
The Vertebral Artery: A Systematic Review and a Meta-Analysis of the Current Literature

1
Division of Anatomy, Faculty of Dentistry, “Carol Davila” University of Medicine and Pharmacy, 020021 Bucharest, Romania
2
Division of Legal Medicine and Bioethics, Faculty of Dentistry, “Carol Davila” University of Medicine and Pharmacy, 050474 Bucharest, Romania
*
Author to whom correspondence should be addressed.
Diagnostics 2023, 13(12), 2036; https://doi.org/10.3390/diagnostics13122036
Submission received: 9 May 2023
/
Revised: 1 June 2023
/
Accepted: 9 June 2023
/
Published: 12 June 2023
(This article belongs to the Section Medical Imaging and Theranostics)
Abstract
:(1) Background. The anatomical variations of the vertebral arteries (VAs) have a significant impact both in neurosurgery and forensic pathology. The purpose of this study was to evaluate the variational anatomy of the vertebral artery. We evaluated anatomical aspects regarding the V1 and V2 segments of the VA: origin, course, tortuosity, hypoplasia, and dominance, and established the prevalence of each variation. (2) Methods. We conducted a systematic search in PubMed and Google Scholar databases, up to December 2022. Sixty-two studies, comprising 32,153 vessels, were included in the current meta-analysis. We used a random-effects model with a DerSimonian-Laird estimator. The confidence intervals were set at 95%. The heterogeneity between studies was assessed using I2. The funnel plot and Egger’s regression test for plot asymmetry were used for the evaluation of publication bias. Statistical significance was considered at p < 0.05. (3) Results. The most common site for the origin of both VAs was the subclavian artery. The aortic arch origin of the left VA had a prevalence of 4.81%. Other origins of the right VAs were noted: aortic arch (0.1%), right common carotid artery (0.1%), and brachiocephalic trunk (0.5%). Ninety-two percent of the VAs entered the transverse foramen (TF) of the C6 vertebra, followed by C5, C7, C4, and least frequently, C3 (0.1%). Roughly one out of four (25.9%) VAs presented a sort of tortuosity, the transversal one representing the most common variant. Hypoplasia occurred in 7.94% of the vessels. Left VA dominance (36.1%) is more common, compared to right VA dominance (25.3%). (4) Conclusions. The anatomy of the VA is highly irregular, and eventual intraoperative complications may be life-threatening. The prevalence of VA origin from the subclavian artery is 94.1%, 92.0% of the VAs entered the TF at C6, 26.6% were tortuous, and 7.94% were hypoplastic.
1. Introduction
The vertebral arteries (VA), left (LVA) and right (RVA), supply the upper spinal cord, brainstem, cerebellum, and the posterior part of the brain with oxygenated blood, accounting for 28% of its supply [1,2]. Commonly, the VA originates from the first cervical part of the subclavian artery (SA), medial to the anterior scalene muscle, continuing its ascending course through the transverse foramina (TF) of cervical transverse processes, passing through the foramen magnum, to end in the posterior fossa by forming the basilar artery with the opposite VA [3].
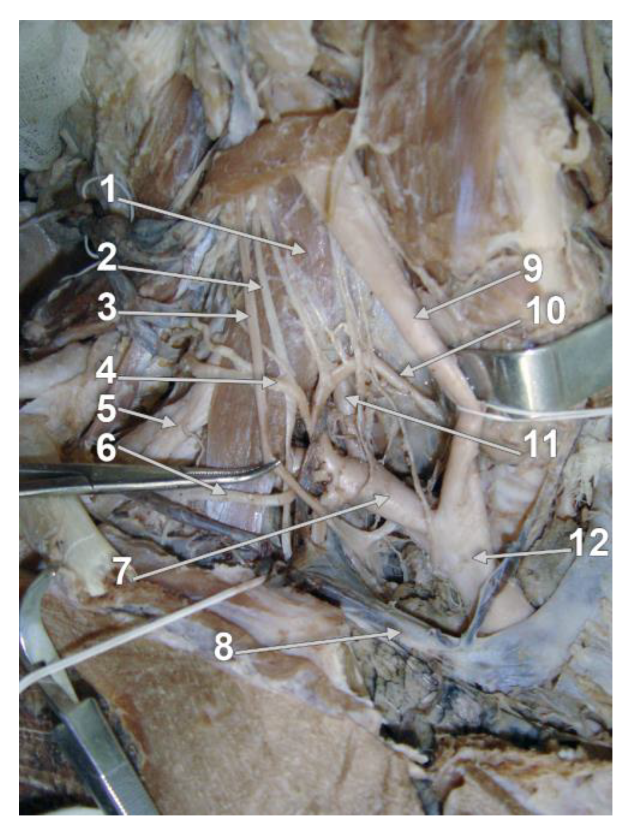
For an improved overview of the VA, it has been divided anatomically into four segments, three extracranial, and one intracranial [4,5]. The first V1 segment (extraosseous, prevertebral or pretransverse, ostial, proximal) describes the course of the VA from its origin until it enters the TF of (usually) either the fifth or the sixth cervical vertebra (Figure 1) [6,7]. The second V2 segment (cervical, foraminal, transforaminal), ascends through the TF of C6 to C2 [8], continuing with the third V3 segment (atlantal/atlantic [9,10], extraspinal) behind the lateral mass of the atlas, further entering the foramen magnum. The final intracranial and intradural V4 segment starts as the VA perforates the dura and arachnoid mater in the foramen magnum and pursues its ascending course on clivus. At the lower border of the pons, the confluence of the VAs forms the basilar artery [11].
The study aimed to assess the morphology of the VA’s V1 and V2 segments from a qualitative perspective. There were evaluated the course of the VA, the origin, the vertebral level of entrance in the TF, tortuosity and straightness, planes of tortuosity, hypoplasia, and dominance of this artery.
2. Materials and Methods
The study was performed according to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines for reporting systematic reviews and meta-analyses [12].
2.1. Search Method
Articles were obtained by performing systematic searches on different databases, PubMed and Web of Science, using the following keywords: “Vertebral artery” AND “Anatomy” AND “V1” and “Vertebral artery” AND “Anatomy” AND “V2”. The reference list of all the relevant articles was thoroughly scrutinized for other appropriate references to be included in the analysis. Extensive searches were also performed on Google Scholar, Google, and Research Gate. Every potentially relevant article was obtained as a full article, analyzed by two reviewers, and included in the current paper if it fulfilled the inclusion criteria and did not fulfill any of the exclusion criteria. Selected articles were imported into a Paperpile database.
2.2. Selection Criteria
The following exclusion criteria were used: (1) articles that did not mention any relevant measurements regarding the first two segments of the VA, (2) results duplicating previously published articles, (3) low-quality articles comprising inadequate methods of measurement and irrelevant results or published in unknown/low impact factor journals, (4) less than 10 subjects, (5) studies conducted on fetuses, (6) inability to obtain the full article, (7) studies that measured the prevalence of tortuosity in patients with Loeys–Dietz syndrome, Marfan syndrome or any other vascular disease, as the frequency of tortuous vessels in these subjects is known to be much higher compared to healthy subjects [13,14], (8) case reports, reviews, meta-analyses, or any other prevalence studies based on published values.
2.3. Data Collection and Analysis
Two reviewers separately extracted data from each study in different Excel 365 databases. If any major discrepancy appeared, a third reviewer was co-opted to check the inconsistency and select the appropriate result. The following information was extracted: name of the first author, year, method (CT, autopsy reports, surgical reports, etc.), total number of cases, total number of left and right VAs (LVAs and RVAs), the analyzed segment of the VA (V1 or V2) and its measurements, each in a separate, specific column.
2.4. Quality Assessment and Risk of Bias
Newcastle–Ottawa Scale (NOS) for case-control studies was used, with the following adjustments for a prevalence analysis: item 3 from Selection and Exposure was excluded. Each article was noted with a mark ranging from 0 to 7 to assess the quality. Articles with at least 4 points were included in the current paper.
2.5. Statistical Analysis
Results were statistically analyzed using Jamovi 2.3 software (Sydney, Australia) for data analysis. Three columns were created: authors, total cases, and the third one which varied, depending on the measured variable. The “Proportions” tab was used to process the variables. The “Total cases” column also varied in accordance with the variable. If the analyzed variable concerned only one side (left or right), then the standardized/true prevalence for that particular side was determined. The following analyses were conducted by determining the crude prevalence for each anatomical variant: C3, C4, C5, C6, and C7 TF entrance, overall tortuosity, VA dominance, and hypoplasia. VA origin, TF entrance corelated to VA origin and plane of tortuosity were assessed as standardized prevalence, as well as the results reported in Table 1, based on study type (autopsy or imaging). Cases that did not mention the exact number of VAs (e.g., 70 specimens) were analyzed carefully. If, after scrutinizing the entire article, the published data indicated a number of arteries double the mentioned one, we considered the first as the real number of VAs (70 LVAs and 70 RVAs) and the latter as the number of patients [15]. The following configuration was used for the statistical processing of the data. The model estimator was DerSimonian–Laird, Raw Proportion was used for effect size model measures, Moderator Type was set on no moderator, and the Confidence Interval (CI) level was established at 95%. Statistical significance was considered at p < 0.05. The funnel plot and Egger’s regression test for plot asymmetry were used for the analysis of the publication bias. I2 was used to test the presence of heterogeneity between studies, using the following thresholds: 0–35%—most likely not important, 36–55%—moderate heterogeneity, 56–85%—most likely substantial heterogeneity, and 86–100%—significant heterogeneity (average values based on [16]). Considering VA course prevalence, Trattnig et al., (1993) [17] report two types of results, measured on two different groups of subjects (140 and 160 subjects, respectively) and with different methods (cadavers and imagistic). The article was, therefore, used twice in the analyses. Regarding hypoplasia, as each author defines a hypoplastic VA differently, we adopted the highest reported value, to include all the reported measurements. Thus, hypoplasia is interpreted as a diameter of 3.5 mm or less. If reported data of hypoplasia or dominance were split into V1 and V2 segments, they were summed up, so the prevalence of hypoplastic/dominant VA was calculated as a whole for the mentioned segments. Vaiman et al. [18] analyzed a total of 400 VAs, with 23 anomalous VAs. We used 23 as the total number of vessels to determine the prevalences, since the article reported data about the origin and TF entrance only for these anomalous VAs. For each description of the forest plot in the Result section, we reported the number of studies, the total number of vessels included in the analysis, and the number of vessels displaying the anatomical variant. Then, we added the results of the statistical analysis: prevalence, CI, p-value, heterogeneity, and Egger’s regression test for plot asymmetry. We also evaluated the standardized prevalence disparity between autopsy and imaging studies and specified whether it was significant or not.
3. Results
3.1. Search Synthesis
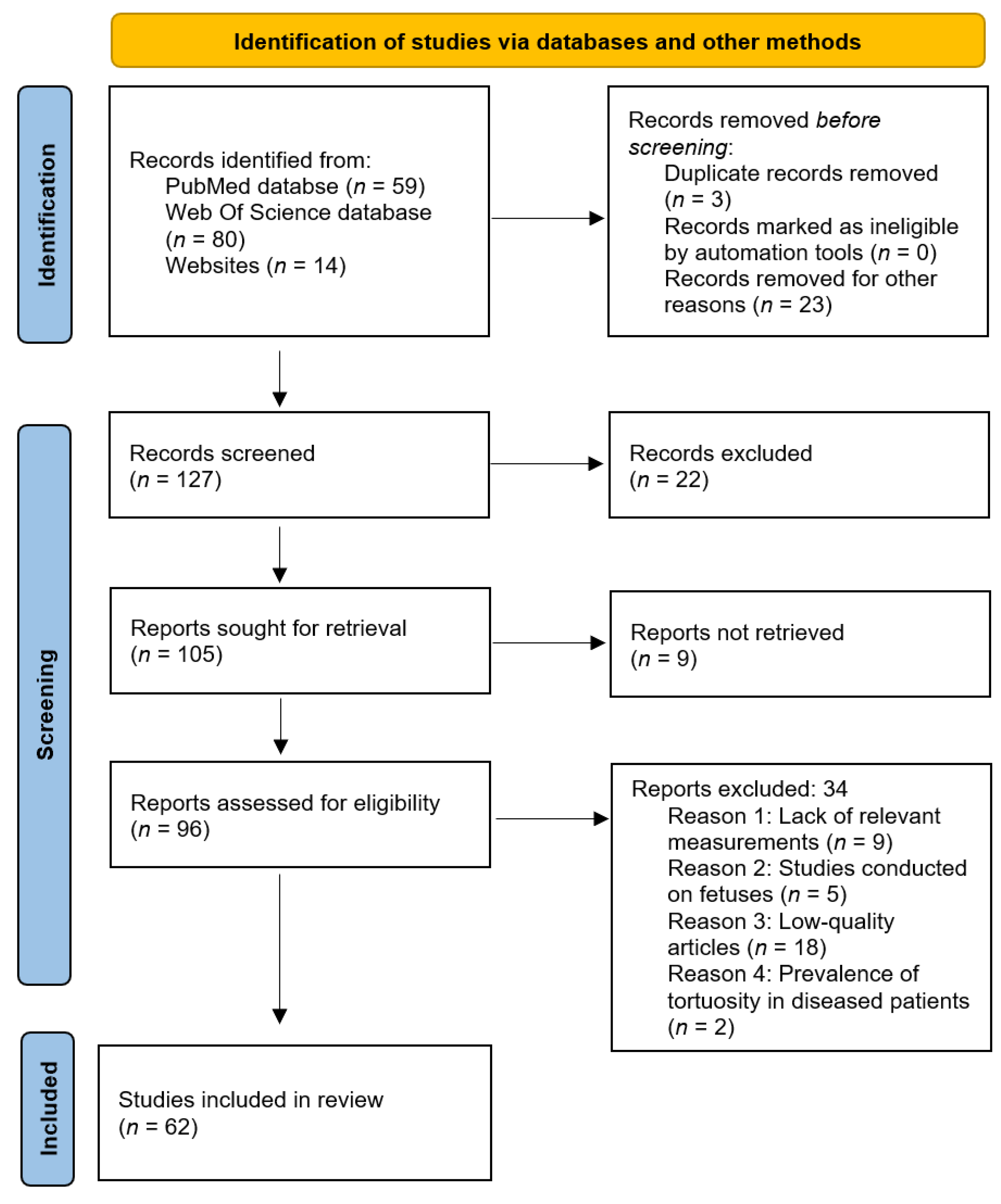
During the initial research via databases and other methods, 60 references were gathered for V1 segment and 93 for V2. After removing all articles that displayed at least one exclusion criterion, 62 papers were further scrutinized and included in the current meta-analysis. The search synthesis is systemized in Figure 2. Each paper contained in the present study is detailed in Table 2.
3.2. Quality Assessment and Risk of Bias
Each article was assessed with a score between 0 and 7. The score for each study was noted in Table 2. There was no significant bias in any of the mentioned papers.
3.3. Prevalence of VA Origin
3.3.1. LVA Originating from the SA
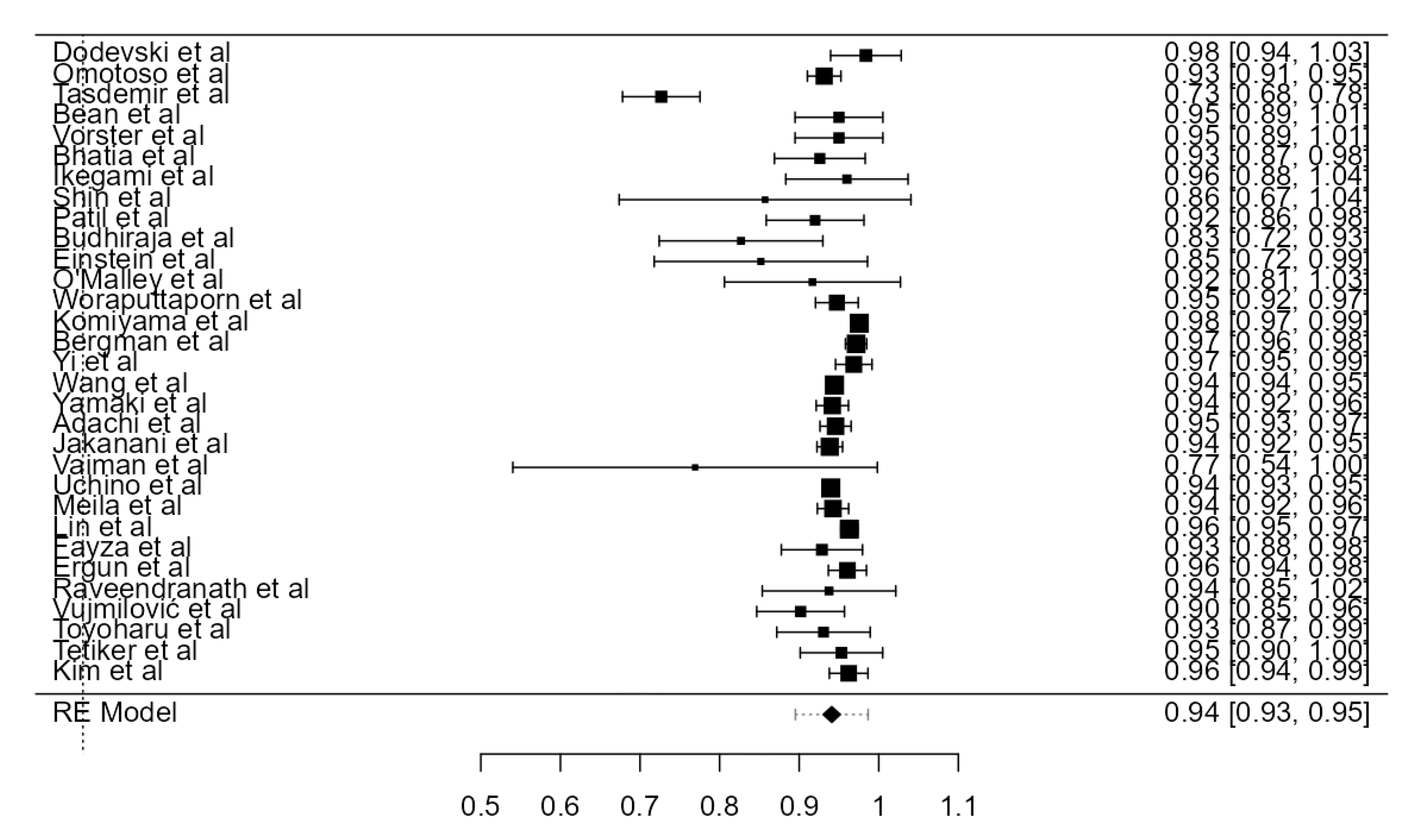
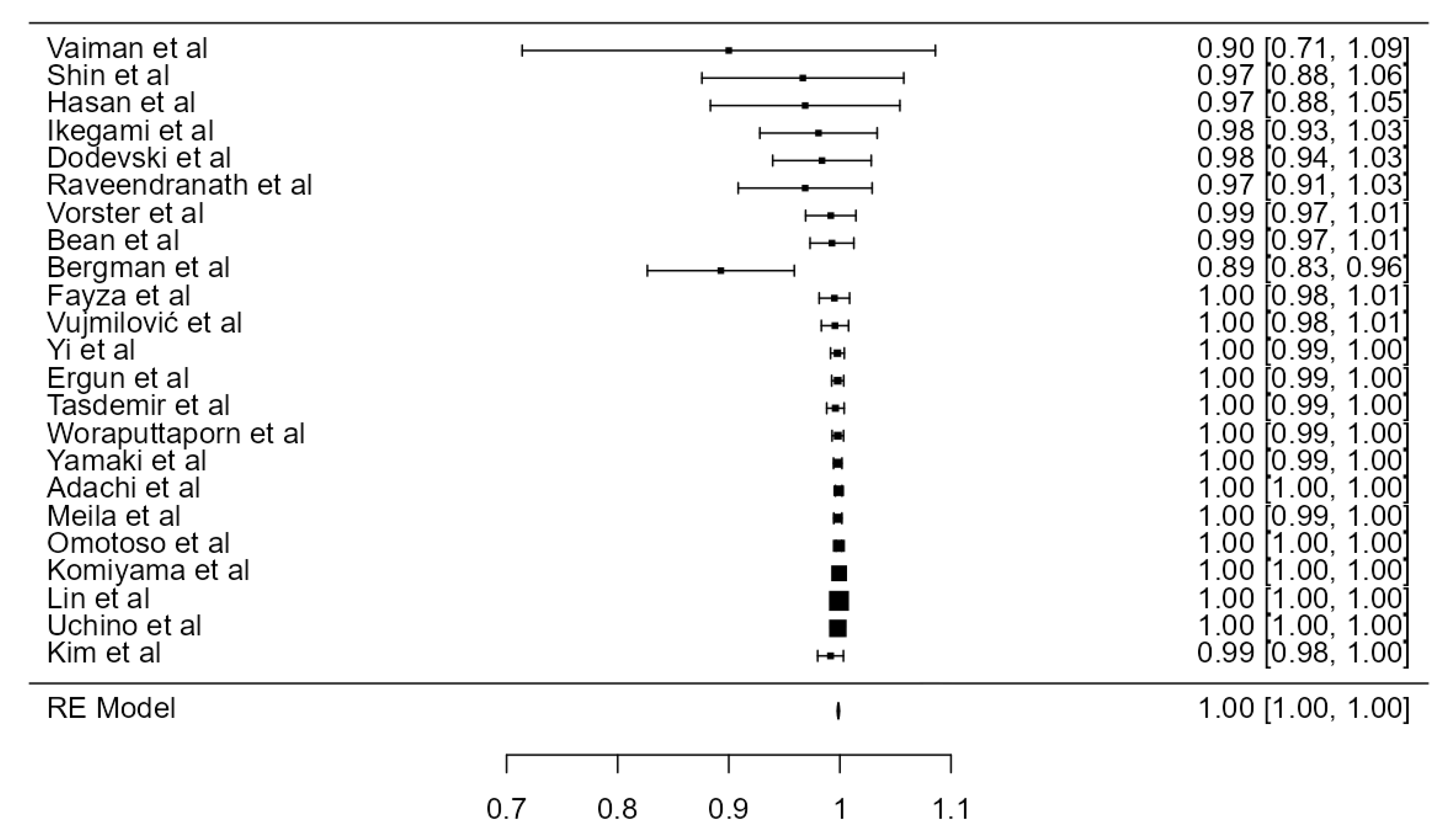
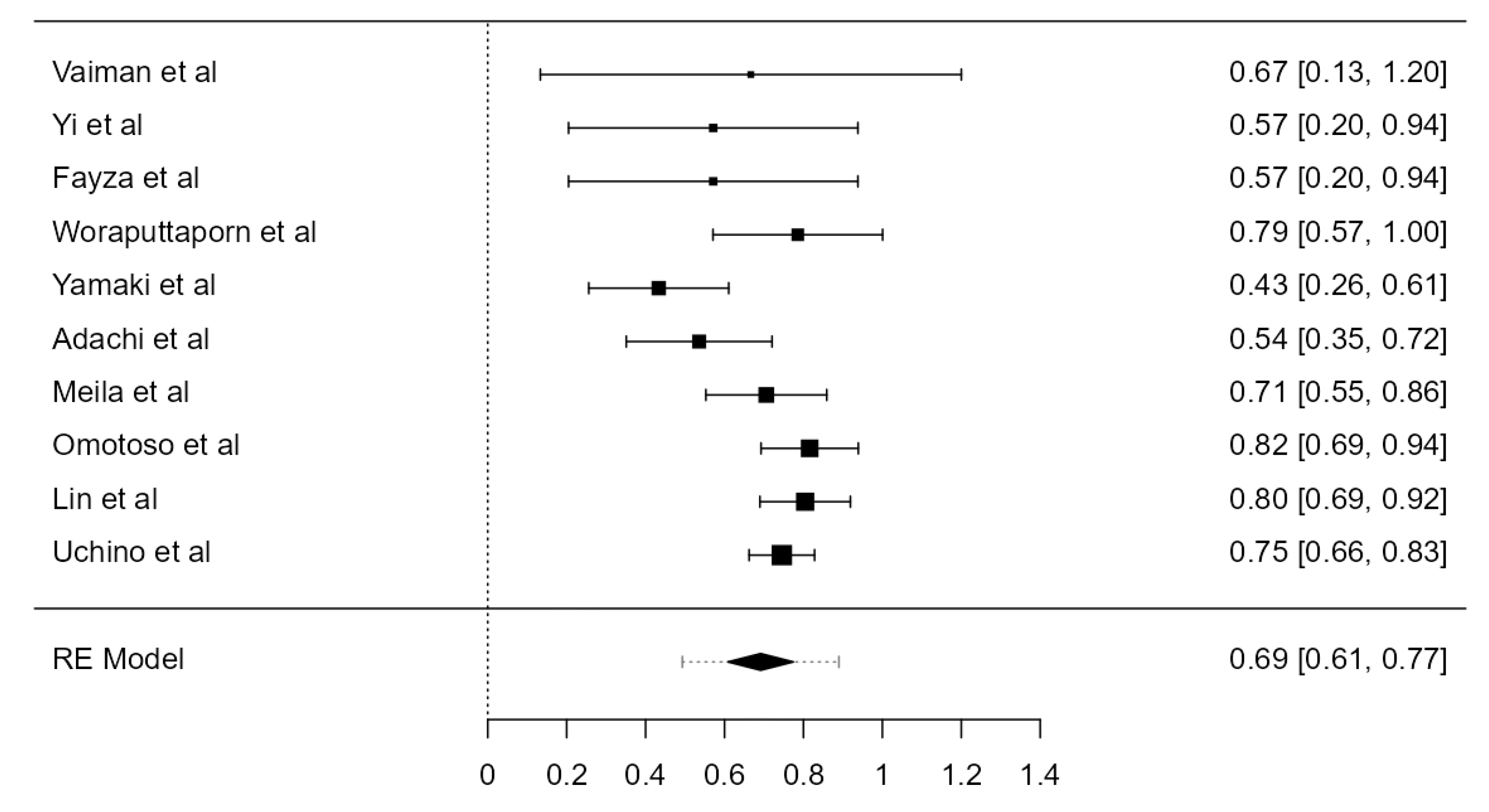
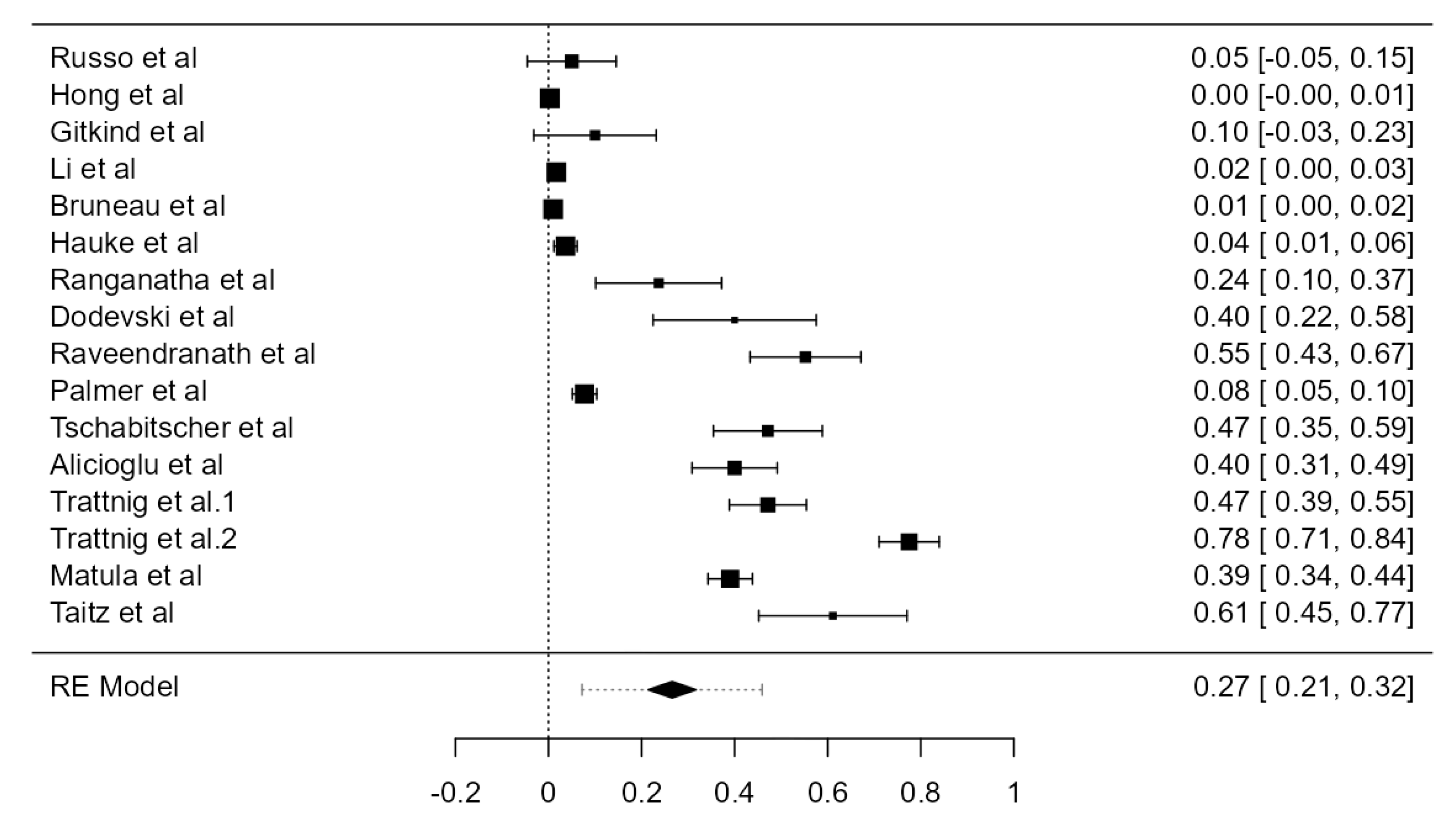
Thirty-one studies, adding up to 12,456 LVAs, contained data about the origin of the LVA. The standardized prevalence of the LVA arising from the SA was 94.1% (CI: 93.0–95.2, p < 0.001), as shown in Figure 3. The heterogeneity was substantial (I2 = 80.7%). Based on Egger’s regression test for plot asymmetry, there was a significant publication bias (p < 0.001). No major difference was found between standardized prevalence determined in autopsy (94.5%) and imaging (93.5%) studies (Table 1).
3.3.2. LVA Originating from the Aortic Arch
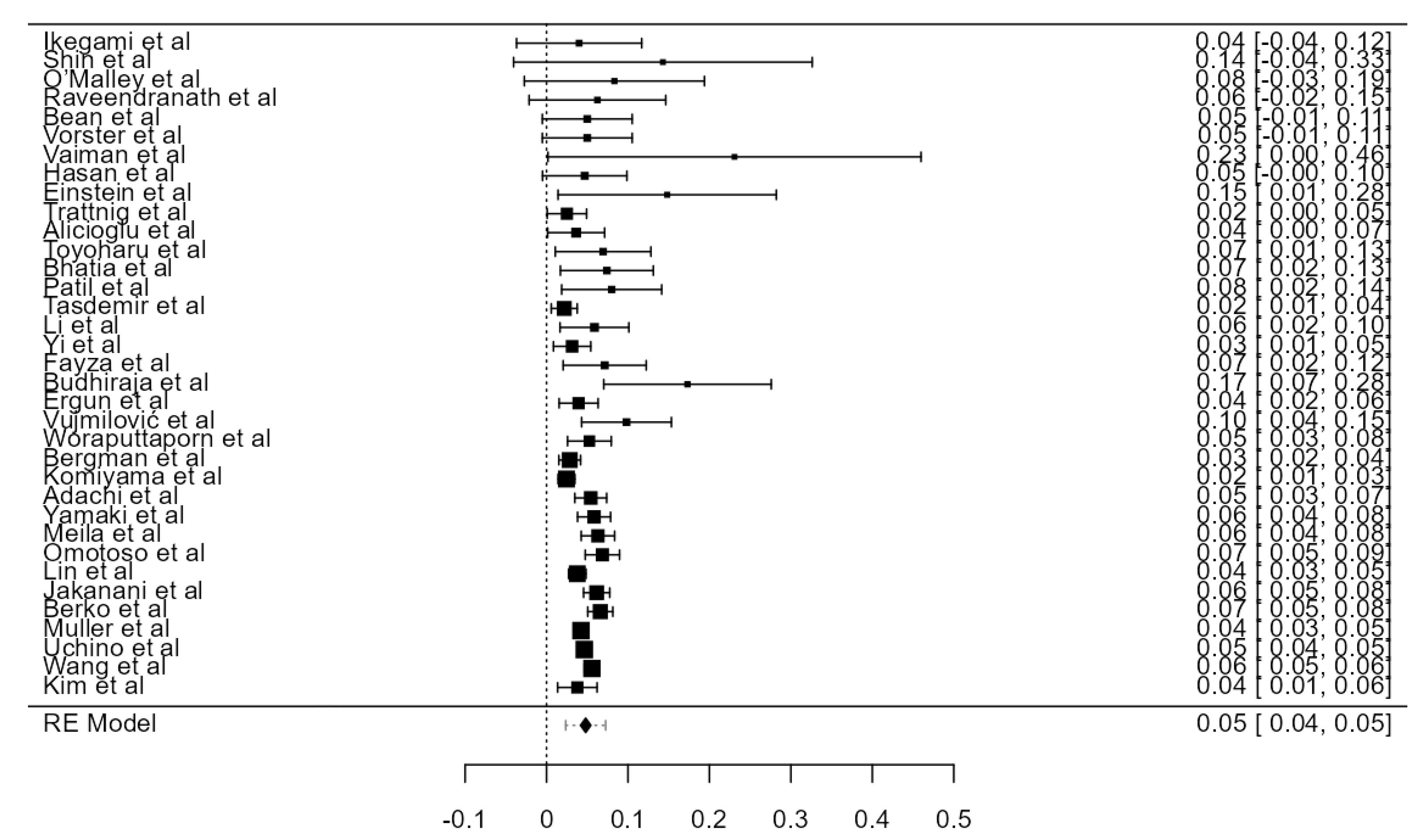
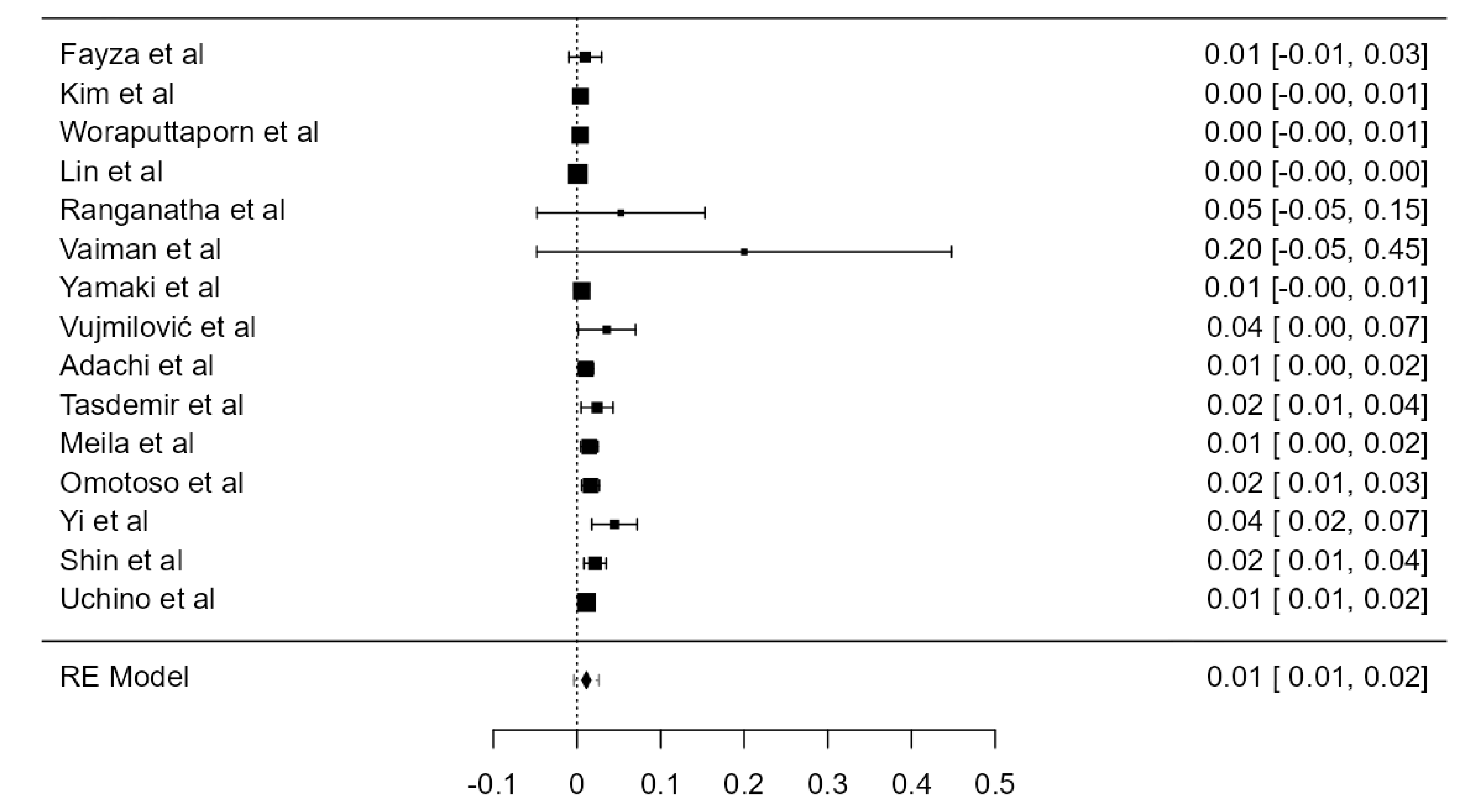
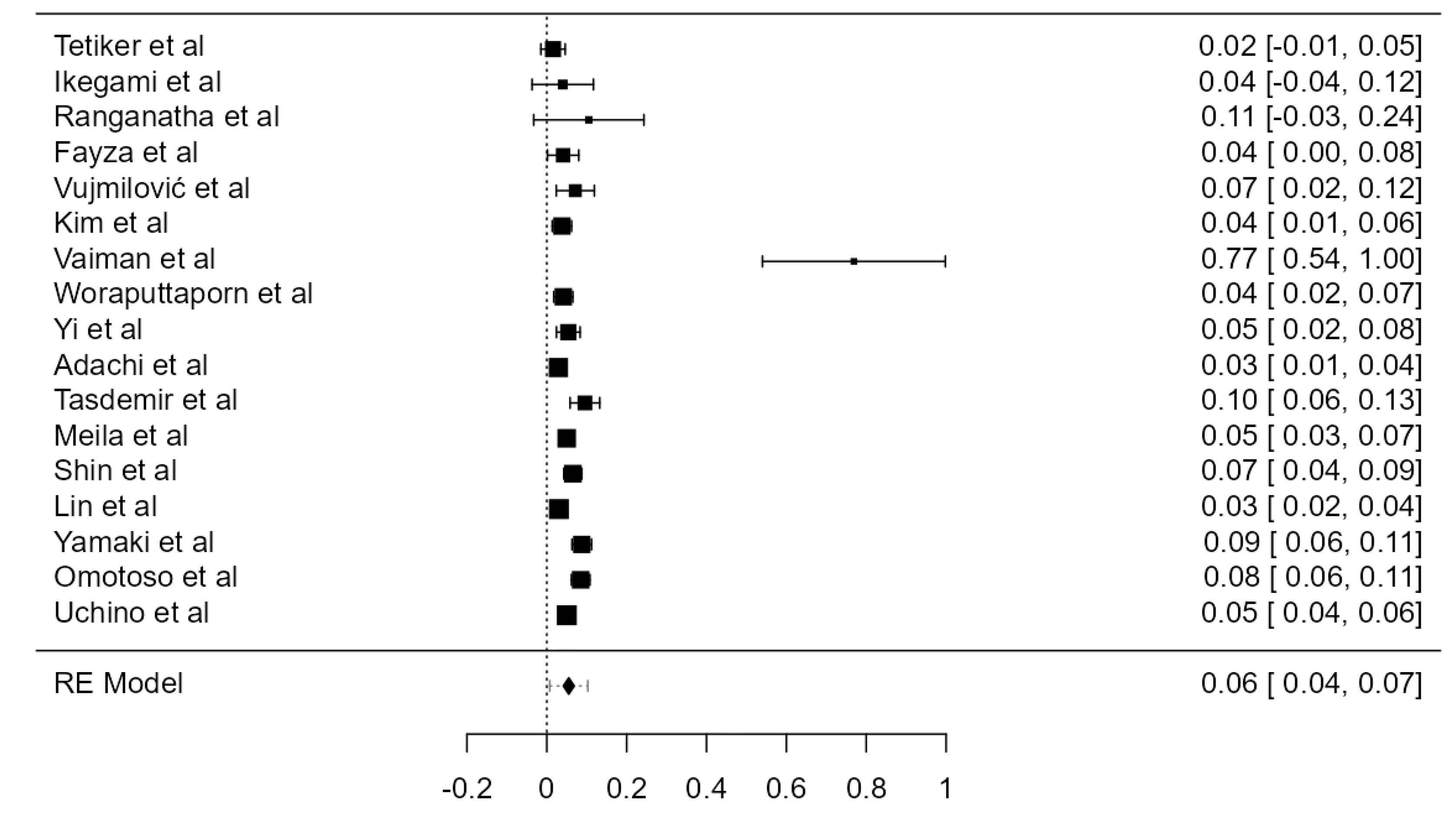
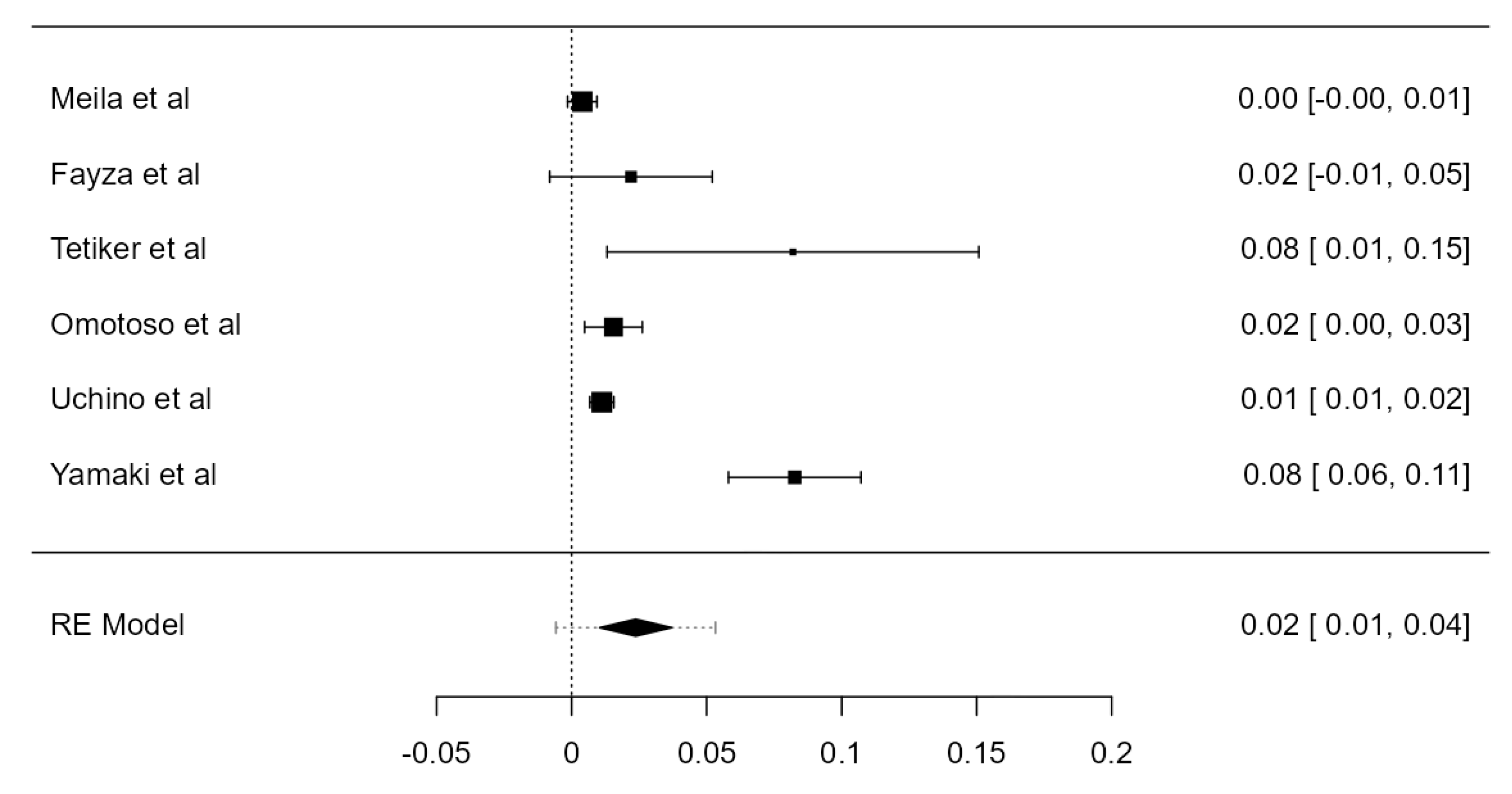
LVA arising from the aortic arch (AA) was found in thirty-five original papers, summing up 15,848 assayed LVAs. The prevalence of such anatomical variant was 4.81% (CI: 4.2–5.4, p < 0.001), as illustrated in Figure 4. The heterogeneity was substantial (I2 = 59.41%). Considering Egger’s regression test for plot asymmetry, there is a significant publication bias (p < 0.001). We did not identify any considerable difference between the prevalence determined in autopsy (5.47%) and imaging (4.59%) studies (Table 1).
3.3.3. RVA Originating from the SA
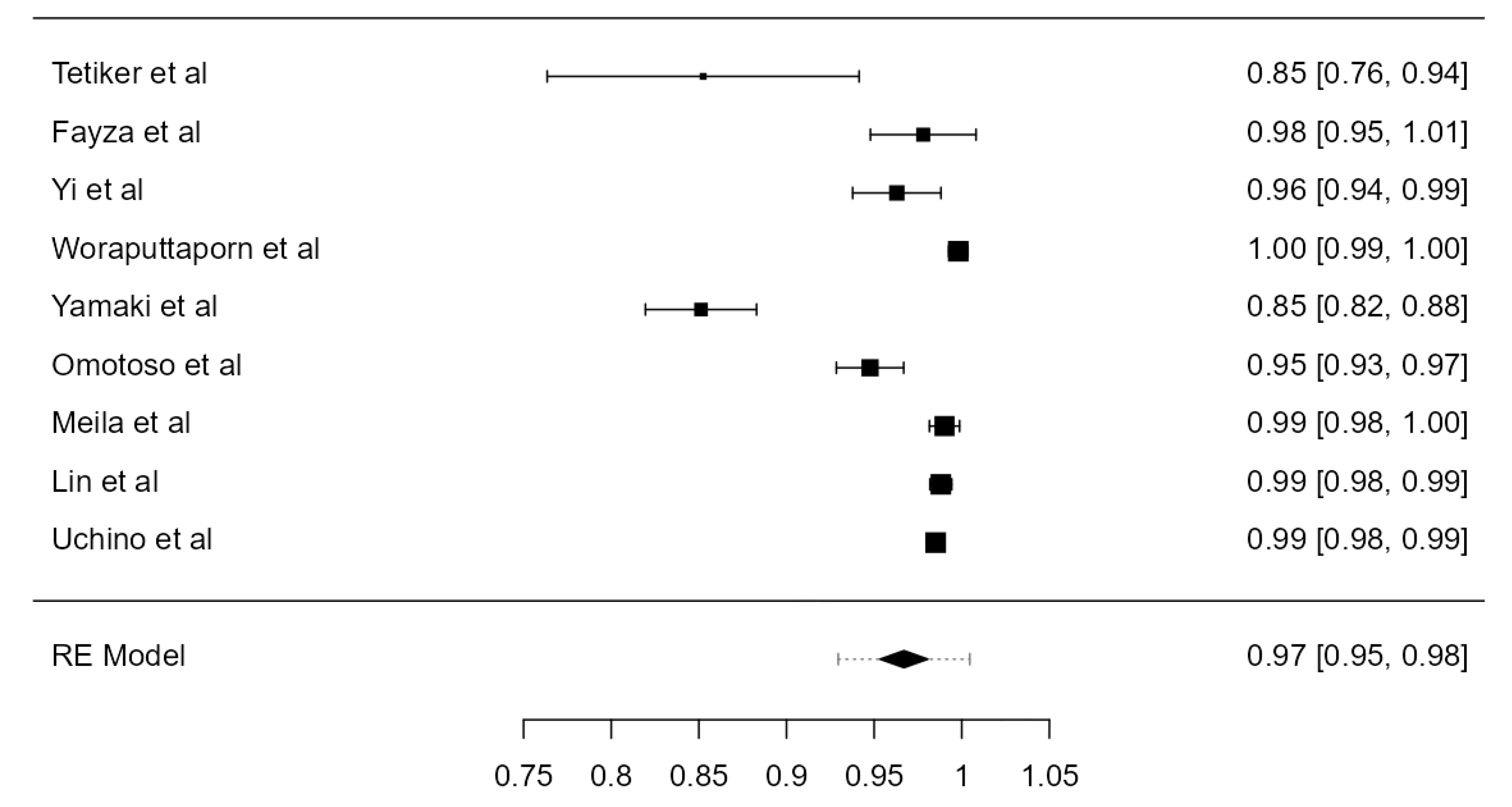
The origin of the RVA from the SA (normal or aberrant) was inspected in twenty-three studies. The total amount of investigated RVAs was 8002. The determined prevalence was 99.9% (CI: 99.8–99.9, p < 0.001), as shown in Figure 5. The heterogeneity was not important (I2 = 0%). Regarding Egger’s plot asymmetry regression test, a significant publication bias was found (p < 0.001). No significant prevalence divergence was discovered in autopsy (99.8%) and imaging studies (99.9%) (Table 1).
3.3.4. RVA Originating from the AA
In total, 2992 RVAs were examined in four different original studies that reported the presence of an RVA arising from the AA. This type of origin was only found in 5 RVAs. The prevalence was not statistically significant (p = 0.306). The heterogeneity was not important (I2 = 11.7%) and the publication bias was not statistically significant (p = 0.069), as shown in Table 3.
3.3.5. RVA Originating from the Right Common Carotid Artery
Four articles, analyzing 4368 RVAs, described 8 vessels arising from the right common carotid artery (RCCA). The overall prevalence was 0.126% (CI: 0–0.2, p = 0.019), presented in Table 3. The heterogeneity was not important (I2 = 0%). Based on Egger’s regression test for plot asymmetry, there was not a significant publication bias (p = 0.130).
3.3.6. RVA Originating from the Brachiocephalic Trunk
Three original papers described 9 out of 848 RVAs arising from the brachiocephalic trunk (BCT). The overall prevalence was 0.539% (CI: −0.5–1.6, p = 0.325), as shown in Table 3. The heterogeneity was substantial (I2 = 73%). Considering Egger’s regression test for plot asymmetry, there is a significant publication bias (p = 0.009).
3.4. TF Entrance of the VA
3.4.1. C3 TF Entrance Prevalence
C3 TF Entrance of the LVAs Originating from the AA
Out of forty LVAs that originated from the AA, four of them entered the TF at the level of the third vertebra. The prevalence was 8.11% (CI: −0.2–16.4, p = 0.057), as in Table 3. The heterogeneity was not important (I2 = 0%). Based on Egger’s regression test for plot asymmetry, there was not a significant publication bias (p = 0.280).
C3 TF Entrance
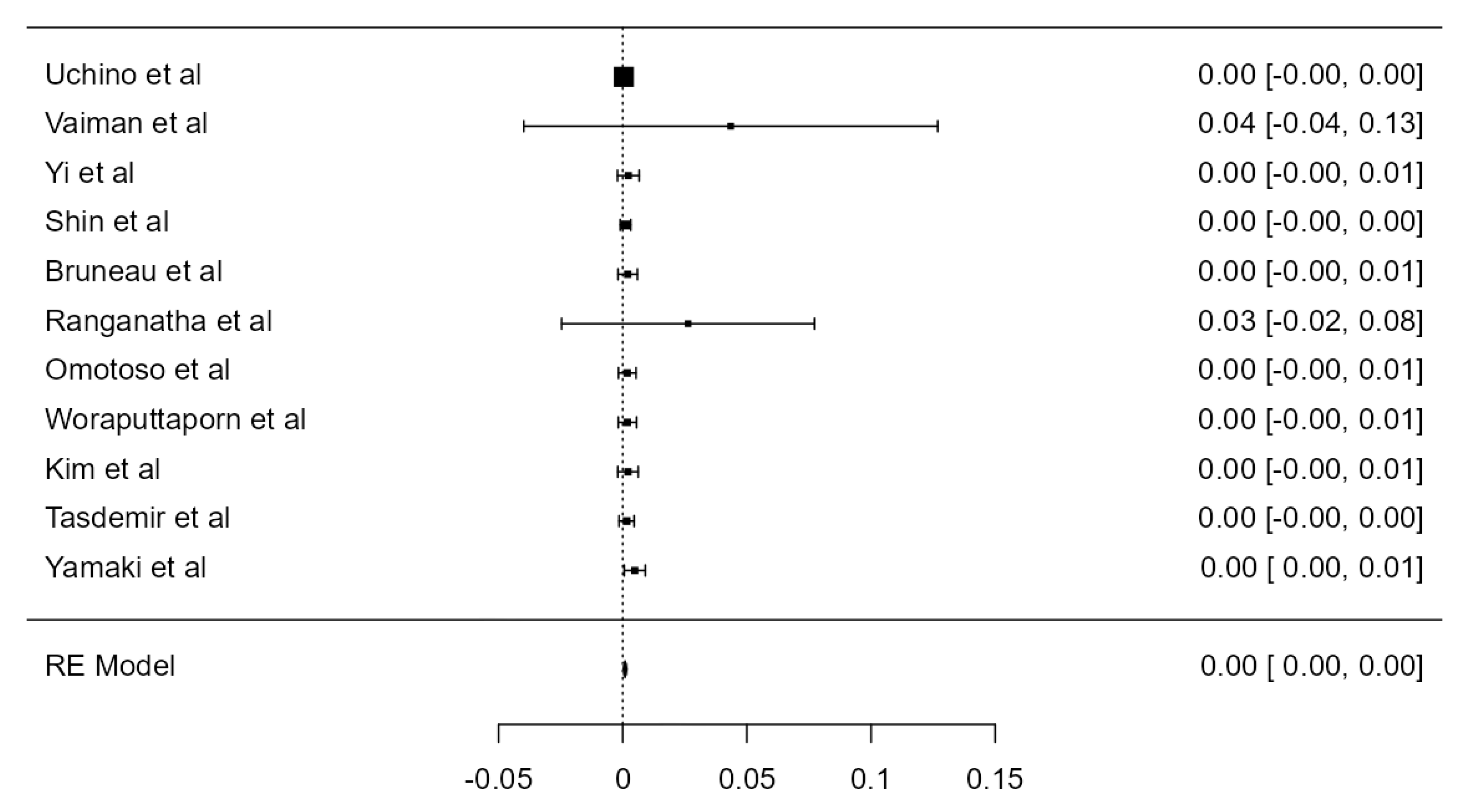
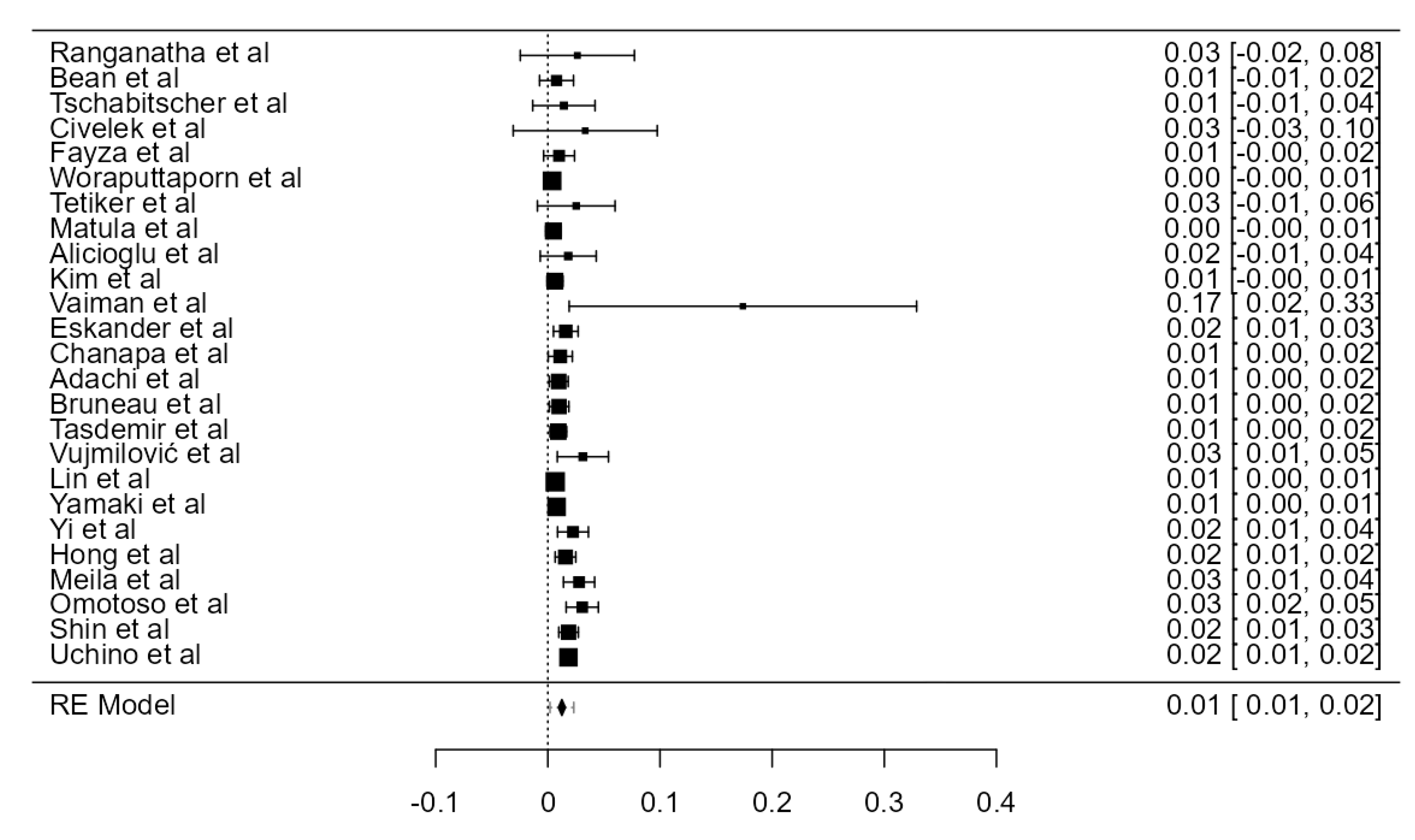
Considering the crude prevalence of the VAs entering the TF at the level of C3, eleven articles, adding up to 7449 VAs, described 15 vessels presenting such an anatomical variant (Figure 6, Figures S1 and S2). The prevalence (0.1%, CI: 0–0.2) was statistically significant (p = 0.008). The heterogeneity was not important (I2 = 0%). Publication bias measured with Egger’s regression test for plot asymmetry was significant (p = 0.009).
3.4.2. C4 TF Entrance Prevalence
C4 TF Entrance of the LVAs Originating from the AA
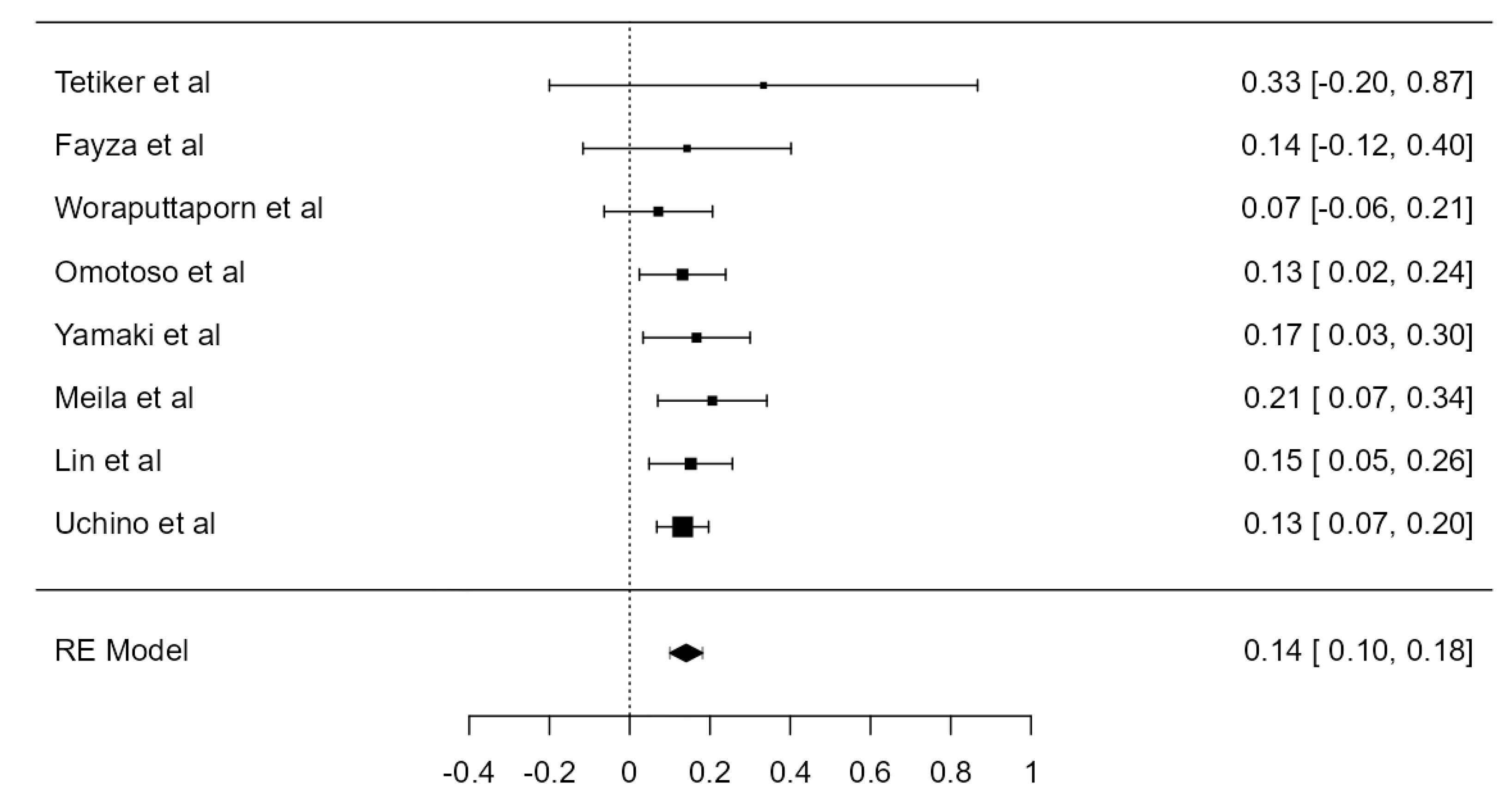
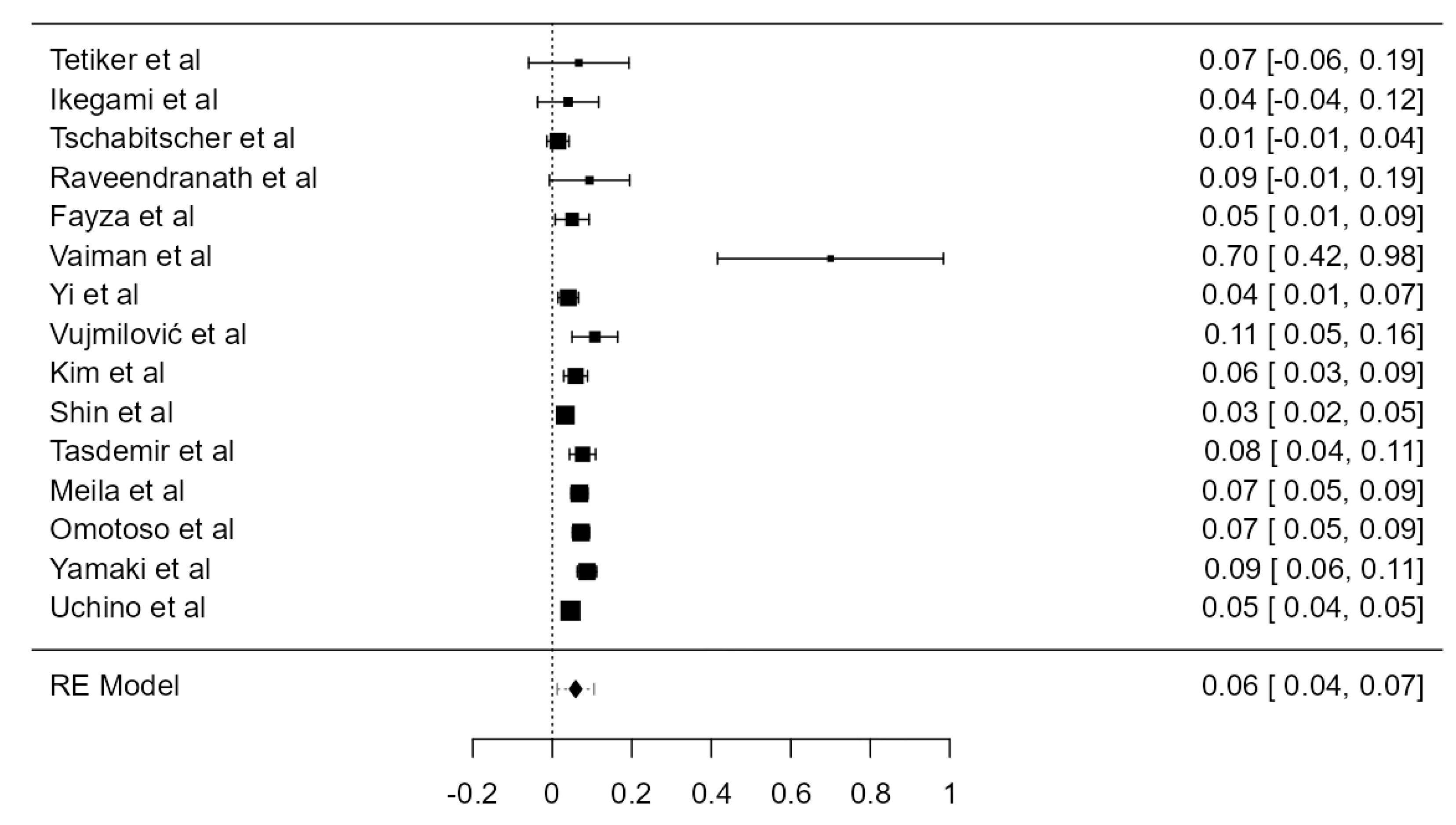
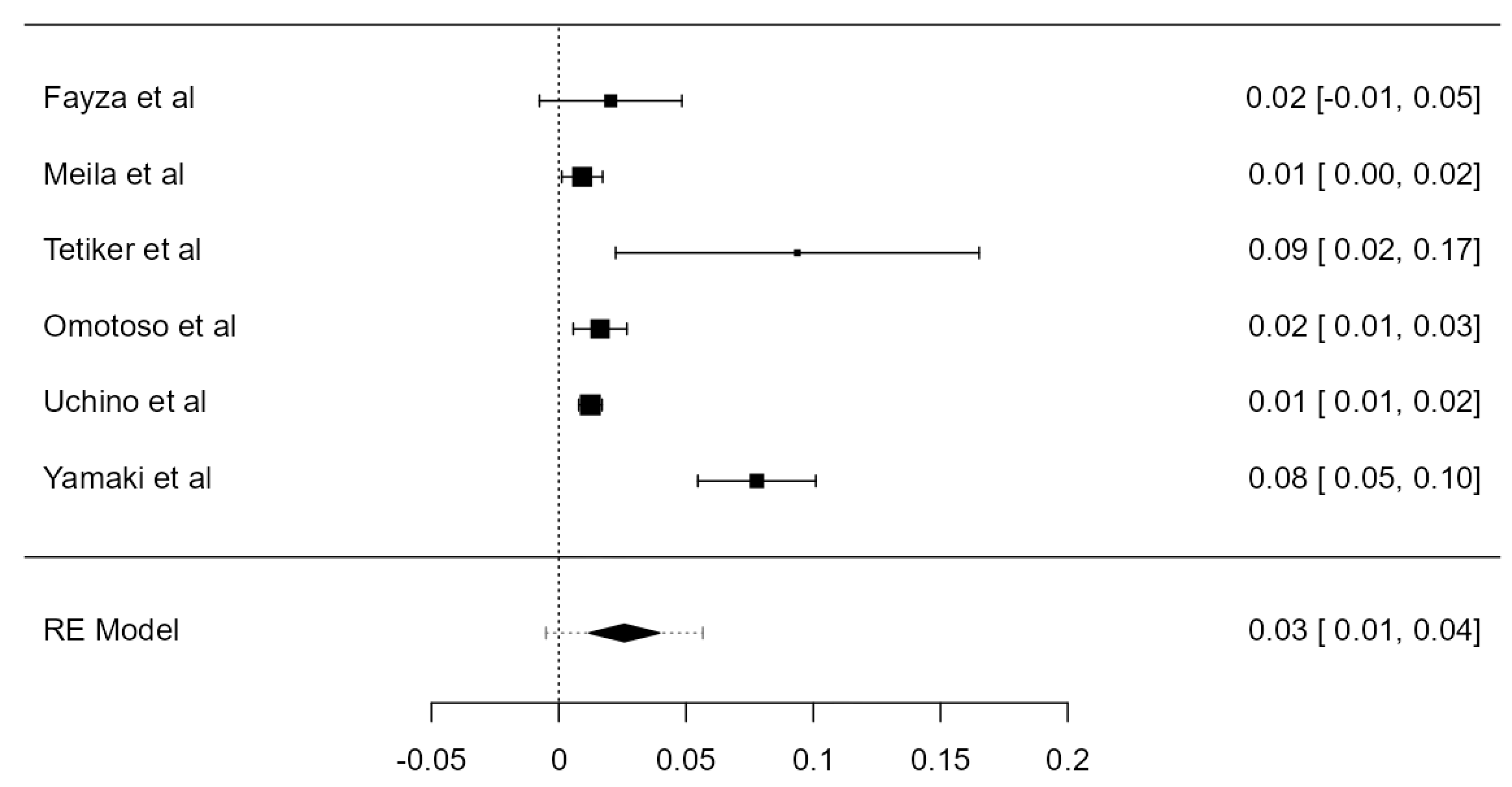
Eight articles described forty-one out of 278 LVAs arising from the AA that entered the TF at the level of the fourth vertebra. The overall prevalence was 14.1% (CI: 10–18.2, p < 0.001), as in Figure 7. The heterogeneity was not important (I2 = 0%). Publication bias was not statistically significant (p = 0.514).
C4 TF Entrance of the LVAs Originating from the SA
Four original papers presented nine out of 2736 LVAs arising from the SA, which entered the TF at C4. The prevalence was 0.337% (CI: −0.2–0.9, p = 0.216). The heterogeneity was moderate (I2 = 39.11%). The publication bias was statistically significant (p = 0.031) (Table 3).
C4 TF Entrance of the LVAs
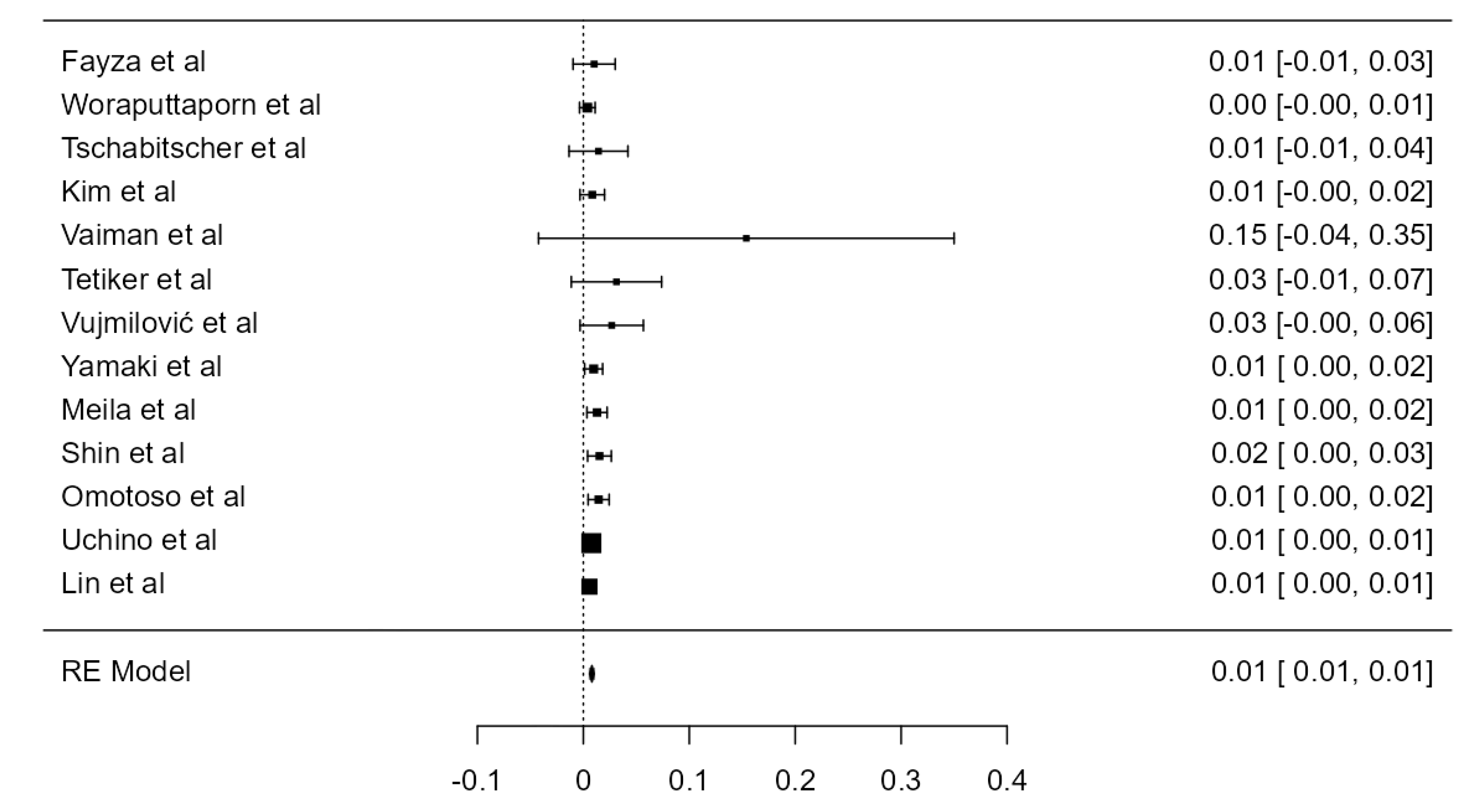
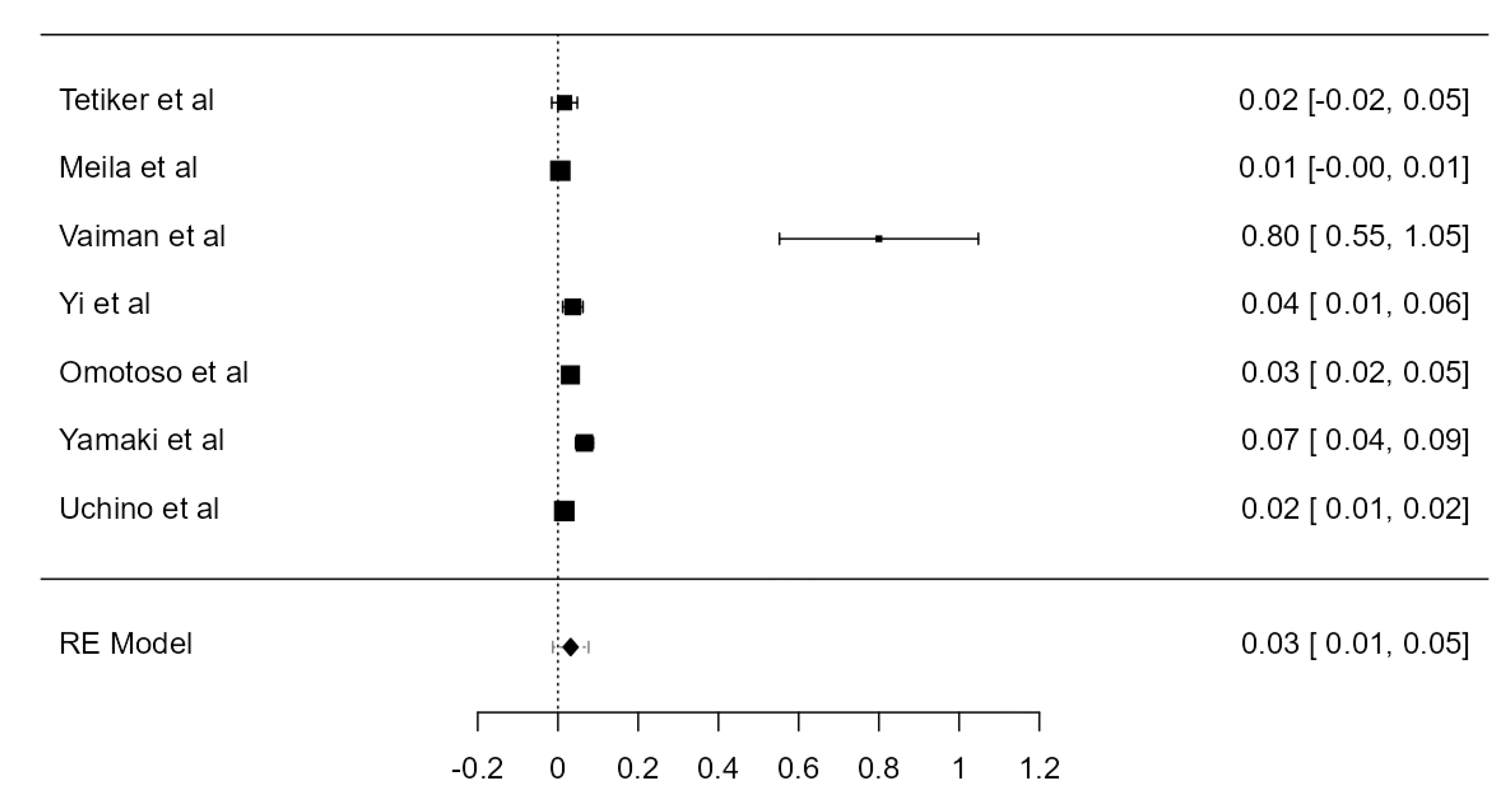
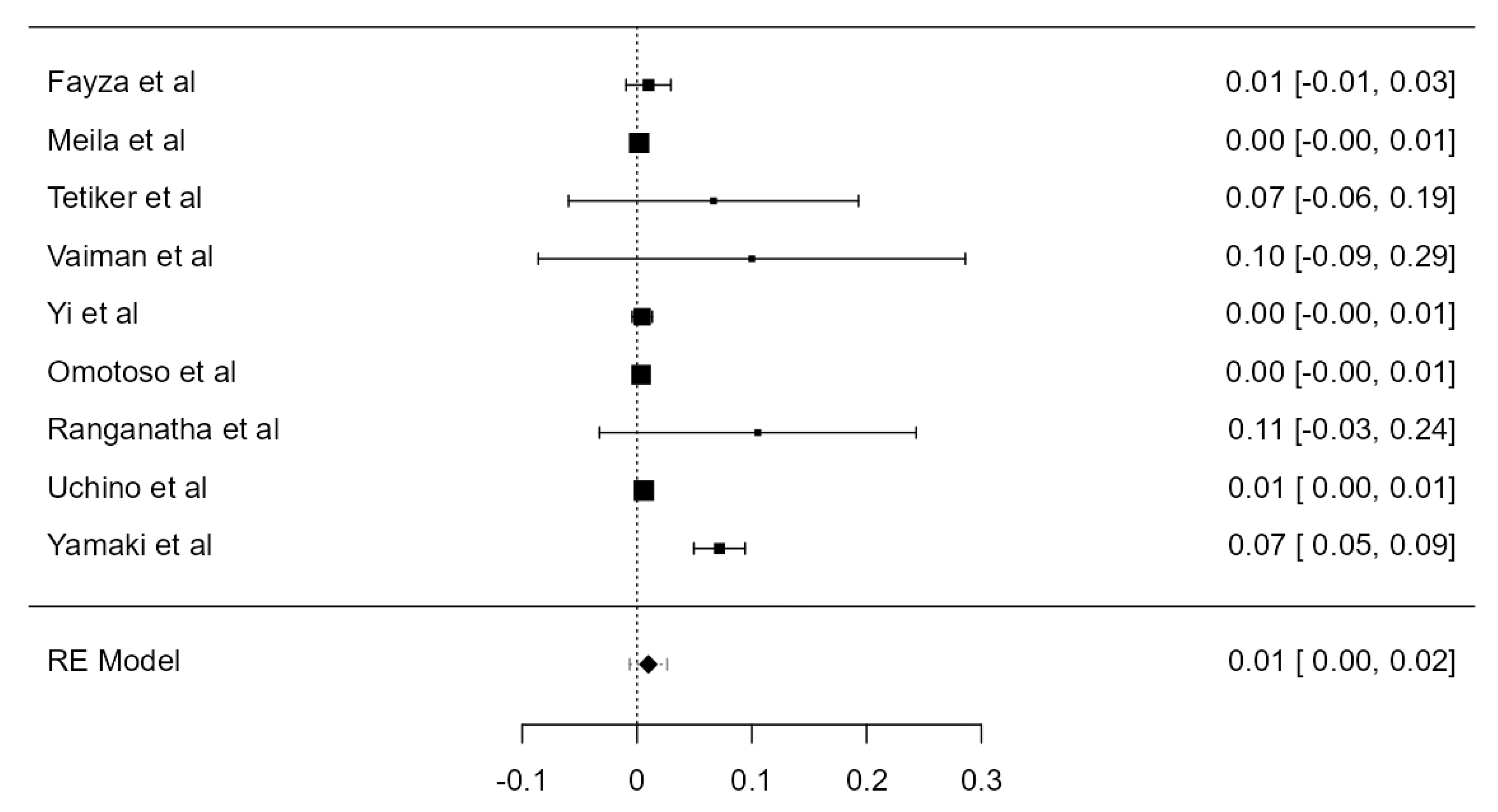
In total, 6405 LVAs analyzed in thirteen papers described sixty-three which entered the TF at C4. The overall prevalence was 0.807% (CI: 0.6–1.0, p < 0.001), as in Figure 8, Figures S3 and S4. The heterogeneity was not important (I2 = 0%). Considering Egger’s regression test for plot asymmetry, there is a significant publication bias (p = 0.009).
C4 TF Entrance of the RVAs
The TF entrance of 7183 RVAs was analyzed in 15 studies. Eighty-seven were seen entering at the level of the C4 vertebra. The prevalence was 1.14% (CI: 0.6–1.6, p < 0.001), shown in Figure 9, Figures S5 and S6. The heterogeneity was substantial (I2 = 77.99%). Egger’s regression test for plot asymmetry showed a significant publication bias (p < 0.001).
C4 TF Entrance
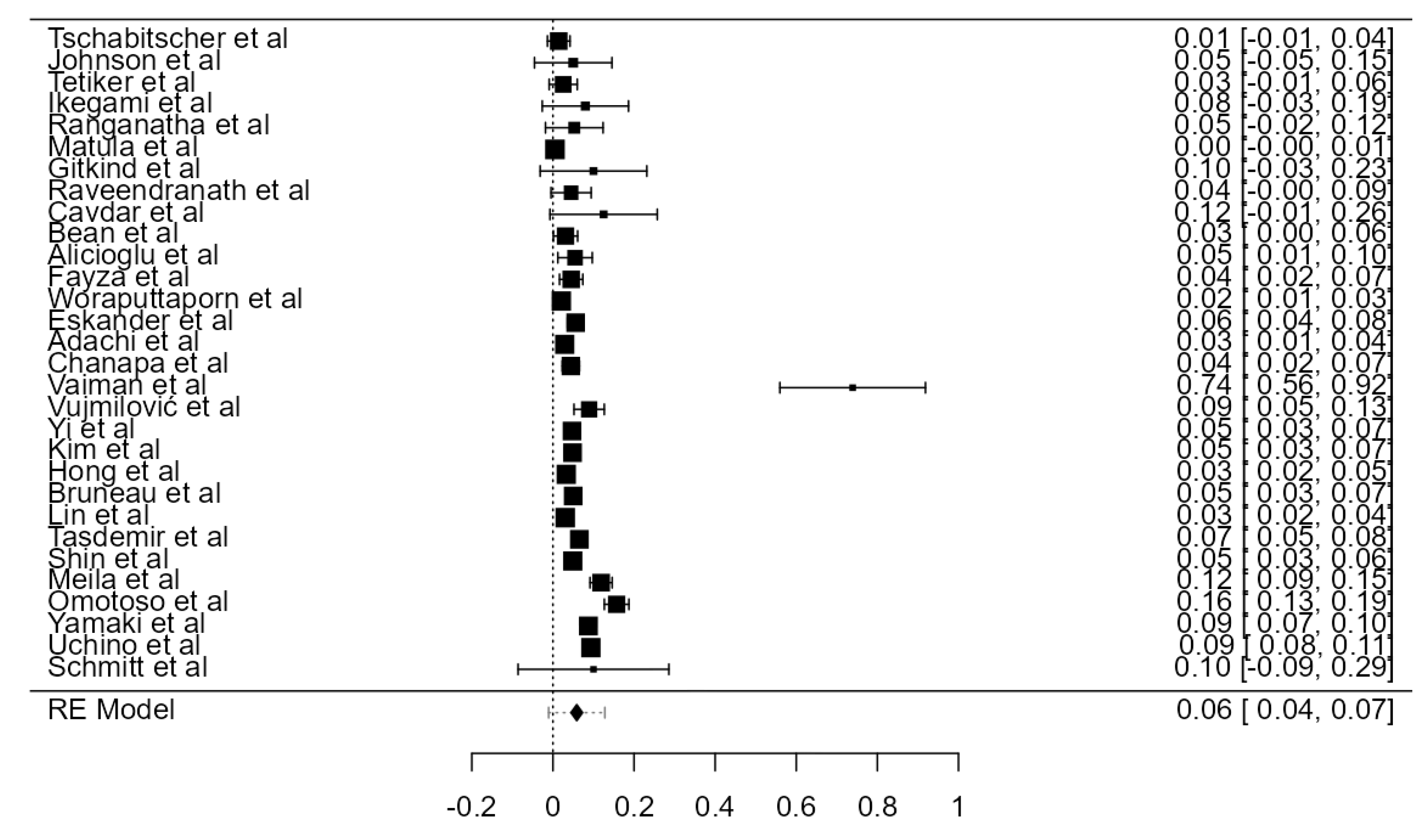
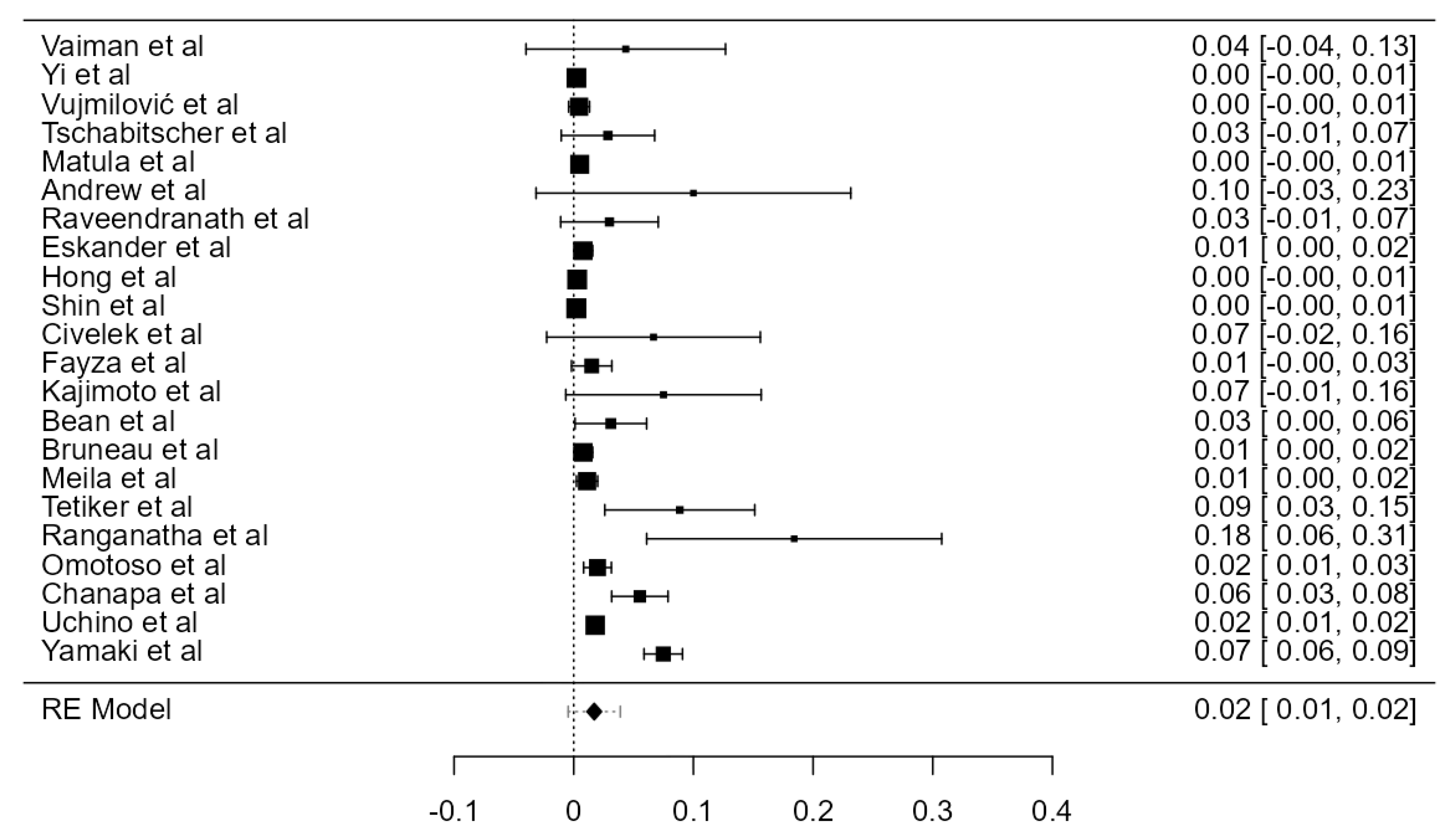
Twenty-five articles reported the entrance of 184 VAs (out of 12,528 VAs) in the TF of the fourth cervical vertebra. The crude prevalence was estimated at 1.25% (CI: 0.9–1.6, p < 0.001), as in Figure 10, Figures S7 and S8. The heterogeneity was moderate (I2 = 55.23%). Egger’s regression test for plot asymmetry showed a significant publication bias (p < 0.001). A notable disparity was noticed between prevalences from autopsy (0.7%) and imaging (1.45%) studies (Table 1).
3.4.3. C5 TF Entrance Prevalence
C5 TF Entrance of the LVAs Originating from the AA
Ten original papers analyzed 313 LVAs with AA origin. The prevalence of entrance in the TF of the fifth vertebra was 69.2% (CI: 60.8–77.5, p < 0.001), represented in Figure 11. The heterogeneity was moderate (I2 = 55.69%). The publication bias was not significant (p = 0.177).
C5 TF Entrance of the LVAs Originating from the SA
In total, 3944 AA-originated LVAs were scrutinized in seven papers. The prevalence was 3.17% (CI: 1.3–5.0, p < 0.001). Both the heterogeneity (I2 = 91.83%) and the publication bias (p < 0.001) were significant (Figure 12, Figures S9 and S10).
C5 TF Entrance of the LVAs
In total, 7359 LVAs examined in seventeen studies were included in the current evaluation. The prevalence of the TF entrance at C5 was 5.51% (CI: 4.1–6.9, p < 0.001), as in Figure 13, Figures S11 and S12. The heterogeneity was substantial (I2 = 82.74%). Considering Egger’s regression test for plot asymmetry, there was a significant publication bias (p < 0.001).
C5 TF Entrance of the RVAs
Analyzing the prevalence of RVAs entering the TF at the level of C5, we found a result of 5.88% (CI: 4.4–7.4, p < 0.001). The heterogeneity was substantial (I2 = 74.81%), and the publication bias was significant (p = 0.002) (Figure 14, Figures S13 and S14).
C5 TF Entrance
In total, 12,664 VAs, examined in thirty articles, were included in the present analysis. The crude prevalence of the VA entering the TF at C5 was 5.87% (CI: 4.4–7.3, p < 0.001), as shown in Figure 15, Figures S15 and S16. The heterogeneity was significant (I2 = 92.73%). Based on Egger’s regression test for plot asymmetry, there was a significant publication bias (p < 0.001). We discovered a notable difference between prevalences determined in autopsy (4.37%) and imaging (8.36%) studies (Table 1).
3.4.4. C6 TF Entrance Prevalence
C6 TF Entrance of the AA-Originating LVAs
In total, 251 LVAs with AA origin from eight papers were evaluated. The prevalence of the C6 TF entrance in such vessels was 10.6% (CI: 4.2–17.0, p = 0.001), shown in Figure 16. The heterogeneity was substantial (I2 = 61.06%). The publication bias was significant (p = 0.001).
C6 TF Entrance of the SA-Originated LVAs
In total, 5450 SA-originating VAs from 9 studies were included. The determined prevalence of the C6 TF entrance was 96.7% (CI: 95.3–98.1, p < 0.001), presented in Figure 17. The heterogeneity (I2 = 93.09%) and the publication bias (p < 0.001) were significant.
C6 TF Entrance of the LVAs
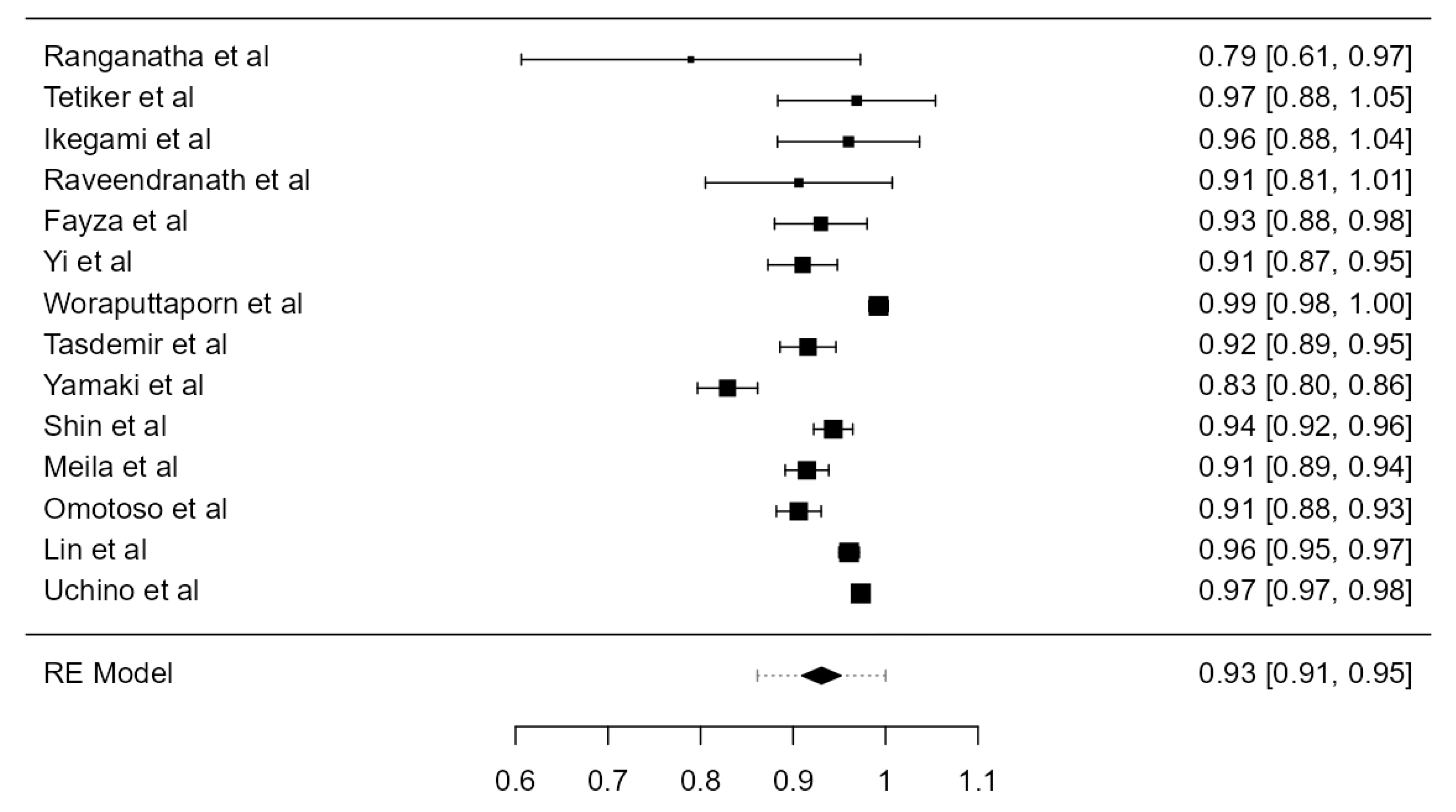
Fourteen articles, adding up to 6593 LVAs, were included. The overall prevalence was 92.2% (CI: 90.3–94.1, p < 0.001), as in Figure 18. Both the heterogeneity (I2 = 86.21%) and the publication bias (p = 0.014) were significant.
C6 TF Entrance of the RVAs
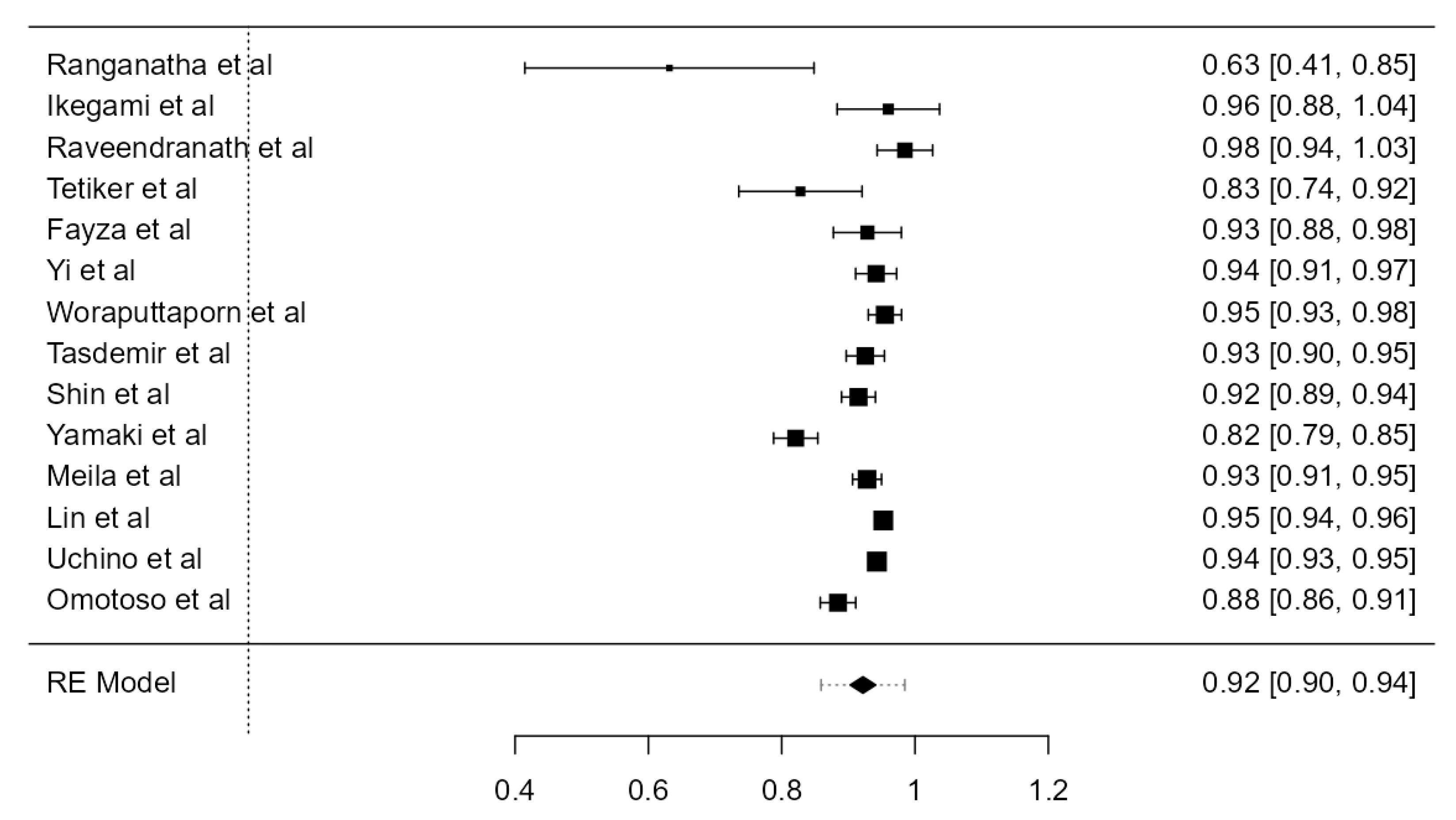
Fourteen studies, describing 6495 RVAs, contained data about the TF entrance of the RVAs. The overall prevalence was 93.1% (CI: 91.0–95.2, p < 0.001), as in Figure 19. The heterogeneity was significant (I2 = 92.29%). The publication bias was not significant (p = 0.061).
C6 TF Entrance
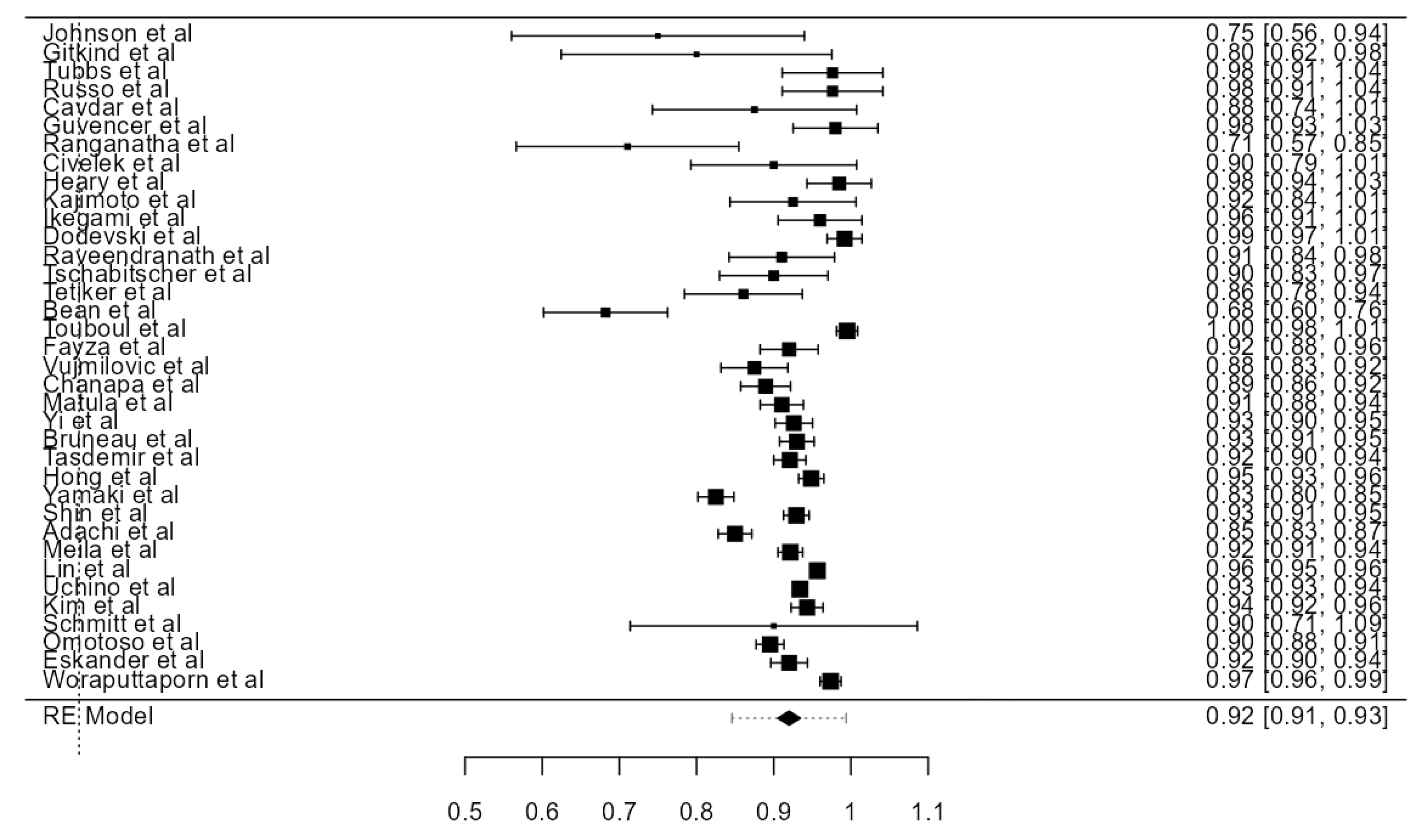
Thirty-six papers, including 18,002 VAs, were examined and included in the current analysis. The crude prevalence of the VA entering the TF at the C6 level was 92.0% (CI: 90.5–93.4, p < 0.001), presented in Figure 20. The heterogeneity was significant (I2 = 91.63%). Based on an Egger’s regression test for plot asymmetry, there was a significant publication bias (p = 0.001). A prevalence difference of 5.4% was detected, comparing autopsy (88.2%) and imaging (93.6%) studies (Table 1).
3.4.5. C7 TF Entrance Prevalence
C7 TF Entrance of the AA-Originating LVAs
Four studies, including 181 AA-originating LVAs, were analyzed. The prevalence of the C7 TF entrance was 3.95% (CI: 1.1–6.8, p = 0.006), shown in Table 3. The heterogeneity was most likely not important (I2 = 0%). The publication bias was not significant (p = 0.173).
C7 TF Entrance of the SA-Originating LVAs
3809 SA-originating LVAs from six articles were included. The prevalence of the C7 TF entrance was 2.37% (CI: 1.0–3.7, p < 0.001). The heterogeneity (I2 = 88.75%) and the publication bias (p < 0.001) were significant (Figure 21).
C7 TF Entrance of the LVAs
Six articles evaluating 4027 LVAs were evaluated. The prevalence of the C7 TF entrance was 2.58% (CI: 1.2–4.0, p < 0.001), shown in Figure 22. The heterogeneity was significant (I2 = 86.17%). The publication bias was significant (p = 0.002).
C7 TF Entrance of the RVAs
Nine papers, adding up to 4182 RVAs, were included to determine the C7 TF entrance prevalence of the right VAs. The overall value was 0.994% (CI: 0.3–1.7, p = 0.006), as in Figure 23. The heterogeneity was substantial (I2 = 81.03%). The publication bias, determined using Egger’s regression test for plot asymmetry, was significant (p < 0.001).
C7 TF Entrance
Twenty-two papers, adding up to 9159 VAs, were included in the present analysis. The crude prevalence of the C7 TF entrance was 1.72% (CI: 1.1–2.3, p < 0.001), shown in Figure 24. The heterogeneity was significant (I2 = 86.2%). The publication bias was significant (p < 0.001). A major prevalence difference was discovered between autopsy (5.42%) and imaging (0.8%) studies (Table 1).
3.5. Prevalence of the VA Course
3.5.1. Tortuosity
Overall Tortuosity
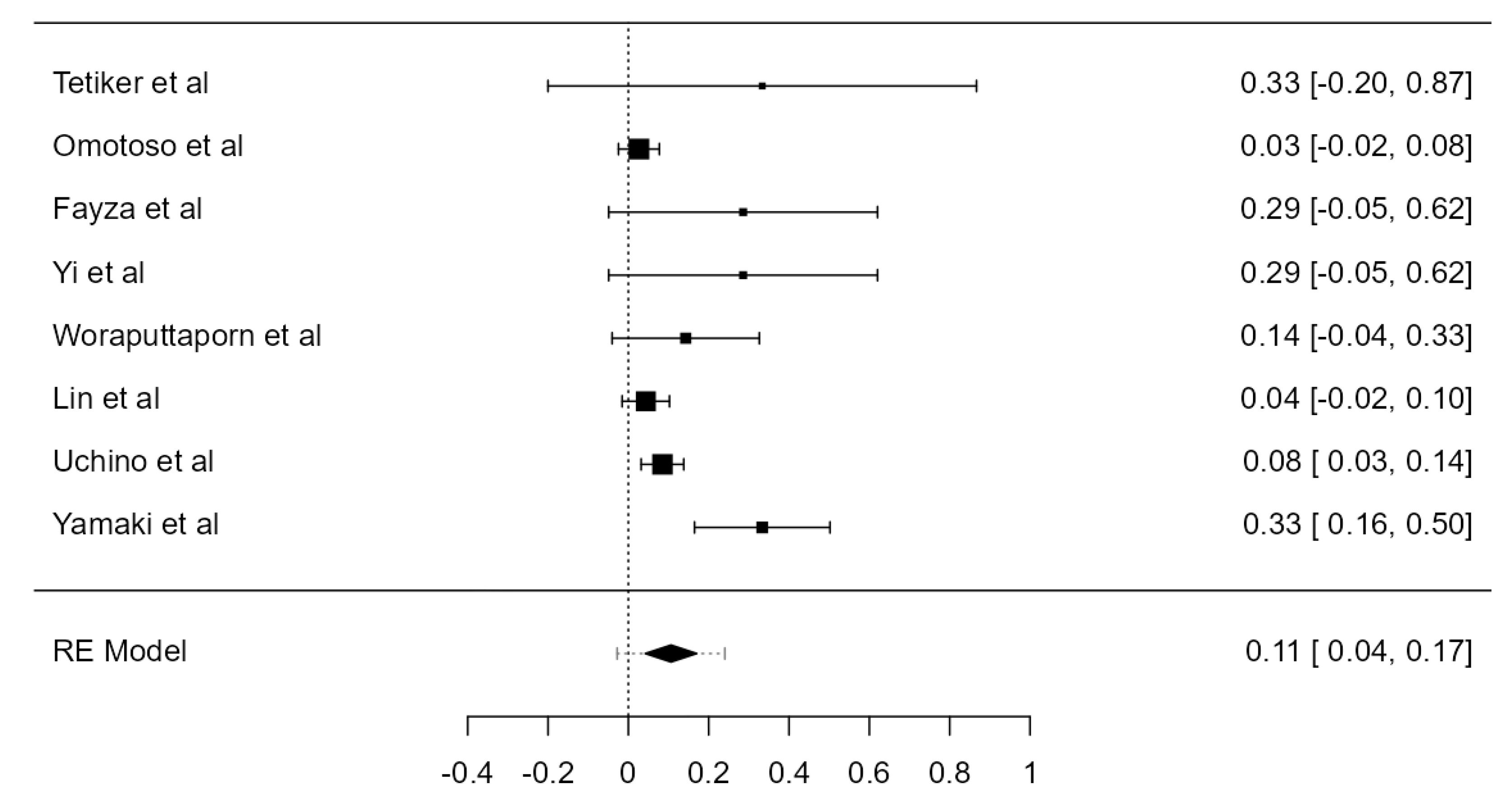
Fifteen original papers, summing 3149 VAs, were examined to determine the crude tortuosity prevalence of the V1 and V2 segments. Two articles reported different values for “significant” or “high” tortuosity [60,69]. These values were added up to the tortuosity value and analyzed altogether. The prevalence was estimated at 26.6% (CI: 21.4–31.7, p < 0.001), as represented in Figure 25. The heterogeneity was significant (I2 = 98.8%). The publication bias, based on Egger’s regression test for plot asymmetry, was significant (p < 0.001). A prevalence difference of 5.2% was found while comparing autopsy (31.0%) and imaging (25.8%) articles (Table 1).
Coronal Tortuosity Prevalence
Three papers, adding up to 380 tortuous VAs, were included in the analysis of coronal tortuosity prevalence. The determined value is 16.6% (CI: 8.4–24.8, p < 0.001), as in Table The heterogeneity was substantial (I2 = 78.87%). The publication bias was significant (p < 0.001).
Sagittal Tortuosity Prevalence
The sagittal tortuosity prevalence was 22.8% (CI: 17.6–28.0, p < 0.001). The heterogeneity was most likely not important (I2 = 27.87%). The publication bias, based on Egger’s regression test for plot asymmetry, was not significant (p = 0.058) (Table 3).
Transverse Tortuosity Prevalence
The transverse tortuosity prevalence was the highest, with a percentage of 30.1 (CI: 18.2–42.0, p < 0.001), shown in Table 3. The heterogeneity was substantial (I2 = 84.63%). The publication bias was significant (p = 0.008).
3.5.2. Straight V1 Segment Prevalence
Three articles, including 430 VAs, were analyzed. The prevalence of a straight pretransverse segment was 45.2% (CI: 35.7–54.6, p < 0.001). The heterogeneity was substantial (I2 = 74.14%). The publication bias was not significant (p = 0.605) (Table 3).
3.6. VA Dominance
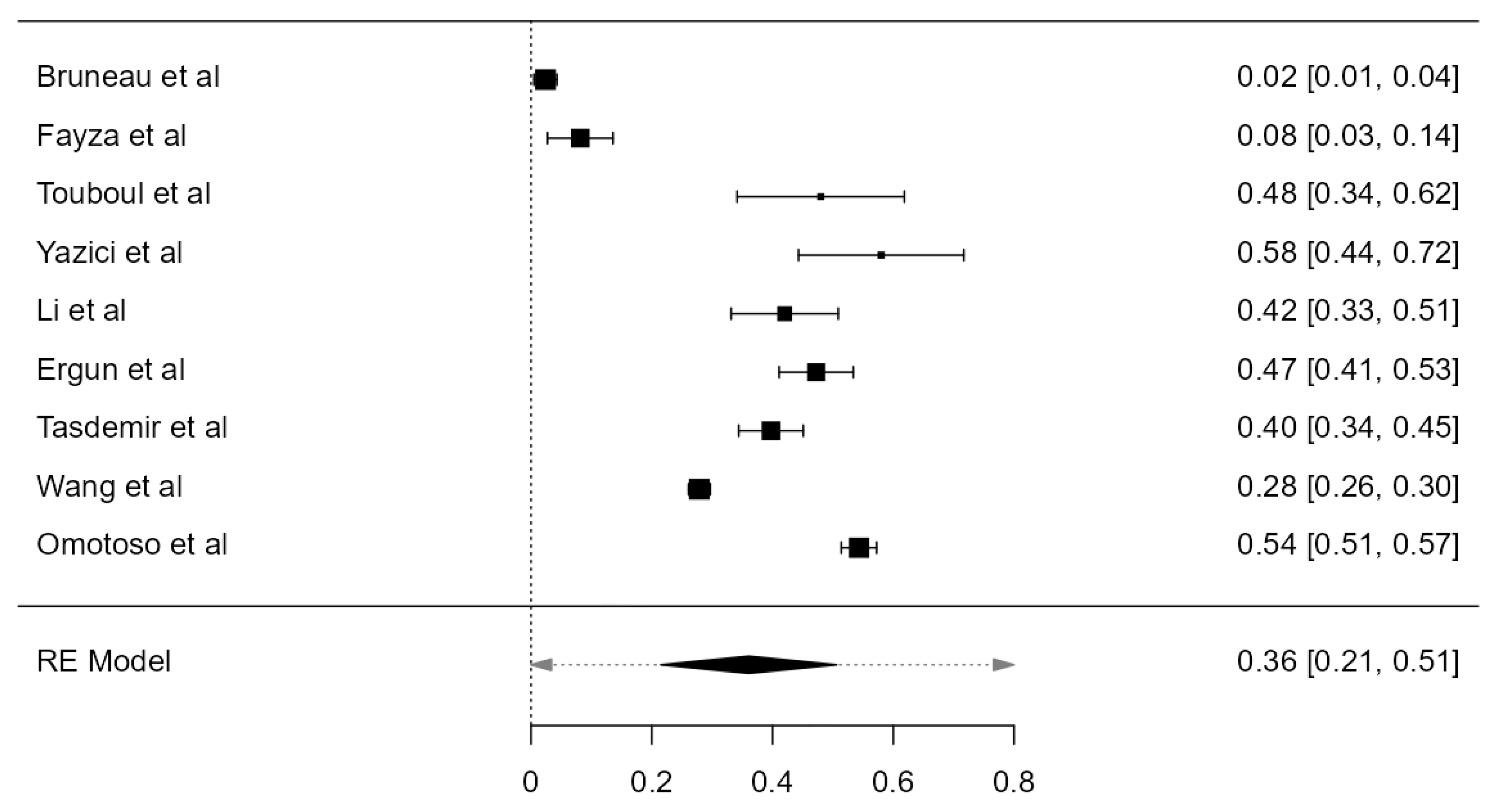
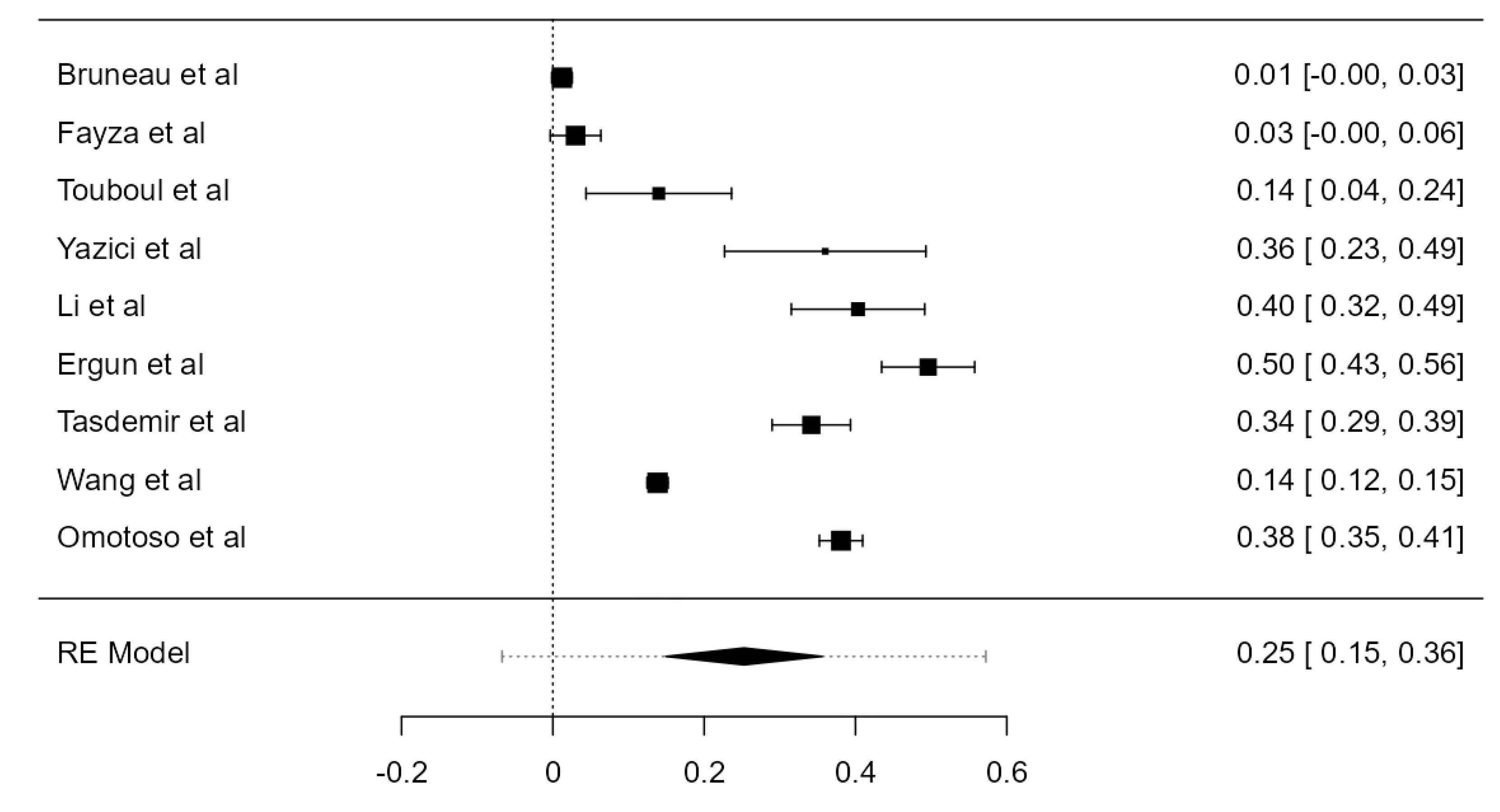
Nine studies, summing 4623 VAs, were included in the current analysis to determine the LVA/RVA dominance crude prevalence. Considering the LVA, the prevalence was 36.1% (CI: 21.5–50.6, p < 0.001), higher in comparison with RVA prevalence, which was 25.3% (CI: 14.9–35.6, p < 0.001), shown in Figure 26 and Figure 27. The heterogeneity was significant (I2 = 99.27%, 99.08%, respectively). The publication bias was not significant (p = 0.150, 0.095, respectively).
3.7. VA Hypoplasia Prevalence
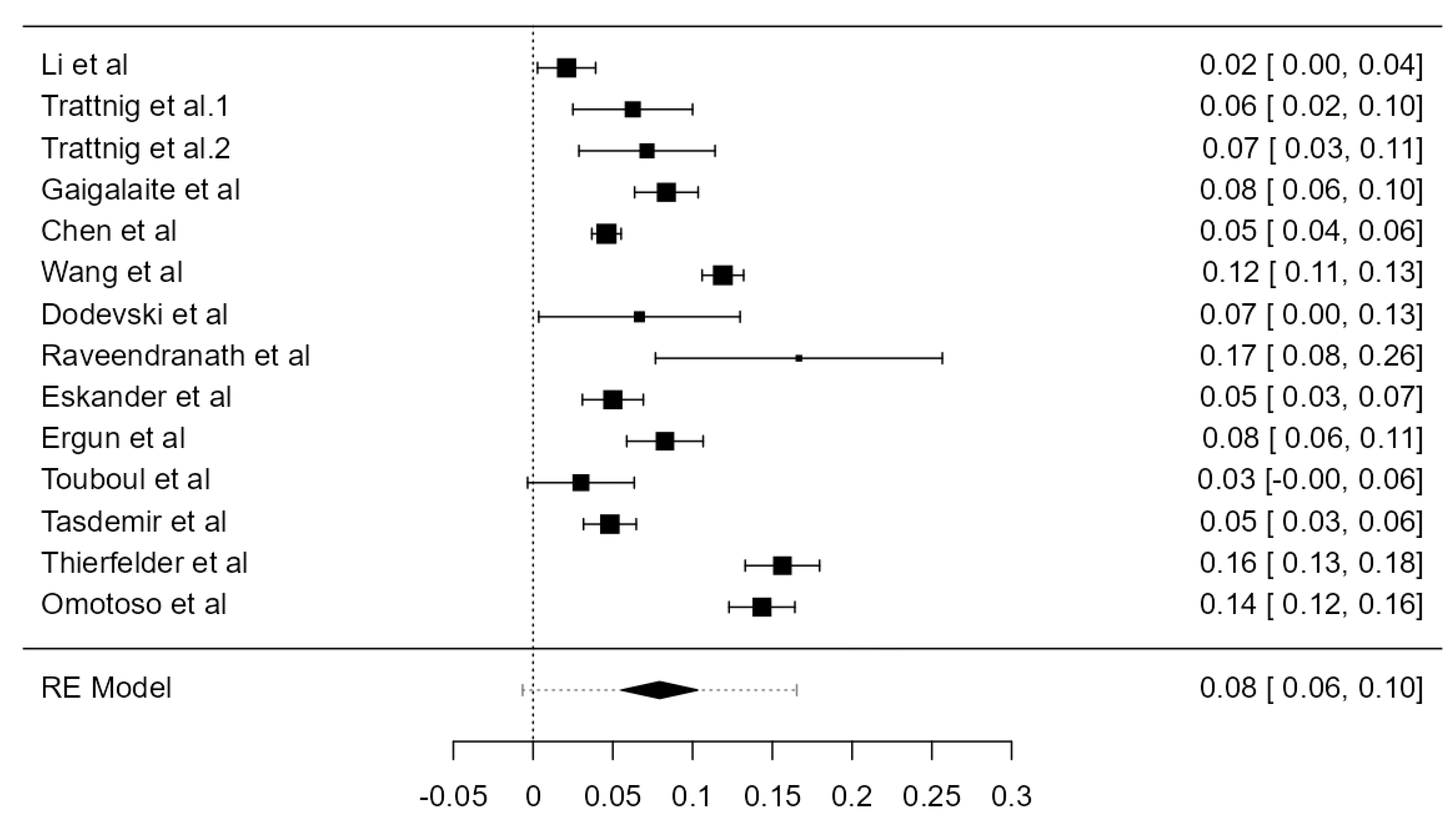
Fourteen articles were included, adding up to 9570 VAs. The crude prevalence of such a condition was 7.94% (CI: 5.6–10.3, p < 0.001), shown in Figure 28. The heterogeneity was significant (I2 = 94.42%). The publication bias was not significant (p = 0.425). No major difference was detected between autopsy and imaging articles (Table 1).
4. Discussion
4.1. Anatomical Incidence
Considering the VA topography and morphology, the results are in accordance with the information stated in different anatomical textbooks [76,77]. The most prevalent site of origin for both LVA and RVA is the SA with a frequency of 94.1%, respectively 99.9%. Regarding the entrance in a certain TF, most VAs (92%) enter at the level of the sixth cervical vertebra, followed by C5, C7, C4, and, less frequently, C3. AA-originated LVAs present the highest frequency of entrance into the fifth cervical vertebra TF (69.2%), then C4, C6, C3, and C7. This result contradicts Morris [78] who stated that AA-originated LVAs commonly enter the TF of the fourth cervical vertebra. Roughly one out of four VAs presented a form of tortuosity, the transverse tortuosity having the highest prevalence. From the current meta-analysis, it also resulted in a higher frequency of LVA dominance compared to RVA, which suggests that a greater volume of blood is conducted through the LVA to the brain. Of significant clinical importance is the fact that LVA damage may lead to deterioration of the brain’s blood supply [79,80]. As regards hypoplastic VAs, the prevalence is relatively low; roughly 8% of the vessels were reported with a diameter lower than 3.5 mm. VA origin has been widely evaluated and it is acknowledged that the most frequent origin on each side is from the SA. Arteries originating from any other site are considered aberrant [81,82]. LVAs most frequent anatomic variant is the direct aortic origin, with a prevalence of 2.4–5.8% [83]. In the current study, we determined a prevalence of 4.81% of the AA-originated LVA, which conforms with the range 2.4–4.8% [83] reported by Adachi et al. [19], Yamaki et al. [73], Uchino et al. [69], etc. Other origins have been reported: left external carotid artery, thyrocervical trunk, carotid bulb, left common carotid artery, but the frequency is extremely low (0.1–0.2%) [82] and there is an insufficient amount of prevalence studies that reported these variants. Concerning RVA’s abnormal origin, the brachiocephalic trunk was the most frequent with a prevalence of 0.539%, followed by RCCA and AA origin. As these variants are remarkably uncommon, they have been mostly communicated as case reports [84,85,86,87,88,89].
As documented in Bergman’s Comprehensive Encyclopedia of Human Anatomic Variation, VAs could originate from any carotid artery, common, internal, or external [90]. However, these anatomical possibilities correspond to persistent proatlantal arteries which are rarely found [91] and could appear as either V3 segments with carotid origin, with normoplastic or hypoplastic V1–V2 VAs supplied from the SAs [92], or as proatlantal arteries with absent VAs [93].
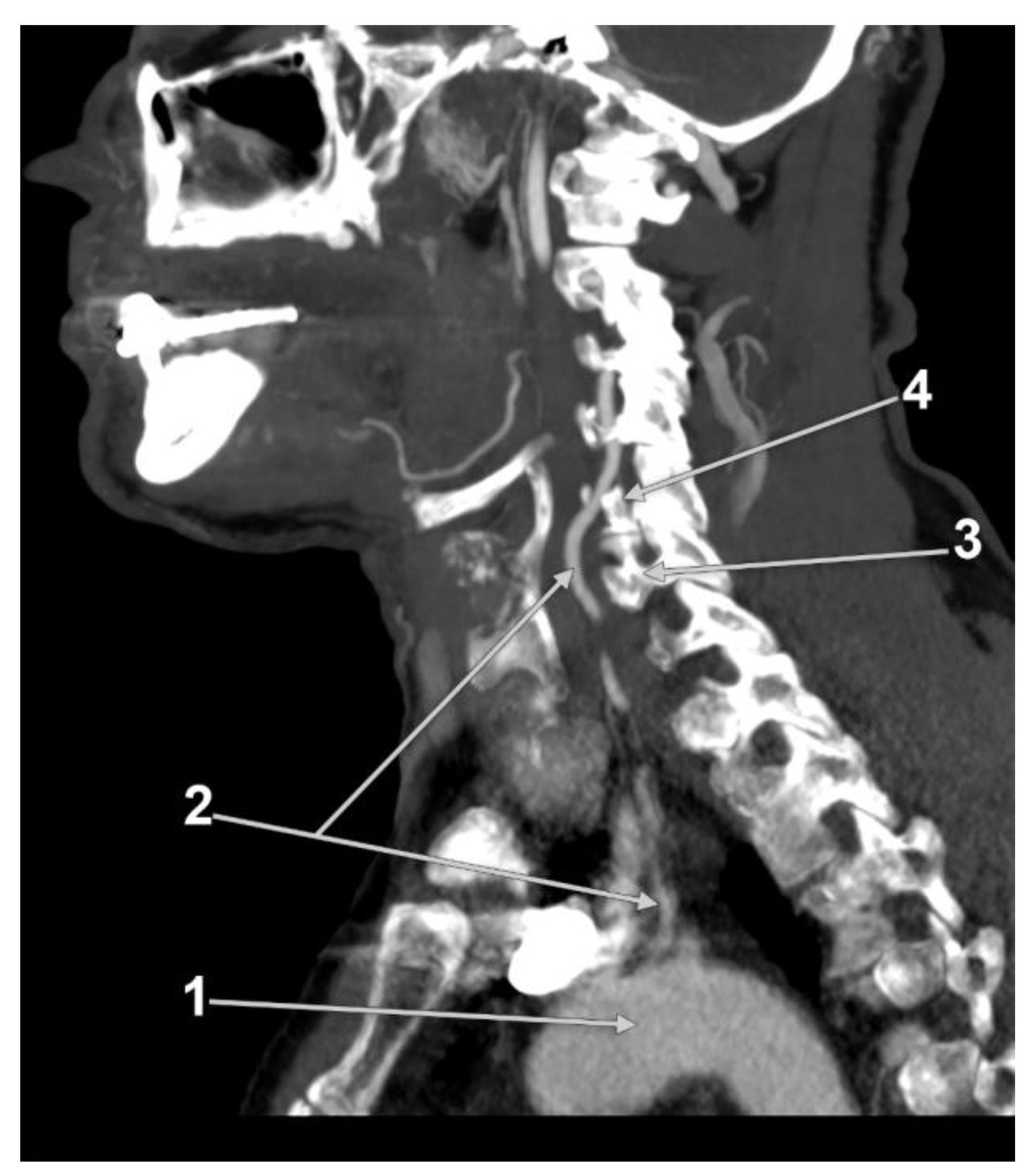
The V2 segment of the VA is commonly situated between C6 and C2. An anomalous entrance is frequently correlated with an abnormal origin [69]; the most prevalent variant is the AA-originated LVA entering the fifth cervical TF in 78.6% (Figure 29) [72], compared to 69.2% stated in the current study. Li et al. [50] confirmed this variant, as the LVA with an anomalous origin entered the TF at C5 and presented a sinuous course. Tardieu et al. [94] also found that AA-originating LVAs were more likely to enter the TF more cranially than C6 and to adopt a more medial course over the cervical vertebral bodies.
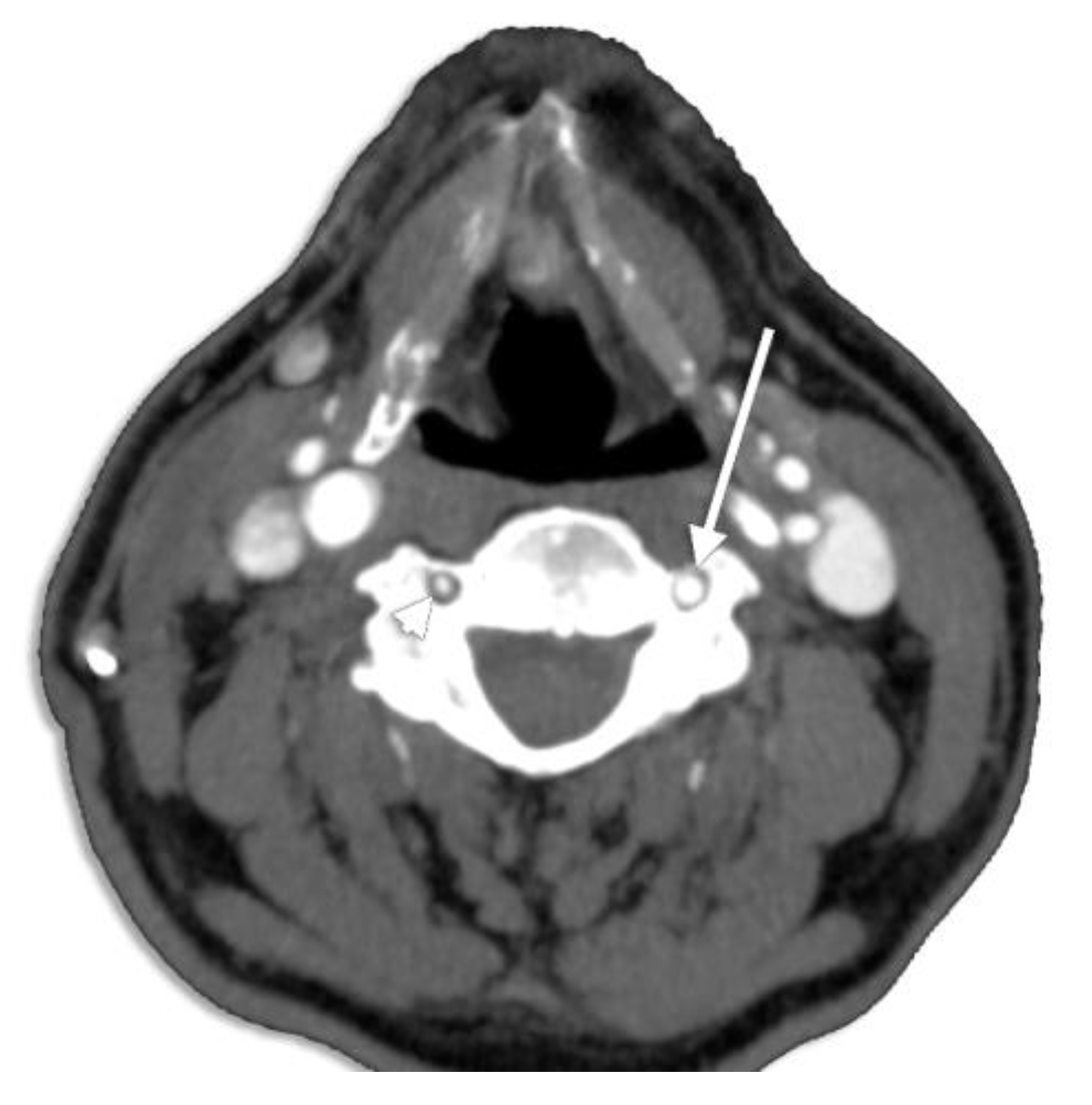
Gantwerker et al. [95] correlated VA’s diameter with the size of the TF; thus, a small TF may presume a hypoplastic or even an aplastic vessel (Figure 30). Hypoplastic VAs have been widely analyzed for their clinical appliance, being a predisposing factor for posterior circulation ischemia [96]. George and Laurian [97] reported a frequency of 5.7% for LVA hypoplasia and 8.8% for hypoplastic RVAs, without mentioning the hypoplastic segment (V1–V4) and including also the atretic arteries.
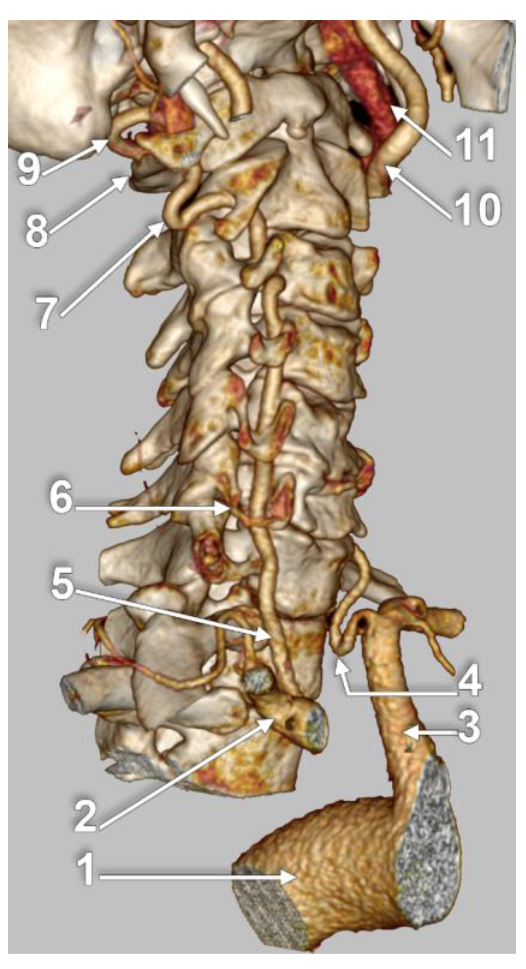
VA loops occur most frequently in the V2 segment (90.5%), followed by V1 (7.6%) and V3 (1.9%) (Figure 31), with the highest occurrence in females, aged between fifty and seventy years old [98].
It worth discussing here that attributing other meanings to generally accepted labels, such as V1, V2, or V3, would lead to misunderstandings and erroneous assumption of the reported data. Kiresi et al. [99] and Cacciola et al. [100] described the anatomical area between C3 and C2 TF as V1, C2 TF to C1 TF as V2, and C1 to dural entry point as V3. Fisher et al. [101] describe the V2 segment as the VA part running between C2–C3 and dura mater. This assignment was also used by Lang et al. [102]. Considering the convention of term usage, V1–V4 labels describe the four segments of the VA, from the SA to the origin of the basilar artery [7,8,103,104,105], as detailed in the Introduction. We strongly advise authors to avoid term reassignments.
4.2. Embryology
During embryogenesis, from the dorsal aspect of the aorta arise seven intersegmental branches, referred to as C1–CUsually, the first part of the VA develops from the dorsal branch of the seventh cervical intersegmental artery. Longitudinal communications of the postcostal anastomoses form the second part of the VA [106,107].
The AA-originating LVA is considered to result from a persisting sixth cervical intersegmental artery, which fails to disappear. The blood flows directly from the AA to the C6 intersegmental artery, creating the AA origin of the LVA [108,109]. Increased resorption of embryonic tissue of the LSA between the AA and LVA origin may also lead to an anomalous origin [110].
It should be pointed out the significance of two persistent arteries, proatlantal and hypoglossal artery, which along with the trigeminal and otic arteries represent the deficient involution of embryonic vascular channels [111]. Hypoplasia of the VA, uni- or bilateral, is correlated with a prevalence of around 50% with the persistence of the proatlantal artery. It usually corresponds to the V3 segment of the VA, originates from the internal or the external carotid artery and enters the skull through the foramen magnum [111,112,113]. Persistence of the hypoglossal artery is related to VA aplasia, with a prevalence of 0.02–0.1%. A persistent hypoglossal artery originates from the internal carotid artery and enters the skull via the hypoglossal canal [113,114]. The entrance in the skull via different foramina also represents a useful criterion in distinguishing the two arteries [115].
4.3. Clinical Relevance
Patients with variation in VA origin are exposed to an increased risk in AA or esophageal surgery, if the case is not previously documented. “Vertebral arteria lusoria” represents a VA originating from the AA, distal to the origin of the left SA, commonly with a retroesophageal course. This anatomical variant has been seldom reported in the literature [83,84,116,117]. Verin et al. reported the case of a lusoria VA entering the fourth cervical vertebra [118], and Meila et al. [52] reported the TF entrance of such a vessel at CThis condition was associated with life-threatening risk during esophageal surgery, as accidental injury to this vessel may lead to hemomediastinum or even neurological impairment [119].
Variation in the entrance into the TF should also be presurgical detailed, as it may expose the patient to risks during anterior neck surgery [51] or dissection during neck rotation [120].
Ignoring the VA anatomical variability could lead to its injury and life-threatening hemorrhage during anterior neck surgery, for instance, thyroidectomy or excision of a pharyngeal diverticulum, as the VA could be damaged while attempting ligation of the inferior thyroid artery [121].
Gluncic et al. [87] stated that atherosclerosis frequently affects the extracranial part of the VA. The origin of the VA is therefore predisposed to subsequent stenosis. Bernard and Dettori [122] presumed that an abnormal VA origin, distribution, or caliber favors cerebral disorders by altering cerebral hemodynamics. The study was conducted on two cases, so their hypothesis may not be generally applicable. Contrarily, Einstein et al. [33] stated that an aberrant LVA may have no vascular consequences, unless being compromised during AA surgery.
Tortuosity and hypoplasia of the VA have a considerable impact on posterior circulation infarctions and atherosclerosis [123,124]. The cause leading to tortuous vessels was speculated by Morris et al. [125] as being a thinner, fragile wall that displays as a meandering vessel. Another etiology proposed by Choi et al. [126] is that the VA adapts as the cervical spine develops a tortuous route due to osteoarthritis. Congenital anomalies of the craniovertebral junction [127] and trauma [128] were also suggested to determine tortuosity. Tortuosity is also linked with vascular vertigo [129] but only if one segment of the VA is affected; if no vascular risk factors exist, symptoms may not appear [130]. A twisted vessel is at higher risk of iatrogenic injuries, as it does not pursue a common course [131]. Thus, a pre-surgical imagistic recognition of the anatomical peculiarities of the VA is fundamental.
4.4. Study Limitations
Although, to our knowledge, this could be regarded as the most extensive meta-analysis study on the VA topic that comprehensively includes numerous anatomical aspects, we should admit that it has several limitations. First, as with any other meta-analysis, the present paper includes a great variety of studies, regardless of the patient’s pathologies, geographic area, number of patients, study types, etc. To minimize this major heterogeneity, we added exclusion criteria, as the removal of papers with patients suffering from vascular disease or studies using less than 10 subjects. Second, considering the Origin and TF Entrance sections, the analyses included all the available studies on the specific anatomic variant. As the total number of evaluated arteries varied, the results are not comparable to each other. Considering the definition of a systematic review or a meta-analysis, we processed the available data in the literature; thus, the assessment of both crude and standardized prevalence was not attainable for each variant analysis. Our results are, thus, highly influenced by the reported results. To diminish any risk of affecting the outcomes of the present study due to biased results published by other authors, we filtered each article rigorously, applying the third exclusion criteria.
4.5. Small-Study Effect
The term “small-study effect” was proposed by Sterne et al. to express the observation that smaller studies typically produce greater effect sizes [132]. According to Yurasakpong et al., the small-study effect, which denotes publication bias, is a frequent issue, particularly in anatomical systematic reviews and meta-analyses [133]. Analyses with high standard errors (SE) and low sample size are more likely to report higher prevalence. Funnel plots of effect size against sample size were used to detect publication bias. The asymmetrical plots may suggest the potential impact of the small-study effect and publication bias on the results of the interested determinations.
5. Conclusions
The anatomy of the VA is extensively variable. The SA origin of the VA has a prevalence of 94.1%. The entrance of the VA at the sixth transverse foramen prevails in 92.0% of cases. Tortuosity (26.6%) and hypoplasia (7.94%) were also documented. Tortuosity in the transverse plane was the most frequent (30.1%), related to sagittal (22.8%) and coronal (16.6%) tortuosity. A straight V1 segment of the VA was prevalent in 45.2% of cases. Considering the VA dominance, LVA was dominant in 36.1% of cases, compared to RVA dominance, found in 25.3% of cases.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/diagnostics13122036/s1, Figure S1: C3_TF_funnel sample size, Figure S2: C3_TF_funnel SE, Figure S3: C4_TF_LEFT_funnel sample size, Figure S4: C4_TF_LEFT_funnel SE, Figure S5: C4_TF_RIGHT_funnel sample size, Figure S6: C4_TF_RIGHT_funnel SE, Figure S7: C4_TF_funnel sample size, Figure S8: C4_TF_funnel SE, Figure S9: C5_TF_LEFT_SA_funnel sample size, Figure S10: C5_TF_LEFT_SA_funnel SE, Figure S11: C5_TF_LEFT_funnel sample size, Figure S12: C5_TF_LEFT_funnel SE, Figure S13: C5_TF_RIGHT_funnel sample size, Figure S14: C5_TF_RIGHT_funnel SE, Figure S15: C5_TF_funnel sample size, Figure S16: C5_TF_funnel SE.
Author Contributions
Conceptualization, R.C.T., M.C.R. and S.H.; methodology, R.C.T. and S.H.; software, S.H.; validation, M.C.R. and S.H.; formal analysis, M.C.R.; investigation, R.C.T.; data collection and analysis, R.C.T. and S.H.; writing—original draft preparation, R.C.T.; writing—review and editing, M.C.R.; supervision, S.H.; project administration, M.C.R.; quality assessment and risk of bias, R.C.T. and S.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| AA | aortic arch |
| BCT | brachiocephalic trunk |
| C3_TF Entrance_LVA_AA | AA-originated LVA entering the TF at C3 |
| C4_TF Entrance_LVA_SA | SA-originated LVA entering the TF at C4 |
| C7_TF Entrance_LVA_AA | AA-originated LVA entering the TF at C7 |
| CI | confidence interval |
| LSA/RSA | left/right SA |
| LVA/RVA | left/right VA |
| LVA_AA | AA-originated LVA |
| LVA_SA | SA-originated LVA |
| RCCA | right common carotid artery |
| RVA_AA | AA-originated RVA |
| RVA_BCT | BCT-originated RVA |
| RVA_RCCA | RCCA-originated RVA |
| RVA_SA | SA_originated RVA |
| SA | subclavian artery |
| TF | transverse foramen |
| VA | vertebral artery |
References
- Tasdemir, R.; Cihan, O.F. Multidetector computed tomography evaluation of origin, V2 segment variations and morphology of vertebral artery. Folia Morphol. 2023, 82, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Zarrinkoob, L.; Ambarki, K.; Wahlin, A.; Birgander, R.; Eklund, A.; Malm, J. Blood flow distribution in cerebral arteries. J. Cereb. Blood Flow Metab. 2015, 35, 648–654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osborn, A.G. Diagnostic Cerebral Angiography, 2nd ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 1999. [Google Scholar]
- Cloud, G.C.; Markus, H.S. Diagnosis and management of vertebral artery stenosis. QJM Int. J. Med. 2003, 96, 27–54. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Cloud, G.C.; Kerry, S.; Markus, H.S. Imaging of vertebral artery stenosis: A systematic review. J. Neurol. Neurosurg. Psychiatry. 2007, 78, 1218–1225. [Google Scholar] [CrossRef] [Green Version]
- Tayebi Meybodi, A.; Borba Moreira, L.; Gandhi, S.; Catapano, J.C.; Preul, M.C.; Lawton, M.T. Exposure of the V1 Segment of the Vertebral Artery: Stepwise Cadaveric Surgical Simulation. Oper. Neurosurg. 2020, 19, E32–E38. [Google Scholar] [CrossRef] [PubMed]
- Bruneau, M.; Cornelius, J.F.; George, B. Anterolateral approach to the V1 segment of the vertebral artery. Neurosurgery 2006, 58, ONS-215-9, discussion ONS-9. [Google Scholar] [CrossRef]
- Bruneau, M.; Cornelius, J.F.; Marneffe, V.; Triffaux, M.; George, B. Anatomical variations of the V2 segment of the vertebral artery. Neurosurgery 2006, 59, ONS20-4, discussion ONS-4. [Google Scholar] [CrossRef]
- Ciołkowski, M.K.; Ciszek, B. Course variability of the atlantic (V3) segment of vertebral artery: Anatomical study with clinical implications. Folia Morphol. 2021, 80, 20–25. [Google Scholar] [CrossRef] [Green Version]
- Magklara, E.P.; Pantelia, E.T.; Solia, E.; Panagouli, E.; Piagkou, M.; Mazarakis, A.; Skandalakis, P.; Troupis, T.; Filippou, D. Vertebral artery variations revised: Origin, course, branches and embryonic development. Folia Morphol 2021, 80, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Abd el-Bary, T.H.; Dujovny, M.; Ausman, J.I. Microsurgical anatomy of the atlantal part of the vertebral artery. Surg. Neurol. 1995, 44, 392–400. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 372, n71. [Google Scholar]
- Morris, S.A. Arterial tortuosity in genetic arteriopathies. Curr. Opin. Cardiol. 2015, 30, 587–593. [Google Scholar] [CrossRef] [Green Version]
- Spinardi, L.; Vornetti, G.; De Martino, S.; Golfieri, R.; Faccioli, L.; Pastore Trossello, M.; Graziano, C.; Mariucci, E.; Donti, A. Intracranial Arterial Tortuosity in Marfan Syndrome and Loeys-Dietz Syndrome: Tortuosity Index Evaluation Is Useful in the Differential Diagnosis. AJNR Am. J. Neuroradiol. 2020, 41, 1916–1922. [Google Scholar] [CrossRef]
- Tschabitscher, M.; Fuss, F.K.; Matula, C.; Klimpel, S. Course of the arteria vertebralis in its segment V1 from the origin to its entry into the foramen processus transversi. Acta Anat. 1991, 140, 373–377. [Google Scholar] [CrossRef] [PubMed]
- Deeks, J.J.; Higgins, J.P.; Altman, D.G. Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Re-views of Interventions; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 2019; pp. 241–284. [Google Scholar]
- Trattnig, S.; Matula, C.; Karnel, F.; Daha, K.; Tschabitscher, M.; Schwaighofer, B. Difficulties in examination of the origin of the vertebral artery by duplex and colour-coded Doppler sonography: Anatomical considerations. Neuroradiology 1993, 35, 296–299. [Google Scholar] [CrossRef] [PubMed]
- Vaiman, M.; Beckerman, I. Importance of preoperative detection of vertebral artery anomalies in neck surgery. ANZ J. Surg. 2011, 81, 164–167. [Google Scholar] [CrossRef] [PubMed]
- Adachi, B. Das Arteriensystem der Japaner; In KenkyuSha; Universität zu Kyoto: Kyoto, Japan, 1928. [Google Scholar]
- Alicioglu, B.; Gulekon, N.; Akpinar, S. Age-related morphologic changes of the vertebral artery in the transverse process. Analysis by multidetector computed tomography angiography. Spine J. 2015, 15, 1981–1987. [Google Scholar] [CrossRef]
- Yazıcı, A.; İnanç, Y. Evaluation of BPPV with vertebral artery values. Neuropsychiatry Dis. Treat. 2018, 14, 1975–1979. [Google Scholar] [CrossRef] [Green Version]
- Gitkind, A.I.; Olson, T.R.; Downie, S.A. Vertebral Artery Anatomical Variations as They Relate to Cervical Transforaminal Epidural Steroid Injections. Pain Med. 2014, 15, 1109–1114. [Google Scholar] [CrossRef]
- Bean, R.B. A composite study of the subclavian artery in man. Am J Anat. 1905, 4, 303–328. [Google Scholar] [CrossRef]
- Bergman, R.A.; Afifi, A.K.; Miyauchi, R. Vertebral Arteries—Illustrated Encyclopedia of Human Anatomic Variation: Opus II: Cardiovascular System: Arteries: Head, Neck and Thorax. 2012. Available online: https://www.anatomyatlases.org/AnatomicVariants/Cardiovascular/Text/Arteries/Vertebral.shtml (accessed on 1 December 2022).
- Berko, N.S.; Jain, V.R.; Godelman, A.; Stein, E.G.; Ghosh, S.; Haramati, L.B. Variants and anomalies of thoracic vasculature on computed tomographic angiography in adults. J. Comput. Assist. Tomogr. 2009, 33, 523–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhatia, K.; Ghabriel, M.N.; Henneberg, M. Anatomical variations in the branches of the human aortic arch: A recent study of a South Australian population. Folia Morphol. 2005, 64, 217–223. [Google Scholar]
- Budhiraja, V.; Rastogi, R.; Jain, V.; Bankwar, V.; Raghuwanshi, S. Anatomical variations in the branching pattern of human aortic arch: A cadaveric study from central India. ISRN Anat. 2013, 2013, 828969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taitz, C.; Arensburg, B. Vertebral artery tortuosity with concomitant erosion of the foramen of the transverse process of the axis. Possible clinical implications. Acta Anat. 1991, 141, 104–108. [Google Scholar] [CrossRef]
- Cavdar, S.; Dalçik, H.; Ercan, F.; Arbak, S.; Arifoğlu, Y. A morphological study on the V2 segment of the vertebral artery. Okajimas Folia Anat. Jpn. 1996, 73, 133–137. [Google Scholar]
- Chanapa, P.; Mahakkanukrauh, P. Anatomical variations of the V2 vertebral artery study by measuring the width of transverse foramen. J. Med. Assoc. Thai 2012, 95, 569–573. [Google Scholar]
- Lin, C.; Liu, Y.; Chen, Y.; Shih, Y.; Chang, C.; Chuang, M. Variations in the Origin and Course of the Extracranial Vertebral Artery on Multidetector Computed Tomography Angiography. Iran J. Radiol. 2018, 15, e61623. [Google Scholar] [CrossRef]
- Dodevski, A.; Lazareska, M.; Tosovska-Lazarova, D.; Zhivadinovik, J.; Aliji, V. Morphological characteristics of the first part of the vertebral artery. Prilozi 2011, 32, 173–188. [Google Scholar]
- Einstein, E.H.; Song, L.H.; Villela, N.L.; Fasani-Feldberg, G.B.; Jacobs, J.L.; Kim, D.O.; Nathawat, A.; Patel, D.; Bender, R.B.; Peters, D.F.J.A. Anomalous origin of the left vertebral artery from the aortic arch. Aorta 2016, 4, 64–67. [Google Scholar] [CrossRef] [Green Version]
- Civelek, E.; Kiris, T.; Hepgul, K.; Canbolat, A.; Ersoy, G.; Cansever, T. Anterolateral approach to the cervical spine: Major anatomical structures and landmarks: Technical note. J. Neurosurg. Spine 2007, 7, 669–678. [Google Scholar] [CrossRef]
- Ergun, O.; Gunes Tatar, I.; Birgi, E.; Hekimoglu, B. Evaluation of vertebral artery dominance, hypoplasia and variations in the origin: Angiographic study in 254 patients. Folia Morphol. 2016, 75, 33–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eskander, M.S.; Drew, J.M.; Aubin, M.E.; Marvin, J.; Franklin, P.D.; Eck, J.C.; Patel, N.; Boyle, K.; Connolly, P.J.J.S. Vertebral artery anatomy: A review of two hundred fifty magnetic resonance imaging scans. Spine 2010, 35, 2035–2040. [Google Scholar] [CrossRef] [PubMed]
- Abd El Gawad, F.A.; Shaaban, M.H.; Shuaib, D.M.; Shallan, H.M. Anatomical variations of the vertebral artery and its relation to the atlas vertebra-radiological and dry bone study. Eur. J. Anat. 2019, 23, 49–58. [Google Scholar]
- Gaigalaite, V.; Vilimas, A.; Ozeraitiene, V.; Dementaviciene, J.; Janilionis, R.; Kalibatiene, D.; Rocka, S. Association between vertebral artery hypoplasia and posterior circulation stroke. BMC Neurol. 2016, 16, 118. [Google Scholar] [CrossRef] [Green Version]
- Güvençer, M.; Men, S.; Naderi, S.; Kiray, A.; Tetik, S. The V2 segment of the vertebral artery in anterior and anterolateral cervical spinal surgery: A cadaver angiographic study. Clin. Neurol. Neurosurg. 2006, 108, 440–445. [Google Scholar] [CrossRef]
- Tetiker, H.; Çimen, M.; Kosar, M.I. Evaluation of the Vertebral Artery by 3D Digital Subtraction Angiography. Int. J. Morphol. 2014, 32, 798–802. [Google Scholar] [CrossRef]
- Hauke, P. Schlingenbildung der Arteria carotis und Arteria vertebralis. Angiogr. Klin Befunde 1973, 98, 2381–2384. [Google Scholar] [CrossRef]
- Heary, R.F.; Albert, T.J.; Ludwig, S.C.; Vaccaro, A.R.; Wolansky, L.J.; Leddy, T.P.; Schmidt, R.R. Surgical anatomy of the vertebral arteries. Spine 1996, 21, 2074–2080. [Google Scholar] [CrossRef]
- Hong, J.T.; Park, D.K.; Lee, M.J.; Kim, S.W.; An, H.S. Anatomical Variations of the Vertebral Artery Segment in the Lower Cervical Spine: Analysis by Three-Dimensional Computed Tomography Angiography. Spine 2008, 33, 2422–2426. [Google Scholar] [CrossRef]
- Ikegami, A.; Ohtani, Y.; Ohtani, O. Bilateral variations of the vertebral arteries: The left originating from the aortic arch and the left and right entering the C5 transverse foramina. Anat. Sci. Int. 2007, 82, 175–179. [Google Scholar] [CrossRef]
- Jakanani, G.C.; Adair, W. Frequency of variations in aortic arch anatomy depicted on multidetector CT. Clin. Radiol. 2010, 65, 481–487. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.P.; Scraggs, M.; How, T.; Burns, J. A necropsy and histomorphometric study of abnormalities in the course of the vertebral artery associated with ossified stylohyoid ligaments. J. Clin. Pathol. 1995, 48, 637–640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kajimoto, B.H.J.; Addeo, R.L.D.; Campos, G.C.d.; Narazaki, D.K.; Correia, L.d.S.; Araújo, M.P.d.; Cristante, A.F.; Iutaka, A.S.; Marcon, R.M.; Oliveira, R.P.; et al. Estudo anatômico do trajeto da artéria vertebral na coluna cervical inferior humana. Acta Ortopédica Bras. 2007, 15, 84–86. [Google Scholar] [CrossRef] [Green Version]
- Kim, C.; Sohn, J.H.; Choi, H.C. Are the anomalous vertebral arteries more hypoplastic?: Retrospective linear mixed model approach. BMC Neurol. 2017, 17, 168. [Google Scholar] [CrossRef] [Green Version]
- Komiyama, M.; Morikawa, T.; Nakajima, H.; Nishikawa, M.; Yasui, T. High Incidence of Arterial Dissection Associated With Left Vertebral Artery of Aortic Origin. Neurol. Med. Chir. 2001, 41, 8–12. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Guan, L.; Zilundu, P.L.M.; Chen, J.; Chen, Z.; Ma, M.; Zhuang, H.; Zhuang, Z.; Qiu, Y.; Ye, F.; et al. The applied anatomy and clinical significance of the proximal, V1 segment of vertebral artery. Folia Morphol. 2019, 78, 710–719. [Google Scholar] [CrossRef] [Green Version]
- Matula, C.; Trattnig, S.; Tschabitscher, M.; Day, J.D.; Koos, W.T. The course of the prevertebral segment of the vertebral artery: Anatomy and clinical significance. Surg. Neurol. 1997, 48, 131. [Google Scholar] [CrossRef]
- Meila, D.; Tysiac, M.; Petersen, M.; Theisen, O.; Wetter, A.; Mangold, A.; Schlunz-Hendann, M.; Papke, K.; Brassel, F.; Berenstein, A.J.C.N. Origin and course of the extracranial vertebral artery: CTA findings and embryologic considerations. Clin. Neuroradiol. 2012, 22, 327–333. [Google Scholar] [CrossRef]
- Müller, M.; Schmitz, B.L.; Pauls, S.; Schick, M.; Röhrer, S.; Kapapa, T.; Schlötzer, W. Variations of the aortic arch—A study on the most common branching patterns. Acta Radiol. 2011, 52, 738–742. [Google Scholar] [CrossRef]
- O’Malley, A.M.; El Kininy, W.H.; Debebe, H.; Burukan, A.B.; Davy, S.W. A cadaveric study of aortic arch variation in an Irish population. Ir. J. Med. Sci. 2018, 187, 853–858. [Google Scholar] [CrossRef]
- Omotoso, B.R.; Harrichandparsad, R.; Moodley, I.G.; Satyapal, K.S.; Lazarus, L. An anatomical investigation of the proximal vertebral arteries (V1, V2) in a select South African population. Surg. Radiol. Anat. 2021, 43, 929–941. [Google Scholar] [CrossRef]
- Palmer, F.J.; Sequiera, M. Cervical Vertebral Erosion & Vertebral Artery Tortuosity: An Angiographic Study. Australas Radiol. 1980, 24, 20–23. [Google Scholar]
- Patil, S.T.; Meshram, M.M.; Kamdi, N.Y.; Kasote, A.P.; Parchand, M.P. Study on branching pattern of aortic arch in Indian. Anat. Cell Biol. 2012, 45, 203–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ranganatha Sastry, V.; Manjunath, K.Y. The course of the V1 segment of the vertebral artery. Ann. Indian Acad. Neurol. 2006, 9, 223–226. [Google Scholar]
- Raveendranath, V.; Shankar, N. Anatomical variations of the pre-transverse segment of the vertebral artery in Indian cadavers. Eur. J. Anat. 2014, 18, 159–163. [Google Scholar]
- Russo, V.M.; Graziano, F.; Peris-Celda, M.; Russo, A.; Ulm, A.J. The V(2) segment of the vertebral artery: Anatomical considerations and surgical implications. J. Neurosurg. Spine 2011, 15, 610–619. [Google Scholar] [CrossRef]
- Vujmilović, S.; Spasojević, G.; Vujnović, S.; Malobabić, S.; Vujković, Z. Variability of the vertebral artery origin and transverse foramen entrance level—CT angiographic study. Folia Morphol. 2018, 77, 687–692. [Google Scholar] [CrossRef] [Green Version]
- Schmitt, P.J.; Altafulla, J.J.; Kikuta, S.; Dupont, G.; Iwanaga, J.; Monteith, S.; Litvack, Z.; Dumont, A.S.; Tubbs, R.S. Internal Thoracic Artery to Vertebral Artery Bypass Surgery: A Cadaveric Feasibility Study. World Neurosurg. 2019, 130, e722–e725. [Google Scholar] [CrossRef]
- Shin, H.Y.; Park, J.K.; Park, S.K.; Jung, G.S.; Choi, Y.S. Variations in Entrance of Vertebral Artery in Korean Cervical Spine: MDCT-based Analysis. Korean J. Pain 2014, 27, 266–270. [Google Scholar] [CrossRef]
- Shin, I.Y.; Chung, Y.G.; Shin, W.H.; Im, S.B.; Hwang, S.C.; Kim, B.T. A morphometric study on cadaveric aortic arch and its major branches in 25 korean adults: The perspective of endovascular surgery. J. Korean Neurosurg. Soc. 2008, 44, 78–83. [Google Scholar] [CrossRef]
- Thierfelder, K.M.; Baumann, A.B.; Sommer, W.H.; Armbruster, M.; Opherk, C.; Janssen, H.; Reiser, M.F.; Straube, A.; von Baumgarten, L.J.S. Vertebral artery hypoplasia: Frequency and effect on cerebellar blood flow characteristics. Stroke 2014, 45, 1363–1368. [Google Scholar] [CrossRef] [PubMed]
- Touboul, P.; Bousser, M.; LaPlane, D.; Castaigne, P.J.S. Duplex scanning of normal vertebral arteries. Stroke 1986, 17, 921–923. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takafuji, T.; Sato, Y. Study on the subclavian artery and its branches in Japanese adults. Okajimas Folia Anat. Jpn. 1991, 68, 171–185. [Google Scholar] [CrossRef] [Green Version]
- Tubbs, R.S.; Shah, N.A.; Sullivan, B.P.; Marchase, N.D.; Cohen-Gadol, A.A. Surgical anatomy and quantitation of the branches of the V2 and V3 segments of the vertebral artery. Laboratory investigation. J. Neurosurg. Spine 2009, 11, 84–87. [Google Scholar] [CrossRef]
- Uchino, A.; Saito, N.; Takahashi, M.; Okada, Y.; Kozawa, E.; Nishi, N.; Mizukoshi, W.; Nakajima, R.; Watanabe, Y. Variations in the origin of the vertebral artery and its level of entry into the transverse foramen diagnosed by CT angiography. Neuroradiology 2013, 55, 585–594. [Google Scholar] [CrossRef]
- Vorster, W.; du Plooy, P.T.; Meiring, J.H. Abnormal origin of internal thoracic and vertebral arteries. Clin. Anat. 1998, 11, 33–37. [Google Scholar] [CrossRef]
- Wang, L.; Zhang, J.; Xin, S. Morphologic features of the aortic arch and its branches in the adult Chinese population. J. Vasc. Surg. 2016, 64, 1602–1608. [Google Scholar] [CrossRef] [Green Version]
- Woraputtaporn, W.; Ananteerakul, T.; Iamsaard, S.; Namking, M. Incidence of vertebral artery of aortic arch origin, its level of entry into transverse foramen, length, diameter and clinical significance. Anat. Sci. Int. 2019, 94, 275–279. [Google Scholar] [CrossRef]
- Yamaki, K.i.; Saga, T.; Hirata, T.; Sakaino, M.; Nohno, M.; Kobayashi, S.; Hirao, T. Anatomical study of the vertebral artery in Japanese adults. Anat. Sci. Int. 2006, 81, 100–106. [Google Scholar] [CrossRef]
- Chen, Y.Y.; Chao, A.C.; Hsu, H.Y.; Chung, C.P.; Hu, H.H. Vertebral artery hypoplasia is associated with a decrease in net vertebral flow volume. Ultrasound Med. Biol. 2010, 36, 38–43. [Google Scholar] [CrossRef]
- Yi, X.; Xie, P.; Zhang, L.; Lu, F.; Chen, H.; Liu, K. Entrance and origin of the extracranial vertebral artery found on computed tomography angiography. Sci. Rep. 2022, 12, 15274. [Google Scholar] [CrossRef] [PubMed]
- Gray, H.; Standring, S.; Anand, N.; Birch, R.; Collins, P.; Crossman, A.; Gleeson, M.; Jawaheer, G.; Smith, A.L.; Spratt, J.D.; et al. Gray’s Anatomy: The Anatomical Basis of Clinical Practice, 41st ed.; Elsevier: Amsterdam, The Netherlands, 2016. [Google Scholar]
- Rouviere, H.; Delmas, A. Anatomie Humaine; Tête et cou; Masson: Paris, France, 1985. [Google Scholar]
- Morris, P. Practical Neuroangiography; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2007. [Google Scholar]
- Peng, C.W.; Chou, B.T.; Bendo, J.A.; Spivak, J.M. Vertebral artery injury in cervical spine surgery: Anatomical considerations, management, and preventive measures. Spine J. 2009, 9, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Biffl, W.L.; Moore, E.E.; Elliott, J.P.; Ray, C.; Offner, P.J.; Franciose, R.J.; Brega, K.E.; Burch, J.M. The Devastating Potential of Blunt Vertebral Arterial Injuries. Ann. Surg. 2000, 231, 672–681. [Google Scholar] [CrossRef] [PubMed]
- Mahmodlou, R.; Sepehrvand, N.; Hatami, S. Aberrant Right Subclavian Artery: A Life-threatening Anomaly that should be considered during Esophagectomy. J. Surg. Tech. Case Rep. 2014, 6, 61–63. [Google Scholar] [PubMed] [Green Version]
- Yuan, S.M. Aberrant Origin of Vertebral Artery and its Clinical Implications. Braz. J. Cardiovasc. Surg. 2016, 31, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Lemke, A.-J.; Benndorf, G.; Liebig, T.; Felix, R. Anomalous origin of the right vertebral artery: Review of the literature and case report of right vertebral artery origin distal to the left subclavian artery. Am. J. Neuroradiol. 1999, 20, 1318–1321. [Google Scholar] [PubMed]
- Goray, V.B.; Joshi, A.R.; Garg, A.; Merchant, S.; Yadav, B.; Maheshwari, P. Aortic arch variation: A unique case with anomalous origin of both vertebral arteries as additional branches of the aortic arch distal to left subclavian artery. AJNR Am. J. Neuroradiol. 2005, 26, 93–95. [Google Scholar]
- Al-Okaili, R.; Schwartz, E.D. Bilateral aortic origins of the vertebral arteries with right vertebral artery arising distal to left subclavian artery: Case report. Surg. Neurol. 2007, 67, 174–176, discussion 6. [Google Scholar] [CrossRef]
- Schwarzacher, S.W.; Krammer, E.B. Complex anomalies of the human aortic arch system: Unique case with both vertebral arteries as additional branches of the aortic arch. Anat. Rec. 1989, 225, 246–250. [Google Scholar] [CrossRef]
- Gluncic, V.; Ivkic, G.; Marin, D.; Percac, S. Anomalous origin of both vertebral arteries. Clin. Anat. 1999, 12, 281–284. [Google Scholar] [CrossRef]
- Nasir, S.; Hussain, M.; Khan, S.A.; Mansoor, M.A.; Sharif, S. Anomalous origin of right vertebral artery from right external carotid artery. J. Coll. Physicians Surg. Pak. 2010, 20, 208–210. [Google Scholar] [PubMed]
- Ali, A.; Sedora Roman, N.I.; Cox, M.; Kung, D.; Choudhri, O.; Hurst, R.W.; Pukenas, B.A. Anomalous Origin of the Right Vertebral Artery from the Right Common Carotid Artery. Cureus 2018, 10, e3602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergman, R.A.; Tubbs, R.S.; Shoja, M.M.; Loukas, M. Bergman’s Comprehensive Encyclopedia of Human Anatomic Variation; John Wiley & Sons: Hoboken, NJ, USA, 2016. [Google Scholar]
- Lasjaunias, P.; Theron, J.; Moret, J. The occipital artery. Anatomy–Normal arteriographic aspects–Embryological significance. Neuroradiology 1978, 15, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Uchino, A.; Tokushige, K. Type 2 left proatlantal artery with normal left vertebral artery and association with an aberrant right subclavian artery and a bi-carotid trunk. Surg. Radiol. Anat. 2022, 44, 419–421. [Google Scholar] [CrossRef]
- Cohen, J.E.; Grigoriadis, S.; Itshayek, E. Type II proatlantal artery (occipital subtype) with bilateral absence of the vertebral arteries. Clin. Anat. 2011, 24, 950–952. [Google Scholar] [CrossRef] [PubMed]
- Tardieu, G.G.; Edwards, B.; Alonso, F.; Watanabe, K.; Saga, T.; Nakamura, M.; Motomura, M.; Sampath, R.; Iwanaga, J.; Goren, O.; et al. Aortic arch origin of the left vertebral artery: An Anatomical and Radiological Study with Significance for Avoiding Complications with Anterior Approaches to the Cervical Spine. Clin. Anat. 2017, 30, 811–816. [Google Scholar] [CrossRef]
- Gantwerker, B.R.; Baaj, A.A.; Maughan, P.H.; McDougall, C.G.; White, W.L. Vertebral artery injury during cervical discectomy and fusion in a patient with bilateral anomalous arteries in the disc space: Case report. Neurosurgery 2010, 67, E874–E875, discussion E5. [Google Scholar] [CrossRef]
- Katsanos, A.H.; Kosmidou, M.; Kyritsis, A.P.; Giannopoulos, S. Is vertebral artery hypoplasia a predisposing factor for posterior circulation cerebral ischemic events? A comprehensive review. Eur Neurol. 2013, 70, 78–83. [Google Scholar] [CrossRef]
- George, B.; Laurian, C. The Vertebral Artery: Pathology and Surgery; Springer: Vienna, Austria, 1987. [Google Scholar]
- Ekşi, M.; Toktaş, Z.O.; Yılmaz, B.; Demir, M.K.; Özcan-Ekşi, E.E.; Bayoumi, A.B.; Yener, Y.; Akakın, A.; Konya, D. Vertebral artery loops in surgical perspective. Eur. Spine J. 2016, 25, 4171–4180. [Google Scholar] [CrossRef]
- Kiresi, D.; Gumus, S.; Cengiz, S.L.; Cicekcibasi, A. The morphometric analysis of the V2 and V3 segments of the vertebral artery: Normal values on MDCT. Comput. Med. Imaging Graph. 2009, 33, 399–407. [Google Scholar] [CrossRef]
- Cacciola, F.; Phalke, U.; Goel, A. Vertebral artery in relationship to C1-C2 vertebrae: An anatomical study. Neurol. India 2004, 52, 178–184. [Google Scholar]
- Fisher, C.M. The pathology and pathogenesis of intracerebral hemorrhage. In Pathogenesis and Treatment of Cerebral Vascular Disease; Fields, W.S., Ed.; Charles C. Thomas Publisher: Sprinfield, IL, USA, 1961; pp. 295–342. [Google Scholar]
- Lang, J.; Kessler, B. About the Suboccipital Part of the Vertebral Artery and the Neighboring Bone-Joint and Nerve Relationships. Skull Base. 1991, 1, 64–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Argenson, C. The vertebral arteries (segments V1 and V2). Anat. Clin. 1980, 2, 29–41. [Google Scholar] [CrossRef]
- Francke, J.; Di Marino, V.; Pannier, M.; Argenson, C.; Libersa, C. The vertebral arteries (arteria vertebralis). The V3 atlanto-axial and V4 intracranial segments-collaterals. Anat. Clin. 1981, 2, 229–242. [Google Scholar] [CrossRef]
- George, B. Exposure of the upper cervical vertebral artery. In Surgery of the Craniovertebral Junction; Springer: Berlin/Heidelberg, Germany, 1998; pp. 545–567. [Google Scholar]
- Panicker, H.; Tarnekar, A.; Dhawane, V.; Ghosh, S. Anomalous origin of left vertebral artery-embryological basis and applied aspects-a case report. J Anat Soc India. 2002, 51, 234–235. [Google Scholar]
- Satti, S.R.; Cerniglia, C.A.; Koenigsberg, R.A. Cervical vertebral artery variations: An anatomic study. AJNR Am. J. Neuroradiol. 2007, 28, 976–980. [Google Scholar]
- Jung, S.; Jung, C.; Bae, Y.J.; Choi, B.S.; Kim, J.H. Duplicated Origin of the Left Vertebral Artery: A Case Report and Embryological Review. Neurointervention 2016, 11, 50–54. [Google Scholar] [CrossRef] [Green Version]
- Bordes, S.J.; Iwanaga, J.; Zarrintan, S.; Watanabe, K.; Tubbs, R.S. Accessory Vertebral Artery: An Embryological Review with Translation from Adachi. Cureus 2021, 13, e13448. [Google Scholar] [CrossRef]
- Suresh, R.; Ovchinnikov, N.; McRae, A. Variations in the branching pattern of the aortic arch in three Trinidadians. West Indian Med. J. 2006, 55, 351–353. [Google Scholar] [CrossRef]
- Gumus, T.; Onal, B.; Ilgit, E.T. Bilateral persistence of type 1 proatlantal arteries: Report of a case and review of the literature. AJNR Am. J. Neuroradiol. 2004, 25, 1622–1624. [Google Scholar]
- Anderson, R.A.; Sondheimer, F.K. Rare carotid-vertebrobasilar anastomoses with notes on the differentiation between proatlantal and hypoglossal arteries. Neuroradiology 1976, 11, 113–118. [Google Scholar] [CrossRef]
- Menshawi, K.; Mohr, J.P.; Gutierrez, J. A Functional Perspective on the Embryology and Anatomy of the Cerebral Blood Supply. J. Stroke 2015, 17, 144–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oelerich, M.; Schuierer, G. Primitive hypoglossal artery: Demonstration with digital subtraction-, MR- and CT angiography. Eur. Radiol. 1997, 7, 1492–1494. [Google Scholar] [CrossRef] [PubMed]
- Hutchinson, N.A.; Miller, J.D. Persistent proatlantal artery. J. Neurol. Neurosurg. Psychiatry 1970, 33, 524–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canyigit, M.; Akgoz, A.; Koksal, A.; Yucesoy, C. Aberrant right vertebral artery: A rare aortic arch anomaly. Br. J. Radiol. 2009, 82, 789–791. [Google Scholar] [CrossRef]
- Hsu, D.P.; Alexander, A.D.; Gilkeson, R.C. Anomalous vertebral artery origins: The first and second reports of two variants. J. Neurointerv. Surg. 2010, 2, 160–162. [Google Scholar] [CrossRef]
- Verin, A.L.; Creuze, N.; Musset, D. Multidetector CT scan findings of a right aberrant retroesophageal vertebral artery with an anomalous origin from a cervical aortic arch. Chest 2010, 138, 418–422. [Google Scholar] [CrossRef]
- Lacout, A.; Khalil, A.; Figl, A.; Liloku, R.; Marcy, P.Y. Vertebral arteria lusoria: A life-threatening condition for oesophageal surgery. Surg. Radiol. Anat. 2012, 34, 381–383. [Google Scholar] [CrossRef]
- Jackson, R.S.; Wheeler, A.H.; Darden, B.V. Vertebral artery anomaly with atraumatic dissection causing thromboembolic ischemia: A case report. Spine 2000, 25, 1989–1992. [Google Scholar] [CrossRef]
- Daseler, E.H.; Anson, B.J. Surgical anatomy of the subclavian artery and its branches. Surg. Gynecol. Obstet. 1959, 108, 149–174. [Google Scholar]
- Bernardi, L.; Dettori, P. Angiographic study of a rare anomalous origin of the vertebral artery. Neuroradiology 1975, 9, 43–47. [Google Scholar] [CrossRef]
- Gutierrez, J.; Sacco, R.L.; Wright, C.B. Dolichoectasia-an evolving arterial disease. Nat. Rev. Neurol. 2011, 7, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Kim, J.M.; Roh, J.K. Hypoplastic vertebral artery: Frequency and associations with ischaemic stroke territory. J. Neurol. Neurosurg. Psychiatry 2007, 78, 954–958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, S.A.; Orbach, D.B.; Geva, T.; Singh, M.N.; Gauvreau, K.; Lacro, R.V. Increased vertebral artery tortuosity index is associated with adverse outcomes in children and young adults with connective tissue disorders. Circulation 2011, 124, 388–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, J.W.; Lee, J.K.; Moon, K.S.; Kim, Y.S.; Kwak, H.J.; Joo, S.P.; Kim, J.H.; Kim, S.H. Endovascular embolization of iatrogenic vertebral artery injury during anterior cervical spine surgery: Report of two cases and review of the literature. Spine 2006, 31, E891–E894. [Google Scholar] [CrossRef] [PubMed]
- Sivaraju, L.; Mani, S.; Prabhu, K.; Daniel, R.T.; Chacko, A.G. Three-dimensional computed tomography angiographic study of the vertebral artery in patients with congenital craniovertebral junction anomalies. Eur. Spine J. 2017, 26, 1028–1038. [Google Scholar] [CrossRef]
- Lindsey, R.W.; Piepmeier, J.; Burkus, J.K. Tortuosity of the vertebral artery: An adventitious finding after cervical trauma—A case report. J. Bone Joint Surg. Am. 1985, 67, 806–808. [Google Scholar] [CrossRef]
- Zhang, D.P.; Zhang, S.L.; Zhang, H.T.; Zhang, S.J. Vertebral artery dominance, brainstem auditory evoked potential, and vertigo of vascular origin. Neurol. Res. 2012, 34, 498–503. [Google Scholar] [CrossRef]
- Hong-tao, Z.; Shu-ling, Z.; Dao-pei, Z. Two case reports of bilateral vertebral artery tortuosity and spiral twisting in vascular vertigo. BMC Neurol. 2014, 14, 14. [Google Scholar] [CrossRef] [Green Version]
- Oga, M.; Yuge, I.; Terada, K.; Shimizu, A.; Sugioka, Y. Tortuosity of the vertebral artery in patients with cervical spondylotic myelopathy. Risk factor for the vertebral artery injury during anterior cervical decompression. Spine 1996, 21, 1085–1089. [Google Scholar] [CrossRef]
- Sterne, J.A.; Gavaghan, D.; Egger, M. Publication and related bias in meta-analysis: Power of statistical tests and prevalence in the literature. J. Clin. Epidemiol. 2000, 53, 1119–1129. [Google Scholar] [CrossRef] [PubMed]
- Yurasakpong, L.; Yammine, K.; Limpanuparb, T.; Janta, S.; Chaiyamoon, A.; Kruepunga, N.; Meemon, K.; Suwannakhan, A. The prevalence of the azygos lobe: A meta-analysis of 1,033,083 subjects. Clin. Anat. 2021, 34, 872–883. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Dissection of the V1 segment of the right vertebral artery in the scalenovertebral triangle. Major veins, the right clavicle, the first rib and, partly, the manubrium, were removed: 1. anterior scalene muscle; 2. phrenic nerve; 3. vagus nerve; 4. transverse cervical artery; 5. brachial plexus; 6. suprascapular artery; 7. subclavian artery; 8. right brachiocephalic vein; 9. common carotid artery; 10. inferior thyroid artery; 11. V1 segment of vertebral artery; 12. brachiocephalic trunk.
Figure 1.
Dissection of the V1 segment of the right vertebral artery in the scalenovertebral triangle. Major veins, the right clavicle, the first rib and, partly, the manubrium, were removed: 1. anterior scalene muscle; 2. phrenic nerve; 3. vagus nerve; 4. transverse cervical artery; 5. brachial plexus; 6. suprascapular artery; 7. subclavian artery; 8. right brachiocephalic vein; 9. common carotid artery; 10. inferior thyroid artery; 11. V1 segment of vertebral artery; 12. brachiocephalic trunk.

Figure 2.
PRISMA flow diagram, adapted after [12].
Figure 2.
PRISMA flow diagram, adapted after [12].

Figure 3.
Forest plot—LVA originating from the SA.

Figure 4.
Forest plot—LVA originating from the AA.

Figure 5.
Forest plot—RVA originating from the SA.

Figure 6.
Forest plot—C3 TF entrance.

Figure 7.
Forest plot—C4 TF entrance of the LVAs originating from the AA.

Figure 8.
Forest plot—C4 TF entrance of the LVAs.

Figure 9.
Forest plot—C4 TF entrance of the RVAs.

Figure 10.
Forest plot—C4 TF entrance.

Figure 11.
Forest plot—C5 TF entrance of the LVAs originating from the AA.

Figure 12.
Forest plot—C5 TF entrance of the SA-originating LVAs.

Figure 13.
Forest plot—C5 TF entrance of the LVAs.

Figure 14.
Forest plot—C5 TF entrance of the RVAs.

Figure 15.
Forest plot—C5 TF entrance.

Figure 16.
Forest plot—C6 TF entrance of AA-originating LVAs.

Figure 17.
Forest plot—C6 TF entrance of SA-originated LVAs.

Figure 18.
Forest plot—C6 TF entrance of the LVAs.

Figure 19.
Forest plot—C6 TF entrance of the RVAs.

Figure 20.
Forest plot—C6 TF entrance.

Figure 21.
Forest plot—C7 TF entrance of the SA-originated LVAs.

Figure 22.
Forest plot—C7 TF entrance of the LVAs.

Figure 23.
Forest plot—C7 TF entrance of the RVAs.

Figure 24.
Forest plot—C7 TF entrance.

Figure 25.
Forest plot—Tortuosity prevalence.

Figure 26.
Forest plot—LVA dominance prevalence.

Figure 27.
Forest plot—RVA dominance prevalence.

Figure 28.
Forest plot—Hypoplasia prevalence.

Figure 29.
Computed tomography angiogram. Sagittal slice through the left vertebral artery originating the aortic arch and entering the transverse foramen of the fifth cervical vertebra. Original evidence: 1. aortic arch; 2. left vertebral artery; 3. transverse process of sixth cervical vertebra; 4. transverse process of fifth cervical vertebra.
Figure 29.
Computed tomography angiogram. Sagittal slice through the left vertebral artery originating the aortic arch and entering the transverse foramen of the fifth cervical vertebra. Original evidence: 1. aortic arch; 2. left vertebral artery; 3. transverse process of sixth cervical vertebra; 4. transverse process of fifth cervical vertebra.

Figure 30.
Axial CT slice at the level of C4 viewed inferiorly. Right vertebral artery hypoplasia (arrowhead). Normoplastic left vertebral artery (arrow).
Figure 30.
Axial CT slice at the level of C4 viewed inferiorly. Right vertebral artery hypoplasia (arrowhead). Normoplastic left vertebral artery (arrow).

Figure 31.
Angio-CT, three-dimensional volume rendering of the vertebral arteries (VAs). Right infero-lateral view. Kinked V1 segment of left VA and V2 segment of right VA: 1. aortic arch; 2. right subclavian artery; 3. left subclavian artery; 4. inferiorly kinked V1 segment of left VA; 5. right VA; 6. right transverse process of C6 vertebra; 7. laterally kinked V2 segment of right VA, in the C1–C2 intertransverse space; 8. posterior arch of atlas; 9. V3 segment of right VA; 10. left internal carotid artery; 11. left internal jugular vein.
Figure 31.
Angio-CT, three-dimensional volume rendering of the vertebral arteries (VAs). Right infero-lateral view. Kinked V1 segment of left VA and V2 segment of right VA: 1. aortic arch; 2. right subclavian artery; 3. left subclavian artery; 4. inferiorly kinked V1 segment of left VA; 5. right VA; 6. right transverse process of C6 vertebra; 7. laterally kinked V2 segment of right VA, in the C1–C2 intertransverse space; 8. posterior arch of atlas; 9. V3 segment of right VA; 10. left internal carotid artery; 11. left internal jugular vein.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Determined prevalence for anatomical characteristics based on study type (autopsy or imaging).
Table 1.
Determined prevalence for anatomical characteristics based on study type (autopsy or imaging).
| Anatomical Characteristics | Study Type | Total No. of Articles | Prevalence (%) | Statistical Significance (p < 0.05) | Heterogeneity (%) | Significant Publication Bias (p < 0.05) |
|---|---|---|---|---|---|---|
| LVA_AA | Autopsy | 16 | 5.47 | Yes | 31.05 | Yes |
| LVA_AA | Imaging | 19 | 4.59 | Yes | 73.16 | No |
| LVA_SA | Autopsy | 15 | 94.5 | Yes | 33.29 | Yes |
| LVA_SA | Imaging | 16 | 93.5 | Yes | 97.31 | Yes |
| RVA_SA | Autopsy | 9 | 99.8 | Yes | 19.18 | Yes |
| RVA_SA | Imaging | 14 | 99.9 | Yes | 0 | Yes |
| C4_TF entrance | Autopsy | 8 | 0.7 | Yes | 0 | No |
| C4_TF entrance | Imaging | 17 | 1.45 | Yes | 61.08 | Yes |
| C5_TF entrance | Autopsy | 13 | 4.37 | Yes | 72.12 | No |
| C5_TF entrance | Imaging | 17 | 8.36 | Yes | 99.34 | Yes |
| C6_TF entrance | Autopsy | 17 | 88.2 | Yes | 92.46 | No |
| C6_TF entrance | Imaging | 19 | 93.6 | Yes | 91.53 | No |
| C7_TF entrance | Autopsy | 9 | 5.42 | Yes | 44.21 | No |
| C7_TF entrance | Imaging | 13 | 0.8 | Yes | 71.82 | Yes |
| Tortuosity | Autopsy | 8 | 31.0 | Yes | 96.84 | No |
| Tortuosity | Imaging | 8 | 25.8 | Yes | 99.92 | No |
| Hypoplasia | Autopsy | 3 | 7.63 | No | 89.36 | Yes |
| Hypoplasia | Imaging | 11 | 8.16 | Yes | 94.72 | No |
Table 2.
Studies included in the analysis.
| Reference & Year | Study Type | Number of Specimens | Area of Interest | NOS-Modified Score |
|---|---|---|---|---|
| Adachi 1928 [19] | Autopsy | 516 | Origin/TF entrance | 5 |
| Alicioglu 2015 [20] | Imaging | 110 | Origin/Tortuosity | 5 |
| Yazici 2018 [21] | Imaging | 100 | Dominance | 4 |
| Gitkind 2014 [22] | Autopsy | 20 | TF entrance/Tortuosity | 5 |
| Bean 1905 [23] | Autopsy | 129 | Origin/TF entrance | 6 |
| Bergman 2012 [24] | Autopsy | 693 | Origin | 5 |
| Berko 2009 [25] | Imaging | 1000 | Origin | 7 |
| Bhatia 2005 [26] | Autopsy | 81 | Origin | 4 |
| Bruneau 2006 [8] | Imaging | 500 | TF entrance/Dominance/Tortuosity | 5 |
| Budhiraja 2013 [27] | Autopsy | 52 | Origin | 5 |
| Taitz 1991 [28] | Autopsy | 36 | Tortuosity | 5 |
| Cavdar 1996 [29] | Autopsy | 24 | TF entrance | 5 |
| Chanapa 2012 [30] | Autopsy | 362 | TF entrance | 4 |
| Lin 2018 [31] | Imaging | 2437 | Origin/TF entrance | 6 |
| Dodevski 2011 [32] | Imaging | 60 | Origin/TF entrance/Tortuosity/Hypoplasia | 5 |
| Einstein 2016 [33] | Autopsy | 27 | Origin | 4 |
| Civelek 2007 [34] | Autopsy | 30 | TF entrance | 4 |
| Ergun 2016 [35] | Imaging | 508 | Origin/Hypoplasia/Dominance | 6 |
| Eskander 2010 [36] | Imaging | 500 | TF entrance/Hypoplasia | 5 |
| Fayza 2019 [37] | Imaging | 200 | Origin/TF entrance/Dominance | 5 |
| Gaigalaite 2016 [38] | Imaging | 742 | Hypoplasia | 6 |
| Güvençer 2006 [39] | Imaging | 24 | TF entrance | 4 |
| Tetiker 2014 [40] | Imaging | 79 | Origin/TF entrance | 4 |
| Hauke 1973 [41] | Imaging | 218 | Tortuosity | 5 |
| Heary 1996 [42] | Imaging | 16 | TF entrance | 4 |
| Hong 2008 [43] | Imaging | 700 | TF entrance/Tortuosity | 6 |
| Ikegami 2007 [44] | Autopsy | 50 | Origin/TF entrance | 4 |
| Jakanani 2010 [45] | Imaging | 861 | Origin | 7 |
| Johnson 1995 [46] | Autopsy | 20 | TF entrance | 5 |
| Kajimoto 2007 [47] | Autopsy | 40 | TF entrance | 5 |
| Kim 2017 [48] | Imaging | 476 | Origin/TF entrance | 5 |
| Komiyama 2001 [49] | Imaging | 1567 | Origin | 6 |
| Li 2019 [50] | Autopsy | 238 | Origin/Tortuosity/Hypoplasia | 6 |
| Matula 1997 [51] | Imaging | 402 | TF entrance/Tortuosity | 6 |
| Meila 2012 [52] | Imaging | 1083 | Origin/TF entrance | 6 |
| Muller 2011 [53] | Imaging | 2033 | Origin | 7 |
| O’Malley 2018 [54] | Autopsy | 24 | Origin | 5 |
| Omotoso 2021 [55] | Imaging | 1108 | Origin/TF entrance/Hypoplasia/Dominance | 5 |
| Palmer 1980 [56] | Imaging | 400 | Tortuosity | 5 |
| Patil 2012 [57] | Autopsy | 75 | Origin | 5 |
| Ranganatha 2006 [58] | Autopsy | 38 | TF entrance/Tortuosity | 4 |
| Raveendranath 2014 [59] | Autopsy | 66 | Origin/TF entrance/Tortuosity/Hypoplasia | 5 |
| Russo 2011 [60] | Autopsy | 20 | TF entrance/Tortuosity | 5 |
| Vujmilović 2018 [61] | Imaging | 224 | Origin/TF entrance | 5 |
| Schmitt 2019 [62] | Autopsy | 10 | TF entrance | 5 |
| Shin 2014 [63] | Imaging | 920 | TF entrance | 6 |
| Shin 2008 [64] | Autopsy | 28 | Origin | 6 |
| Tasdemir 2022 [1] | Imaging | 644 | Origin/TF entrance/Hypoplasia/Dominance | 6 |
| Thierfelder 2014 [65] | Imaging | 934 | Hypoplasia | 6 |
| Touboul 1986 [66] | Imaging | 100 | TF entrance/Hypoplasia/Dominance | 6 |
| Toyoharu 1991 [67] | Autopsy | 144 | Origin | 5 |
| Trattnig 1993 [17] | Autopsy | 140 | Tortuosity/Hypoplasia | 5 |
| Trattnig 1993 [17] | Imaging | 160 | Origin/Tortuosity/Hypoplasia | 6 |
| Tschabitscher 1991 [15] | Autopsy | 70 | TF entrance/Tortuosity | 5 |
| Tubbs 2009 [68] | Autopsy | 20 | TF entrance | 4 |
| Uchino 2013 [69] | Imaging | 4574 | Origin/TF entrance | 6 |
| Vaiman 2010 [18] | Imaging | 23 | Origin/TF entrance | 5 |
| Vorster 1998 [70] | Autopsy | 120 | Origin | 5 |
| Wang 2016 [71] | Imaging | 2370 | Origin/Hypoplasia/Dominance | 4 |
| Woraputtaporn 2019 [72] | Autopsy | 532 | Origin/TF entrance | 6 |
| Yamaki 2006 [73] | Autopsy | 1029 | Origin/TF entrance | 6 |
| Chen 2009 [74] | Imaging | 2000 | Hypoplasia | 6 |
| Yi 2022 [75] | Imaging | 446 | Origin/TF entrance | 6 |
Table 3.
Determined prevalence for anatomical characteristics reported in fewer than 5 articles.
| Anatomical Characteristic | Total No. of Articles | Total No. of Cases | Prevalence (%) | Statistical Significance (p < 0.05) | Heterogeneity (%) |
|---|---|---|---|---|---|
| RVA_AA | 4 | 2992 | 0.1 | No | 11.7 |
| RVA_RCCA | 4 | 4368 | 0.126 | Yes | 0 |
| RVA_BCT | 3 | 848 | 0.539 | No | 73 |
| C3_TF ENTRANCE_LVA_AA | 3 | 40 | 8.11 | No | 0 |
| C4_TF ENTRANCE_LVA_SA | 4 | 2736 | 0.337 | No | 39.11 |
| C7_TF ENTRANCE_LVA_AA | 4 | 181 | 3.95 | Yes | 0 |
| Coronal Tortuosity | 3 | 380 | 16.6 | Yes | 78.87 |
| Sagittal Tortuosity | 3 | 380 | 22.8 | Yes | 27.87 |
| Transverse Tortuosity | 3 | 380 | 30.1 | Yes | 84.63 |
| Straight V1 | 3 | 430 | 45.2 | Yes | 74.14 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Tudose, R.C.; Rusu, M.C.; Hostiuc, S. The Vertebral Artery: A Systematic Review and a Meta-Analysis of the Current Literature. Diagnostics 2023, 13, 2036. https://doi.org/10.3390/diagnostics13122036
AMA Style
Tudose RC, Rusu MC, Hostiuc S. The Vertebral Artery: A Systematic Review and a Meta-Analysis of the Current Literature. Diagnostics. 2023; 13(12):2036. https://doi.org/10.3390/diagnostics13122036
Chicago/Turabian StyleTudose, Răzvan Costin, Mugurel Constantin Rusu, and Sorin Hostiuc. 2023. "The Vertebral Artery: A Systematic Review and a Meta-Analysis of the Current Literature" Diagnostics 13, no. 12: 2036. https://doi.org/10.3390/diagnostics13122036
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.