
Machine Learning Predicts Pathologic Complete Response to Neoadjuvant Chemotherapy for ER+HER2- Breast Cancer: Integrating Tumoral and Peritumoral MRI Radiomic Features


Abstract
:1. Introduction
2. Materials and Methods
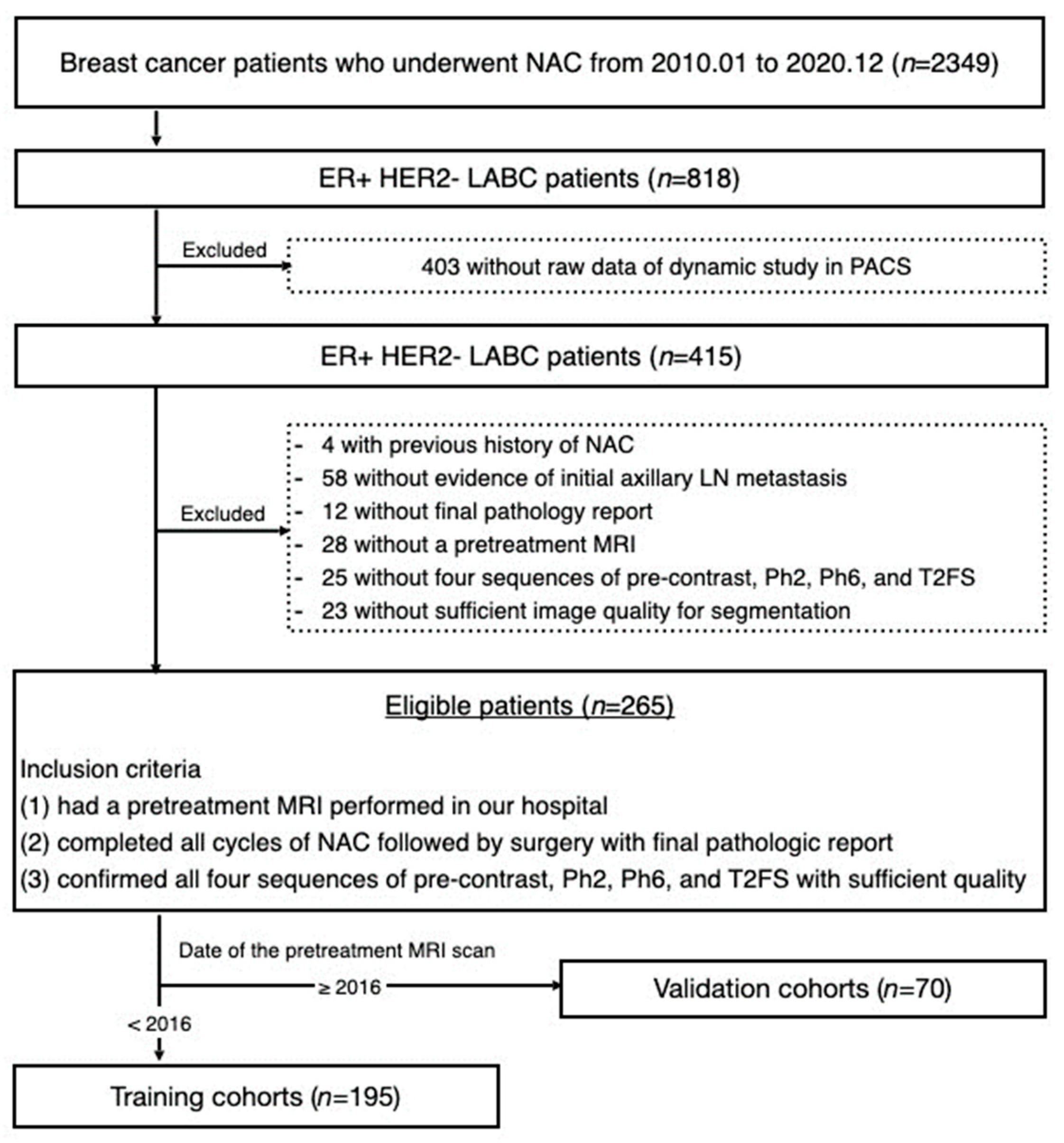
2.1. Patient Population and Study Design
2.2. MRI Acquisition
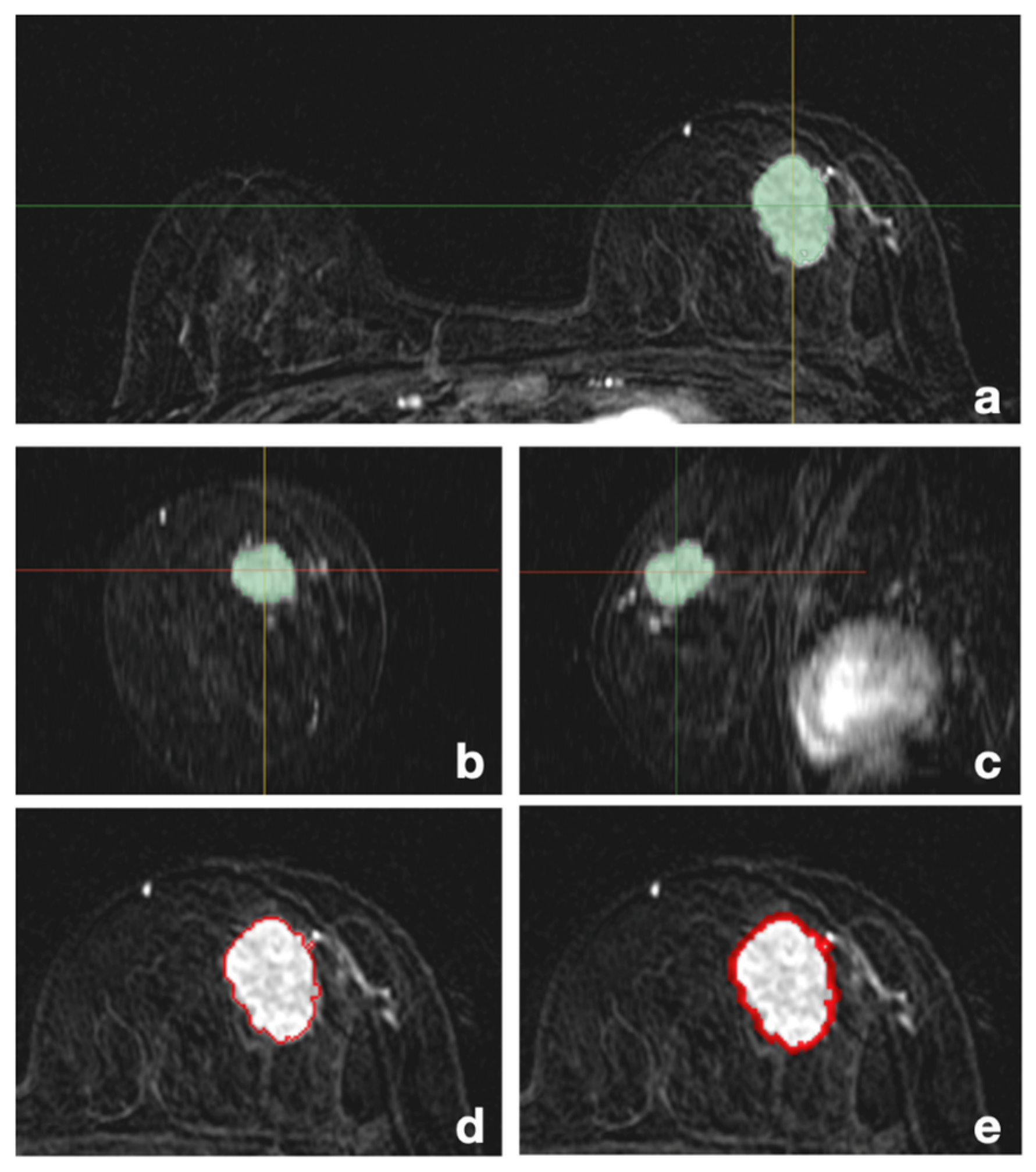
2.3. Volume of Interest (VOI) Segmentation
2.4. MRI Preprocessing and Radiomic Texture Feature Extraction
2.5. Dimension Reduction
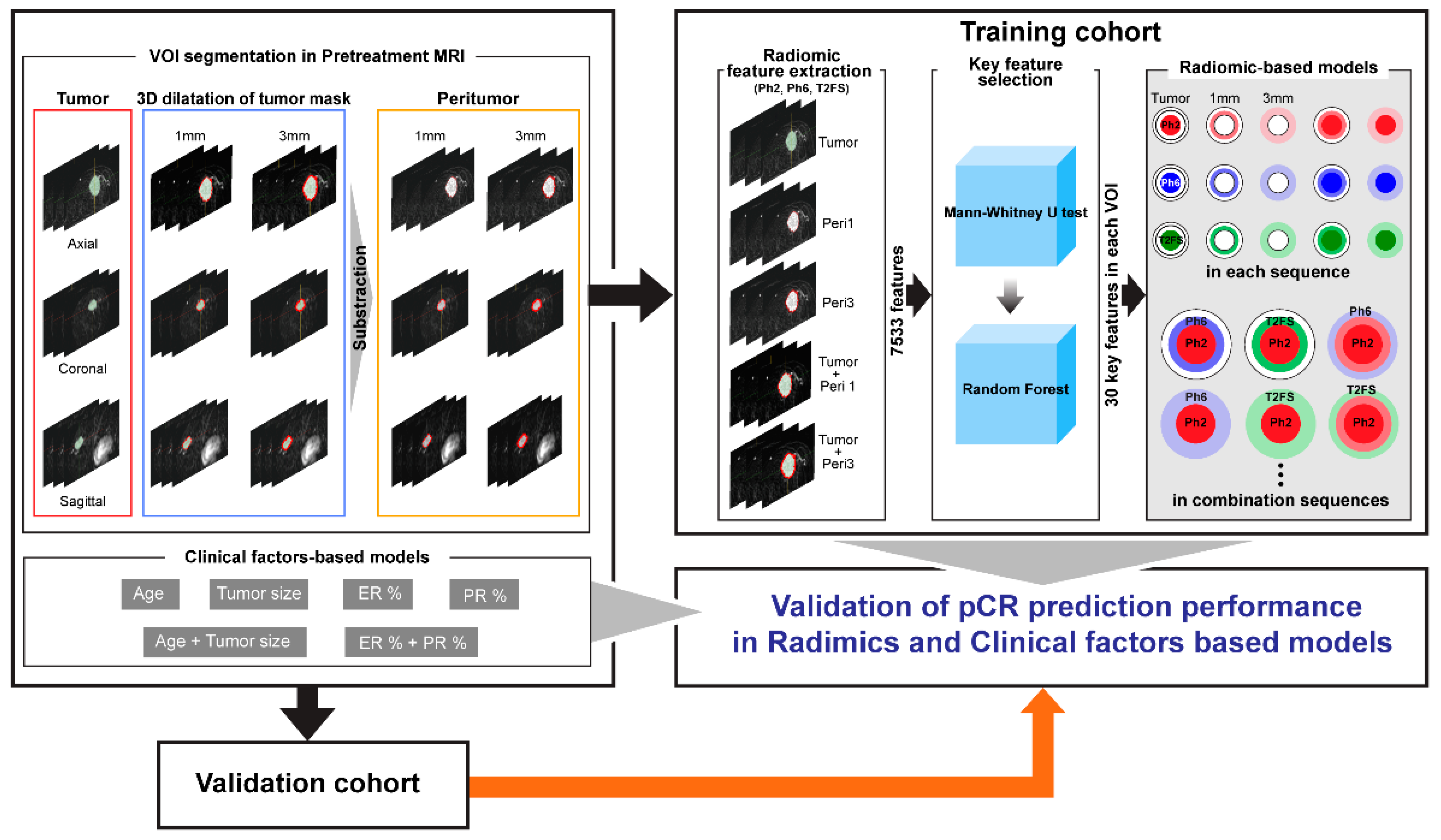
2.6. Development of pCR Prediction Model in the Training Cohort
2.7. Assessment of pCR Prediction Model Performance with the Validation Cohort
2.8. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Radiomic Texture Feature Composition and Dimension Reduction
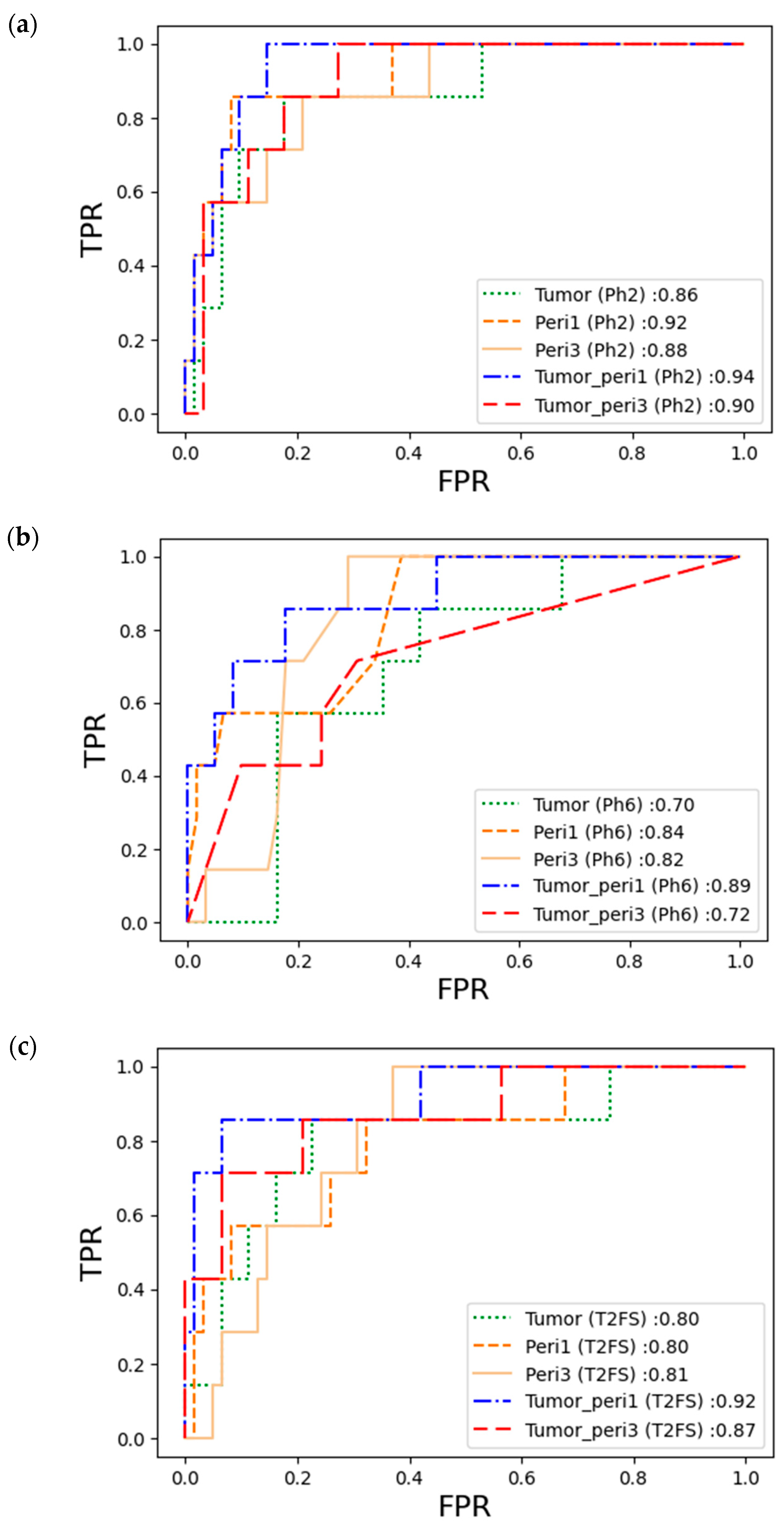
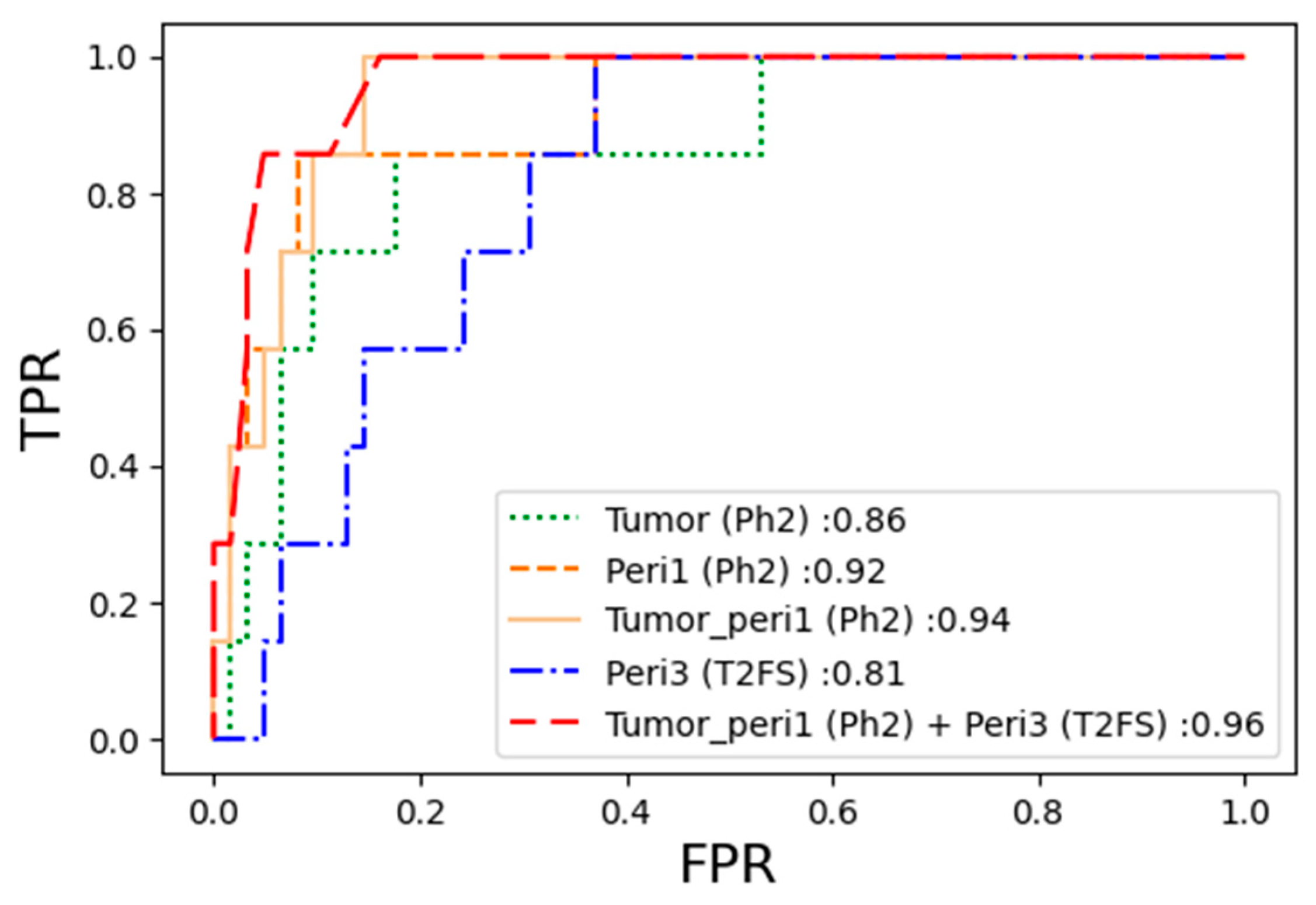
3.3. Performance of the pCR Prediction Model in Each Sequence
3.4. Performance of the pCR Prediction Model with Combination of Sequences
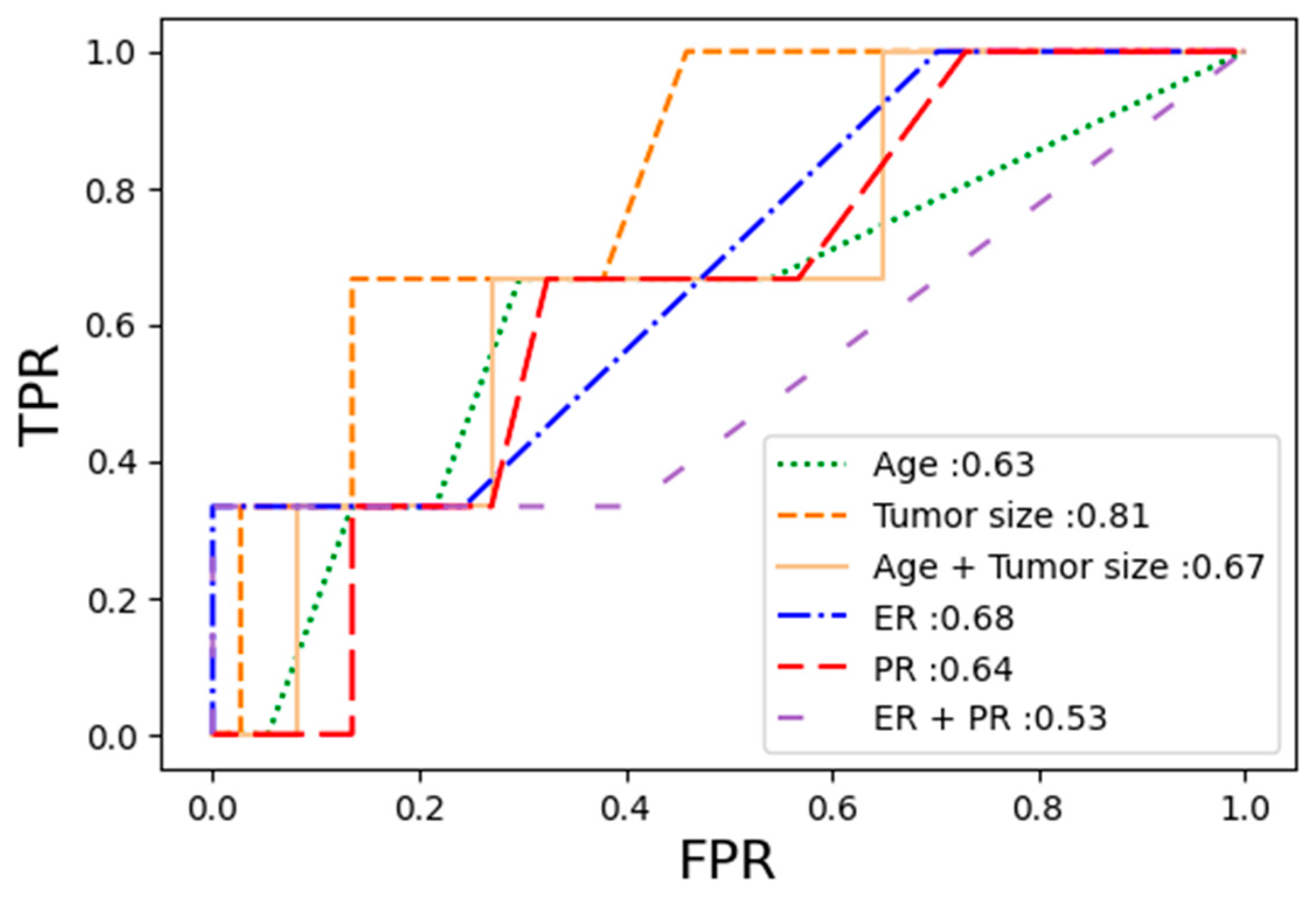
3.5. Diagnostic Performance of Clinical Model
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Azadnajafabad, S.; Saeedi Moghaddam, S.; Keykhaei, M.; Shobeiri, P.; Rezaei, N.; Ghasemi, E.; Mohammadi, E.; Ahmadi, N.; Ghamari, A.; Shahin, S.; et al. Expansion of the quality of care index on breast cancer and its risk factors using the Global Burden of Disease Study 2019. Cancer Med. 2023, 12, 1729–1743. [Google Scholar] [CrossRef] [PubMed]
- Belete, A.M.; Aynalem, Y.A.; Gemeda, B.N.; Demelew, T.M.; Shiferaw, W.S. The Effect of Estrogen Receptor Status on Survival in Breast Cancer Patients in Ethiopia. Retrospective Cohort Study. Breast Cancer Targets Ther. 2022, 14, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Nam, K.J.; Park, H.; Ko, E.S.; Lim, Y.; Cho, H.H.; Lee, J.E. Radiomics signature on 3T dynamic contrast-enhanced magnetic resonance imaging for estrogen receptor-positive invasive breast cancers: Preliminary results for correlation with Oncotype DX recurrence scores. Medicine 2019, 98, 23. [Google Scholar] [CrossRef] [PubMed]
- von Minckwitz, G.; Raab, G.; Caputo, A.; Schutte, M.; Hilfrich, J.; Blohmer, J.U.; Gerber, B.; Costa, S.D.; Merkle, E.; Eidtmann, H.; et al. Doxorubicin with cyclophosphamide followed by docetaxel every 21 days compared with doxorubicin and docetaxel every 14 days as preoperative treatment in operable breast cancer: The GEPARDUO study of the German Breast Group. J. Clin. Oncol. 2005, 23, 2676–2685. [Google Scholar] [CrossRef]
- Chica-Parrado, M.R.; Godoy-Ortiz, A.; Jiménez, B.; Ribelles, N.; Barragan, I.; Alba, E. Resistance to neoadjuvant treatment in breast cancer: Clinicopathological and molecular predictors. Cancers 2020, 12, 2012. [Google Scholar] [CrossRef]
- Kim, M.J.; Kim, E.K.; Park, S.; Moon, H.J.; Kim, S.; Park, B.W. Evaluation with 3.0-T MR imaging: Predicting the pathological response of triple-negative breast cancer treated with anthracycline and taxane neoadjuvant chemotherapy. Acta Radiol. 2015, 56, 1069–1077. [Google Scholar] [CrossRef]
- Chen, L.; Yang, Q.; Bao, J.; Liu, D.; Huang, X.; Wang, J. Direct comparison of PET/CT and MRI to predict the pathological response to neoadjuvant chemotherapy in breast cancer: A meta-analysis. Sci. Rep. 2017, 7, 8479. [Google Scholar] [CrossRef]
- Shohdy, K.S.; Almeldin, D.S.; Fekry, M.A.; Ismail, M.A.; AboElmaaref, N.A.; ElSadany, E.G.; Hamza, B.M.; El-Shorbagy, F.H.; Ali, A.S.; Attia, H.; et al. Pathological responses and survival outcomes in patients with locally advanced breast cancer after neoadjuvant chemotherapy: A single-institute experience. J. Egypt. Natl. Cancer Inst. 2021, 33, 39. [Google Scholar] [CrossRef]
- Spring, L.M.; Fell, G.; Arfe, A.; Sharma, C.; Greenup, R.; Reynolds, K.L.; Smith, B.L.; Alexander, B.; Moy, B.; Isakoff, S.J.; et al. Pathologic complete response after neoadjuvant chemotherapy and impact on breast cancer recurrence and survival: A comprehensive meta-analysispCR and association with clinical outcomes in breast cancer. Clin. Cancer Res. 2020, 26, 2838–2848. [Google Scholar] [CrossRef]
- Bian, T.; Wu, Z.; Lin, Q.; Wang, H.; Ge, Y.; Duan, S.; Fu, G.; Cui, C.; Su, X. Radiomic signatures derived from multiparametric MRI for the pretreatment prediction of response to neoadjuvant chemotherapy in breast cancer. Br. J. Radiol. 2020, 93, 20200287. [Google Scholar] [CrossRef]
- Ko, E.S.; Han, B.K.; Kim, R.B.; Ko, E.Y.; Shin, J.H.; Hahn, S.Y. Analysis of factors that influence the accuracy of magnetic resonance imaging for predicting response after neoadjuvant chemotherapy in locally advanced breast cancer. Ann. Surg. Oncol. 2013, 20, 2562–2568. [Google Scholar] [CrossRef]
- Overcast, W.B.; Davis, K.M.; Ho, C.Y.; Hutchins, G.D.; Green, M.A.; Graner, B.D.; Veronesi, M.C. Advanced imaging techniques for neuro-oncologic tumor diagnosis, with an emphasis on PET-MRI imaging of malignant brain tumors. Curr. Oncol. Rep. 2021, 23, 34. [Google Scholar] [CrossRef] [PubMed]
- Varghese, B.A.; Cen, S.Y.; Hwang, D.H.; Duddalwar, V.A. Texture analysis of imaging: What radiologists need to know. Am. J. Roentgenol. 2019, 212, 520–528. [Google Scholar] [CrossRef] [PubMed]
- Wagner, M.W.; Namdar, K.; Biswas, A.; Monah, S.; Khalvati, F.; Ertl-Wagner, B.B. Radiomics, machine learning, and artificial intelligence—What the neuroradiologist needs to know. Neuroradiology 2021, 63, 1957–1967. [Google Scholar] [CrossRef]
- Parikh, J.; Selmi, M.; Charles-Edwards, G.; Glendenning, J.; Ganeshan, B.; Verma, H.; Mansi, J.; Tutt, A. Changes in primary breast cancer heterogeneity may augment midtreatment MR imaging assessment of response to neoadjuvant chemotherapy. Radiology 2014, 272, 100–112. [Google Scholar] [CrossRef]
- Henderson, S.; Purdie, C.; Michie, C.; Evans, A.; Lerski, R.; Johnston, M.; Alastair, M. Interim heterogeneity changes measured using entropy texture features on T2-weighted MRI at 3.0 T are associated with pathological response to neoadjuvant chemotherapy in primary breast cancer. Eur. Radiol. 2017, 27, 4602–4611. [Google Scholar] [CrossRef]
- Panico, C.; Ferrara, F.; Woitek, R.; D’Angelo, A.; Di Paola, V.; Bufi, E.; Conti, M. Staging Breast Cancer with MRI, the T. A Key Role in the Neoadjuvant Setting. Cancers 2022, 14, 5786. [Google Scholar] [CrossRef] [PubMed]
- Umutlu, L.; Kirchner, J.; Bruckmann, N.M.; Morawitz, J.; Antoch, G.; Ting, S.; Catalano, O.A. Multiparametric 18F-FDG PET/MRI-based Radiomics for prediction of pathological complete response to neoadjuvant chemotherapy in breast cancer. Cancers 2022, 14, 1727. [Google Scholar] [CrossRef] [PubMed]
- Braman, N.M.; Etesami, M.; Prasanna, P.; Dubchuk, C.; Gilmore, H.; Tiwari, P.; Plecha, D. Intratumoral and peritumoral radiomics for the pretreatment prediction of pathological complete response to neoadjuvant chemotherapy based on breast DCE-MRI. Breast Cancer Res. 2017, 19, 57. [Google Scholar]
- Herrero Vicent, C.; Tudela, X.; Moreno Ruiz, P.; Pedralva, V.; Jiménez Pastor, A.; Ahicart, D. Machine Learning Models and Multiparametric Magnetic Resonance Imaging for the Prediction of Pathologic Response to Neoadjuvant Chemotherapy in Breast Cancer. Cancers 2022, 14, 3508. [Google Scholar] [CrossRef]
- Han, X.; Cao, W.; Wu, L.; Liang, C. Radiomics assessment of the tumor immune microenvironment to predict outcomes in breast cancer. Front. Immunol. 2022, 12, 5356. [Google Scholar] [CrossRef]
- Li, C.; Lu, N.; He, Z.; Tan, Y.; Liu, Y.; Chen, Y.; Wu, Z. A Noninvasive Tool Based on Magnetic Resonance Imaging Radiomics for the Preoperative Prediction of Pathological Complete Response to Neoadjuvant Chemotherapy in Breast Cancer. Ann. Surg. Oncol. 2022, 29, 7685–7693. [Google Scholar] [CrossRef]
- Granzier, R.W.; Ibrahim, A.; Primakov, S.P.; Samiei, S.; van Nijnatten, T.J.; de Boer, M.; Heuts, M.E. MRI-based radiomics analysis for the pretreatment prediction of pathologic complete tumor response to neoadjuvant systemic therapy in breast cancer patients: A multicenter study. Cancers 2021, 13, 2447. [Google Scholar] [CrossRef]
- Tustison, N.J.; Avants, B.B.; Cook, P.A.; Zheng, Y.; Egan, A.; Yushkevich, P.A.; Gee, J.C. N4ITK: Improved N3 bias correction. IEEE Trans. Med. Imaging 2010, 29, 1310–1320. [Google Scholar] [CrossRef]
- Collewet, G.; Strzelecki, M.; Mariette, F. Influence of MRI acquisition protocols and image intensity normalization methods on texture classification. Magn. Reson. Imaging 2004, 22, 81–91. [Google Scholar] [CrossRef]
- Hanley, J.A.; McNeil, B.J. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology 1982, 143, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Taha, A.A.; Hanbury, A.A. Metrics for evaluating 3D medical image segmentation: Analysis, selection, and tool. BMC Med. Imaging 2015, 15, 29. [Google Scholar] [CrossRef] [PubMed]
- Chamming’s, F.; Ueno, Y.; Ferré, R.; Kao, E.; Jannot, A.S.; Chong, J. Features from computerized texture analysis of breast cancers at pretreatment MR imaging are associated with response to neoadjuvant chemotherapy. Radiology 2018, 286, 412–420. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Lu, J.; Gao, C.; Zeng, J.; Zhou, C.; Lai, X.; Cai, W.; Xu, M. Predicting the response to neoadjuvant chemotherapy for breast cancer: Wavelet transforming radiomics in MRI. BMC Cancer 2020, 20, 100. [Google Scholar] [CrossRef]
- Hussain, L.; Huang, P.; Nguyen, T.; Lone, K.J.; Ali, A.; Khan, M.S. Machine learning classification of texture features of MRI breast tumor and peri-tumor of combined pre-and early treatment predicts pathologic complete response. BioMed. Eng. OnLine 2021, 20, 63. [Google Scholar] [CrossRef]
- Li, Q.; Xiao, Q.; Li, J.; Wang, Z.; Wang, H.; Gu, Y. Value of machine learning with multiphases ce-mri radiomics for early prediction of pathological complete response to neoadjuvant therapy in her2-positive invasive breast cancer. Cancer Manag. Res. 2021, 13, 5053–5062. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Kim, J.J.; Hwangbo, L.; Suh, H.B.; Kim, S.; Choo, K.S. Kinetic heterogeneity of breast cancer determined using computer-aided diagnosis of preoperative MRI scans: Relationship to distant metastasis-free survival. Radiology 2020, 295, 517–526. [Google Scholar] [CrossRef]
- Smith, A.S.; Weinstein, M.A.; Modic, M.T.; Pavlicek, W.; Rogers, L.R.; Budd, T.G.; Bukowski, R.M.; Purvis, J.D.; Weick, J.K.; Duchesneau, P.M. Magnetic resonance with marked T2-weighted images: Improved demonstration of brain lesions, tumor, and edema. Am. J. Neuroradiol. 1985, 6, 691–697. [Google Scholar] [CrossRef] [PubMed]
- Kociemba, A.; Pyda, M.; Katulska, K.; Łanocha, M.; Siniawski, A.; Janus, M.; Grajek, S. Comparison of diffusion-weighted with T2-weighted imaging for detection of edema in acute myocardial infarction. J. Cardiovasc. Magn. Reson. 2013, 15, 90. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Non-pCR | pCR | p Value | |
|---|---|---|---|
| n = 238 (89.8%) | n = 27 (10.2%) | ||
| Age, years | 49.2 ± 9.1 | 48.6 ± 6.2 | 0.975 |
| Tumor size, mm | 37.9 ± 21.3 | 22.1 ± 8.8 | <0.001 |
| ER expression, % | 85.6 ± 20.5 | 75.3 ± 30.7 | 0.058 |
| PR expression, % | 34.3 ± 36.3 | 28.9 ± 38.9 | 0.386 |
| Train | Validation | p Value | ||
|---|---|---|---|---|
| n = 195 (73.6%) | n = 70 (26.4%) | |||
| Pathology | non-pCR | 176 (90.3%) | 62 (88.6%) | 0.865 |
| pCR | 19 (9.7%) | 8 (11.4%) | ||
| Age, years | 48.5 ± 8.4 | 51.0 ± 9.9 | 0.043 | |
| Tumor size, mm | 35.0 ± 21.1 | 40.0 ± 19.9 | 0.086 | |
| ER expression, % | 85.2 ± 21.7 | 82.8 ± 22.5 | 0.408 | |
| PR expression, % | 30.9 ± 35.7 | 41.7 ± 38.0 | 0.016 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.; Kim, M.J.; Yoon, J.-H.; Han, K.; Kim, E.-K.; Sohn, J.H.; Lee, Y.H.; Yoo, Y. Machine Learning Predicts Pathologic Complete Response to Neoadjuvant Chemotherapy for ER+HER2- Breast Cancer: Integrating Tumoral and Peritumoral MRI Radiomic Features. Diagnostics 2023, 13, 3031. https://doi.org/10.3390/diagnostics13193031
Park J, Kim MJ, Yoon J-H, Han K, Kim E-K, Sohn JH, Lee YH, Yoo Y. Machine Learning Predicts Pathologic Complete Response to Neoadjuvant Chemotherapy for ER+HER2- Breast Cancer: Integrating Tumoral and Peritumoral MRI Radiomic Features. Diagnostics. 2023; 13(19):3031. https://doi.org/10.3390/diagnostics13193031
Chicago/Turabian StylePark, Jiwoo, Min Jung Kim, Jong-Hyun Yoon, Kyunghwa Han, Eun-Kyung Kim, Joo Hyuk Sohn, Young Han Lee, and Yangmo Yoo. 2023. "Machine Learning Predicts Pathologic Complete Response to Neoadjuvant Chemotherapy for ER+HER2- Breast Cancer: Integrating Tumoral and Peritumoral MRI Radiomic Features" Diagnostics 13, no. 19: 3031. https://doi.org/10.3390/diagnostics13193031