
High Levels of Leptin and Adipsin Are Associated with Clinical Activity in Early Rheumatoid Arthritis Patients with Overweight and Periodontal Infection
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Examination
2.2. Adipokine Levels and Serum Markers Measurements
2.3. Detection of DNA of P. gingivalis, IgG1 and IgG2 Anti-P. gingivalis Antibodies
2.4. Statistical Analysis
3. Results
3.1. Sociodemographic Characteristics
3.2. Periodontal Status
3.3. Rheumatologic Serum Biomarkers and Disease Activity Scores
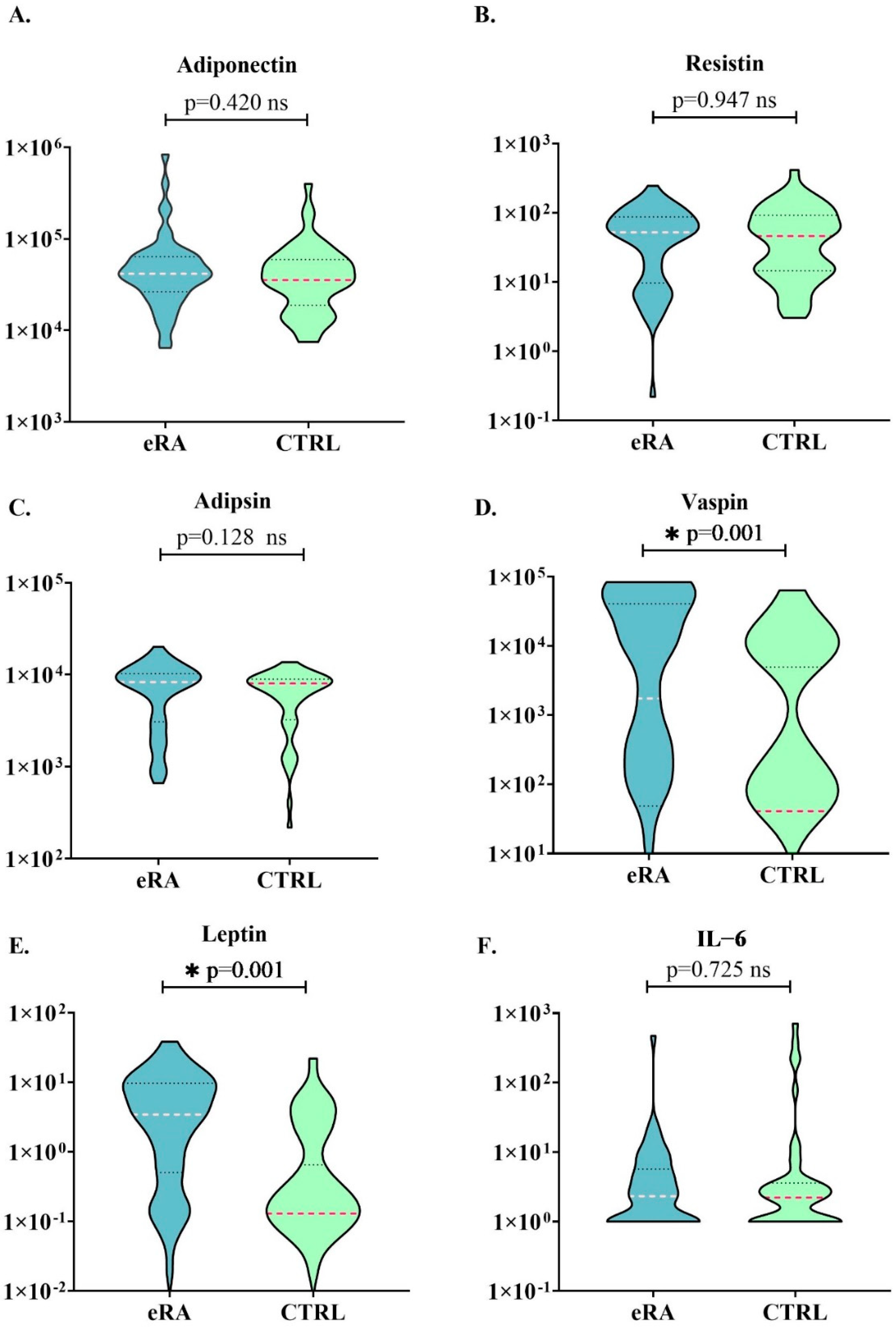
3.4. Adipokine Profile
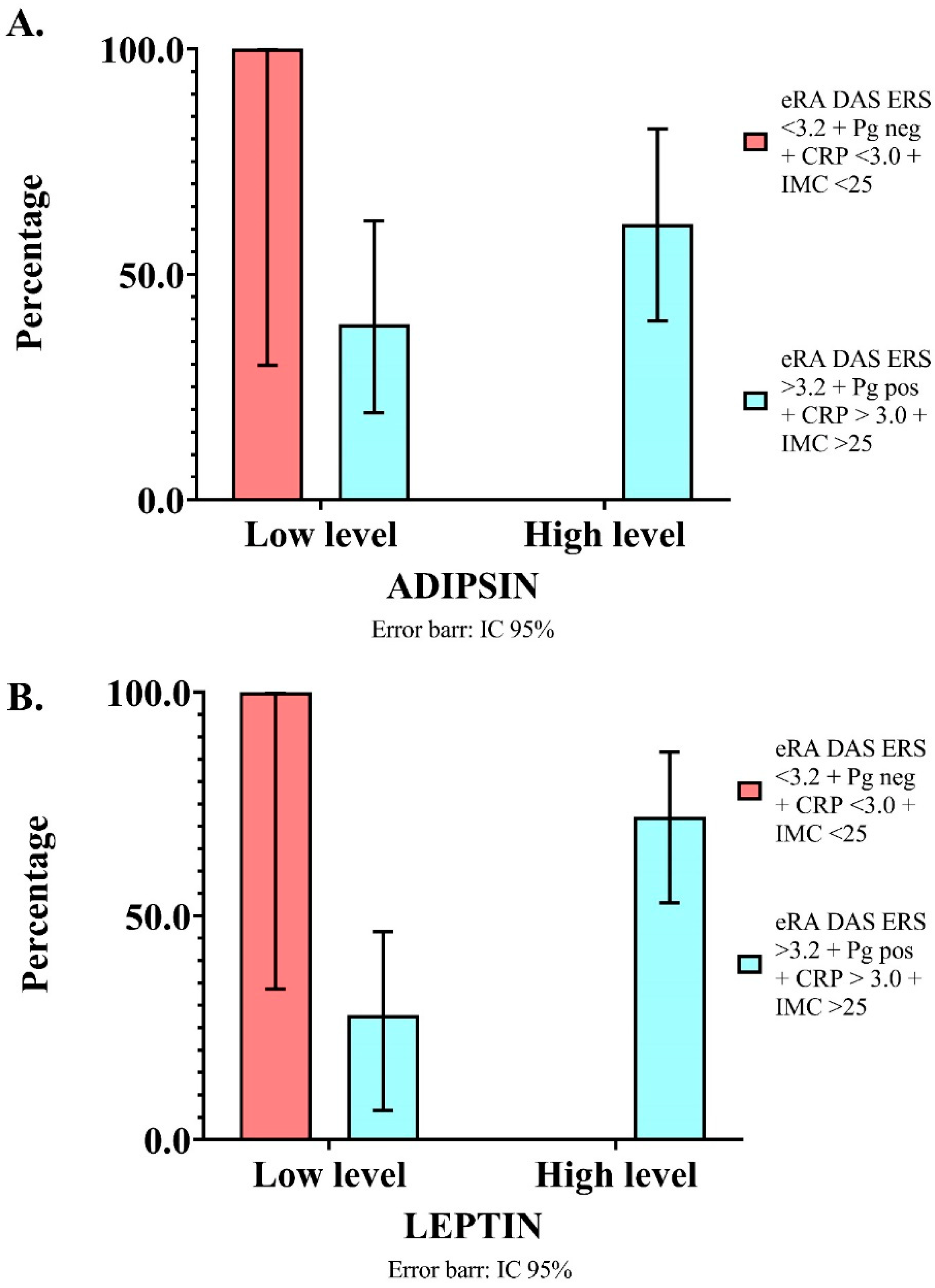
3.5. Multivariate Analysis
4. Discussion
5. Conclusions
6. Strengths and Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Malmström, V.; Catrina, A.I.; Klareskog, L. The Immunopathogenesis of Seropositive Rheumatoid Arthritis: From Triggering to Targeting. Nat. Rev. Immunol. 2017, 17, 60–75. [Google Scholar] [CrossRef] [PubMed]
- Lundberg, K.; Wegner, N.; Yucel-Lindberg, T.; Venables, P.J. Periodontitis in RA—The Citrullinated Enolase Connection. Nat. Rev. Rheumatol. 2010, 6, 727–730. [Google Scholar] [CrossRef] [PubMed]
- Londoño, J.; Peláez Ballestas, I.; Cuervo, F.; Angarita, I.; Giraldo, R.; Rueda, J.C.; Ballesteros, J.G.; Baquero, R.; Forero, E.; Cardiel, M.; et al. Prevalencia de La Enfermedad Reumática En Colombia, Según Estrategia COPCORD-Asociación Colombiana de Reumatología. Estudio de Prevalencia de Enfermedad Reumática En Población Colombiana Mayor de 18 Años. Rev. Colomb. Reumatol. 2018, 25, 245–256. [Google Scholar] [CrossRef]
- Bautista-Molano, W.; van der Heijde, D.; Landewé, R.; Lafaurie, G.I.; de Ávila, J.; Valle-Oñate, R.; Romero-Sanchez, C. Is There a Relationship between Spondyloarthritis and Periodontitis? A Case–Control Study. RMD Open 2017, 3, e000547. [Google Scholar] [CrossRef]
- Nikiphorou, E.; Norton, S.; Young, A.; Dixey, J.; Walsh, D.; Helliwell, H.; Kiely, P. The Association of Obesity with Disease Activity, Functional Ability and Quality of Life in Early Rheumatoid Arthritis: Data from the Early Rheumatoid Arthritis Study/Early Rheumatoid Arthritis Network UK Prospective Cohorts. Rheumatology 2018, 57, 1194–1202. [Google Scholar] [CrossRef] [Green Version]
- Suvan, J.; D’Aiuto, F.; Moles, D.R.; Petrie, A.; Donos, N. Association between Overweight/Obesity and Periodontitis in Adults. A Systematic Review. Obes. Rev. 2011, 12, e381–e404. [Google Scholar] [CrossRef]
- Deschner, J.; Eick, S.; Damanaki, A.; Nokhbehsaim, M. The Role of Adipokines in Periodontal Infection and Healing. Mol. Oral Microbiol. 2014, 29, 258–269. [Google Scholar] [CrossRef]
- Dodson, M.V.; Du, M.; Wang, S.; Bergen, W.G.; Fernyhough-Culver, M.; Basu, U.; Poulos, S.P.; Hausman, G.J. Adipose Depots Differ in Cellularity, Adipokines Produced, Gene Expression, and Cell Systems. Adipocyte 2014, 3, 236–241. [Google Scholar] [CrossRef] [Green Version]
- Leal, V.d.O.; Mafra, D. Adipokines in Obesity. Clin. Chim. Acta 2013, 419, 87–94. [Google Scholar] [CrossRef]
- Shimada, Y.; Komatsu, Y.; Ikezawa-Suzuki, I.; Tai, H.; Sugita, N.; Yoshie, H. The Effect of Periodontal Treatment on Serum Leptin, Interleukin-6, and C-Reactive Protein. J. Periodontol. 2010, 81, 1118–1123. [Google Scholar] [CrossRef]
- Zimmermann, G.S.; Bastos, M.F.; Dias Gonçalves, T.E.; Chambrone, L.; Duarte, P.M. Local and Circulating Levels of Adipocytokines in Obese and Normal Weight Individuals with Chronic Periodontitis. J. Periodontol. 2013, 84, 624–633. [Google Scholar] [CrossRef]
- Nokhbehsaim, M.; Keser, S.; Nogueira, A.V.B.; Jäger, A.; Jepsen, S.; Cirelli, J.A.; Bourauel, C.; Eick, S.; Deschner, J. Leptin Effects on the Regenerative Capacity of Human Periodontal Cells. Int. J. Endocrinol. 2014, 2014, 180304. [Google Scholar] [CrossRef] [Green Version]
- Nokhbehsaim, M.; Keser, S.; Nogueira, A.V.B.; Cirelli, J.A.; Jepsen, S.; Jäger, A.; Eick, S.; Deschner, J. Beneficial Effects of Adiponectin on Periodontal Ligament Cells under Normal and Regenerative Conditions. J. Diabetes Res. 2014, 2014, 796565. [Google Scholar] [CrossRef] [Green Version]
- Hutcheson, J. Adipokines Influence the Inflammatory Balance in Autoimmunity. Cytokine 2015, 75, 272–279. [Google Scholar] [CrossRef]
- Chaparro-Sanabria, J.A.; Bautista-Molano, W.; Bello-Gualtero, J.M.; Chila-Moreno, L.; Castillo, D.M.; Valle-Oñate, R.; Chalem, P.; Romero-Sánchez, C. Association of Adipokines with Rheumatic Disease Activity Indexes and Periodontal Disease in Patients with Early Rheumatoid Arthritis and Their First-Degree Relatives. Int. J. Rheum. Dis. 2019, 22, 1990–2000. [Google Scholar] [CrossRef]
- Klein-Wieringa, I.R.; van der Linden, M.P.M.; Knevel, R.; Kwekkeboom, J.C.; van Beelen, E.; Huizinga, T.W.J.; van der Helm-van Mil, A.; Kloppenburg, M.; Toes, R.E.M.; Ioan-Facsinay, A. Baseline Serum Adipokine Levels Predict Radiographic Progression in Early Rheumatoid Arthritis. Arthritis Rheum. 2011, 63, 2567–2574. [Google Scholar] [CrossRef]
- Maijer, K.I.; Neumann, E.; Müller-Ladner, U.; Drop, D.A.C.A.D.; Ramwadhdoebe, T.H.; Choi, I.Y.K.; Gerlag, D.M.; de Hair, M.J.H.; Tak, P.P. Serum Vaspin Levels Are Associated with the Development of Clinically Manifest Arthritis in Autoantibody-Positive Individuals. PLoS ONE 2015, 10, e0144932. [Google Scholar] [CrossRef] [Green Version]
- Romero-Sanchez, C.; Chaparro-Sanabria, J.A.; Bello-Gualtero, J.M.; Valle-Oñate, R.; Chila, L.; Castillo, D.M.; Lafaurie, G.; Chalem Ch, P.; Bautista-Molano, W. OP0171 Leptin Levels, Overweight and P gingivalis Presence Contribute to the Mechanism of Systemic Inflammation in First-Degree Relatives of Rheumatoid Arthritis Individuals. Ann. Rheum. Dis. 2018, 77, 135–136. [Google Scholar] [CrossRef]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O.; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid Arthritis Classification Criteria: An American College of Rheumatology/European League Against Rheumatism Collaborative Initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus Report of Workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89, S173–S182. [Google Scholar] [CrossRef] [Green Version]
- Bello-Gualtero, J.M.; Lafaurie, G.I.; Hoyos, L.X.; Castillo, D.M.; De-Avila, J.; Munevar, J.C.; Unriza, S.; Londoño, J.; Valle-Onate, R.; Romero-Sánchez, C. Periodontal Disease in Individuals with a Genetic Risk of Developing Arthritis and Early Rheumatoid Arthritis: A Cross-Sectional Study. J. Periodontol. 2016, 87, 346–356. [Google Scholar] [CrossRef]
- Kasper, N.M.; Herrán, O.F.; Villamor, E. Obesity Prevalence in Colombian Adults Is Increasing Fastest in Lower Socio-Economic Status Groups and Urban Residents: Results from Two Nationally Representative Surveys. Public Health Nutr. 2014, 17, 2398–2406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nikiphorou, E.; Guh, D.; Bansback, N.; Zhang, W.; Dixey, J.; Williams, P.; Young, A. Work Disability Rates in RA. Results from an Inception Cohort with 24 Years Follow-Up. Rheumatology 2012, 51, 385–392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uhlig, T. Which Patients with Rheumatoid Arthritis Are Still Working? Arthritis Res. Ther. 2010, 12, 114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministerio de Salud y Protección Social. IV Estudio Nacional de Salud Bucal—ENSAB IV; Ministerio de Salud y Protección Social: Bogotá, Colombia, 2014. [Google Scholar]
- Johansson, L.; Sherina, N.; Kharlamova, N.; Potempa, B.; Larsson, B.; Israelsson, L.; Potempa, J.; Rantapää-Dahlqvist, S.; Lundberg, K. Concentration of Antibodies against Porphyromonas gingivalis Is Increased before the Onset of Symptoms of Rheumatoid Arthritis. Arthritis Res. Ther. 2016, 18, 201. [Google Scholar] [CrossRef] [Green Version]
- Lafaurie, G.I.; Contreras, A.; Barón, A.; Botero, J.; Mayorga-Fayad, I.; Jaramillo, A.; Giraldo, A.; González, F.; Mantilla, S.; Botero, A.; et al. Demographic, Clinical, and Microbial Aspects of Chronic and Aggressive Periodontitis in Colombia: A Multicenter Study. J. Periodontol. 2007, 78, 629–639. [Google Scholar] [CrossRef]
- Gómez, R.; Conde, J.; Scotece, M.; Gómez-Reino, J.J.; Lago, F.; Gualillo, O. What’s New in Our Understanding of the Role of Adipokines in Rheumatic Diseases? Nat. Rev. Rheumatol. 2011, 7, 528–536. [Google Scholar] [CrossRef]
- Le Sage, F.; Meilhac, O.; Gonthier, M.-P.P. Porphyromonas gingivalis Lipopolysaccharide Induces Pro-Inflammatory Adipokine Secretion and Oxidative Stress by Regulating Toll-like Receptor-Mediated Signaling Pathways and Redox Enzymes in Adipocytes. Mol. Cell Endocrinol. 2017, 446, 102–110. [Google Scholar] [CrossRef]
- Jaedicke, K.M.; Roythorne, A.; Padget, K.; Todryk, S.; Preshaw, P.M.; Taylor, J.J. Leptin Up-Regulates TLR2 in Human Monocytes. J. Leukoc. Biol. 2013, 93, 561–571. [Google Scholar] [CrossRef]
- Zhao, Y.; Chen, C. Adipsin as Adipokine. In Adipokines; Preedy, V.R., Hunter, R.J., Eds.; CRC Press: London, UK, 2017; pp. 20–27. [Google Scholar]
- Li, Y.; Zou, W.; Brestoff, J.R.; Rohatgi, N.; Wu, X.; Atkinson, J.P.; Harris, C.A.; Teitelbaum, S.L. Fat-Produced Adipsin Regulates Inflammatory Arthritis. Cell Rep. 2019, 27, 2809–2816. [Google Scholar] [CrossRef] [Green Version]
- Chaparro, J.A.; Bello-Gualtero, J.M.; Valle-Oñate, R.; Bautista-Molano, W.; Chila, L.; Castillo, D.M.; Lafaurie, G.; Chalem Ch, P.; Romero-Sanchez, C. AB0120 Adiponectin Could Be a Mediator of the Presence of P gingivalis in Patients with Early Rheumatoid Arthritis. Ann. Rheum. Dis. 2018, 77, 1254. [Google Scholar]
- Mills, E.L.; Kelly, B.; O’Neill, L.A.J. Mitochondria Are the Powerhouses of Immunity. Nat. Immunol. 2017, 18, 488–498. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Macias, H.; Romieu, I. Effects of Antioxidant Supplements and Nutrients on Patients with Asthma and Allergies. J. Allergy Clin. Immunol. 2014, 133, 1237–1244. [Google Scholar] [CrossRef] [PubMed]
- Pisoschi, A.M.; Pop, A. The Role of Antioxidants in the Chemistry of Oxidative Stress: A Review. Eur. J. Med. Chem. 2015, 97, 55–74. [Google Scholar] [CrossRef]
- Quinonez-Flores, C.M.; Gonzalez-Chavez, S.A.; del Rio Najera, D.; Pacheco-Tena, C. Oxidative Stress Relevance in the Pathogenesis of the Rheumatoid Arthritis: A Systematic Review. Biomed. Res. Int. 2016, 2016, 6097417. [Google Scholar] [CrossRef] [Green Version]
- Sezer, U.; Erciyas, K.; Üstün, K.; Pehlivan, Y.; Ziya Şenyurt, S.; Aksoy, N.; Tarakçıoğlu, M.; Taysı, S.; Onat, A.M. Effect of Chronic Periodontitis on Oxidative Status in Patients with Rheumatoid Arthritis. J. Periodontol. 2013, 84, 785–792. [Google Scholar] [CrossRef]
- Martu, M.A.; Surlin, P.; Lazar, L.; Maftei, G.A.; Luchian, I.; Gheorghe, D.N.; Rezus, E.; Toma, V.; Foia, L.G. Evaluation of Oxidative Stress before and after Using Laser and Photoactivation Therapy as Adjuvant of Non-Surgical Periodontal Treatment in Patients with Rheumatoid Arthritis. Antioxidants 2021, 10, 226. [Google Scholar] [CrossRef]
- Galiutina, O.; Shevchuk, S.; Seheda, Y.; Kuvikova, I. AB0130 Serum Leptin and Adiponectin Levels in Rheumatoid Arthritis Patients, Their Association with Inflammatory Process. Ann. Rheum. Dis. 2018, 77, 1257–1258. [Google Scholar]
- Curtis, J.R.; van der Helm-van Mil, A.H.; Knevel, R.; Huizinga, T.W.; Haney, D.J.; Shen, Y.; Ramanujan, S.; Cavet, G.; Centola, M.; Hesterberg, L.K.; et al. Validation of a Novel Multibiomarker Test to Assess Rheumatoid Arthritis Disease Activity. Arthritis Care Res. 2012, 64, 1794–1803. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Controls n = 51 | eRA n = 51 | p Value | |||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Age ± SD | 48.20 ± 11.13 | 48.86 ± 10.86 | 0.745 | ||
| BMI † | 24.52 (21.95–26.34) | 25.26 (23.38–28.58) | 0.051 | ||
| Sex | |||||
| Female | 41 | 80.39 | 41 | 80.39 | 0.521 |
| BMI > 25 | 17 | 33.33 | 26 | 50.98 | 0.019 * |
| Former smoker | 18 | 35.29 | 17 | 33.33 | 0.552 |
| Passive smoker | 11 | 21.56 | 8 | 15.68 | 0.242 |
| Occupational status | |||||
| Homemaker | 12 | 23.53 | 19 | 37.25 | 0.011 ** |
| Independent worker | 0 | 0.00 | 3 | 5.88 | |
| Employee | 36 | 70.59 | 21 | 41.18 | |
| Pensioner | 2 | 3.92 | 6 | 11.76 | |
| Student | 1 | 1.96 | 2 | 3.92 | |
| Marital status | |||||
| Single | 11 | 21.57 | 10 | 19.61 | 0.140 |
| Widowed | 6 | 11.76 | 2 | 3.92 | |
| Common-law marriage | 9 | 17.65 | 6 | 11.76 | |
| Separated | 5 | 9.80 | 3 | 5.88 | |
| Education level | |||||
| Elementary school | 10 | 19.61 | 6 | 11.76 | 0.764 |
| High school | 11 | 21.57 | 15 | 29.41 | |
| Technician | 11 | 21.57 | 8 | 15.69 | |
| College | 19 | 37.25 | 22 | 43.14 | |
| Controls n = 51 | eRA n = 51 | p Value | |||
|---|---|---|---|---|---|
| n | % | n | % | ||
| IgG1 P. gingivalis > 1/100 titers | 29 | 56.86 | 17 | 33.33 | 0.015 * |
| IgG1 P. gingivalis > 1/400 titers | 18 | 35.29 | 8 | 15.69 | 0.035 * |
| IgG2 P. gingivalis > 1/100 titers | 31 | 60.78 | 14 | 27.45 | 0.003 * |
| IgG2 P. gingivalis > 1/400 titers | 15 | 29.41 | 4 | 7.84 | 0.012 * |
| IgG1 and IgG2 P. gingivalis | 37 | 72.55 | 20 | 39.22 | 0.002 * |
| P. gingivalis presence | 23 | 45.10 | 40 | 78.43 | 0.003 * |
| P. gingivalis by qPCR > 4 CFU | 22 | 43.14 | 31 | 60.78 | 0.120 |
| Periodontal disease diagnostic | |||||
| No compromise | 15 | 29.41 | 14 | 27.45 | 0.575 |
| Periodontitis | 36 | 70.59 | 37 | 72.55 | |
| Severity of periodontal disease | |||||
| No compromise | 15 | 29.41 | 14 | 27.45 | |
| Mild | 5 | 9.80 | 6 | 11.76 | 0.411 |
| Moderate | 27 | 52.94 | 21 | 41.18 | |
| Severe | 4 | 7.84 | 10 | 19.61 | |
|
Tertile 1
Low Levels |
Tertile 2
Medium Levels |
Tertile 3
High Levels | Median | |
|---|---|---|---|---|
| Adiponectin (pg/mL) | 0.001–28,303.75 | 28,303.76–41,753.2 | >41,753.2 | 34,769.60 |
| Leptin (ng/mL) | 0.001–0.15 | 0.16–1.67 | >1.67 | 0.18 |
| IL-6 (pg/mL) | 0.001–1.0 | 1.1–2.29 | >2.29 | 1.0 |
| Resistin (pg/mL) | 0.001–16.83 | 16.84–65.69 | >65.69 | 49.34 |
| Adipsin (pg/mL) | 0.001–3076.9 | 3076.9–8729.5 | >8729.58 | 7728.36 |
| Vaspin (pg/mL) | 0.001–68.80 | 68.81–1273.1 | >1273.19 | 87.50 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romero-Sánchez, C.; De Avila, J.; Ramos-Casallas, A.; Chila-Moreno, L.; Delgadillo, N.A.; Chalem-Choueka, P.; Pacheco-Tena, C.; Bello-Gualtero, J.M.; Bautista-Molano, W. High Levels of Leptin and Adipsin Are Associated with Clinical Activity in Early Rheumatoid Arthritis Patients with Overweight and Periodontal Infection. Diagnostics 2023, 13, 1126. https://doi.org/10.3390/diagnostics13061126
Romero-Sánchez C, De Avila J, Ramos-Casallas A, Chila-Moreno L, Delgadillo NA, Chalem-Choueka P, Pacheco-Tena C, Bello-Gualtero JM, Bautista-Molano W. High Levels of Leptin and Adipsin Are Associated with Clinical Activity in Early Rheumatoid Arthritis Patients with Overweight and Periodontal Infection. Diagnostics. 2023; 13(6):1126. https://doi.org/10.3390/diagnostics13061126
Chicago/Turabian StyleRomero-Sánchez, Consuelo, Juliette De Avila, Alejandro Ramos-Casallas, Lorena Chila-Moreno, Nathaly Andrea Delgadillo, Philippe Chalem-Choueka, César Pacheco-Tena, Juan Manuel Bello-Gualtero, and Wilson Bautista-Molano. 2023. "High Levels of Leptin and Adipsin Are Associated with Clinical Activity in Early Rheumatoid Arthritis Patients with Overweight and Periodontal Infection" Diagnostics 13, no. 6: 1126. https://doi.org/10.3390/diagnostics13061126