
Diagnosis and Orthodontic Treatment of Obstructive Sleep Apnea Syndrome Children—A Systematic Review
 , , ,
, , ,  , ,
, ,  ,
,  ,
,  and
and
Abstract
:1. Introduction
1.1. Risk Factors
1.1.1. Hypertrophy of Adenotonsillary
1.1.2. Obesity
1.1.3. Craniofacial Syndromes
1.1.4. Neuromuscular Diseases
1.1.5. Hypercapnia
1.1.6. Pediatric OSAS Symptoms and Signs
1.2. Complications
1.3. Management
1.3.1. Adenotonsillectomy (AT)
1.3.2. CPAP
1.3.3. Medical Therapy
1.3.4. Bariatric Surgery
1.3.5. Orthodontic Treatment
2. Materials and Methods
2.1. Protocol and Registration
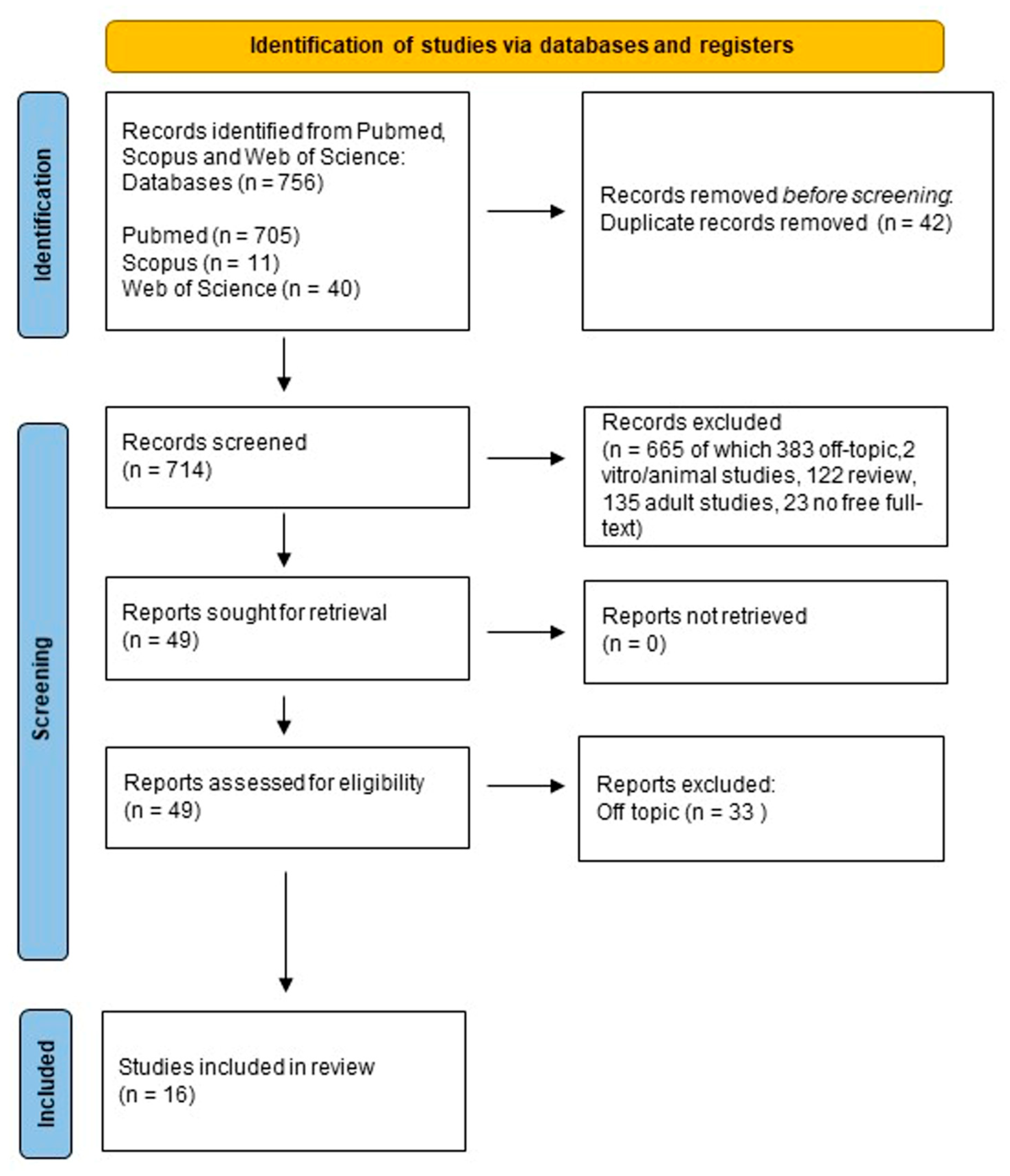
2.2. Search Processing
2.3. Eligibility Criteria
2.4. Data Processing
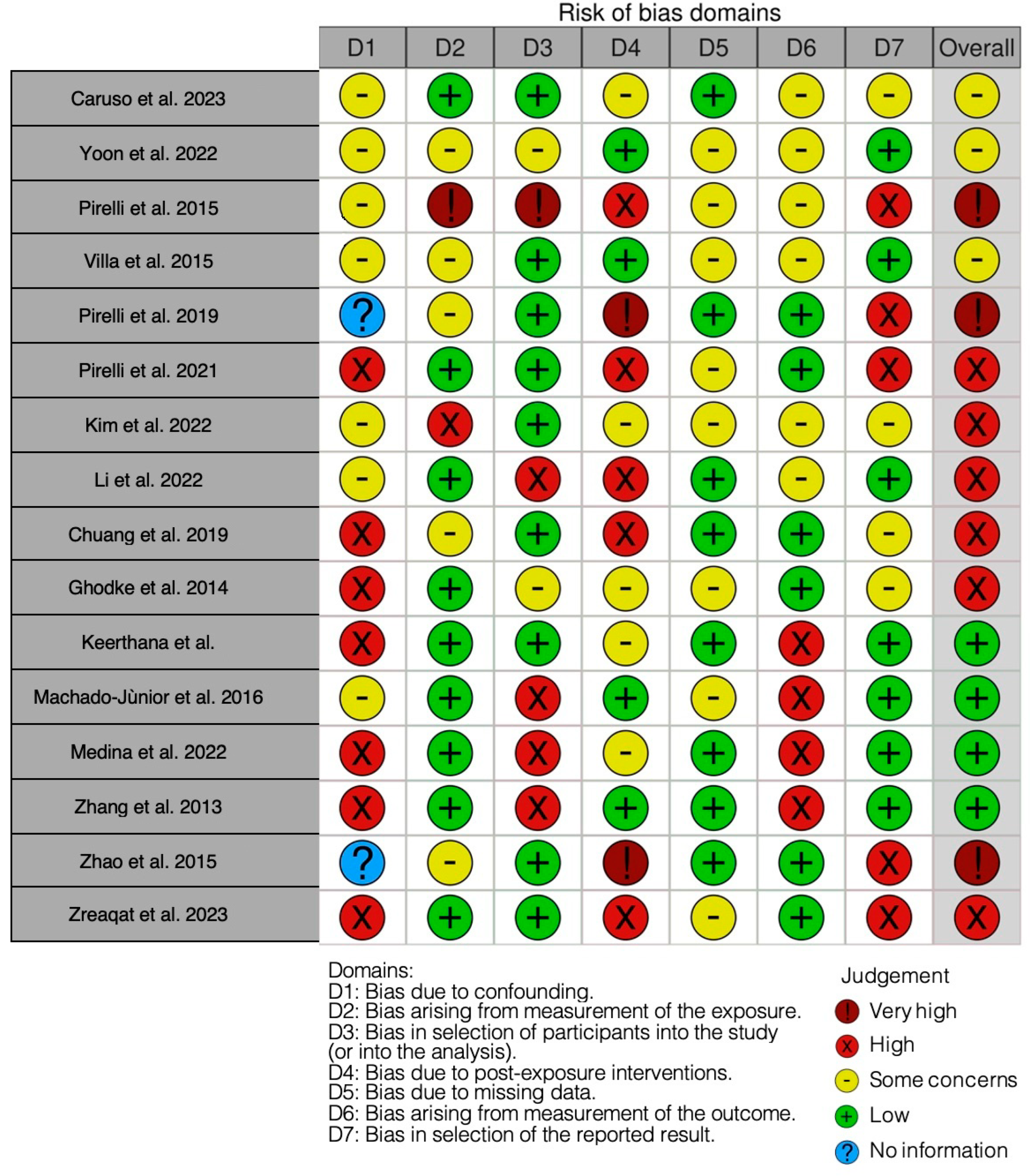
2.5. Quality Assessment
3. Results
Quality Assessment and Risk of Bias
4. Discussion
4.1. OSAS Treatment with Rapid Palatal Expander
4.1.1. Effectiveness of RPE in Modifying the Upper Airway
4.1.2. Radiographic Evaluation of the Effects of RPE
4.1.3. Alternative Treatments in Cases of RPE Failure
4.1.4. Long-Term Effectiveness
4.2. OSAS Treatment with Mandibular Advancement Devices
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AT | Adenotonsillectomy |
| AHI | Apnea-hypopnea index |
| BMIs | Body mass indices |
| CBCT | Cone beam computational tomography |
| CPAP | Continuous positive airway pressure |
| CT | Computed tomography |
| MAA | Mandibular advancement appliance |
| MCA | Minimum cross-sectional area |
| OSA | Obstructive sleep apnea |
| OSAS | Obstructive Sleep Apnea Syndrome |
| PAP | Pharyngeal airway passage |
| PMFT | Passive myofunctional therapy |
| PSG | Polysomnography |
| RME | Rapid maxillary expansion |
| RPE | Rapid palatal expansion/Rapid palatal expander |
| TB | Twin Block |
| TPD | Nasomaxillary expansion using skeletally anchored trans-palatal distraction |
References
- Marcus, C.L.; Brooks, L.J.; Draper, K.A.; Gozal, D.; Halbower, A.C.; Jones, J.; Schechter, M.S.; Ward, S.D.; Sheldon, S.H.; Shiffman, R.N.; et al. Diagnosis and Management of Childhood Obstructive Sleep Apnea Syndrome. Pediatrics 2012, 130, e714–e755. [Google Scholar] [CrossRef] [PubMed]
- Katz, E.S.; D’Ambrosio, C.M. Pediatric Obstructive Sleep Apnea Syndrome. Clin. Chest Med. 2010, 31, 221–234. [Google Scholar] [CrossRef] [PubMed]
- Alexander, N.S.; Schroeder, J.W. Pediatric Obstructive Sleep Apnea Syndrome. Pediatr. Clin. N. Am. 2013, 60, 827–840. [Google Scholar] [CrossRef] [PubMed]
- Schwengel, D.A.; Dalesio, N.M.; Stierer, T.L. Pediatric Obstructive Sleep Apnea. Anesthesiol. Clin. 2014, 32, 237–261. [Google Scholar] [CrossRef]
- Arens, R.; Muzumdar, H. Childhood Obesity and Obstructive Sleep Apnea Syndrome. J. Appl. Physiol. 1985 2010, 108, 436–444. [Google Scholar] [CrossRef]
- Alonso-Álvarez, M.L.; Cordero-Guevara, J.A.; Terán-Santos, J.; Gonzalez-Martinez, M.; Jurado-Luque, M.J.; Corral-Peñafiel, J.; Duran-Cantolla, J.; Kheirandish-Gozal, L.; Gozal, D. Obstructive Sleep Apnea in Obese Community-Dwelling Children: The NANOS Study. Sleep 2014, 37, 943–949. [Google Scholar] [CrossRef]
- Reddy, L.K.V.; Madithati, P.; Narapureddy, B.R.; Ravula, S.R.; Vaddamanu, S.K.; Alhamoudi, F.H.; Minervini, G.; Chaturvedi, S. Perception about Health Applications (Apps) in Smartphones towards Telemedicine during COVID-19: A Cross-Sectional Study. J. Pers. Med. 2022, 12, 1920. [Google Scholar] [CrossRef]
- Rathi, S.; Chaturvedi, S.; Abdullah, S.; Rajput, G.; Alqahtani, N.M.; Chaturvedi, M.; Gurumurthy, V.; Saini, R.; Bavabeedu, S.S.; Minervini, G. Clinical Trial to Assess Physiology and Activity of Masticatory Muscles of Complete Denture Wearer Following Vitamin D Intervention. Medicina 2023, 59, 410. [Google Scholar] [CrossRef]
- Qazi, N.; Pawar, M.; Padhly, P.P.; Pawar, V.; D’Amico, C.; Nicita, F.; Fiorillo, L.; Alushi, A.; Minervini, G.; Meto, A. Teledentistry: Evaluation of Instagram Posts Related to Bruxism. Technol. Health Care 2023, 31, 1923–1934. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; Franco, R.; Marrapodi, M.M.; Ronsivalle, V.; Shapira, I.; Cicciù, M. Prevalence of Temporomandibular Disorders in Subjects Affected by Parkinson Disease: A Systematic Review and Metanalysis. J. Oral Rehabil. 2023, 50, 1535–1543. [Google Scholar] [CrossRef] [PubMed]
- Crescente, G.; Minervini, G.; Spagnuolo, C.; Moccia, S. Cannabis Bioactive Compound-Based Formulations: New Perspectives for the Management of Orofacial Pain. Molecules 2022, 28, 106. [Google Scholar] [CrossRef]
- Minervini, G.; Lucchese, A.; Perillo, L.; Serpico, R.; Minervini, G. Unilateral Superior Condylar Neck Fracture with Dislocation in a Child Treated with an Acrylic Splint in the Upper Arch for Functional Repositioning of the Mandible. CRANIO® 2017, 35, 337–341. [Google Scholar] [CrossRef] [PubMed]
- Kohler, M.J.; Thormaehlen, S.; Kennedy, J.D.; Pamula, Y.; van den Heuvel, C.J.; Lushington, K.; Martin, A.J. Differences in the Association Between Obesity and Obstructive Sleep Apnea Among Children and Adolescents. J. Clin. Sleep Med. JCSM Off. Publ. Am. Acad. Sleep Med. 2009, 5, 506–511. [Google Scholar] [CrossRef]
- Xanthopoulos, M.S.; Gallagher, P.R.; Berkowitz, R.I.; Radcliffe, J.; Bradford, R.; Marcus, C.L. Neurobehavioral Functioning in Adolescents With and Without Obesity and Obstructive Sleep Apnea. Sleep 2015, 38, 401–410. [Google Scholar] [CrossRef] [PubMed]
- Hull, J.; Aniapravan, R.; Chan, E.; Chatwin, M.; Forton, J.; Gallagher, J.; Gibson, N.; Gordon, J.; Hughes, I.; McCulloch, R.; et al. British Thoracic Society Guideline for Respiratory Management of Children with Neuromuscular Weakness. Thorax 2012, 67 (Suppl. S1), i1–i40. [Google Scholar] [CrossRef] [PubMed]
- Gozal, D. Sleep, Sleep Disorders and Inflammation in Children. Sleep Med. 2009, 10 (Suppl. S1), S12–S16. [Google Scholar] [CrossRef] [PubMed]
- Horwood, L.; Brouillette, R.T.; McGregor, C.D.; Manoukian, J.J.; Constantin, E. Testing for Pediatric Obstructive Sleep Apnea When Health Care Resources Are Rationed. JAMA Otolaryngol.—Head Neck Surg. 2014, 140, 616–623. [Google Scholar] [CrossRef] [PubMed]
- Kaditis, A.; Kheirandish-Gozal, L.; Gozal, D. Pediatric OSAS: Oximetry Can Provide Answers When Polysomnography Is Not Available. Sleep Med. Rev. 2016, 27, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Nixon, G.M.; Kermack, A.S.; Davis, G.M.; Manoukian, J.J.; Brown, K.A.; Brouillette, R.T. Planning Adenotonsillectomy in Children with Obstructive Sleep Apnea: The Role of Overnight Oximetry. Pediatrics 2004, 113, e19–e25. [Google Scholar] [CrossRef]
- Crincoli, V.; Anelli, M.G.; Quercia, E.; Piancino, M.G.; Di Comite, M. Temporomandibular Disorders and Oral Features in Early Rheumatoid Arthritis Patients: An Observational Study. Int. J. Med. Sci. 2019, 16, 253–263. [Google Scholar] [CrossRef]
- Tan, H.-L.; Gozal, D.; Ramirez, H.M.; Bandla, H.P.R.; Kheirandish-Gozal, L. Overnight Polysomnography versus Respiratory Polygraphy in the Diagnosis of Pediatric Obstructive Sleep Apnea. Sleep 2014, 37, 255–260. [Google Scholar] [CrossRef]
- Inchingolo, A.M.; Patano, A.; De Santis, M.; Del Vecchio, G.; Ferrante, L.; Morolla, R.; Pezzolla, C.; Sardano, R.; Dongiovanni, L.; Inchingolo, F.; et al. Comparison of Different Types of Palatal Expanders: Scoping Review. Children 2023, 10, 1258. [Google Scholar] [CrossRef]
- Cantore, S.; Ballini, A.; Farronato, D.; Malcangi, G.; Dipalma, G.; Assandri, F.; Garagiola, U.; Inchingolo, F.; De Vito, D.; Cirulli, N. Evaluation of an Oral Appliance in Patients with Mild to Moderate Obstructive Sleep Apnea Syndrome Intolerant to Continuous Positive Airway Pressure Use: Preliminary Results. Int. J. Immunopathol. Pharmacol. 2016, 29, 267–273. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Malcangi, G.; Semjonova, A.; Inchingolo, A.M.; Patano, A.; Coloccia, G.; Ceci, S.; Marinelli, G.; Di Pede, C.; Ciocia, A.M.; et al. Oralbiotica/Oralbiotics: The Impact of Oral Microbiota on Dental Health and Demineralization: A Systematic Review of the Literature. Children 2022, 9, 1014. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Inchingolo, A.M.; Marinelli, G.; Malcangi, G.; Montenegro, V.; Laudadio, C.; Palmieri, G.; et al. Genetic Pattern, Orthodontic and Surgical Management of Multiple Supplementary Impacted Teeth in a Rare, Cleidocranial Dysplasia Patient: A Case Report. Medicina 2021, 57, 1350. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, F.; Hazballa, D.; Inchingolo, A.D.; Malcangi, G.; Marinelli, G.; Mancini, A.; Maggiore, M.E.; Bordea, I.R.; Scarano, A.; Farronato, M.; et al. Innovative Concepts and Recent Breakthrough for Engineered Graft and Constructs for Bone Regeneration: A Literature Systematic Review. Materials 2022, 15, 1120. [Google Scholar] [CrossRef]
- Rapone, B.; Ferrara, E.; Santacroce, L.; Topi, S.; Gnoni, A.; Dipalma, G.; Mancini, A.; Di Domenico, M.; Tartaglia, G.M.; Scarano, A.; et al. The Gaseous Ozone Therapy as a Promising Antiseptic Adjuvant of Periodontal Treatment: A Randomized Controlled Clinical Trial. Int. J. Environ. Res. Public Health 2022, 19, 985. [Google Scholar] [CrossRef]
- Dohan Ehrenfest, D.M.; Del Corso, M.; Inchingolo, F.; Sammartino, G.; Charrier, J.-B. Platelet-Rich Plasma (PRP) and Platelet-Rich Fibrin (PRF) in Human Cell Cultures: Growth Factor Release and Contradictory Results. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2010, 110, 418–421. [Google Scholar] [CrossRef] [PubMed]
- Vanek, J.; Prasko, J.; Genzor, S.; Ociskova, M.; Kantor, K.; Holubova, M.; Slepecky, M.; Nesnidal, V.; Kolek, A.; Sova, M. Obstructive sleep apnea, depression and cognitive impairment. Sleep Med. 2020, 72, 50–58. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Ceci, S.; Patano, A.; Inchingolo, A.M.; Montenegro, V.; Di Pede, C.; Malcangi, G.; Marinelli, G.; Coloccia, G.; Garibaldi, M.; et al. Elastodontic Therapy of Hyperdivergent Class II Patients Using AMCOP® Devices: A Retrospective Study. Appl. Sci. 2022, 12, 3259. [Google Scholar] [CrossRef]
- Ballini, A.; Dipalma, G.; Isacco, C.G.; Boccellino, M.; Di Domenico, M.; Santacroce, L.; Nguyễn, K.C.D.; Scacco, S.; Calvani, M.; Boddi, A.; et al. Oral Microbiota and Immune System Crosstalk: A Translational Research. Biology 2020, 9, 131. [Google Scholar] [CrossRef]
- Minervini, G.; Franco, R.; Marrapodi, M.M.; Di Blasio, M.; Ronsivalle, V.; Cicciù, M. Children Oral Health and Parents Education Status: A Cross Sectional Study. BMC Oral Health 2023, 23, 787. [Google Scholar] [CrossRef]
- Alonso-Álvarez, M.L.; Terán-Santos, J.; Ordax Carbajo, E.; Cordero-Guevara, J.A.; Navazo-Egüia, A.I.; Kheirandish-Gozal, L.; Gozal, D. Reliability of Home Respiratory Polygraphy for the Diagnosis of Sleep Apnea in Children. Chest 2015, 147, 1020–1028. [Google Scholar] [CrossRef]
- Carroll, J.L. Obstructive Sleep-Disordered Breathing in Children: New Controversies, New Directions. Clin. Chest Med. 2003, 24, 261–282. [Google Scholar] [CrossRef] [PubMed]
- Crincoli, V.; Ballini, A.; Fatone, L.; Di Bisceglie, M.B.; Nardi, G.M.; Grassi, F.R. Cytokine Genotype Distribution in Patients with Periodontal Disease and Rheumatoid Arthritis or Diabetes Mellitus. J. Biol. Regul. Homeost. Agents 2016, 30, 863–866. [Google Scholar] [PubMed]
- Goldoni, R.; Dolci, C.; Boccalari, E.; Inchingolo, F.; Paghi, A.; Strambini, L.; Galimberti, D.; Tartaglia, G.M. Salivary Biomarkers of Neurodegenerative and Demyelinating Diseases and Biosensors for Their Detection. Ageing Res. Rev. 2022, 76, 101587. [Google Scholar] [CrossRef] [PubMed]
- Isacco, C.G.; Ballini, A.; De Vito, D.; Nguyen, K.C.D.; Cantore, S.; Bottalico, L.; Quagliuolo, L.; Boccellino, M.; Di Domenico, M.; Santacroce, L.; et al. Rebalancing the Oral Microbiota as an Efficient Tool in Endocrine, Metabolic and Immune Disorders. Endocr Metab. Immune Disord Drug Targets 2021, 21, 777–784. [Google Scholar] [CrossRef] [PubMed]
- Massa, F.; Gonsalez, S.; Laverty, A.; Wallis, C.; Lane, R. The Use of Nasal Continuous Positive Airway Pressure to Treat Obstructive Sleep Apnoea. Arch. Dis. Child. 2002, 87, 438–443. [Google Scholar] [CrossRef] [PubMed]
- Kushida, C.A.; Chediak, A.; Berry, R.B.; Brown, L.K.; Gozal, D.; Iber, C.; Parthasarathy, S.; Quan, S.F.; Rowley, J.A. Clinical Guidelines for the Manual Titration of Positive Airway Pressure in Patients with Obstructive Sleep Apnea. J. Clin. Sleep Med. Off. Publ. Am. Acad. Sleep Med. 2008, 4, 157–171. [Google Scholar]
- Brouillette, R.T.; Manoukian, J.J.; Ducharme, F.M.; Oudjhane, K.; Earle, L.G.; Ladan, S.; Morielli, A. Efficacy of Fluticasone Nasal Spray for Pediatric Obstructive Sleep Apnea. J. Pediatr. 2001, 138, 838–844. [Google Scholar] [CrossRef] [PubMed]
- Alexopoulos, E.I.; Kaditis, A.G.; Kalampouka, E.; Kostadima, E.; Angelopoulos, N.V.; Mikraki, V.; Skenteris, N.; Gourgoulianis, K. Nasal Corticosteroids for Children with Snoring. Pediatr. Pulmonol. 2004, 38, 161–167. [Google Scholar] [CrossRef]
- Kheirandish-Gozal, L.; Gozal, D. Intranasal Budesonide Treatment for Children with Mild Obstructive Sleep Apnea Syndrome. Pediatrics 2008, 122, e149–e155. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; Franco, R.; Marrapodi, M.M.; Fiorillo, L.; Cervino, G.; Cicciù, M. Economic Inequalities and Temporomandibular Disorders: A Systematic Review with Meta-Analysis. J. Oral Rehabil. 2023, 50, 715–723. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, A.M.; Ceci, S.; Coloccia, G.; Azzollini, D.; Malcangi, G.; Mancini, A.; Inchingolo, F.; Trerotoli, P.; Dipalma, G.; Patano, A. Predictability and Effectiveness of Nuvola® Aligners in Dentoalveolar Transverse Changes: A Retrospective Study. Biomedicines 2023, 11, 1366. [Google Scholar] [CrossRef] [PubMed]
- Ballini, A.; Cantore, S.; Signorini, L.; Saini, R.; Scacco, S.; Gnoni, A.; Inchingolo, A.D.; De Vito, D.; Santacroce, L.; Inchingolo, F.; et al. Efficacy of Sea Salt-Based Mouthwash and Xylitol in Improving Oral Hygiene among Adolescent Population: A Pilot Study. Int. J. Environ. Res. Public Health 2021, 18, 44. [Google Scholar] [CrossRef] [PubMed]
- Goldbart, A.D.; Goldman, J.L.; Veling, M.C.; Gozal, D. Leukotriene Modifier Therapy for Mild Sleep-Disordered Breathing in Children. Am. J. Respir. Crit. Care Med. 2005, 172, 364–370. [Google Scholar] [CrossRef]
- Kheirandish, L.; Goldbart, A.D.; Gozal, D. Intranasal Steroids and Oral Leukotriene Modifier Therapy in Residual Sleep-Disordered Breathing after Tonsillectomy and Adenoidectomy in Children. Pediatrics 2006, 117, e61–e66. [Google Scholar] [CrossRef] [PubMed]
- Farronato, M.; Farronato, D.; Giannì, A.B.; Inchingolo, F.; Nucci, L.; Tartaglia, G.M.; Maspero, C. Effects on Muscular Activity after Surgically Assisted Rapid Palatal Expansion: A Prospective Observational Study. Bioengineering 2022, 9, 361. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; D’Amico, C.; Cicciù, M.; Fiorillo, L. Temporomandibular Joint Disk Displacement: Etiology, Diagnosis, Imaging, and Therapeutic Approaches. J. Craniofacial Surg. 2023, 34, 1115–1121. [Google Scholar] [CrossRef]
- Minervini, G.; Mariani, P.; Fiorillo, L.; Cervino, G.; Cicciù, M.; Laino, L. Prevalence of Temporomandibular Disorders in People with Multiple Sclerosis: A Systematic Review and Meta-Analysis. Cranio J. Craniomandib. Pract. 2022, 1–9. [Google Scholar] [CrossRef]
- Di Stasio, D.; Lauritano, D.; Romano, A.; Salerno, C.; Minervini, G.; Minervini, G.; Gentile, E.; Serpico, R.; Lucchese, A. In Vivo Characterization of Oral Pemphigus Vulgaris by Optical Coherence Tomography. J. Biol. Regul. Homeost. Agents 2015, 29, 39–41. [Google Scholar]
- Kheirandish-Gozal, L.; Bhattacharjee, R.; Bandla, H.P.R.; Gozal, D. Antiinflammatory Therapy Outcomes for Mild OSA in Children. Chest 2014, 146, 88–95. [Google Scholar] [CrossRef]
- Di Venere, D.; Laforgia, A.; Azzollini, D.; Barile, G.; De Giacomo, A.; Inchingolo, A.D.; Rapone, B.; Capodiferro, S.; Kazakova, R.; Corsalini, M. Calcification of the Atlanto-Occipital Ligament (Ponticulus Posticus) in Orthodontic Patients: A Retrospective Study. Healthcare 2022, 10, 1234. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Ferrara, I.; Viapiano, F.; Netti, A.; Campanelli, M.; Buongiorno, S.; Latini, G.; Carpentiere, V.; Ciocia, A.M.; Ceci, S.; et al. Rapid Maxillary Expansion on the Adolescent Patient: Systematic Review and Case Report. Children 2022, 9, 1046. [Google Scholar] [CrossRef]
- Kheirandish-Gozal, L.; Bandla, H.P.R.; Gozal, D. Montelukast for Children with Obstructive Sleep Apnea: Results of a Double-Blind, Randomized, Placebo-Controlled Trial. Ann. Am. Thorac. Soc. 2016, 13, 1736–1741. [Google Scholar] [CrossRef]
- Coloccia, G.; Inchingolo, A.D.; Inchingolo, A.M.; Malcangi, G.; Montenegro, V.; Patano, A.; Marinelli, G.; Laudadio, C.; Limongelli, L.; Di Venere, D.; et al. Effectiveness of Dental and Maxillary Transverse Changes in Tooth-Borne, Bone-Borne, and Hybrid Palatal Expansion through Cone-Beam Tomography: A Systematic Review of the Literature. Medicina 2021, 57, 288. [Google Scholar] [CrossRef]
- Adina, S.; Dipalma, G.; Bordea, I.R.; Lucaciu, O.; Feurdean, C.; Inchingolo, A.D.; Septimiu, R.; Malcangi, G.; Cantore, S.; Martin, D.; et al. Orthopedic Joint Stability Influences Growth and Maxillary Development: Clinical Aspects. J. Biol. Regul. Homeost. Agents 2020, 34, 747–756. [Google Scholar] [CrossRef] [PubMed]
- Ballini, A.; Cantore, S.; Altini, C.; Dipalma, G.; Ferrari, C.; Niccoli Asabella, A.; Rubini, G.; Inchingolo, F. 99mTc-Diphosphonates Bone Scintigraphy for Vitality Evaluation in Cleft Palate. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 8497–8501. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, F.; Derla, C.; Pacifici, A.; Cagiano, R.; Gargari, M.; Marrelli, M.; Amantea, M.; Inchingolo, A.M.; Dipalma, G.; Signorini, L.; et al. Dental and Maxillofacial Alterations in Patients Affected from Odontochondrodysplasia: A Rare Case Report and Review of Literature. Oral Health Dent. Manag. 2014, 13, 614–618. [Google Scholar] [PubMed]
- Kiaee, B.; Nucci, L.; Sarkarat, F.; Talaeipour, A.R.; Eslami, S.; Amiri, F.; Jamilian, A. Three-Dimensional Assessment of Airway Volumes in Patients with Unilateral Cleft Lip and Palate. Prog. Orthod. 2021, 22, 35. [Google Scholar] [CrossRef] [PubMed]
- Michalsky, M.; Reichard, K.; Inge, T.; Pratt, J.; Lenders, C. American Society for Metabolic and Bariatric Surgery ASMBS Pediatric Committee Best Practice Guidelines. Surg. Obes. Relat. Dis. Off. J. Am. Soc. Bariatr. Surg. 2012, 8, 1–7. [Google Scholar] [CrossRef]
- Fagundes, N.C.F.; Minervini, G.; Furio Alonso, B.; Nucci, L.; Grassia, V.; d’Apuzzo, F.; Puigdollers, A.; Perillo, L.; Flores-Mir, C. Patient-reported outcomes while managing obstructive sleep apnea with oral appliances: A scoping review. J. Evid.-Based Dent. Pract. 2023, 23, 101786. [Google Scholar] [CrossRef]
- Lo Giudice, A.; Quinzi, V.; Ronsivalle, V.; Farronato, M.; Nicotra, C.; Indelicato, F.; Isola, G. Evaluation of Imaging Software Accuracy for 3-Dimensional Analysis of the Mandibular Condyle. A Comparative Study Using a Surface-to-Surface Matching Technique. Int. J. Environ. Res. Public Health 2020, 17, 4789. [Google Scholar] [CrossRef]
- Daniele, V.; Macera, L.; Taglieri, G.; Di Giambattista, A.; Spagnoli, G.; Massaria, A.; Messori, M.; Quagliarini, E.; Chiappini, G.; Campanella, V.; et al. Thermoplastic Disks Used for Commercial Orthodontic Aligners: Complete Physicochemical and Mechanical Characterization. Materials 2020, 13, 2386. [Google Scholar] [CrossRef]
- Mummolo, S.; Nota, A.; Albani, F.; Marchetti, E.; Gatto, R.; Marzo, G.; Quinzi, V.; Tecco, S. Salivary Levels of Streptococcus Mutans and Lactobacilli and Other Salivary Indices in Patients Wearing Clear Aligners versus Fixed Orthodontic Appliances: An Observational Study. PLoS ONE 2020, 15, e0228798. [Google Scholar] [CrossRef]
- Saccomanno, S.; Quinzi, V.; Sarhan, S.; Laganà, D.; Marzo, G. Perspectives of Tele-Orthodontics in the COVID-19 Emergency and as a Future Tool in Daily Practice. Eur. J. Paediatr. Dent. 2020, 21, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; Franco, R.; Marrapodi, M.M.; Fiorillo, L.; Cervino, G.; Cicciù, M. The Association between Parent Education Level, Oral Health, and Oral-Related Sleep Disturbance. An Observational Crosssectional Study. Eur. J. Paediatr. Dent. 2023, 24, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Lo Giudice, A.; Quinzi, V.; Ronsivalle, V.; Martina, S.; Bennici, O.; Isola, G. Description of a Digital Work-Flow for CBCT-Guided Construction of Micro-Implant Supported Maxillary Skeletal Expander. Materials 2020, 13, 1815. [Google Scholar] [CrossRef] [PubMed]
- Rosa, M.; Quinzi, V.; Marzo, G. Paediatric Orthodontics Part 1: Anterior Open Bite in the Mixed Dentition. Eur. J. Paediatr. Dent. 2019, 1, 80–82. [Google Scholar]
- Marchetti, E.; Tecco, S.; Caterini, E.; Casalena, F.; Quinzi, V.; Mattei, A.; Marzo, G. Alcohol-Free Essential Oils Containing Mouthrinse Efficacy on Three-Day Supragingival Plaque Regrowth: A Randomized Crossover Clinical Trial. Trials 2017, 18, 154. [Google Scholar] [CrossRef] [PubMed]
- Kawakami, S.; Shiota, M.; Kon, K.; Shimogishi, M.; Iijima, H.; Kasugai, S. Autologous Micrografts from the Palatal Mucosa for Bone Regeneration in Calvarial Defects in Rats: A Radiological and Histological Analysis. Int. J. Implant. Dent. 2021, 7, 6. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Malcangi, G.; Inchingolo, A.M.; Piras, F.; Settanni, V.; Garofoli, G.; Palmieri, G.; Ceci, S.; Patano, A.; De Leonardis, N.; et al. Benefits and Implications of Resveratrol Supplementation on Microbiota Modulations: A Systematic Review of the Literature. Int. J. Mol. Sci. 2022, 23, 4027. [Google Scholar] [CrossRef] [PubMed]
- Malcangi, G.; Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Garibaldi, M.; Inchingolo, A.M.; Piras, F.; Cardarelli, F.; Settanni, V.; et al. Impacted Central Incisors in the Upper Jaw in an Adolescent Patient: Orthodontic-Surgical Treatment—A Case Report. Appl. Sci. 2022, 12, 2657. [Google Scholar] [CrossRef]
- Langaliya, A.; Alam, M.K.; Hegde, U.; Panakaje, M.S.; Cervino, G.; Minervini, G. Occurrence of Temporomandibular Disorders among Patients Undergoing Treatment for Obstructive Sleep Apnoea Syndrome (OSAS) Using Mandibular Advancement Device (MAD): A Systematic Review Conducted According to PRISMA Guidelines and the Cochrane Handbook for Systematic Reviews of Interventions. J. Oral Rehabil. 2023, 50, 1554–1563. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; Nucci, L.; Lanza, A.; Femiano, F.; Contaldo, M.; Grassia, V. Temporomandibular Disc Displacement with Reduction Treated with Anterior Repositioning Splint: A 2-Year Clinical and Magnetic Resonance Imaging (MRI) Follow-Up. J. Biol. Regul. Homeost. Agents 2020, 34, 151–160. [Google Scholar] [PubMed]
- Marchetti, E.; Casalena, F.; Capestro, A.; Tecco, S.; Mattei, A.; Marzo, G. Efficacy of Two Mouthwashes on 3-day Supragingival Plaque Regrowth: A Randomized Crossover Clinical Trial. Int. J. Dent. Hyg. 2017, 15, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Quinzi, V.; Panetta, G.; Filippi, P.; Rizzo, F.A.; Mancini, L.; Mummolo, S. Autotransplatation of Immature Third Molars as Substitutes for Congenitally Missing Second Premolars: An Alternative Solution in a Young Patient with Oligodontia. J. Biol. Regul. Homeost. Agents 2020, 34 (Suppl. S1), 155–163. [Google Scholar] [PubMed]
- Dinoi, M.T.; Marchetti, E.; Garagiola, U.; Caruso, S.; Mummolo, S.; Marzo, G. Orthodontic Treatment of an Unerupted Mandibular Canine Tooth in a Patient with Mixed Dentition: A Case Report. J. Med. Case Reports 2016, 10, 170. [Google Scholar] [CrossRef] [PubMed]
- Mummolo, S.; Nota, A.; Marchetti, E.; Padricelli, G.; Marzo, G. The 3D Tele Motion Tracking for the Orthodontic Facial Analysis. BioMed Res. Int. 2016, 2016, 4932136. [Google Scholar] [CrossRef]
- Quinzi, V.; Saccomanno, S.; Manenti, R.J.; Giancaspro, S.; Coceani Paskay, L.; Marzo, G. Efficacy of Rapid Maxillary Expansion with or without Previous Adenotonsillectomy for Pediatric Obstructive Sleep Apnea Syndrome Based on Polysomnographic Data: A Systematic Review and Meta-Analysis. Appl. Sci. 2020, 10, 6485. [Google Scholar] [CrossRef]
- Pasini, M.; Giuca, M.R.; Ligori, S.; Mummolo, S.; Fiasca, F.; Marzo, G.; Quinzi, V. Association between Anatomical Variations and Maxillary Canine Impaction: A Retrospective Study in Orthodontics. Appl. Sci. 2020, 10, 5638. [Google Scholar] [CrossRef]
- Caruso, S.; Lisciotto, E.; Caruso, S.; Marino, A.; Fiasca, F.; Buttarazzi, M.; Sarzi Amadè, D.; Evangelisti, M.; Mattei, A.; Gatto, R. Effects of Rapid Maxillary Expander and Delaire Mask Treatment on Airway Sagittal Dimensions in Pediatric Patients Affected by Class III Malocclusion and Obstructive Sleep Apnea Syndrome. Life 2023, 13, 673. [Google Scholar] [CrossRef]
- Yoon, A.; Abdelwahab, M.; Bockow, R.; Vakili, A.; Lovell, K.; Chang, I.; Ganguly, R.; Liu, S.Y.-C.; Kushida, C.; Hong, C. Impact of Rapid Palatal Expansion on the Size of Adenoids and Tonsils in Children. Sleep Med. 2022, 92, 96–102. [Google Scholar] [CrossRef]
- Pirelli, P.; Saponara, M.; Guilleminault, C. Rapid Maxillary Expansion (RME) for Pediatric Obstructive Sleep Apnea: A 12-Year Follow-Up. Sleep Med. 2015, 16, 933–935. [Google Scholar] [CrossRef] [PubMed]
- Villa, M.P.; Rizzoli, A.; Rabasco, J.; Vitelli, O.; Pietropaoli, N.; Cecili, M.; Marino, A.; Malagola, C. Rapid Maxillary Expansion Outcomes in Treatment of Obstructive Sleep Apnea in Children. Sleep Med. 2015, 16, 709–716. [Google Scholar] [CrossRef]
- Pirelli, P.; Fanucci, E.; Giancotti, A.; Di Girolamo, M.; Guilleminault, C. Skeletal Changes after Rapid Maxillary Expansion in Children with Obstructive Sleep Apnea Evaluated by Low-Dose Multi-Slice Computed Tomography. Sleep Med. 2019, 60, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Pirelli, P.; Fiaschetti, V.; Fanucci, E.; Giancotti, A.; Condo’, R.; Saccomanno, S.; Mampieri, G. Cone Beam CT Evaluation of Skeletal and Nasomaxillary Complex Volume Changes after Rapid Maxillary Expansion in OSA Children. Sleep Med. 2021, 86, 81–89. [Google Scholar] [CrossRef]
- Kim, J.E.; Hwang, K.J.; Kim, S.W.; Liu, S.Y.C.; Kim, S.J. Correlation between Craniofacial Changes and Respiratory Improvement after Nasomaxillary Skeletal Expansion in Pediatric Obstructive Sleep Apnea Patients. Sleep Breath. 2022, 26, 585–594. [Google Scholar] [CrossRef]
- Li, K.; Iwasaki, T.; Quo, S.; Li, C.; Young, K.; Leary, E.; Guilleminault, C. Persistent Pediatric Obstructive Sleep Apnea Treated with Skeletally Anchored Transpalatal Distraction. L’Orthodontie Fr. 2022, 93, 47–60. [Google Scholar] [CrossRef]
- Chuang, L.-C.; Hwang, Y.-J.; Lian, Y.-C.; Hervy-Auboiron, M.; Pirelli, P.; Huang, Y.-S.; Guilleminault, C. Changes in Craniofacial and Airway Morphology as Well as Quality of Life after Passive Myofunctional Therapy in Children with Obstructive Sleep Apnea: A Comparative Cohort Study. Sleep Breath. Schlaf Atm. 2019, 23, 1359–1369. [Google Scholar] [CrossRef]
- Ghodke, S.; Utreja, A.K.; Singh, S.P.; Jena, A.K. Effects of Twin-Block Appliance on the Anatomy of Pharyngeal Airway Passage (PAP) in Class II Malocclusion Subjects. Prog. Orthod. 2014, 15, 68. [Google Scholar] [CrossRef]
- Keerthana, P.; Negi, G.; Chitra, P. Airway Changes in Patients with Sleep Apnea Using AdvanSync2 Class II Correctors—A Case Series. Med. Pharm. Rep. 2022, 95, 337–347. [Google Scholar] [CrossRef]
- Machado-Júnior, A.-J.; Signorelli, L.-G.; Zancanella, E.; Crespo, A.-N. Randomized Controlled Study of a Mandibular Advancement Appliance for the Treatment of Obstructive Sleep Apnea in Children: A Pilot Study. Med. Oral Patol. Oral Cir. Bucal 2016, 21, e403–e407. [Google Scholar] [CrossRef]
- Concepción Medina, C.; Ueda, H.; Iwai, K.; Kunimatsu, R.; Tanimoto, K. Changes in Airway Patency and Sleep-Breathing in Healthy Skeletal Class II Children Undergoing Functional Activator Therapy. Eur. Oral Res. 2022, 56, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; He, H.; Ngan, P. Effects of Twin Block Appliance on Obstructive Sleep Apnea in Children: A Preliminary Study. Sleep Breath. 2013, 17, 1309–1314. [Google Scholar] [CrossRef] [PubMed]
- Zhao, T.; Ngan, P.; Hua, F.; Zheng, J.; Zhou, S.; Zhang, M.; Xiong, H.; He, H. Impact of Pediatric Obstructive Sleep Apnea on the Development of Class II Hyperdivergent Patients Receiving Orthodontic Treatment: A Pilot Study. Angle Orthod. 2018, 88, 560–566. [Google Scholar] [CrossRef] [PubMed]
- Zreaqat, M.; Hassan, R.; Samsudin, A.; Alforaidi, S. Effects of Twin-Block Appliance on Upper Airway Parameters in OSA Children with Class II Malocclusion and Mandibular Retrognathia: A CBCT Study. Eur. J. Pediatr. 2023, 182, 5501–5510. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Lowe, A.A. Updates in Oral Appliance Therapy for Snoring and Obstructive Sleep Apnea. Sleep Breath. Schlaf Atm. 2013, 17, 473–486. [Google Scholar] [CrossRef]
- D’Apuzzo, F.; Nucci, L.; Delfino, I.; Portaccio, M.; Minervini, G.; Isola, G.; Serino, I.; Camerlingo, C.; Lepore, M. Application of Vibrational Spectroscopies in the Qualitative Analysis of Gingival Crevicular Fluid and Periodontal Ligament during Orthodontic Tooth Movement. J. Clin. Med. 2021, 10, 1405. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; Franco, R.; Marrapodi, M.M.; Fiorillo, L.; Cervino, G.; Cicciù, M. Prevalence of Temporomandibular Disorders in Children and Adolescents Evaluated with Diagnostic Criteria for Temporomandibular Disorders: A Systematic Review with Meta-analysis. J. Oral Rehabil. 2023, 50, 522–530. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; Franco, R.; Marrapodi, M.M.; Crimi, S.; Badnjević, A.; Cervino, G.; Bianchi, A.; Cicciù, M. Correlation between Temporomandibular Disorders (TMD) and Posture Evaluated Trough the Diagnostic Criteria for Temporomandibular Disorders (DC/TMD): A Systematic Review with Meta-Analysis. J. Clin. Med. 2023, 12, 2652. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diseases with a Craniofacial Component | Associations with Soft Tissues | Neuromuscular Associations | Inflammatory Associations |
|---|---|---|---|
| Apert’s syndrome | Obesity | Cerebral palsy | Asthma |
| Crouzon’s syndrome | Cystic hygroma | Hypothyroidism | Metabolic syndrome |
| Pfeiffer’s syndrome | Papillomatosis (oroparingea) | Achondroplasia | Sickle cell disease |
| Pierre–Robin syndrome | Prader–Willi syndrome | Patients with cleft palate after repair | |
| Treacher Collins syndrome | Mucopolysaccharidosis | Down syndrome | |
| Goldenhar syndrome (hemifacial microsomy) | Beckwith–Wiedernann’s syndrome | ||
| Atresia/coanal stenosis | Down syndrome | ||
| Hallermann–Streiff’s syndrome | Syndromes with cleft | ||
| Klippel–Feil syndrome | |||
| Osteopetrosis | |||
| Sickle cell anemia (sickle cell disease) | |||
| Syndromes with cleft |
| Night Symptoms | Daytime Speaker | Signs |
|---|---|---|
| Snoring | Difficulty awakening | Tonsil hypertrophy |
| Gasping | Lack of rest upon waking | High/wide lingual position |
| Noisy breathing (typically inspiratory) | Drowsiness | Growth disorders (obesity, insufficient growth) |
| Respiration paradox | Hyperactivity | Pulmonary hypertension |
| Indentations (jugular or rib) | Aggression, bad mood | Systemic hypertension |
| Apnee testifies | Oral respiration | Craniofacial abnormalities |
| Restless sleep | Meager appetite | Laryngeal |
| Hyperextension of the neck | Dysphagia | Obstruction of the nasal airways |
| Oral respiration | School difficulties | Hypotonia |
| Night sweating | Daytime speaker | Gastroesophageal reflux |
| Metabolic | Neurocognitive | Cardiovascular |
|---|---|---|
| Increased C-reactive protein | Decreased quality of life | Autonomic dysfunction |
| Insulin resistance | Aggressive behavior | Systemic hypertension |
| Hypercholesterolemia | Poor school performance | Absence of drop in blood pressure in sleep |
| Increased transaminases | Depression | Left ventricular dysfunction |
| Reduced insulin-like growth factor | Attention deficit | Pulmonary hypertension |
| Reduced/altered growth hormone secretion | Hyperactivity | Variability of heart rate altered |
| Moodiness | Increased vascular endothelial growth factor |
| Authors (Year) | Type of Study | Aim of the Study | Materials | Results |
|---|---|---|---|---|
| Caruso et al., 2023 [82] | Clinical study | To evaluate the cephalometric variations in upper airway dimensions and OSA-related clinical conditions after orthodontic treatment with an RME and the Delaire mask in patients affected by class III malocclusion. | In total, 14 children, ages 6 to 10, with mixed dentition were treated with a Delaire mask and an RME. | The study reports an increase in nasopharyngeal and oropharyngeal spaces. Improvements in OSAS-related clinical conditions and airway patency result from this increase. |
| Yoon et al., 2022 [83] | Retrospective cohort study | To assess the alterations in palatine and adenoid tonsil sizes subsequent to RPE through 3D volumetric analysis of cone beam computed tomography (CBCT) images. | In total, 60 pediatric patients with tonsillar hypertrophy were divided into 2 groups: one treated with RPE and a control group without any treatment. | RPE enormously decreased the size of the palatine and adenoid tonsils. |
| Pirelli et al., 2015 [84] | Clinical prospective study | To assess the long-term effectiveness of rapid maxillary expansion (RME) in a group of children with obstructive sleep apnea (OSA); RPE was found to significantly reduce the size of both the palatine and adenoid tonsils. | The study Ided 31 children with an OSA diagnosis. At baseline, these children had isolated maxillary narrowing and no enlarged adenotonsils. The subjects experienced repeated polysomnography (PSG) in their late teens or early 20s, as well as ongoing clinical evaluation. | Following RME treatment for a history of OSA, a subgroup of OSA children with isolated maxillary narrowing (initially followed up into adulthood) showed stable, long-term results. |
| Villa et al., 2015 [85] | Clinical retrospective study | To validate the effectiveness of RPE in children with mild to moderate adenotonsillar hypertrophy. | Pediatric patients with narrow palate, tonsillar hypertrophy, and OSA undergoing RPE therapy and reassessed over time. | RPE therapy was confirmed to be effective in resolving malocclusions associated with OSA. |
| Pirelli et al., 2019 [86] | Clinical prospective study | To evaluate the skeletal effects of RPE via low-dose computed tomography (CT). | In total, 14 pediatric patients with contracted palate and OSA underwent RPE therapy. | Opening of the mid-palatal suture was demonstrated in all cases. |
| Pirelli et al., 2021 [87] | Clinical study | To evaluate skeletal changes and changes in dimensions and volume of the upper airways before and after rapid RPE in children with OSA via CBCT. To evaluate if RPE therapy can improve both the patency of the nasal airways and the obstructive sleep apnea syndrome (OSAS). | In total, 19 pediatric patients with contracted palate and OSA underwent RPE therapy. | In all cases, the opening of the mid-palatal suture was demonstrated. Significant increases were observed in nasal osseous width, nasal cavity volume, total upper airway volume, and the nasopharynx and oropharynx. |
| Kim et al., 2022 [88] | Clinical study | To assess changes in respiratory function related to increased upper airway volume in patients with OSA treated with RPE. | In total, 26 patients (mean age, 13.6 years) were treated with RPE. Pre- and post-treatment CBCT assessment of airway and pre- and post-treatment assessment of mean apnea-hypopnea index (AHI). | In all cases, there was an increase in the size of the nasomaxillary complex, with improvement in parameters related to OSA. |
| Li et al., 2022 [89] | Clinical study | To evaluate the efficacy of nasomaxillary expansion via trans-palatal distraction (TPD) with skeletal anchorage in the resolution of OSA. | In total, 25 children without maxillary contraction with OSA were treated with TPD. | In children treated with RPE previously but without transverse maxillary deficiency, nasomaxillary expansion via skeletally anchored TPD improved OSA. |
| Chuang et al., 2019 [90] | Comparative cohort study | To compare the quality of life and the morphology of the airways, and cranium both before and after a year of passive myofunctional treatment (MFT) in children with OSA. | For a year, forty OSA youngsters who wore an oral device every night (the treatment group) and seventeen who did not (the control group) were monitored. | One year of passive MFT enhanced nasal breathing during sleep, as well as mandibular development and upper airway morphology in the oropharyngeal area. |
| Ghodke et al., 2014 [91] | Clinical study | To assess how class II malocclusion participants with retrognathic mandibles respond to a twin block device in terms of pharyngeal airway passage dimensions and posterior pharyngeal wall thickness. | Thirty-eight class II malocclusion individuals with mandibular retrusion, ages 8 to 14 | The twin block device enhanced PAP dimensions while maintaining posterior pharyngeal wall thickness prior to treatment. |
| Keerthana et al., 2022 [92] | Case series | To summarize the results of using the AdvanSync2 Class II corrector in the treatment of three orthodontic patients who complained of breathing issues and a retrognathic mandible that interfered with their ability to sleep. | Three people who require treatment for class II malocclusion were linked to sleep apnea. | By increasing airway dimensions, the AdvanSync2 Class II corrector, when used in conjunction with fixed orthodontic equipment, improved the quality of life for class II patients. |
| Machado-Júnior et al., 2016 [93] | Pilot study | To assess mandibular advancement appliance in children who have OSA. | Adolescents diagnosed as apneic were those with an apnea–hypopnea index of one or more events per hour. | One year following the implementation of mandibular advancement devices, there was a reduction in the apnea–hypopnea index as compared with the non-user group. |
| Medina et al., 2022 [94] | Clinical study | To ascertain if using this equipment causes healthy children’s upper airways to enlarge and their sleep-breathing habits to improve. | In total, 39 healthy children: 20 for the activator group; 19 for the control group. | By opening the upper airway, the activator helps to enhance the quality of breathing during sleep. |
| Zhang et al., 2013 [95] | Clinical study | To look at how twin block (TB) appliances affect children who have mandibular retrognathia and OSA. | In total, 46 children (aged 9.7 ± 1.5 years, BMI: 18.1 ± 1.04 kg/m2) with mandibular retrognathia and OSA. | The patients’ facial profiles improved following therapy with the TB appliance. |
| Zhao et al., 2015 [96] | Pilot Study | To find out if class II hyperdivergent individuals undergoing complete orthodontic treatment are affected differently by the existence of OSA. | Patients who underwent orthodontic treatment and were between the ages of 12 and 14. | The results of these children’s orthodontic treatments may be impacted by the early detection and treatment of pediatric OSA. |
| Zreaqat et al., 2023 [97] | CBCT study | To assess rapid maxillary expansion (RME)’s long-term effectiveness in treating a group of children with obstructive sleep apnea (OSA). | In this study, 31 children with OSA diagnoses were included. At baseline, these children did not have enlarged adenotonsils and only had isolated maxillary constriction. The subjects experienced repeat polysomnography (PSG) in their late teens or early 20s, as well as ongoing clinical reevaluation. | Following RME therapy for juvenile OSA, a subgroup of children with isolated maxillary constriction who were first followed up into adulthood showed consistent, long-term improvements. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferati, K.; Bexheti-Ferati, A.; Palermo, A.; Pezzolla, C.; Trilli, I.; Sardano, R.; Latini, G.; Inchingolo, A.D.; Inchingolo, A.M.; Malcangi, G.; et al. Diagnosis and Orthodontic Treatment of Obstructive Sleep Apnea Syndrome Children—A Systematic Review. Diagnostics 2024, 14, 289. https://doi.org/10.3390/diagnostics14030289
Ferati K, Bexheti-Ferati A, Palermo A, Pezzolla C, Trilli I, Sardano R, Latini G, Inchingolo AD, Inchingolo AM, Malcangi G, et al. Diagnosis and Orthodontic Treatment of Obstructive Sleep Apnea Syndrome Children—A Systematic Review. Diagnostics. 2024; 14(3):289. https://doi.org/10.3390/diagnostics14030289
Chicago/Turabian StyleFerati, Kenan, Arberesha Bexheti-Ferati, Andrea Palermo, Carmen Pezzolla, Irma Trilli, Roberta Sardano, Giulia Latini, Alessio Danilo Inchingolo, Angelo Michele Inchingolo, Giuseppina Malcangi, and et al. 2024. "Diagnosis and Orthodontic Treatment of Obstructive Sleep Apnea Syndrome Children—A Systematic Review" Diagnostics 14, no. 3: 289. https://doi.org/10.3390/diagnostics14030289