
Radiomics and Artificial Intelligence Can Predict Malignancy of Solitary Pulmonary Nodules in the Elderly

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients Selection
2.2. The Radiomic Feature Set
- First-order features: this category described the distribution of voxel intensities within the region of interest (ROI), which in this study was related to the areas in the magnetic resonance image (MRI) associated with cancer. One feature belonging to this category was considered.
- Shape: this feature category included descriptors of the three-dimensional size and shape of the ROI. These features were independent of the gray level intensity distribution in the ROI and therefore were only calculated on the basis of non-derived images and masks. Fourteen features belonging to this category were considered.
- Gray-Level Co-occurrence Matrix (GLCM): this category considered the spatial relationships of pixels in the gray-level co-occurrence matrix, i.e., the gray-level spatial dependence matrix. The GLCM functions characterized the texture of an image by computing how often pairs of pixels with specific values and in a specified spatial relationship occurred in an image, and then extracting measures from this matrix. Twenty-four different features belonging to this category were considered.
- Gray-Level Run Length Matrix (GLRLM): this category was related to the size of homogeneous runs for each gray level. It quantified gray-level runs, which were defined as the length (expressed as a number of pixels) of consecutive pixels that had the same gray-level value. Sixteen features belonging to this category were considered.
- Gray-Level Size Zone Matrix (GLSZM): the features of this category were used to quantify gray-level zones in an image. A gray--level zone was defined as the number of connected voxels that shared the same gray-level intensity. A voxel was considered connected if the distance was one according to the infinity norm. Sixteen different features were considered from this category.
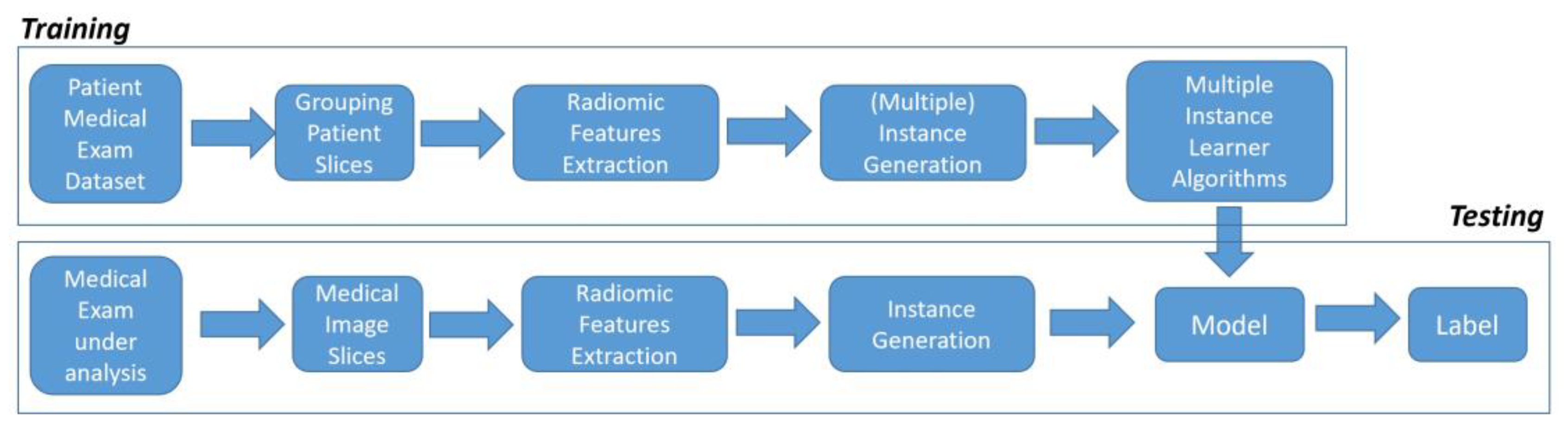
2.3. The Classification Process
2.4. Experimental Analysis
3. Results
3.1. Clinical Results
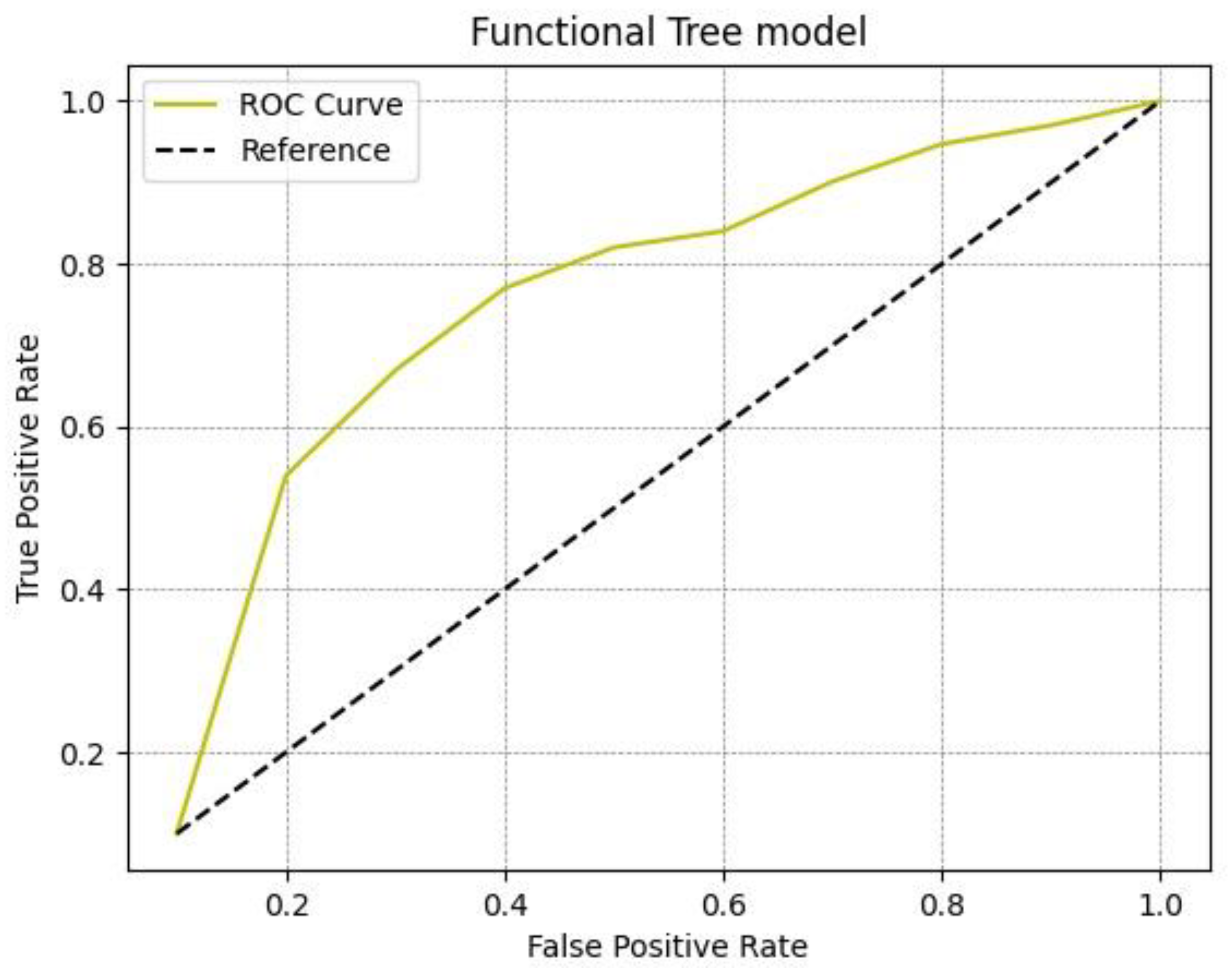
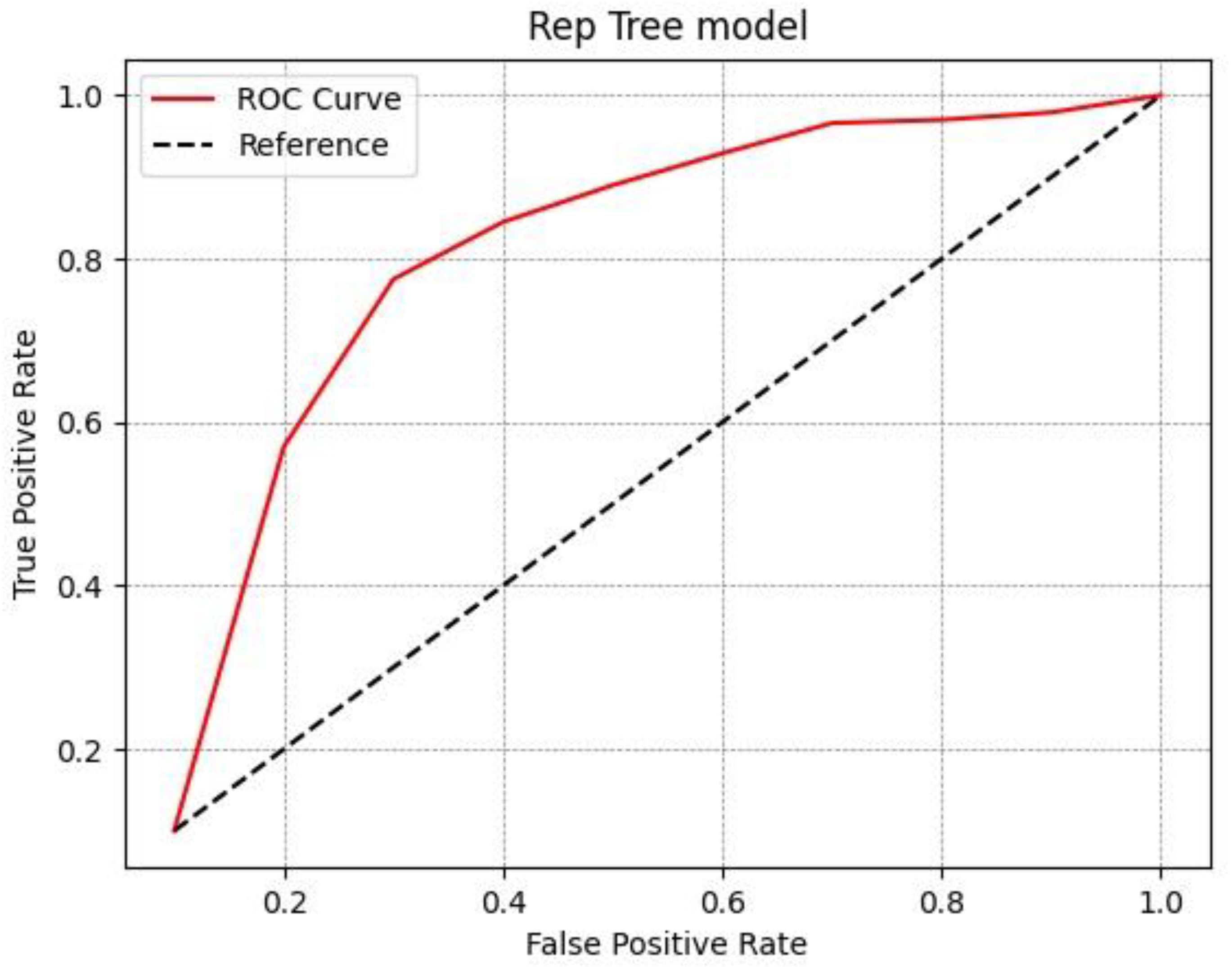
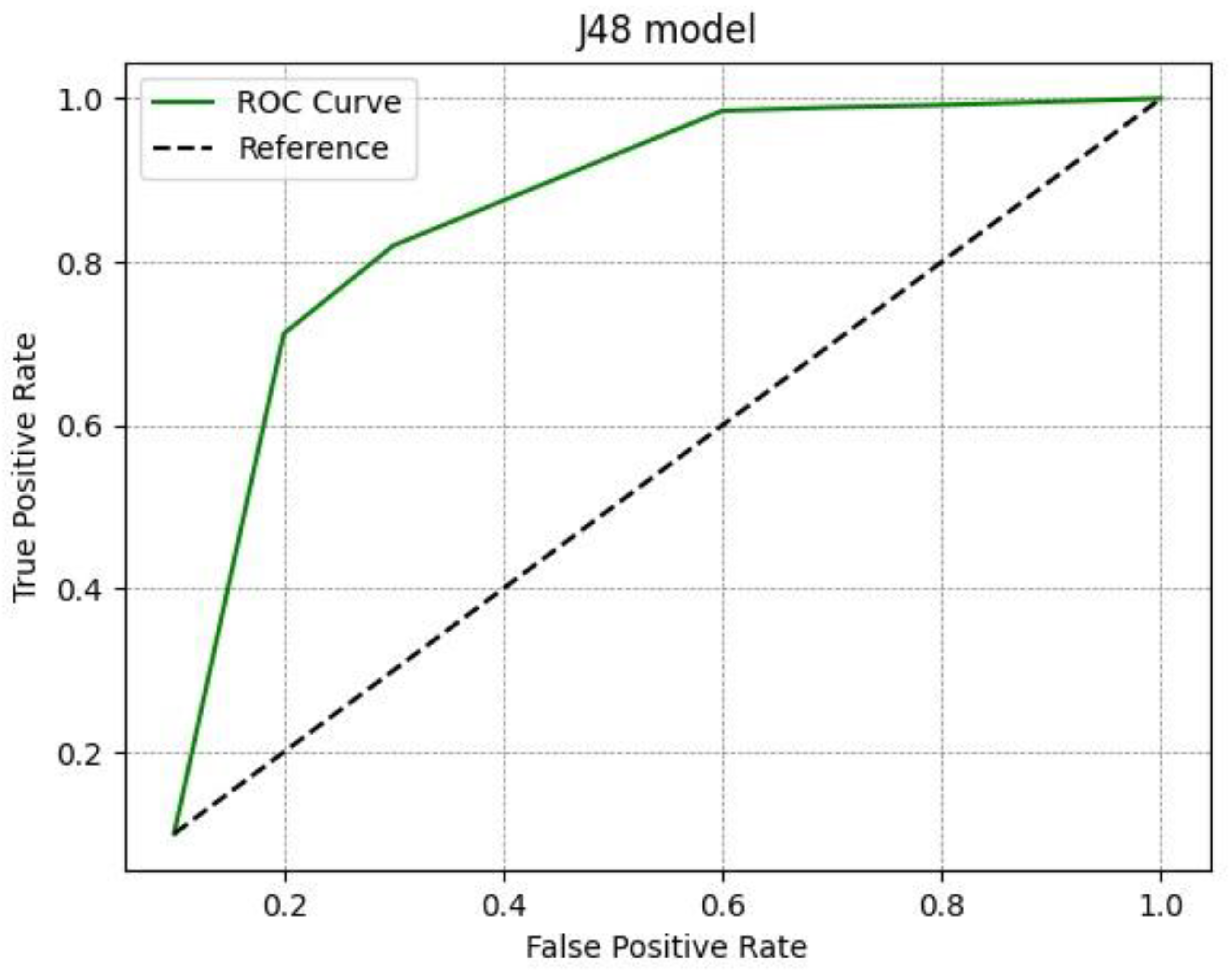
3.2. Results of AI-Integrated Radiomic Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- Detterbeck, F.C.; Boffa, D.J.; Kim, A.W.; Tanoue, L.T. The Eighth Edition Lung Cancer Stage Classification. Chest 2017, 151, 193–203. [Google Scholar] [CrossRef]
- Khan, A.N.; Al-Jahdali, H.H.; Irion, K.L.; Arabi, M.; Koteyar, S.S. Solitary pulmonary nodule: A diagnostic algorithm in the light of current imaging technique. Avicenna J. Med. 2011, 1, 39–51. [Google Scholar] [CrossRef]
- Gould, M.K.; Tang, T.; Liu, I.L.; Lee, J.; Zheng, C.; Danforth, K.N.; Kosco, A.E.; Di Fiore, J.L.; Suh, D.E. Recent Trends in the Identification of Incidental Pulmonary Nodules. Am. J. Respir. Crit. Care Med. 2015, 192, 1208–1214. [Google Scholar] [CrossRef]
- Modini, C.; Passariello, R.; Iascone, C.; Cicconetti, F.; Simonetti, G.; Zerilli, M.; Tirindelli-Danesi, D.; Stipa, S. TNM staging in lung cancer: Role of computed tomography. J. Thorac. Cardiovasc. Surg. 1982, 84, 569–574. [Google Scholar] [CrossRef]
- Brunelli, A.; Charloux, A.; Bolliger, C.T.; Rocco, G.; Sculier, J.P.; Varela, G.; Licker, M.; Ferguson, M.K.; Faivre-Finn, C.; Huber, R.M.; et al. ERS/ESTS clinical guidelines on fitness for radical therapy in lung cancer patients (surgery and chemo-radiotherapy). Eur. Respir. J. 2009, 34, 17–41. [Google Scholar] [CrossRef] [Green Version]
- Krochmal, R.; Arias, S.; Yarmus, L.; Feller-Kopman, D.; Lee, H. Diagnosis and management of pulmonary nodules. Expert Rev. Respir. Med. 2014, 8, 677–691. [Google Scholar] [CrossRef]
- Wilson, R.; Devaraj, A. Radiomics of pulmonary nodules and lung cancer. Transl. Lung Cancer Res. 2017, 6, 86–91. [Google Scholar] [CrossRef] [Green Version]
- Xiong, Z.; Jiang, Y.; Che, S.; Zhao, W.; Guo, Y.; Li, G.; Liu, A.; Li, Z. Use of CT Radiomics to Differentiate Minimally Invasive Adenocarcinomas and Invasive Adenocarcinomas Presenting as Pure Ground-Glass Nodules Larger Than 10 Mm. Eur. J. Radiol. 2021, 141, 109772. [Google Scholar] [CrossRef] [PubMed]
- Lambin, P.; Rios-Velazquez, E.; Leijenaar, R.; Carvalho, S.; van Stiphout, R.G.; Granton, P.; Zegers, C.M.; Gillies, R.; Boellard, R.; Dekker, A.; et al. Radiomics: Extracting more information from medical images using advanced feature analysis. Eur. J. Cancer 2012, 48, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.J.; Wu, F.Z.; Yang, S.C.; Tang, E.K.; Liang, C.H. Radiomics in Early Lung Cancer Diagnosis: From Diagnosis to Clinical Decision Support and Education. Diagnostic 2022, 12, 1064. [Google Scholar] [CrossRef] [PubMed]
- Bueno, J.; Landeras, L.; Chung, J.H. Updated Fleischner Society Guidelines for Managing Incidental Pulmonary Nodules: Common Questions and Challenging Scenarios. Radiographics 2018, 38, 1337–1350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roffman, C.E.; Buchanan, J.; Allison, G.T. Charlson Comorbidities Index. J. Physiother. 2016, 62, 171. [Google Scholar] [CrossRef] [Green Version]
- Falcoz, P.E.; Conti, M.; Brouchet, L.; Chocron, S.; Puyraveau, M.; Mercier, M.; Etievent, J.P.; Dahan, M. The Thoracic Surgery Scoring System (Thoracoscore): Risk model for in-hospital death in 15,183 patients requiring thoracic surgery. J. Thorac. Cardiovasc. Surg. 2007, 133, 325–332. [Google Scholar] [CrossRef]
- Campillo-Soto, A.; Flores-Pastor, B.; Soria-Aledo, V.; Candel-Arenas, M.; Andrés-García, B.; Martín-Lorenzo, J.G.; Aguayo-Albasini, J.L. Sistema POSSUM. Un instrumento de medida de la calidad en el paciente quirúrgico [The POSSUM scoring system: An instrument for measuring quality in surgical patients]. Cirugía Española 2006, 80, 395–399. [Google Scholar] [CrossRef] [PubMed]
- Maron, O.; Lozano-Pérez, T. A framework for multiple-instance learning. In Advances in Neural Information Processing Systems; Jordan, M., Kearns, M., Soll, S., Eds.; Morgan Kaufman: San Mateo, CA, USA, 1998; pp. 570–576. [Google Scholar]
- Petrou, M.; Quint, L.E.; Nan, B.; Baker, L.H. Pulmonary nodule volumetric measurement variability as a function of CT slice thickness and nodule morphology. AJR Am. J. Roentgenol. 2007, 188, 306–312. [Google Scholar] [CrossRef]
- Goo, J.M.; Tongdee, T.; Tongdee, R.; Yeo, K.; Hildebolt, C.F.; Bae, K.T. Volumetric measurement of synthetic lung nodules with multi- detector row CT: Effect of various image reconstruction parameters and segmentation thresholds on measurement accuracy. Radiology 2005, 235, 850–856. [Google Scholar] [CrossRef]
- Ravenel, J.G.; Leue, W.M.; Nietert, P.J.; Miller, J.V.; Taylor, K.K.; Silvestri, G.A. Pulmonary nodule volume: Effects of reconstruction parameters on automated measurements—A phantom study. Radiology 2008, 247, 400–408. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; de Bock, G.H.; van Klaveren, R.J.; van Ooyen, P.; Tukker, W.; Zhao, Y.; Dorrius, M.D.; Proença, R.V.; Post, W.J.; Oudkerk, M. Volumetric measurement of pulmonary nodules at low-dose chest CT: Effect of re- construction setting on measurement variability. Eur. Radiol. 2010, 20, 1180–1187. [Google Scholar] [CrossRef] [Green Version]
- Kaaki, S.; Kidane, B.; Srinathan, S.; Tan, L.; Buduhan, G. Is tissue still the issue? Lobectomy for suspicious lung nodules without confirmation of malignancy. J. Surg. Oncol. 2018, 117, 977–984. [Google Scholar] [CrossRef] [PubMed]
- Izumo, T.; Terada, Y.; Inomata, M.; Kuse, N.; Awano, N.; Tone, M.; Jo, T.; Yoshimura, H.; Moriya, A.; Furuhata, Y. Impact of preoperative pathological confirmation on surgical and postoperative outcomes of lung resection for early stage lung cancer. Adv. Respir. Med. 2019, 87, 203–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elia, S.; Loprete, S.; De Stefano, A.; Hardavella, G. Does aggressive management of solitary pulmonary nodules pay off? Breathe 2019, 15, 15–23. [Google Scholar] [CrossRef] [Green Version]
- Finlayson, E.; Fan, Z.; Birkmeyer, J.D. Outcomes in octogenarians undergoing high-risk cancer operation: A national study. J. Am. Coll. Surg. 2007, 205, 729–734. [Google Scholar] [CrossRef]
- Rivera, C.; Dahan, M.; Bernard, A.; Falcoz, P.E.; Thomas, P. Surgical treatment of lung cancer in the octogenarians: Results of a nationwide audit. Eur. J. Cardiothorac. Surg. 2011, 39, 981–986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dominguez-Ventura, A.; Allen, M.S.; Cassivi, S.D.; Nichols, F.C., 3rd; Deschamps, C.; Pairolero, P.C. Lung cancer in octogenarians: Factors affecting morbidity and mortality after pulmonary resection. Ann. Thorac. Surg. 2006, 82, 1175–1179. [Google Scholar] [CrossRef]
- Albano, D.; Gatta, R.; Marini, M.; Rodella, C.; Camoni, L.; Dondi, F.; Giubbini, R.; Bertagna, F. Role of 18F-FDG PET/CT Radiomics Features in the Differential Diagnosis of Solitary Pulmonary Nodules: Diagnostic Accuracy and Comparison between Two Different PET/CT Scanners. J. Clin. Med. 2021, 10, 5064. [Google Scholar] [CrossRef]
- Kumar, D.; Chung, A.G.; Shaifee, M.J.; Khalvati, F.; Haider, M.A.; Wong, A. Discovery radiomics for pathologically-proven computed tomography lung cancer prediction. In Proceedings 14th International Conference on Image Analysis and Recognition, Montreal, QC, Canada, 5–7 July 2017; Karray, F., Campilho, A., Cheriet, F., Eds.; Springer: Cham, Switzerland, 2017; pp. 54–62. [Google Scholar]
- Liu, Y.; Balagurunathan, Y.; Atwater, T.; Antic, S.; Li, Q.; Walker, R.C.; Smith, G.T.; Massion, P.P.; Schabath, M.B.; Gillies, R.J. Radiological image traits predictive of cancer status in pulmonary nodules. Clin. Cancer Res. 2017, 23, 1442–1449. [Google Scholar] [CrossRef] [Green Version]
- Wu, W.; Parmar, C.; Grossmann, P.; Quackenbush, J.; Lambin, P.; Bussink, J.; Mak, R.; Aerts, H.J. Exploratory study to identify radiomics classifiers for lung cancer histology. Front. Oncol. 2016, 6, 71. [Google Scholar] [CrossRef] [Green Version]
- Niu, R.; Gao, J.; Shao, X.; Wang, J.; Jiang, Z.; Shi, Y.; Zhang, F.; Wang, Y.; Shao, X. Maximum Standardized Uptake Value of 18F-deoxyglucose PET Imaging Increases the Effectiveness of CT Radiomics in Differentiating Benign and Malignant Pulmonary Ground-Glass Nodules. Front. Oncol. 2021, 11, 727094. [Google Scholar] [CrossRef]
- Astaraki, M.; Yang, G.; Zakko, Y.; Toma-Dasu, I.; Smedby, O.; Wang, C. A Comparative Study of Radiomics and Deep-Learning Based Methods for Pulmonary Nodule Malignancy Prediction in Low Dose CT Images. Front. Oncol. 2021, 11, 737368. [Google Scholar] [CrossRef] [PubMed]
- Parmar, C.; Grossmann, P.; Bussink, J.; Lambin, P.; Aerts, H.J.W.L. Machine Learning methods for Quantitative Radiomic Biomarkers. Sci. Rep. 2015, 5, 13087. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghamati, M.R.; Li, W.W.L.; van der Heijden, E.H.F.M.; Verhagen, A.F.T.M.; Damhuis, R.A. Surgery without preoperative histological confirmation of lung cancer: What is the current clinical practice? J. Thorac. Dis. 2021, 13, 5765–5775. [Google Scholar] [CrossRef]
- Senent-Valero, M.; Librero, J.; Pastor-Valero, M. Solitary pulmonary nodule malignancy predictive models applicable to routine clinical practice: A systematic review. Syst. Rev. 2021, 10, 308. [Google Scholar] [CrossRef]
- Zhang, R.; Sun, H.; Chen, B.; Xu, R.; Li, W. Developing of risk models for small solid and subsolid pulmonary nodules based on clinical and quantitative radiomics features. J. Thorac. Dis. 2021, 13, 4156–4168. [Google Scholar] [CrossRef] [PubMed]
- Zhao, W.; Zou, C.; Li, C.; Li, J.; Wang, Z.; Chen, L. Development of a diagnostic model for malignant solitary pulmonary nodules based on radiomics features. Ann. Transl. Med. 2022, 10, 201. [Google Scholar] [CrossRef] [PubMed]
- Rafael-Palou, X.; Aubanell, A.; Ceresa, M.; Ribas, V.; Piella, G.; Ballester, M.A.G. Prediction of Lung Nodule Progression with an Uncertainty-Aware Hierarchical Probabilistic Network. Diagnostics 2022, 12, 2639. [Google Scholar] [CrossRef]
- Zheng, S.; Kong, S.; Huang, Z.; Pan, L.; Zeng, T.; Zheng, B.; Liu, Z. A Lower False Positive Pulmonary Nodule Detection Approach for Early Lung Cancer Screening. Diagnostics 2022, 12, 2660. [Google Scholar] [CrossRef]
- Ather, S.; Kadir, T.; Gleeson, F. Artificial intelligence and radiomics in pulmonary nodule management: Current status and future applications. Clin. Radiol. 2020, 75, 13–19. [Google Scholar] [CrossRef] [Green Version]
- Koh, D.M.; Papanikolaou, N.; Bick, U.; Illing, R.; Kahn, C.E., Jr.; Kalpathi-Cramer, J.; Matos, C.; Martí-Bonmatí, L.; Miles, A.; Mun, S.K.; et al. Artificial intelligence and machine learning in cancer imaging. Commun. Med. 2022, 2, 133. [Google Scholar] [CrossRef]
- Gu, Y.; Chi, J.; Liu, J.; Yang, L.; Zhang, B.; Yu, D.; Zhao, Y.; Lu, X. A survey of computer-aided diagnosis of lung nodules from CT scans using deep learning. Comput. Biol. Med. 2021, 137, 104806. [Google Scholar] [CrossRef] [PubMed]
- Lin, F.Y.; Chang, Y.C.; Huang, H.Y.; Li, C.C.; Chen, Y.C.; Chen, C.M. A radiomics approach for lung nodule detection in thoracic CT images based on the dynamic patterns of morphological variation. Eur. Radiol. 2022, 32, 3767–3777. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Lin, W.; Xie, D.; Yu, Y.; Cao, H.; Liao, G.; Wu, S.; Yao, L.; Wang, Z.; Wang, M.; et al. Development and validation of a preoperative CT-based radiomic nomogram to predict pathology invasiveness in patients with a solitary pulmonary nodule: A machine learning approach, multicenter, diagnostic study. Eur. Radiol. 2022, 32, 1983–1996. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1 | Class First Order | Feature Mean | Description ROI Average Gray Intensity |
|---|---|---|---|
| 2 | Shape | Elongation | relationship between two largest principal components |
| 3 | Shape | Flatness | relationship between largest and smallest principal components |
| 4 | Shape | LeastAxisLength | yield smallest axis length of the ROI-enclosing ellipsoid |
| 5 | Shape | MajorAxisLength | yield largest axis length of ROI-enclosing ellipsoid |
| 6 | Shape | Maximum2DDiameterColumn | mesh vertices in row-slice plane |
| 7 | Shape | Maximum2DDiameterRow | mesh vertices in the column-slice plane |
| 8 | Shape | Maximum2DDiameterSlice | mesh vertices in row-column plane |
| 9 | Shape | Maximum3DDiameter | mesh vertices |
| 10 | Shape | MeshVolume | volume is obtained using the surface mesh |
| 11 | Shape | MinorAxisLength | second-largest axis length of the ROI-enclosing ellipsoid |
| 12 | Shape | Sphericity | roundness of shape of the tumor region relative to a sphere |
| 13 | Shape | SurfaceArea | the sum of all sub-areas |
| 14 | Shape | SurfaceVolumeRatio | Surface Area to Volume ratio |
| 15 | Shape | VoxelVolume | approximate volume |
| 16 | GLCM | Autocorrelation | magnitude of the fineness and coarseness of texture |
| 17 | GLCM | ClusterProminence | skewness and asymmetry of the GLCM |
| 18 | GLCM | ClusterShade | skewness and uniformity of the GLCM |
| 19 | GLCM | ClusterTendency | voxels with similar gray-level values |
| 20 | GLCM | Contrast | the local intensity variation |
| 21 | GLCM | Correlation | linear dependency of gray-level values |
| 22 | GLCM | DifferenceAverage | occurrences of pairs with similar and differing intensity values |
| 23 | GLCM | DifferenceEntropy | randomness/variability in neighborhood intensity value differences |
| 24 | GLCM | DifferenceVariance | heterogeneity of higher weights on differing intensity level pairs |
| 25 | GLCM | Id | inverse difference |
| 26 | GLCM | Idm | inverse difference moment |
| 27 | GLCM | Idmn | Inverse difference Moment Normalized |
| 28 | GLCM | Idn | Inverse difference Normalized |
| 29 | GLCM | Imc1 | informational measure of correlation 1 |
| 30 | GLCM | Imc2 | informational measure of correlation 2 |
| 31 | GLCM | InverseVariance | inverse of the variance |
| 32 | GLCM | JointAverage | the mean gray-level intensity of the distribution |
| 33 | GLCM | JointEnergy | a measure of homogeneous patterns in the image |
| 34 | GLCM | JointEntropy | measure of the randomness/variability in neighborhood intensity values |
| 35 | GLCM | MCC | maximal correlation coefficient |
| 36 | GLCM | MaximumProbability | occurrences of the most predominant pair of neighboring intensity values |
| 37 | GLCM | SumAverage | occurrences of pairs with lower and higher intensity values |
| 38 | GLCM | SumEntropy | sum of neighborhood intensity value differences |
| 39 | GLCM | SumSquares | distribution of neigboring intensity level pairs |
| 41 | GLRLM | GLN | gray-level non-uniformity |
| 42 | GLRLM | GLNN | gray-level non-uniformity normalized |
| 43 | GLRLM | GLV | gray-level variance |
| 44 | GLRLM | HGLRE | high gray-level run emphasis |
| 45 | GLRLM | LRE | long run emphasis |
| 46 | GLRLM | LRHGLE | long run high gray-level emphasis |
| 47 | GLRLM | LRLGLE | long run low gray-level emphasis |
| 48 | GLRLM | LGLRE | low gray-level run emphasis |
| 49 | GLRLM | RE | run entropy |
| 50 | GLRLM | RLN | run length non-uniformity |
| 51 | GLRLM | RLNN | run length non-uniformity normalized |
| 52 | GLRLM | RP | run percentage |
| 53 | GLRLM | RV | run variance |
| 54 | GLRLM | SRE | short run emphasis |
| 55 | GLRLM | SRHGLE | short run high gray-level emphasis |
| 56 | GLRLM | SRLGLE | short run low gray-level emphasis |
| 57 | GLSZM | GLN | gray-level non-uniformity |
| 58 | GLSZM | GLNN | gray-level non-uniformity (normalized) |
| 59 | GLSZM | GLV | gray-level variance |
| 59 | GLSZM | HGLZE | high gray-level zone emphasis |
| 60 | GLSZM | LAE | large area emphasis |
| 61 | GLSZM | LAHGLE | large area high gray-level emphasis |
| 62 | GLSZM | LALGLE | large area low gray-level emphasis |
| 63 | GLSZM | LGLZE | low gray-level zone emphasis |
| 64 | GLSZM | SZN | size-zone non-uniformity |
| 65 | GLSZM | SZNN | size-zone non-uniformity normalized |
| 66 | GLSZM | SAE | small area emphasis |
| 67 | GLSZM | SAHGLE | small area high gray-level emphasis |
| 68 | GLSZM | SALGLE | small area low gray-level Emphasis |
| 69 | GLSZM | ZE | zone entropy |
| 70 | GLSZM | ZP | zone percentage |
| 71 | GLSZM | ZV | zone variance |
| Variable | |
|---|---|
| Median age, years (IQR) | 79 (76–81) |
| Gender, n (%) | |
| Male Female | 45 (63.4%) 26 (36.6%) |
| Median number of comorbidities (IQR) | 3 (IQR 2–5) |
| Cardiac comorbidities, n (%) Coronary artery disease Any previous cardiac surgery Current treatment for hypertension Current treatment for arrhythmia Current treatment for cardiac failure | 18 (25.3%) 13 (18.3%) 51 (71.8%) 15 (21.1%) 8 (11.3%) |
| Non-cardiac comorbidities, n (%) Insulin-dependent diabetes Serum creatinine >2 mg/dL Cerebral vascular accident Chronic kidney failure Chronic obstructive pulmonary disease Gastric ulcer Liver disease Previous malignancy Other comorbidities | 19 (26.8%) 2 (2.8%) 8 (11.3%) 6 (8.4%) 36 (50.7%) 8 (11.3%) 8 (11.3%) 30 (42.2%) 35 (49.3%) |
| Smoking history, n (%) Never smoked Former smoker Current smoker Unknown | 12 (17.9%) 44 (65.7%) 10 (14.9%) 1 (1.5%) |
| Median Charlson Comorbidity Index (IQR) | 6 (5–7) |
| Median Thorascore (IQR) | 2.8% (1.2–6.3%) |
| Median POSSUM mortality (IQR) | 4.2% (3.1–8.5%) |
| Median POSSUM morbidity (IQR) | 23.9% (17.7–44.3%) |
| Surgical procedure, n (%) Pneumonectomy Lobectomy Segmentectomy Wedge resection | 1 (1.5%) 25 (35.2%) 4 (5.6%) 41 (57.7%) |
| Final histology, n (%) Lung adenocarcinoma Lung squamous carcinoma Lung metastasis Typical carcinoid Atypical carcinoid Benign lesion | 30 (42.3%) 11 (15.5%) 1 (1.4%) 2 (2.8%) 2 (2.8%) 25 (35.2%) |
| 30-day post-operative mortality, n (%) | 0 (0.0%) |
| Post-operative morbidity, n (%) | 22 (31.0%) |
| Median hospitalization, days (IQR) | 8 (6–12) |
| Model | Precision | Recall | F-Measure | ROC Area | Accuracy | Label |
|---|---|---|---|---|---|---|
| Functional Tree | 0.88 | 1 | 1 | 0.94 | 0.93 | Healthy |
| 0.866 | 0.913 | 0.889 | 0.847 | 0.88 | Disease | |
| 0.854 | 0.855 | 0.854 | 0.847 | 0.905 | weighted avg. | |
| Rep Tree | 0.836 | 0.741 | 0.786 | 0.915 | 0.769 | Healthy |
| 0.861 | 0.916 | 0.888 | 0.915 | 0.887 | Disease | |
| 0.852 | 0.853 | 0.850 | 0.915 | 0.828 | weighted avg. | |
| J48 | 0.854 | 0.740 | 0.792 | 0.932 | 0.761 | Healthy |
| 0.861 | 0.927 | 0.893 | 0.932 | 0.889 | Disease | |
| 0.858 | 0.859 | 0.856 | 0.932 | 0.825 | weighted avg. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elia, S.; Pompeo, E.; Santone, A.; Rigoli, R.; Chiocchi, M.; Patirelis, A.; Mercaldo, F.; Mancuso, L.; Brunese, L. Radiomics and Artificial Intelligence Can Predict Malignancy of Solitary Pulmonary Nodules in the Elderly. Diagnostics 2023, 13, 384. https://doi.org/10.3390/diagnostics13030384
Elia S, Pompeo E, Santone A, Rigoli R, Chiocchi M, Patirelis A, Mercaldo F, Mancuso L, Brunese L. Radiomics and Artificial Intelligence Can Predict Malignancy of Solitary Pulmonary Nodules in the Elderly. Diagnostics. 2023; 13(3):384. https://doi.org/10.3390/diagnostics13030384
Chicago/Turabian StyleElia, Stefano, Eugenio Pompeo, Antonella Santone, Rebecca Rigoli, Marcello Chiocchi, Alexandro Patirelis, Francesco Mercaldo, Leonardo Mancuso, and Luca Brunese. 2023. "Radiomics and Artificial Intelligence Can Predict Malignancy of Solitary Pulmonary Nodules in the Elderly" Diagnostics 13, no. 3: 384. https://doi.org/10.3390/diagnostics13030384