
Factors Associated with Large Renal Function Decline in Patients with Chronic Hepatitis C Successfully Treated with Direct-Acting Antiviral Therapy
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
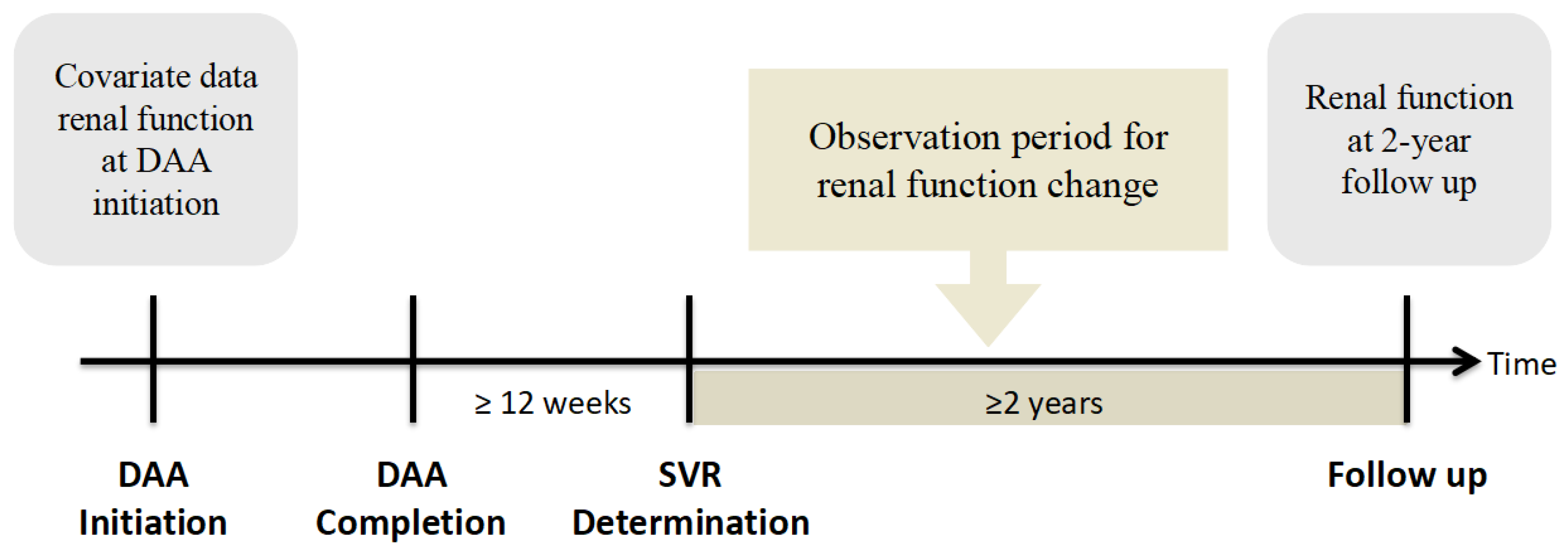
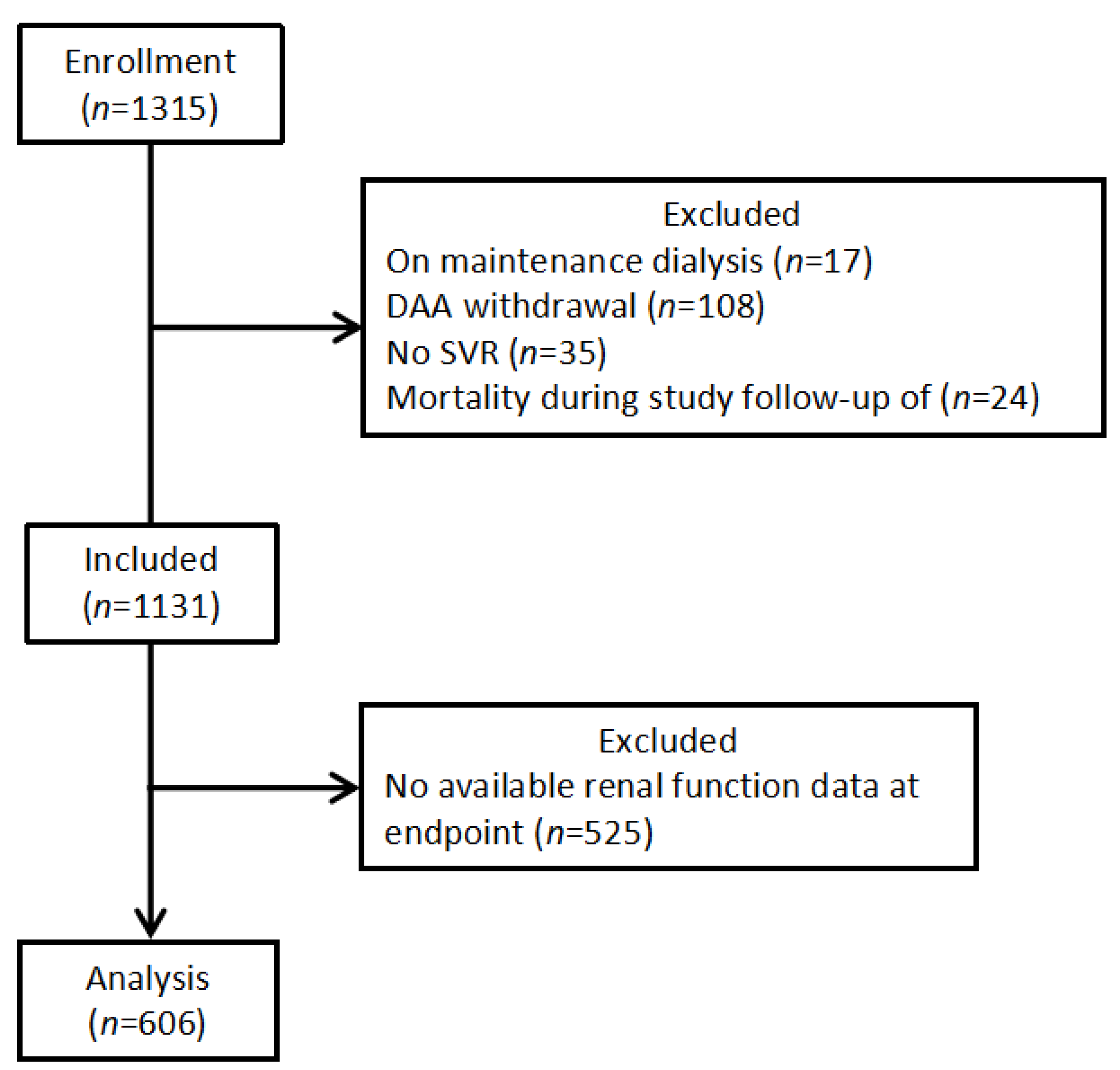
2.1. Study Design and Patient Population
2.2. Assessments and Measurement of Clinical Parameters
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Study Cohort
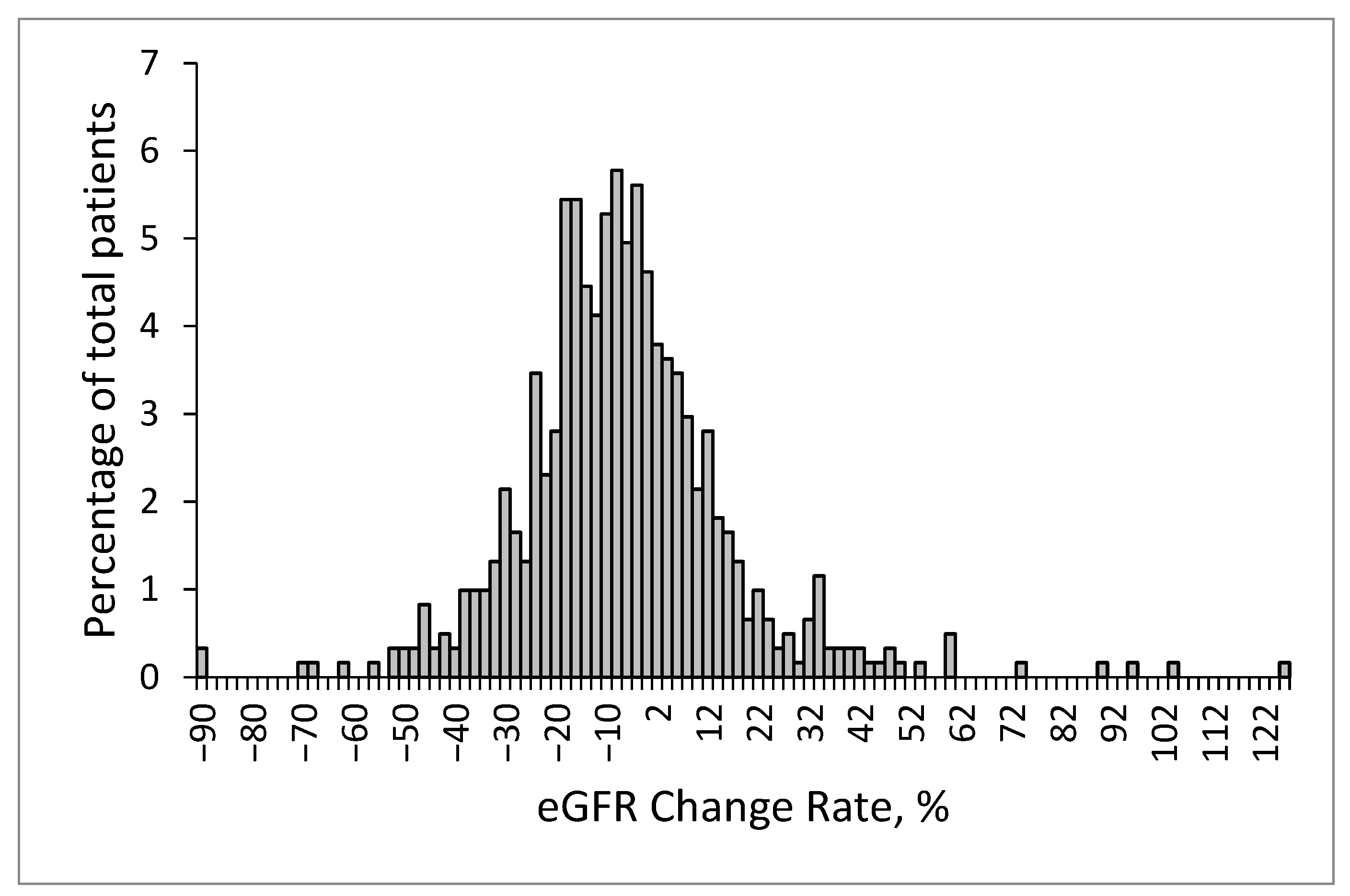
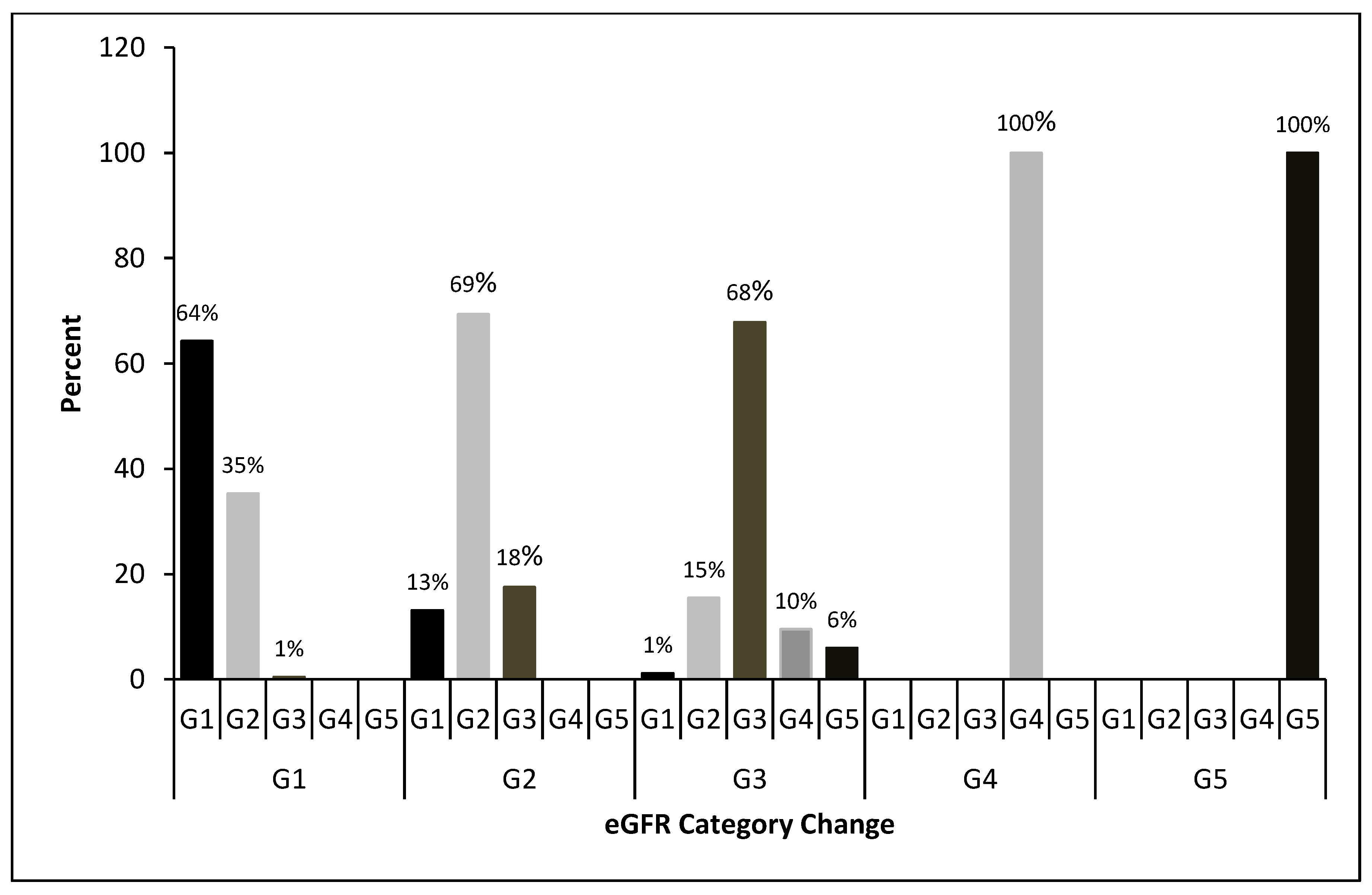
3.2. Renal Function Change
3.3. Multivariable Models for a Large eGFR Decline
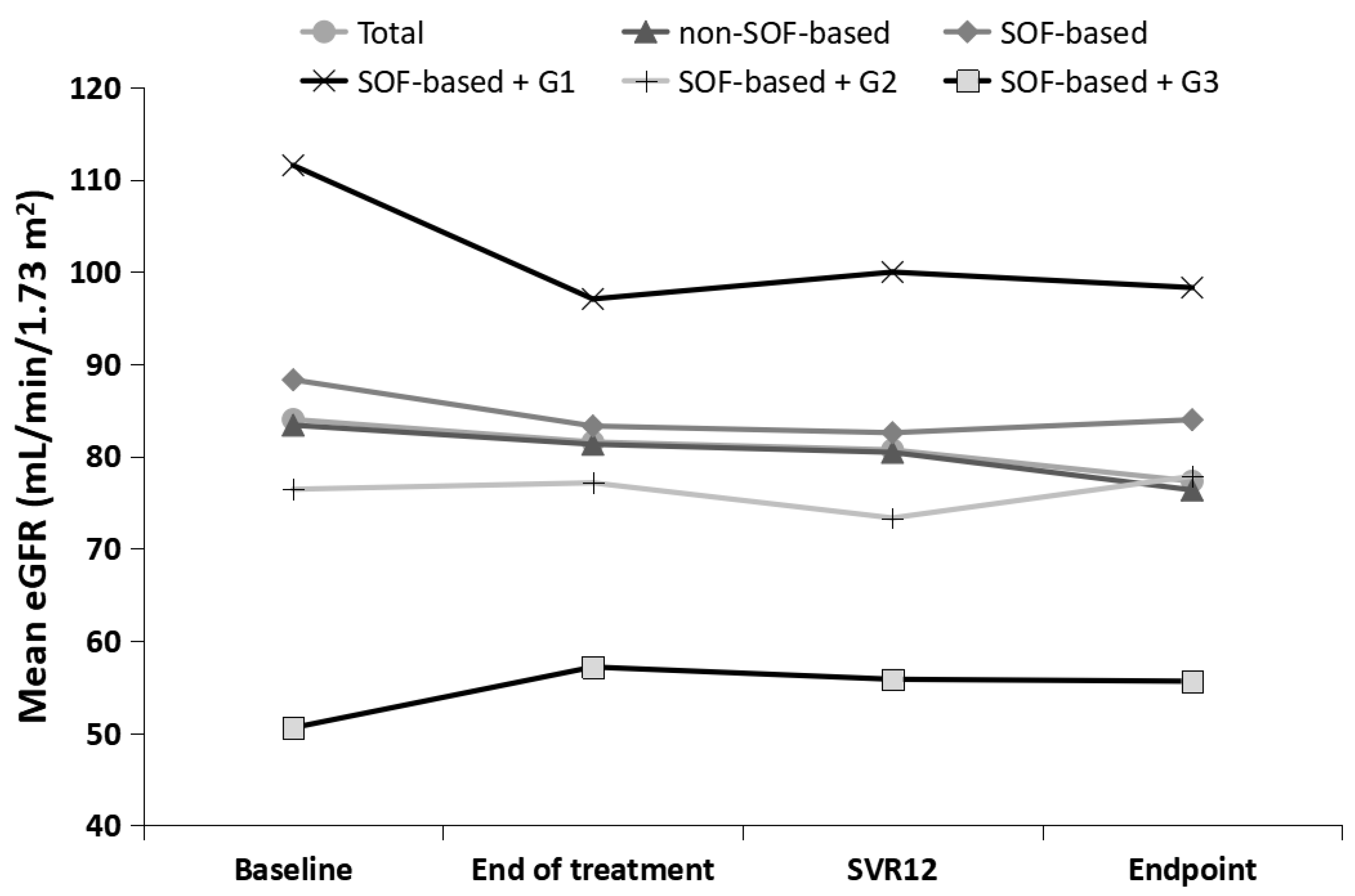
3.4. Impact of SOF-Based Treatment on Renal Function
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thrift, A.P.; Hashem, B.E.-S.; Fasiha, K. Global epidemiology and burden of HCV infection and HCV-related disease. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 122–132. [Google Scholar] [CrossRef]
- van der Meer, A.J.; Marina, B. Reversion of disease manifestations after HCV eradication. J. Hepatol. 2016, 65, S95–S108. [Google Scholar] [CrossRef] [Green Version]
- Mohanty, A.; Sarah, S.; Adeel, A.B. Impact of direct acting antiviral agent therapy upon extrahepatic manifestations of hepatitis C virus infection. Curr. HIV/AIDS Rep. 2019, 16, 389–394. [Google Scholar] [CrossRef]
- Lanini, S.; Scognamiglio, P.; Pisapia, R.; Minosse, C.; Agresta, A.; Ippolito, G. Recovery of metabolic impairment in patients who cleared chronic hepatitis C infection after direct-acting antiviral therapy. Int. J. Antimicrob. Agents 2019, 53, 559–563. [Google Scholar] [CrossRef]
- Liu, C.H.; Lin, J.W.; Liu, C.J.; Su, T.H.; Wu, J.H.; Tseng, T.C.; Chen, P.J.; Kao, J.H. Long-term Evolution of Estimated Glomerular Filtration Rate in Patients with Antiviral Treatment for Hepatitis C Virus Infection. Clin. Gastroenterol. Hepatol. 2022, in press. [Google Scholar] [CrossRef]
- Sadler, M.D.; Samuel, S.L. Revolution in hepatitis C antiviral therapy. Br. Med. Bull. 2015, 113, 31–44. [Google Scholar] [CrossRef] [Green Version]
- Chien, R.N.; Lu, S.N.; Pwu, R.F.; Wu, G.H.; Yang, W.W.; Liu, C.L. Taiwan accelerates its efforts to eliminate hepatitis C. Glob. Health Med. 2021, 5, 293–300. [Google Scholar] [CrossRef]
- World Health Organization Global Hepatitis Report; WHO: Geneva, Switzerland, 2017; Available online: https://apps.who.int/iris/bitstream/handle/10665/255016/9789?sequence=1 (accessed on 20 September 2022).
- El-Serag, H.B.; Christie, I.C.; Puenpatom, A.; Castillo, D.; Kanwal, F.; Kramer, J.R. The effects of sustained virological response to direct-acting anti-viral therapy on the risk of extrahepatic manifestations of hepatitis C infection. Aliment. Pharmacol. Ther. 2019, 49, 442–1447. [Google Scholar] [CrossRef]
- Sise, M.E. Direct-acting antiviral therapy slows kidney function decline in patients with hepatitis C virus infection and chronic kidney disease. Kidney Int. 2020, 97, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Fabrizi, F.; Cerutti, R.; Alfieri, C.M.; Ridruejo, E. Impact of antiviral therapy with Direct Acting Antiviral Agents (DAAs) on kidney disease in patients with chronic hepatitis C. Minerva Gastroenterol. 2021, 67, 244–253. [Google Scholar] [CrossRef]
- Elmowafy, A.Y.; El Maghrabi, H.M.; Mashaly, M.E.; Eldahshan, K.F.; Rostaing, L.; Bakr, M.A. High rate of acute kidney injury in patients with chronic kidney disease and hepatitis C virus genotype 4 treated with direct-acting antiviral agents. Int. Urol. Nephrol. 2019, 51, 2243–2254. [Google Scholar] [CrossRef] [PubMed]
- Duque, J.C.; Dejman, A.; Venkat, V.; Hernandez, M.; Roth, D.; Ladino, M.A. Acute interstitial nephritis following treatment with direct-acting antiviral agents in hepatitis C virus-infected patients: A case series. Clin. Nephrol. 2021, 95, 22–27. [Google Scholar] [CrossRef]
- Tsai, M.C.; Lin, C.Y.; Hung, C.H.; Lu, S.N.; Tung, S.Y.; Chien, R.N.; Lin, C.L.; Wang, J.H.; Chien-Hung, C.; Chang, K.C.; et al. Evolution of renal function under direct-acting antivirals treatment for chronic hepatitis C: A real-world experience. J. Viral Hepat. 2019, 26, 1404–1412. [Google Scholar] [CrossRef]
- Driedger, M.; Chrissi, G.; Curtis, C. Direct acting antiviral HCV treatment does not influence renal function. Medicine 2020, 99, e20436. [Google Scholar] [CrossRef]
- Wai, C.T.; Greenson, J.K.; Fontana, R.J.; Kalbfleisch, J.D.; Marrero, J.A.; Conjeevaram, H.S.; Lok, A.S. A simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C. Hepatology 2003, 38, 518–526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garabed, E.; Norbert, L.; Bertram, L.K. Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Update Work Group. KDIGO 2017 Clinical practice guideline update for the diagnosis, evaluation, prevention, and treatment of chronic kidney disease–mineral and bone disorder (CKD-MBD). Kidney Int. Suppl. 2017, 7, 1–59. [Google Scholar]
- Khattab, M.A.; Mohammed, E.; Seyed, M.A. Hepatitis C virus as a multifaceted disease: A simple and updated approach for extrahepatic manifestations of hepatitis C virus infection. Hepat. Mon. 2010, 10, 258–269. [Google Scholar]
- Sulkowski, M.; Telep, L.E.; Colombo, M.; Durand, F.; Reddy, K.R.; Lawitz, E.; Bourlière, M.; Cheinquer, N.; Scherbakovsky, S.; Ni, L.; et al. Sofosbuvir and risk of estimated glomerular filtration rate decline or end-stage renal disease in patients with renal impairment. Aliment. Pharmacol. Ther. 2022, 55, 1169–1178. [Google Scholar] [CrossRef]
- Su, P.K.; Chang, T.S.; Tung, S.Y.; Wei, K.L.; Shen, C.H.; Hsieh, Y.Y.; Chen, W.M.; Chen, Y.H.; Chen, C.H.; Yen, C.W.; et al. Changes in renal function in patients with chronic hepatitis C treated with sofosbuvir-velpatasvir. Adv. Dig. Med. 2022, 1–9. [Google Scholar] [CrossRef]
- Liu, C.H.; Lee, M.H.; Lin, J.W.; Liu, C.J.; Su, T.H.; Tseng, T.C.; Chen, P.J.; Chen, D.S.; Kao, J.H. Evolution of eGFR in chronic HCV patients receiving sofosbuvir-based or sofosbuvir-free direct-acting antivirals. J. Hepatol. 2020, 72, 839–846. [Google Scholar] [CrossRef]
- Saxena, V.; Koraishy, F.M.; Sise, M.E.; Lim, J.K.; Schmidt, M.; Chung, R.T.; Liapakis, A.; Nelson, D.R.; Fried, M.W.; Terrault, N.A. HCV-TARGET. Safety and efficacy of sofosbuvir-containing regimens in hepatitis C-infected patients with impaired renal function. Liver Int. 2016, 36, 807–816. [Google Scholar] [CrossRef]
- Liu, C.H.; Chen, P.Y.; Chen, J.J.; Lo, C.C.; Su, W.W.; Tseng, K.C.; Liu, C.J.; Huang, C.S.; Huang, K.J.; Yang, S.S.; et al. Sofosbuvir/velpatasvir for patients with chronic hepatitis C virus infection and compensated liver disease: Real-world data in Taiwan. Hepatol. Int. 2021, 15, 338–349. [Google Scholar] [CrossRef] [PubMed]
- Okubo, T.; Atsukawa, M.; Tsubota, A.; Toyoda, H.; Shimada, N.; Abe, H.; Kato, K.; Hayama, K.; Arai, T.; Nakagawa-Iwashita, A.; et al. Efficacy and safety of ledipasvir/sofosbuvir for genotype 1b chronic hepatitis C patients with moderate renal impairment. Hepatol. Int. 2018, 12, 133–142. [Google Scholar] [CrossRef]
- D’Ambrosio, R.; Pasulo, L.; Giorgini, A.; Spinetti, A.; Messina, E.; Fanetti, I.; Puoti, M.; Aghemo, A.; Viganò, P.; Vinci, M.; et al. Renal safety in 3264 HCV patients treated with DAA-based regimens: Results from a large Italian real-life study. Dig. Liver Dis. 2020, 52, 190–198. [Google Scholar] [CrossRef]
- Huang, C.F.; Tseng, K.C.; Cheng, P.N.; Hung, C.H.; Lo, C.C.; Peng, C.Y.; Bair, M.J.; Yeh, M.L.; Chen, C.H.; Lee, P.L.; et al. Impact of Sofosbuvir-based direct-acting antivirals on renal function in chronic hepatitis C patients with impaired renal function: A large Cohort Study from the Nationwide HCV Registry Program (TACR). Clin. Gastroenterol. Hepatol. 2022, 20, 1151–1162. [Google Scholar] [CrossRef]
- O’Donnell, A.; Pham, N.; Battisti, L.; Epstein, R.; Nunes, D.; Sawinski, D.; Lodi, S. Estimating the causal effect of treatment with direct-acting antivirals on kidney function among individuals with hepatitis C virus infection. PLoS ONE 2022, 17, e0268478. [Google Scholar] [CrossRef]
- Ku, E.; Lee, B.J.; Wei, J.; Weir, M.R. Hypertension in CKD: Core curriculum 2019. Am. J. Kidney Dis. 2019, 74, 120–131. [Google Scholar] [CrossRef] [Green Version]
- Sasso, F.C.; Pafundi, P.C.; Caturano, A.; Galiero, R.; Vetrano, E.; Nevola, R.; Petta, S.; Fracanzani, A.L.; Coppola, C.; Di Marco, V.; et al. Impact of direct acting antivirals (DAAs) on cardiovascular events in HCV cohort with pre-diabetes. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 2345–2353. [Google Scholar] [CrossRef]
- Adinolfi, L.E.; Jacobson, I.; Bondin, M.; Cacoub, P. Expert opinion on managing chronic HCV infection in patients with type 2 diabetes mellitus. Antivir. Ther. 2018, 23 (Suppl. S2), 11–21. [Google Scholar] [CrossRef]
- Villani, R.; Romano, A.D.; Sangineto, M.; Serviddio, G. Direct-acting antivirals improve kidney function in diabetic patients with HCV infection and chronic kidney disease. Intern. Emerg. Med. 2021, 16, 1239–1245. [Google Scholar] [CrossRef]
- Hum, J.; Jou, J.H.; Green, P.K.; Berry, K.; Lundblad, J.; Hettinger, B.D.; Chang, M.; Ioannou, G.N. Improvement in glycemic control of type 2 diabetes after successful treatment of hepatitis C virus. Diabetes Care 2017, 40, 1173–1180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alicic, R.Z.; Michele, T.R.; Katherine, R.T. Diabetic kidney disease: Challenges, progress, and possibilities. Clin. J. Am. Soc. Nephrol. CJASN 2017, 12, 2032–2045. [Google Scholar] [CrossRef] [PubMed]
- Moman, R.N.; Gupta, N.; Varacallo, M. Physiology, Albumin. In StatPearls; StatPearls Publishing: Tampa, FL, USA.
- Terawaki, H.; Yoshimura, K.; Hasegawa, T.; Matsuyama, Y.; Negawa, T.; Yamada, K.; Matsushima, M.; Nakayama, M.; Hosoya, T.; Era, S. Oxidative stress is enhanced in correlation with renal dysfunction: Examination with the redox state of albumin. Kidney Int. 2004, 66, 1988–1993. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Ji, X.; Ni, W.; Luo, Y.; Ding, B.; Ma, J.; Zhu, J. Serum albumin and albuminuria predict the progression of chronic kidney disease in patients with newly diagnosed type 2 diabetes: A retrospective study. PeerJ 2021, 9, e11735. [Google Scholar] [CrossRef]
- Foley, R.N.; Parfrey, P.S.; Harnett, J.D.; Kent, G.M.; Murray, D.C.; Barre, P.E. Hypoalbuminemia, cardiac morbidity, and mortality in end-stage renal disease. J. Am. Soc. Nephrol. 1996, 7, 728–736. [Google Scholar] [CrossRef]
- Amano, H.; Yoshimura, K.; Iijima, R.; Waki, K.; Matsumoto, K.; Ueda, H.; Ito, Y.; Akimoto, K.; Yokoo, T.; Inoue, K.; et al. A slight decrease in the serum albumin level is associated with the rapid progression of kidney dysfunction, even within the normal range. Intern. Med. 2020, 59, 2679–2685. [Google Scholar] [CrossRef] [PubMed]
- Baba, M.; Shimbo, T.; Horio, M.; Ando, M.; Yasuda, Y.; Komatsu, Y.; Masuda, K.; Matsuo, S.; Maruyama, S. Longitudinal study of the decline in renal function in healthy subjects. PLoS ONE 2015, 10, e0129036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, C.K.; Chen, L.W.; Chang, T.S.; Tung, S.Y.; Lin, C.Y.; Hung, C.H.; Lu, S.N.; Lin, C.L.; Chen, C.H.; Hsu, C.W.; et al. The Novel Finding of Dynamic Change in eGFR up to One Year after End of Treatment in HCV-Infected Patients Receiving Sofosbuvir and Velpatasvir. Viruses 2022, 14, 362. [Google Scholar] [CrossRef]
- Chiu, S.M.; Tsai, M.C.; Lin, C.Y.; Chen, C.H.; Lu, S.N.; Hung, C.H.; Sheen, I.S.; Chien, R.N.; Lin, C.L.; Hu, T.H.; et al. Serial changes of renal function after directly acting antivirals treatment for chronic hepatitis C: A 1-year follow-up study after treatment. PLoS ONE 2020, 15, e0231102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nevola, R.; Rinaldi, L.; Zeni, L.; Sasso, F.C.; Pafundi, P.C.; Guerrera, B.; Marrone, A.; Giordano, M.; Adinolfi, L.E. Metabolic and renal changes in patients with chronic hepatitis C infection after hepatitis C virus clearance by direct-acting antivirals. JGH Open 2020, 4, 713–721. [Google Scholar] [CrossRef] [PubMed]
- Ioannou, G.N.; Jordan, J.F. What are the benefits of a sustained virologic response to direct-acting antiviral therapy for hepatitis C virus infection? Gastroenterology 2019, 156, 446–460. [Google Scholar] [CrossRef] [PubMed]
- Rinaldi, L.; Perrella, A.; Guarino, M.; De Luca, M.; Piai, G.; Coppola, N.; Pafundi, P.C.; Ciardiello, F.; Fasano, M.; Martinelli, E.; et al. Incidence and risk factors of early HCC occurrence in HCV patients treated with direct acting antivirals: A prospective multicentre study. J. Transl. Med. 2019, 17, 292. [Google Scholar] [CrossRef] [PubMed]
- Adinolfi, L.E.; Petta, S.; Fracanzani, A.L.; Nevola, R.; Coppola, C.; Narciso, V.; Rinaldi, L.; Calvaruso, V.; Pafundi, P.C.; Lombardi, R.; et al. Reduced incidence of type 2 diabetes in patients with chronic hepatitis C virus infection cleared by direct-acting antiviral therapy: A prospective study. Diabetes Obes. Metab. 2020, 22, 2408–2416. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Patients (n = 606) | No or Mild eGFR Decline (<10%) | n | Large eGFR Decline (≥10%) | n | p Value | |
|---|---|---|---|---|---|---|
| Age, year | 67.0 (10.9) | 66.5 (11.2) | 355 | 67.8 (10.4) | 251 | 0.165 |
| Male gender, n (%) | 290 (47.9%) | 180 (50.7%) | 355 | 110 (43.8%) | 251 | 0.095 |
| Body weight, kg | 64.3 (12.0) | 64.4 (12.2) | 346 | 64.2 (11.7) | 245 | 0.830 |
| BMI, kg/m2 | 25.4 (3.9) | 25.3 (3.8) | 346 | 25.5 (4.0) | 245 | 0.596 |
| Current smoking, n (%) | 102 (16.8%) | 61 (17.2%) | 355 | 41 (16.3%) | 251 | 0.783 |
| Diabetes mellitus, n (%) | 185 (30.5%) | 102 (28.7%) | 355 | 83 (33.1%) | 251 | 0.254 |
| Hypertension, n (%) | 320 (52.8%) | 174 (49.0%) | 355 | 146 (58.2%) | 251 | 0.026 |
| Dyslipidemia, n (%) | 133 (21.9%) | 78 (22.0%) | 355 | 55 (21.9%) | 251 | 0.986 |
| HBsAg positive, n (%) | 77 (12.7%) | 47 (13.2%) | 355 | 30 (12.0%) | 251 | 0.639 |
| HCC, n (%) | 64 (10.6%) | 36 (10.1%) | 355 | 28 (11.2%) | 251 | 0.689 |
| Prior IFN, n (%) | 160 (26.4%) | 98 (27.6%) | 157 | 62 (24.7%) | 106 | 0.391 |
| AST, U/L | 61.8 (45.6) | 60.7 (45.3) | 355 | 63.4 (46.0) | 251 | 0.473 |
| ALT, U/L | 76.1 (71.7) | 73.6 (64.5) | 355 | 79.6 (80.8) | 251 | 0.312 |
| Albumin, g/dL | 4.2 (0.3) | 4.3 (0.3) | 355 | 4.2 (0.3) | 251 | 0.001 |
| Albumin ≤ 3.5 g/dL, n (%) | 23 (3.8%) | 13 (3.7%) | 355 | 10 (4.0%) | 251 | 0.838 |
| Total bilirubin, mg/dL | 0.8 (0.4) | 0.8 (0.3) | 355 | 0.8 (0.5) | 251 | 0.586 |
| Platelet, 103/μL | 167.3 (65.9) | 168.3 (66.1) | 355 | 166.0 (65.6) | 251 | 0.669 |
| FIB-4 score | 3.67 (2.86) | 3.61 (2.87) | 355 | 3.75 (2.85) | 251 | 0.552 |
| FIB-4 score, n (%) | 355 | 251 | ||||
| <1.45 | 112 (18.5%) | 71 (20.0%) | 41 (16.3%) | 0.252 | ||
| 1.45–3.25 | 237 (39.1%) | 130 (36.6%) | 107 (42.7%) | 0.135 | ||
| >3.25 | 257 (42.4%) | 154 (43.4%) | 103 (41.0%) | 0.565 | ||
| AFP, ng/mL | 8.7 (27.3) | 6.6 (8.8) | 355 | 11.6 (40.9) | 251 | 0.059 |
| HCV-RNA, 106 IU/mL | 12.0 (229.5) | 18.6 (299.8) | 355 | 2.7 (3.3) | 251 | 0.399 |
| HCV-RNA, log-transformed | 5.9 (0.9) | 5.9 (0.9) | 355 | 5.9 (1.0) | 251 | 0.418 |
| HCV genotype, n (%) | 355 | 251 | ||||
| 1a | 9 (1.5%) | 5 (1.4%) | 4 1.6(%) | 1.000 | ||
| 1b | 436 (71.9%) | 260 (73.2%) | 176 (70.1%) | 0.400 | ||
| 2 | 140 (23.1%) | 81 (22.8%) | 59 (23.5%) | 0.843 | ||
| 3 | 1 (0.2%) | 0 (0%) | 1 (0.4%) | 0.414 | ||
| 6 | 8 (1.3%) | 4 (1.1%) | 4 (1.6%) | 0.724 | ||
| mixed | 12 (2.0%) | 5 (1.4%) | 7 (2.8%) | 0.250 | ||
| DAAs, n (%) | 355 | 251 | ||||
| DCV/ASV | 38 (6.3%) | 22 (6.2%) | 16 (6.4%) | 0.929 | ||
| ProD | 119 (19.6%) | 73 (20.6%) | 46 (18.3%) | 0.495 | ||
| Zepatier | 217 (35.8%) | 134 (37.7%) | 83 (33.1%) | 0.237 | ||
| Maviret | 45 (7.4%) | 22 (6.2%) | 23 (9.2%) | 0.170 | ||
| SOF-based | 187 (30.9%) | 104 (29.3%) | 83 (33.1%) | 0.322 | ||
| Ribavirin use, n (%) | 87 (14.4%) | 46 (13.0%) | 355 | 41 (16.3%) | 251 | 0.243 |
| Hemoglobin, g/dL | 13.8 (1.7) | 13.9 (1.7) | 355 | 13.7 (1.7) | 251 | 0.150 |
| Fasting plasma glucose, mg/dL | 115.8 (39.3) | 115.3 (37.9) | 200 | 116.6 (41.5) | 135 | 0.768 |
| Creatinine, mg/dL | 0.91 (0.33) | 0.94 (0.34) | 355 | 0.87 (0.32) | 251 | 0.016 |
| eGFR, mL/min/1.73 m2 | 84.11 (24.38) | 81.74 (22.82) | 355 | 87.45 (26.10) | 251 | 0.005 |
| eGFR category, n (%) | 355 | 251 | ||||
| G1: ≥90 mL/min/1.73 m2 | 221 (36.5%) | 114 (32.1%) | 107 (42.6%) | 0.008 | ||
| G2: 60–89 mL/min/1.73 m2 | 297 (49.0%) | 186 (52.4%) | 111 (44.2%) | 0.047 | ||
| G3: 30–59 mL/min/1.73 m2 | 84 (13.9%) | 52 (14.6%) | 32 (12.7%) | 0.505 | ||
| G4: 15–29 mL/min/1.73 m2 | 3 (0.5%) | 3 (0.8%) | 0 (0%) | 0.271 | ||
| G5: <15 mL/min/1.73 m2 | 1 (0.2%) | 0 (0%) | 1 (0.4%) | 0.414 |
| Variables | Univariate | Multivariate | ||
|---|---|---|---|---|
| OR (95%CI) | p Value | OR (95%CI) | p Value | |
| Age, year | 1.011 (0.996–1.026) | 0.166 | 1.015 (0.997–1.034) | 0.113 |
| Gender, Male vs. Female | 0.758 (0.548–1.049) | 0.095 | 0.770 (0.544–1.090) | 0.141 |
| Body weight, kg | 0.999 (0.985–1.012) | 0.830 | ||
| BMI, kg/m2 | 1.011 (0.970–1.054) | 0.596 | 1.016 (0.970–1.064) | 0.505 |
| Current smoking, Yes vs. No | 0.941 (0.610–1.452) | 0.783 | ||
| Diabetes mellitus, Yes vs. No | 1.225 (0.864–1.738) | 0.254 | 1.283 (0.878–1.876) | 0.198 |
| Hypertension, Yes vs. No | 1.446 (1.044–2.004) | 0.026 | 1.481 (1.010–2.173) | 0.044 |
| Dyslipidemia, Yes vs. No | 0.997 (0.674–1.473) | 0.986 | ||
| HBsAg positive, Yes vs. No | 0.890 (0.545–1.451) | 0.639 | ||
| HCC, Yes vs. No | 1.113 (0.660–1.876) | 0.689 | ||
| AST, U/L | 1.001 (0.998–1.005) | 0.473 | ||
| ALT, U/L | 1.001 (0.999–1.003) | 0.314 | ||
| Albumin, g/dL | 0.500 (0.325–0.768) | 0.002 | 0.546 (0.342–0.872) | 0.011 |
| Total bilirubin, mg/dL | 1.099 (0.781–1.548) | 0.588 | ||
| Platelet, 103/μL | 0.999 (0.997–1.002) | 0.668 | ||
| FIB-4 score | 1.017 (0.962–1.076) | 0.552 | ||
| <1.45 | Reference | |||
| 1.45–3.25 | 1.425 (0.898–2.262) | 0.133 | ||
| >3.25 | 1.158 (0.732–1.832) | 0.530 | ||
| AFP, ng/mL | 1.014 (1.001–1.026) | 0.035 | 1.007 (0.995–1.019) | 0.258 |
| HCV-RNA, 106 IU/mL | 0.999 (0.996–1.002) | 0.644 | ||
| HCV genotype | ||||
| 1a | NA a | |||
| 1b | Reference | |||
| 2 | 1.076 (0.731–1.583) | 0.710 | ||
| 3 | NA a | |||
| 6 | NA a | |||
| Mixed | NA a | |||
| DAAs | ||||
| DCV/ASV | 0.911 (0.450–1.845) | 0.796 | ||
| ProD | 0.790 (0.494–1.261) | 0.323 | ||
| Zepatier | 0.776 (0.521–1.155) | 0.212 | ||
| Maviret | 1.310 (0.683–2.514) | 0.417 | ||
| SOF-based | Reference | |||
| SOF-based, Yes vs. No | 1.192 (0.842–1.689) | 0.322 | 1.190 (0.754–1.878) | 0.455 |
| Ribavirin use, Yes vs. No | 1.311 (0.831–2.069) | 0.244 | 1.123 (0.614–2.054) | 0.706 |
| Hemoglobin, g/dL | 0.933 (0.849–1.025) | 0.151 | ||
| Fasting plasma glucose, mg/dL | 1.001 (0.995–1.006) | 0.767 | ||
| Creatinine, mg/dL | 0.510 (0.293–0.890) | 0.018 | ||
| eGFR, mL/min/1.73 m2 | 1.010 (1.003–1.017) | 0.005 | 1.016 (1.007–1.024) | <0.001 |
| eGFR category, n (%) | ||||
| G1: ≥90 mL/min/1.73 m2 | Reference | |||
| G2: 60–89 mL/min/1.73 m2 | 0.636 (0.447–0.905) | 0.012 | ||
| G3: 30–59 mL/min/1.73 m2 | 0.656 (0.392–1.095) | 0.107 | ||
| G4: 15–29 mL/min/1.73 m2 | NA a | |||
| G5: <15 mL/min/1.73 m2 | NA a | |||
| Baseline | End of Treatment | SVR12 | Endpoint | |
|---|---|---|---|---|
| Total (n = 439) | 83.99 ± 24.65 | 81.55 ± 23.42 | 80.69 ± 24.76 | 77.30 ± 24.55 |
| Reference | p < 0.001 | p < 0.001 | p < 0.001 | |
| Non-SOF-based (n = 384) | 83.37 ± 24.51 | 81.30 ± 23.94 | 80.43 ± 24.82 | 76.35 ± 24.62 |
| Reference | p = 0.001 | p < 0.001 | p < 0.001 | |
| SOF-based (n = 55) | 88.29 ± 25.43 | 83.28 ± 19.54 | 82.55 ± 24.46 | 83.96 ± 23.20 |
| Reference | p = 0.037 | p = 0.007 | p = 0.073 | |
| G1 (n = 23) | 111.54 ± 19.71 | 97.05 ± 18.11 | 99.97 ± 23.91 | 98.28 ± 21.72 |
| Reference | p = 0.002 | p = 0.001 | p < 0.001 | |
| G2 (n = 26) | 76.43 ± 7.89 | 77.13 ± 12.07 | 73.32 ± 15.09 | 77.83 ± 17.58 |
| Reference | p = 0.776 | p = 0.314 | p = 0.700 | |
| G3 (n = 6) | 50.58 ± 6.40 | 57.16 ± 8.04 | 55.83 ± 10.44 | 55.62 ± 9.46 |
| Reference | p = 0.137 | p = 0.317 | p = 0.248 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.-H.; Shen, C.-H.; Wei, K.-L.; Xu, H.-W.; Chen, W.-M.; Chang, K.-C.; Huang, Y.-T.; Hsieh, Y.-Y.; Lu, S.-N.; Hung, C.-H.; et al. Factors Associated with Large Renal Function Decline in Patients with Chronic Hepatitis C Successfully Treated with Direct-Acting Antiviral Therapy. Diagnostics 2023, 13, 473. https://doi.org/10.3390/diagnostics13030473
Chen C-H, Shen C-H, Wei K-L, Xu H-W, Chen W-M, Chang K-C, Huang Y-T, Hsieh Y-Y, Lu S-N, Hung C-H, et al. Factors Associated with Large Renal Function Decline in Patients with Chronic Hepatitis C Successfully Treated with Direct-Acting Antiviral Therapy. Diagnostics. 2023; 13(3):473. https://doi.org/10.3390/diagnostics13030473
Chicago/Turabian StyleChen, Chun-Hsien, Chien-Heng Shen, Kuo-Liang Wei, Huang-Wei Xu, Wei-Ming Chen, Kao-Chi Chang, Yu-Ting Huang, Yung-Yu Hsieh, Sheng-Nan Lu, Chao-Hung Hung, and et al. 2023. "Factors Associated with Large Renal Function Decline in Patients with Chronic Hepatitis C Successfully Treated with Direct-Acting Antiviral Therapy" Diagnostics 13, no. 3: 473. https://doi.org/10.3390/diagnostics13030473