
Impact of Aortic Valve Regurgitation on Doppler Echocardiographic Parameters in Patients with Severe Aortic Valve Stenosis

Abstract
:1. Introduction
2. Methods
2.1. Morphology and Function
2.2. Aortic Valve Stenosis
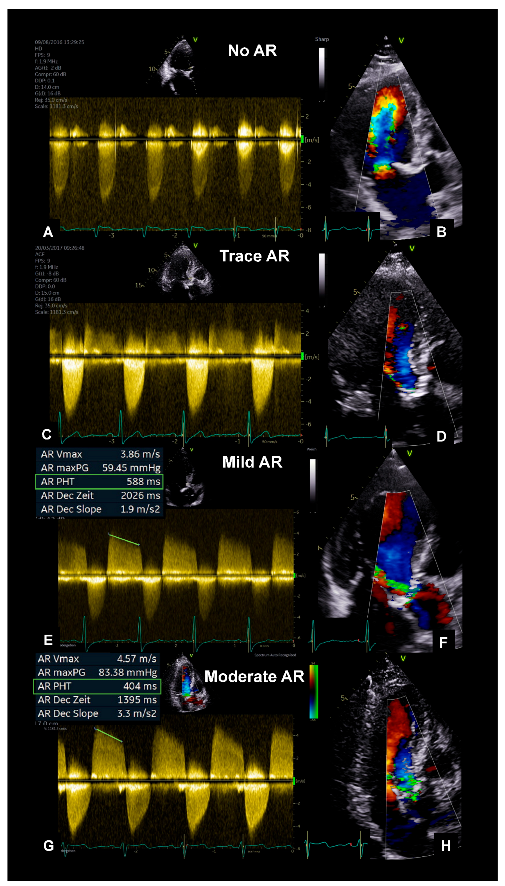
2.3. Aortic Valve Regurgitation
2.4. Classification by Flow and Pressure Gradients
2.5. Transesophageal Echocardiography
2.6. Statistical Analysis
3. Results
3.1. Basic Echocardiographic Parameters
3.2. Doppler-Derived Echocardiographic Parameters
3.3. Determination ofAaortic Valve Area
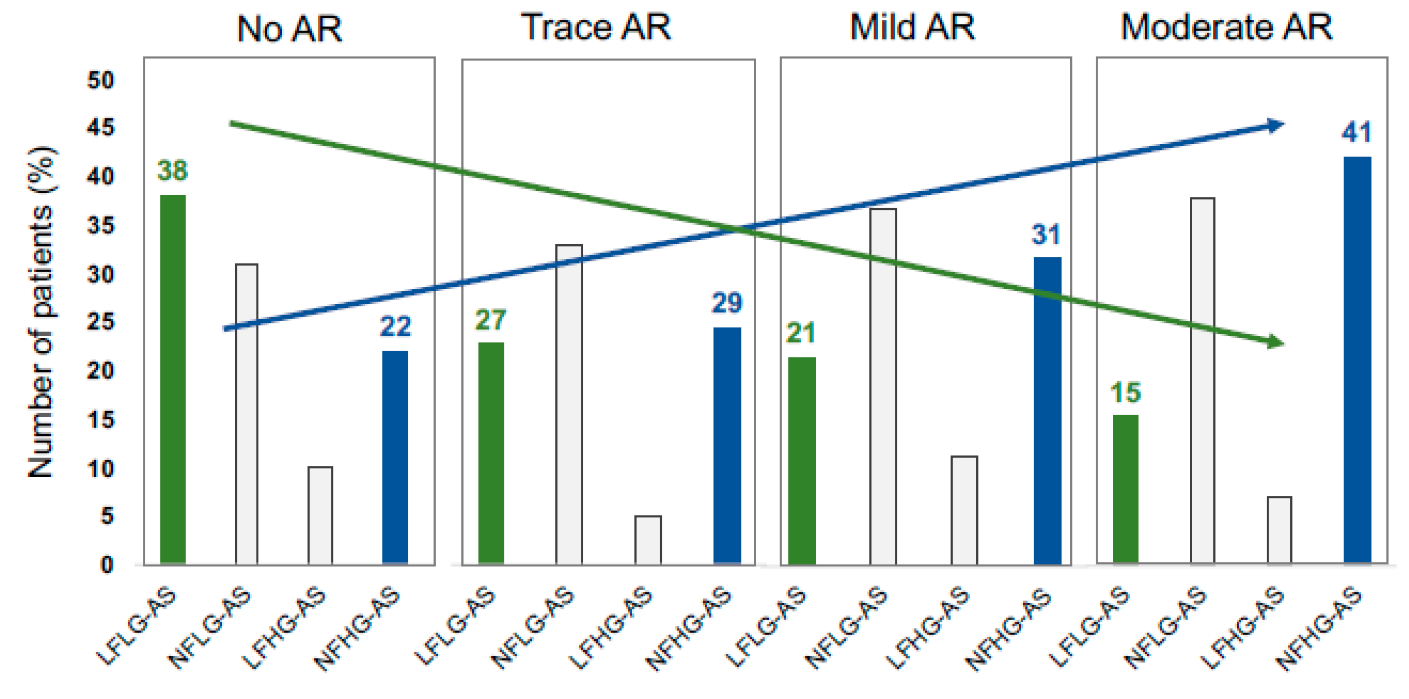
3.4. Classification by Flow and Pressure Gradients
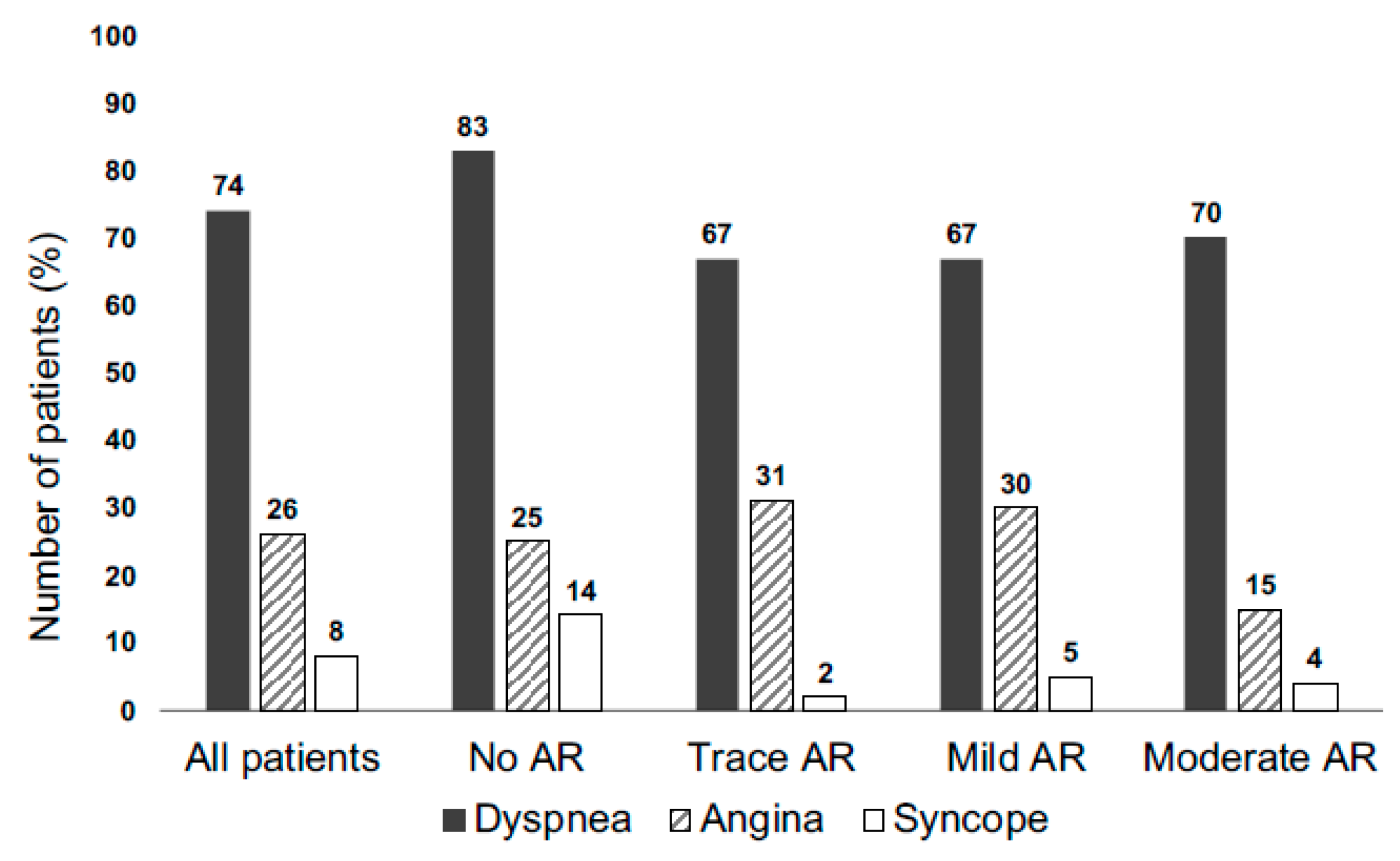
3.5. Symptoms
3.6. Intra- and Interobserver Variability
4. Discussion
The Main Findings of the Present Study
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Osnabrugge, R.L.J.; Mylotte, D.; Head, S.J.; Van Mieghem, N.M.; Nkomo, V.T.; LeReun, C.M.; Bogers, A.J.J.C.; Piazza, N.; Kappetein, A.P. Aortic stenosis in the elderly: Disease prevalence and number of candidates for transcatheter aortic valve replacement: A meta-analysis and modeling study. J. Am. Coll. Cardiol. 2013, 62, 1002–1012. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, F.; Fanti, D.; Tafciu, E.; Fezzi, S.; Setti, M.; Rossi, A.; Ribichini, F.; Benfari, G. When Aortic Stenosis Is Not Alone: Epidemiology, Pathophysiology, Diagnosis and Management in Mixed and Combined Valvular Disease. Front. Cardiovasc. Med. 2021, 8, 744497. [Google Scholar] [CrossRef] [PubMed]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, H.; Hung, J.; Bermejo, J.; Chambers, J.B.; Edvardsen, T.; Goldstein, S.; Lancellotti, P.; LeFevre, M.; Miller, F.; Otto, C.M. Recommendations on the echocardiographic assessment of aortic valve stenosis: A focused update from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 254–275. [Google Scholar] [CrossRef]
- Lancellotti, P.; Magne, J.; Donal, E.; Davin, L.; O’Connor, K.; Rosca, M.; Szymanski, C.; Cosyns, B.; Piérard, L.A. Clinical outcome in asymptomatic severe aortic stenosis: Insights from the new proposed aortic stenosis grading classification. J. Am. Coll. Cardiol. 2012, 59, 235–243. [Google Scholar] [CrossRef]
- Garcia, D.; Pibarot, P.; Landry, C.; Allard, A.; Chayer, B.; Dumesnil, J.G.; Durand, L.-G. Estimation of aortic valve effective orifice area by Doppler echocardiography: Effects of valve inflow shape and flow rate. J. Am. Soc. Echocardiogr. 2004, 17, 756–765. [Google Scholar] [CrossRef]
- Hagendorff, A.; Knebel, F.; Helfen, A.; Knierim, J.; Sinning, C.; Stöbe, S.; Fehske, W.; Ewen, S. Expert consensus document on the assessment of the severity of aortic valve stenosis by echocardiography to provide diagnostic conclusiveness by standardized verifiable documentation. Clin. Res. Cardiol. Off. J. Ger. Card. Soc. 2020, 109, 271–288. [Google Scholar] [CrossRef]
- Hagendorff, A.; Evangelista, A.; Fehske, W.; Schäfers, H.-J. Improvement in the Assessment of Aortic Valve and Aortic Aneurysm Repair by 3-Dimensional Echocardiography. JACC Cardiovasc. Imaging 2019, 12, 2225–2244. [Google Scholar] [CrossRef]
- Sun, L.; Feng, H.; Ni, L.; Wang, H.; Gao, D. Realization of fully automated quantification of left ventricular volumes and systolic function using transthoracic 3D echocardiography. Cardiovasc. Ultrasound 2018, 16, 2. [Google Scholar] [CrossRef]
- Kvaslerud, A.B.; Santic, K.; Hussain, A.I.; Auensen, A.; Fiane, A.; Skulstad, H.; Aaberge, L.; Gullestad, L.; Broch, K. Outcomes in asymptomatic, severe aortic stenosis. PLoS ONE 2021, 16, e0249610. [Google Scholar] [CrossRef]
- Zilberszac, R.; Gabriel, H.; Schemper, M.; Zahler, D.; Czerny, M.; Maurer, G.; Rosenhek, R. Outcome of Combined Stenotic and Regurgitant Aortic Valve Disease. J. Am. Coll. Cardiol. 2013, 61, 1489–1495. [Google Scholar] [CrossRef]
- Egbe, A.C.; Poterucha, J.T.; Warnes, C.A. Mixed aortic valve disease: Midterm outcome and predictors of adverse events. Eur. Heart J. 2016, 37, 2671–2678. [Google Scholar] [CrossRef] [PubMed]
- Rashedi, N.; Popović, Z.B.; Stewart, W.J.; Marwick, T. Outcomes of Asymptomatic Adults with Combined Aortic Stenosis and Regurgitation. J. Am. Soc. Echocardiogr. 2014, 27, 829–837. [Google Scholar] [CrossRef] [PubMed]
- Sorajja, P.; Nelson, P.; Garberich, R.; Bradley, S.M.; Athappan, G.; Bae, R.; Harris, K.; Lesser, J.; Tindell, L.; Farivar, R.S.; et al. Clinical Impact of Chronic Aortic Regurgitation in Asymptomatic Patients with Native Aortic Valve Stenosis. Struct. Heart 2018, 2, 398–404. [Google Scholar] [CrossRef]
- Maurer, G. Aortic regurgitation. Heart 2006, 92, 994–1000. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef]
- Devereux, R.B.; Alonso, D.R.; Lutas, E.M.; Gottlieb, G.J.; Campo, E.; Sachs, I.; Reichek, N. Echocardiographic assessment of left ventricular hypertrophy: Comparison to necropsy findings. Am. J. Cardiol. 1986, 57, 450–458. [Google Scholar] [CrossRef]
- Mor-Avi, V.; Lang, R.M.; Badano, L.P.; Belohlavek, M.; Cardim, N.M.; Derumeaux, G.; Galderisi, M.; Marwick, T.; Nagueh, S.F.; Sengupta, P.P.; et al. Current and evolving echocardiographic techniques for the quantitative evaluation of cardiac mechanics: ASE/EAE consensus statement on methodology and indications endorsed by the Japanese Society of Echocardiography. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2011, 24, 277–313. [Google Scholar] [CrossRef]
- Voigt, J.-U.; Pedrizzetti, G.; Lysyansky, P.; Marwick, T.H.; Houle, H.; Baumann, R.; Pedri, S.; Ito, Y.; Abe, Y.; Metz, S.; et al. Definitions for a common standard for 2D speckle tracking echocardiography: Consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 1–11. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F.; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef]
- Hachicha, Z.; Dumesnil, J.G.; Bogaty, P.; Pibarot, P. Paradoxical Low-Flow, Low-Gradient Severe Aortic Stenosis Despite Preserved Ejection Fraction Is Associated with Higher Afterload and Reduced Survival. Circulation 2007, 115, 2856–2864. [Google Scholar] [CrossRef] [PubMed]
- Pibarot, P.; Dumesnil, J.G. Paradoxical Low-Flow, Low-Gradient Aortic Stenosis: New Evidence, More Questions. Circulation 2013, 128, 1729–1732. [Google Scholar] [CrossRef] [PubMed]
- Kandels, J.; Tayal, B.; Hagendorff, A.; Lavall, D.; Laufs, U.; Sogaard, P.; Andersen, N.H.; Stöbe, S. “Pure” severe aortic stenosis without concomitant valvular heart diseases: Echocardiographic and pathophysiological features. Int. J. Cardiovasc. Imaging 2020, 36, 1917–1929. [Google Scholar] [CrossRef]
- Grayburn, P.A.; Smith, M.D.; Harrison, M.R.; Gurley, J.C.; DeMaria, A.N. Pivotal role of aortic valve area calculation by the continuity equation for Doppler assessment of aortic stenosis in patients with combined aortic stenosis and regurgitation. Am. J. Cardiol. 1988, 61, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Adda, J.; Stanova, V.; Habib, G.; Rieu, R. In vitro correlation between the effective and geometric orifice area in aortic stenosis. J. Cardiol. 2021, 77, 334–340. [Google Scholar] [CrossRef]
- de la Fuente Galán, L.; San Román Calvar, J.A.; Muñoz San José, J.C.; Vega Barbado, J.L.; del Pozo Crespo, F.; Martín, J.A.; Durán Hernández, J.M.; Gimeno de Carlos, F.; Fernández-Avilés, F. Influence of the degree of aortic valve calcification on the estimate of valvular area using planimetry with transesophageal echocardiography. Rev. Esp. Cardiol. 1996, 49, 663–668. [Google Scholar]
- Gilon, D.; Cape, E.G.; Handschumacher, M.D.; Song, J.K.; Solheim, J.; VanAuker, M.; King, M.E.E.; Levine, R.A. Effect of three-dimensional valve shape on the hemodynamics of aortic stenosis: Three-dimensional echocardiographic stereolithography and patient studies. J. Am. Coll. Cardiol. 2002, 40, 1479–1486. [Google Scholar] [CrossRef]
- Elmariah, S.; Delaney, J.A.C.; Bluemke, D.A.; Budoff, M.J.; O’Brien, K.D.; Fuster, V.; Kronmal, R.A.; Halperin, J.L. Associations of LV Hypertrophy with Prevalent and Incident Valve Calcification. JACC Cardiovasc. Imaging 2012, 5, 781–788. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | All Patients (n = 238) | No AR (n = 101) | Trace AR (n = 49) | Mild AR (n = 61) | Moderate AR (n = 27) | p Value |
|---|---|---|---|---|---|---|
| Age (year) | 75.9 ± 9.8 | 75.7 ± 9.4 | 75.4 ± 10.6 | 76.2 ± 10.1 | 76.7 ± 9.0 | 0.998 |
| Sex (% male) | 104 (44%) | 42 (42%) | 21 (43%) | 30 (49%) | 11 (41%) | 0.667 |
| Height (cm) | 165.7 ± 9.5 | 165.7 ± 10.3 | 166.9 ± 9.6 | 165.9 ± 7.9 | 163.2 ± 9.4 | 0.445 |
| Weight (kg) | 76.3 ± 16.4 | 76.5 ± 18.7 | 78.6 ± 12.0 | 75.4 ± 15.8 | 73.2 ± 15.1 | 0.546 |
| BSA (m2) | 1.87 ± 0.23 | 1.86 ± 0.27 | 1.90 ± 0.18 ⧧ | 1.86 ± 0.21 | 1.81 ± 0.22 | 0.451 |
| BMI (kg/m2) | 27.7 ± 5.1 | 27.7 ± 5.6 | 28.3 ± 4.2 | 27.4 ± 5.2 | 27.4 ± 5.0 | 0.812 |
| sBP (mmHg) | 137.4 ± 21.5 | 136.8 ± 21.4 | 133.3 ± 21.2 | 141.3 ± 21.9 | 138.3 ± 21.2 | 0.272 |
| dBP (mmHg) | 80.0 ± 12.9 | 80.3 ± 11.7 | 79.5 ± 13.0 | 81.6 ± 14.7 | 76.2 ± 12.7 | 0.335 |
| HR (1/min) | 75.7 ± 16.1 | 79.0 ± 18.0 †,⧧ | 74.6 ± 13.3 | 70.8 ± 13.8 | 76.2 ± 15.4 | 0.016 * |
| Variables | All Patients (n = 238) | No AR (n = 101) | Trace AR (n = 49) | Mild AR (n = 61) | Moderate AR (n = 27) | p Value |
|---|---|---|---|---|---|---|
| IVSD (mm) | 14.6 ± 2.8 | 14.5 ± 2.9 | 14.9 ± 2.4 | 14.5 ± 2.7 | 14.8 ± 3.2 | 0.824 |
| LVPWD (mm) | 14.5 ± 2.9 | 14.4 ± 2.6 | 14.2 ± 1.9 | 14.7 ± 4.0 | 14.9 ± 2.4 | 0.693 |
| LVEDD (mm) | 44.4 ± 6.1 | 43.7 ± 6.4 † | 44.2 ± 6.2 | 45.5 ± 6.1 | 44.7 ± 4.4 | 0.331 |
| LVESD (mm) | 28.2 ± 5.6 | 28.0 ± 6.1 | 28.2 ± 5.7 | 28.5 ± 5.1 | 28.0 ± 5.0 | 0.999 |
| RWT | 0.67 ± 0.18 | 0.67 ± 0.17 | 0.66 ± 0.15 | 0.66 ± 0.24 | 0.67 ± 0.12 | 0.999 |
| LVMi (g/m2) | 141.1 ± 39.7 | 137.2 ± 41.2 | 136.0 ± 30.9 | 147.3 ± 42.0 | 151.2 ± 45.0 | 0.178 |
| LVEDV (mL) | 105.6 ± 30.0 | 103.3 ± 30.8 | 104.3 ± 24.1 | 107.7 ± 33.1 | 111.5 ± 29.6 | 0.569 |
| LVESV (mL) | 36.2 ± 14.7 | 36.3 ± 14.0 | 35.7 ± 13.4 | 36.2 ± 16.7 | 37.2 ± 15.3 | 0.999 |
| LVSVBP (mL) | 69.4 ± 18.7 | 67.0 ± 19.7 ⧧ | 68.6 ± 14.2 | 71.5 ± 19.8 | 74.4 ± 18.5 | 0.215 |
| LVSViBP (mL) | 36.9 ± 9.5 | 35.2 ± 10.0 †,⧧ | 36.2 ± 7.7 ⧧ | 38.4 ± 9.3 | 41.1 ± 9.3 | 0.015 * |
| LVSVDop (mL) | 69.4 ± 17.6 | 67.4 ± 17.4 | 69.5 ± 16.2 | 71.3 ± 19.2 | 72.8 ± 16.9 | 0.340 |
| LVSViDop (mL) | 37.4 ± 9.0 | 36.3 ± 8.6 ⧧ | 36.7 ± 8.6 ⧧ | 38.4 ± 9.5 | 40.7 ± 9.8 | 0.105 |
| Variables | All Patients (n = 238) | No AR (n = 101) | Trace AR (n = 49) | Mild AR (n = 61) | Moderate AR (n = 27) | p Value |
|---|---|---|---|---|---|---|
| LVEF (%) | 66.0 ± 7.1 | 65.2 ± 6.6 | 65.4 ± 6.7 | 66.6 ± 7.3 | 67.9 ± 8.4 | 0.259 |
| GLS (%) | −15.5 ± 7.5 | −15.0 ± 7.4 | −15.1 ± 7.4 | −16.7 ± 6.7 | −14.5 ± 9.9 | 0.468 |
| CI (L/m2) | 2.5 ± 0.06 | 2.6 ± 0.8 †,⧧ | 2.5 ± 0.6 ⧧ | 2.4 ± 0.7 ⧧ | 3.0 ± 0.7 | 0.004 * |
| E/E’ | 19.3 ± 9.5 | 17.8 ± 7.7 ⧧ | 17.8 ± 7.8 | 19.3 ± 8.4 | 21.1 ± 9.2 | 0.215 |
| E/A | 1.69 ± 1.85 | 1.69 ± 2.03 ⧧ | 1.69± 1.87 | 1.87 ± 2.1 | 1.25 ± 0.59 | 0.578 |
| LAEDV (mL) | 70.3 ± 29.2 | 68.3 ± 29.5 ⧧ | 65.9 ± 17.2 ⧧ | 73.3 ± 32.6 | 79.7 ± 30.5 | 0.154 |
| sPAP (mmHg) | 40.7 ± 12.1 | 39.8 ± 12.2 ⧧ | 39.2 ± 12.4 ⧧ | 40.5 ± 10.8 ⧧ | 47.6 ± 12.8 | 0.018 * |
| Variables | All Patients (n = 238) | No AR (n = 101) | Trace AR (n = 49) | Mild AR (n = 61) | Moderate AR (n = 27) | p Value |
|---|---|---|---|---|---|---|
| EOA (cm2) | 0.75 ± 0.14 | 0.75 ± 0.15 | 0.74 ± 0.14 | 0.75 ± 0.14 | 0.75 ± 0.15 | 0.998 |
| GOA (cm2) | 0.80 ± 0.18 | 0.78 ± 0.20 | 0.79 ± 0.15 | 0.82 ± 0.19 | 0.83 ± 0.14 | 0.424 |
| maxVAV (m/s) | 4.12 ± 0.77 | 4.04 ± 0.76 ⧧ | 4.08 ± 0.68 ⧧ | 4.15 ± 0.85 ⧧ | 4.45 ± 0.70 | 0.097 |
| maxVLVOT(m/s) | 0.98 ± 0.21 | 0.98 ± 0.22 ⧧ | 0.94 ± 0.17 ⧧ | 0.98 ± 0.24 ⧧ | 1.10 ± 0.19 | 0.019 * |
| mPGAV (mmHg) | 37.2 ± 15.5 | 35.6 ± 15.3 ⧧ | 35.7 ± 13.3 ⧧ | 38.7 ± 16.3 | 43.1 ± 16.8 | 0.109 |
| maxVLVOT/maxVAV | 0.24 ± 0.06 | 0.25 ± 0.06 | 0.24 ± 0.05 | 0.24 ± 0.07 | 0.25 ± 0.05 | 0.243 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kandels, J.; Metze, M.; Hagendorff, A.; Stöbe, S. Impact of Aortic Valve Regurgitation on Doppler Echocardiographic Parameters in Patients with Severe Aortic Valve Stenosis. Diagnostics 2023, 13, 1828. https://doi.org/10.3390/diagnostics13111828
Kandels J, Metze M, Hagendorff A, Stöbe S. Impact of Aortic Valve Regurgitation on Doppler Echocardiographic Parameters in Patients with Severe Aortic Valve Stenosis. Diagnostics. 2023; 13(11):1828. https://doi.org/10.3390/diagnostics13111828
Chicago/Turabian StyleKandels, Joscha, Michael Metze, Andreas Hagendorff, and Stephan Stöbe. 2023. "Impact of Aortic Valve Regurgitation on Doppler Echocardiographic Parameters in Patients with Severe Aortic Valve Stenosis" Diagnostics 13, no. 11: 1828. https://doi.org/10.3390/diagnostics13111828