
High Prognostic Value of 68Ga-PSMA PET/CT in Renal Cell Carcinoma and Association with PSMA Expression Assessed by Immunohistochemistry
 ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Imaging Protocol
2.2. Pathological Assessment of PSMA Expression
2.3. Statistical Analysis
3. Results
3.1. Immunohistochemistry Patterns
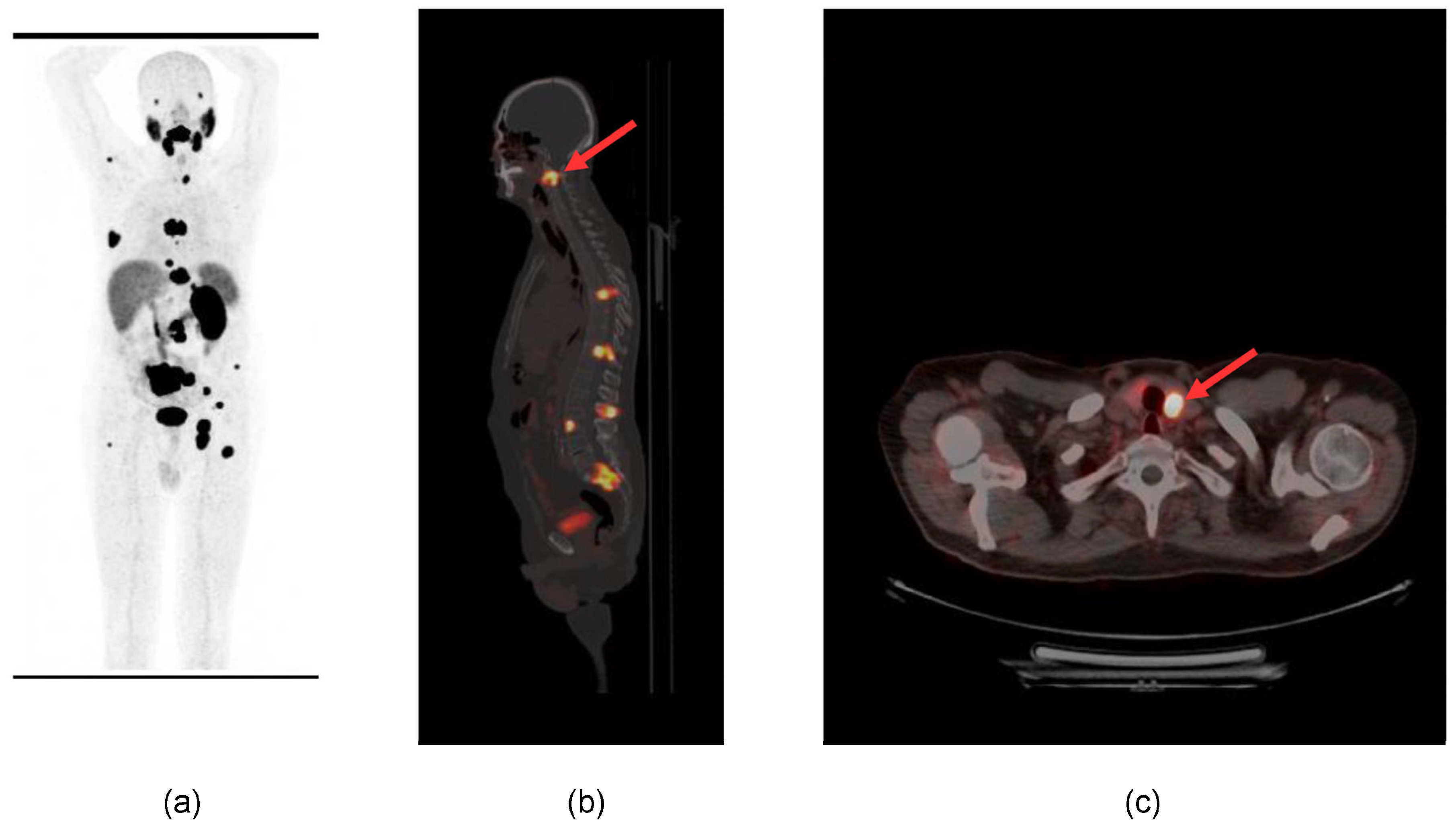
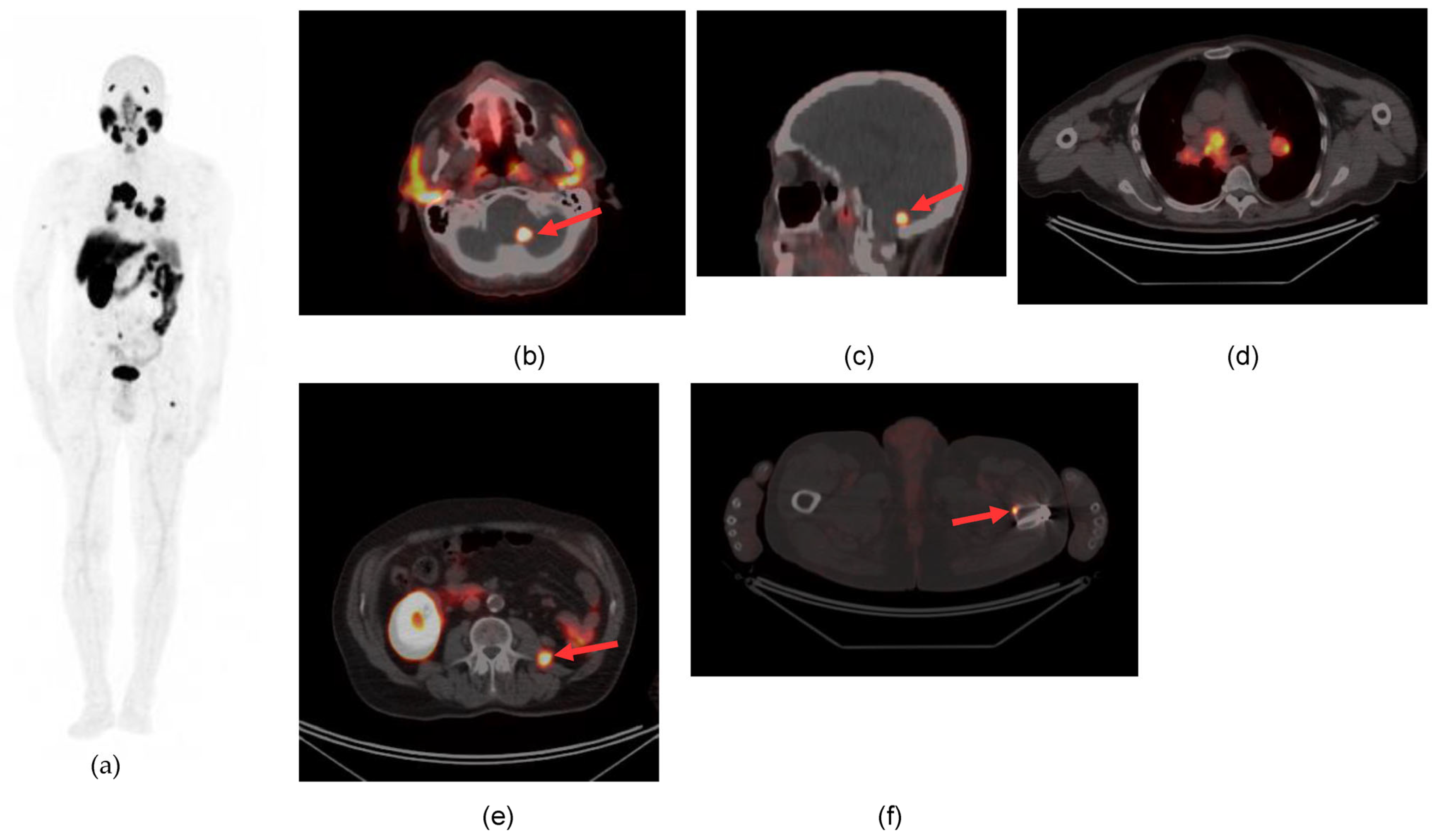
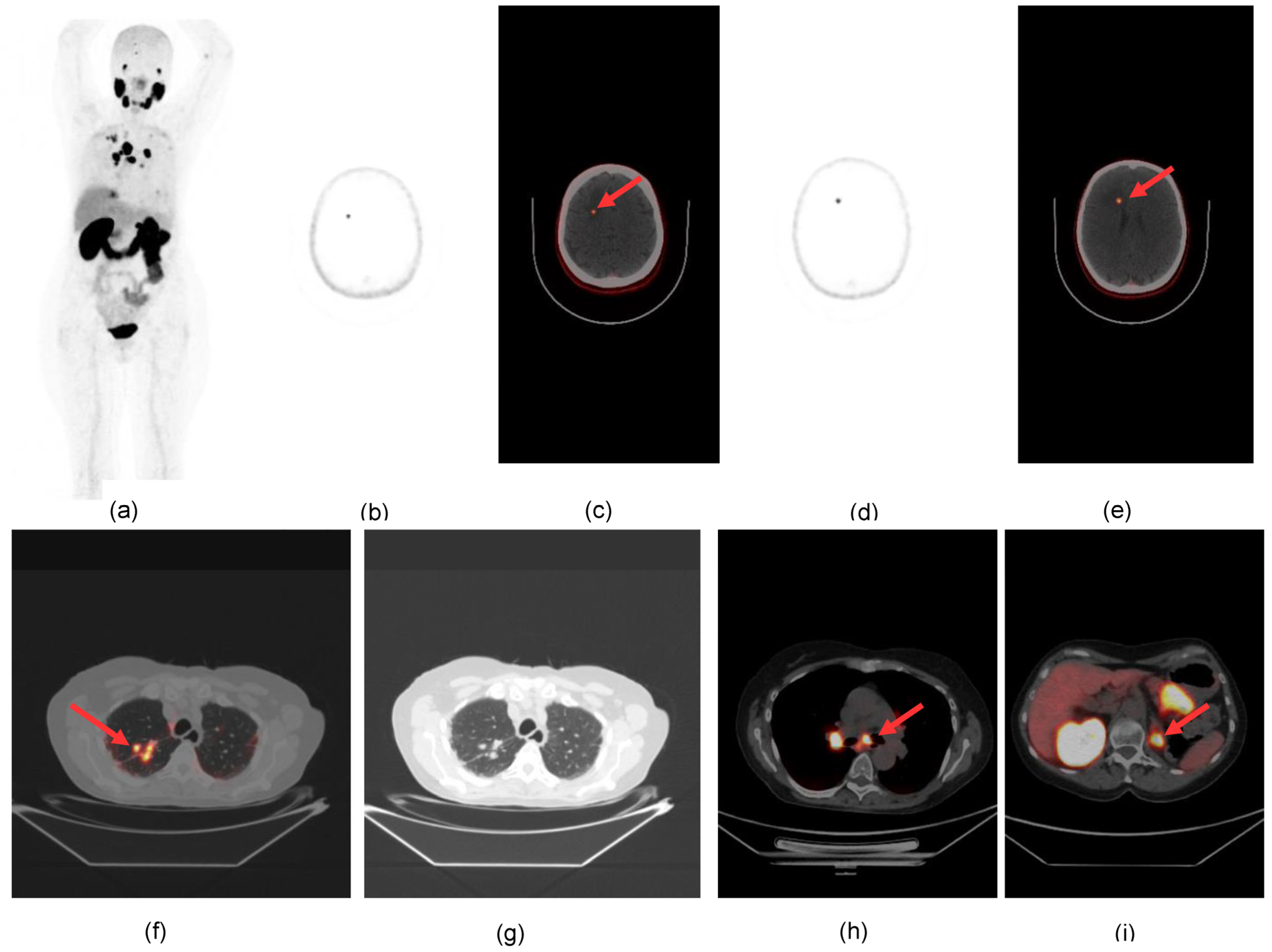
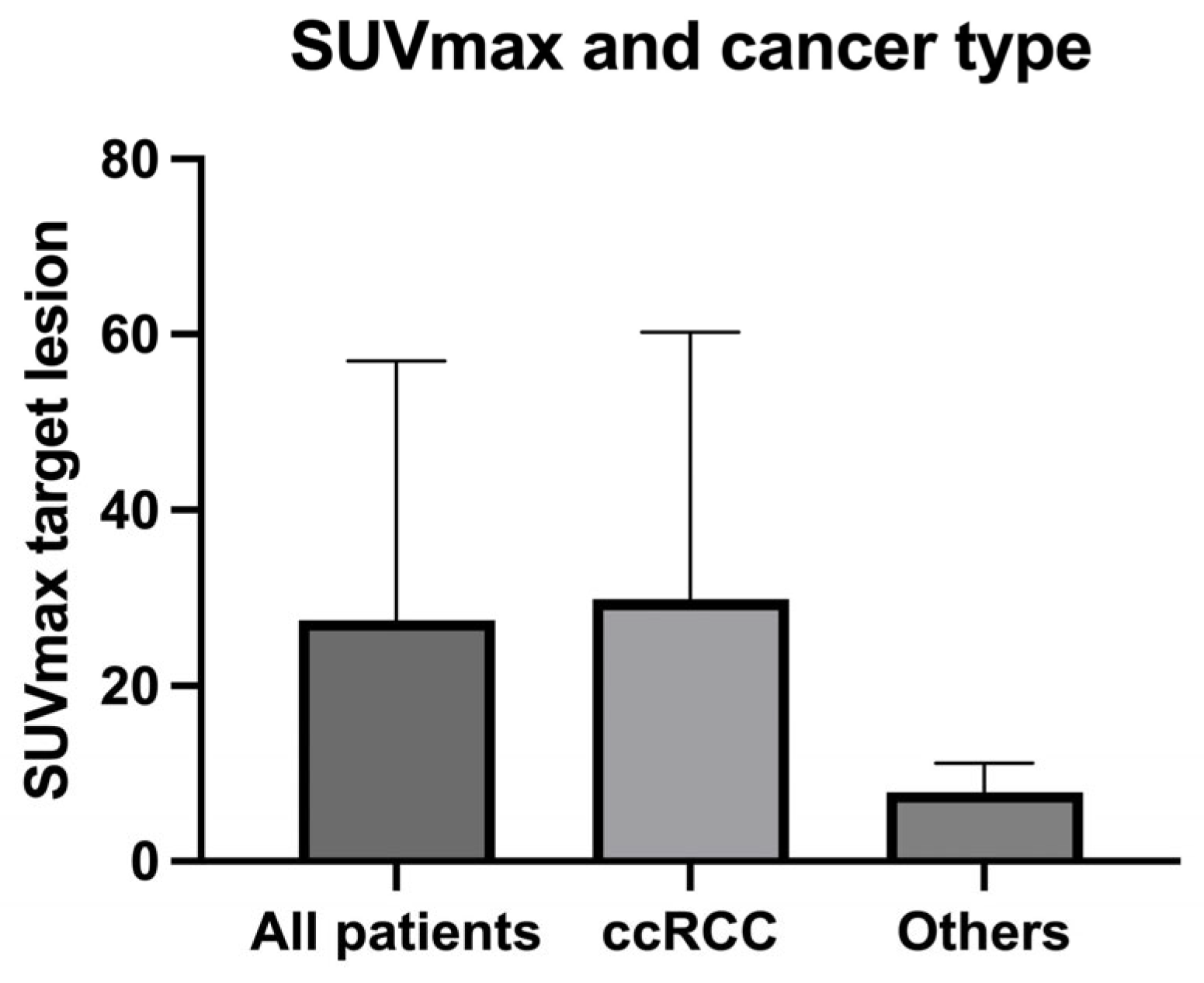
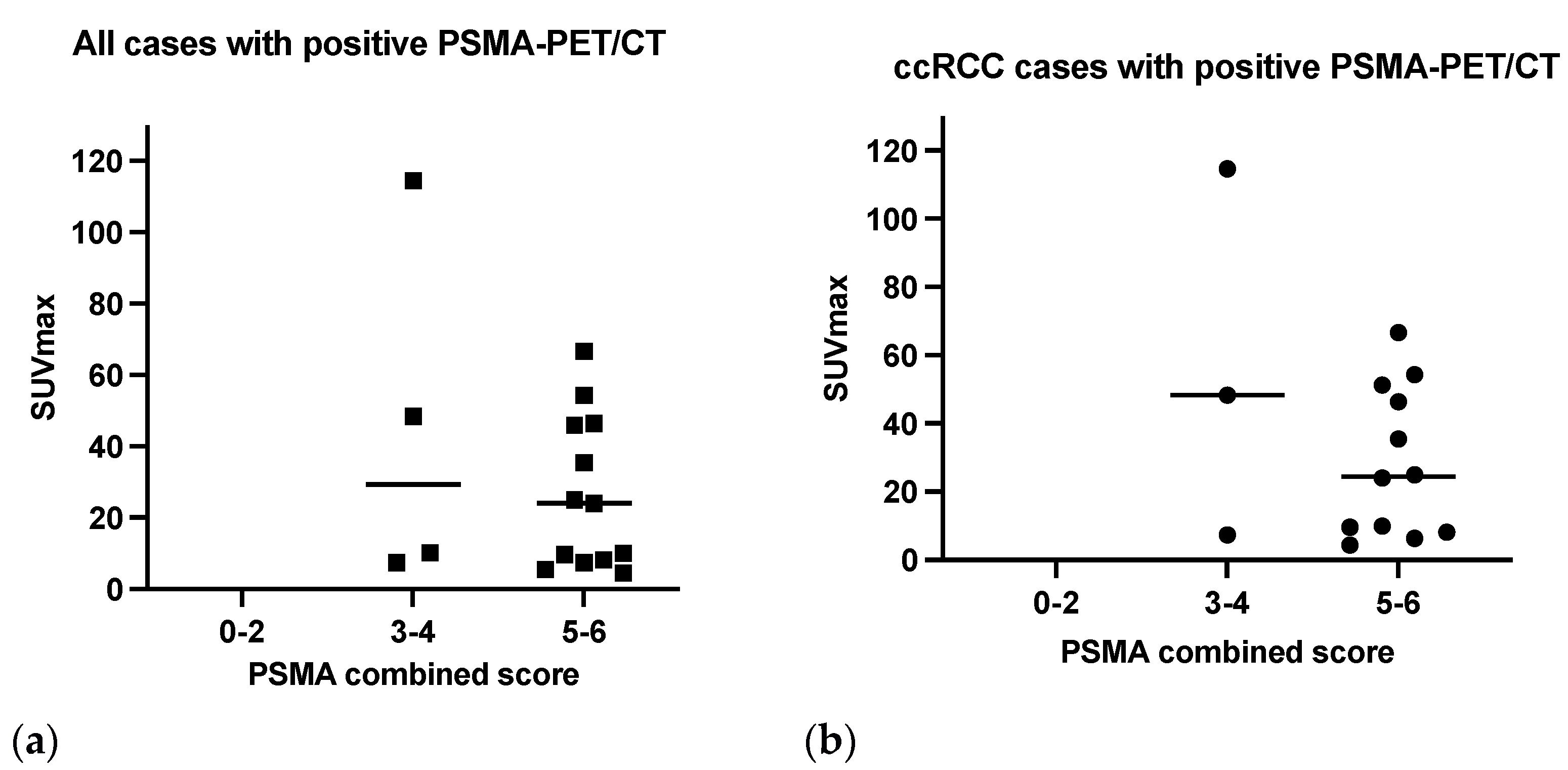
3.2. PSMA-PET Signal
3.3. PET Results and Cancer Type
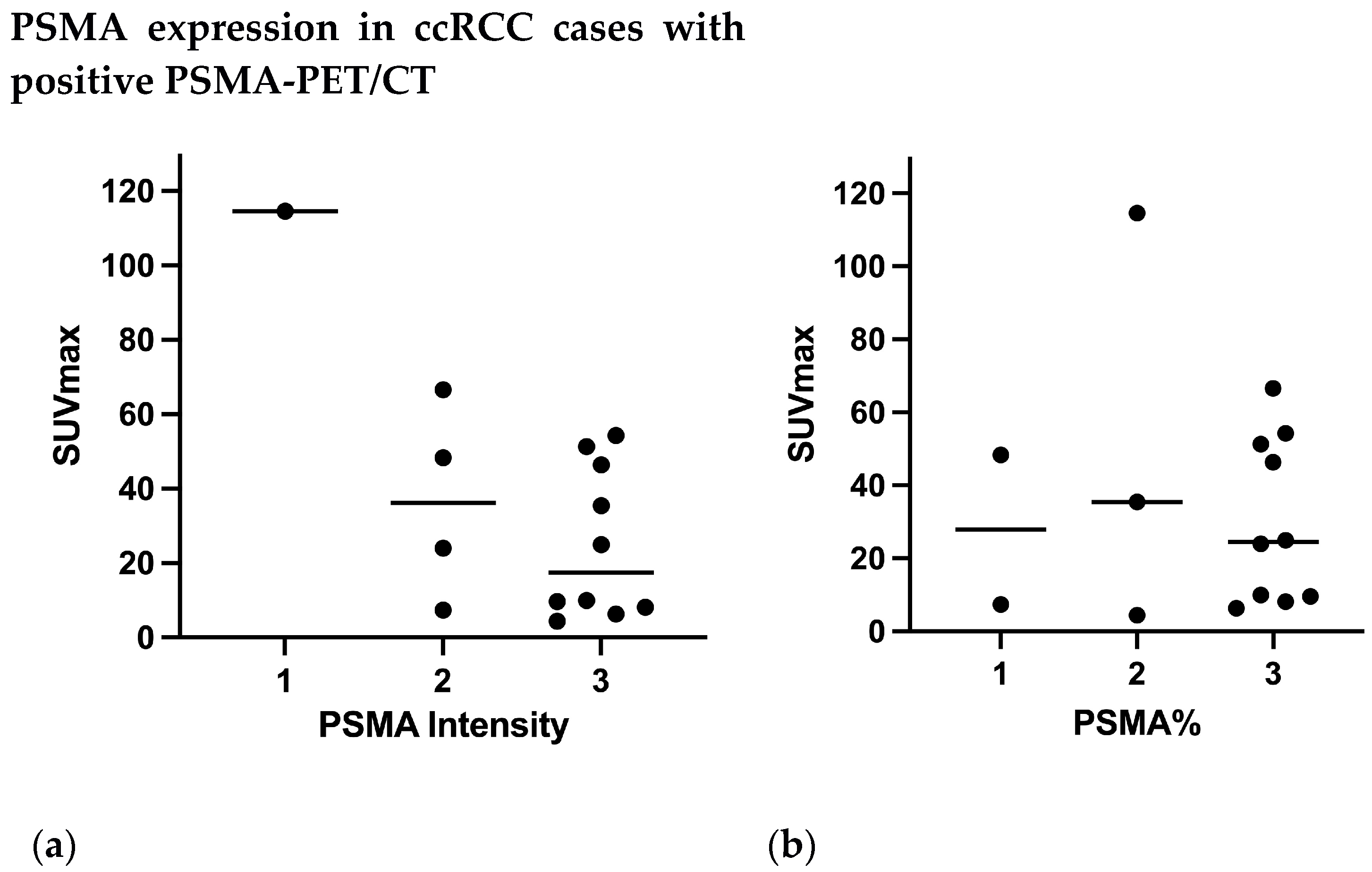
3.4. PSMA Expression on IHC and PET Results
3.5. Impact of PSMA-Directed PET/CT on Management
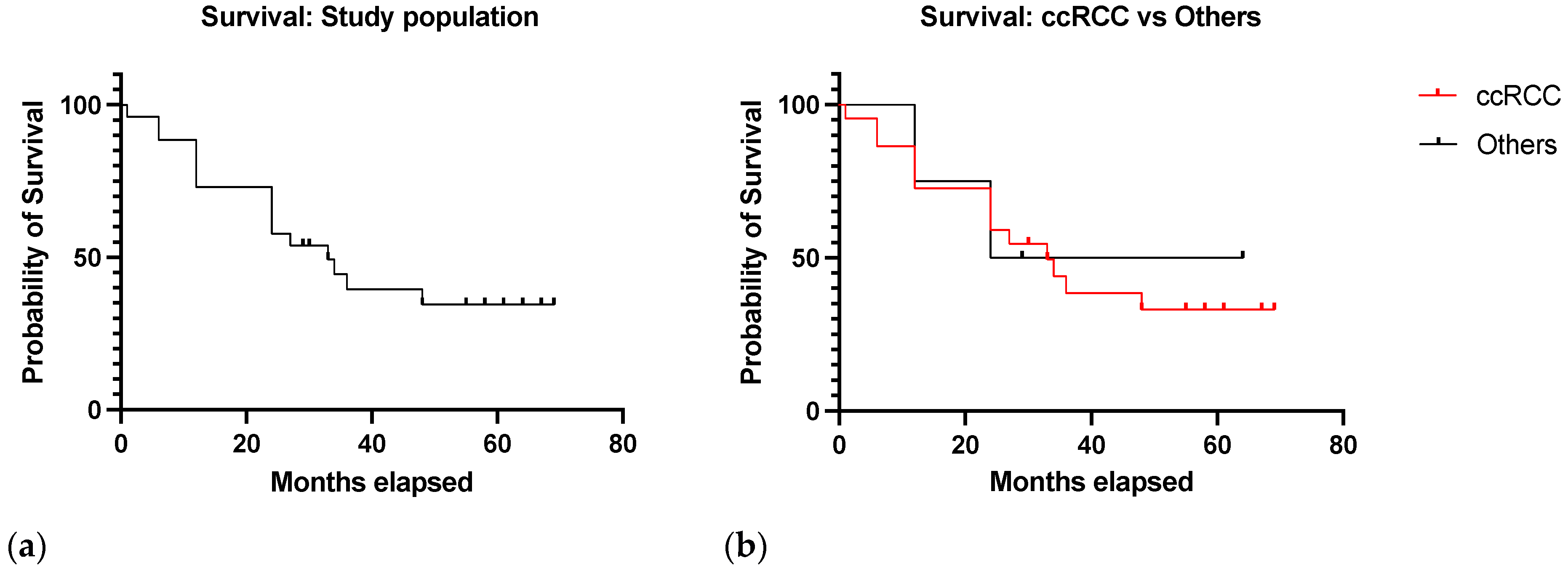
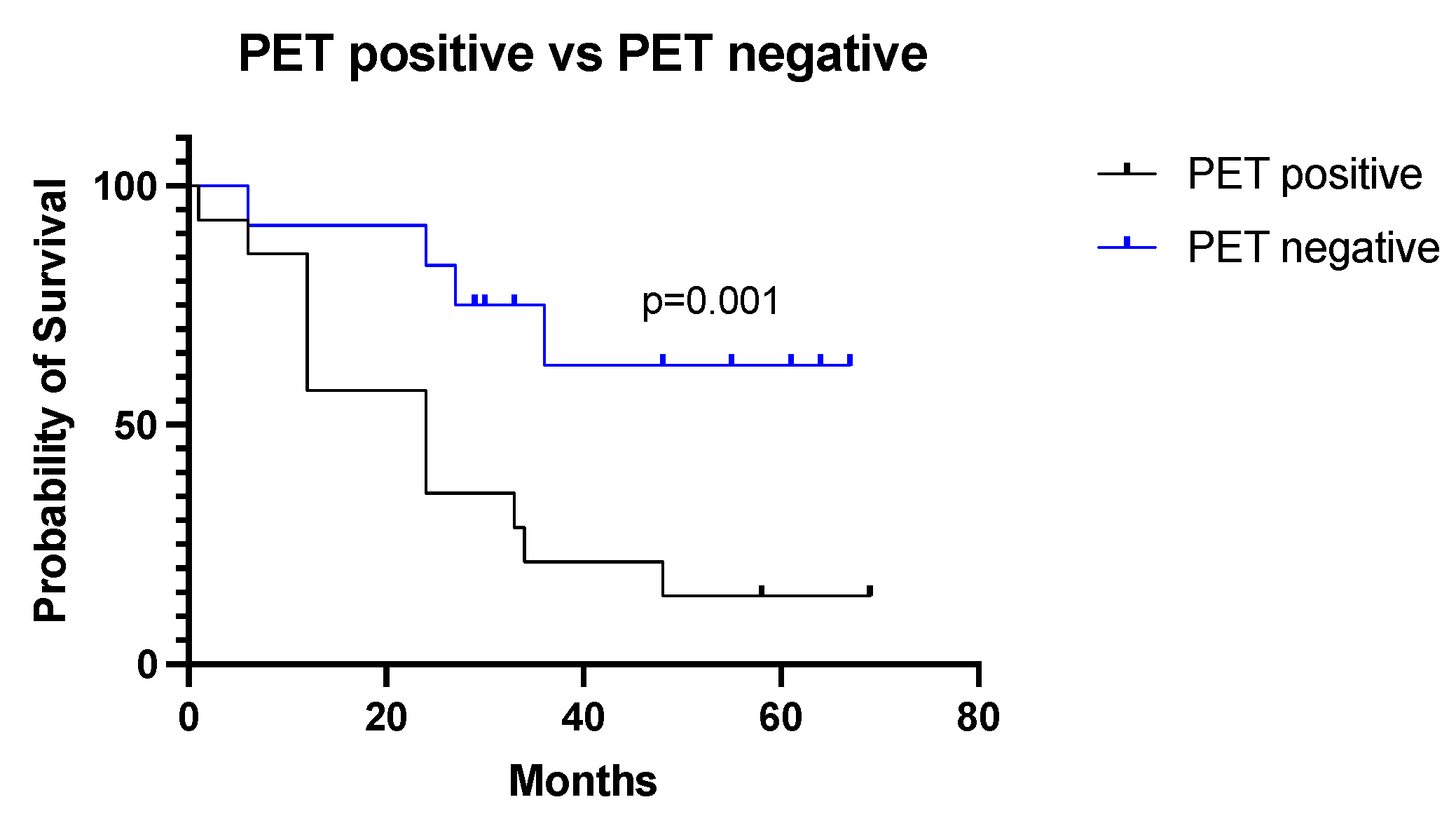
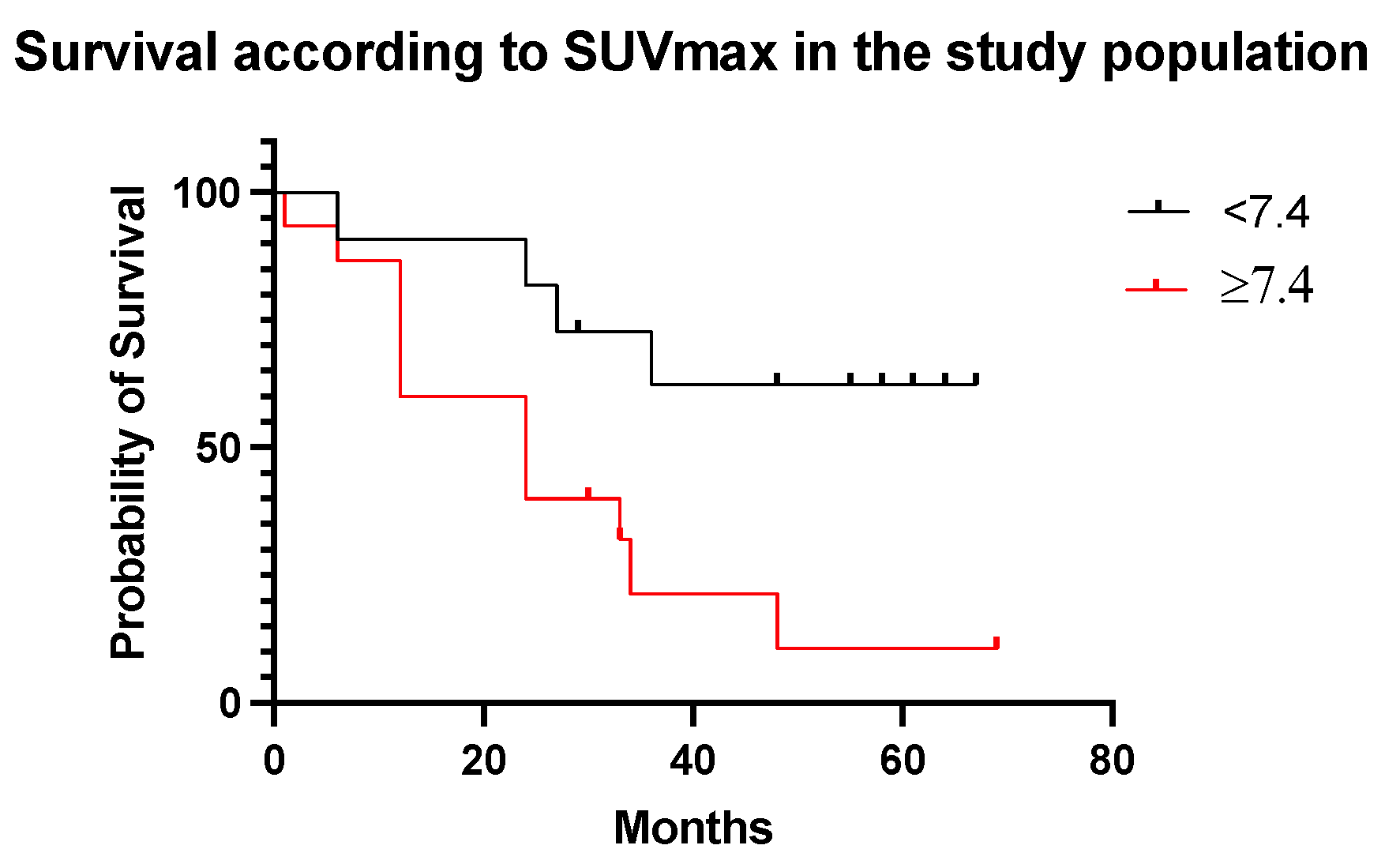
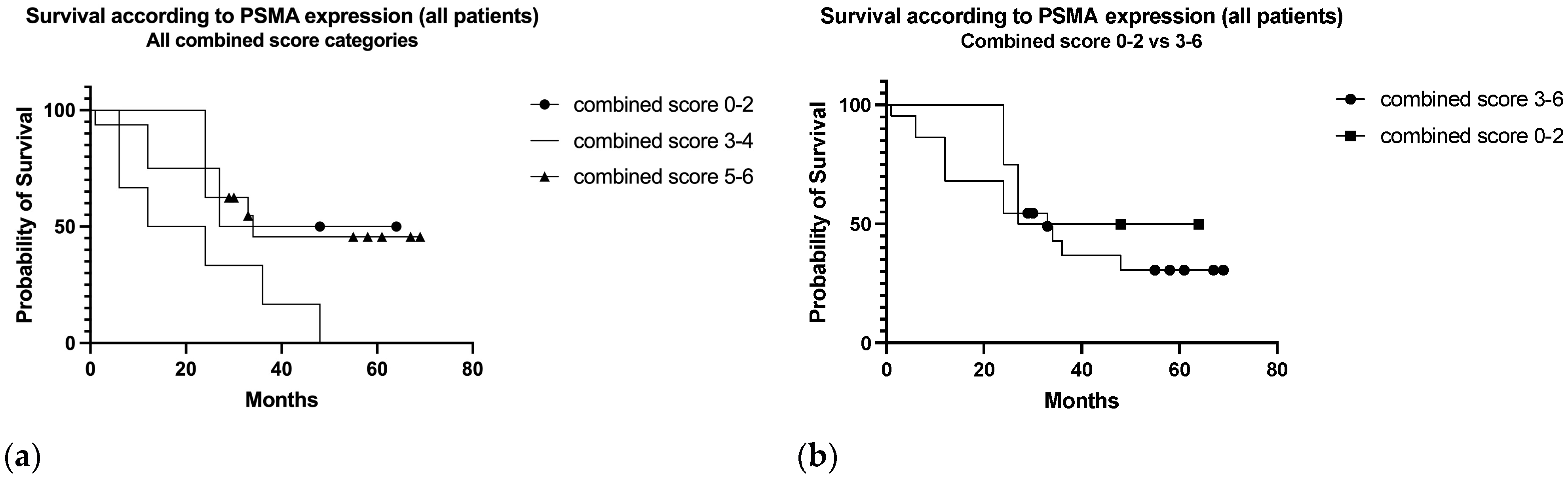
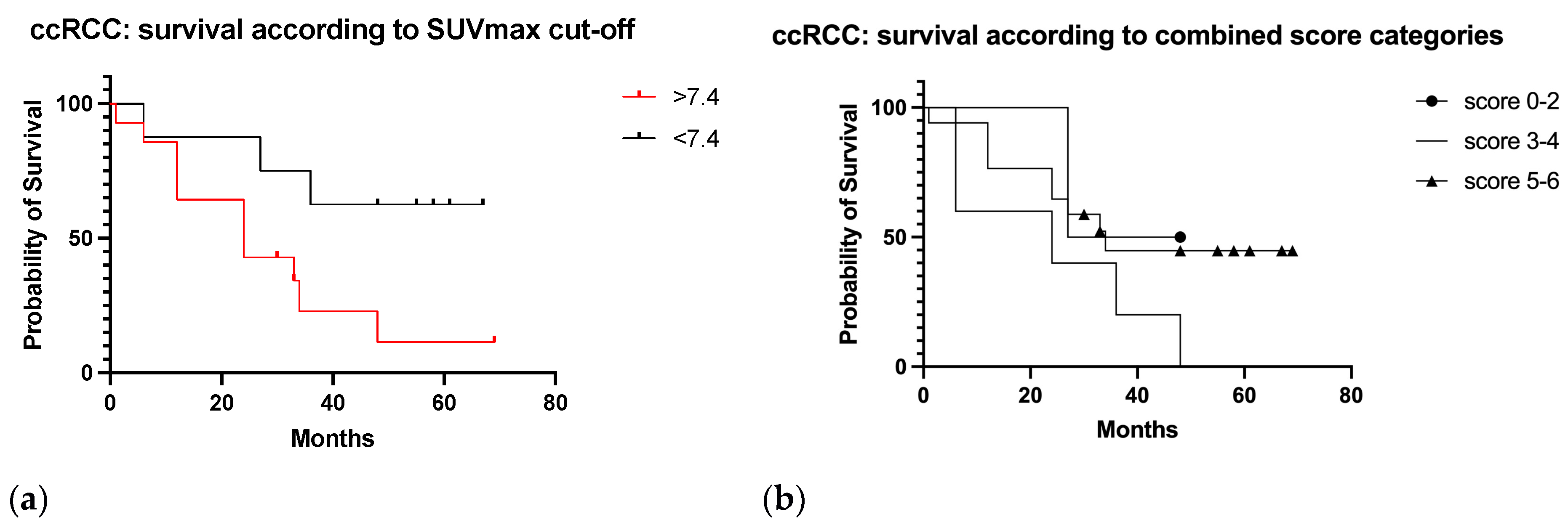
3.6. Survival Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kidney and Renal Pelvis Cancer—Cancer Stat Facts. Available online: https://seer.cancer.gov/statfacts/html/kidrp.html (accessed on 1 August 2023).
- Srigley, J.R.; Delahunt, B.; Eble, J.N.; Egevad, L.; Epstein, J.I.; Grignon, D.; Hes, O.; Moch, H.; Montironi, R.; Tickoo, S.K.; et al. The International Society of Urological Pathology (ISUP) Vancouver classification of renal neoplasia. Am. J. Surg. Pathol. 2013, 37, 1469–1489. [Google Scholar] [CrossRef] [PubMed]
- Dabestani, S.; Thorstenson, A.; Lindblad, P.; Harmenberg, U.; Ljungberg, B.; Lundstam, S. Renal cell carcinoma recurrences and metastases in primary non-metastatic patients: A population-based study. World J. Urol. 2016, 34, 1081–1086. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef]
- Osawa, T.; Takeuchi, A.; Kojima, T.; Shinohara, N.; Eto, M.; Nishiyama, H. Overview of current and future systemic therapy for metastatic renal cell carcinoma. Jpn. J. Clin. Oncol. 2019, 49, 395–403. [Google Scholar] [CrossRef]
- Bianchi, M.; Sun, M.; Jeldres, C.; Shariat, S.F.; Trinh, Q.-D.; Briganti, A.; Tian, Z.; Schmitges, J.; Graefen, M.; Perrotte, P.; et al. Distribution of metastatic sites in renal cell carcinoma: A population-based analysis. Ann. Oncol. 2012, 23, 973–980. [Google Scholar] [CrossRef] [PubMed]
- Rosiello, G.; Pecoraro, A.; Deuker, M.; Stolzenbach, L.F.; Martin, T.; Tian, Z.; Larcher, A.; Capitanio, U.; Montorsi, F.; Shariat, S.F.; et al. The impact of sex and age on distribution of metastases in patients with renal cell carcinoma. Int. J. Clin. Oncol. 2021, 26, 962–970. [Google Scholar] [CrossRef] [PubMed]
- Marconi, L.; Kuusk, T.; Capitanio, U.; Beisland, C.; Lam, T.; Pello, S.F.; Stewart, G.D.; Klatte, T.; Volpe, A.; Ljungberg, B.; et al. Local Treatment of Recurrent Renal Cell Carcinoma May Have a Significant Survival Effect Across All Risk-of-recurrence Groups. Eur. Urol. Open Sci. 2022, 47, 65–72. [Google Scholar] [CrossRef]
- Ljungberg, B.; Albiges, L.; Abu-Ghanem, Y.; Bensalah, K.; Dabestani, S.; Fernández-Pello, S.; Giles, R.H.; Hofmann, F.; Hora, M.; Kuczyk, M.A.; et al. European Association of Urology Guidelines on Renal Cell Carcinoma: The 2019 Update. Eur. Urol. 2019, 75, 799–810. [Google Scholar] [CrossRef]
- Dabestani, S.; Marconi, L.; Hofmann, F.; Stewart, F.; Lam, T.B.L.; Canfield, S.; Staehler, M.; Powles, T.; Ljungberg, B.; Bex, A. Local treatments for metastases of renal cell carcinoma: A systematic review. Lancet Oncol. 2014, 15, e549–e561. [Google Scholar] [CrossRef]
- Zaid, H.B.; Parker, W.P.; Safdar, N.S.; Gershman, B.; Erwin, P.J.; Murad, M.H.; Boorjian, S.A.; Costello, B.A.; Thompson, R.H.; Leibovich, B.C. Outcomes Following Complete Surgical Metastasectomy for Patients with Metastatic Renal Cell Carcinoma: A Systematic Review and Meta-Analysis. J. Urol. 2017, 197, 44–49. [Google Scholar] [CrossRef]
- Shinagare, A.B.; Krajewski, K.M.; Braschi-Amirfarzan, M.; Ramaiya, N.H. Advanced Renal Cell Carcinoma: Role of the Radiologist in the Era of Precision Medicine. Radiology 2017, 284, 333–351. [Google Scholar] [CrossRef] [PubMed]
- Sirous, R.; Henegan, J.C.; Zhang, X.; Howard, C.M.; Souza, F.; Smith, A.D. Metastatic renal cell carcinoma imaging evaluation in the era of anti-angiogenic therapies. Abdom. Radiol. 2016, 41, 1086–1099. [Google Scholar] [CrossRef] [PubMed]
- Grünwald, V.; Powles, T.; Kopyltsov, E.; Kozlov, V.; Alonso-Gordoa, T.; Eto, M.; Hutson, T.; Motzer, R.; Winquist, E.; Maroto, P.; et al. Survival by Depth of Response and Efficacy by International Metastatic Renal Cell Carcinoma Database Consortium Subgroup with Lenvatinib Plus Pembrolizumab Versus Sunitinib in Advanced Renal Cell Carcinoma: Analysis of the Phase 3 Randomized CLEAR Study. Eur. Urol. Oncol. 2023, 6, 437–446. [Google Scholar] [CrossRef]
- Motzer, R.J.; Escudier, B.; McDermott, D.F.; George, S.; Hammers, H.J.; Srinivas, S.; Tykodi, S.S.; Sosman, J.A.; Procopio, G.; Plimack, E.R.; et al. CheckMate 025 Investigators. Nivolumab versus everolimus in advanced renal-cell carcinoma. N. Engl. J. Med. 2015, 373, 1803–1813. [Google Scholar] [CrossRef] [PubMed]
- Yip, S.M.; Wells, C.; Moreira, R.; Wong, A.; Srinivas, S.; Beuselinck, B.; Porta, C.; Sim, H.W.; Ernst, D.S.; Rini, B.I.; et al. Checkpoint inhibitors in patients with metastatic renal cell carcinoma: Results from the International Metastatic Renal Cell Carcinoma Database Consortium. Cancer 2018, 124, 3677–3683. [Google Scholar] [CrossRef]
- Atkins, M.B.; McDermott, D.F.; Powles, T.; Motzer, R.J.; Rini, B.I.; Fong, L.; Joseph, R.W.; Pal, S.K.; Sznol, M.; Hainsworth, J.D.; et al. IMmotion150: A phase II trial in untreated metastatic renal cell carcinoma (mRCC) patients (pts) of atezolizumab (atezo) and bevacizumab (bev) vs and following atezo or sunitinib (sun) [abstract]. J. Clin. Oncol. 2017, 35 (Suppl. S15), 4505. [Google Scholar] [CrossRef]
- Motzer, R.J.; Tannir, N.M.; McDermott, D.F.; Arén Frontera, O.; Melichar, B.; Choueiri, T.K.; Plimack, E.R.; Barthélémy, P.; Porta, C.; George, S.; et al. Nivolumab plus ipilimumab versus sunitinib in advanced renal-cell carcinoma. N. Engl. J. Med. 2018, 378, 1277–1290. [Google Scholar] [CrossRef]
- Rini, B.I.; Plimack, E.R.; Stus, V.; Gafanov, R.; Hawkins, R.; Nosov, D.; Pouliot, F.; Alekseev, B.; Soulières, D.; Melichar, B.; et al. Pembrolizumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. N. Engl. J. Med. 2019, 380, 1116–1127. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Penkov, K.; Haanen, J.; Rini, B.; Albiges, L.; Campbell, M.T.; Venugopal, B.; Kollmannsberger, C.; Negrier, S.; Uemura, M.; et al. Avelumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. N. Engl. J. Med. 2019, 380, 1103–1115. [Google Scholar] [CrossRef]
- Harrison, M.R.; Costello, B.A.; Bhavsar, N.A.; Vaishampayan, U.; Pal, S.K.; Zakharia, Y.; Jim, H.S.L.; Fishman, M.N.; Molina, A.M.; Kyriakopoulos, C.E.; et al. Active surveillance of metastatic renal cell carcinoma: Results from a prospective observational study (MaRCC). Cancer 2021, 127, 2204–2212. [Google Scholar] [CrossRef]
- Mankoff, D.A. A definition of molecular imaging. J. Nucl. Med. 2007, 48, 18N–21N. [Google Scholar] [PubMed]
- Ma, H.; Shen, G.; Liu, B.; Yang, Y.; Ren, P.; Kuang, A. Diagnostic performance of 18F-FDG PET or PET/CT in restaging renal cell carcinoma: A systematic review and meta-analysis. Nucl. Med. Commun. 2017, 38, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Ueno, D.; Yao, M.; Tateishi, U.; Minamimoto, R.; Makiyama, K.; Hayashi, N.; Sano, F.; Murakami, T.; Kishida, T.; Miura, T.; et al. Early assessment by FDG-PET/CT of patients with advanced renal cell carcinoma treated with tyrosine kinase inhibitors is predictive of disease course. BMC Cancer 2012, 12, 162. [Google Scholar] [CrossRef] [PubMed]
- Ferdinandus, J.; Maríc, I.; Darr, C.; Kesch, C.; Bartel, T.; Fendler, W.P.; Grünwald, V. FDG-PET Positivity and Overall Survival in Renal Cell Carcinoma. JAMA Netw. Open 2022, 5, e2242289. [Google Scholar] [CrossRef] [PubMed]
- Nakaigawa, N.; Kondo, K.; Kaneta, T.; Tateishi, U.; Minamimoto, R.; Namura, K.; Ueno, D.; Kobayashi, K.; Kishida, T.; Ikeda, I.; et al. FDG PET/CT after first molecular targeted therapy predicts survival of patients with renal cell carcinoma. Cancer Chemother. Pharmacol. 2018, 81, 739–744. [Google Scholar] [CrossRef]
- Ramdave, S.; Thomas, G.W.; Berlangieri, S.U.; Bolton, D.M.; Davis, I.; Macgregor, D.; Scott, A.M. Clinical role of F-18 fluorodeoxyglucose positron emission tomography for detection and management of renal cell carcinoma. J. Urol. 2001, 166, 825–830. [Google Scholar] [CrossRef]
- Kumar, R.; Chauhan, A.; Lakhani, P.; Xiu, Y.; Zhuang, H.; Alavi, A. 2-Deoxy-2-[F-18]fluoro-D-glucose-positron emission tomography in characterization of solid renal masses. Mol. Imaging Biol. 2005, 7, 431–439. [Google Scholar] [CrossRef]
- Chang, S.S.; E Reuter, V.; Heston, W.D.; Bander, N.H.; Grauer, L.S.; Gaudin, P.B. Five different anti-prostate-specific membrane antigen (PSMA) antibodies confirm PSMA expression in tumor-associated neovasculature. Cancer Res. 1999, 59, 3192–3198. [Google Scholar]
- Baccala, A.; Sercia, L.; Li, J.; Heston, W.; Zhou, M. Expression of prostate-specific membrane antigen in tumor-associated neovasculature of renal neoplasms. Urology 2007, 70, 385–390. [Google Scholar] [CrossRef]
- Silver, D.A.; Pellicer, I.; Fair, W.R.; Heston, W.D.; Cordon-Cardo, C. Prostate-specific membrane antigen expression in normal and malignant human tissues. Clin. Cancer Res. 1997, 3, 81–85. [Google Scholar]
- Spatz, S.; Tolkach, Y.; Jung, K.; Stephan, C.; Busch, J.; Ralla, B.; Rabien, A.; Feldmann, G.; Brossart, P.; Bundschuh, R.A.; et al. Comprehensive evaluation of prostate specific membrane antigen expression in the vasculature of renal tumors: Implications for imaging studies and prognostic role. J. Urol. 2018, 199, 370–377. [Google Scholar] [CrossRef] [PubMed]
- Eder, M.; Schäfer, M.; Bauder-Wüst, U.; Hull, W.-E.; Wängler, C.; Mier, W.; Haberkorn, U.; Eisenhut, M. 68Ga-complex lipophilicity and the targeting property of a urea-based PSMA inhibitor for PET imaging. Bioconjugate Chem. 2012, 23, 688–697. [Google Scholar] [CrossRef] [PubMed]
- Szabo, Z.; Mena, E.; Rowe, S.P.; Plyku, D.; Nidal, R.; Eisenberger, M.A.; Antonarakis, E.S.; Fan, H.; Dannals, R.F.; Chen, Y.; et al. Initial Evaluation of [(18)F]DCFPyL for Prostate-Specific Membrane Antigen (PSMA)-Targeted PET Imaging of Prostate Cancer. Mol. Imaging Biol. 2015, 17, 565–574. [Google Scholar] [CrossRef] [PubMed]
- Eder, M.; Neels, O.; Müller, M. Novel preclinical and radiopharmaceutical aspects of [68Ga] Ga-PSMA-HBED-CC: A New PET tracer for imaging of prostate cancer. Pharmaceuticals 2014, 7, 779–796. [Google Scholar] [CrossRef] [PubMed]
- European Pharmacopoeia 10.4; Monograph no. 3044 “Gallium (68Ga) PSMA-11 Injection”; Council of Europe: Strasbourg, France, 2021.
- Hennrich, U.; Eder, M. [68Ga]Ga-PSMA-11: The First FDA-Approved 68Ga-Radiopharmaceutical for PET Imaging of Prostate Cancer. Pharmaceuticals 2021, 14, 713. [Google Scholar] [CrossRef] [PubMed]
- Sawicki, L.M.; Buchbender, C.; Boos, J.; Giessing, M.; Ermert, J.; Antke, C.; Antoch, G.; Hautzel, H. Diagnostic potential of PET/CT using a (68)Ga-labelled prostate-specific membrane antigen ligand in whole-body staging of renal cell carcinoma: Initial experience. Eur. J. Nucl. Med. Mol. Imaging. 2017, 44, 102–107. [Google Scholar] [CrossRef]
- Raveenthiran, S.; Esler, R.; Yaxley, J.; Kyle, S. The use of 68Ga-PET/CT PSMA in the staging of primary and suspected recurrent renal cell carcinoma. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2280–2288. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, G.; Yu, H.; Wu, Y.; Lin, M.; Gao, J.; Xu, B. Comparison of 18F-DCFPyL and 18F-FDG PET/computed tomography for the restaging of clear cell renal cell carcinoma: Preliminary results of 15 patients. Nucl. Med. Commun. 2020, 41, 1299–1305. [Google Scholar] [CrossRef]
- Tariq, A.; Kwok, M.; Pearce, A.; Rhee, H.; Kyle, S.; Marsh, P.; Raveenthiran, S.; Wong, D.; McBean, R.; Westera, J.; et al. The role of dual tracer PSMA and FDG PET/CT in renal cell carcinoma (RCC) compared to conventional imaging: A multi-institutional case series with intra-individual comparison. Urol. Oncol. 2022, 40, 66.e1–66.e9. [Google Scholar] [CrossRef]
- Rowe, S.P.; Gorin, M.A.; Hammers, H.J.; Javadi, M.S.; Hawasli, H.; Szabo, Z.; Cho, S.Y.; Pomper, M.G.; Allaf, M.E. Imaging of metastatic clear cell renal cell carcinoma with PSMA-targeted ¹⁸F-DCFPyL PET/CT. Ann. Nucl. Med. 2015, 29, 877–882. [Google Scholar] [CrossRef]
- Rhee, H.; Blazak, J.; Tham, C.M.; Ng, K.L.; Shepherd, B.; Lawson, M.; Preston, J.; Vela, I.; Thomas, P.; Wood, S. Pilot study: Use of gallium-68 PSMA PET for detection of metastatic lesions in patients with renal tumour. EJNMMI Res. 2016, 6, 76. [Google Scholar] [CrossRef] [PubMed]
- Meyer, A.R.; Carducci, M.A.; Denmeade, S.R.; Markowski, M.C.; Pomper, M.G.; Pierorazio, P.M.; Allaf, M.E.; Rowe, S.P.; Gorin, M.A. Improved identification of patients with oligometastatic clear cell renal cell carcinoma with PSMA-targeted 18F-DCFPyL PET/CT. Ann. Nucl. Med. 2019, 33, 617–623. [Google Scholar] [CrossRef] [PubMed]
- Gühne, F.; Seifert, P.; Theis, B.; Steinert, M.; Freesmeyer, M.; Drescher, R. PSMA-PET/CT in Patients with Recurrent Clear Cell Renal Cell Carcinoma: Histopathological Correlations of Imaging Findings. Diagnostics 2021, 11, 1142. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zheng, R.; Zhang, Y.; Huang, C.; Tian, L.; Liu, R.; Liu, Y.; Zhang, Z.; Han, H.; Zhou, F.; et al. Special issue “The advance of solid tumor research in China”: 68Ga-PSMA-11 PET/CT for evaluating primary and metastatic lesions in different histological subtypes of renal cell carcinoma. Int. J. Cancer 2023, 152, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Golan, S.; Aviv, T.; Groshar, D.; Yakimov, M.; Zohar, Y.; Prokocimer, Y.; Nadu, A.; Baniel, J.; Domachevsky, L.; Bernstine, H. Dynamic 68Ga-PSMA-11 PET/CT for the Primary Evaluation of Localized Renal Mass: A Prospective Study. J. Nucl. Med. 2021, 62, 773–778. [Google Scholar] [CrossRef]
- Udovicich, C.; Callahan, J.; Bressel, M.; Ong, W.L.; Perera, M.; Tran, B.; Azad, A.; Haran, S.; Moon, D.; Chander, S.; et al. Impact of Prostate-specific Membrane Antigen Positron Emission Tomography/Computed Tomography in the Management of Oligometastatic Renal Cell Carcinoma. Eur. Urol. Open Sci. 2022, 44, 60–68. [Google Scholar] [CrossRef]
- Pathmanathan, S.; Tariq, A.; Pearce, A.; Rhee, H.; Kyle, S.; Raveenthiran, S.; Wong, D.; McBean, R.; Marsh, P.; Goodman, S.; et al. Clinical impact of Prostate-Specific Membrane Antigen Positron Emission Tomography (PET) on intensification or deintensification of advanced renal cell carcinoma management. Eur. J. Nucl. Med. Mol. Imaging 2023. [Google Scholar] [CrossRef]
- Migliari, S.; Sammartano, A.; Scarlattei, M.; Serreli, G.; Ghetti, C.; Cidda, C.; Baldari, G.; Ortenzia, O.; Ruffini, L. Development and Validation of a High-Pressure Liquid Chromatography Method for the Determination of Chemical Purity and Radiochemical Purity of a [68Ga]-Labeled Glu-Urea-Lys(Ahx)-HBED-CC (Positron Emission Tomography) Tracer. ACS Omega 2017, 2, 7120–7126. [Google Scholar] [CrossRef]
- Al-Ahmadie, H.; Olgac, S.; Gregor, P.D.; Tickoo, S.K.; Fine, S.W.; Kondagunta, G.V.; I Scher, H.; Morris, M.J.; Russo, P.; Motzer, R.J.; et al. Expression of prostate-specific membrane antigen in renal cortical tumors. Mod. Pathol. 2008, 21, 727–732. [Google Scholar] [CrossRef]
- Zschäbitz, S.; Erlmeier, F.; Stöhr, C.; Herrmann, E.; Polifka, I.; Agaimy, A.; Trojan, L.; Ströbel, P.; Becker, F.; Wülfing, C.; et al. Expression of Prostate-specific Membrane Antigen (PSMA) in Papillary Renal Cell Carcinoma-Overview and Report on a Large Multicenter Cohort. J. Cancer 2022, 13, 1706–1712. [Google Scholar] [CrossRef]
- Bauman, T.M.; Huang, W.; Lee, M.H.; Abel, E.J. Neovascularity as a prognostic marker in renal cell carcinoma. Hum. Pathol. 2016, 57, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Gasparro, D.; Scarlattei, M.; Manuguerra, R.; Guglielmo, P.; Migliari, S.M.; Sammartano, A.M.; Baldari, G.; Maestroni, U.; Silini, E.M.; Ruffini, L. 18F-FDG and 68GA-Prostate-Specific Membrane Antigen PET/CT Perform Better Than CT Alone in Restaging Papillary Renal Cell Carcinoma Recurrence. Clin. Nucl. Med. 2021, 46, e458–e460. [Google Scholar] [CrossRef] [PubMed]
- Siva, S.; Callahan, J.; Pryor, D.; Martin, J.; Lawrentschuk, N.; Hofman, M.S. Utility of (68) Ga prostate specific membrane antigen-positron emission tomography in diagnosis and response assessment of recurrent renal cell carcinoma. J. Med. Imaging Radiat. Oncol. 2017, 61, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Morgantetti, G.; Ng, K.L.; Samaratunga, H.; Rhee, H.; Gobe, G.C.; Wood, S.T. Prostate specific membrane antigen (PSMA) expression in vena cava tumour thrombi of clear cell renal cell carcinoma suggests a role for PSMA-driven tumour neoangiogenesis. Transl. Androl. Urol. 2019, 8 (Suppl. S2), S147–S155. [Google Scholar] [CrossRef]
- Ahn, T.; Roberts, M.J.; Abduljabar, A.; Joshi, A.; Perera, M.; Rhee, H.; Wood, S.; Vela, I. A review of prostate-specific membrane antigen (PSMA) positron emission tomography (PET) in renal cell carcinoma (RCC). Mol. Imaging Biol. 2019, 21, 799–807. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient’s Characteristics | Data |
|---|---|
| Mean age (range, yrs) | 65.6 (42–85) |
| No. male (%) | 16 (61.5) |
| No. female (%) | 10 (38.5) |
| Median months follow up (range) | 29.5 (1–69) |
| No. follow up end status (%) | |
| Alive (No.) | 10 (38.5) |
| Dead (No.) | 16 (61.5) |
| No. histological subtype (%) | |
| Clear cell | 22 (84.6) |
| Papillary | 2 (7.7) |
| Chromophobe | 1 (3.8) |
| NAS | 1 (3.8) |
| No. primary intervention (%) | |
| Radical nephrectomy | 22 (84.6) |
| Partial nephrectomy | 2 (7.69) |
| RFA | 1 (3.85) |
| None | 1 (3.85) |
| No. patients on therapy | |
| Current | 4 |
| Before PSMA-PET/CT scan | 7 |
| None | 15 |
| Site of Metastatic Lesions at PSMA PET/CT in cc-RCC | No. Patients | SUVmax Mean Value (Range) |
|---|---|---|
| Lung | 7 | 12.08 (3.2–24.9) |
| Liver | 2 | 29.8 (11.2–48.3) |
| Bone | 3 | 24.0 (10.0–46.3) |
| Lymph nodes | 4 | 20.6 (7.6–35.4) |
| Brain | 2 | 15.5 (10.7–20.2) |
| Adrenal gland | 2 | 12.8 (9.6–15.9) |
| Vascular | 2 | 11.8 (5.8–17.8) |
| Soft tissue | 2 | 36.1 (5.6–66.6) |
| Retroperitoneum | 2 | 22.8 (26.7–18.9) |
| Thyroid | 1 | 24.5 |
| No. Patients | Planned Therapy | Performed Therapy |
|---|---|---|
| 4 | systemic | SABR or surgery +/− systemic |
| 11 | surveillance or local treatment (surgery, RT, radiofrequency ablation) | systemic |
| 4 | surveillance | surgery or systemic |
| 1 | systemic | palliation |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gasparro, D.; Scarlattei, M.; Silini, E.M.; Migliari, S.; Baldari, G.; Cervati, V.; Graziani, T.; Campanini, N.; Maestroni, U.; Ruffini, L. High Prognostic Value of 68Ga-PSMA PET/CT in Renal Cell Carcinoma and Association with PSMA Expression Assessed by Immunohistochemistry. Diagnostics 2023, 13, 3082. https://doi.org/10.3390/diagnostics13193082
Gasparro D, Scarlattei M, Silini EM, Migliari S, Baldari G, Cervati V, Graziani T, Campanini N, Maestroni U, Ruffini L. High Prognostic Value of 68Ga-PSMA PET/CT in Renal Cell Carcinoma and Association with PSMA Expression Assessed by Immunohistochemistry. Diagnostics. 2023; 13(19):3082. https://doi.org/10.3390/diagnostics13193082
Chicago/Turabian StyleGasparro, Donatello, Maura Scarlattei, Enrico Maria Silini, Silvia Migliari, Giorgio Baldari, Veronica Cervati, Tiziano Graziani, Nicoletta Campanini, Umberto Maestroni, and Livia Ruffini. 2023. "High Prognostic Value of 68Ga-PSMA PET/CT in Renal Cell Carcinoma and Association with PSMA Expression Assessed by Immunohistochemistry" Diagnostics 13, no. 19: 3082. https://doi.org/10.3390/diagnostics13193082