
Electric Bioimpedance Sensing for the Detection of Head and Neck Squamous Cell Carcinoma
 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients Selection
2.2. SmartProbe Device
2.3. Measurement Procedures
2.4. Matching Process with Histopathology
2.5. Data Analysis
2.6. Classifiers
3. Results
3.1. Clinico-Pathological Features of the Cohort
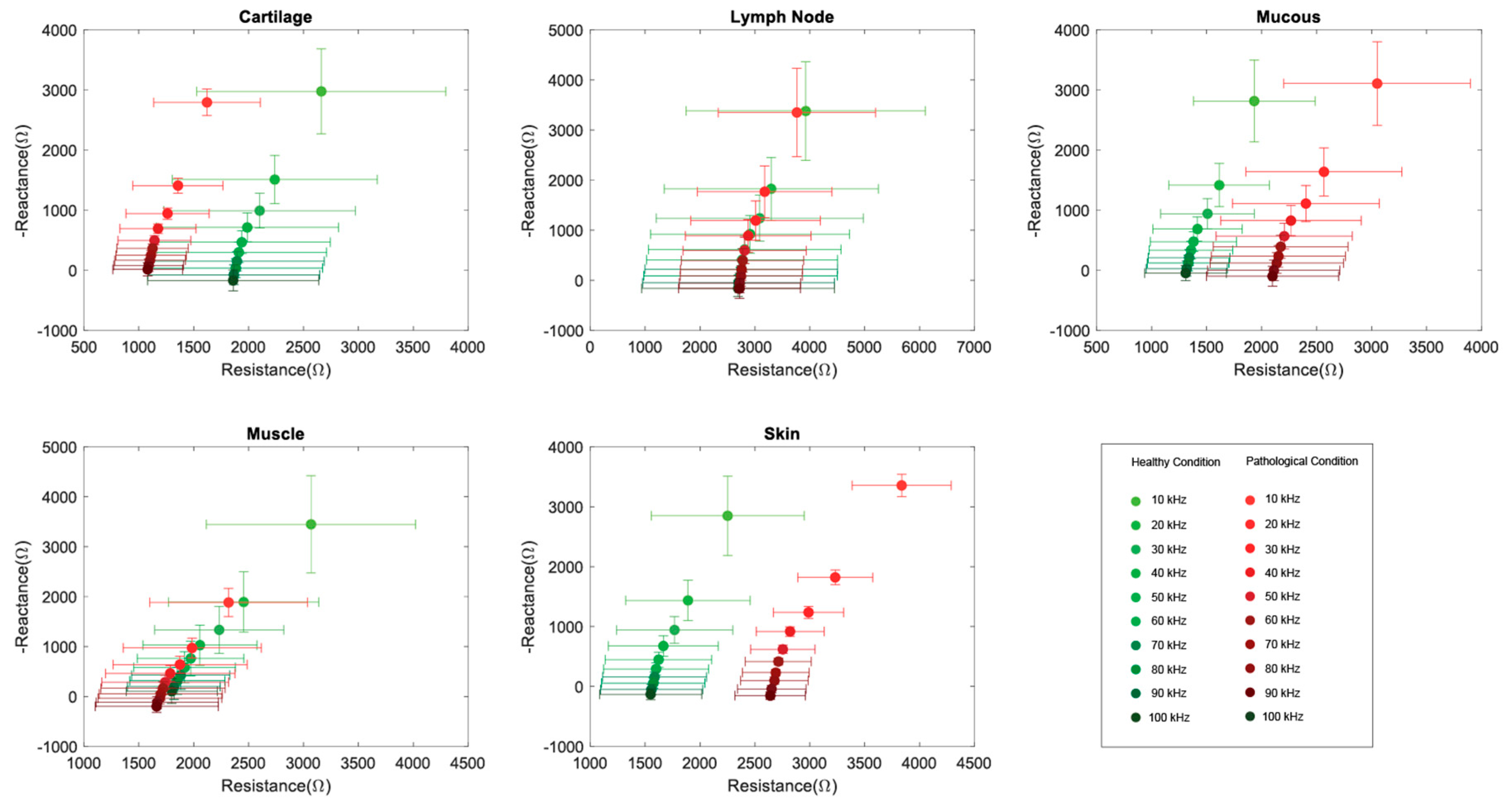
3.2. Tissue-Specific Data
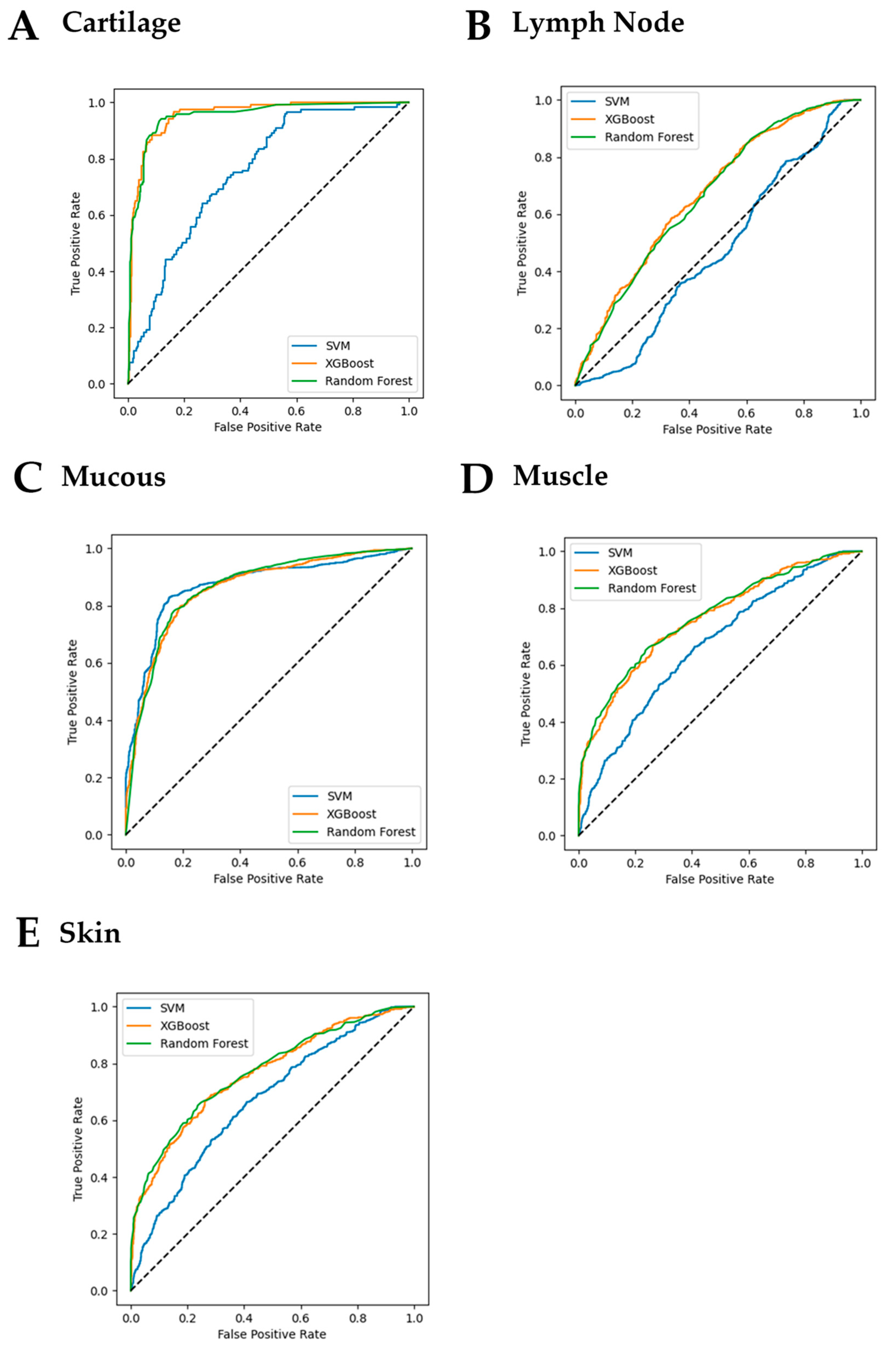
3.3. Performance of the Tissue-Specific Classifiers
3.4. Patient-Specific Data
- Mucosa: For 10 out of 13 patients, the SVM classifiers achieved 1.00 sensitivity and specificity. For the other 3 patients, considerably high sensitivity (0.85, 0.93, and 0.97) and specificity (0.93, 0.79 and 0.97) were also achieved. The accuracies of 12 classifiers were higher than 0.87, while one classifier achieved an accuracy of only 0.54. In addition, we found that for 3 out of 13 patients, the differences in the bioimpedance of healthy mucosa and SCC mucosa were not statistically significant. However, for the other 10 patients, the differences were statistically significant (p-values < 0.001). For the results based on random forest classifiers, only data from four subjects achieved 1.00 sensitivity and specificity. Nevertheless, the classification accuracy was generally high, given that data from 9 patients were higher than 0.90, from 2 patients were between 0.80 to 0.90 and from the other 2 patients were between 0.75 to 0.80. The results of the classification using the XGBoost method revealed that data from 2 patients achieved 1.00 accuracy, data from 8 patients achieved an accuracy ranging from 0.90 to 1.00, and data from another 3 patients achieved an accuracy between 0.80 and 0.90.
- Lymph node: The analysis here included only one patient for whom data from both healthy and pathologic lymph nodes were available. The data of healthy specimens and pathologic specimens were found to have statistically significant differences. The accuracies achieved by the developed SVM, XGBoost, and Random Forest classifiers were found to be 0.79, 0.81 and 0.82 respectively. Statistical analysis (Kruskal-Wallis test) on the data revealed that the values from pathological lymph node tissue were significantly different from those obtained from healthy tissues, given a p-value < 0.001.
- Muscle: In this case, only one patient was included in the analysis. Both the SVM classifier and the Random Forest classifier achieved 0.93 accuracy, while a slightly higher accuracy, i.e., 0.95, was achieved by the XGBoost classifier. Statistical analysis also proved that the bioimpedance of healthy muscle tissue was significantly different from that of pathologic muscle tissue.
- Cartilage: Data from two patients were available for this analysis. The SVM classifier for one of them achieved 1.00 accuracy and 0.63 accuracy for the other patient. The classification accuracies achieved by the XGBoost classifier and the Random Forest classifier were relatively lower, but all were higher than 0.75. Significant differences were found between healthy tissue data and pathologic tissue data for both patients’ data (p-value < 0.001).
- Skin: In this case, data from three patients were included in the analysis, and accuracies of 1.00, 0.99 and 0.72 were achieved by the developed SVMs. The accuracies by XGBoost were found to be 1.00, 0.98 and 0.84. When the Random Forest classifier was used, the accuracies were reported to be 1.00, 0.98 and 0.86. The p-values of the statistical analysis between healthy and pathologic data were found p < 0.001, p = 0.006, and p = 0.051.
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alsaha, E.; Begg, K.; Amelio, I.; Tavassoli, M.; Raulf, N.; Lucarelli, P. Clinical update on head and neck cancer: Molecular biology and ongoing challenges. Cell Death Dis. 2019, 10, 540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marur, S.; Forastiere, A.A. Head and neck cancer: Changing epidemiology, diagnosis, and treatment. Mayo Clin. Proc. 2008, 83, 489–501. [Google Scholar] [CrossRef] [PubMed]
- Mccullough, M.J.; Prasad, G.; Farah, C.S. Oral mucosal malignancy and potentially malignant lesions: An update on the epidemiology, risk factors, diagnosis and management. Aust. Dent. J. 2010, 55 (Suppl. 1), 61–65. [Google Scholar] [CrossRef]
- Ni, X.G.; Wang, G.Q. The Role of Narrow Band Imaging in Head and Neck Cancers. Curr. Oncol. Rep. 2016, 18, 1–7. [Google Scholar] [CrossRef]
- Cosway, B.; Drinnan, M.; Paleri, V. Narrow band imaging for the diagnosis of head and neck squamous cell carcinoma: A systematic review. Head Neck 2016, 38 (Suppl. 1), E2358–E2367. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Zhang, J.; Guo, L.; Nie, J.; Zhu, C.; Ma, X. The value of narrow band imaging in diagnosis of head and neck cancer: A meta-analysis. Sci. Rep. 2018, 8, 515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravanelli, M.; Paderno, A.; Del, B.F.; Montalto, N.; Pessina, C.; Battocchio, S.; Farina, D.; Nicolai, P.; Maroldi, R.; Piazza, C. Prediction of Posterior Paraglottic Space and Cricoarytenoid Unit Involvement in Endoscopically T3 Glottic Cancer with Arytenoid Fixation by Magnetic Resonance with Surface Coils. Cancers 2019, 11, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filauro, M.; Missale, F.; Marchi, F.; Iandelli, A.; Carobbio, A.L.C.; Mazzola, F.; Parrinello, G.; Barabino, E.; Cittadini, G.; Farina, D.; et al. Intraoral ultrasonography in the assessment of DOI in oral cavity squamous cell carcinoma: A comparison with magnetic resonance and histopathology. Eur. Arch. Oto-Rhino-Laryngol. 2020, 278, 2943–2952. [Google Scholar] [CrossRef]
- Widmann, G.; Henninger, B.; Kremser, C.; Jaschke, W. MRI Sequences in Head & Neck Radiology—State of the Art. Rofo 2017, 189, 413–422. [Google Scholar]
- Pérez-Lara, A.; Forghani, R. Spectral Computed Tomography: Technique and Applications for Head and Neck Cancer. Magn. Reson. Imaging Clin. N. Am. 2018, 26, 1–17. [Google Scholar] [CrossRef]
- Kumar, R.; Mukherjee, A.; Mittal, B.R. Special Techniques in PET/Computed Tomography Imaging for Evaluation of Head and Neck Cancer. PET Clin. 2016, 11, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Moqadam, S.M.; Grewal, P.K.; Haeri, Z.; Ingledew, P.A.; Kohli, K.; Golnaraghi, F. Cancer detection based on electrical impedance spectroscopy: A clinical study. J. Electr. Bioimpedance 2018, 9, 17–23. [Google Scholar] [CrossRef] [Green Version]
- Sarode, G.; Sarode, S.; Kulkarni, M.; Karmarkar, S.; Patil, S. Role of bioimpedance in cancer detection: A brief review. Int. J. Dent. Sci. Res. 2016, 3, 15–21. [Google Scholar] [CrossRef]
- Grimnes, S.; Martinsen, O. Bioimpedance and Bioelectricity Basics; Elsevier: Chatswood, NSW, Australia, 2014. [Google Scholar]
- Surowiec, A.J.; Stuchly, S.S.; Barr, J.B.; Swarup, A. Dielectric properties of breast carcinoma and the surrounding tissues. IEEE Trans. Biomed. Eng. 1988, 35, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.R.; Roberts, W.W.; Smith, D.G.; Ko, H.W.; Epstein, J.I.; Lecksell, K.; Partin, A.W. Bioimpedance: Novel use of a minimally invasive technique for cancer localization in the intact prostate. Prostate 1999, 39, 213–218. [Google Scholar] [CrossRef]
- Laufer, S.; Ivorra, A.; Reuter, V.E.; Rubinsky, B.; Solomon, S.B. Electrical impedance characterization of normal and cancerous human hepatic tissue. Physiol. Meas. 2010, 31, 995–1009. [Google Scholar] [CrossRef]
- O’Rourke, A.P.; Lazebnik, M.; Bertram, J.M.; Converse, M.C.; Hagness, S.C.; Webster, J.G.; Mahvi, D.M. Dielectric properties of human normal, malignant and cirrhotic liver tissue: In Vivo and ex vivo measurements from 0.5 to 20 GHz using a precision open-ended coaxial probe. Phys. Med. Biol. 2007, 52, 4707–4719. [Google Scholar] [CrossRef] [Green Version]
- Bereś-Pawlik, E.; Grobelny, A.; Fraczek, M.; Zalesska-Krecicka, M.; Krecicki, T. Electrical Impedance Measurements in Assessing Laryngeal Squamous Cell Carcinoma Pomiary impedancji elektrycznej w diagnostyce raka pBaskonacBonkowego krtani. Adv. Clin. Exp. Med. 2006, 15, 619–624. [Google Scholar]
- Yu, D.; Jun, D.; Qing, Y.; Jianxun, Z. Development of a noninvasive electrical impedance probe for minimally invasive tumor localization. Physiol. Meas. 2015, 36, 1785–1799. [Google Scholar] [CrossRef]
- Ching, C.T.S.; Sun, T.P.; Huang, S.H.; Hsiao, C.S.; Chang, C.H.; Huang, S.Y.; Chen, Y.J.; Cheng, C.S.; Shieh, H.L.; Chen, C.Y. A preliminary study of the use of bioimpedance in the screening of squamous tongue cancer. Int. J. Nanomed. 2010, 5, 213–220. [Google Scholar] [CrossRef] [Green Version]
- Sun, T.P.; Ching, C.T.S.; Cheng, C.S.; Huang, S.H.; Chen, Y.J.; Hsiao, C.S.; Chang, C.H.; Huang, S.Y.; Shieh, H.L.; Liu, W.H.; et al. The use of bioimpedance in the detection/screening of tongue cancer. Cancer Epidemiol. 2010, 34, 207–211. [Google Scholar] [CrossRef]
- Sarode, G.S.; Sarode, S.C.; Kulkarni, M.; Karmarkar, S.; Patll, S.; Auciustine, D. Bioimpedance Assessment of Oral Squamous Cell Carcinoma with Clinicopathological Correlation. J. Contemp. Dent. Pract. 2015, 16, 715–722. [Google Scholar] [PubMed]
- Sarode, G.; Sarode, S.; Panta, P. Bioimpedance in Oral Cancer. In Oral Cancer Detection; Springer: Berlin/Heidelberg, Germany, 2019; pp. 239–254. ISBN 978-3-319-61255-3. [Google Scholar]
- Cheng, Z.; Carobbio, A.L.C.; Carobbio, A.L.C.; Soggiu, L.; Migliorini, M.; Guastini, L.; Guastini, L.; Mora, F.; Mora, F.; Fragale, M.; et al. SmartProbe: A bioimpedance sensing system for head and neck cancer tissue detection. Physiol. Meas. 2020, 41, 054003. [Google Scholar] [CrossRef]
- Carpano Maglioli, C.; Caldwell, D.G.; Mattos, L.S. A bioimpedance sensing system for in-vivo cancer tissue identification: Design and preliminary evaluation. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju Island, Republic of Korea, 11–15 July 2017; pp. 4235–4238. [Google Scholar]
- Amini, M.; Hisdal, J.; Kalvøy, H. Applications of bioimpedance measurement techniques in tissue engineering. J. Electr. Bioimpedance 2018, 9, 142–158. [Google Scholar] [CrossRef] [Green Version]
- Femmam, S. Fundamentals of Signals and Control Systems; John Wiley & Sons: Hoboken, NJ, USA, 2017; ISBN 1119335698. [Google Scholar]
- Boser, B.E.; Guyon, I.M.; Vapnik, V.N. A Training Algorithm for Optimal Margin Classifiers. In Proceedings of the Proceedings of the Fifth Annual Workshop on Computational Learning Theory; Association for Computing Machinery: New York, NY, USA, 1992; pp. 144–152. [Google Scholar]
- Chen, T.; Guestrin, C. Xgboost: A scalable tree boosting system. In Proceedings of the 22nd Acm Sigkdd International Conference on Knowledge Discovery and Data Mining; Association for Computing Machinery: New York, NY, USA, 2016; pp. 785–794. [Google Scholar]
- Ho, T.K. Proceedings of 3rd International Conference on Document Analysis and Recognition; IEEE: Piscataway, NJ, USA, 1995; pp. 278–282. [Google Scholar]
- De Luis, D.A.; Aller, R.; Izaola, O.; Terroba, M.C.; Cabezas, G.; Cuellar, L. Tissue electric properties in head and neck cancer patients. Ann. Nutr. Metab. 2006, 50, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Bera, T.K. Bioelectrical Impedance and the Frequency Dependent Current Conduction Through Biological Tissues: A Short Review. IOP Conf. Ser. Mater. Sci. Eng. 2018, 331, 012005. [Google Scholar] [CrossRef]
- Brown, B.H.; Milnes, P.; Abdul, S.; Tidy, J.A. Detection of cervical intraepithelial neoplasia using impedance spectroscopy: A prospective study. BJOG Int. J. Obstet. Gynaecol. 2005, 112, 802–806. [Google Scholar] [CrossRef]
- Morucci, J.P.; Rigaud, B. Bioelectrical impedance techniques in medicine. Part III: Impedance imaging. Third section: Medical applications. Crit. Rev. Biomed. Eng. 1996, 24, 655–677. [Google Scholar] [CrossRef]
- Schwan, H.P.; Kay, C.F. Capacitive properties of body tissues. Circ. Res. 1957, 5, 439–443. [Google Scholar] [CrossRef]
- Astbury, J.C.; Goldschmidt, M.H.; Evans, S.M.; Niebauer, G.W.; Foster, K.R. The dielectric properties of canine and normal and neoplastic splenic tissues. In Proceedings of the 1988 Fourteenth Annual Northeast Bioengineering Conference, Durham, NH, USA, 10–11 March 1988; pp. 107–108. [Google Scholar]
- Cole, K.S.; Cole, R.H. Dispersion and Absorption in Dielectrics I. Alternating Current Characteristics. J. Chem. Phys. 1941, 9, 341–351. [Google Scholar] [CrossRef] [Green Version]
- Meroni, D.; Bovio, D.; Frisoli, P.A.; Aliverti, A. Measurement of electrical impedance in different ex-vivo tissues. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 2311–2314. [Google Scholar]
- Surowiec, A.; Stuchly, S.S.; Swarup, A. Radiofrequency dielectric properties of animal tissues as a function of time following death. Phys. Med. Biol. 1985, 30, 1131–1141. [Google Scholar] [CrossRef] [PubMed]
- Foster, K.R.; Schwan, H.P. Dielectric properties of tissues and biological materials: A critical review. Crit. Rev. Biomed. Eng. 1989, 17, 25–104. [Google Scholar]
- Dik, E.A.; Ipenburg, N.A.; Adriaansens, S.O.; Kessler, P.A.; van Es, R.J.; Willems, S.M. Poor Correlation of Histologic Parameters Between Biopsy and Resection Specimen in Early Stage Oral Squamous Cell Carcinoma. Am. J. Clin. Pathol. 2015, 144, 659–666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ganti, A.; Tajudeen, B.A.; Plitt, M.A.; Rossi, I.; Gattuso, P.; Batra, P.S. Discordance in Preoperative and Postoperative Histopathology of Sinonasal Tumors. Am. J. Rhinol. Allergy 2018, 32, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Isenberg, J.S.; Crozier, D.L.; Dailey, S.H. Institutional and comprehensive review of laryngeal leukoplakia. Ann. Otol. Rhinol. Laryngol. 2008, 117, 74–79. [Google Scholar] [CrossRef]
- Latikka, J.; Eskola, H. The Resistivity of Human Brain Tumours In Vivo. Ann. Biomed. Eng. 2019, 47, 706–713. [Google Scholar] [CrossRef] [PubMed]
- Horváth, A.; Prekopp, P.; Polony, G.; Székely, E.; Tamás, L.; Dános, K. Accuracy of the preoperative diagnostic workup in patients with head and neck cancers undergoing neck dissection in terms of nodal metastases. Eur. Arch. Oto-Rhino-Laryngol. 2020, 278, 2041–2046. [Google Scholar] [CrossRef]
- Ahn, S.-H. Usage and Diagnostic Yield of Fine-Needle Aspiration Cytology and Core Needle Biopsy in Thyroid Nodules: A Systematic Review and Meta-Analysis of Literature Published by Korean Authors. Clin. Exp. Otorhinolaryngol. 2020, 14, 116–130. [Google Scholar] [CrossRef]
- Zhou, J.; Li, F.; Meng, L.; Hao, F.; Liu, X.; Zhao, C.; Zhang, K.; Dong, A. Fine needle aspiration cytology for lymph nodes: A three-year study. Br. J. Biomed. Sci. 2016, 73, 28–31. [Google Scholar] [CrossRef]
- de Bondt, R.B.J.; Nelemans, P.J.; Hofman, P.A.M.; Casselman, J.W.; Kremer, B.; van Engelshoven, J.M.A.; Beets-Tan, R.G.H. Detection of lymph node metastases in head and neck cancer: A meta-analysis comparing US, USgFNAC, CT and MR imaging. Eur. J. Radiol. 2007, 64, 266–272. [Google Scholar] [CrossRef]
- Takes, R.P.; Knegt, P.; Manni, J.J.; Meeuwis, C.A.; Marres, H.A.; Spoelstra, H.A.; de Boer, M.F.; Bruaset, I.; van Oostayen, J.A.; Laméris, J.S.; et al. Regional metastasis in head and neck squamous cell carcinoma: Revised value of US with US-guided FNAB. Radiology 1996, 198, 819–823. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Type | Overall (N) | Healthy Tissue N (%) | Pathologic Tissue N (%) | n° of Patients (Total) | n° of Patients (*) |
|---|---|---|---|---|---|
| Cartilage | 162 | 115 (71%) | 47 (29%) | 11 | 2 |
| Lymph Node | 763 | 491 (64%) | 272 (36%) | 25 | 1 |
| Mucous | 525 | 141 (27%) | 384 (73%) | 28 | 13 |
| Muscle | 421 | 261 (62%) | 160 (38%) | 32 | 1 |
| Skin | 144 | 82 (57%) | 62 (43%) | 9 | 3 |
| Tissue Type | Excitation Frequency (kHz) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 10 | 20 | 30 | 40 | 50 | 60 | 70 | 80 | 90 | 100 | |
| Mucosa | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Lymph node | 0.44 | 0.19 | 0.19 | 0.62 | 0.49 | 0.15 | 0.13 | 0.21 | 0.48 | 0.09 |
| Muscle | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Cartilage | 0.016 | 0.021 | <0.001 | <0.001 | 0.0157 | 0.012 | 0.009 | 0.046 | 0.141 | 0.001 |
| Skin | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Performance Metric | Classifier | Mucosa | Lymph Node | Muscle | Cartilage | Skin |
|---|---|---|---|---|---|---|
| Sensitivity | SVM | 0.86 | 0.99 | 0.20 | 0.42 | 0.91 |
| XGBoost | 0.87 | 0.81 | 0.58 | 0.76 | 0.95 | |
| Random Forest | 0.86 | 0.79 | 0.58 | 0.72 | 0.94 | |
| Specificity | SVM | 0.76 | 0.07 | 0.93 | 0.98 | 0.86 |
| XGBoost | 0.70 | 0.43 | 0.81 | 0.95 | 0.91 | |
| Random Forest | 0.71 | 0.44 | 0.83 | 0.95 | 0.92 | |
| Accuracy | SVM | 0.83 | 0.65 | 0.65 | 0.82 | 0.89 |
| XGBoost | 0.81 | 0.67 | 0.72 | 0.92 | 0.93 | |
| Random Forest | 0.82 | 0.67 | 0.73 | 0.91 | 0.93 | |
| F1 score | SVM | 0.87 | 0.78 | 0.30 | 0.79 | 0.90 |
| XGBoost | 0.86 | 0.76 | 0.62 | 0.77 | 0.94 | |
| Random Forest | 0.86 | 0.75 | 0.62 | 0.74 | 0.94 | |
| MCC | SVM | 0.61 | 0.16 | 0.19 | 0.46 | 0.77 |
| XGBoost | 0.56 | 0.26 | 0.40 | 0.72 | 0.86 | |
| Random Forest | 0.57 | 0.25 | 0.42 | 0.68 | 0.86 | |
| AUC | SVM | 0.81 | 0.53 | 0.56 | 0.52 | 0.88 |
| XGBoost | 0.78 | 0.62 | 0.69 | 0.86 | 0.93 | |
| Random Forest | 0.79 | 0.62 | 0.70 | 0.83 | 0.93 |
| Classifier | Mucosa | Lymph Node | Muscle | Cartilage | Skin |
|---|---|---|---|---|---|
| SVM vs. XGBoost | 1.0 | 1.0 | 0.74 | 0.93 | 1.0 |
| SVM vs. Random Forest | 1.0 | 1.0 | 0.74 | 0.93 | 1.0 |
| XGBoost vs. Random Forest | 1.0 | 0.76 | 0.74 | 0.056 | 1.0 |
| Performance Metric | Classifier | Mucosa | Lymph Node | Muscle | Cartilage | Skin |
|---|---|---|---|---|---|---|
| Sensitivity | SVM | 0.95 ± 0.12 | 0.24 | 1.00 | 0.80 ± 0.21 | 0.93 ± 0.09 |
| XGBoost | 0.93.5 ± 0.09 | 0.91 | 0.94 | 0.73 ± 0.07 | 0.97 ± 0.04 | |
| Random Forest | 0.88 ± 0.26 | 0.88 | 0.95 | 0.83 ± 0.17 | 0.93 ± 0.08 | |
| Specificity | SVM | 0.94 ± 0.14 | 0.96 | 0.90 | 0.86 ± 0.14 | 0.88 ± 0.17 |
| XGBoost | 0.85 ± 0.21 | 0.52 | 0.98 | 0.92 ± 0.83 | 0.92 ± 0.09 | |
| Random Forest | 0.85 ± 0.26 | 0.63 | 0.90 | 0.88 ± 0.86 | 0.96 ± 0.04 | |
| Accuracy | SVM | 0.94 ± 0.13 | 0.79 | 0.93 | 0.82 ± 0.18 | 0.90 ± 0.13 |
| XGBoost | 0.91 ± 0.13 | 0.81 | 0.95 | 0.87 ± 0.10 | 0.94 ± 0.07 | |
| Random Forest | 0.87 ± 0.26 | 0.82 | 0.93 | 0.86 ± 0.11 | 0.95 ± 0.06 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carobbio, A.L.C.; Cheng, Z.; Gianiorio, T.; Missale, F.; Africano, S.; Ascoli, A.; Fragale, M.; Filauro, M.; Marchi, F.; Guastini, L.; et al. Electric Bioimpedance Sensing for the Detection of Head and Neck Squamous Cell Carcinoma. Diagnostics 2023, 13, 2453. https://doi.org/10.3390/diagnostics13142453
Carobbio ALC, Cheng Z, Gianiorio T, Missale F, Africano S, Ascoli A, Fragale M, Filauro M, Marchi F, Guastini L, et al. Electric Bioimpedance Sensing for the Detection of Head and Neck Squamous Cell Carcinoma. Diagnostics. 2023; 13(14):2453. https://doi.org/10.3390/diagnostics13142453
Chicago/Turabian StyleCarobbio, Andrea Luigi Camillo, Zhuoqi Cheng, Tomaso Gianiorio, Francesco Missale, Stefano Africano, Alessandro Ascoli, Marco Fragale, Marta Filauro, Filippo Marchi, Luca Guastini, and et al. 2023. "Electric Bioimpedance Sensing for the Detection of Head and Neck Squamous Cell Carcinoma" Diagnostics 13, no. 14: 2453. https://doi.org/10.3390/diagnostics13142453