
Diagnostic Accuracy of PET with 18F-Fluciclovine ([18F]FACBC) in Detecting High-Grade Gliomas: A Systematic Review and Meta-Analysis
 , , ,
, , ,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol
2.2. Literature Search Strategy and Information Sources
2.3. Eligibility Criteria
2.4. Study Selection
2.5. Data Collection Process and Data Extraction
2.6. Quality Assessment
2.7. Statistical Analysis and Diagnostic Accuracy Measures
3. Results
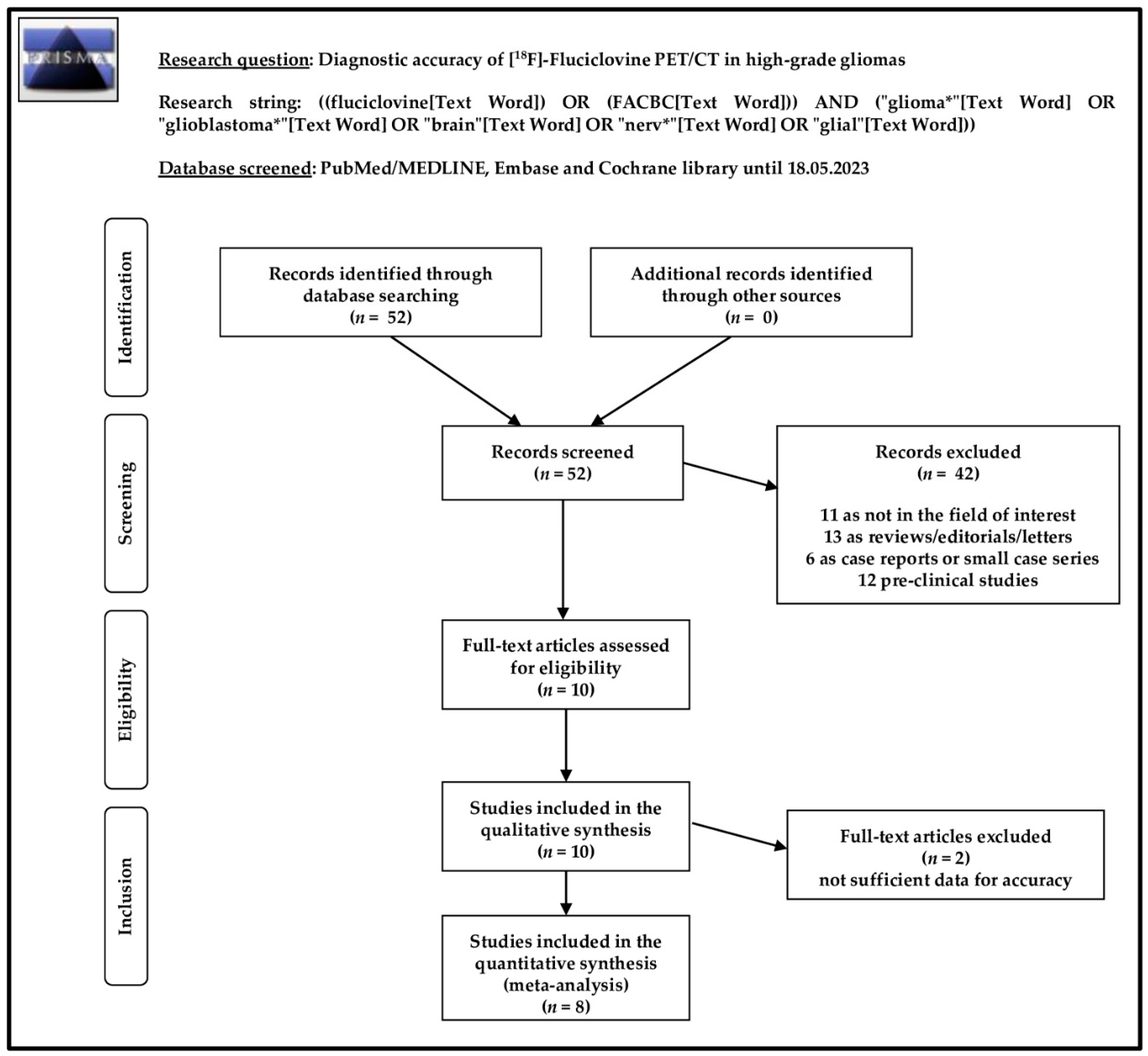
3.1. Literature Search and Study Selection
3.2. Study Characteristics
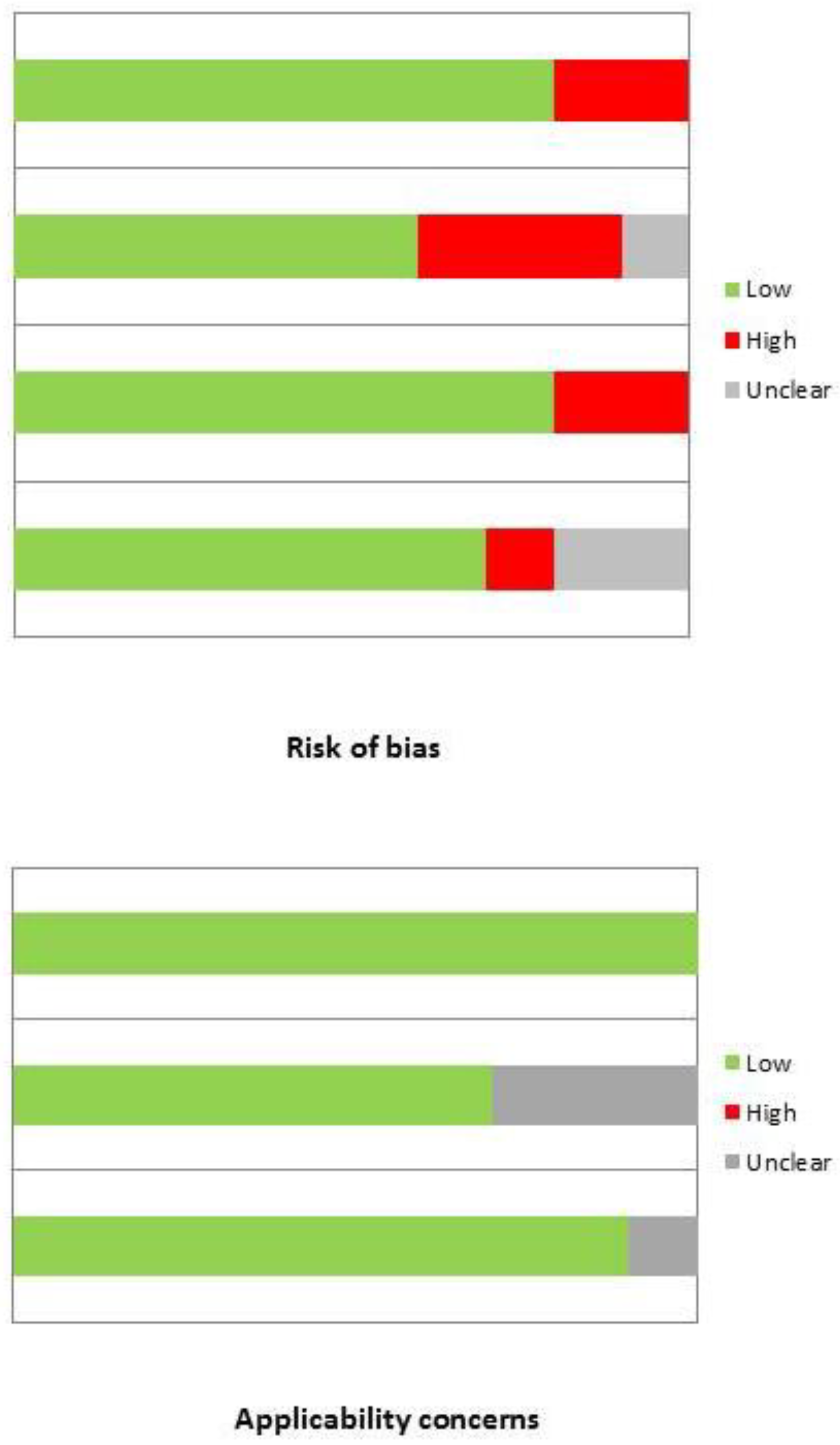
3.3. Risk of Bias and Applicability
3.4. Results of Qualitative Analysis
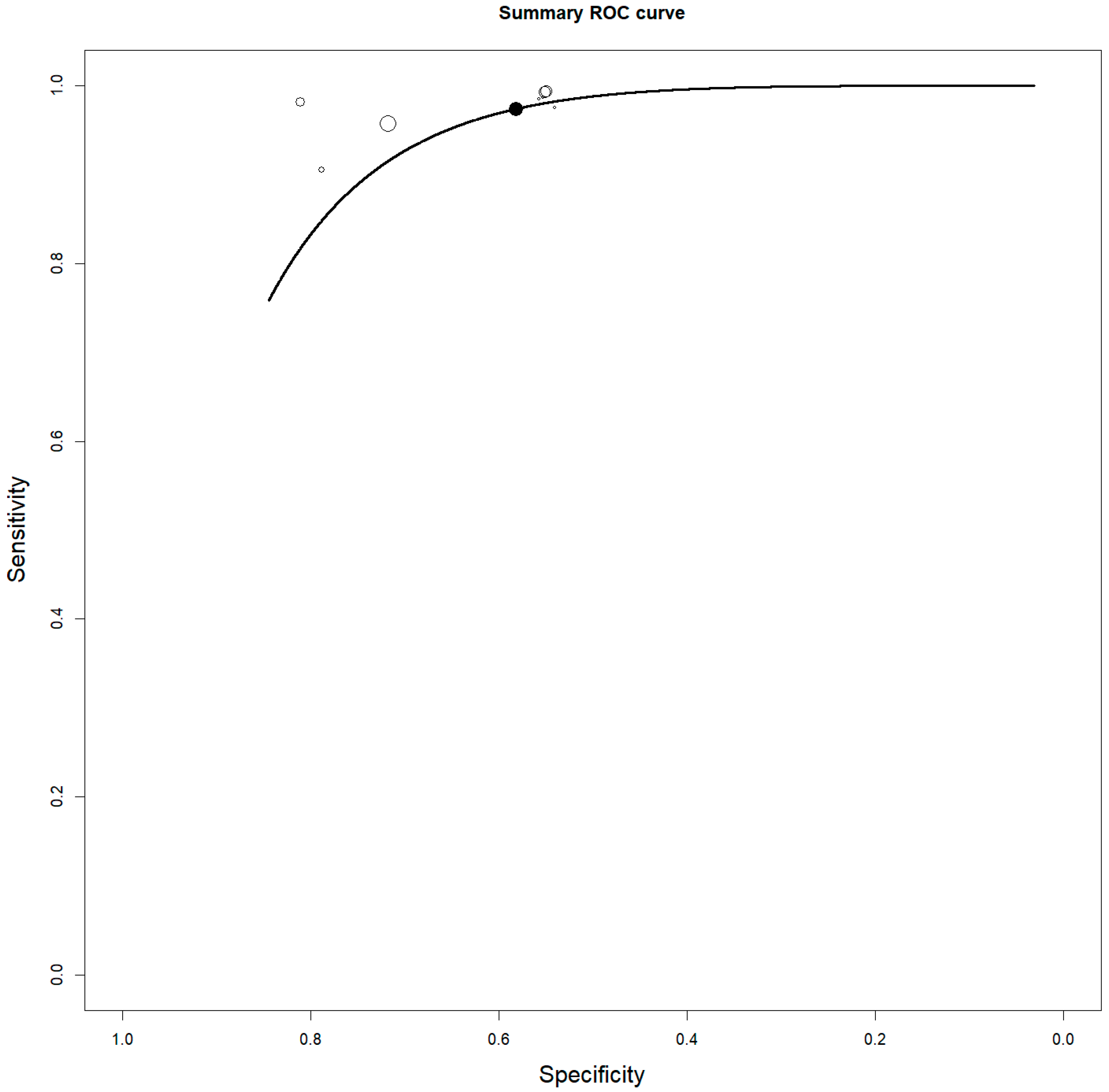
3.5. Quantitative Analysis: Meta-Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Francis, S.S.; Ostrom, Q.T.; Cote, D.J.; Smith, T.R.; Claus, E.; Barnholtz-Sloan, J.S. The Epidemiology of Central Nervous System Tumors. Hematol. Oncol. Clin. 2022, 36, 23–42. [Google Scholar] [CrossRef] [PubMed]
- Komori, T. Grading of adult diffuse gliomas according to the 2021 WHO Classification of Tumors of the Central Nervous System. Lab. Investig. 2022, 102, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Xue, C.; Ke, X.; Zhou, J. Treatment Response and Prognosis Evaluation in High-Grade Glioma: An Imaging Review Based on MRI. J. Magn. Reason. Imaging 2022, 56, 325–340. [Google Scholar] [CrossRef] [PubMed]
- Upadhyay, N.; Waldman, A.D. Conventional MRI evaluation of gliomas. Br. J. Radiol. 2011, 84, S107–S111. [Google Scholar] [CrossRef] [PubMed]
- Shooli, H.; Nemati, R.; Ahmadzadehfar, H.; Aboian, M.; Jafari, E.; Jokar, N.; Nabipour, I.; Dadgar, H.; Gholamrezanezhad, A.; Larvie, M.; et al. Theranostics in Brain Tumors. PET Clin. 2021, 16, 397–418. [Google Scholar] [CrossRef]
- Law, I.; Albert, N.L.; Arbizu, J.; Boellaard, R.; Drzezga, A.; Galldiks, N.; la Fougère, C.; Langen, K.J.; Lopci, E.; Lowe, V.; et al. Joint EANM/EANO/RANO practice guidelines/SNMMI procedure standards for imaging of gliomas using PET with radiolabelled amino acids and [18F]FDG: Version 1. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 540–557. [Google Scholar] [CrossRef]
- Piccardo, A.; Albert, N.L.; Borgwardt, L.; Fahey, F.H.; Hargrave, D.; Galldiks, N.; Jehanno, N.; Kurch, L.; Law, I.; Lim, R.; et al. Joint EANM/SIOPE/RAPNO practice guidelines/SNMMI procedure standards for imaging of paediatric gliomas using PET with radiolabelled amino acids and [18F]FDG: Version 1. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 3852–3869. [Google Scholar] [CrossRef]
- Treglia, G.; Muoio, B.; Trevisi, G.; Mattoli, M.V.; Albano, D.; Bertagna, F.; Giovanella, L. Diagnostic Performance and Prognostic Value of PET/CT with Different Tracers for Brain Tumors: A Systematic Review of Published Meta-Analyses. Int. J. Mol. Sci. 2019, 20, 4669. [Google Scholar] [CrossRef]
- Castello, A.; Castellani, M.; Florimonte, L.; Ciccariello, G.; Mansi, L.; Lopci, E. PET radiotracers in glioma: A review of clinical indications and evidence. Clin. Transl. Imaging 2022, 10, 535–551. [Google Scholar] [CrossRef]
- Muoio, B.; Albano, D.; Dondi, F.; Bertagna, F.; Garibotto, V.; Kunikowska, J.; Piccardo, A.; Annunziata, S.; Espeli, V.; Migliorini, D.; et al. Diagnostic Accuracy of PET/CT or PET/MRI Using PSMA-Targeting Radiopharmaceuticals in High-Grade Gliomas: A Systematic Review and a Bivariate Meta-Analysis. Diagnostics 2022, 12, 1665. [Google Scholar] [CrossRef] [PubMed]
- Savir-Baruch, B.; Schuster, D.M. Prostate Cancer Imaging with 18F-Fluciclovine. PET Clin. 2022, 17, 607–620. [Google Scholar] [CrossRef] [PubMed]
- Albano, D.; Tomasini, D.; Bonù, M.; Giubbini, R.; Bertagna, F. 18F-Fluciclovine (18F-FACBC) PET/CT or PET/MRI in gliomas/glioblastomas. Ann. Nucl. Med. 2020, 34, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Oka, S.; Hattori, R.; Kurosaki, F.; Toyama, M.; Williams, L.A.; Yu, W.; Votaw, J.R.; Yoshida, Y.; Goodman, M.M.; Ito, O. A preliminary study of anti-1-amino-3-18F-fluorocyclobutyl-1-carboxylic acid for the detection of prostate cancer. J. Nucl. Med. 2007, 48, 46–55. [Google Scholar] [PubMed]
- Shoup, T.M.; Olson, J.; Hoffman, J.M.; Votaw, J.; Eshima, D.; Eshima, L.; Camp, V.M.; Stabin, M.; Votaw, D.; Goodman, M.M. Synthesis and evaluation of [18F]1-amino-3-fluorocyclobutane-1-carboxylic acid to image brain tumors. J. Nucl. Med. 1999, 40, 331–338. [Google Scholar] [PubMed]
- Sadeghi, R.; Treglia, G. Systematic reviews and meta-analyses of diagnostic studies: A practical guideline. Clin. Transl. Imaging 2017, 5, 83–87. [Google Scholar] [CrossRef]
- McInnes, M.D.F.; Moher, D.; Thombs, B.D.; McGrath, T.A.; Bossuyt, P.M.; The PRISMA-DTA Group. Preferred Reporting Items for a Systematic Review and Meta-analysis of Diagnostic Test Accuracy Studies: The PRISMA-DTA Statement. JAMA 2018, 319, 388–396. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M.; QUADAS-2 Group. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Bogsrud, T.V.; Londalen, A.; Brandal, P.; Leske, H.; Panagopoulos, I.; Borghammer, P.; Bach-Gansmo, T. 18F-Fluciclovine PET/CT in Suspected Residual or Recurrent High-Grade Glioma. Clin. Nucl. Med. 2019, 44, 605–611. [Google Scholar] [CrossRef]
- Fatania, K.; Frood, R.; Tyyger, M.; McDermott, G.; Fernandez, S.; Shaw, G.C.; Boissinot, M.; Salvatore, D.; Ottobrini, L.; Teh, I.; et al. Exploratory Analysis of Serial 18F-fluciclovine PET-CT and Multiparametric MRI during Chemoradiation for Glioblastoma. Cancers 2022, 14, 3485. [Google Scholar] [CrossRef]
- Karlberg, A.; Berntsen, E.M.; Johansen, H.; Skjulsvik, A.J.; Reinertsen, I.; Dai, H.Y.; Xiao, Y.; Rivaz, H.; Borghammer, P.; Solheim, O.; et al. 18F-FACBC PET/MRI in Diagnostic Assessment and Neurosurgery of Gliomas. Clin. Nucl. Med. 2019, 44, 550–559. [Google Scholar] [CrossRef]
- Kondo, A.; Ishii, H.; Aoki, S.; Suzuki, M.; Nagasawa, H.; Kubota, K.; Minamimoto, R.; Arakawa, A.; Tominaga, M.; Arai, H. Phase IIa clinical study of [18F]fluciclovine: Efficacy and safety of a new PET tracer for brain tumors. Ann. Nucl. Med. 2016, 30, 608–618. [Google Scholar] [CrossRef] [PubMed]
- Michaud, L.; Beattie, B.J.; Akhurst, T.; Dunphy, M.; Zanzonico, P.; Finn, R.; Mauguen, A.; Schöder, H.; Weber, W.A.; Lassman, A.B.; et al. 18F-Fluciclovine (18F-FACBC) PET imaging of recurrent brain tumors. Eur. J. Nucl. Med. Mol. Imaging 2019, 47, 1353–1367. [Google Scholar] [CrossRef] [PubMed]
- Nabavizadeh, A.; Bagley, S.J.; Doot, R.K.; Ware, J.B.; Young, A.J.; Ghodasara, S.; Zhao, C.; Anderson, H.; Schubert, E.; Carpenter, E.L.; et al. Distinguishing Progression from Pseudoprogression in Glioblastoma Using 18F-Fluciclovine PET. J. Nucl. Med. 2023, 64, 852–858. [Google Scholar] [CrossRef] [PubMed]
- Parent, E.E.; Benayoun, M.; Ibeanu, I.; Olson, J.J.; Hadjipanayis, C.G.; Brat, D.J.; Adhikarla, V.; Nye, J.; Schuster, D.M.; Goodman, M.M. [18F]Fluciclovine PET discrimination between high- and low-grade gliomas. EJNMMI Res. 2018, 8, 67. [Google Scholar] [CrossRef] [PubMed]
- Tsuyuguchi, N.; Terakawa, Y.; Uda, T.; Nakajo, K.; Kanemura, Y. Diagnosis of Brain Tumors Using Amino Acid Transport PET Imaging with 18F-fluciclovine: A Comparative Study with L-methyl-11C-methionine PET Imaging. Ocean. J. Nucl. Med. Biol. 2017, 5, 85–94. [Google Scholar]
- Wakabayashi, T.; Iuchi, T.; Tsuyuguchi, N.; Nishikawa, R.; Arakawa, Y.; Sasayama, T.; Miyake, K.; Nariai, T.; Narita, Y.; Hashimoto, N.; et al. Diagnostic Performance and Safety of Positron Emission Tomography Using 18F-Fluciclovine in Patients with Clinically Suspected High- or Low-grade Gliomas: A Multicenter Phase IIb Trial. Ocean. J. Nucl. Med. Biol. 2017, 5, 10–21. [Google Scholar]
- Wakabayashi, T.; Hirose, Y.; Miyake, K.; Arakawa, Y.; Kagawa, N.; Nariai, T.; Narita, Y.; Nishikawa, R.; Tsuyuguchi, N.; Fukami, T.; et al. Determining the extent of tumor resection at surgical planning with 18F-fluciclovine PET/CT in patients with suspected glioma: Multicenter phase III trials. Ann. Nucl. Med. 2021, 35, 1279–1292. [Google Scholar] [CrossRef] [PubMed]
- Biscontini, G.; Romagnolo, C.; Cottignoli, C.; Palucci, A.; Fringuelli, F.M.; Caldarella, C.; Ceci, F.; Burroni, L. 18F-Fluciclovine Positron Emission Tomography in Prostate Cancer: A Systematic Review and Diagnostic Meta-Analysis. Diagnostics 2021, 11, 304. [Google Scholar] [CrossRef]
- Mei, R.; Farolfi, A.; Castellucci, P.; Nanni, C.; Zanoni, L.; Fanti, S. PET/CT Variants and Pitfalls in Prostate Cancer: What You Might See on PET and Should Never Forget. Semin. Nucl. Med. 2021, 51, 621–632. [Google Scholar] [CrossRef]
- Schuster, D.M.; Nanni, C.; Fanti, S.; Oka, S.; Okudaira, H.; Inoue, Y.; Sörensen, J.; Owenius, R.; Choyke, P.; Turkbey, B.; et al. Anti-1-amino-3-18F-fluorocyclobutane-1-carboxylic acid: Physiologic uptake patterns, incidental findings, and variants that may simulate disease. J. Nucl. Med. 2014, 55, 1986–1992. [Google Scholar] [CrossRef]
- Sasajima, T.; Ono, T.; Shimada, N.; Doi, Y.; Oka, S.; Kanagawa, M.; Baden, A.; Mizoi, K. Trans-1-amino-3-18F-fluorocyclobutanecarboxylic acid (anti-18F-FACBC) is a feasible alternative to 11C-methyl-L-methionine and magnetic resonance imaging for monitoring treatment response in gliomas. Nucl. Med. Biol. 2013, 40, 808–815. [Google Scholar] [CrossRef] [PubMed]
- Ono, M.; Oka, S.; Okudaira, H.; Schuster, D.M.; Goodman, M.M.; Kawai, K.; Shirakami, Y. Comparative evaluation of transport mechanisms of trans-1-amino-3-[18F]fluorocyclobutanecarboxylic acid and L-[methyl-11C]methionine in human glioma cell lines. Brain Res. 2013, 1535, 24–37. [Google Scholar] [CrossRef]
- Oka, S.; Okudaira, H.; Ono, M.; Schuster, D.M.; Goodman, M.M.; Kawai, K.; Shirakami, Y. Differences in transport mechanisms of trans-1-amino-3-[18F]fluorocyclobutanecarboxylic acid in inflammation, prostate cancer, and glioma cells: Comparison with L-[methyl-11C]methionine and 2-deoxy-2-[18F]fluoro-D-glucose. Mol. Imaging Biol. 2014, 16, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Ono, T.; Sasajima, T.; Doi, Y.; Oka, S.; Ono, M.; Kanagawa, M.; Baden, A.; Mizoi, K.; Shimizu, H. Amino acid PET tracers are reliable markers of treatment responses to single-agent or combination therapies including temozolomide, interferon-β, and/or bevacizumab for glioblastoma. Nucl. Med. Biol. 2015, 42, 598–607. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Authors [Ref.] | Year | Country | Study Design/N° of Involved Centers | Funding Sources |
|---|---|---|---|---|
| Bogsrud et al. [18] | 2019 | Norway | Retrospective/monocentric | None |
| Fatania et al. [19] | 2022 | UK | Prospective/monocentric | Blue Earth Diagnostics |
| Karlberg et al. [20] | 2019 | Norway | Prospective/monocentric | Norwegian National Advisory Unit for Ultrasound and Image Guided Therapy |
| Kondo et al. [21] | 2016 | Japan | Prospective/bicentric | Nihon Medi-Physics Co., Ltd. |
| Michaud et al. [22] | 2020 | USA | Prospective/monocentric | National Cancer Institute and internal source |
| Nabavizadeh et al. [23] | 2023 | USA | Prospective/monocentric | Blue Earth Diagnostics |
| Parent et al. [24] | 2018 | USA | Prospective/monocentric | National Institutes of Health |
| Tsuguyuchi et al. [25] | 2017 | Japan | Prospective/monocentric | Nihon Medi-Physics Co., Ltd. |
| Wakabayashi et al. [26] | 2017 | Japan | Prospective/multicentric | Nihon Medi-Physics Co., Ltd. |
| Wakabayashi et al. [27] | 2021 | Japan | Prospective/multicentric | Nihon Medi-Physics Co., Ltd. |
| Authors [Ref.] | Sample Size | Mean/Median Age (Years) | Sex M/F | Glioma Grading (II/III/IV) | Clinical Setting | Prior Imaging |
|---|---|---|---|---|---|---|
| Bogsrud et al. [18] | 21 | Mean: 55.8 | 13/8 | 3/1/17 | Suspicious recurrence | MRI |
| Fatania et al. [19] | 6 | Mean: 61 | 4/2 | 0/0/6 | Evaluation during chemotherapy | MRI |
| Karlberg et al. [20] | 11 | Mean: 44 | 7/4 | 4/2/5 | Primary or recurrent HGG vs. LGG | None |
| Kondo et al. [21] | 5 | Median: 51 | 2/3 | 0/0/5 | Initial diagnosis of gliomas | MRI |
| Michaud et al. [22] | 27 | Mean: 51.2 | 18/9 | 9/6/12 | Suspicious recurrence | MRI + MET-PET |
| Nabavizadeh et al. [23] | 30 | Median: 62 | 10/20 | 0/0/30 | Suspicious recurrence | MRI |
| Parent et al. [24] | 16 | Mean: 49.6 | 8/8 | 6/1/9 | HGG vs. LGG | MRI |
| Tsuguyuchi et al. [25] | 6 | Mean: 44.2 | 4/2 | 4/2/1 | Initial diagnosis of gliomas | MRI + MET-PET |
| Wakabayashi et al. [26] | 35 | Mean: 55 | 31/9 | 10/10/5 (8 not reported, 2 no tumor evidence) | HGG vs. LGG | MRI |
| Wakabayashi et al. [27] | 36 | Mean: 54.9 | 31/14 | not reported | Initial diagnosis of gliomas | MRI |
| Authors [Ref.] | Hybrid Imaging | Tomograph | Injected Activity | Time from Injection to Acquisition (min) | PET Analysis |
|---|---|---|---|---|---|
| Bogsrud et al. [18] | PET/CT + fusion with MRI | Biograph mCT (Siemens) | 200–376 MBq | 19 ± 12.6 | Semi-quantitative (SUVmax, SUVmean, L/B) |
| Fatania et al. [19] | PET/CT | Discovery 690 (GE Healthcare) | 185 MBq ± 20% | 30 min dynamic acquisition in list mode (+ reconstruction of a static image of 10 min) | Semi-quantitative 2, 3, 4, x SUVmax PET volumes |
| Karlberg et al. [20] | PET/MRI | Biograph mMR (Siemens) | 235.5 ± 54.4 MBq | 0–45 | Semi-quantitative (SUVmax, SUVpeak, SUVbg, TBRmax, TBRpeak) |
| Kondo et al. [21] | PET/CT | Discovery STE (GE Healthcare) | 185 MBq | 60 min dynamic acquisition | Semi-quantitative (SUVmax, SUVmean, T/N, TAC) |
| Michaud et al. [22] | PET/CT + fusion with MRI | Discovery STE (6 patients), GE Advance (21 patients) (GE Healthcare) | 370 MBq | 45 min dynamic acquisition + delayed 20 min static acquisition 90–240 min post injection | visual and semi-quantitative (Tmax, Tmax/Co_mean, Tmax/Ce_mean, cm3) |
| Nabavizadeh et al. [23] | PET/CT + fusion with MRI | Ingenuity TF (Philips) | 191 ± 21 MBq | 60 min dynamic acquisition | visual and semi-quantitative (SUVmax, SUVpeak, SUVmean, SUVratios, TAC, TTP) |
| Parent et al. [24] | PET + fusion with MRI | High Resolution Research Tomograph (HRRT) (Siemens) | 366–399 MBq | 65 min dynamic acquisition | Semi-quantitative (SUVmax, SUVmean, T/Bmax, T/Bmean, TAC) |
| Tsuguyuchi et al. [25] | PET/CT + fusion with MRI | Biograph 16 (Siemens) | 235.5 ± 35.2 MBq 4 MBq/kg | 19 | Semi-quantitative (SUVmax, SUVmean, LNmax, LNmean) |
| Wakabayashi et al. [26] | PET/CT | Not reported | 186.1 ± 67.0 MBq | 10–20 | Visual |
| Wakabayashi et al. [27] | PET/CT + fusion with MRI | Not reported | 78.3–297.0 MBq | 10–50 | Visual |
| Authors [Ref.] | Reference Standard | TP | FP | TN | FN | Sen | Spe | PPV | NPV | Acc |
|---|---|---|---|---|---|---|---|---|---|---|
| Bogsrud et al. [18] | Histology | 21 | 0 | 0 | 0 | 100% | 100% | NC | NC | 100% |
| Fatania et al. [19] | Clinical/imaging FU | 6 | 0 | 0 | 0 | 100% | 100% | NC | NC | 100% |
| Karlberg et al. [20] | Histology | 6 | 0 | 4 | 1 | 85.7% | 100% | 100% | 80% | 90.9% |
| Kondo et al. [21] | Histology | 5 | 0 | 0 | 0 | 100% | 100% | NC | NC | 100% |
| Michaud et al. [22] | Histology or clinical/imaging FU | 20 | 0 | 0 | 0 | 100% | 100% | NC | NC | 100% |
| Nabavizadeh et al. [23] | Histology | 21 | 1 | 5 | 1 | 95.5% | 83.3% | 95.5% | 83.3% | 92.9% |
| Parent et al. [24] | Histology | 10 | 0 | 6 | 0 | 100% | 100% | 100% | 100% | 100% |
| Tsuguyuchi et al. [25] | Histology | 2 | 2 | 2 | 0 | 100% | 50% | 50% | 100% | 66.7% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castello, A.; Albano, D.; Muoio, B.; Castellani, M.; Panareo, S.; Rizzo, A.; Treglia, G.; Urso, L. Diagnostic Accuracy of PET with 18F-Fluciclovine ([18F]FACBC) in Detecting High-Grade Gliomas: A Systematic Review and Meta-Analysis. Diagnostics 2023, 13, 3610. https://doi.org/10.3390/diagnostics13243610
Castello A, Albano D, Muoio B, Castellani M, Panareo S, Rizzo A, Treglia G, Urso L. Diagnostic Accuracy of PET with 18F-Fluciclovine ([18F]FACBC) in Detecting High-Grade Gliomas: A Systematic Review and Meta-Analysis. Diagnostics. 2023; 13(24):3610. https://doi.org/10.3390/diagnostics13243610
Chicago/Turabian StyleCastello, Angelo, Domenico Albano, Barbara Muoio, Massimo Castellani, Stefano Panareo, Alessio Rizzo, Giorgio Treglia, and Luca Urso. 2023. "Diagnostic Accuracy of PET with 18F-Fluciclovine ([18F]FACBC) in Detecting High-Grade Gliomas: A Systematic Review and Meta-Analysis" Diagnostics 13, no. 24: 3610. https://doi.org/10.3390/diagnostics13243610