.; Eszes, N.; Vincze, K.; Bárczi, E.; Bohács, A.; et al. Clinical Predictors of Lung-Function Decline in Systemic-Sclerosis-Associated Interstitial Lung Disease Patients with Normal Spirometry. Biomedicines 2022, 10, 2129. [Google Scholar] [CrossRef]
- Wu, W.; Jordan, S.; Becker, M.O.; Dobrota, R.; Maurer, B.; Fretheim, H.; Ye, S.; Siegert, E.; Allanore, Y.; Hoffmann-Vold, A.-M.; et al. Prediction of progression of interstitial lung disease in patients with systemic sclerosis: The SPAR model. Ann. Rheum. Dis. 2018, 77, 1326–1332. [Google Scholar] [CrossRef]
- Ahmed, S.S.; Johnson, S.R.; Meaney, C.; Chau, C. Lung function and survival in systemic sclerosis interstitial lung disease. J. Rheumatol. 2014, 41, 2326–2328. [Google Scholar] [CrossRef]
- Volkmann, E.R.; Tashkin, D.P.; Sim, M.; Li, N.; Goldmuntz, E.; Keyes-Elstein, L.; Pinckney, A.; Furst, D.E.; Clements, P.J.; Khanna, D.; et al. Short-teOh dear IBoy they’re not gonna be happyrm progression of interstitial lung disease in systemic sclerosis predicts long-term survival in two independent clinical trial cohorts. Ann. Rheum. Dis. 2019, 78, 122–130. [Google Scholar] [CrossRef]
- Nihtyanova, S.I.; Denton, C.P. Pathogenesis of systemic sclerosis associated interstitial lung disease. J. Scleroderma. Relat. Disord. 2020, 5, 6–16. [Google Scholar] [CrossRef]
- Steen, V.; Domsic, R.T.; Lucas, M.; Fertig, N.; Medsger, T.A. A clinical and serologic comparison of African American and Caucasian patients with systemic sclerosis. Arthritis Rheum. 2012, 64, 2986–2994. [Google Scholar] [CrossRef]
- Nihtyanova, S.I.; Schreiber, B.E.; Ong, V.H.; Rosenberg, D.; Moinzadeh, P.; Coghlan, J.G.; Wells, A.U.; Denton, C.P. Prediction of Pulmonary Complications and Long-Term Survival in Systemic Sclerosis. Arthritis Rheumatol. 2014, 66, 1625–1635. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Jordan, S.; de Oliveira Graf, N.; Pena, J.d.O.; Curram, J.; Allanore, Y.; Matucci-Cerinic, M.; Pope, J.E.; Denton, C.P.; Khanna, D.; et al. Progressive skin fibrosis is associated with a decline in lung function and worse survival in patients with diffuse cutaneous systemic sclerosis in the European Scleroderma Trials and Research (EUSTAR) cohort. Ann. Rheum. Dis. 2019, 78, 648–656. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Features | Number of Patients (% of Patients with Available Data) |
|---|---|
| Sex (F) | 403 (85.0%) |
| Cigarette smoking ever | 33 (20.8%) |
| N.A. | 315 |
| Current cigarette smoker | 14 (26.4%) |
| N.A. | 421 |
| Disease duration (from Raynaud’s phenomenon onset) in months (median; Q1–Q3) | 77.4 (28.0–165.8) |
| Dysphagia | 286 (60.5%) |
| N.A. | 1 |
| Renal crisis | 6 (1.3%) |
| N.A. | 2 |
| Dyspnoea NYHA stage | |
| 353 (79.0%) |
| 89 (19.9%) |
| 5 (1.1%) |
| 0 |
| N.A. | 27 |
| Palpitations | 63 (13.6%) |
| N.A. | 9 |
| Conduction block | 50 (11.6%) |
| N.A. | 42 |
| Skin involvement | |
| 122 (26.0%) |
| 274 (58.3%) |
| 56 (11.9%) |
| 18 (3.8%) |
| N.A. | 4 |
| mRSS (mean ± SD) | 7.6 ± 7.1 |
| Digital pitting scars | |
| 36 (26.3%) |
| 26 (19.0%) |
| 75 (54.7%) |
| N.A. | 337 |
| Digital ulcers | |
| 16 (11.6%) |
| 44 (31.9%) |
| 78 (56.5%) |
| N.A. | 336 |
| Telangiectasia | 58 (37.9%) |
| N.A. | 321 |
| SSc-specific Antibody positivity | |
| 220 (48.0%) (N.A. 18) |
| 117 (25.4%) (N.A. 16) |
| 12 (4.7%) (N.A. 224) |
| CRP Elevation | 50 (10.9%) |
| N.A. | 16 |
| Presence of proteinuria | 15 (3.3%) |
| N.A. | 9 |
| Capillaroscopic scleroderma pattern | |
| 52 (28.3%) |
| 82 (44.6%) |
| 50 (27.2%) |
| N.A. | 290 |
| Features | Patients with Negative t2 HRCT n (%) | Patients with Positive t2 HRCT n (%) | p-Value |
|---|---|---|---|
| Gender | |||
| 365 (91.0%) | 36 (9.0%) | 0.2101 |
| 63 (86.3%) | 10 (13.7%) | |
| Disease duration (from Raynaud onset) in months (median; Q1–Q3) (n) | 77.8 (28.4–161.7) (206) | 71.2 (17.4–194.1) (18) | 0.7537 |
| Skin involvement | |||
| 106 (86.9%) | 16 (13.1%) | |
| 250 (91.2%) | 24 (8.8%) | |
| 52 (92.9%) | 4 (7.1%) | 0.2832 |
| 18 | 0 | |
| mRSS (mean ± SD) (median; Q1-Q3) (n) | 6 (3–10) (393) | 7 (3–13) | 0.1563 |
| SSc-specific Antibody positivity | |||
| 211 (95.9%) | 9 (4.1%) | 0.0001 |
| 203 (85.3%) | 35 (14.7%) | |
| 97 (82.9%) | 20 (17.1%) | 0.0031 |
| 317 (92.4%) | 26 (7.6%) | |
| 9 (75.0%) | 3 (25.0%) | 0.1003 |
| 222 (91.0%) | 22 (9%) | |
| PFTs (values reported as %predicted ±SD) | |||
| 79.0 (±16.6) | 69.9 (±17.4) | 0.0006 |
| 102.2 (±17.3) | 94.6 (±16.2) | 0.0052 |
| 78.4 (±16.8) | 68.9 (±18.6) | 0.0005 |
| 101.9 (±17.9) | 94.7 (±16.5) | 0.0092 |
| 78.0 (±17.0) | 65.1 (±19.1) | <0.0001 |
| 101.6 (±17.6) | 94.5 (±20.0) | 0.126 |
| Trend in DLCO from t0 to t1 | Pts with Negative t2 HRCT | Pts with Positive t2 HRCT | Odds Ratio (Confidence Limits) | p-Value |
|---|---|---|---|---|
| DLCO ≥ 80% at t0 and t1 | 152 (94.4%) | 9 (5.6%) | Ref | |
| DLCO ≥ 80% at t0 and <80% at t1 | 46 (9.7%) | 1 (2.2%) | 0.37 (0.05–2.98) | 0.3479 |
| DLCO < 80% at t0 and ≥80% at t1 | 33 (86.6%) | 5 (13.3%) | 2.56 (0.81–8.13) | 0.1112 |
| DLCO < 80% at t0 and at t1 | 197 (86.6%) | 31 (13.3%) | 2.66 (1.23–5.75) | 0.0130 |
| Trend in FVC from t0 to t1 | Pts with Negative t2 HRCT | Pts with Positive t2 HRCT | Odds Ratio (Confidence Limits) | p-Value |
| FVC ≥ 80% at t0 and t1 | 380 (91.0%) | 35 (8.9%) | Ref | |
| FVC ≥ 80% at t0 and <80% at t1 | 12 (75.5%) | 4 (25.5%) | 3.62 (1.11–11.82) | 0.0331 |
| FVC < 80% at t0 and ≥80% at t1 | 10 (91.0%) | 1 (8.9%) | 1.09 (0.14–8.73) | 0.9384 |
| FVC < 80% at t0 and at t1 | 26 (81.0%) | 6 (18.9%) | 2.51 (0.97–6.50) | 0.0588 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lepri, G.; Bruni, C.; Tofani, L.; Moggi-Pignone, A.; Orlandi, M.; Tomassetti, S.; Hughes, M.; Del Galdo, F.; Irace, R.; Distler, O.; et al. The Performance of Pulmonary Function Tests in Predicting Systemic Sclerosis—Interstitial Lung Disease in the European Scleroderma Trial and Research Database. Diagnostics 2024, 14, 295. https://doi.org/10.3390/diagnostics14030295
Lepri G, Bruni C, Tofani L, Moggi-Pignone A, Orlandi M, Tomassetti S, Hughes M, Del Galdo F, Irace R, Distler O, et al. The Performance of Pulmonary Function Tests in Predicting Systemic Sclerosis—Interstitial Lung Disease in the European Scleroderma Trial and Research Database. Diagnostics. 2024; 14(3):295. https://doi.org/10.3390/diagnostics14030295
Chicago/Turabian StyleLepri, Gemma, Cosimo Bruni, Lorenzo Tofani, Alberto Moggi-Pignone, Martina Orlandi, Sara Tomassetti, Michael Hughes, Francesco Del Galdo, Rosaria Irace, Oliver Distler, and et al. 2024. "The Performance of Pulmonary Function Tests in Predicting Systemic Sclerosis—Interstitial Lung Disease in the European Scleroderma Trial and Research Database" Diagnostics 14, no. 3: 295. https://doi.org/10.3390/diagnostics14030295