
Hydatid Disease: A Radiological Pictorial Review of a Great Neoplasms Mimicker
 , ,
, , 
Abstract
:1. Introduction
2. Diagnosis of Hydatid Cyst
3. Structure of the Hydatid Cyst
4. Classification of Hydatid Cysts
5. Discussion
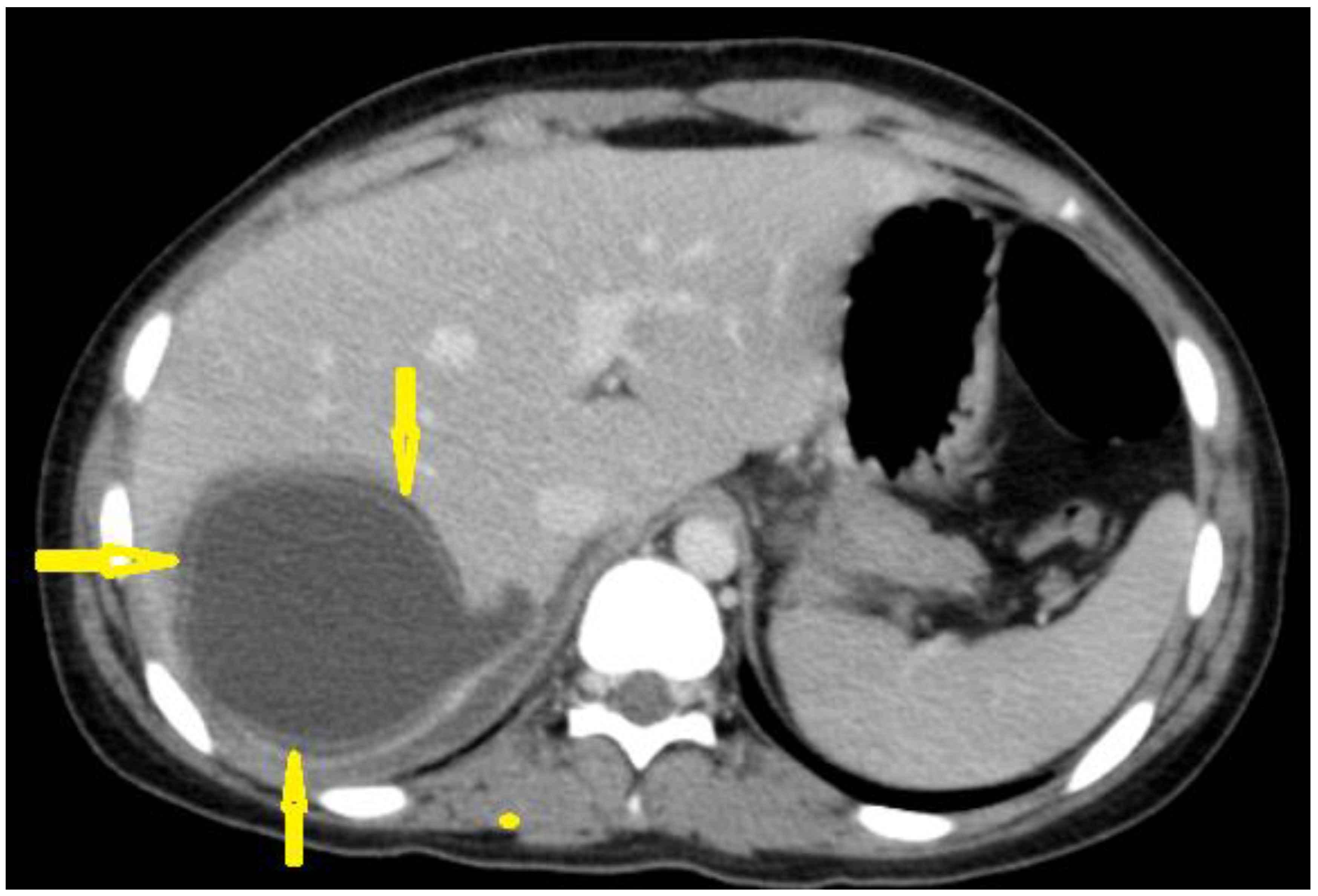
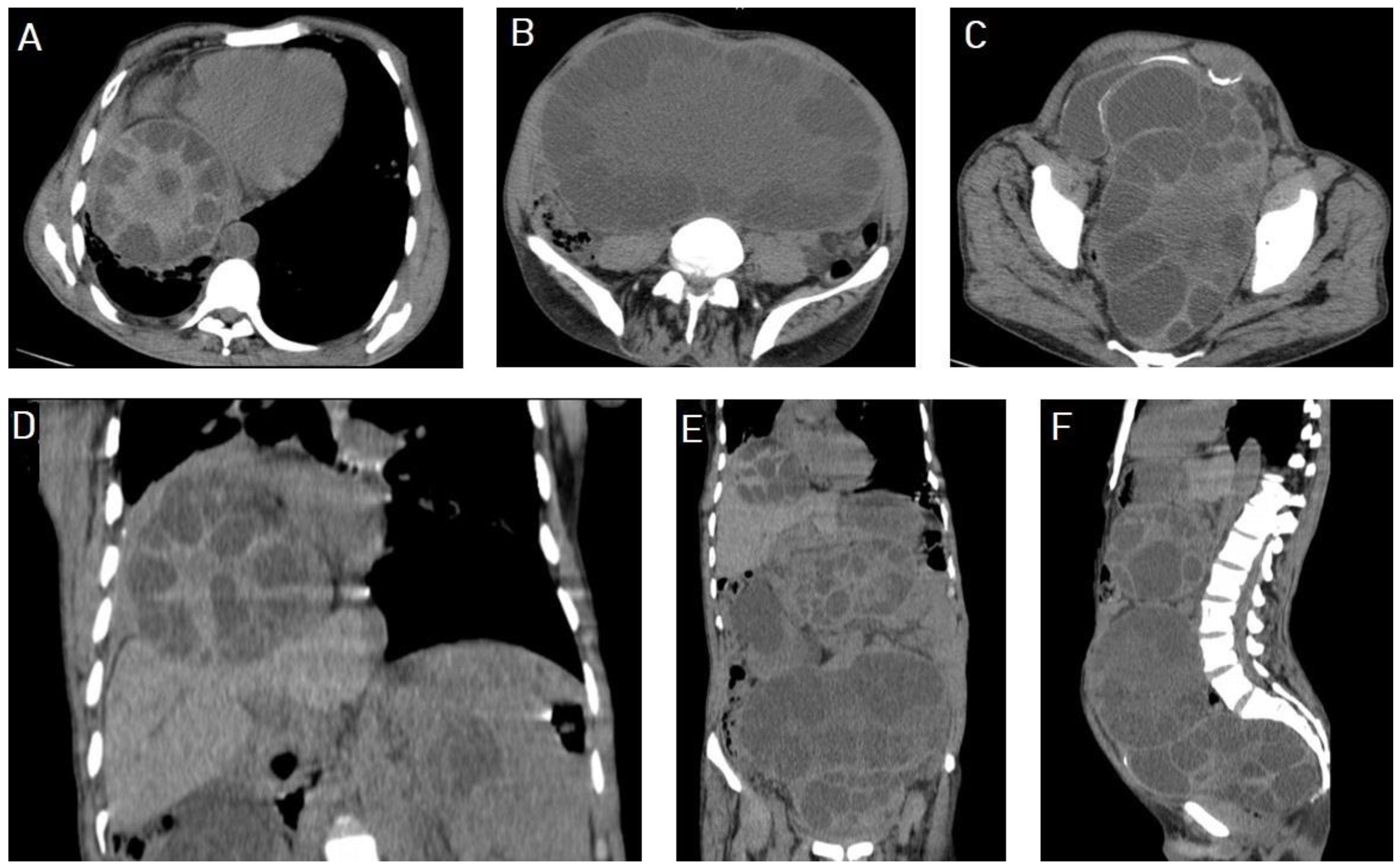
5.1. Hydatid Cysts of the Liver
5.2. Hydatid Cysts of the Lung
5.3. Hydatid Cysts of the Spleen
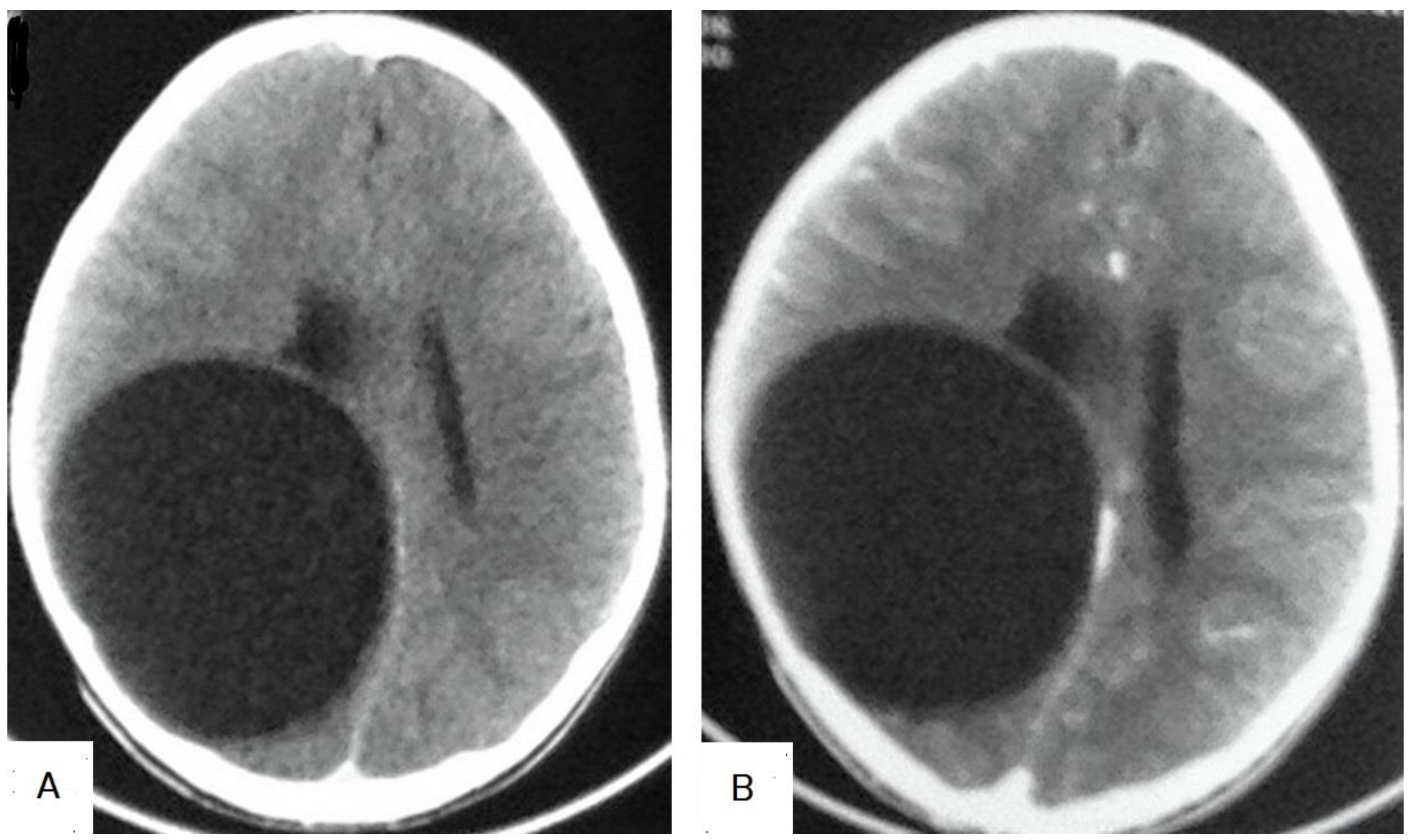
5.4. Hydatid Cysts of the Brain
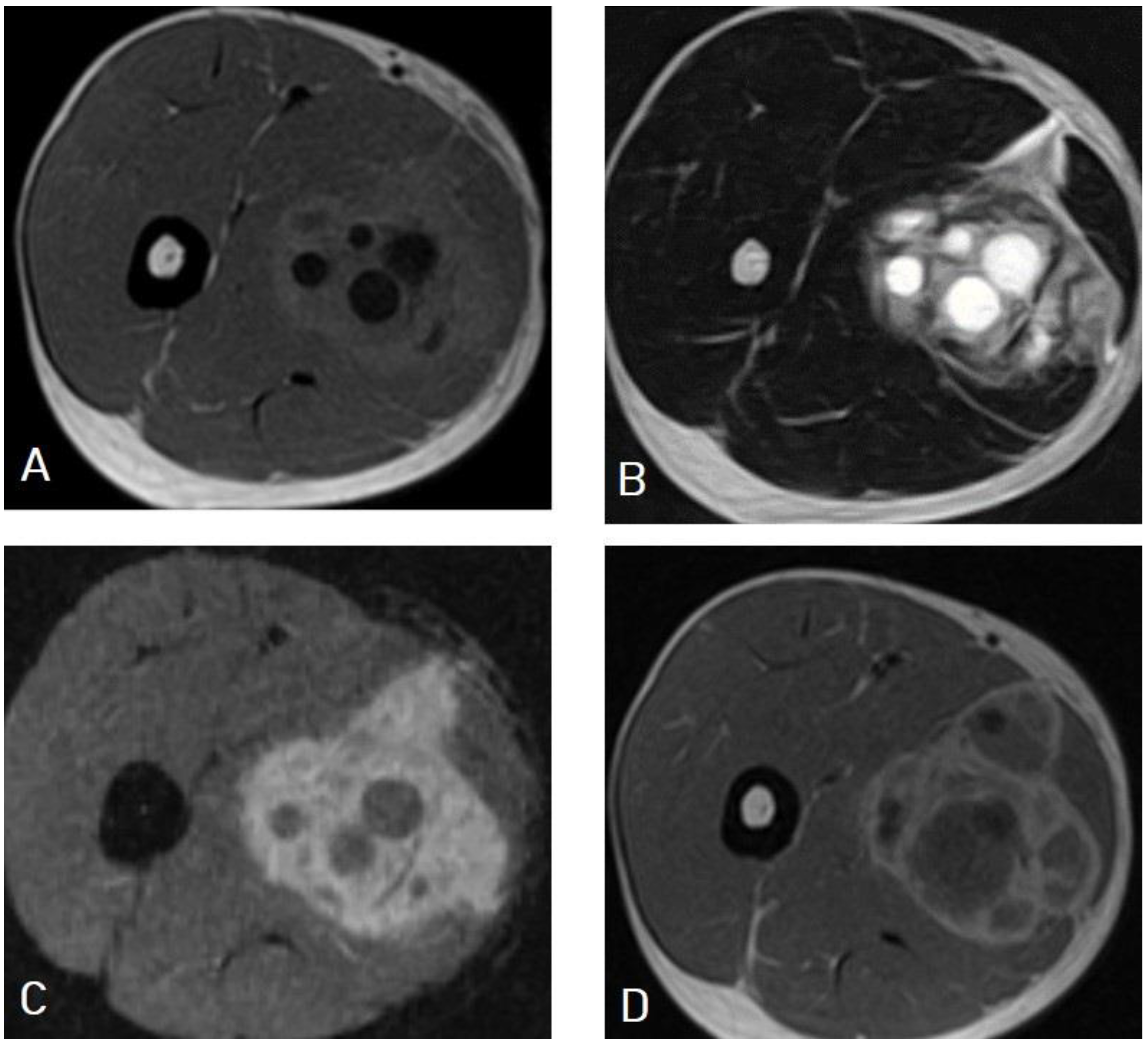
5.5. Hydatid Cysts of the Musculoskeletal System
5.6. Rare Sites of Hydatid Cysts
6. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CT | Computed tomography |
| MRI | Magnetic resonance imaging |
| CE | Cystic echinococcosis |
| AE | Alveolar echinococcosis |
| E. granulosus | Echinococcus granulosus |
| E. multilocularis | Echinococcus multilocularis |
| WHO | World Health Organization |
| WHO-IWGE | WHO Informal Working Group on Echinococcosis |
| ELISA | Enzyme-linked immunosorbent assay |
| T1WIs | T1-weighted images |
| T2WIs | T2-weighted images |
| DWI | Diffusion-weighted imaging |
References
- Agudelo Higuita, N.I.; Brunetti, E.; McCloskey, C. Cystic Echinococcosis. J. Clin. Microbiol. 2016, 54, 518–523. [Google Scholar] [CrossRef] [Green Version]
- Zhang, T.; Li, B.; Liu, Y.; Liu, S. Risk Factors Associated With Echinococcosis in the General Chinese Population: A Meta-Analysis and Systematic Review. Front. Public Health 2022, 10, 821265. [Google Scholar] [CrossRef]
- Lodhia, J.; Chugulu, S.; Sadiq, A.; Msuya, D.; Mremi, A. Giant isolated hydatid lung cyst: Two case reports. J. Med. Case Rep. 2020, 14, 200. [Google Scholar] [CrossRef]
- Torgerson, P.R.; Devleesschauwer, B.; Praet, N.; Speybroeck, N.; Willingham, A.L.; Kasuga, F.; Rokni, M.B.; Zhou, X.N.; Fèvre, E.M.; Sripa, B.; et al. World Health Organization Estimates of the Global and Regional Disease Burden of 11 Foodborne Parasitic Diseases, 2010: A Data Synthesis. PLoS Med. 2015, 12, e1001920. [Google Scholar] [CrossRef] [Green Version]
- Da Silva, A.M. Human echinococcosis: A neglected disease. Gastroenterol. Res. Pract. 2010, 2010, 583297. [Google Scholar] [CrossRef]
- Ines, M.; Mariem, B.L.; Marwa, M.; Amina, B.S.; Chiraz, H. Isolated breast hydatid cyst: Imaging features. Clin. Case Rep. 2022, 10, e06362. [Google Scholar] [CrossRef]
- Santivañez, S.J.; Arias, P.; Portocarrero, M.; Rodriguez, S.; Gonzalez, A.E.; Gilman, R.H.; Gavidia, C.M.; Garcia, H.H. Serological diagnosis of lung cystic hydatid disease using the synthetic p176 peptide. Clin. Vaccine Immunol. 2012, 19, 944–947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunetti, E.; Tamarozzi, F.; Macpherson, C.; Filice, C.; Piontek, M.S.; Kabaalioglu, A.; Dong, Y.; Atkinson, N.; Richter, J.; Schreiber-Dietrich, D.; et al. Ultrasound and Cystic Echinococcosis. Ultrasound Int. Open. 2018, 4, E70–E78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polat, P.; Atamanalp, S.S. Hepatic hydatid disease: Radiographics findings. Eurasian J. Med. 2009, 41, 49. [Google Scholar]
- Golzari, S.E.; Sokouti, M. Pericyst: The outermost layer of hydatid cyst. World J. Gastroenterol. 2014, 20, 1377–1378. [Google Scholar] [CrossRef] [PubMed]
- WHO Informal Working Group. International classification of ultrasound images in cystic echinococcosis for application in clinical and field epidemiological settings. Acta Trop. 2003, 85, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Mehta, P.; Prakash, M.; Khandelwal, N. Radiological manifestations of hydatid disease and its complications. Trop. Parasitol. 2016, 6, 103–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marrone, G.; Crino, F.; Caruso, S.; Mamone, G.; Carollo, V.; Milazzo, M.; Gruttadauria, S.; Luca, A.; Gridelli, B. Multidisciplinary imaging of liver hydatidosis. World J. Gastroenterol. 2012, 18, 1438–1447. [Google Scholar] [CrossRef]
- Moreno Rojas, J.; Vas, D. Liver Hydatid Cyst Rupture with Respiratory Distress During COVID-19 Pandemic. J. Belg. Soc. Radiol. 2022, 106, 41. [Google Scholar] [CrossRef] [PubMed]
- Botezatu, C.; Mastalier, B.; Patrascu, T. Hepatic hydatid cyst—Diagnose and treatment algorithm. J. Med. Life 2018, 11, 203–209. [Google Scholar] [CrossRef]
- Ferrer Inaebnit, E.; Molina Romero, F.X.; Segura Sampedro, J.J.; González Argenté, X.; Morón Canis, J.M. A review of the diagnosis and management of liver hydatid cyst. Rev. Esp. Enferm. Dig. 2022, 114, 35–41. [Google Scholar] [CrossRef]
- Sakhri, J.; Ben Ali, A. Le kyste hydatique du foie [Hydatid cyst of the liver]. J. Chir. 2004, 141, 381–389. [Google Scholar] [CrossRef]
- Pakala, T.; Molina, M.; Wu, G.Y. Hepatic Echinococcal Cysts: A Review. J. Clin. Transl. Hepatol. 2016, 4, 39–46. [Google Scholar] [CrossRef]
- Ran, B.; Aji, T.; Jiang, T.; Zhang, R.; Guo, Q.; Abulizi, A.; Yimiti, Y.; Wen, H.; Shao, Y. Differentiation between hepatic cystic echinococcosis types 1 and simple hepatic cysts: A retrospective analysis. Medicine 2019, 98, e13731. [Google Scholar] [CrossRef]
- Malik, A.; Chandra, R.; Prasad, R.; Khanna, G.; Thukral, B.B. Imaging appearances of atypical hydatid cysts. Indian J. Radiol. Imaging 2016, 26, 33–39. [Google Scholar] [CrossRef]
- Dundar, I.; Ozgokce, M.; Durmaz, F.; Ozkacmaz, S.; Turkoglu, S.; Goya, C. Efficiency of diffusion-weighted MRI for differentiating radiologically similar simple and type I hydatid cysts of the liver. Acta Radiol. 2022, 63, 143–148. [Google Scholar] [CrossRef]
- Erdem, H.; Karaman, U. Hydatid cyst mimickers and cases mimicked by hydatid cyst; with two cases. ODU Med. J. 2022, 9, 110–115. [Google Scholar]
- Salemis, N.S. Giant hydatid liver cyst. Management of residual cavity. Ann. Hepatol. 2008, 7, 174–176. [Google Scholar] [CrossRef] [PubMed]
- Thambidurai, L.; Santhosham, R.; Dev, B. Hydatid cyst: Anywhere, everywhere. Radiol. Case Rep. 2015, 6, 486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarkar, M.; Pathania, R.; Jhobta, A.; Thakur, B.R.; Chopra, R. Cystic pulmonary hydatidosis. Lung India 2016, 33, 179–191. [Google Scholar] [CrossRef]
- Rawat, S.; Kumar, R.; Raja, J.; Singh, R.S.; Thingnam, S.K.S. Pulmonary hydatid cyst: Review of literature. J. Fam. Med. Prim. Care 2019, 8, 2774–2778. [Google Scholar] [CrossRef]
- Ranjan, A. Water lily sign and serpent sign in pulmonary hydatid cystic disease. Arch. Med. Health Sci. 2017, 5, 129–130. [Google Scholar] [CrossRef]
- Sayir, F.; Cobanoglu, U.; Sehitogullari, A. Surgical treatment of pulmonary hydatid cysts, which perforated to the pleura. Eurasian J. Med. 2012, 44, 79–83. [Google Scholar] [CrossRef]
- Garg, M.K.; Sharma, M.; Gulati, A.; Gorsi, U.; Aggarwal, A.N.; Agarwal, R.; Khandelwal, N. Imaging in pulmonary hydatid cysts. World J. Radiol. 2016, 8, 581–587. [Google Scholar] [CrossRef]
- Usluer, O.; Ceylan, K.C.; Kaya, S.; Sevinc, S.; Gursoy, S. Surgical management of pulmonary hydatid cysts: Is size an important prognostic indicator? Tex. Heart Inst. J. 2010, 37, 429–434. [Google Scholar]
- Rasheed, K.; Zargar, S.A.; Telwani, A.A. Hydatid cyst of spleen: A diagnostic challenge. North Am. J. Med. Sci. 2013, 5, 10–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, S.; Kisee, S.; Amatya, S.; Singh, S.; Bista, S.; Shrestha, R.; Kumar Chhantel Thapa, M. A case of giant primary splenic hydatid cyst: Case report. Ann. Med. Surg. 2022, 84, 104829. [Google Scholar] [CrossRef] [PubMed]
- Merad, Y.; Derrar, H.; Zeggai, A.; Chadli, M.; Bemrah, N.; ElHabachi, B. Primary splenic hydatid cyst an unexpected diagnosis: Case report. Ann. Med. Surg. 2021, 65, 102293. [Google Scholar] [CrossRef] [PubMed]
- Mejri, A.; Arfaoui, K.; Ayadi, M.F.; Aloui, B.; Yaakoubi, J. Primitive isolated hydatid cyst of the spleen: Total splenectomy versus spleen saving surgical modalities. BMC Surg. 2021, 21, 46. [Google Scholar] [CrossRef] [PubMed]
- Arega, G.; Merga, G.; Tafa, G.; Salah, F.O.; Abebe, G.; Maru, S.; Ergete, W. Temporoparietal Brain Hydatid Cyst in an Eight-Year-Old Child: A Rare Case Report. Pediatr. Health Med. Ther. 2022, 13, 361–365. [Google Scholar] [CrossRef]
- Duransoy, Y.K.; Mete, M.; Barutçuoğlu, M.; Unsal, U.Ü.; Selçuki, M. Intracranial hydatid cyst is a rare cause of midbrain herniation: A case report and literature review. J. Pediatr. Neurosci. 2013, 8, 224–227. [Google Scholar] [CrossRef]
- Baboli, S.; Baboli, S.; Soleiman Meigooni, S. Brain Hydatid Cyst with Atypical Symptoms in an Adult: A Case Report. Iran J. Parasitol. 2016, 11, 422–425. [Google Scholar]
- Turgut, M. Intracranial hydatidosis in Turkey: Its clinical presentation, diagnostic studies, surgical management, and outcome. A review of 276 cases. Neurosurg. Rev. 2001, 24, 200–208. [Google Scholar] [CrossRef]
- Abbasi, B.; Akhavan, R.; Ghamari Khameneh, A.; Darban Hosseini Amirkhiz, G.; Rezaei-Dalouei, H.; Tayebi, S.; Hashemi, J.; Aminizadeh, B.; Darban Hosseini Amirkhiz, S. Computed tomography and magnetic resonance imaging of hydatid disease: A pictorial review of uncommon imaging presentations. Heliyon 2021, 7, e07086. [Google Scholar] [CrossRef]
- Yaghoobi, M.H.; Sabahi, M.M.; Zibaei, M. Imaging features of the lungs hydatid cyst disseminated into the brain and spleen. Radiol. Case Rep. 2019, 14, 903–905. [Google Scholar] [CrossRef]
- Agrawal, V.M.; Giri, P.J. Largest Intracranial Calcified Hydatid Cyst: A Case Report with Review of Literature. Asian J. Neurosurg. 2020, 15, 713–715. [Google Scholar] [CrossRef]
- Ganjeifar, B.; Ghafouri, M.; Shokri, A.; Rahbarian Yazdi, F.; Hashemi, S.A. Giant Cerebral Hydatid Cyst: A Rare Case Report. Clin. Case Rep. 2021, 9, 1774–1778. [Google Scholar] [CrossRef]
- Simsek, O.; Ciledag, N. Musculoskeletal Hydatid Disease: The Serpent Sign. Radiology 2021, 301, 280–281. [Google Scholar] [CrossRef] [PubMed]
- Soltany, S.; Hemmati, H.R.; Toussy, J.A.; Nazifi, M.; Alibakhshi, A.; Toosi, P.A. Evaluation of Musculoskeletal Hydatid Cyst Cases in Terms of Clinical Manifestations, Method of Dealing, Treatment, and Recurrence. Maced. J. Med. Sci. 2020, 8, 99–104. [Google Scholar] [CrossRef]
- Toğral, G.; Arıkan, Ş.M.; Ekiz, T.; Kekeç, A.F.; Ekşioğlu, M.F. Musculoskeletal Hydatid Cysts Resembling Tumors: A Report of Five Cases. Orthop. Surg. 2016, 8, 246–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geramizadeh, B. Unusual locations of the hydatid cyst: A review from iran. Iran. J. Med. Sci. 2013, 38, 2–14. [Google Scholar]
- Sachar, S.; Goyal, S.; Goyal, S.; Sangwan, S. Uncommon locations and presentations of hydatid cyst. Ann. Med. Health Sci. Res. 2014, 4, 447–452. [Google Scholar] [CrossRef] [Green Version]
- Assimakopoulos, S.F.; Marangos, M. Orbital Hydatid Cyst. N. Engl. J. Med. 2020, 382, 1352. [Google Scholar] [CrossRef]
- Eshraghi, M.; Shahmoradi, L.; Ghoddoosi, M.; Sadati, S.J.A. Diagnosis of Primary Hydatid Cyst of Thyroid Gland: A Case Report. Biomol. Concepts 2019, 10, 106–110. [Google Scholar] [CrossRef]
- Karmarkar, P.J.; Mahore, S.D.; Wilkinson, A.R.; Joshi, A.M. Isolated hydatid cyst in the submandibular salivary gland: A rare primary presentation (diagnosis by fine needle aspiration cytology). Indian J. Pathol. Microbiol. 2011, 54, 411–413. [Google Scholar] [CrossRef]
- Safioleas, M.; Giannopoulos, A.; Manti, C.; Stamatakos, M.; Safioleas, K.; Stavrou, E. Hydatid disease of the parotid gland: A rare case report. Parasitol. Int. 2007, 56, 247–249. [Google Scholar] [CrossRef] [PubMed]
- Alareqi, A.A.; Alshoabi, S.A.; Alhazmi, F.H.; Hamid, A.M.; Alsharif, W.M.; Gameraddin, M.B. A rare phenotype of breast hydatid cyst causing misdiagnosis and unnecessary intervention: A case report. Radiol. Case Rep. 2021, 16, 3226–3230. [Google Scholar] [CrossRef] [PubMed]
- Limaiem, F.; Bouslama, S.; Haddad, I.; Bouraoui, S.; Lahmar, A.; Mzabi, S. Hydatid cyst presenting as a breast lump in a male patient. Pathologica 2013, 105, 101–103. [Google Scholar]
- Traibi, A.; Atoini, F.; Zidane, A.; Arsalane, A.; Kabiri, E.H. Mediastinal hydatid cyst. J. Chin. Med. Assoc. 2010, 73, 3–7. [Google Scholar] [CrossRef] [Green Version]
- Aljaber, N.N.; Alshoabi, S.A.; Qurashi, A.A.; Daqqaq, T.S. Cardiac hydatid cyst in the right ventricle: An unusual case at a rare site. J. Taibah Univ. Med. Sci. 2020, 15, 249–252. [Google Scholar] [CrossRef]
- Makni, A.; Jouini, M.; Kacem, M.; Safta, Z.B. Acute pancreatitis due to pancreatic hydatid cyst: A case report and review of the literature. World J. Emerg. Surg. 2012, 7, 7. [Google Scholar] [CrossRef] [Green Version]
- Tazi, F.; Ahsaini, M.; Khalouk, A.; Mellas, S.; Stuurman-Wieringa, R.E.; Elfassi, M.J.; Farih, M.H. Giant primary adrenal hydatid cyst presenting with arterial hypertension: A case report and review of the literature. J. Med. Case Rep. 2012, 6, 46. [Google Scholar] [CrossRef] [Green Version]
- Başgül, A.; Kavak, Z.N.; Gökaslan, H.; Küllü, S. Hydatid cyst of the uterus. Infect. Dis. Obstet. Gynecol. 2002, 10, 67–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cattorini, L.; Trastulli, S.; Milani, D.; Cirocchi, R.; Giovannelli, G.; Avenia, N.; Sciannameo, F. Ovarian hydatid cyst: A case report. Int. J. Surg. Case Rep. 2011, 2, 100–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giriyan, S.S.; Navyashree, N. An unusual presentation of hydatid cyst in the neck: A cytological diagnosis. Indian J. Pathol. Microbiol. 2018, 61, 454–455. [Google Scholar] [CrossRef]
- Ewnte, B. Hydatid cyst of the foot: A case report. J. Med. Case Rep. 2020, 14, 6. [Google Scholar] [CrossRef] [PubMed]
- Nischal, N.; Verma, A.K.; Bhangale, D. Primary Subcutaneous Hydatid Cyst of the Face: A Rare Entity with Emphasis on Radiological Evaluation. Arch. Clin. Infect. Dis. 2017, 12, e63543. [Google Scholar] [CrossRef] [Green Version]


























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Differential Diagnosis of the Hydatid Cysts |
|---|---|
| Erdem et al. [22] | Liver hydatid cyst can mimic multiple cystic or solid lesions of the liver, such as the following: 1: Simple liver cysts. 2: Choledochal cysts. 3: Caroli’s disease. 4: Hemangioendotheliomas. 5: Mesenchymal hamartomas. 6: Teratomas. |
| Garg et al. [29] | I: Intact lung hydatid cyst can mimic the following: 1: Any lung cysts. II: Lung hydatid cysts with crescent signs can mimic the following: 1: Mycetomas. 2: Blood clots. 3: Rasmussen aneurysms. 4: Lung carcinomas. |
| Merad et al. [33] | Hydatid cysts of the spleen can mimic other splenic cystic lesions, such as the following: 1: Epidermoid cysts. 2: Epidermoid cysts. 3: Solitary abscesses. 4: Hematomas. 5: Cystic hemangiomas. 6: Intrasplenic pancreatic pseudocysts. 7: Lymphangiomas. |
| Abbasi et al. [39] Agrawal et al. [41] | Brain hydatid cysts can mimic brain cystic lesions, such as the following: 1: Arachnoid cysts. 2: Porencephalic cysts. 3: Pyogenic abscesses. 4: Cystic tumors of the brain. 5-Neurocysticercosis. |
| Ganjeifar et al. [42] | Brain hydatid cysts can mimic brain lesions, such as the following: 1: Pyogenic abscesses. 2: Granulomas. 3: Cystic gliomas. 4: Epidermoid cysts. 5: Arachnoid cysts. |
| Togral et al. [45] | Hydatid cyst of the musculoskeletal system can resemble tumors and tumor-like lesions, such as the following: 1: Tuberculosis infections of the bones and muscles. 2: Fungal infections of the bones. 3: Others. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alshoabi, S.A.; Alkalady, A.H.; Almas, K.M.; Magram, A.O.; Algaberi, A.K.; Alareqi, A.A.; Hamid, A.M.; Alhazmi, F.H.; Qurashi, A.A.; Abdulaal, O.M.; et al. Hydatid Disease: A Radiological Pictorial Review of a Great Neoplasms Mimicker. Diagnostics 2023, 13, 1127. https://doi.org/10.3390/diagnostics13061127
Alshoabi SA, Alkalady AH, Almas KM, Magram AO, Algaberi AK, Alareqi AA, Hamid AM, Alhazmi FH, Qurashi AA, Abdulaal OM, et al. Hydatid Disease: A Radiological Pictorial Review of a Great Neoplasms Mimicker. Diagnostics. 2023; 13(6):1127. https://doi.org/10.3390/diagnostics13061127
Chicago/Turabian StyleAlshoabi, Sultan Abdulwadoud, Abdulaziz H. Alkalady, Khaled M. Almas, Abdullatif O. Magram, Ali K. Algaberi, Amal A. Alareqi, Abdullgabbar M. Hamid, Fahad H. Alhazmi, Abdulaziz A. Qurashi, Osamah M. Abdulaal, and et al. 2023. "Hydatid Disease: A Radiological Pictorial Review of a Great Neoplasms Mimicker" Diagnostics 13, no. 6: 1127. https://doi.org/10.3390/diagnostics13061127