
Development and Evaluation of a Multifrequency Ultrafast Doppler Spectral Analysis (MFUDSA) Algorithm for Wall Shear Stress Measurement: A Simulation and In Vitro Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
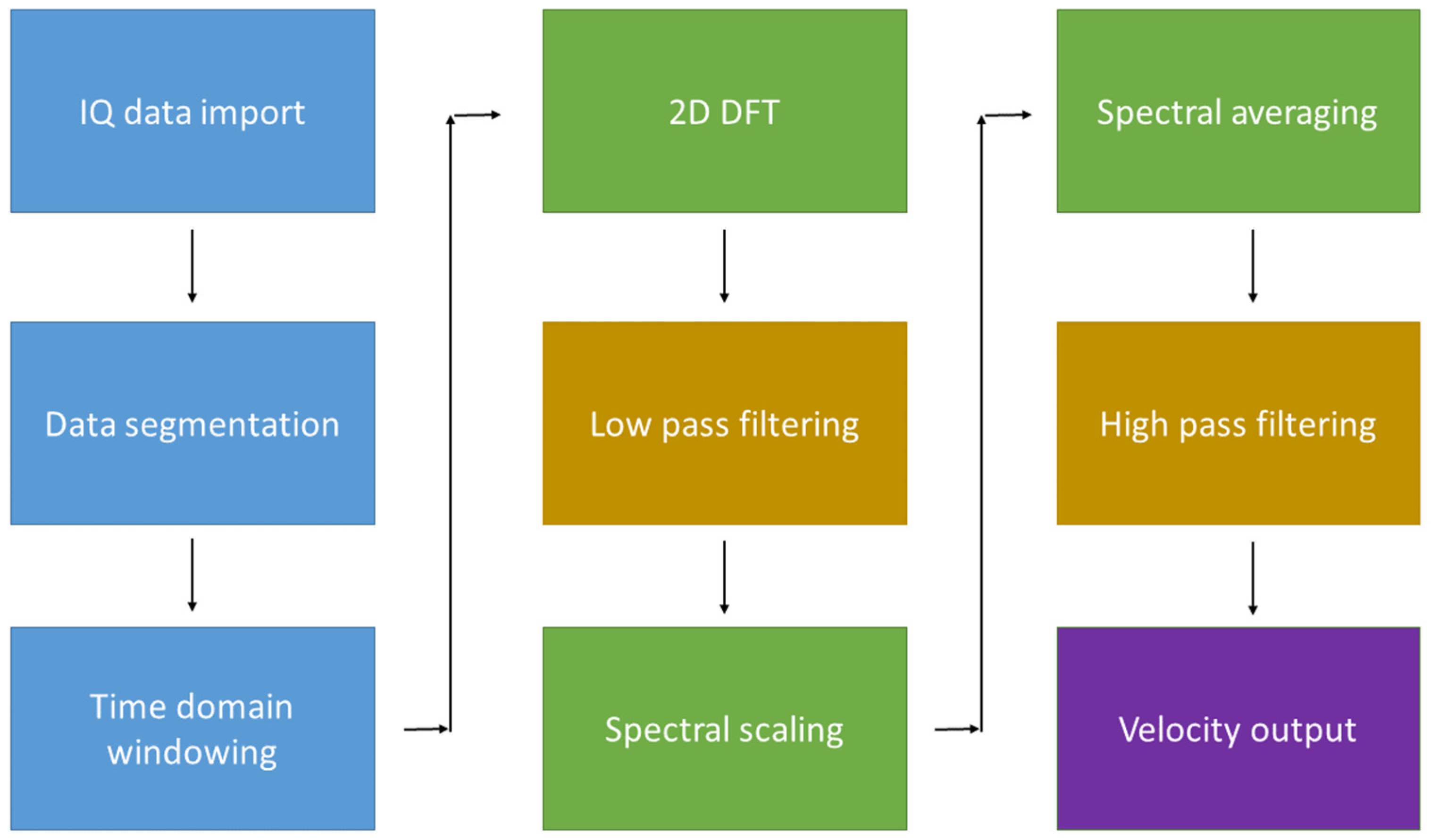
2.1. MFUDSA Algorithm Development
2.2. MFUDSA Algorithm Optimisation
2.3. MFUDSA Algorithm Evaluation
2.4. Validation of Algorithm in Comparison to Other Techniques
2.5. Analysis
3. Results
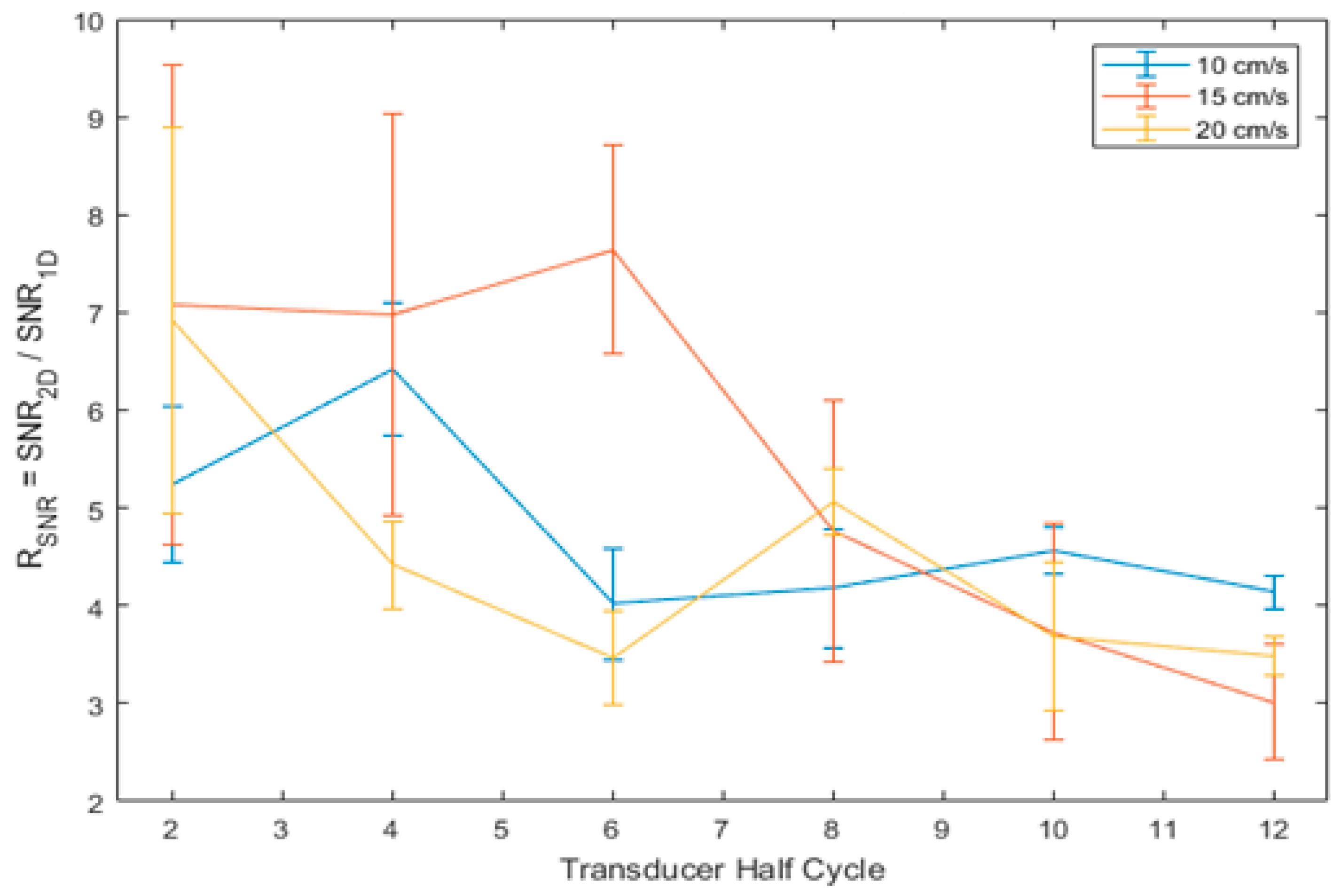
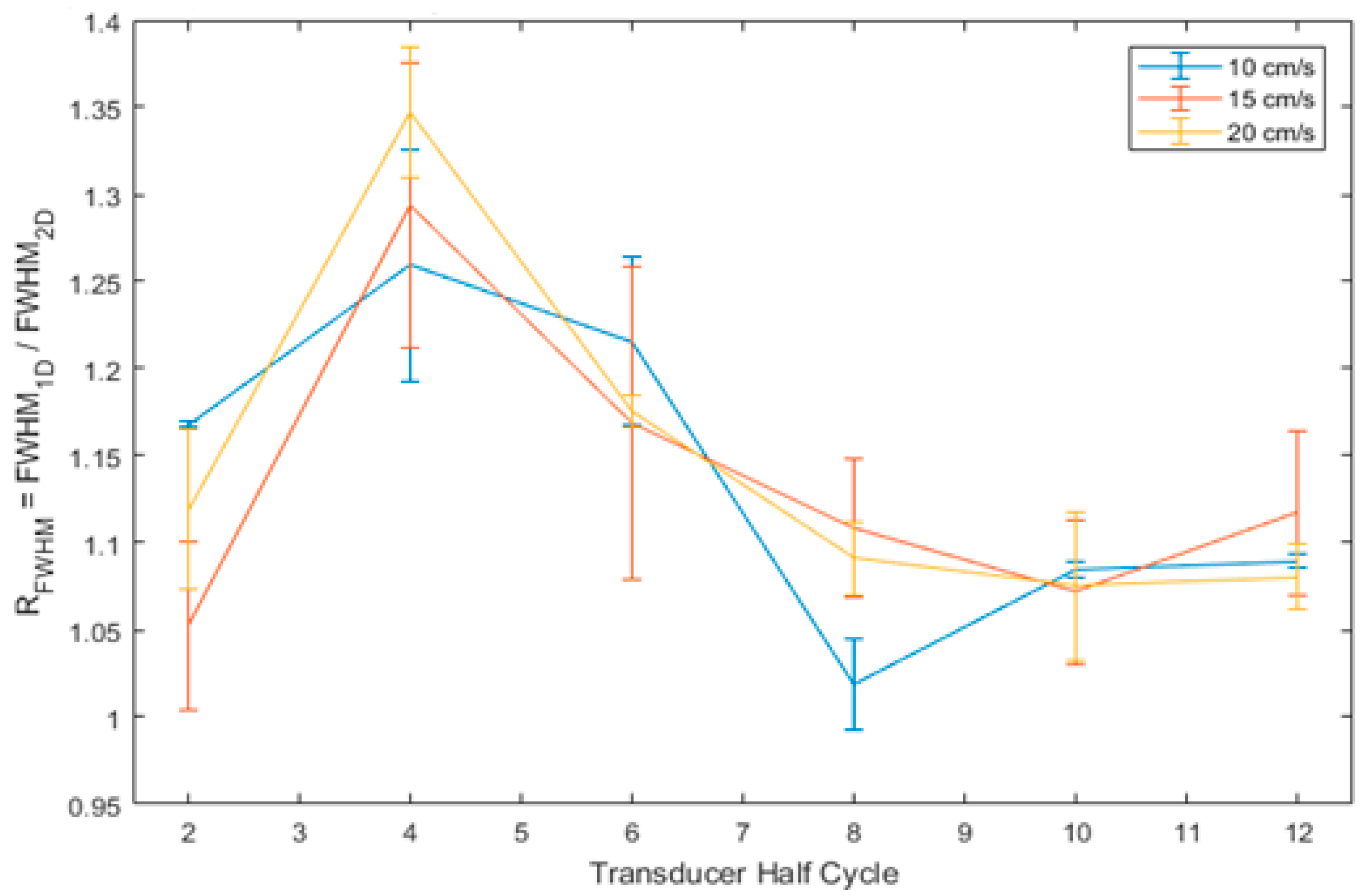
3.1. MFUDSA Algorithm Optimisation
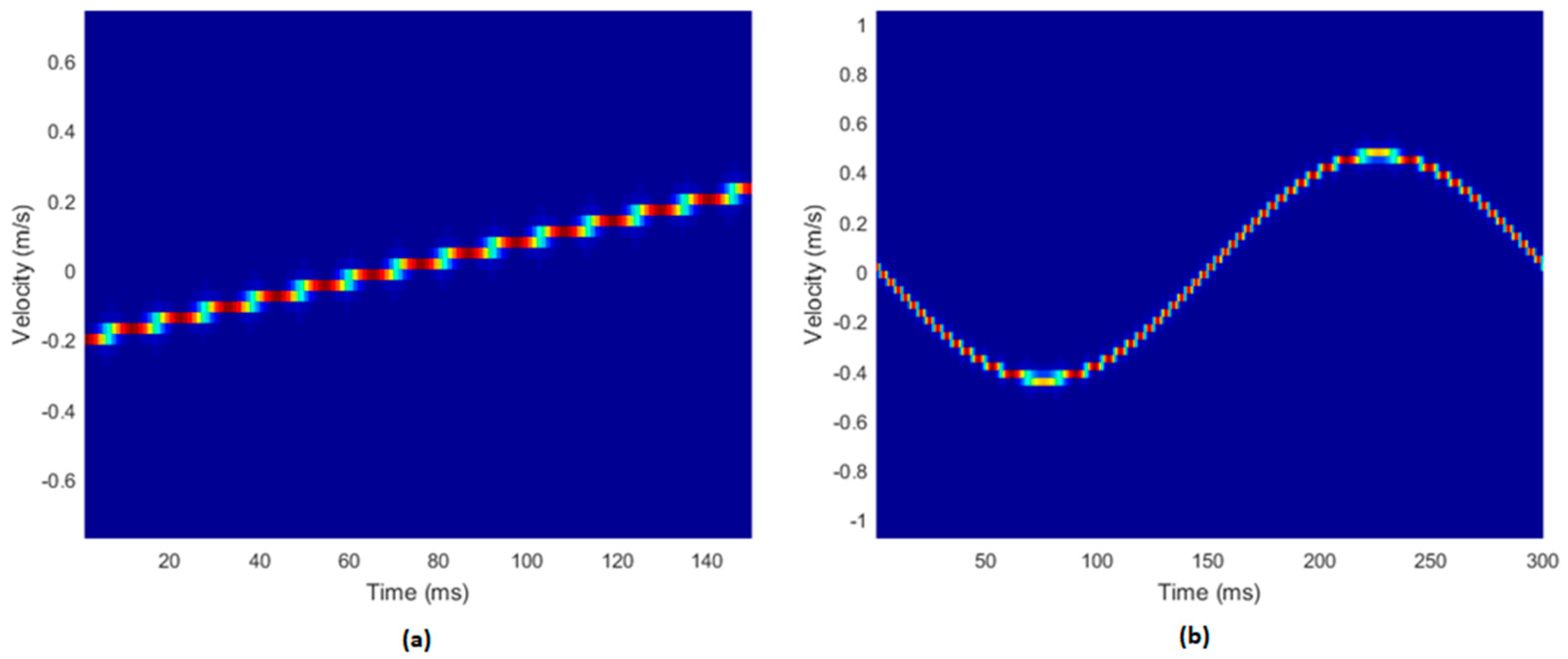
3.2. Simulation Data
3.3. In Vitro Phantom Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organisation Cardiovascular Diseases (CVDs). Available online: https://www.who.int/en/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 16 May 2019).
- Brusseau, E.; Fromageau, J.; Finet, G.; Delachartre, P.; Vray, D. Axial Strain Imaging of Intravascular Data: Results on Polyvinyl Alcohol Cryogel Phantoms and Carotid Artery. Ultrasound Med. Biol. 2001, 27, 1631–1642. [Google Scholar] [CrossRef]
- Zaman, A.; Helft, G.; Worthley, S.; Badimon, J. The Role of Plaque Rupture and Thrombosis in Coronary Artery Disease. Atherosclerosis 2000, 149, 251–266. [Google Scholar] [CrossRef]
- Palombo, C.; Kozakova, M. Arterial Stiffness, Atherosclerosis and Cardiovascular Risk: Pathophysiologic Mechanisms and Emerging Clinical Indications. Vascul. Pharmacol. 2016, 77, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Aboyans, V.; Ricco, J.-B.; Bartelink, M.-L.E.L.; Björck, M.; Brodmann, M.; Cohnert, T.; Collet, J.-P.; Czerny, M.; De Carlo, M.; Debus, S.; et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in Collaboration with the European Society for Vascular Surgery (ESVS). Eur. J. Vasc. Endovasc. Surg. 2017, 39, 763–816. [Google Scholar] [CrossRef] [PubMed]
- Herzig, R.; Burval, S.; Krupka, B.; Vlachova, I.; Urbanek, K.; Mares, J. Comparison of Ultrasonography, CT Angiography, and Digital Subtraction Angiography in Severe Carotid Stenoses. Eur. J. Neurol. 2004, 11, 774–781. [Google Scholar] [CrossRef] [PubMed]
- Hartung, M.P.; Grist, T.M.; François, C.J. Magnetic Resonance Angiography: Current Status and Future Directions. J. Cardiovasc. Magn. Reson. 2011, 13, 19. [Google Scholar] [CrossRef] [PubMed]
- Gnasso, A.; Carallo, C.; Irace, C.; De Franceschi, M.S.; Mattioli, P.L.; Motti, C.; Cortese, C. Association between Wall Shear Stress and Flow-Mediated Vasodilation in Healthy Men. Atherosclerosis 2001, 156, 171–176. [Google Scholar] [CrossRef]
- Gnasso, A.; Carallo, C.; Irace, C.; Spagnuolo, V.; De Novara, G.; Mattioli, P.L.; Pujia, A. Association Between Intima-Media Thickness and Wall Shear Stress in Common Carotid Arteries in Healthy Male Subjects. Circulation 1996, 94, 3257–3262. [Google Scholar] [CrossRef]
- Gnasso, A.; Irace, C.; Carallo, C.; De Franceschi, M.S.; Motti, C.; Mattioli, P.L.; Pujia, A. In Vivo Association Between Low Wall Shear Stress and Plaque in Subjects With Asymmetrical Carotid Atherosclerosis. Stroke 1997, 28, 993–998. [Google Scholar] [CrossRef]
- Malek, A.M.; Alper, S.L.; Izumo, S. Hemodynamic Shear Stress and Its Role in Atherosclerosis. JAMA 1999, 282, 2035–2042. [Google Scholar] [CrossRef]
- Wei, H.; Yao, K.; Tian, Q.; Han, S.; Gao, W.; Han, W.; Liu, S.; Wang, G.; Chen, Q.; Li, M. Low Wall Shear Stress and High Intra-Aneurysmal Pressure Are Associated with Ruptured Status of Vertebral Artery Dissecting Aneurysms. Cardiovasc. Intervent. Radiol. 2023, 46, 240–248. [Google Scholar] [CrossRef] [PubMed]
- Hochareon, P.; Manning, K.B.; Fontaine, A.A.; Tarbell, J.M.; Deutsch, S. Wall Shear-Rate Estimation Within the 50cc Penn State Artificial Heart Using Particle Image Velocimetry. J. Biomech. Eng. 2004, 126, 430. [Google Scholar] [CrossRef] [PubMed]
- Natarajan, S.; Mokhtarzadeh-Dehghan, M. A Numerical and Experimental Study of Periodic Flow in a Model of a Corrugated Vessel with Application to Stented Arteries. Med. Eng. Phys. 2000, 22, 555–566. [Google Scholar] [CrossRef] [PubMed]
- Anastasiou, A.D.; Spyrogianni, A.S.; Koskinas, K.C.; Giannoglou, G.D.; Paras, S.V. Experimental Investigation of the Flow of a Blood Analogue Fluid in a Replica of a Bifurcated Small Artery. Med. Eng. Phys. 2012, 34, 211–218. [Google Scholar] [CrossRef]
- Vennemann, P.; Kiger, K.T.; Lindken, R.; Groenendijk, B.C.W.; Stekelenburg-De Vos, S.; Ten Hagen, T.L.M.; Ursem, N.T.C.; Poelmann, R.E.; Westerweel, J.; Hierck, B.P. In Vivo Micro Particle Image Velocimetry Measurements of Blood—Plasma in the Embryonic Avian Heart. J. Biomech. 2006, 39, 1191–1200. [Google Scholar] [CrossRef]
- Shaaban, A.M.; Duerinckx, A.J. Wall Shear Stress and Early Atherosclerosis: A Review. AJR. Am. J. Roentgenol. 2000, 174, 1657–1665. [Google Scholar] [CrossRef]
- Osinnski, J.; Ku, D.; Mukundan, S. Determination of Wall Shear Stress in the Aorta with the Use of MR Phase Velocity Mapping. J. Magn. 1995, 5, 640–647. [Google Scholar] [CrossRef]
- Reneman, R.; Arts, T.; Hoeks, A. Wall Shear Stress–an Important Determinant of Endothelial Cell Function and Structure–in the Arterial System in Vivo. J. Vasc. Res. 2006, 43, 251–269. [Google Scholar] [CrossRef]
- Katritsis, D.; Kaiktsis, L.; Chaniotis, A.; Pantos, J.; Efstathopoulos, E.P.; Marmarelis, V. Wall Shear Stress: Theoretical Considerations and Methods of Measurement. Prog. Cardiovasc. Dis. 2007, 49, 307–329. [Google Scholar] [CrossRef]
- Evans, D.H.; McDicken, W.N. Doppler Ultrasound: Physics, Instrumentation and Signal Processing, 2nd ed.; Wiley: Hoboken, NJ, USA, 2000. [Google Scholar]
- Hoskins, P.R.; Thrush, A.; Martin, K.; Whittingham, T.A. Diagnostic Ultrasound: Physics and Equipment, 1st ed.; Greenwich Medical Media Ltd.: London, UK, 2003. [Google Scholar]
- Bercoff, J. Ultrafast Ultrasound Imaging. In Ultrasound Imaging—Medical Applications; InTech: London, UK, 2011. [Google Scholar]
- Bercoff, J.; Montaldo, G.; Loupas, T.; Savery, D.; Mézière, F.; Fink, M. Ultrafast Compound Doppler Imaging: Providing Full Blood Flow Characterization. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2011, 58, 134–147. [Google Scholar] [CrossRef]
- Loupas, T.; Gill, R.W. Multifrequency Doppler: Improving the Quality of Spectral Estimation by Making Full Use of the Information Present in the Backscattered RF Echoes. IEEE Trans. Ultrason. Ferroelectr. Freq. Control. 1994, 41, 522–531. [Google Scholar] [CrossRef]
- Loupas, T.; Powers, J.T.; Gill, R.W. An Axial Velocity Estimator for Ultrasound Blood Flow Imaging, Based on a Full Evaluation of the Doppler Equation by Means of a Two-Dimensional Autocorrelation Approach. IEEE Trans. Ultrason. Ferroelectr. Freq. Control. 1995, 42, 672–688. [Google Scholar] [CrossRef]
- Loupas, T.; Peterson, R.B.; Gill, R.W. Experimental Evaluation of Velocity and Power Estimation for Ultrasound Blood Flow Imaging, by Means of a Two-Dimensional Autocorrelation Approach. IEEE Trans. Ultrason. Ferroelectr. Freq. Control. 1995, 42, 689–699. [Google Scholar] [CrossRef]
- Ivory, A. Development of an Optimised Subharmonic Dynamic Contrast-Enhanced Ultrasound Imaging Tehnique for Liver Cancer. Ph.D. Thesis, The University of Dublin, Dublin, Ireland, 2018. [Google Scholar]
- Ivory, A.M.; Meaney, J.F.; Fagan, A.J.; Browne, J.E. Optimisation of the transmit beam parameters for generation of subharmonic signals in native and altered populations of a commercial microbubble contrast agent SonoVue®. Phys. Med. 2020, 70, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Malone, A.J.; Cournane, S.; Naydenova, I.G.; Fagan, A.J.; Browne, J.E. Polyvinyl Alcohol Cryogel Based Vessel Mimicking Material for Modelling the Progression of Atherosclerosis. Phys. Med. 2020, 69, 1–8. [Google Scholar] [CrossRef]
- Yamamoto, T.; Ogasawara, Y.; Kimura, A.; Tanaka, H.; Hiramatsu, O.; Tsujioka, K.; Lever, M.J.; Parker, K.H.; Jones, C.J.H.; Caro, C.G.; et al. Blood Velocity Profiles in the Human Renal Artery by Doppler Ultrasound and Their Relationship to Atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 1996, 16, 172–177. [Google Scholar] [CrossRef]
- Chu, K.C.; Rutt, B.K. Polyvinyl Alcohol Cryogel: An Ideal Phantom Material for MR Studies of Arterial Flow and Elasticity. Magn. Reson. Med. 1997, 37, 314–319. [Google Scholar] [CrossRef]
- King, D.M.; Moran, C.M.; McNamara, J.D.; Fagan, A.J.; Browne, J.E. Development of a Vessel-Mimicking Material for Use in Anatomically Realistic Doppler Flow Phantoms. Ultrasound Med. Biol. 2011, 37, 813–826. [Google Scholar] [CrossRef]
- Teirlinck, C.J.P.M.; Bezemer, R.A.; Kollmann, C.; Lubbers, J.; Hoskins, P.R.; Fish, P.; Fredfeldt, K.-E.; Schaarschmidt, U.G. Development of an Example Flow Test Object and Comparison of Five of These Test Objects, Constructed in Various Laboratories. Ultrasonics 1998, 36, 653–660. [Google Scholar] [CrossRef]
- IEC 61685; Ultrasonics—Flow Measurement—Flow Test Objects. International Electrotechnical Commission: Geneva, Switzerland, 2001.
- Beattie, D.; Golledge, J.; Greenhalgh, R.; Davies, A. Duplex Imaging and Renal Artery Stenosis. J. Vasc. Investig. 1997, 3, 52–60. [Google Scholar]
- Chatzizisis, Y.S.; Coskun, A.U.; Jonas, M.; Edelman, E.R.; Feldman, C.L.; Stone, P.H. Role of Endothelial Shear Stress in the Natural History of Coronary Atherosclerosis and Vascular Remodeling. J. Am. Coll. Cardiol. 2007, 49, 2379–2393. [Google Scholar] [CrossRef]
- Angelsen, B.A. Ultrasound Imaging: Waves, Signals, and Signal Processing. 2. Propagation and Scattering in Heterogeneous, Nonlinear Tissue with Contrast Agent Imaging and Doppler Measurements; Emantec: Trondheim, Norway, 2000. [Google Scholar]
- Meunier, J.; Bertrand, M. Ultrasonic Texture Motion Analysis: Theory and Simulation. IEEE Trans. Med. Imaging 1995, 14, 293–300. [Google Scholar] [CrossRef]
- Ford, M.D.; Xie, Y.J.; Wasserman, B.A.; Steinman, D.A. Is Flow in the Common Carotid Artery Fully Developed? Physiol. Meas. 2008, 29, 1335–1349. [Google Scholar] [CrossRef] [PubMed]
- Malone, A.; Chari, D.; Cournane, S.; Naydenova, I.; Fagan, A.J.; Browne, J.E. Investigation of the Assessment of Low Degree Renal Artery Stenosis Based on Velocity Flow Profile Analysis Using Doppler Ultrasound: An in-Vitro Study). Phys. Med. 2019, 65, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Mynard, J.P.; Wasserman, B.A.; Steinman, D.A. Errors in the Estimation of Wall Shear Stress by Maximum Doppler Velocity. Atherosclerosis 2013, 227, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Yang, K.; Hoskins, P.R.; Corner, G.A.; Xia, C.; Huang, Z. Wall Shear Stress Measurement in Carotid Artery Phantoms with Variation in Degree of Stenosis Using Plane Wave Vector Doppler. Appl. Sci. 2023, 13, 617. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Estimation Technique | Low to Medium Stiffness (Steady Flow) | Low to High Stiffness (Steady Flow) | Low to Medium Stiffness (Pulsatile Flow) | Low to High Stiffness (Pulsatile Flow) |
|---|---|---|---|---|
| PW Doppler | 0.045 | 0.032 | 0.084 | 0.041 |
| Parabolic Doppler | 0.161 | 0.041 | 0.201 | 0.062 |
| Ultrafast Doppler | 0.051 | 0.039 | 0.097 | 0.032 |
| MFUDSA Doppler | 0.003 | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malone, A.J.; Cournane, S.; Naydenova, I.; Meaney, J.F.; Fagan, A.J.; Browne, J.E. Development and Evaluation of a Multifrequency Ultrafast Doppler Spectral Analysis (MFUDSA) Algorithm for Wall Shear Stress Measurement: A Simulation and In Vitro Study. Diagnostics 2023, 13, 1872. https://doi.org/10.3390/diagnostics13111872
Malone AJ, Cournane S, Naydenova I, Meaney JF, Fagan AJ, Browne JE. Development and Evaluation of a Multifrequency Ultrafast Doppler Spectral Analysis (MFUDSA) Algorithm for Wall Shear Stress Measurement: A Simulation and In Vitro Study. Diagnostics. 2023; 13(11):1872. https://doi.org/10.3390/diagnostics13111872
Chicago/Turabian StyleMalone, Andrew J., Seán Cournane, Izabela Naydenova, James F. Meaney, Andrew J. Fagan, and Jacinta E. Browne. 2023. "Development and Evaluation of a Multifrequency Ultrafast Doppler Spectral Analysis (MFUDSA) Algorithm for Wall Shear Stress Measurement: A Simulation and In Vitro Study" Diagnostics 13, no. 11: 1872. https://doi.org/10.3390/diagnostics13111872