
Diagnostic Performance of ACR TI-RADS and ATA Guidelines in the Prediction of Thyroid Malignancy: A Prospective Single Tertiary Center Study and Literature Review
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
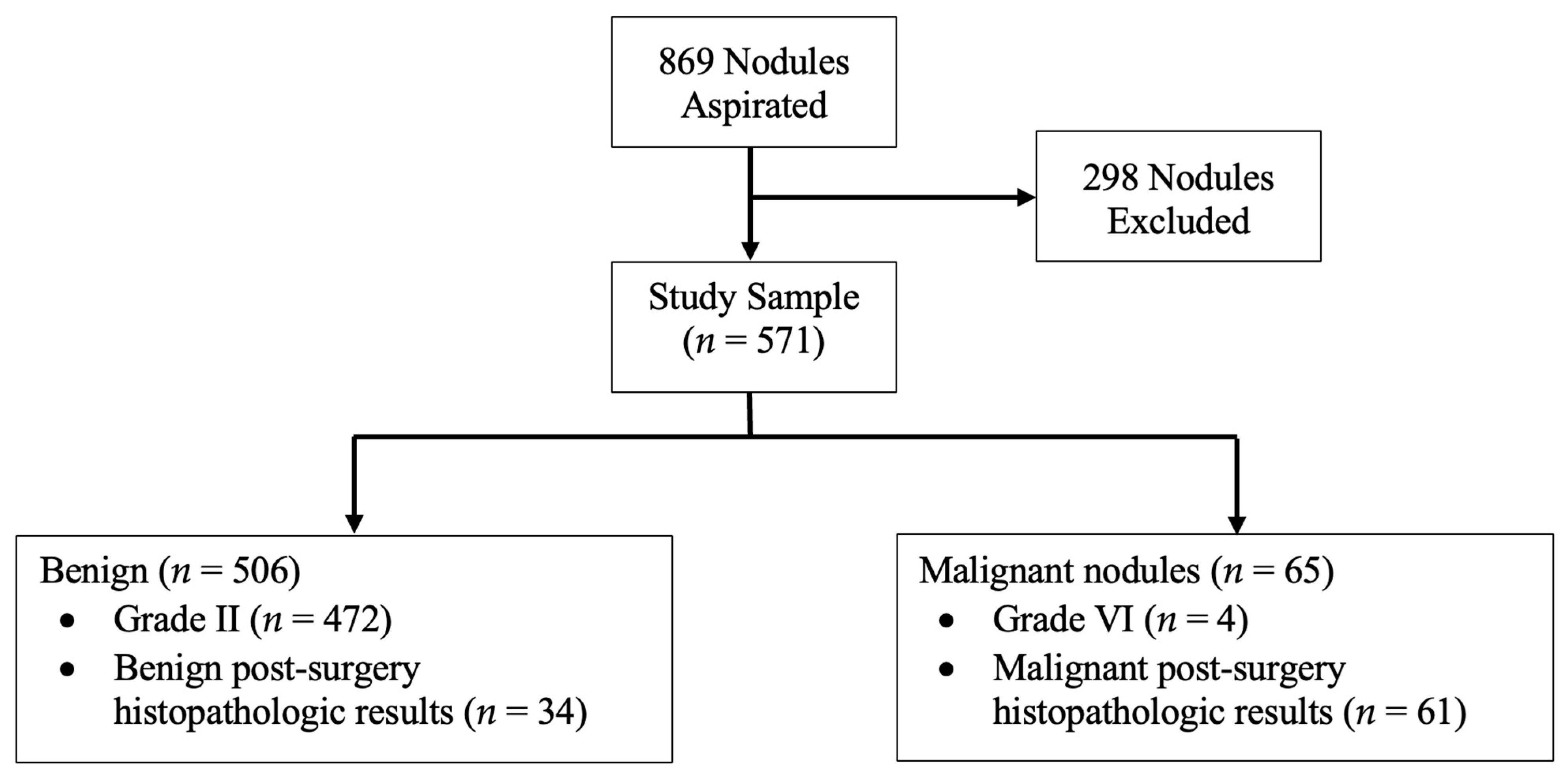
2.1. Patient Selection
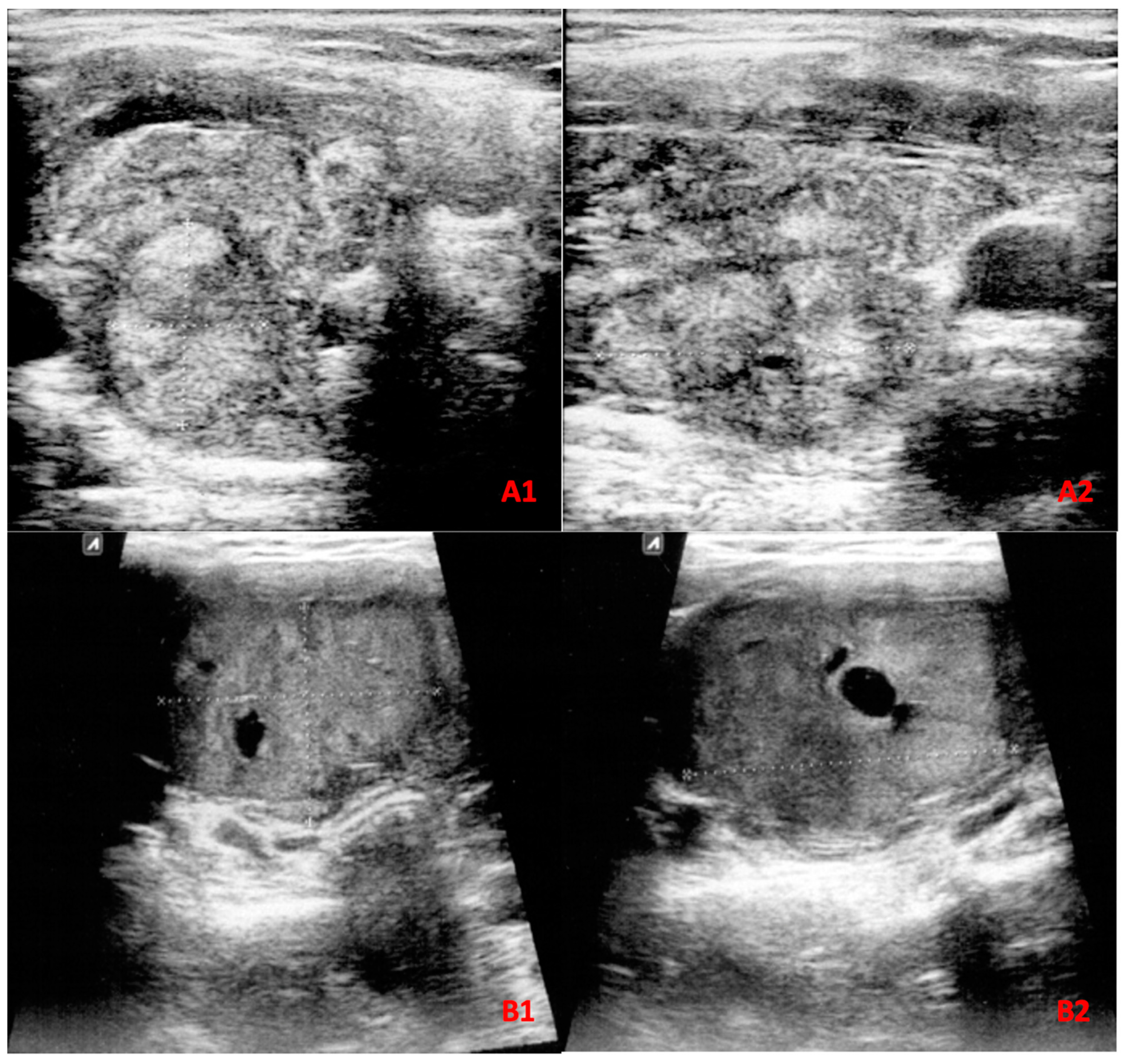
2.2. US Assessment
2.3. FNA Assessment
2.4. Statistical Analysis
3. Ethical Considerations
4. Results
4.1. Correlation of ACR TI-RADS and ATA Guidelines with Malignancy
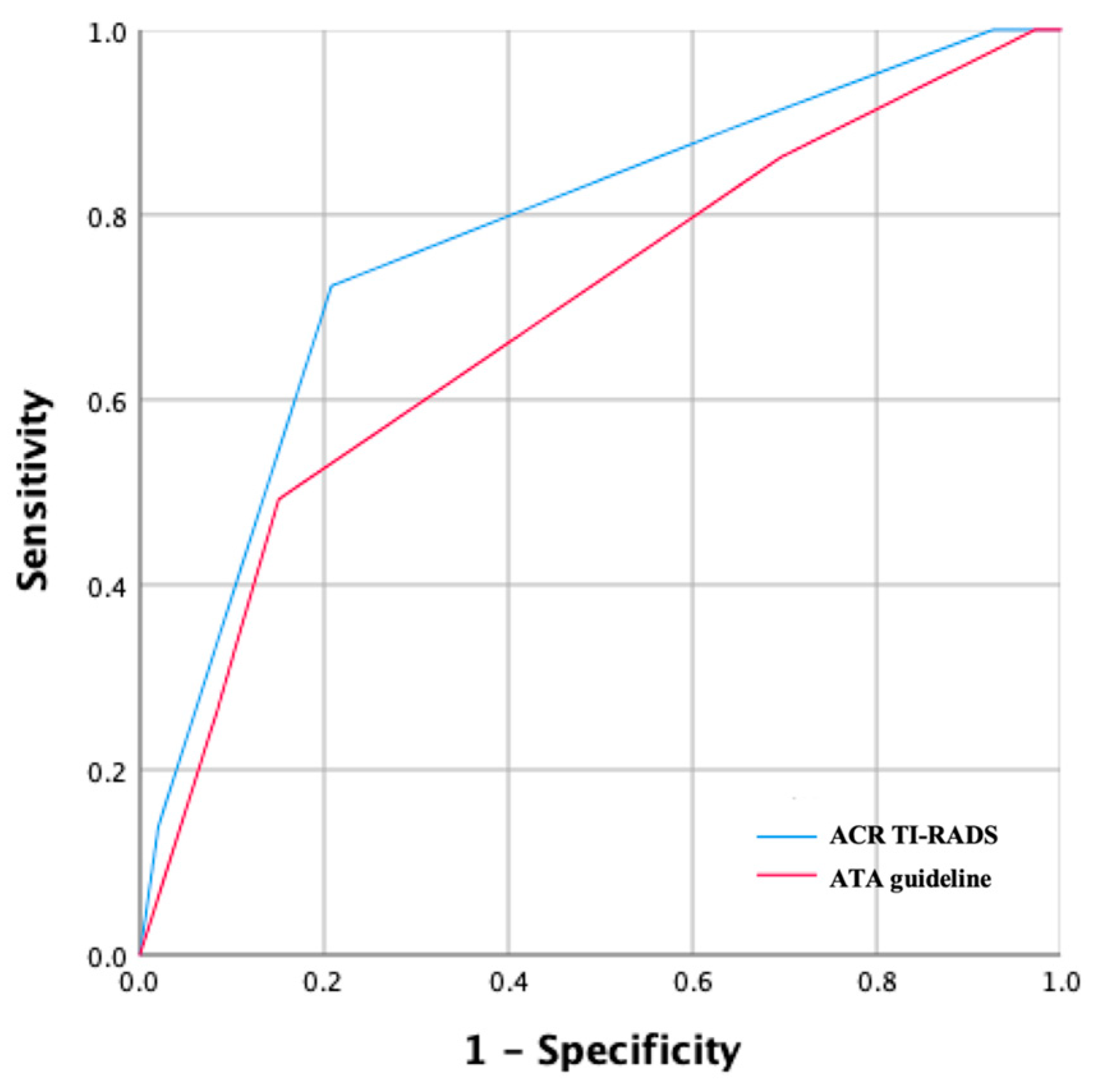
4.2. ACR TI-RADS and ATA Guidelines Diagnostic Performance
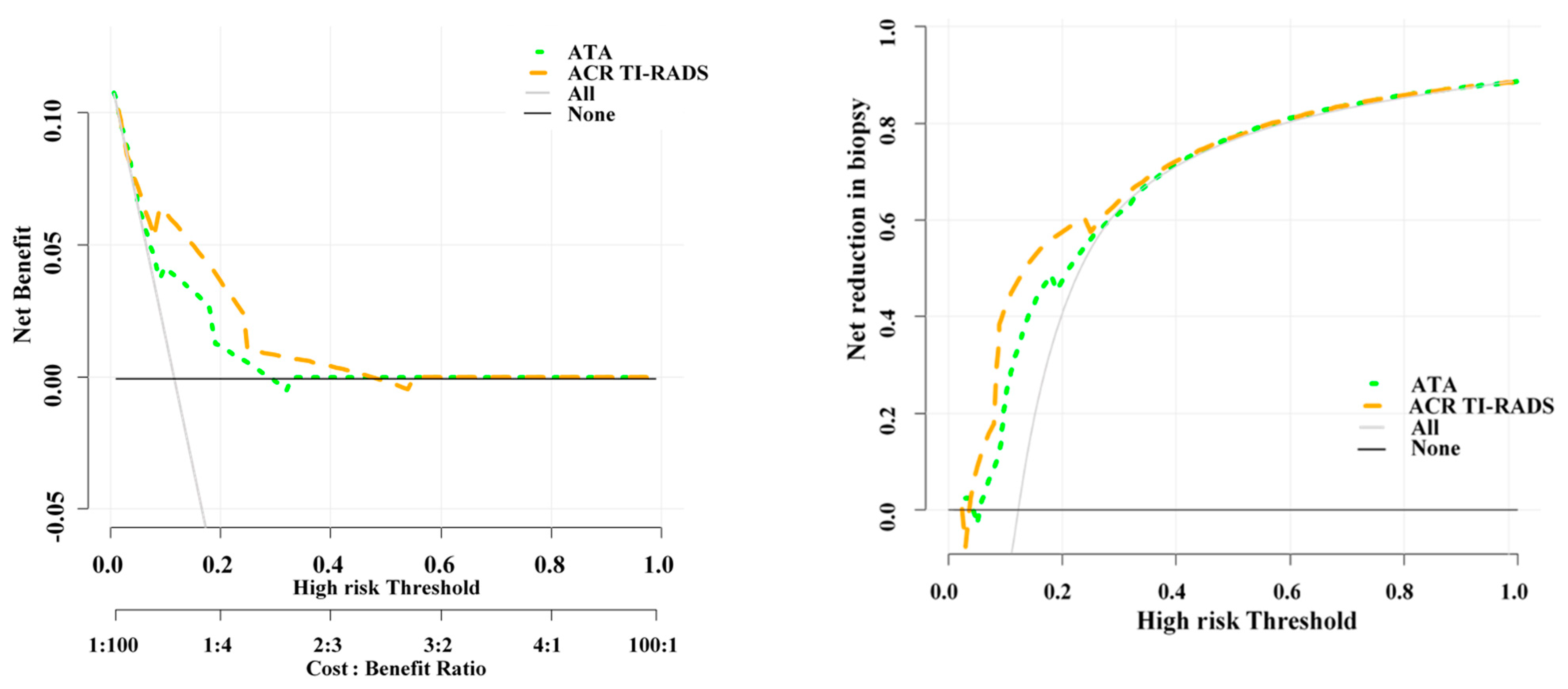
4.3. Unnecessary FNA Biopsy Rates of the Two Guidelines
4.4. Malignancy Predictors
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lim, H.; Devesa, S.S.; Sosa, J.A.; Check, D.; Kitahara, C.M. Trends in Thyroid Cancer Incidence and Mortality in the United States, 1974–2013. JAMA 2017, 317, 1338–1348. [Google Scholar] [CrossRef]
- Dean, D.S.; Gharib, H. Epidemiology of thyroid nodules. Best Pract. Res. Clin. Endocrinol. Metab. 2008, 22, 901–911. [Google Scholar] [CrossRef] [PubMed]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [PubMed]
- Frates, M.C.; Benson, C.B.; Charboneau, J.W.; Cibas, E.S.; Clark, O.H.; Coleman, B.G.; Cronan, J.J.; Doubilet, P.M.; Evans, D.B.; Goellner, J.R.; et al. Management of thyroid nodules detected at US: Society of Radiologists in Ultrasound consensus conference statement. Ultrasound Q. 2006, 22, 231–238, discussion 239–240. [Google Scholar] [CrossRef]
- Gharib, H.; Papini, E.; Paschke, R.; Duick, D.S.; Valcavi, R.; Hegedüs, L.; Vitti, P. AACE/AME/ETA Task Force on Thyroid Nodules American Association of Clinical Endocrinologists, Associazione Medici Endocrinologi, and European Thyroid Association Medical guidelines for clinical practice for the diagnosis and management of thyroid nodules: Executive summary of recommendations. Endocr. Pract. 2010, 16, 468–475. [Google Scholar] [CrossRef]
- Tessler, F.N.; Middleton, W.D.; Grant, E.G.; Hoang, J.K.; Berland, L.L.; Teefey, S.A.; Cronan, J.J.; Beland, M.D.; Desser, T.S.; Frates, M.C.; et al. ACR Thyroid Imaging, Reporting and Data System (TI-RADS): White Paper of the ACR TI-RADS Committee. J. Am. Coll. Radiol. 2017, 14, 587–595. [Google Scholar] [CrossRef]
- Lin, Y.; Lai, S.; Wang, P.; Li, J.; Chen, Z.; Wang, L.; Guan, H.; Kuang, J. Performance of current ultrasound-based malignancy risk stratification systems for thyroid nodules in patients with follicular neoplasms. Eur. Radiol. 2022, 32, 3617–3630. [Google Scholar] [CrossRef]
- Seifert, P.; Schenke, S.; Zimny, M.; Stahl, A.; Grunert, M.; Klemenz, B.; Freesmeyer, M.; Kreissl, M.C.; Herrmann, K.; Görges, R. Diagnostic Performance of Kwak, EU, ACR, and Korean TIRADS as Well as ATA Guidelines for the Ultrasound Risk Stratification of Non-Autonomously Functioning Thyroid Nodules in a Region with Long History of Iodine Deficiency: A German Multicenter Trial. Cancers 2021, 13, 4467. [Google Scholar] [CrossRef]
- Qiang, J.K.; Betel, C.; Hack, K.; Ghorab, Z.; Gilmour, J.; Mohammadi, M.; Burton, K.; Higgins, K.M.; Burton, K.; Higgins, K.M.; et al. Comparison of ACR-TIRADS to the ATA Guidelines for Thyroid Nodules: A Neck to Neck Comparison. Arch. Otolaryngol. Head Neck Surg. 2022, 1, 1–8. [Google Scholar] [CrossRef]
- Koc, A.M.; Adıbelli, Z.H.; Erkul, Z.; Sahin, Y.; Dilek, I. Comparison of diagnostic accuracy of ACR-TIRADS, American Thyroid Association (ATA), and EU-TIRADS guidelines in detecting thyroid malignancy. Eur. J. Radiol. 2020, 133, 109390. [Google Scholar] [CrossRef]
- Kim, J.-S.; Kim, B.G.; Stybayeva, G.; Hwang, S.H. Diagnostic Performance of Various Ultrasound Risk Stratification Systems for Benign and Malignant Thyroid Nodules: A Meta-Analysis. Cancers 2023, 15, 424. [Google Scholar] [CrossRef] [PubMed]
- Decaussin-Petrucci, M.; Albarel, F.; Leteurtre, E.; Borson-Chazot, F.; Cochand Priollet, B. SFE-AFCE-SFMN 2022 Consensus on the management of thyroid nodules: Recommendations in thyroid cytology: From technique to interpretation. Ann. D’endocrinologie 2022, 83, 389–394. [Google Scholar] [CrossRef]
- Er, D.; Dm, D.; Dl, C.-P. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. Available online: https://pubmed.ncbi.nlm.nih.gov/3203132/ (accessed on 7 February 2023).
- Ahmadi, S.; Herbst, R.; Oyekunle, T.; Strickland, K.; Roman, S.; Sosa, J.A. Using the ATA and ACR TI-RADS sonographic classifications as adjunctive predictors of malignancy for indeterminate thyroid nodules. Endocr. Pract. 2019, 25, 908–917. [Google Scholar] [CrossRef]
- Kim, M.J.; Shin, J.H.; Hahn, S.Y.; Oh, Y.L.; Kim, S.W.; Kim, T.H.; Lim, Y.; Lee, S. Ultrasonographic characteristics of Hürthle cell neoplasms: Prediction of malignancy. Ultrasonography 2022, 41, 689–697. [Google Scholar] [CrossRef]
- Kim, T.H.; Lim, J.A.; Ahn, H.Y.; Lee, E.K.; Min, H.S.; Won Kim, K.; Choi, Y.-H.; Park, Y.J.; Park, D.J.; Kim, K.H.; et al. Tumor size and age predict the risk of malignancy in Hürthle cell neoplasm of the thyroid and can therefore guide the extent of initial thyroid surgery. Thyroid 2010, 20, 1229–1234. [Google Scholar] [CrossRef]
- Strazisar, B.; Petric, R.; Sesek, M.; Zgajnar, J.; Hocevar, M.; Besic, N. Predictive factors of carcinoma in 279 patients with Hürthle cell neoplasm of the thyroid gland. J. Surg. Oncol. 2010, 101, 582–586. [Google Scholar] [CrossRef]
- Kim, D.H.; Kim, S.W.; Basurrah, M.A.; Lee, J.; Hwang, S.H. Diagnostic Performance of Six Ultrasound Risk Stratification Systems for Thyroid Nodules: A Systematic Review and Network Meta-Analysis. Am. J. Roentgenol. 2023, 220, 791–803. [Google Scholar] [CrossRef]
- Kim, H.K.; Kim, S.Y.; Lee, Y.S.; Soh, E.Y.; Chang, H.-S.; Park, C.S. Suspicious thyroid nodules 4 cm require a diagnostic lobectomy regardless of their benign fine needle aspiration results. Asian J. Surg. 2022, 45, 1113–1116. [Google Scholar] [CrossRef]
- Rastegar, H.; Torshizian, A.; Yaghoubi, M.A.; Khoshhal, N.; Asadi, M.; Morovatdar, N.; Mohebbi, M. Accuracy of fine-needle aspiration cytopathology to differentiate malignant and benign thyroid nodules with ≥4 cm diameter: A retrospective study. Diagn. Cytopathol. 2023, 51, 263–269. [Google Scholar] [CrossRef]
- Huh, S.; Lee, H.S.; Yoon, J.; Kim, E.-K.; Moon, H.J.; Yoon, J.H.; Park, V.Y.; Kwak, J.Y. Diagnostic performances and unnecessary US-FNA rates of various TIRADS after application of equal size thresholds. Sci. Rep. 2020, 10, 10632. [Google Scholar] [CrossRef]
- Sultan, L.R.; Xiong, H.; Zafar, H.M.; Schultz, S.M.; Langer, J.E.; Sehgal, C.M. Vascularity Assessment of Thyroid Nodules by Quantitative Color Doppler Ultrasound. Ultrasound Med. Biol. 2015, 41, 1287–1293. [Google Scholar] [CrossRef]
- Shin, J.J.; Caragacianu, D.; Randolph, G.W. Impact of thyroid nodule size on prevalence and post-test probability of malignancy: A systematic review: Impact of Thyroid Nodule Size on Malignancy. Laryngoscope 2015, 125, 263–272. [Google Scholar] [CrossRef]
- Floridi, C.; Cellina, M.; Buccimazza, G.; Arrichiello, A.; Sacrini, A.; Arrigoni, F.; Pompili, G.; Barile, A.; Carrafiello, G. Ultrasound imaging classifications of thyroid nodules for malignancy risk stratification and clinical management: State of the art. Gland Surg. 2019, 8, S233–S244. [Google Scholar] [CrossRef]
- Han, Z.; Huang, Y.; Wang, H.; Chu, Z. Multimodal ultrasound imaging: A method to improve the accuracy of diagnosing thyroid TI-RADS 4 nodules. J. Clin. Ultrasound 2022, 50, 1345–1352. [Google Scholar] [CrossRef]
- Baz, A.A.A.; Mohamed, A.H.I.; El-Esawy, Y.F.G.; El-kaffas, K.H. Conventional ultrasound, color Doppler, TI-RADS, and shear wave elastography for thyroid nodule differentiation: A study of efficacy compared with the histopathology results. Egypt. J. Radiol. Nucl. Med. 2021, 52, 103. [Google Scholar] [CrossRef]
- Chen, X.; Kutaiba, N.; Pearce, S.; Digby, S.; Van Gelderen, D. Application of Thyroid Imaging Reporting and Data System (TIRADS) guidelines to thyroid nodules with cytopathological correlation and impact on healthcare costs. Intern. Med. J. 2022, 52, 1366–1373. [Google Scholar] [CrossRef]
- Thedinger, W.; Raman, E.; Dhingra, J.K. Comparative Study of ACR TI-RADS and ATA 2015 for Ultrasound Risk Stratification of Thyroid Nodules. Otolaryngol. Head Neck Surg. 2022, 167, 35–40. [Google Scholar] [CrossRef]
- Qi, T.-Y.; Chen, X.; Liu, H.; Mao, L.; Chen, J.; He, B.-L.; Zhang, W.-B. Comparison of thyroid nodule FNA rates recommended by ACR TI-RADS, Kwak TI-RADS and ATA guidelines. Eur. J. Radiol. 2022, 148, 110152. [Google Scholar] [CrossRef]
- Gacayan, R.J.; Kasala, R.; Puno-Ramos, P.; Mojica, D.J.; Castro, K. Comparison of the Diagnostic Performance of Ultrasound-Based Thyroid Imaging Reporting and Data System (TIRADS) Classification with American Thyroid Association (ATA) Guidelines in the Prediction of Thyroid Malignancy in a Single Tertiary Center in Manila, Philippines. J. ASEAN Fed. Endocr. Soc. 2021, 36, 69–75. [Google Scholar] [CrossRef]
- Zhu, H.; Yang, Y.; Wu, S.; Chen, K.; Luo, H.; Huang, J. Diagnostic performance of US-based FNAB criteria of the 2020 Chinese guideline for malignant thyroid nodules: Comparison with the 2017 American College of Radiology guideline, the 2015 American Thyroid Association guideline, and the 2016 Korean Thyroid Association guideline. Quant Imaging Med. Surg. 2021, 11, 3604–3618. [Google Scholar] [CrossRef]
- Zhang, W.-B.; Xu, W.; Fu, W.-J.; He, B.-L.; Liu, H.; Deng, W.-F. Comparison of ACR TI-RADS, Kwak TI-RADS, ATA guidelines and KTA/KSThR guidelines in combination with SWE in the diagnosis of thyroid nodules. Clin. Hemorheol. Microcirc. 2021, 78, 163–174. [Google Scholar] [CrossRef]
- Godoi Cavalheiro, B.; Kober Nogueira Leite, A.; Luongo de Matos, L.; Palermo Miazaki, A.; Marcel Ientile, J.; Aurelio, V.; Kulcsar, M.; Roberto Cernea, C. Malignancy Rates in Thyroid Nodules Classified as Bethesda Categories III and IV: Retrospective Data from a Tertiary Center. Int. J. Endocrinol. Metab. 2017, 16, e12871. Available online: https://brieflands.com/articles/ijem-12871.html (accessed on 28 February 2023). [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total (n: 571) | Benign (n: 506) | Malignant (n: 65) | Malignancy Rate (%) | p-Value | |
|---|---|---|---|---|---|---|
| Age | Median (IQR) | 48 (41–57) | 48 (41–57) | 45 (30–56) | - | 0.197 |
| Range | 17–86 | 18–86 | 20–84 | |||
| Gender | Male | 51 (8.9) | 41 (8.1) | 10 (15.4) | 19.6 | 0.053 |
| Female | 520 (91.9) | 465 (91.9) | 55 (84.6) | 9.4 | ||
| Size | Median (IQR) | 3.0 (2.3–4.1) | 3.0 (2.2–4.0) | 4.0 (2.9–5.0) | - | <0.001 |
| Range | 1.0–13.7 | 1.0–13.7 | 1.5–7.0 | |||
| TSH | Median (IQR) | 2.0 (1.0–2.3) | 2.0 (1.0–2.3) | 2.0 (0.7–2.3) | - | 0.992 |
| Range | 0.3–15 | 0.5–14.8 | 0.3–15 | |||
| Composition | Predominantly cystic | 41 (7.2) | 41 (8.1) | 0 (0) | 0 | 0.165 |
| Spongiform | 2 (0.4) | 2 (0.4) | 0 (0) | 0 | ||
| Mixed | 198 (34.7) | 182 (36) | 16 (8.1) | 8.1 | ||
| Solid | 330 (57.8) | 281 (55.5) | 49(75.4) | 14.8 | ||
| Margin | Regular | 418 (73.2) | 387 (76.5) | 31 (47.7) | 7.4 | <0.001 |
| Irregular | 153 (26.8) | 119 (23.5) | 34 (52.3) | 22.2 | ||
| Echogenicity | Anechoic | 18 (3.2) | 18 (3.6) | 0 (0.0) | 0 | <0.001 |
| Isoechoic | 445 (77.9) | 410 (81) | 35 (53.8) | 7.9 | ||
| Hypoechoic | 49 (8.6) | 27 (5.3) | 22 (33.8) | 44.9 | ||
| Hyperechoic | 59 (10.3) | 51 (10.1) | 8 (12.3) | 13.6 | ||
| Calcifications | None | 489 (85.6) | 440 (87) | 49 (75.4) | 10 | <0.001 |
| Microcalcification | 39 (6.8) | 26 (5.1) | 13 (20) | 33.3 | ||
| Macrocalcification | 43 (7.5) | 40 (7.9) | 3 (4.6) | 7 | ||
| Shape | Taller-than-wide | 59 (10.3) | 38 (7.5) | 21 (32.3) | 35.6 | <0.001 |
| Wider-than-tall | 512 (89.7) | 468 (92.5) | 44 (67.7) | 8.6 | ||
| Vascularity | Central | 63 (11) | 43 (8.5) | 20 (30.8) | 31.7 | <0.001 |
| Peripheral | 508 (89) | 463 (91.5) | 45 (69.2) | 11.4 | ||
| Scoring System and Category | Benign n (%) | Malignant n (%) | Malignancy Rate (%) | Suggested Risk of Malignancy | p-Value (R) | |
|---|---|---|---|---|---|---|
| ACR TI-RADS | TR1 | 38 (7.5) | 0 (0.0) | 0.0 | 0–2% | <0.01 (0.320) |
| TR2 | 145 (28.7) | 7 (10.8) | 4.6 | 0–2% | ||
| TR3 | 218 (43.1) | 11 (16.9) | 4.8 | 5% | ||
| TR4 | 95 (18.8) | 38 (58.5) | 31.7 | 5–20% | ||
| TR5 | 10 (2) | 9 (13.8) | 47.4 | >20% | ||
| ATA guideline | Benign | 14 (2.8) | 0 (0) | 0 | <1% | <0.01 (0.230) |
| Very low suspicion | 140(27.7) | 9 (13.8) | 6 | <3% | ||
| Low suspicion | 275 (54.5) | 24 (36.9) | 8 | 5–10% | ||
| Intermediate suspicion | 34 (6.7) | 15 (23.1) | 30.6 | 10–20% | ||
| High suspicion | 42(8.3) | 17 (26.2) | 28.8 | >70% | ||
| Scoring System | Cut-Off | Accuracy (95% CI) | AUC (95% CI) | Sensitivity (95% CI) | Specificity (95% CI) | PPV (95% CI) | NPV (95% CI) | |
|---|---|---|---|---|---|---|---|---|
| Overall n = 571 | ACR TI-RADS | TR4/TR5 | 78.4 (74.8–81.76) | 0.776 (0.740–0.810) | 72.3 (59.8–82.7) | 79.2 (75.4–82.7) | 30.9 (26.3–36) | 95.7 (93.7–97) |
| ATA guideline | Intermediate/high suspicion | 80.9 (77.4–84.0) | 0.691 (0.651–0.728) | 49.2 (36.6–61.9) | 84.9 (81.5–87.9) | 29.6 (23.4–36.7) | 92.8 (91.1–94.3) | |
| p-value | 0.203 | 0.03 | 0.003 | < 0.001 | - | - | ||
| Nodules ≥ 4 cm n = 169 | ACR TI-RADS | TR4/TR5 | 78.7 (71.7–84.6) | 0.806 (0.740–0.862) | 78.4 (61.8–90.2) | 78.8 (71.0–85.3) | 50.0 (40.1–59.0) | 93.1 (87.9–96.1) |
| ATA guideline | Intermediate/high suspicion | 80.5 (73.7–86.2) | 0.706 (0.632–0.772) | 43.2 (27.1–60.5) | 89.8 (83.4–94.3) | 53.3 (38.1–68.0) | 84.5 (81.5–88.6) | |
| p-value | 0.885 | 0.09 | 0.002 | 0.011 | - | - | ||
| Scoring System | No. of Indicated Biopsies | No. of Malignant Nodules among FNAB Indicated Nodules | Unnecessary FNAB Rate | No. of Missed Malignant Nodules | Detection Rate | |
|---|---|---|---|---|---|---|
| ACR TI-RADS | Total | 293 | 58 | 80.2% | 7 | 89.2% |
| TR5 | 19 | 9 | 52.6% | 0 | 100% | |
| TR4 | 116 | 38 | 67.2% | 0 | 100% | |
| TR3 | 158 | 11 | 93% | 0 | 100% | |
| TR2 | 0 | 0 | - | 7 | 0% | |
| ATA Guideline | Total | 527 | 64 | 87.8% | 1 | 98.4% |
| High suspicion | 59 | 17 | 71.2% | 0 | 100% | |
| Intermediate suspicion | 49 | 15 | 69.4% | 0 | 100% | |
| Low suspicion | 291 | 24 | 91.8% | 0 | 100% | |
| Very low suspicion | 128 | 8 | 93.7% | 1 | 90% | |
| Parameters | Univariate Analysis (Crude) | Multivariate Analysis (Adjusted) * | ||||||
|---|---|---|---|---|---|---|---|---|
| β | SE | OR | p-Value | β | SE | OR | p-Value | |
| Microcalcification | 1.50 | 0.37 | 4.48 (2.16–9.30) | <0.001 | 1.64 | 0.45 | 5.17 (2.10–12.69) | <0.001 |
| Hypoechogenicity | 2.25 | 0.33 | 9.54 (4.93–18.47) | <0.001 | 2.12 | 0.43 | 8.34 (3.57–19.45) | <0.001 |
| Irregular margin | 1.27 | 0.26 | 3.56 (2.10–6.04) | <0.001 | 0.74 | 0.34 | 2.09 (1.06–4.13) | 0.032 |
| Taller-than-wide shape | 1.77 | 0.31 | 5.87 (3.17–10.88) | <0.001 | 1.90 | 0.40 | 6.73 (3.07–14.77) | <0.001 |
| Central vascularity | 1.56 | 0.30 | 4.78 (2.58–8.82) | <0.001 | 1.07 | 0.39 | 2.93 (1.35–6.38) | 0.006 |
| Size | 0.32 | 0.08 | 1.39 (1.18–1.63) | <0.001 | 0.31 | 0.08 | 1.36 (1.14–1.61) | <0.001 |
| Male gender | 0.72 | 0.38 | 2.06 (0.978–4.34) | 0.057 | 1.20 | 0.46 | 3.35 (1.34–8.36) | <0.009 |
| Study (Year) | No. of Nodules | Age | Gender (F/M) | Mean Nodule’s Size | Optimal Cut-Off Value | Sensitivity (%) | Specificity (%) | AUC | Unnecessary FNA Rate (%) | Reference Test | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ATA Guideline | ACR TI-RADS | ATA Guideline | ACR TI-RADS | ATA Guideline | ACR TI-RADS | ATA Guideline | ACR TI-RADS | ATA Guideline | ACR TI-RADS | ||||||
| Thedinger et al. (2022) [28] | 236 | 58.7 ± 0.6 | 538/182 | - | Indication of FNA by guideline | FNA indication | 81.6 | 73.7 | 54.5 | 27.0 | - | - | 72.3 | 82.3 | Cytology |
| Qi et al. (2022) [29] | 820 | 44.5 ± 13.4 | 619/201 | 13 mm | High suspicion | TR5 | 92.1 | 79.3 | 88.3 | 93.2 | 0.921 | 0.925 | 47.4 | 26.3 | Cytology or pathology |
| Lin et al. (2022) [7] | 455 | 43.5 ± 14.3 | 216/113 | 3.6 ± 1.7 cm | High and intermediate suspicion | TR4-TR5 | 23.3 | 38.8 | 87.7 | 80.2 | 0.555 | 0.595 | 90.5 | 65.3 | Pathology |
| Gacayan et al. (2021) [30] | 197 | 53 (21–77) | 103/18 | - | High and intermediate suspicion | TR4-TR5 | 88.2 | 100 | 57.8 | 52.2 | - | - | - | - | Cytology |
| Qiang et al. (2021) [9] | 417 | 58.7 ± 14 | 334/83 | - | Indication of FNA by guideline | FNA indication | 97 | 70 | 11 | 29 | - | - | Cytology or pathology | ||
| Zhu et al. (2021) [31] | 2309 | 53.2 ± 12.7 | 1336/361 | 13.1 ± 10.6 mm | High suspicion | TR5 | 96.51 | 93.71 | 67.1 | 74.82 | 0.824 | 0.854 | 29.41 | 29.41 | Cytology or pathology |
| Zhang et al. (2021) [32] | 566 | 47.4 ± 13.4 | 442/124 | 11.4 ± 5.8 mm | High suspicion | TR5 | 89.7 | 86.5 | 84.4 | 88.4 | 0.907 | 0.894 | - | - | Cytology or pathology |
| Seifert et al. (2021) [8] | 1211 | 51 ± 14 | 604/249 | 26 ± 13 mm | High suspicion | TR5 | 77 | 68 | 80 | 80 | 0.795 | 0.801 | - | - | Cytology or pathology |
| Huh et al. (2021) [21] | 1384 | 50.2 ± 13.6 | 1062/239 | 23.2 ± 12.6 mm | Indication of FNA by guideline | FNA indication | 98.6 | 80.4 | 19.9 | 62.2 | 0.592 | 0.713 | 75.3 | 63.8 | Cytology or pathology |
| Chen et al. (2022) [27] | 146 | 56.7 | 99/26 | median: 2.3 cm | High and intermediate suspicion | TR4-TR5 | 91 | 75 | 26 | 41 | - | - | 68.5 | 54.8 | Cytology or pathology |
| Koc et al. (2020) [10] | 492 | 52 (18–84) | 375/85 | - | High and intermediate suspicion | TR4-TR5 | 82.22 | 48.89 | 53.47 | 60.63 | 0.740 | 0.550 | 88.8 | 80.8 | Cytology or pathology |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Torshizian, A.; Hashemi, F.; Khoshhal, N.; Ghodsi, A.; Rastegar, H.; Mousavi, Z.; Dadgar Moghadam, M.; Mohebbi, M. Diagnostic Performance of ACR TI-RADS and ATA Guidelines in the Prediction of Thyroid Malignancy: A Prospective Single Tertiary Center Study and Literature Review. Diagnostics 2023, 13, 2972. https://doi.org/10.3390/diagnostics13182972
Torshizian A, Hashemi F, Khoshhal N, Ghodsi A, Rastegar H, Mousavi Z, Dadgar Moghadam M, Mohebbi M. Diagnostic Performance of ACR TI-RADS and ATA Guidelines in the Prediction of Thyroid Malignancy: A Prospective Single Tertiary Center Study and Literature Review. Diagnostics. 2023; 13(18):2972. https://doi.org/10.3390/diagnostics13182972
Chicago/Turabian StyleTorshizian, Ashkan, Fatemeh Hashemi, Nastaran Khoshhal, Alireza Ghodsi, Houra Rastegar, Zohreh Mousavi, Maliheh Dadgar Moghadam, and Masoud Mohebbi. 2023. "Diagnostic Performance of ACR TI-RADS and ATA Guidelines in the Prediction of Thyroid Malignancy: A Prospective Single Tertiary Center Study and Literature Review" Diagnostics 13, no. 18: 2972. https://doi.org/10.3390/diagnostics13182972