
Prognostic Factors for Cardiotoxicity among Children with Cancer: Definition, Causes, and Diagnosis with Omics Technologies

 , , and
, , and
Abstract
:1. Introduction
2. Cardiotoxicity
Definition
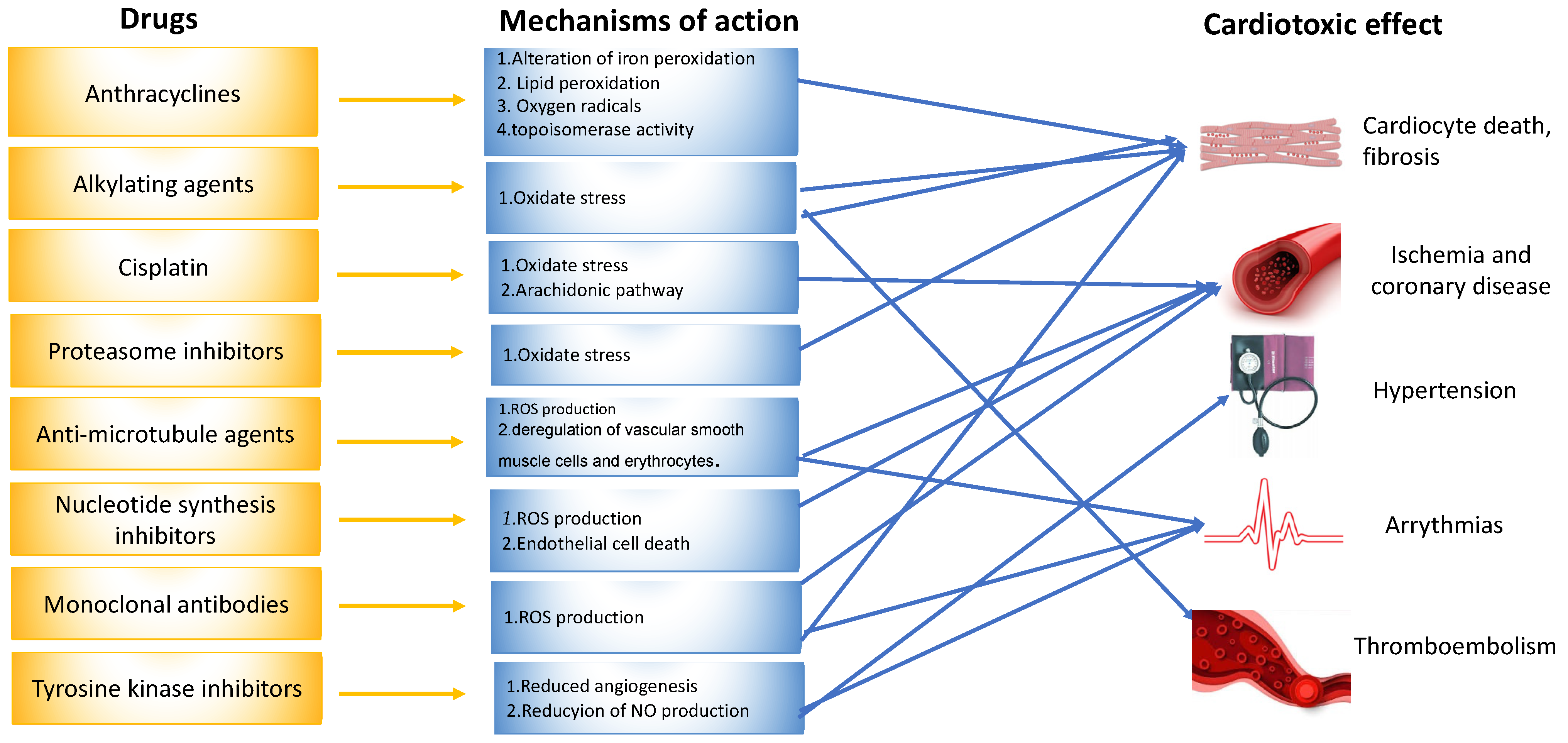
3. Chemotherapeutic Drugs
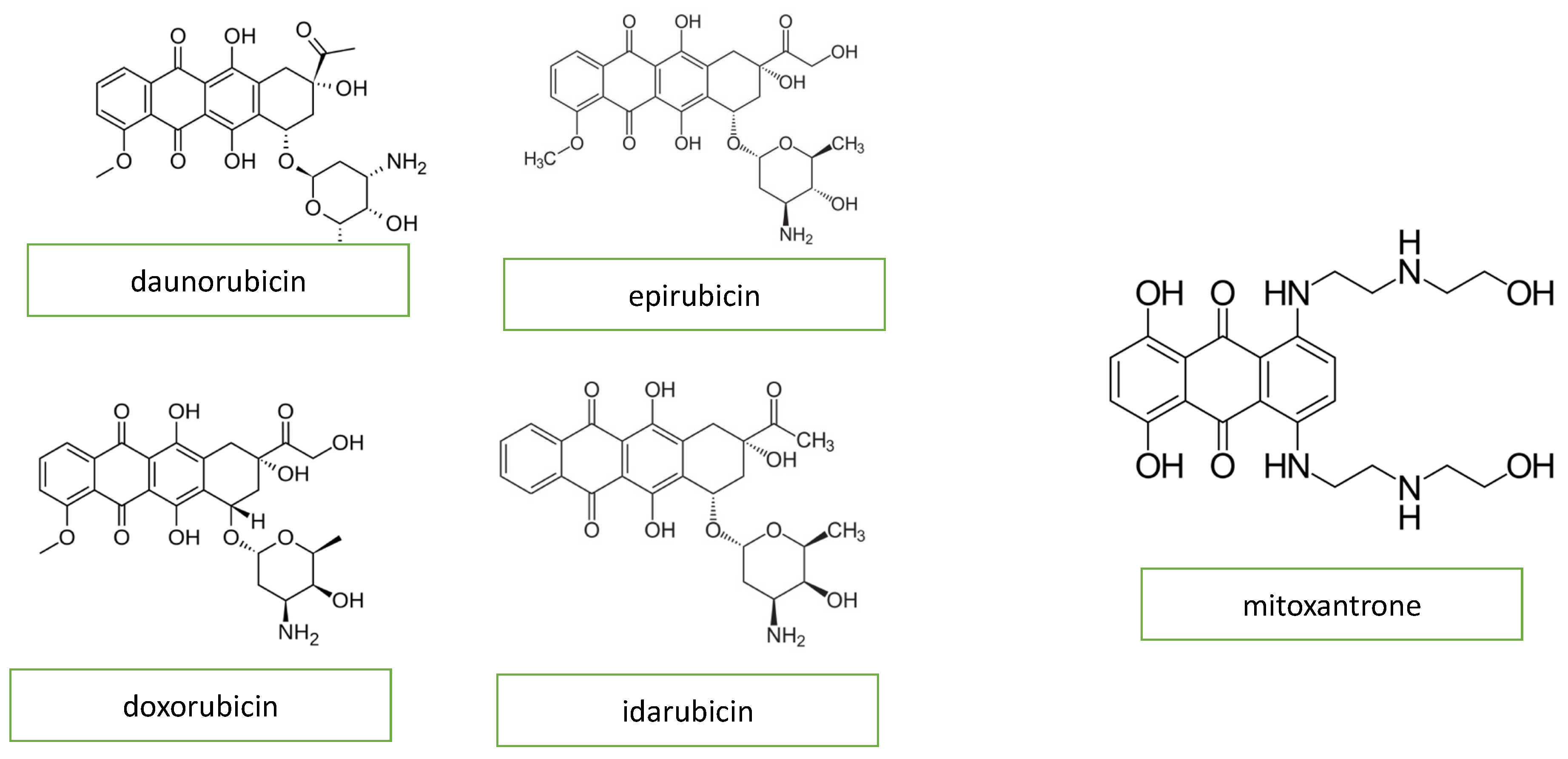
3.1. Anthracyclines
3.2. Nucleotide Synthesis Inhibitors
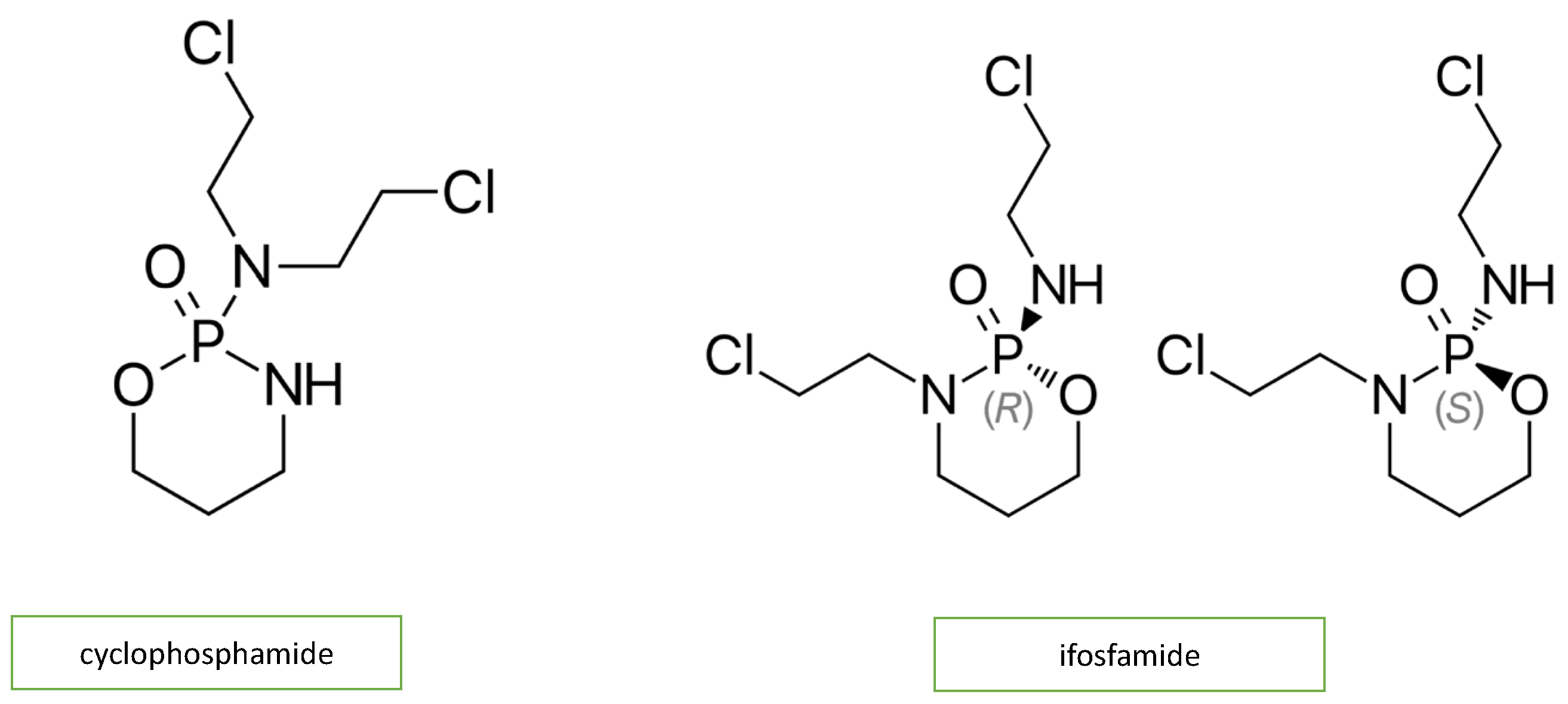
3.3. Alkylating Agents
3.4. Tyrosine Kinase Inhibitors
3.5. Anti-Microtubule Agents
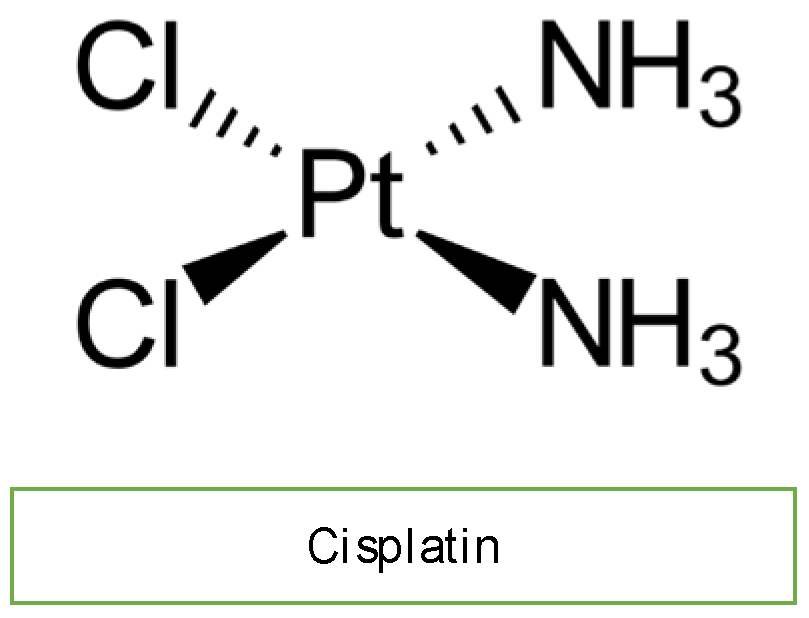
3.6. Cisplatin
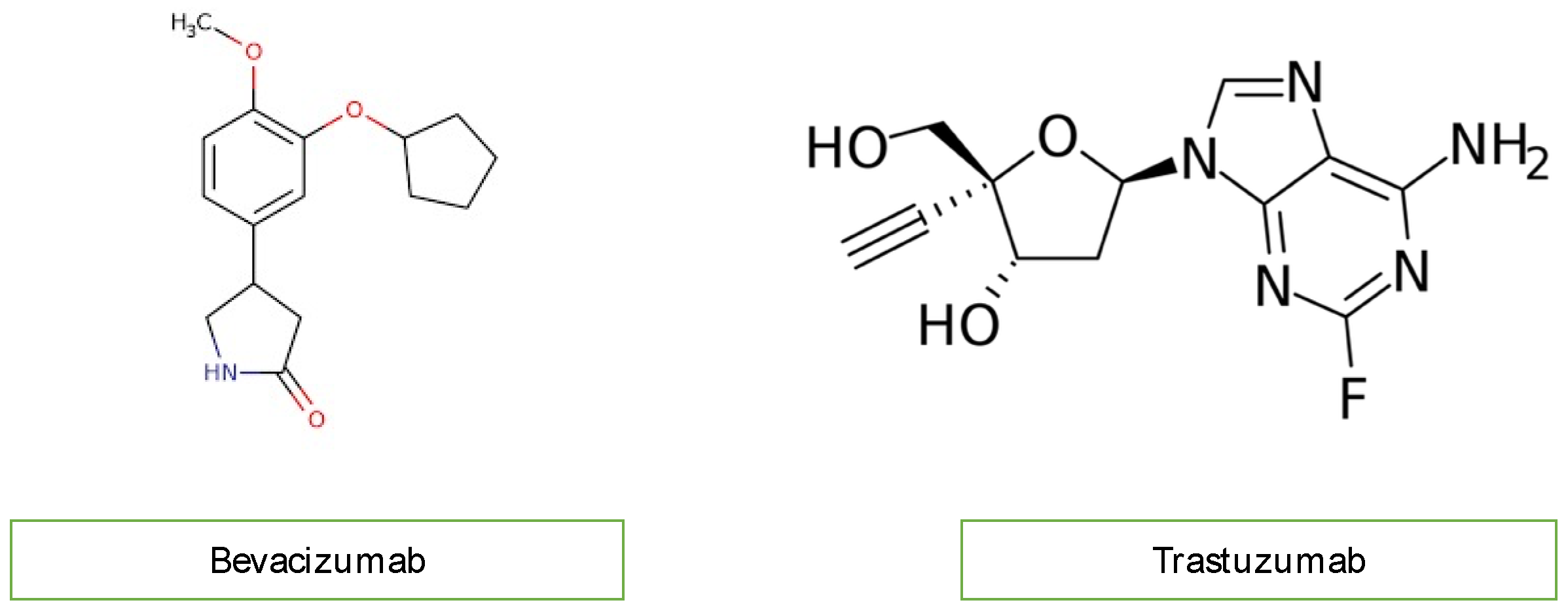
3.7. Monoclonal Antibodies
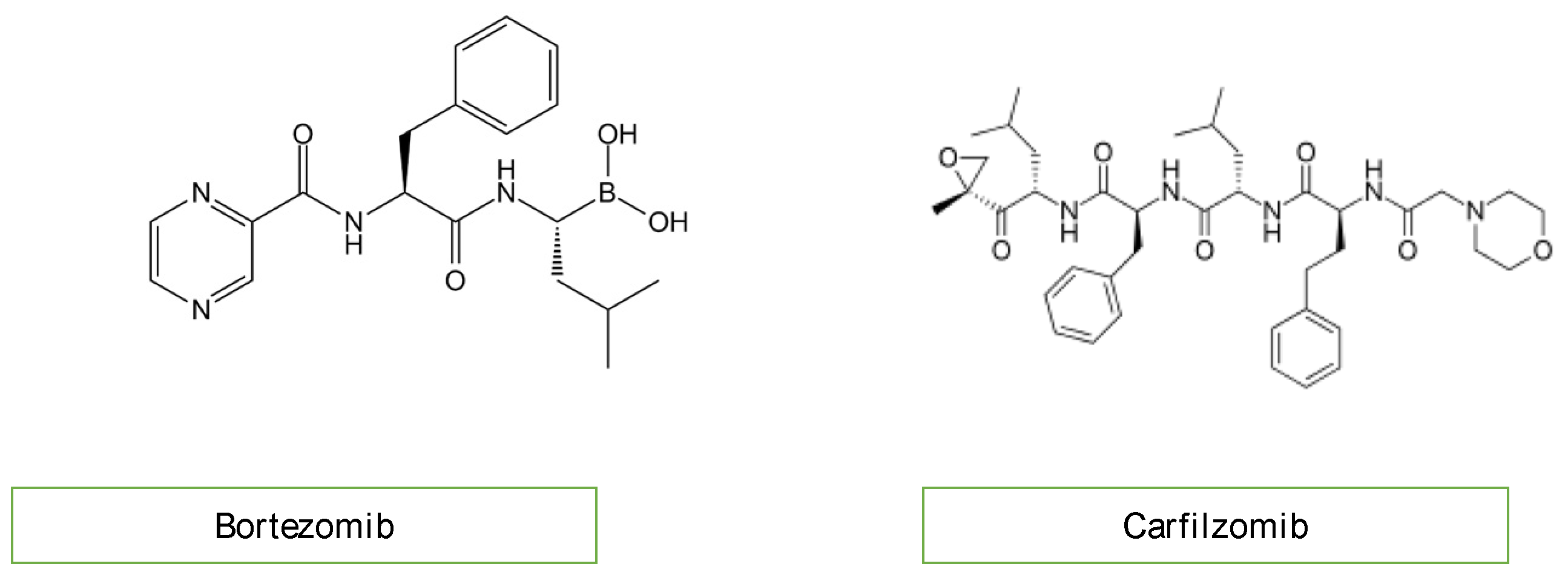
3.8. Proteasome Inhibitors
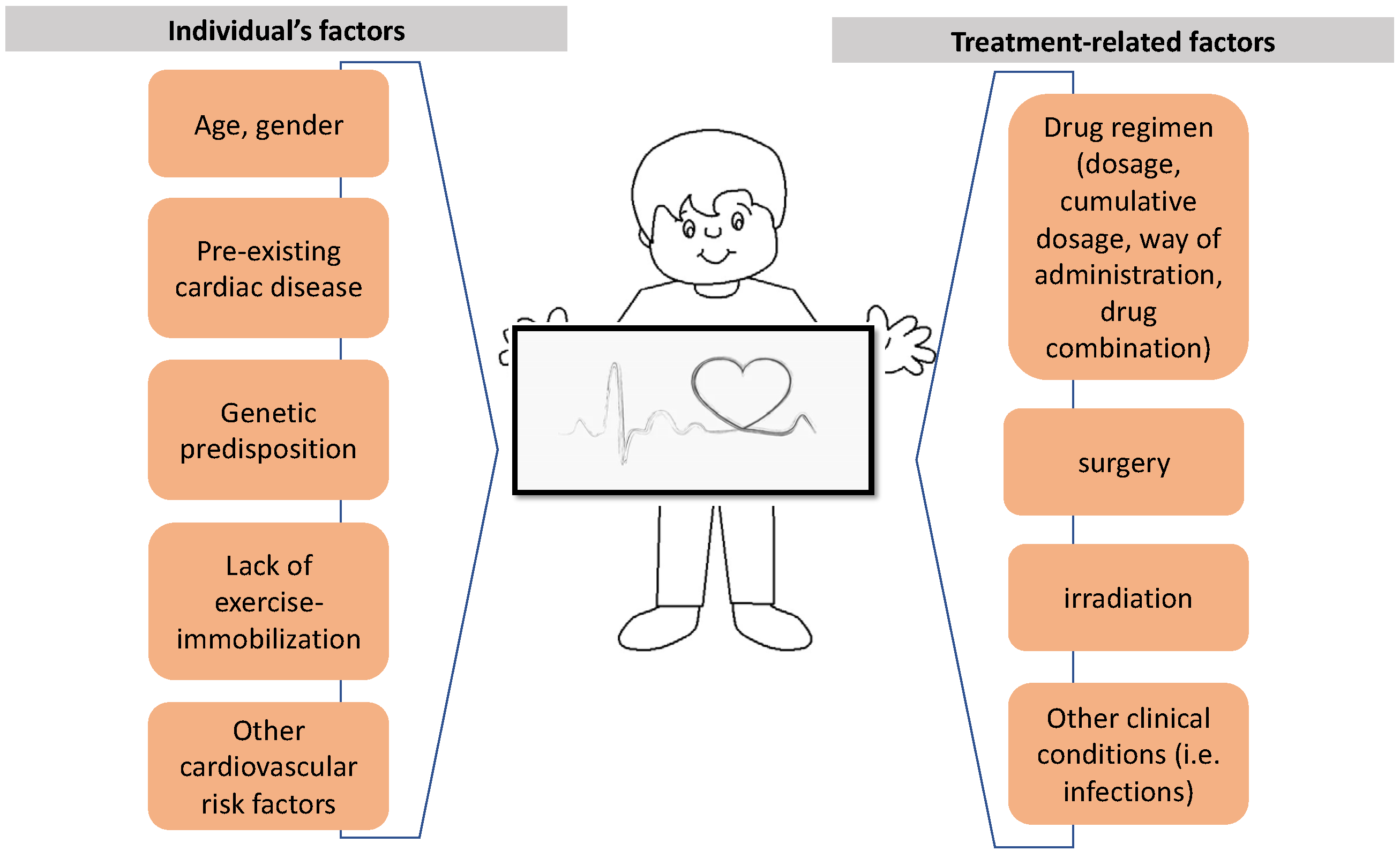
4. Risk Factors
5. Diagnosis
Imaging
6. Biomarkers
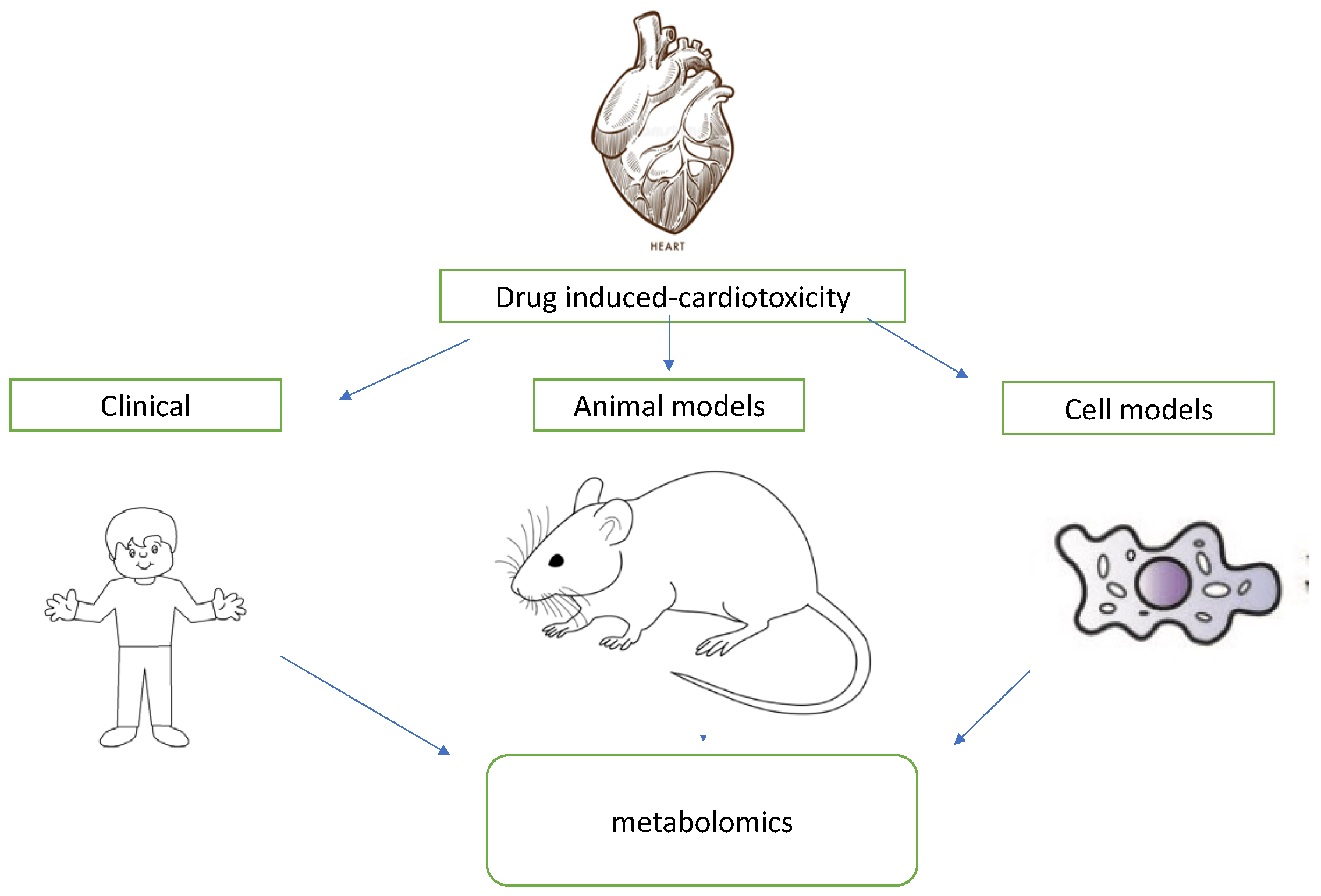
7. Omics
7.1. Genomics
7.2. Transcriptomics
7.3. Proteomics
7.4. Metabolomics
8. Conclusions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ABC | Adenosine triphosphate-binding cassette transporter |
| ABCC2 | ATP-binding cassette subfamily C member 2 |
| ACT | Anthracycline-related cardiotoxicity |
| ALL | Acute lymphoblastic leukemia |
| BNP | B-type natriuretic peptide |
| CBR | Carbonyl reductase |
| CELF4 | CUGBP Elav-like family member 4 |
| CHF | Congestive heart failure |
| CP | Cyclophosphamide |
| CMR | Cardiac magnetic resonance imaging |
| CRP | C-reactive protein |
| CVAEs | Cardiovascular adverse events |
| DOX | Doxorubicin |
| ECG | Electrocardiography |
| EVs | Extracellular vesicles |
| GC | Gas chromatography |
| GDF-15 | Growth/differentiation factor 15 |
| GLS | Global systolic longitudinal myocardial strain |
| HER2 | Human epidermal growth factor receptor 2 |
| HF | Heart failure |
| IFO | Ifosfamide |
| LC | Liquid chromatography high-performance |
| LC-MS | Liquid chromatography–mass spectrometry |
| LPC | Lysophosphatidylcholine |
| LV | Left ventricular |
| LVD | Left ventricular dysfunction |
| LVEF | Left ventricular ejection fraction |
| miRNAs | MicroRNAs |
| mRNAs | Messenger RNAs |
| MPI | Myocardial perfusion imaging |
| MS | Molecular mass spectrometry |
| MUGA | Nuclear cardiac imaging |
| NMR | Nuclear magnetic resonance spectrometry |
| NOTCH1 | Neurogenic locus notch homolog protein 1 |
| NT-proBNP | N-terminal pro b-natriuretic peptide |
| PET | Positron emission tomography |
| PYGB | Glycogen phosphorylase |
| RARG | Retinoic acid receptor gamma |
| SAL | Saline |
| SLC | Solute carrier transporters |
| SNP | Single-nucleotide polymorphism |
| SPECT | Single-photon emission computed tomography |
| SVM | Vector machine |
| TKI | Tyrosine kinase inhibitors |
| TCA | Tricarboxylic acid |
| TnT | Troponin T |
| TOP2 | Topoisomerase II |
| Top2β | Topoisomerase-II β |
| UGT1A6 | Glucuronosyltransferase family |
| UPLC-QqTOF HRMS | Ultra-performance liquid chromatography quadrupole time-of-flight mass spectrometry |
| VEGF | Vascular endothelial growth factor |
| vWF | Von Willebrand factor |
| 2D | Two-dimensional echocardiography |
| 5-FU | Fluorouracil |
References
- Pritchard-Jones, K.; Bergeron, C.; de Camargo, B.; van den Heuvel-Eibrink, M.M.; Acha, T.; Godzinski, J.; Oldenburger, F.; Boccon-Gibod, L.; Leuschner, I.; Vujanic, G.; et al. Omission of doxorubicin from the treatment of stage II-III, intermediate-risk Wilms’ tumour (SIOP WT 2001): An open-label, non-inferiority, randomised controlled trial. Lancet 2015, 386, 1156–1164. [Google Scholar] [CrossRef]
- Ampatzidou, M.; Kelaidi, C.; Dworzak, M.N.; Polychronopoulou, S. Adolescents and young adults with acute lymphoblastic and acute myeloid leukemia. MEMO-Mag. Eur. Med. Oncol. 2018, 11, 47–53. [Google Scholar]
- Ampatzidou, M.; Panagiotou, J.P.; Paterakis, G.; Papadakis, V.; Papadimitriou, S.I.; Parcharidou, A.; Papargyri, S.; Rigatou, E.; Avgerinou, G.; Tsitsikas, K.; et al. Childhood acute lymphoblastic leukemia: 12 years of experience, using a Berlin-Frankfurt-Münster approach, in a Greek center. Leuk. Lymphoma 2015, 56, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Polychronopoulou, S.; Baka, M.; Servitzoglou, M.; Papadakis, V.; Pourtsidis, A.; Avgerinou, G.; Abatzidou, M.; Kosmidis, H. Treatment and clinical results in childhood AML in Greece. MEM-Mag. Eur. Med. Oncol. 2014, 7, 50–55. [Google Scholar] [CrossRef]
- Georgakis, M.K.; Karalexi, M.A.; Agius, D.; Antunes, L.; Bastos, J.; Coza, D.; Demetriou, A.; Dimitrova, N.; Eser, S.; Florea, M.; et al. Incidence and time trends of childhood lymphomas: Findings from 14 Southern and Eastern European cancer registries and the Surveillance, Epidemiology and End Results, USA. Cancer Causes Control 2016, 27, 1381–1394. [Google Scholar] [CrossRef]
- Petridou, E.T.; Dimitrova, N.; Eser, S.; Kachanov, D.; Karakilinc, H.; Varfolomeeva, S.; Belechri, M.; Baka, M.; Moschovi, M.; Polychronopoulou, S.; et al. Childhood leukemia and lymphoma: Time trends and factors affecting survival in five Southern and Eastern European Cancer Registries. Cancer Causes Control 2013, 24, 1111–1118. [Google Scholar] [CrossRef]
- Lyon, A.R.; López-Fernández, T.; Couch, L.S.; Asteggiano, R.; Aznar, M.C.; Bergler-Klein, J.; Boriani, G.; Cardinale, D.; Cordoba, R.; Cosyns, B.; et al. 2022 ESC Guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur. Heart J. 2022, 43, 4229–4361. [Google Scholar]
- Herrmann, J.; Lenihan, D.; Armenian, S.; Barac, A.; Blaes, A.; Cardinale, D.; Carver, J.; Dent, S.; Ky, B.; Lyon, A.R.; et al. Defining cardiovascular toxicities of cancer therapies: An International Cardio-Oncology Society (IC-OS) consensus statement. Eur. Heart J. 2022, 43, 280–299. [Google Scholar] [CrossRef]
- Chow, E.J.; Leger, K.J.; Bhatt, N.S.; Mulrooney, D.A.; Ross, C.J.; Aggarwal, S.; Bansal, N.; Ehrhardt, M.J.; Armenian, S.H.; Scott, J.M.; et al. Paediatric cardio-oncology: Epidemiology, screening, prevention, and treatment. Cardiovasc. Res. 2019, 115, 922–934. [Google Scholar] [CrossRef]
- Morelli, M.B.; Bongiovanni, C.; Da Pra, S.; Miano, C.; Sacchi, F.; Lauriola, M.; D’Uva, G. Cardiotoxicity of Anticancer Drugs: Molecular Mechanisms and Strategies for Cardioprotection. Front. Cardiovasc. Med. 2022, 9, 847012, PMCID:PMC9051244. [Google Scholar] [CrossRef] [PubMed]
- Lipshultz, S.E.; Lipshultz, E.R.; Chow, E.J.; Doody, D.R.; Armenian, S.H.; Asselin, B.L.; Baker, K.S.; Bhatia, S.; Constine, L.S.; Freyer, D.R.; et al. Cardiometabolic Risk in Childhood Cancer Survivors: A Report from the Children’s Oncology Group. Cancer Epidemiol. Biomark. Prev. 2022, 31, 536–542. [Google Scholar] [CrossRef] [PubMed]
- Ward, E.; DeSantis, C.; Robbins, A.; Kohler, B.; Jemal, A. Childhood and adolescent cancer statistics, 2014. CA Cancer J. Clin. 2014, 64, 83–103. [Google Scholar] [CrossRef] [PubMed]
- Mulrooney, D.A.; Yeazel, M.W.; Kawashima, T.; Mertens, A.C.; Mitby, P.; Stovall, M.; Donaldson, S.S.; Green, D.M.; Sklar, C.A.; Robison, L.L.; et al. Cardiac outcomes in a cohort of adult survivors of childhood and adolescent cancer: Retrospective analysis of the Childhood Cancer Survivor Study cohort. BMJ 2009, 339, b4606. [Google Scholar] [CrossRef] [PubMed]
- Bansal, N.; Amdani, S.; Lipshultz, E.R.; Lipshultz, S.E. Chemotherapy-induced cardiotoxicity in children. Expert Opin. Drug Metab. Toxicol. 2017, 13, 817–832. [Google Scholar] [CrossRef]
- Minotti, G.; Menna, P.; Salvatorelli, E.; Cairo, G.; Gianni, L. Anthracyclines: Molecular advances and pharmacologic developments in antitumor activity and cardiotoxicity. Pharmacol. Rev. 2004, 56, 185–229. [Google Scholar] [CrossRef]
- Sawyer, D.B.; Peng, X.; Chen, B.; Pentassuglia, L.; Lim, C.C. Mechanisms of anthracycline cardiac injury: Can we identify strategies for cardioprotection? Prog. Cardiovasc. Dis. 2010, 53, 105–113. [Google Scholar] [CrossRef]
- Simbre, V.C.; Duffy, S.A.; Dadlani, G.H.; Miller, T.L.; Lipshultz, S.E. Cardiotoxicity of cancer chemotherapy: Implications for children. Paediatr. Drugs 2005, 7, 187–202. [Google Scholar] [CrossRef]
- Herrmann, J.; Lerman, A.; Sandhu, N.P.; Villarraga, H.R.; Mulvagh, S.L.; Kohli, M. Evaluation and management of patients with heart disease and cancer: Cardio-oncology. Mayo Clin. Proc. 2014, 89, 1287–1306. [Google Scholar] [CrossRef]
- Sayed-Ahmed, M.M.; Aldelemy, M.L.; Al-Shabanah, O.A.; Hafez, M.M.; Al-Hosaini, K.A.; Al-Harbi, N.O.; Al-Sharary, S.D.; Al-Harbi, M.M. Inhibition of gene expression of carnitine palmitoyltransferase I and heart fatty acid binding protein in cyclophosphamide and ifosfamide-induced acute cardiotoxic rat models. Cardiovasc. Toxicol. 2014, 14, 232–242. [Google Scholar] [CrossRef]
- Rhea, I.B.; Oliveira, G.H. Cardiotoxicity of Novel Targeted Chemotherapeutic Agents. Curr. Treat. Options Cardiovasc. Med. 2018, 20, 53. [Google Scholar] [CrossRef]
- Zhang, K.; Heidrich, F.M.; DeGray, B.; Boehmerle, W.; Ehrlich, B.E. Paclitaxel accelerates spontaneous calcium oscillations in cardiomyocytes by interacting with NCS-1 and the InsP3R. J. Mol. Cell. Cardiol. 2010, 49, 829–835. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K.; Inukai, T.; Imamura, T.; Yano, M.; Tomoyasu, C.; Lucas, D.M.; Nemoto, A.; Sato, H.; Huang, M.; Abe, M.; et al. Anti-leukemic activity of bortezomib and carfilzomib on B-cell precursor ALL cell lines. PLoS ONE 2017, 12, e0188680. [Google Scholar] [CrossRef] [PubMed]
- Shah, C.; Bishnoi, R.; Jain, A.; Bejjanki, H.; Xiong, S.; Wang, Y.; Zou, F.; Moreb, J.S. Cardiotoxicity associated with carfilzomib: Systematic review and meta-analysis. Leuk. Lymphoma 2018, 59, 2557–2569. [Google Scholar] [CrossRef] [PubMed]
- Waxman, A.J.; Clasen, S.; Hwang, W.; Garfall, A.; Vogl, D.T.; Carver, J.; O’Quinn, R.; Cohen, A.D.; Stadtmauer, E.A.; Ky, B.; et al. Carfilzomib-Associated Cardiovascular Adverse Events: A Systematic Review and Meta-analysis. JAMA Oncol. 2018, 4, e174519. [Google Scholar] [CrossRef] [PubMed]
- Rochette, L.; Guenancia, C.; Gudjoncik, A.; Hachet, O.; Zeller, M.; Cottin, Y.; Vergely, C. Anthracyclines/trastuzumab: New aspects of cardiotoxicity and molecular mechanisms. Trends Pharmacol. Sci. 2015, 36, 326–348. [Google Scholar] [CrossRef] [PubMed]
- Lipshultz, S.E.; Karnik, R.; Sambatakos, P.; Franco, V.I.; Ross, S.W.; Miller, T.L. Anthracycline-related cardiotoxicity in childhood cancer survivors. Curr. Opin. Cardiol. 2014, 29, 103–112. [Google Scholar] [CrossRef]
- Manrique, C.R.; Park, M.; Tiwari, N.; Plana, J.C.; Garcia, M.J. Diagnostic strategies for early recognition of cancer therapeutics-related cardiac dysfunction. Clin. Med. Insights Cardiol. 2017, 11, 1179546817697983. [Google Scholar] [CrossRef]
- Von Hoff, D.D.; Layard, M.W.; Basa, P.; Davis, H.L., Jr.; Von Hoff, A.L.; Rozencweig, M.; Muggia, F.M. Risk factors for doxorubicin-induced congestive heart failure. Ann. Intern. Med. 1979, 91, 710–717. [Google Scholar] [CrossRef]
- Vandecruys, E.; Mondelaers, V.; De Wolf, D.; Benoit, Y.; Suys, B. Late cardiotoxicity after low dose of anthracycline therapy for acute lymphoblastic leukemia in childhood. J. Cancer Surviv. 2012, 6, 95–101. [Google Scholar] [CrossRef]
- Nysom, K.; Holm, K.; Lipsitz, S.R.; Mone, S.M.; Co-lan, S.D.; Orav, E.J.; Sallan, S.E.; Olsen, J.H.; Hertz, H.; Jacobsen, J.R.; et al. Relationship between cumulative anthracycline dose and late cardiotoxicity in childhood acute lymphoblastic leukemia. J. Clin. Oncol. 1998, 16, 545–550. [Google Scholar] [CrossRef]
- Lipshultz, S.E.; Adams, M.J. Cardiotoxicity after childhood cancer: Beginning with the end in mind. J. Clin. Oncol. 2010, 28, 1276–1281. [Google Scholar] [CrossRef] [PubMed]
- Van der Pal, H.J.; van Dalen, E.C.; Hauptmann, M.; Kok, W.E.; Caron, H.N.; van den Bos, C.; Ol-Denburger, F.; Koning, C.C.; van Leeuwen, F.E.; Kremer, L.C. Cardiac function in 5-year survivors of childhood cancer: A long-term follow-up study. Arch. Intern. Med. 2010, 170, 1247–1255. [Google Scholar] [CrossRef] [PubMed]
- Brickler, M.; Raskin, A.; Ryan, T.D. Current State of Pediatric Cardio-Oncology: A Review. Children 2022, 9, 127. [Google Scholar] [CrossRef] [PubMed]
- Loar, R.W.; Noel, C.V.; Tunuguntla, H.; Colquitt, J.L.; Pignatelli, R.H. State of the art review: Chemotherapy-induced cardiotoxicity in children. Congenit. Heart Dis. 2018, 13, 5–15. [Google Scholar] [CrossRef]
- Mornoş, C.; Manolis, A.J.; Cozma, D.; Kouremenos, N.; Zacharopoulou, I.; Ionac, A. The value of left ventricular global longitudinal strain assessed by three-dimensional strain imaging in the early detection of anthracyclinemediated cardiotoxicity. Hellenic. J. Cardiol. 2014, 55, 235–244. [Google Scholar]
- Lipshultz, S.E.; Miller, T.L.; Scully, R.E.; Lipsitz, S.R.; Rifai, N.; Silverman, L.B.; Colan, S.D.; Neuberg, D.S.; Dahlberg, S.E.; Henkel, J.M.; et al. Changes in cardiac biomarkers during doxorubicin treatment of pediatric patients with high-risk acute lymphoblastic leukemia: Associations with long-term echocardiographic outcomes. J. Clin. Oncol. 2012, 30, 1042–1049. [Google Scholar] [CrossRef]
- Dixon, S.B.; Howell, C.R.; Lu, L.; Plana, J.C.; Joshi, V.M.; Luepker, R.V.; Durand, J.B.; Ky, B.; Lenihan, D.J.; Jefferies, J.L.; et al. Cardiac biomarkers and association with subsequent cardiomyopathy and mortality among adult survivors of childhood cancer: A report from the St. Jude Lifetime Cohort. Cancer 2021, 127, 458–466. [Google Scholar] [CrossRef]
- Sherief, L.M.; Kamal, A.G.; Khalek, E.A.; Kamal, N.M.; Soliman, A.A.; Esh, A.M. Biomarkers and early detection of late onset anthracycline-induced cardiotoxicity in children. Hematology 2012, 17, 151–156. [Google Scholar] [CrossRef]
- Armenian, S.H.; Gelehrter, S.K.; Vase, T.; Venkatramani, R.; Landier, W.; Wilson, K.D.; Herrera, C.; Reichman, L.; Menteer, J.D.; Mascarenhas, L.; et al. Screening for cardiac dysfunction in anthracycline-exposed childhood cancer survivors. Clin. Cancer Res. 2014, 20, 6314–6323. [Google Scholar] [CrossRef]
- Lam, E.; Higgins, V.; Zhang, L.; Chan, M.K.; Bohn, M.K.; Trajcevski, K.; Liu, P.; Adeli, K.; Nathan, P.C. Normative Values of High-Sensitivity Cardiac Troponin T and N-Terminal pro-B-Type Natriuretic Peptide in Children and Adolescents: A Study from the CALIPER Cohort. J. Appl. Lab. Med. 2021, 6, 344–353. [Google Scholar] [CrossRef]
- Joolharzadeh, P.; Rodriguez, M.; Zaghlol, R.; Pedersen, L.N.; Jimenez, J.; Bergom, C.; Mitchell, J.D. Recent Advances in Serum Biomarkers for Risk Stratification and Patient Management in Cardio-Oncology. Curr. Cardiol. Rep. 2023, 25, 133–146. [Google Scholar] [CrossRef] [PubMed]
- Christensona, E.S.; Jamesa, T.; Agrawala, V.; ParkbaJohns, B.H. Use of biomarkers for the assessment of chemotherapy-induced cardiac toxicity. Curr. Heart Fail. Rep. 2015, 12, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Cardinale, D.; Biasillo, G.; Salvatici, M.; Sandri, M.T.; Cipolla, C.M. Using biomarkers to predict and to prevent cardiotoxicity of cancer therapy. Expert Rev. Mol. Diagn. 2017, 17, 245–256. [Google Scholar] [CrossRef] [PubMed]
- Horacek, J.M.; Jebavy, L.; Vasatova, M.; Pudil, R.; Tichy, M.; Jakl, M.; Maly, J. Glycogen phosphorylase BB as a potential marker of cardiac toxicity in patients treated with anthracyclines for acute leukemia. Bratisl. Lek. Listy. 2013, 114, 708–710. [Google Scholar] [CrossRef] [PubMed]
- Horacek, J.M.; Vasatova, M.; Tichy, M.; Pudil, R.; Jebavy, L.; Maly, J. The use of cardiac biomarkers in detection of cardiotoxicity associated with conventional and high-dose chemotherapy for acute leukemia. Exp. Oncol. 2010, 32, 97–99. [Google Scholar]
- Horacek, J.M.; Tichy, M.; Jebavy, L.; Pudil, R.; Ulrychova, M. Maly Use of multiple biomarkers for evaluation of anthracycline-induced cardiotoxicity in patients with acute myeloid leukemia. J. Exp. Oncol. 2008, 30, 157–159. [Google Scholar]
- Horacek, J.M.; Vasatova, M.; Pudil, R.; Tichy, M.; Zak, P.; Jakl, M.; Jebavy, L.; Maly, J. Biomarkers for the early detection of anthracycline-induced cardiotoxicity: Current status. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc. Czech. Repub. 2014, 158, 511–517. [Google Scholar] [CrossRef]
- Cao, L.; Zhu, W.; Wagar, E.A.; Meng, Q.H. Biomarkers for monitoring chemotherapy-induced cardiotoxicity. Crit. Rev. Clin. Lab. Sci. 2017, 54, 87–101. [Google Scholar] [CrossRef]
- Arslan, D.; Cihan, T.; Kose, D.; Vatansev, H.; Cimen, D.; Koksal, Y.; Oran, B.; Akyurek, F. Growth-differentiation factor-15 and tissue doppler ımaging in detection of asymptomatic anthracycline cardiomyopathy in childhood cancer survivors. Clin. Biochem. 2013, 46, 1239–1243. [Google Scholar] [CrossRef]
- Armenian, S.; Bhatia, S. Predicting and Preventing Anthracycline-Related Cardiotoxicity. Am. Soc. Clin. Oncol. Educ. Book 2018, 38, 3–12. [Google Scholar] [CrossRef]
- Aminkeng, F.; Bhavsar, A.P.; Visscher, H.; Rassekh, S.R.; Li, Y.; Lee, J.W.; Brunham, L.R.; Caron, H.N.; van Dalen, E.C.; Kremer, L.C.; et al. Canadian Pharmacogenomics Network for Drug Safety Consortium. A coding variant in RARG confers susceptibility to anthracycline-induced cardiotoxicity in childhood cancer. Nat. Genet. 2015, 47, 1079–1084. [Google Scholar] [CrossRef] [PubMed]
- Madonna, R. Early diagnosis and prediction of anticancer drug-induced cardiotoxicity: From cardiac imaging to “Omics” technologies. Rev. Espanol. Cardiol. 2017, 70, 576–582. [Google Scholar] [CrossRef]
- Linschoten, M.; Teske, A.J.; Cramer, M.J.; van der Wall, E.; Asselbergs, F.W. Chemotherapy-Related Cardiac Dysfunction: A Systematic Review of Genetic Variants Modulating Individual Risk. Circ. Genom. Precis. Med. 2018, 11, e001753. [Google Scholar] [CrossRef] [PubMed]
- Semsei, A.F.; Erdelyi, D.J.; Ungvari, I.; Csagoly, E.; Hegyi, M.Z.; Kiszel, P.S.; Lautner-Csorba, O.; Szabolcs, J.; Masat, P.; Fekete, G.; et al. ABCC1 polymorphisms in anthracycline- induced cardiotoxicity in childhood acute lymphoblastic leukaemia. Cell Biol. Int. 2012, 36, 79–86. [Google Scholar] [CrossRef]
- Wojnowski, L.; Kulle, B.; Schirmer, M.; Schlüter, G.; Schmidt, A.; Rosenberger, A.; Vonhof, S.; Bickeböller, H.; Toliat, M.R.; Suk, E.K.; et al. NAD(P)H oxidase and multidrug resistance protein genetic polymorphisms are associated with doxorubicin-induced cardiotoxicity. Circulation 2005, 112, 3754–3762. [Google Scholar] [CrossRef] [PubMed]
- Vulsteke, C.; Pfeil, A.M.; Maggen, C.; Schwenkglenks, M.; Pettengell, R.; Szucs, T.D.; Lambrechts, D.; Dieudonné, A.-S.; Hatse, S.; Neven, P.; et al. Clinical and genetic risk factors for epirubicin-induced cardiac toxicity in early breast cancer patients. Breast Cancer Res. Treat. 2015, 152, 67–76. [Google Scholar] [CrossRef]
- Blanco, J.G.; Leisenring, W.M.; Gonzalez-Covarrubias, V.M.; Kawashima, T.I.; Davies, S.M.; Relling, M.V.; Robison, L.L.; Sklar, C.A.; Stovall, M.; Bhatia, S. Genetic polymorphisms in the carbonyl reductase 3 gene CBR3 and the NAD(P)H: Quinone oxidoreductase 1 gene NQO1 in patients who developed anthracycline-related congestive heart failure after childhood cancer. Cancer 2008, 112, 2789–2795. [Google Scholar] [CrossRef]
- Blanco, J.G.; Sun, C.L.; Landier, W.; Chen, L.; Esparza-Duran, D.; Leisenring, W.; Mays, A.; Friedman, D.L.; Ginsberg, J.P.; Hudson, M.M.; et al. Anthracycline-related cardiomyopathy after childhood cancer: Role of polymorphisms in carbonyl reductase genes—A report from the Children’s Oncology Group. J. Clin. Oncol. 2012, 30, 1415–1421. [Google Scholar] [CrossRef]
- Wang, X.; Sun, C.-L.; Quiñones-Lombraña, A.; Singh, P.; Landier, W.; Hageman, L.; Mather, M.; Rotter, J.I.; Taylor, K.D.; Chen, Y.-D.I.; et al. CELF4 variant and anthracycline-related cardiomyopathy: A Children’s Oncology Group genome-wide association study. J. Clin. Oncol. 2016, 34, 863–870. [Google Scholar] [CrossRef]
- Vos, H.I.; Coenen, M.J.; Guchelaar, H.J.; Te Loo, D.M. The role of pharmacogenetics in the treatment of osteosarcoma. Drug Discov. Today 2016, 21, 1775–1786. [Google Scholar] [CrossRef]
- Leong, S.L.; Chaiyakunapruk, N.; Lee, S.W. Candidate Gene Association Studies of Anthracycline-induced Cardiotoxicity: A Systematic Review and Meta-analysis. Sci. Rep. 2017, 7, 39. [Google Scholar] [CrossRef] [PubMed]
- McOwan, T.N.; Craig, L.A.; Tripdayonis, A.; Karavendzas, K.; Cheung, M.M.; Porrello, E.R.; Conyers, R.; Elliott, D.A. Evaluating anthracycline cardiotoxicity associated single nucleotide polymorphisms in a paediatric cohort with early onset cardiomyopathy. Cardiooncology 2020, 6, 5. [Google Scholar] [CrossRef] [PubMed]
- Petrykey, K.; Andelfinger, G.U.; Laverdière, C.; Sinnett, D.; Krajinovic, M. Genetic factors in anthracycline-induced cardiotoxicity in patients treated for pediatric cancer. Expert Opin. Drug Metab. Toxicol. 2020, 16, 865–883. [Google Scholar] [CrossRef] [PubMed]
- Lipshultz, S.E.; Lipsitz, S.R.; Kutok, J.L.; Miller, T.L.; Colan, S.D.; Neuberg, D.S.; Stevenson, K.E.; Fleming, M.D.; Sallan, S.E.; Franco, V.I.; et al. Impact of hemochromatosis gene mutations on cardiac status in doxorubicin-treated survivors of childhood high-risk leukemia. Cancer 2013, 119, 3555–3562. [Google Scholar] [CrossRef]
- Visscher, H.; Ross, C.J.D.; Rassekh, S.R.; Sandor, G.S.S.; Caron, H.N.; van Dalen, E.C.; Kremer, L.C.; van der Pal, H.J.; Rogers, P.C.; Rieder, M.J.; et al. Validation of Variants in SLC28A3 and UGT1A6 as Genetic Markers Predictive of Anthracycline-Induced Cardiotoxicity in Children. Pediatr. Blood Cancer 2013, 60, 1375–1381. [Google Scholar] [CrossRef]
- Visscher, H.; Ross, C.J.D.; Rassekh, S.R.; Sandor, G.S.S.; Caron, H.N.; van Dalen, E.C.; Kremer, L.C.; van der Pal, H.J.; Rogers, P.C.; Rieder, M.J.; et al. Genetic variants in SLC22A17 and SLC22A7 are associated with anthracycline- induced cardiotoxicity in children. Pharmacogenomics 2015, 16, 1065–1076. [Google Scholar] [CrossRef]
- Visscher, H.; Ross, C.J.D.; Rassekh, S.R.; Barhdadi, A.; Dube, M.-P.; Al-Saloos, H.; Sandor, S.; Caron, H.N.; van Dalen, E.C.; Kremer, L.C.; et al. Pharmacogenomic Prediction of Anthracycline-Induced Cardiotoxicity in Children. J. Clin. Oncol. 2012, 30, 1422–1428. [Google Scholar] [CrossRef]
- Sági, J.C.; Egyed, B.; Kelemen, A.; Kutszegi, N.; Hegyi, M.; Gézsi, A.; Herlitschke, M.A.; Rzepiel, A.; Fodor, L.E.; Ottóffy, G.; et al. Possible roles of genetic variations in chemotherapy related cardiotoxicity in pediatric acute lymphoblastic leukemia and osteosarcoma. BMC Cancer 2018, 18, 704. [Google Scholar] [CrossRef]
- Aminkeng, F.; Ross, C.J.D.; Rassekh, S.R.; Hwang, S.; Rieder, M.J.; Bhavsar, A.P.; Smith, A.; Sanatani, S.; Gelmon, K.A.; Bernstein, D.; et al. Recommendations for genetic testing to reduce the incidence of anthracycline-induced cardiotoxicity. Br. J. Clin. Pharmacol. 2016, 82, 683–695. [Google Scholar] [CrossRef]
- Marcoux, S.; Drouin, S.; Laverdière, C.; Alos, N.; Andelfinger, G.U.; Bertout, L.; Curnier, D.; Friedrich, M.G.; Kritikou, E.A.; Lefebvre, G.; et al. The PETALE study: Late adverse effects and biomarkers in childhood acute lymphoblastic leukemia survivors. Pediatr. Blood Cancer 2017, 64. [Google Scholar] [CrossRef]
- Kashyap, V.; Laursen, K.B.; Brenet, F.; Viale, A.J.; Scandura, J.M.; Gudas, L.J. RARgamma is essential for retinoic acid induced chromatin remodeling and transcriptional activation in embryonic stem cells. J. Cell. Sci. 2013, 126, 999–1008. [Google Scholar] [PubMed]
- Krajinovic, M.; Elbared, J.; Drouin, S.; Bertout, L.; Rezgui, A.; Ansari, M.; Raboisson, M.-J.; Lipshultz, S.E.; Silverman, L.B.; Sallan, S.E.; et al. Polymorphisms of ABCC5 and NOS3 genes influence doxorubicin cardiotoxicity in survivors of childhood acute lymphoblastic leukemia. Pharm. J. 2015, 16, 530–535. [Google Scholar]
- Oatmen, K.E.; Toro-Salazar, O.H.; Hauser, K.; Zellars, K.N.; Mason, K.C.; Hor, K.; Gillan, E.; Zeiss, C.J.; Gatti, D.M.; Spinale, F.G. Identification of a Novel microRNA Profile in Pediatric Patients with Cancer Treated with Anthracycline Chemotherapy. Am. J. Physiol. Heart Circ. Physiol. 2018, 315, H1443–H1452. [Google Scholar] [CrossRef] [PubMed]
- Oliveira-Carvalho, V.; Ferreira, L.R.P.; Bocchi, E.A. Circulating mir-208a fails as a biomarker of doxorubicin-induced cardiotoxicity in breast cancer patients. J. Appl. Toxicol. 2015, 35, 1071–1072. [Google Scholar] [CrossRef] [PubMed]
- Oikonomou, E.; Siasos, G.; Tousoulis, D.; Kokkou, E.; Genimata, V.; Zisimos, K.; Latsios, G.; Stefanadis, C. Diagnostic, and therapeutic potentials of microRNAs in heart failure. Curr. Top. Med. Chem. 2013, 13, 1548–1558. [Google Scholar] [CrossRef] [PubMed]
- Papageorgiou, N.; Tousoulis, D.; Androulakis, E.; Siasos, G.; Briasoulis, A.; Vogiatzi, G.; Kampoli, A.M.; Tsiamis, E.; Tentolouris, C.; Stefanadis, C. The role of microRNAs in cardiovascular disease. Curr. Med. Chem. 2012, 19, 2605–2610. [Google Scholar] [CrossRef]
- Ruggeri, C.; Gioffre, S.; Achilli, F.; Colombo, G.I.; D’Alessandra, Y. Role of microRNAs in doxorubicin-induced cardiotoxicity: An overview of preclinical models and cancer patients. Heart Fail. Rev. 2018, 23, 109–122. [Google Scholar] [CrossRef]
- Holmgren, G.; Synnergren, J.; Andersson, C.X.; Lindahl, A.; Sartipy, P. MicroRNAs as potential biomarkers for doxorubicininduced cardiotoxicity. Toxicol. Vitr. 2016, 34, 26–34. [Google Scholar] [CrossRef]
- Ludwig, N.; Leidinger, P.; Becker, K.; Backes, C.; Fehlmann, T.; Pallasch, C.; Rheinheimer, S.; Meder, B.; Stähler, C.; Meese, E.; et al. Distribution of miRNA expression across human tissues. Nucleic Acids Res. 2016, 44, 3865–3877. [Google Scholar] [CrossRef]
- Skála, M.; Hanousková, B.; Skálová, L.; Matoušková, P. MicroRNAs in the diagnosis and prevention of drug-induced Cardiotoxicity. Arch. Toxicol. 2019, 93, 1–9. [Google Scholar] [CrossRef]
- Zhou, S.-S.; Jin, J.-P.; Wang, J.-Q.; Zhang, Z.-G.; Freedman, J.H.; Zheng, Y.; Cai, L. miRNAS in cardiovascular diseases: Potential biomarkers, therapeutic targets and challenges. Acta Pharmacol. Sin. 2018, 39, 1073–1084. [Google Scholar] [CrossRef]
- Pellegrini, L.; Sileno, S.; D’Agostino, M.; Foglio, E.; Florio, M.C.; Guzzanti, V.; Russo, M.A.; Limana, F.; Magenta, A. MicroRNAs in Cancer Treatment-Induced Cardiotoxicity. Cancers 2020, 12, 704. [Google Scholar] [CrossRef] [PubMed]
- Kuwabara, Y.; Ono, K.; Horie, T.; Nishi, H.; Nagao, K.; Kinoshita, M.; Watanabe, S.; Baba, O.; Kojima, Y.; Shizuta, S.; et al. Increased MicroRNA-1 and MicroRNA-133a levels in serum of patients with cardiovascular disease indicate myocardial damage. Circ. Cardiovasc. Genet. 2011, 4, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Rigaud, V.O.C.; Ferreira, L.R.P.; Ayub-Ferreira, S.M.; Ávila, M.S.; Brandão, S.M.G.; Cruz, F.D.; Santos, M.H.H.; Cruz, C.B.B.V.; Alves, M.S.L.; Issa, V.S.; et al. Circulating miR-1 as a potential biomarker of doxorubicin-induced cardiotoxicity in breast cancer patients. Oncotarget 2017, 8, 6994–7002. [Google Scholar] [CrossRef] [PubMed]
- Leger, K.J.; Leonard, D.; Nielson, D.; de Lemos, J.A.; Mammen, P.P.; Winick, N.J. Circulating microRNAs: Potential Markers of Cardiotoxicity in Children and Young Adults Treated with Anthracycline Chemotherapy. J. Am. Heart Assoc. 2017, 6, e004653. [Google Scholar] [CrossRef]
- Kumar, S.N.; Konorev, E.A.; Aggarwal, D.; Kalyanaraman, B. Analysis of Proteome Changes in Doxorubicin-Treated Adult Rat Cardiomyocyte. J. Proteom. 2011, 74, 683–697. [Google Scholar] [CrossRef] [PubMed]
- Creemers, E.E.; Tijsen, A.J.; Pinto, Y.M. Circulating microRNAs: Novel biomarkers and extracellular communicators in cardiovascular disease? Circ. Res. 2012, 110, 483–495. [Google Scholar] [CrossRef]
- Todorova, V.K.; Makhoul, I.; Wei, J.N.; Klimberg, V.S. Circulating miRNA profiles of doxorubicin-induced cardiotoxicity in breast cancer patients. Ann. Clin. Lab. Sci. 2017, 47, 115–119. [Google Scholar]
- Zhao, Z.Y.; He, J.; Zhang, J.; Liu, M.; Yang, S.; Li, N.; Li, X. Dysregulated miR1254 and miR579 for cardiotoxicity in patients treated with bevacizumab in colorectal cancer. Tumor. Biol. 2014, 35, 5227–5235. [Google Scholar] [CrossRef]
- Petricoin, E.F.; Rajapaske, V.; Herman, E.H.; Arekani, A.M.; Ross, S.; Johann, D.; Knapton, A.; Zhang, J.; Hitt, B.A.; Conrads, T.P.; et al. Toxicoproteomics: Serum Proteomic Pattern Diagnostics for Early Detection of Drug Induced Cardiac Toxicities and Cardioprotection. Toxicol. Pathol. 2004, 32 (Suppl. S1), 122–130. [Google Scholar] [CrossRef]
- Ohyama, K.; Tomonari, M.; Ichibangase, T.; To, H.; Kishikawa, N.; Nakashima, K.; Imai, K.; Kuroda, N. A Toxicoproteomic Study on Cardioprotective Effects of Pre-Administration of Docetaxel in a Mouse Model of Adriamycin-Induced Cardiotoxicity. Biochem. Pharmacol. 2010, 80, 540–547. [Google Scholar] [CrossRef]
- Desai, V.G.; Lee, T.; Moland, C.L.; Vijay, V.; Han, T.; Lewis, S.M.; Herman, E.H.; Fuscoe, J.C. Candidate Early Predictive Plasma Protein Markers of Doxorubicin-Induced Chronic Cardiotoxicity in B6C3F 1 Mice. Toxicol. Appl. Pharmacol. 2019, 363, 164–173. [Google Scholar] [CrossRef] [PubMed]
- Yarana, C.; Carroll, D.; Chen, J.; Chaiswing, L.; Zhao, Y.; Noel, T.; Alstott, M.; Bae, Y.; Dressler, E.V.; Moscow, J.A.; et al. Extracellular Vesicles Released by Cardiomyocytes in a Doxorubicin-Induced Cardiac Injury Mouse Model Contain Protein Biomarkers of Early Cardiac Injury. Clin. Cancer Res. 2018, 24, 1644–1653. [Google Scholar] [CrossRef] [PubMed]
- Claudino, W.M.; Goncalves, P.H.; di Leo, A.; Philip, P.A.; Sarkar, F.H. Metabolomics in cancer: A bench-to-bedside intersection. Crit. Rev. Oncol. Hematol. 2012, 84, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.H.; Ivanisevic, J.; Siuzdak, G. Metabolomics: Beyond biomarkers and towards mechanisms. Nat. Rev. Mol. Cell. Biol. 2016, 17, 451–459. [Google Scholar] [CrossRef]
- Lewis, G.D.; Asnani, A.; Gerszten, R.E. Application of metabolomics to cardiovascular biomarker and pathway discovery. J. Am. Coll. Cardiol. 2008, 52, 117–123. [Google Scholar] [CrossRef]
- Deidda, M.; Mercurio, V.; Cuomo, A.; Noto, A.; Mercuro, G.; Cadeddu Dessalvi, C. Metabolomic Perspectives in Antiblastic Cardiotoxicity and Cardioprotection. Int. J. Mol. Sci. 2019, 20, 4928. [Google Scholar] [CrossRef]
- Armenian, S.H.; Gelehrter, S.K.; Vase, T.; Venkatramani, R.; Landier, W.; Wilson, K.D.; Herrera, C.; Reichman, L.; Menteer, J.-D.; Mascarenhas, L. Carnitine and cardiac dysfunction in childhood cancer survivors treated with anthracyclines. Cancer Epidemiol. Biomark. Prev. 2014, 23, 1109–1114. [Google Scholar] [CrossRef]
- Li, Y.; Ju, L.; Hou, Z.; Deng, H.; Zhang, Z.; Wang, L.; Yang, Z.; Yin, J.; Zhang, Y. Screening, Verification, and Optimization of Biomarkers for Early Prediction of Cardiotoxicity Based on Metabolomics. J. Proteome Res. 2015, 14, 2437–2445. [Google Scholar] [CrossRef] [PubMed]
- Andreadou, I.; Papaefthimiou, M.; Constantinou, M.; Sigala, F.; Skaltsounis, A.L.; Tsantili-Kakoulidou, A.; Iliodromitis, E.K.; Kremastinos, D.T.; Mikros, E. Metabolomic identification of novel biomarkers in doxorubicin cardiotoxicity and protective eggect of the natural antioxidant oleuropein. NMR Biomed. 2009, 22, 585–592. [Google Scholar]
- Chaudhari, U.; Ellis, J.K.; Wagh, V.; Nemade, H.; Hescheler, J.; Keun, H.C.; Sachinidis, A. Metabolite signatures of doxorubicin induced toxicity in human induced pluripotent stem cell-derived cardiomyocytes. Amino Acids 2017, 49, 1955–1963. [Google Scholar] [CrossRef] [PubMed]
- Schnackenberg, L.K.; Pence, L.; Vijay, V.; Moland, C.L.; George, N.; Cao, Z.; Yu, L.R.; Fuscoe, J.C.; Beger, R.D.; Desai, V.G.J. Early metabolomics changes in heart and plasma during chronic doxorubicin treatment in B6C3F1mice. Appl. Toxicol. 2016, 36, 1486–1495. [Google Scholar] [CrossRef]
- Tan, G.; Lou, Z.; Liao, W.; Zhu, Z.; Dong, X.; Zhang, W.; Chai, W.L. Potential Biomarkers in Mouse Myocardium of Doxorubicin-Induced Cardiomyopathy: A Metabonomic Method and Its Application. PLoS ONE 2011, 6, e27683. [Google Scholar] [CrossRef] [PubMed]
- Jensen, B.C.; Parry, T.L.; Huang, W.; Ilaiwy, A.; Bain, J.R.; Muehlbauer, M.J.; O’Neal, S.K.; Patterson, C.; Johnson, G.L.; Willis, M.S. Non-Targeted Metabolomics Analysis of the Effects of Tyrosine Kinase Inhibitors Sunitinib and Erlotinib on Heart, Muscle, Liver and Serum Metabolism In Vivo. Metabolites 2017, 7, E31. [Google Scholar] [CrossRef]
- Andreadou, I.; Mikros, E.; Ioannidis, K.; Sigala, F.; Naka, K.; Kostidis, S.; Farmakis, D.; Tenta, R.; Kavantzas, N.; Bibli, S.I. Oleuropein prevents doxorubicin-induced cardiomyopathy interfering with signaling molecules and cardiomyocyte metabolism. J. Mol. Cell. Cardiol. 2014, 69, 4–16. [Google Scholar] [CrossRef]
- Geng, C.; Cui, C.; Wang, C.; Lu, S.; Zhang, M.; Chen, D.; Jiang, P. Systematic Evaluations of Doxorubicin-Induced Toxicity in Rats Based on Metabolomics. ACS Omega. 2020, 6, 358–366. [Google Scholar] [CrossRef]
- Tantawy, M.; Chekka, L.M.; Huang, Y.; Garrett, T.J.; Singh, S.; Shah, C.P.; Cornell, R.F.; Baz, R.C.; Fradley, M.G.; Waheed, N.; et al. Lactate Dehydrogenase B and Pyruvate Oxidation Pathway Associated with Carfilzomib-Related Cardiotoxicity in Multiple Myeloma Patients: Result of a Multi-Omics Integrative Analysis. Front. Cardiovasc. Med. 2021, 8, 645122. [Google Scholar] [CrossRef]
- Yin, Y.J.; Xie, J.; Guo, X.; Ju, L.; Li, Y.; Zhang, Y. Plasma metabolic profiling analysis of cyclophosphamide-induced cardiotoxicity using metabolomics coupled with UPLC/Q-TOF-MS and ROC curve. Technol. Biomed. Life Sci. 2016, 1033, 428–435. [Google Scholar] [CrossRef]
- Jensen, B.C.; Parry, T.L.; Huang, W.; Beak, J.Y.; Ilaiwy, A.; Bain, J.R.; Newgard, C.B.; Muehlbauer, M.J.; Patterson, C.; Johnson, G.L.; et al. Effects of the kinase inhibitor sorafenib on heart, muscle, liver, and plasma metabolism in vivo using non-targeted metabolomics analysis. Br. J. Pharmacol. 2017, 174, 4797–4811. [Google Scholar] [CrossRef] [PubMed]
- Park, B.; Sim, S.H.; Lee, K.S.; Kim, H.J.; Park, I.H. Genome-wide association study of genetic variants related to anthracycline-induced cardiotoxicity in early breast cancer. Cancer Sci. 2020, 111, 2579–2587. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Medicine/Cardiotoxicity | Incidence (%) | Arrhythmia | Myocardial Ischemia | Vascular Toxicity | Heart Failure | QT Prolongation | Arterial Hypertension |
|---|---|---|---|---|---|---|---|
| Anthracyclines | |||||||
| Doxorubicin | 3–26 | xxx | x | NE | xxx | NE | x |
| Doxorubicin Liposomal | 2 | x | xx | NE | x | NE | x |
| Epirubicin | 0.9–3.3 | x | x | NE | x | NE | x |
| Daunorubicin | xx | x | NE | x | NE | x | |
| Idarubicin | 5–18 | xxx | x | NE | xx | NE | x |
| Antibiotics | |||||||
| Mitoxantrone | 0.2–30 | xxx | xx | NE | xx | NE | xx |
| Mitomycin-c | 10 | xx | xx | NE | xx | NE | |
| Monoclonal antibodies | |||||||
| Trastuzumab | 1.7–8 | xx | x | xx | xxx | NE | xx |
| Bevacizumab | 1.6–4 | xx | xx | xxx | xx | NE | xx |
| Pertuzumab | 0.7–1.2 | x | x | x | xx | NE | x |
| Dinutuximab beta | NE | xx | NE | xx | NE | xx | |
| Rituximab | x | xx | xxx | x | NE | xx | |
| Tyrosine kinase inhibitors | |||||||
| Dasatinib | 2–4 | xxx | xx | xx | xx | xx | xx |
| Nilotinib | 1 | xx | NE | x | xx | xx | xxx |
| Vermurafenib | xx | xx | xx | x | NE | xx | |
| Sorafenib | 2–28 | x | xx | xx | xx | NE | xx |
| Sunitinib | 2.7–15 | x | xx | xx | xxx | x | xxx |
| Erlotinib | 7–11 | NE | xx | xx | NE | NE | NE |
| Lapatinib | 0.2–1.5 | NE | xx | x | NE | xxx | NE |
| Pazopanib | 7–11 | NE | xx | xx | x | NE | xxx |
| Imatinib | 0.2–2.7 | NE | xxx | xx | xx | NE | NE |
| Proteasome inhibitors | |||||||
| Bortezomib | 2–5 | x | x | x | x | NE | x |
| Carfilzomib | 11–25 | xx | xx | NE | x | NE | x |
| Antimetabolites | |||||||
| 5-fluorouracil | 2–20 | xxx | xxx | NE | x | NE | NE |
| Capecitabine | xxx | xxx | xx | NE | NE | NE | |
| Clofarabine | 27 | NE | |||||
| Alkylating agents | |||||||
| Cyclophosphamide | 7–28 | NE | NE | x | NE | NE | NE |
| Ifosfamide | 0.5–17 | NE | NE | x | xx | NE | NE |
| Cisplatin | rare | NE | NE | xx | NE | NE | NE |
| Antimicrotubule agents | |||||||
| Paclitaxel | <1 | xx | x | NE | x | NE | x |
| Docetaxel | 2.3–13 | xx | xx | NE | x | NE | xx |
| Alkaloids of vinca | |||||||
| Vincristine | 25 | xx | x | NE | NE | xx | x |
| Vinblastine | NE | x | NE | NE | NE | x | |
| Vindesin | NE | NE | NE | NE | NE | NE | |
| Vinorelbin | NE | x | NE | NE | NE | NE |
| Risk Factors Related to Children | Risk Factors Related to Therapy |
|---|---|
hypertension) |
|
| MiRNA | Drug | Modulation | Species | System | References |
|---|---|---|---|---|---|
| miR-1 | Doxorubicin | Increase | Female patients | Plasma | Riguad et al., Oncotarget 2017 [84] |
| miR-1, miR-29b, miR-499 | Anthracyclines | Increase | Children and young adult | Plasma | Leger et al., J Am Heart Assoc. 2017 [85] |
| miR1254 | Bevacizumub | Increase | Humans | Plasma | Zhao et al., Tumour Biol. 2014 [89] |
| miR29 miR499 | Doxorubicin | Increase | Children | Plasma | Oatmen et al., Am J Physiol Heart Circ Physiol, 2018 [73] |
| miR208 | Doxorubicin | Nothing | Female patients | Plasma | Carvalho et al., J Appl Toxicol 2015 [74] |
| Metabolite | Plasma | Stem Cell | Heart | Mice | People | XRT | Medicine | Dose | Biomarker | References |
|---|---|---|---|---|---|---|---|---|---|---|
| Proline | ↓//↑ | ↑ | Yes | No | Cyclophosphamide | 200 mg/kg | Li et al., J Proteome Res, 2015 [99] | |||
| LPC 20:3 | ↓ | Yes | No | Cyclophosphamide | 200 mg/kg | Li et al., J Proteome Res, 2015 [99] | ||||
| Linoleic acid | ↓ | Yes | No | Cyclophosphamide | 200 mg/kg | Li et al., J Proteome Res, 2015 [99] | ||||
| L-carnitine | ↑//↑ | Yes | No | Cyclophosphamide/doxo/isoprotenerol/5-fluorouracil | 200 mg/kg//20 mg/kg//5 mg/kg//125 mg/kg | Li et al., J Proteome Res, 2015 [99] | ||||
| 19-hydroxycorticosterone | ↑//↓ | Yes | No | Cyclophosphamide/doxo/isoprotenerol/5-fluorouracil | 200 mg/kg//20 mg/kg//5 mg/kg//125 mg/kg | Li et al., J Proteome Res, 2015 [99] | ||||
| Phytophingosine | ↓ | Yes | No | Cyclophosphamide | 200 mg/kg | Li et al., J Proteome Res, 2015 [99] | ||||
| Cholid acid | ↓ | Yes | No | Cyclophosphamide | 200 mg/kg | Li et al., J Proteome Res, 2015 [99] | ||||
| LPC 14:0 | ↓//↓ | Yes | No | Cyclophosphamide/doxo/isoprotenerol/5-fluorouracil | 200 mg/kg//20 mg/kg//5 mg/kg//125 mg/kg | Li et al., J Proteome Res, 2015 [99] | ||||
| LPC 18:3 | ↓ | Yes | No | Cyclophosphamide | 200 mg/kg | Li et al., J Proteome Res, 2015 [99] | ||||
| LPC 16:1 | ↓ | Yes | No | Cyclophosphamide | 200 mg/kg | Li et al., J Proteome Res, 2015 [99] | ||||
| LPE 18:2 | ↓ | Yes | No | Cyclophosphamide | 200 mg/kg | Li et al., J Proteome Res, 2015 [99] | ||||
| LPC 22:5 | ↓ | Yes | No | Cyclophosphamide | 200 mg/kg | Li et al., J Proteome Res, 2015 [99] | ||||
| LPC 22:6 | ↓ | Yes | No | Cyclophosphamide | 200 mg/kg | Li et al., J Proteome Res, 2015 [99] | ||||
| LPC 22:4 | ↓ | Yes | No | Cyclophosphamide | 200 mg/kg | Li et al., J Proteome Res, 2015 [99] | ||||
| LPC 20:2 | ↓//↓ | Yes | No | Cyclophosphamide/doxo/isoprotenerol/5-fluorouracil | 200 mg/kg//20 mg/kg//5 mg/kg//125 mg/kg | Li et al., J Proteome Res, 2015 [99] | ||||
| PLE 20:3 | ↓ | Yes | No | Cyclophosphamide | 200 mg/kg | Li et al., J Proteome Res, 2015 [99] | ||||
| Pyruvate | ↑ | Doxorubicin | 20 mg/kg | Troponin T LDH | Andreadou et al., ΝΜR Biomed, 2009 [100] /Chaudhari et al., Amino Acids 2017 [101] | |||||
| Acetate | ↑ | ↑ | Yes | Doxorubicin | 20 mg/kg | Troponin T LDH | Andreadou et al., ΝΜR Biomed, 2009 [100] /Chaudhari et al., Amino Acids 2017 [101] | |||
| Formate | ↑ | Doxorubicin | 20 mg/kg | Troponin T LDH | Andreadou et al., ΝΜR Biomed, 2009 [100] /Chaudhari et al., Amino Acids 2017 [101] | |||||
| Succinate | ↑ | ↑ | Yes | Doxorubicin | 20 mg/kg | Troponin T LDH | Andreadou et al., ΝΜR Biomed, 2009 [100] /Chaudhari et al., Amino Acids 2017 [101] | |||
| Lactate | ↑//↑ | ↓ | Yes | Doxorubicin | 20 mg/kg | Troponin T | Andreadou et al., ΝΜR Biomed, 2009 [100] | |||
| Alanine | ↑//↑ | ↑//↑ | Yes | Doxorubicin | 20 mg/kg | Troponin T | Andreadou et al., ΝΜR Biomed, 2009 [100] | |||
| Glutamine | ↑ | ↓ | Yes | Doxorubicin | 20 mg/kg | Troponin T | Andreadou et al., ΝΜR Biomed, 2009 [100] | |||
| Glutamate | ↑ | no | Yes | ↑ | Doxorubicin | 20 mg/kg | Troponin T | Andreadou et al., ΝΜR Biomed, 2009 [100] | ||
| Creatine | no | Yes | Doxorubicin | 20 mg/kg | Troponin T | Andreadou et al., ΝΜR Biomed, 2009 [100] | ||||
| Taurine | no | Yes | ↓ | Doxorubicin | 20 mg/kg | Troponin T | Andreadou et al., ΝΜR Biomed, 2009 [100] | |||
| Valine | ↑ | ↓ | Yes | ↑ | Doxorubicin | 20 mg/kg | Troponin T | Andreadou et al., ΝΜR Biomed, 2009 [100] | ||
| Leuline | ↑ | ↓ | Yes | Doxorubicin | 20 mg/kg | Troponin T | Andreadou et al., ΝΜR Biomed, 2009 [100] | |||
| Isoleukine | ↑ | ↓ | Yes | ↑ | Doxorubicin | 20 mg/kg | Troponin T | Andreadou et al., ΝΜR Biomed, 2009 [100] | ||
| Carnitine | ↓//↑ | ↓ | Yes | Yes | Anthracyclines/doxorubicin | Troponin T | Armenian et al., Cancer Epidemiol Biomarkers Prev. 2014 [98] | |||
| Threitol | ↓ | Yes | Anthracyclines | Armenian et al., Cancer Epidemiol Biomarkers Prev. 2014 [98] | ||||||
| Mannose | ↓ | Yes | Anthracyclines | Armenian et al., Cancer Epidemiol Biomarkers Prev. 2014 [98] | ||||||
| Pyroglutamine | ↓ | Yes | Anthracyclines | Armenian et al., Cancer Epidemiol Biomarkers Prev. 2014 [98] | ||||||
| N-acetylalanine | ↓ | Yes | Anthracyclines | Armenian et al., Cancer Epidemiol Biomarkers Prev. 2014 [98] | ||||||
| Creatine | ↓ | Yes | Anthracyclines | Armenian et al., Cancer Epidemiol Biomarkers Prev. 2014 [98] | ||||||
| Eicosenoate | ↓ | Yes | Anthracyclines | Armenian et al., Cancer Epidemiol Biomarkers Prev. 2014 [98] | ||||||
| Stearidonate | ↓ | Yes | Anthracyclines | Armenian et al., Cancer Epidemiol Biomarkers Prev. 2014 [98] | ||||||
| Arachidonate | ↓ | Yes | Anthracyclines | Armenian et al., Cancer Epidemiol Biomarkers Prev. 2014 [98] | ||||||
| Dihomo-linoleate | ↓ | Yes | Anthracyclines | Armenian et al., Cancer Epidemiol Biomarkers Prev. 2014 [98] | ||||||
| L-stearoylglcerophoinositol | ↓ | Yes | Anthracyclines | Armenian et al., Cancer Epidemiol Biomarkers Prev. 2014 [98] | ||||||
| Dehydroisoandrosterone sulfate | ↓ | Yes | Anthracyclines | Armenian et al., Cancer Epidemiol Biomarkers Prev. 2014 [98] | ||||||
| Pregnen-dio; disulfate | ↓ | Yes | Anthracyclines | Armenian et al., Cancer Epidemiol Biomarkers Prev. 2014 [98] | ||||||
| Pregn steroid monosulfate | ↓ | Yes | Anthracyclines | Armenian et al., Cancer Epidemiol Biomarkers Prev. 2014 [98] | ||||||
| Arginine | ↑ | ↑ | Yes | Doxorubicin | Schnackenberg et al., Appl. Toxicol. 2016 [102] | |||||
| Asparagine | ↑ | ↑ | Yes | Doxorubicin | Troponin T | Schnackenberg et al., Appl. Toxicol. 2016 [102] | ||||
| Citrulline | ↑ | ↑ | Yes | Doxorubicin | Troponin T | Schnackenberg et al., Appl. Toxicol. 2016 [102] | ||||
| Glycine | ↑ | ↑ | Yes | ↑ | Doxorubicin | Troponin T | Schnackenberg et al., Appl. Toxicol. 2016 [102] | |||
| Histidine | ↑ | ↑ | Yes | Doxorubicin | Troponin T | Schnackenberg et al., Appl. Toxicol. 2016 [102] | ||||
| Lysine | ↑ | ↑ | Yes | Doxorubicin | Troponin T | Schnackenberg et al., Appl. Toxicol. 2016 [102] | ||||
| Methionine | ↑ | ↑ | Yes | Doxorubicin | Troponin T | Schnackenberg et al., Appl. Toxicol. 2016 [102] | ||||
| Ornithine | ↑ | ↑ | Yes | Doxorubicin | Troponin T | Schnackenberg et al., Appl. Toxicol. 2016 [102] | ||||
| Phenylalanine | ↑ | ↑ | Yes | Doxorubicin | Troponin T | Schnackenberg et al., Appl. Toxicol. 2016 [102] | ||||
| Serine | ↑ | ↑ | Yes | Doxorubicin | Troponin T | Schnackenberg et al., Appl. Toxicol. 2016 [102] | ||||
| Threonine | ↑ | ↑ | Yes | ↑ | Doxorubicin | Troponin T | Schnackenberg et al., Appl. Toxicol. 2016 [102] | |||
| Tryptophan | ↑ | ↑ | Yes | Doxorubicin | Troponin T | Schnackenberg et al., Appl. Toxicol. 2016 [102] | ||||
| Tyrosine | ↑ | ↑ | Yes | Doxorubicin | Troponin T | Schnackenberg et al., Appl. Toxicol. 2016 [102] | ||||
| Acetylornithine | ↑ | ↓ | Yes | Doxorubicin | Troponin T | Schnackenberg et al., Appl. Toxicol. 2016 [102] | ||||
| Hydroxproline | ↑ | No | Yes | Doxorubicin | Troponin T | Schnackenberg et al., Appl. Toxicol. 2016 [102] | ||||
| Citrate | no | No | Yes | Doxorubicin | Troponin T | Schnackenberg et al., Appl. Toxicol. 2016 [102] | ||||
| Propionylcarnitine | ↑ | No | Yes | Doxorubicin | Troponin T | Schnackenberg et al., Appl. Toxicol. 2016 [102] | ||||
| Serotonine | no | ↑ | Yes | Doxorubicin | Troponin T | Schnackenberg et al., Appl. Toxicol. 2016 [102] | ||||
| Putrescine | no | ↑ | Yes | Doxorubicin | Troponin T | Schnackenberg et al., Appl. Toxicol. 2016 [102] | ||||
| Malate | ↑ | ↑ | Yes | Doxorubicin | Tan et al., PLoS ONE 2011 [103] | |||||
| Fructose | ↑ | Yes | Doxorubicin | Tan et al., PLoS ONE 2011 [103] | ||||||
| Glycose | ↑ | Yes | Doxorubicin | Tan et al., PLoS ONE 2011 [103] | ||||||
| Cholesterol | ↑ | Yes | Doxorubicin | Tan et al., PLoS ONE 2011 [103] | ||||||
| Alanine | ↑ | Yes | Doxorubicin | Tan et al., PLoS ONE 2011 [103] | ||||||
| Glutamine | Yes | ↓ | Doxorubicin | Tan et al., PLoS ONE 2011 [103] | ||||||
| Docosahexaenoic acid | ↓ | Yes | Sunitinib | Jensen et al., Metabolites. 2017 [104] | ||||||
| Arachidonic acid/eicosapetaenoic acid | ↓ | Yes | Sunitinib | Jensen et al., Metabolites. 2017 [104] | ||||||
| 6-hydroxynicotinic acid | ↓ | Yes | Sunitinib | Jensen et al., Metabolites. 2017 [104] | ||||||
| O-phosphocolamine | ↓ | Yes | Sunitinib | Jensen et al., Metabolites. 2017 [104] | ||||||
| Ethanolamine | ↑ | Yes | Sunitinib | Jensen et al., Metabolites. 2017 [104] | ||||||
| Xenobiotics |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antoniadi, K.; Thomaidis, N.; Nihoyannopoulos, P.; Toutouzas, K.; Gikas, E.; Kelaidi, C.; Polychronopoulou, S. Prognostic Factors for Cardiotoxicity among Children with Cancer: Definition, Causes, and Diagnosis with Omics Technologies. Diagnostics 2023, 13, 1864. https://doi.org/10.3390/diagnostics13111864
Antoniadi K, Thomaidis N, Nihoyannopoulos P, Toutouzas K, Gikas E, Kelaidi C, Polychronopoulou S. Prognostic Factors for Cardiotoxicity among Children with Cancer: Definition, Causes, and Diagnosis with Omics Technologies. Diagnostics. 2023; 13(11):1864. https://doi.org/10.3390/diagnostics13111864
Chicago/Turabian StyleAntoniadi, Kondylia, Nikolaos Thomaidis, Petros Nihoyannopoulos, Konstantinos Toutouzas, Evangelos Gikas, Charikleia Kelaidi, and Sophia Polychronopoulou. 2023. "Prognostic Factors for Cardiotoxicity among Children with Cancer: Definition, Causes, and Diagnosis with Omics Technologies" Diagnostics 13, no. 11: 1864. https://doi.org/10.3390/diagnostics13111864