
Assessing the Use of Telepresence-Guided Video-Based Head and Neck Ultrasound Training: A Step towards Minimizing Dependence on Human Resources?

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participant Recruitment
2.2. Technical Setup
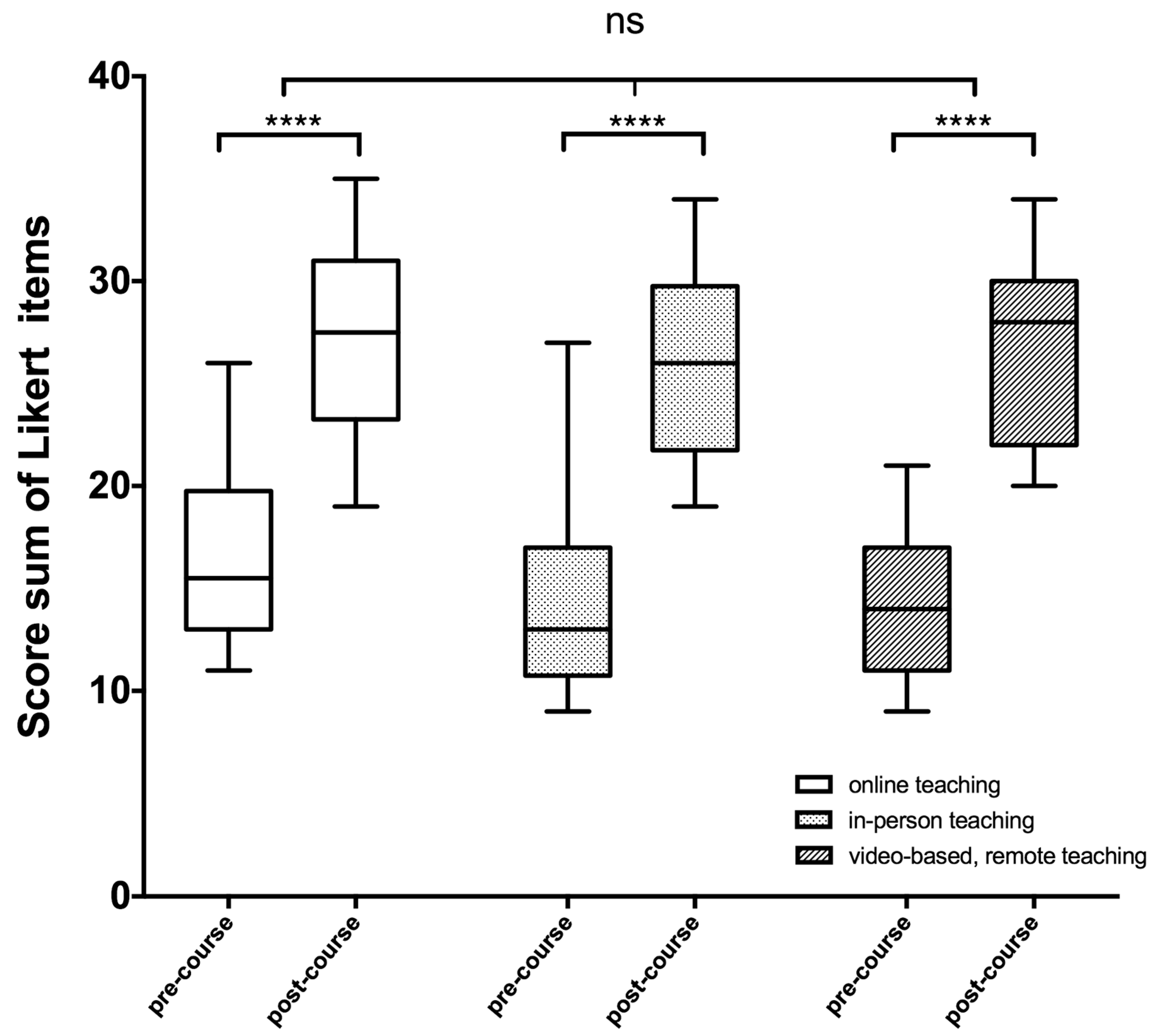
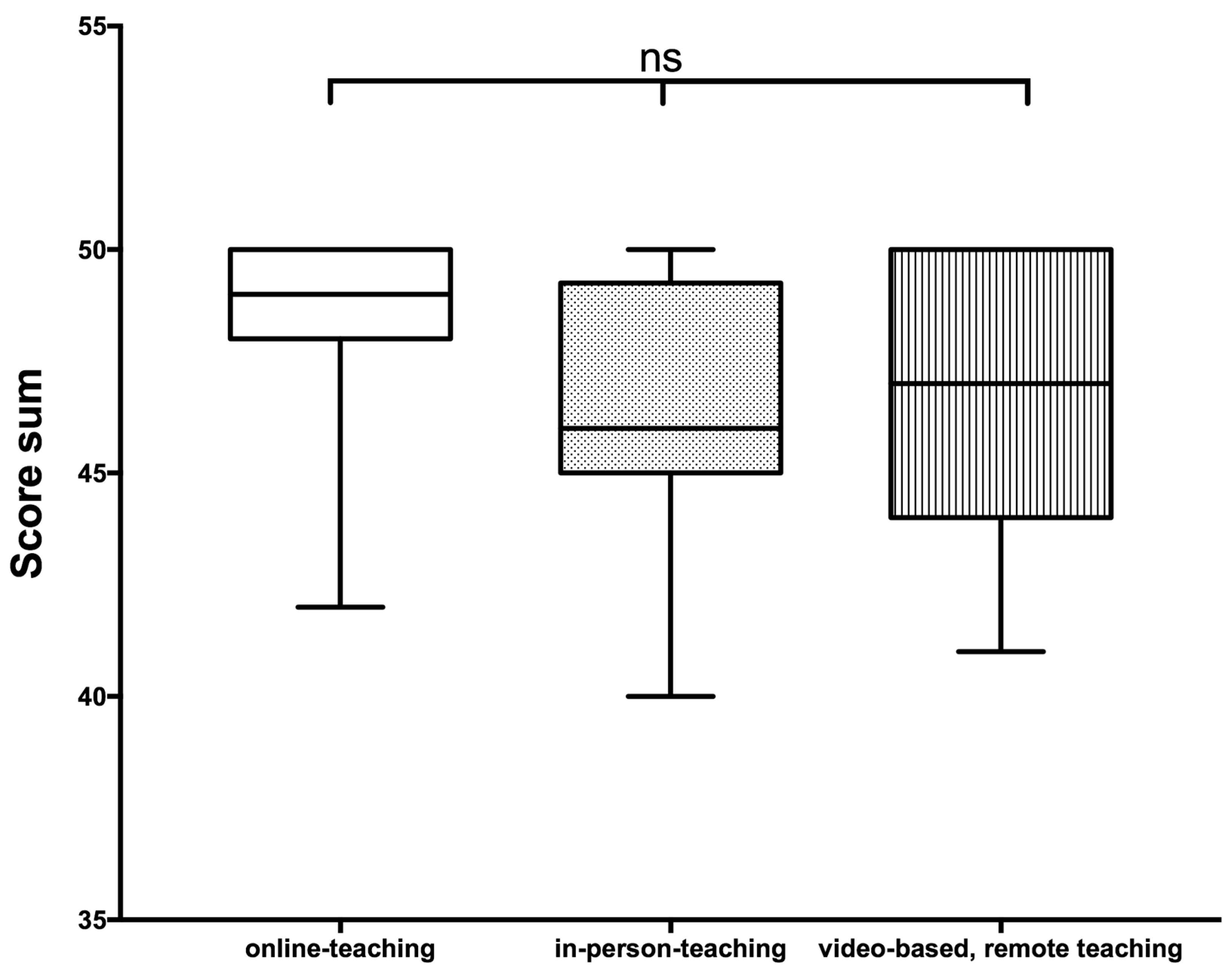
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Solomon, S.D.; Saldana, F. Point-of-Care Ultrasound in Medical Education—Stop Listening and Look. N. Engl. J. Med. 2014, 370, 1083–1085. [Google Scholar] [CrossRef] [PubMed]
- Badran, K.; Jani, P.; Berman, L. Otolaryngologist-Performed Head and Neck Ultrasound: Outcomes and Challenges in Learning the Technique. J. Laryngol. Otol. 2014, 128, 447–453. [Google Scholar] [CrossRef]
- Swamy, M.; Searle, R.F. Anatomy Teaching with Portable Ultrasound to Medical Students. BMC Med. Educ. 2012, 12, 99. [Google Scholar] [CrossRef]
- Tarique, U.; Tang, B.; Singh, M.; Kulasegaram, K.M.; Ailon, J. Ultrasound Curricula in Undergraduate Medical Education: A Scoping Review. J. Ultrasound Med. 2018, 37, 69–82. [Google Scholar] [CrossRef] [PubMed]
- Hammoudi, N.; Arangalage, D.; Boubrit, L.; Renaud, M.C.; Isnard, R.; Collet, J.-P.; Cohen, A.; Duguet, A. Ultrasound-Based Teaching of Cardiac Anatomy and Physiology to Undergraduate Medical Students. Arch. Cardiovasc. Dis. 2013, 106, 487–491. [Google Scholar] [CrossRef]
- Patel, S.G.; Benninger, B.; Mirjalili, S.A. Integrating Ultrasound into Modern Medical Curricula. Clin. Anat. 2017, 30, 452–460. [Google Scholar] [CrossRef]
- Bahner, D.P.; Goldman, E.; Way, D.; Royall, N.A.; Liu, Y.T. The State of Ultrasound Education in U.S. Medical Schools. Acad. Med. 2014, 89, 1681–1686. [Google Scholar] [CrossRef]
- He, X.; Shelden, D.; Kraftson, A.; Else, T.; Auchus, R.J. A Virtual Teaching Clinic for Virtual Care during the COVID-19 Pandemic. Clin. Diabetes Endocrinol. 2020, 6, 25. [Google Scholar] [CrossRef]
- Goldhamer, M.E.J.; Pusic, M.V.; Co, J.P.T.; Weinstein, D.F. Can Covid Catalyze an Educational Transformation? Competency-Based Advancement in a Crisis. N. Engl. J. Med. 2020, 383, 1003–1005. [Google Scholar] [CrossRef] [PubMed]
- Evans, D.J.R.; Bay, B.H.; Wilson, T.D.; Smith, C.F.; Lachman, N.; Pawlina, W. Going Virtual to Support Anatomy Education: A STOPGAP in the Midst of the COVID-19 Pandemic. Anat. Sci. Educ. 2020, 13, 279–283. [Google Scholar] [CrossRef]
- Soled, D.; Goel, S.; Barry, D.; Erfani, P.; Joseph, N.; Kochis, M.; Uppal, N.; Velasquez, D.; Vora, K.; Scott, K.W. Medical Student Mobilization during a Crisis: Lessons from a COVID-19 Medical Student Response Team. Acad. Med. 2020, 95, 1384–1387. [Google Scholar] [CrossRef]
- Camargo, C.P.; Tempski, P.Z.; Busnardo, F.F.; Martins, M.D.A.; Gemperli, R. Online Learning and COVID-19: A Meta-Synthesis Analysis. Clinics 2020, 75, e2286. [Google Scholar] [CrossRef]
- Holtel, M.R. Emerging Technology in Head and Neck Ultrasonography. Otolaryngol. Clin. N. Am. 2010, 43, 1267–1274. [Google Scholar] [CrossRef]
- Siegel-Richman, Y.; Kendall, J. Establishing an Ultrasound Curriculum in Undergraduate Medical Education: How Much Time Does It Take? J. Ultras. Med. 2018, 37, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Stone, N.N.; Wilson, M.P.; Griffith, S.H.; Immerzeel, J.; Debruyne, F.; Gorin, M.A.; Brisbane, W.; Orio, P.F.; Kim, L.S.; Stone, J.J. Remote Surgical Education Using Synthetic Models Combined with an Augmented Reality Headset. Surg. Open Sci. 2022, 10, 27–33. [Google Scholar] [CrossRef]
- Martin, D.A.; Guillen, M.; Farro, A.; Condori, M.; Dreyfuss, A.; Nagdev, A. Role of Tele-Ultrasound for Teaching Ultrasound-Guided Nerve Blocks in the Emergency Department: A Case Series from Peru. Clin. Pract. Cases Emerg. Med. 2022, 6, 204–207. [Google Scholar] [CrossRef]
- Herbert, A.; Russell, F.M.; Zahn, G.; Zakeri, B.; Motzkus, C.; Wallach, P.M.; Ferre, R.M. Point-of-Care Ultrasound Education During a Pandemic: From Webinar to Progressive Dinner-Style Bedside Learning. Cureus 2022, 14, e25141. [Google Scholar] [CrossRef] [PubMed]
- Handaya, A.Y.; Fauzi, A.R.; Andrew, J.; Hanif, A.S.; Tjendra, K.R.; Aditya, A.F.K. Effectiveness of Tutorial Videos Combined with Online Classes in Surgical Knotting Course during COVID-19 Pandemic: A Cohort Study. Ann. Med. Surg. 2021, 69, 102751. [Google Scholar] [CrossRef] [PubMed]
- Olivares-Perez, M.E.; Graglia, S.; Harmon, D.J.; Klein, B.A. Virtual Anatomy and Point-of-care Ultrasonography Integration Pilot for Medical Students. Anat. Sci. Educ. 2022, 15, 464–475. [Google Scholar] [CrossRef]
- Bailey, C.E.; Grauer, J.S.; Chen, P.G.; Rangarajan, S.V.; Chan, Y.; Tewfik, M.A.; Marino, M.J.; Torabi, M.; Le, C.H.; Chang, E.H. Development of a Self-directed Sinonasal Surgical Anatomy Video Curriculum: Phase 1 Validation. Int. Forum Allergy Rhinol. 2021, 11, 1570–1576. [Google Scholar] [CrossRef]
- Pillong, L.; Bozzato, A.; Hecker, D.; Bozzato, V.; Schick, B.; Kulas, P. “AHead Start or a Pain in TheNeck?”—Establishment and Evaluation of a Video-Based “Hands-On” Head and Neck Ultrasound Course. Diagnostics 2022, 12, 1239. [Google Scholar] [CrossRef]
- Weiskittel, T.M.; Lachman, N.; Bhagra, A.; Andersen, K.; St. Jeor, J.; Pawlina, W. Team-Based Ultrasound Objective Structured Practice Examination (OSPE) in the Anatomy Course. Anat. Sci. Educ. 2021, 14, 377–384. [Google Scholar] [CrossRef]
- Situ-LaCasse, E.; Acuña, J.; Huynh, D.; Amini, R.; Irving, S.; Samsel, K.; Patanwala, A.E.; Biffar, D.E.; Adhikari, S. Can Ultrasound Novices Develop Image Acquisition Skills after Reviewing Online Ultrasound Modules? BMC Med. Educ. 2021, 21, 175. [Google Scholar] [CrossRef]
- Valenciaga, A.; Ivancic, R.J.; Khawaja, R.; Way, D.P.; Bahner, D.P. Efficacy of an Integrated Hands-On Thyroid Ultrasound Session for Medical Student Education. Cureus 2021, 13, e12421. [Google Scholar] [CrossRef] [PubMed]
- Dreher, S.M.; DePhilip, R.; Bahner, D. Ultrasound Exposure During Gross Anatomy. J. Emerg. Med. 2014, 46, 231–240. [Google Scholar] [CrossRef]
- Rempell, J.S.; Saldana, F.; DiSalvo, D.; Kumar, N.; Stone, M.B.; Chan, W.; Luz, J.; Noble, V.E.; Liteplo, A.; Kimberly, H.; et al. Pilot Point-of-Care Ultrasound Curriculum at Harvard Medical School: Early Experience. West. J. Emerg. Med. 2016, 17, 734–740. [Google Scholar] [CrossRef] [PubMed]
- Bernard, S.; Richardson, C.; Hamann, C.R.; Lee, S.; Dinh, V.A. Head and Neck Ultrasound Education—A Multimodal Educational Approach in the Predoctoral Setting. J. Ultras. Med. 2015, 34, 1437–1443. [Google Scholar] [CrossRef] [PubMed]
- Oberoi, M.K.; Perera, N.C.; Reynaga, J.; Yoo, B.R.; Miller, C.C.; Lockhart, W.; Entezampour, M.; Friedman, L. Students Teaching Students: Student-Led Ultrasound Curriculum in Medical School Education. Cureus 2021, 13, e19332. [Google Scholar] [CrossRef]
- Russell, F.M.; Herbert, A.; Peterson, D.; Wallach, P.M.; Ferre, R.M. Assessment of Medical Students’ Ability to Integrate Point-of-Care Cardiac Ultrasound Into a Case-Based Simulation after a Short Intervention. Cureus 2022, 14, e27513. [Google Scholar] [CrossRef]
- Eimer, C.; Duschek, M.; Jung, A.E.; Zick, G.; Caliebe, A.; Lindner, M.; Weiler, N.; Elke, G. Video-Based, Student Tutor- versus Faculty Staff-Led Ultrasound Course for Medical Students—A Prospective Randomized Study. BMC Med. Educ. 2020, 20, 512. [Google Scholar] [CrossRef]
- Kameda, T.; Koibuchi, H.; Konno, K.; Taniguchi, N. Self-Learning Followed by Telepresence Instruction of Focused Cardiac Ultrasound with a Handheld Device for Medical Students: A Preliminary Study. J. Med. Ultrason. 2022, 49, 415–423. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Self-Assessment Questionnaire | |||||
|---|---|---|---|---|---|
| Age | |||||
| Sex | |||||
| Clinical Semester | |||||
| Pre-course Ultrasound Experience | YES | NO | |||
| If YES, pre-course knowledge gained through | Courses | Literature | Internships | ||
| Self-assessment | Locating and visualizing the organ | 1 = is not possible | 2 = is rather possible | 3 = Is possible | 4 = is confidently possible |
| Floor of mouth | |||||
| Larynx | |||||
| Trachea | |||||
| Thyroid gland | |||||
| Esophagus | |||||
| Salivary glands | |||||
| Vessels | |||||
| Lymph nodes | |||||
| Pathologies | |||||
| The time allocated for the course was sufficient | 0 | 1 | 2 | 3 | 4 |
| The teaching materials provided were sufficient | 0 | 1 | 2 | 3 | 4 |
| The comments of the tutors were helpful | 0 | 1 | 2 | 3 | 4 |
| The content of the course was sufficient | 0 | 1 | 2 | 3 | 4 |
| The tasks were clearly formulated | 0 | 1 | 2 | 3 | 4 |
| The teaching materials provided were clearly structured | 0 | 1 | 2 | 3 | 4 |
| The learning content did not overwhelm me | 0 | 1 | 2 | 3 | 4 |
| The group size was comfortable | 0 | 1 | 2 | 3 | 4 |
| The explanations of the tutors were well understandable | 0 | 1 | 2 | 3 | 4 |
| My questions were answered sufficiently | 0 | 1 | 2 | 3 | 4 |
| The feedback on my skills was sufficient | 0 | 1 | 2 | 3 | 4 |
| I consider the course format suitable for knowledge transfer | 0 | 1 | 2 | 3 | 4 |
| It would be useful to extend this course to other organ systems | 0 | 1 | 2 | 3 | 4 |
| Assessment Category | Score Points | |
|---|---|---|
| manual skills | max. 8 points | |
| Situs orientation | 0–2 | Landmarks and guiding structures are recognized: 0 = no, 1 = partially 2 = relevant structures can be named |
| Transducer positioning | 0–2 | 0 = no orientation, 1 = partial orientation, 2 = complete orientation |
| Adjusting the focus position | 0–2 | 0 = no focus, 1 = partial focus, 2 = focus is adjusted |
| Adjusting gain | 0–2 | 0 = no gain, 1 = partial gain, 2 = gain is adjusted |
| interaction with the patient | max. 4 points | |
| Patient positioning | 0–2 | 0 = no adjustment of patient position, 1 = partial adjustment of patient position, 2 = patient position is adjusted and properly optimized |
| systematics of the examination | 0–2 | 0 = no systematics, 1 = partial systematics, 2 = good systematics |
| Visualization of the organs | max. 20 points | |
| Measuring | 0–4 | 0–4 organs or structures are measured correctly |
| Demonstration | 0–16 | 0–16 organs are displayed |
| Explanation of the anatomy shown | max. 18 points | |
| Normal findings | 0–14 | 0–16 organs are examined |
| Pathologies | 0–4 | 0–4 pathologies are assessed, if no pathology then 4 points. |
| Score total points | max. 50 points |
| Online Course | In-Person Course | Video-Instruction-Based Remote Teaching | |
|---|---|---|---|
| Age | 24 (21–29) | 24 (22–34) | 23 (19–31) |
| Gender (female:male) | 6:6 | 14:8 | 9:26 |
| Semester | 8 (6–10) | 6 (5–8) | 7 (4–10) |
| Ultrasound-knowledge/experience pre-course (courses, internships, and literature) | 66.6% | 45.5% | 42.9% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kulas, P.; Schick, B.; Helfrich, J.; Bozzato, A.; Hecker, D.J.; Pillong, L. Assessing the Use of Telepresence-Guided Video-Based Head and Neck Ultrasound Training: A Step towards Minimizing Dependence on Human Resources? Diagnostics 2023, 13, 2828. https://doi.org/10.3390/diagnostics13172828
Kulas P, Schick B, Helfrich J, Bozzato A, Hecker DJ, Pillong L. Assessing the Use of Telepresence-Guided Video-Based Head and Neck Ultrasound Training: A Step towards Minimizing Dependence on Human Resources? Diagnostics. 2023; 13(17):2828. https://doi.org/10.3390/diagnostics13172828
Chicago/Turabian StyleKulas, Philipp, Bernhard Schick, Johanna Helfrich, Alessandro Bozzato, Dietmar J. Hecker, and Lukas Pillong. 2023. "Assessing the Use of Telepresence-Guided Video-Based Head and Neck Ultrasound Training: A Step towards Minimizing Dependence on Human Resources?" Diagnostics 13, no. 17: 2828. https://doi.org/10.3390/diagnostics13172828