
NCR, an Inflammation and Nutrition Related Blood-Based Marker in Colon Cancer Patients: A New Promising Biomarker to Predict Outcome
 ,
,  , , ,
, , ,
Abstract
:
1. Introduction
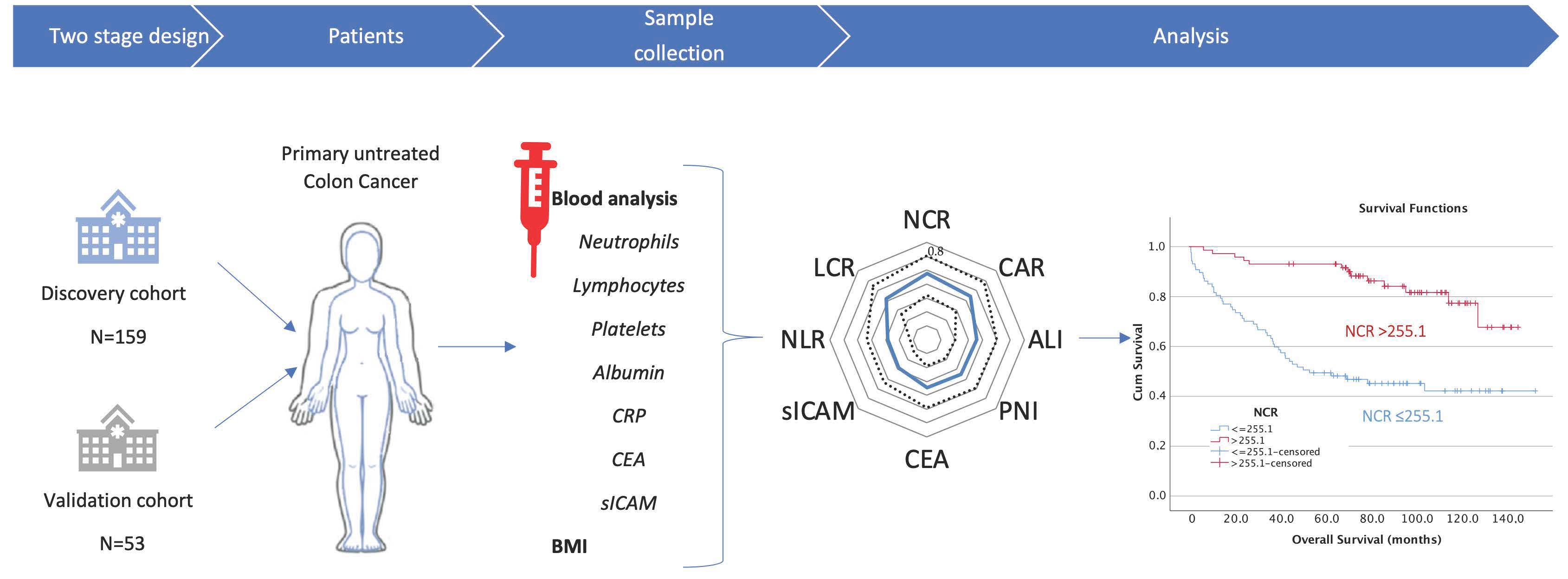
2. Materials and Methods
2.1. Patients
2.2. Laboratory Measurements of Inflammatory-Related Blood Indices
2.3. Laboratory Measurements of sICAM Concentrations Using ELISA
2.4. Statistical Analysis
3. Results
3.1. Patients Characteristics
3.2. Preoperative NCR Predicts Oncological Outcomes of Patients with Colon Cancer with Higher Accuracy Than Other Inflammation-Related Factors
3.3. Association between NCR and Clinicopathological Characteristics in the Discovery Cohort of Patients with Colon Cancer: A Decreased Preoperative NCR Correlated Significantly with Sidedness and the UICC Stage
3.4. Low Levels of NCR Were Associated with Poor Oncological Outcomes for Patients with Colon Cancer: Univariate and Multivariate Cox Regression Analysis of OS in the Discovery Cohort
3.5. Survival Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Global Burden of Disease Cancer Collaboration; Fitzmaurice, C.; Abate, D.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdel-Rahman, O.; Abdelalim, A.; Abdoli, A.; Abdollahpour, I.; et al. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2017: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2019, 5, 1749–1768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vuik, F.E.; Nieuwenburg, S.A.; Bardou, M.; Lansdorp-Vogelaar, I.; Dinis-Ribeiro, M.; Bento, M.J.; Zadnik, V.; Pellise, M.; Esteban, L.; Kaminski, M.F.; et al. Increasing incidence of colorectal cancer in young adults in Europe over the last 25 years. Gut 2019, 68, 1820–1826. [Google Scholar] [CrossRef] [PubMed]
- Paschke, S.; Jafarov, S.; Staib, L.; Kreuser, E.D.; Maulbecker-Armstrong, C.; Roitman, M.; Holm, T.; Harris, C.C.; Link, K.H.; Kornmann, M. Are Colon and Rectal Cancer Two Different Tumor Entities? A Proposal to Abandon the Term Colorectal Cancer. Int. J. Mol. Sci. 2018, 19, 2577. [Google Scholar] [CrossRef] [Green Version]
- Brenner, H.; Kloor, M.; Pox, C.P. Colorectal cancer. Lancet 2014, 383, 1490–1502. [Google Scholar] [CrossRef]
- Vogl, T.J.; Pereira, P.L.; Helmberger, T.; Schreyer, A.G.; Schmiegel, W.; Fischer, S.; Herzog, C. Updated S3 Guidelines-Diagnosis and Treatment of Colorectal Carcinoma: Relevance for Radiological Diagnosis and Intervention. Rofo 2019, 191, 298–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamamoto, T.; Kawada, K.; Obama, K. Inflammation-Related Biomarkers for the Prediction of Prognosis in Colorectal Cancer Patients. Int. J. Mol. Sci. 2021, 22, 8002. [Google Scholar] [CrossRef]
- Das, V.; Kalita, J.; Pal, M. Predictive and prognostic biomarkers in colorectal cancer: A systematic review of recent advances and challenges. Biomed. Pharmacother. 2017, 87, 8–19. [Google Scholar] [CrossRef]
- Shinkins, B.; Nicholson, B.D.; James, T.; Pathiraja, I.; Pugh, S.; Perera, R.; Primrose, J.; Mant, D. What carcinoembryonic antigen level should trigger further investigation during colorectal cancer follow-up? A systematic review and secondary analysis of a randomised controlled trial. Health Technol. Assess 2017, 21, 1–60. [Google Scholar] [CrossRef] [Green Version]
- Tan, E.; Gouvas, N.; Nicholls, R.J.; Ziprin, P.; Xynos, E.; Tekkis, P.P. Diagnostic precision of carcinoembryonic antigen in the detection of recurrence of colorectal cancer. Surg. Oncol. 2009, 18, 15–24. [Google Scholar] [CrossRef]
- Tan, D.; Fu, Y.; Tong, W.; Li, F. Prognostic significance of lymphocyte to monocyte ratio in colorectal cancer: A meta-analysis. Int. J. Surg. 2018, 55, 128–138. [Google Scholar] [CrossRef]
- De Ulibarri, J.I.; Gonzalez-Madrono, A.; de Villar, N.G.; Gonzalez, P.; Gonzalez, B.; Mancha, A.; Rodriguez, F.; Fernandez, G. CONUT: A tool for controlling nutritional status. First validation in a hospital population. Nutr. Hosp. 2005, 20, 38–45. [Google Scholar]
- Gao, Y.; Byrd, D.A.; Prizment, A.; Lazovich, D.; Bostick, R.M. Associations of Novel Lifestyle- and Whole Foods-Based Inflammation Scores with Incident Colorectal Cancer Among Women. Nutr. Cancer 2021, 74, 1356–1369. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, J.; Schellerer, V.S.; Brunner, M.; Geppert, C.I.; Grutzmann, R.; Weber, K.; Merkel, S. The impact of body mass index on prognosis in patients with colon carcinoma. Int. J. Color. Dis. 2022, 37, 1107–1117. [Google Scholar] [CrossRef] [PubMed]
- Andre, T.; Boni, C.; Mounedji-Boudiaf, L.; Navarro, M.; Tabernero, J.; Hickish, T.; Topham, C.; Zaninelli, M.; Clingan, P.; Bridgewater, J.; et al. Oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment for colon cancer. N. Engl. J. Med. 2004, 350, 2343–2351. [Google Scholar] [CrossRef] [Green Version]
- Nasr, R.; Salim Hammoud, M.; Nassar, F.; Mukherji, D.; Shamseddine, A.; Temraz, S. Inflammatory Markers and MicroRNAs: The Backstage Actors Influencing Prognosis in Colorectal Cancer Patients. Int. J. Mol. Sci. 2018, 19, 1867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dolan, R.D.; McSorley, S.T.; Park, J.H.; Watt, D.G.; Roxburgh, C.S.; Horgan, P.G.; McMillan, D.C. The prognostic value of systemic inflammation in patients undergoing surgery for colon cancer: Comparison of composite ratios and cumulative scores. Br. J. Cancer 2018, 119, 40–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tepus, M.; Yau, T.O. Non-Invasive Colorectal Cancer Screening: An Overview. Gastrointest. Tumors 2020, 7, 62–73. [Google Scholar] [CrossRef] [PubMed]
- Schellerer, V.S.; Langheinrich, M.C.; Zver, V.; Grutzmann, R.; Sturzl, M.; Gefeller, O.; Naschberger, E.; Merkel, S. Soluble intercellular adhesion molecule-1 is a prognostic marker in colorectal carcinoma. Int. J. Color. Dis. 2019, 34, 309–317. [Google Scholar] [CrossRef] [Green Version]
- Sepulveda, A.R.; Hamilton, S.R.; Allegra, C.J.; Grody, W.; Cushman-Vokoun, A.M.; Funkhouser, W.K.; Kopetz, S.E.; Lieu, C.; Lindor, N.M.; Minsky, B.D.; et al. Molecular Biomarkers for the Evaluation of Colorectal Cancer: Guideline From the American Society for Clinical Pathology, College of American Pathologists, Association for Molecular Pathology, and American Society of Clinical Oncology. J. Mol. Diagn. 2017, 19, 187–225. [Google Scholar] [CrossRef] [Green Version]
- Twelves, C.; Wong, A.; Nowacki, M.P.; Abt, M.; Burris, H., 3rd; Carrato, A.; Cassidy, J.; Cervantes, A.; Fagerberg, J.; Georgoulias, V.; et al. Capecitabine as adjuvant treatment for stage III colon cancer. N. Engl. J. Med. 2005, 352, 2696–2704. [Google Scholar] [CrossRef]
- Yothers, G.; O’Connell, M.J.; Allegra, C.J.; Kuebler, J.P.; Colangelo, L.H.; Petrelli, N.J.; Wolmark, N. Oxaliplatin as adjuvant therapy for colon cancer: Updated results of NSABP C-07 trial, including survival and subset analyses. J. Clin. Oncol. 2011, 29, 3768–3774. [Google Scholar] [CrossRef]
- Auclin, E.; Zaanan, A.; Vernerey, D.; Douard, R.; Gallois, C.; Laurent-Puig, P.; Bonnetain, F.; Taieb, J. Subgroups and prognostication in stage III colon cancer: Future perspectives for adjuvant therapy. Ann. Oncol. 2017, 28, 958–968. [Google Scholar] [CrossRef] [PubMed]
- Ju, J.H.; Chang, S.C.; Wang, H.S.; Yang, S.H.; Jiang, J.K.; Chen, W.C.; Lin, T.C.; Hung, H.; Wang, F.M.; Lin, J.K. Changes in disease pattern and treatment outcome of colorectal cancer: A review of 5474 cases in 20 years. Int. J. Color. Dis. 2007, 22, 855–862. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, J.B.; Maggard, M.A.; Ko, C.Y. Colon cancer survival rates with the new American Joint Committee on Cancer sixth edition staging. J. Natl. Cancer Inst. 2004, 96, 1420–1425. [Google Scholar] [CrossRef]
- Wiesmueller, F.; Schuetz, R.; Langheinrich, M.; Brunner, M.; Weber, G.F.; Grutzmann, R.; Merkel, S.; Krautz, C. Defining early recurrence in patients with resected primary colorectal carcinoma and its respective risk factors. Int. J. Color. Dis. 2021, 36, 1181–1191. [Google Scholar] [CrossRef] [PubMed]
- Posch, F.; Silina, K.; Leibl, S.; Mundlein, A.; Moch, H.; Siebenhuner, A.; Samaras, P.; Riedl, J.; Stotz, M.; Szkandera, J.; et al. Maturation of tertiary lymphoid structures and recurrence of stage II and III colorectal cancer. Oncoimmunology 2018, 7, e1378844. [Google Scholar] [CrossRef] [Green Version]
- Kalb, M.; Langheinrich, M.C.; Merkel, S.; Krautz, C.; Brunner, M.; Benard, A.; Weber, K.; Pilarsky, C.; Grutzmann, R.; Weber, G.F. Influence of Body Mass Index on Long-Term Outcome in Patients with Rectal Cancer-A Single Centre Experience. Cancers 2019, 11, 609. [Google Scholar] [CrossRef] [Green Version]
- Okugawa, Y.; Toiyama, Y.; Yamamoto, A.; Shigemori, T.; Ichikawa, T.; Yin, C.; Suzuki, A.; Fujikawa, H.; Yasuda, H.; Hiro, J.; et al. Lymphocyte-to-C-reactive protein ratio and score are clinically feasible nutrition-inflammation markers of outcome in patients with gastric cancer. Clin. Nutr. 2020, 39, 1209–1217. [Google Scholar] [CrossRef]
- Suzuki, S.; Akiyoshi, T.; Oba, K.; Otsuka, F.; Tominaga, T.; Nagasaki, T.; Fukunaga, Y.; Ueno, M. Comprehensive Comparative Analysis of Prognostic Value of Systemic Inflammatory Biomarkers for Patients with Stage II/III Colon Cancer. Ann. Surg. Oncol. 2020, 27, 844–852. [Google Scholar] [CrossRef]
- Inamoto, S.; Kawada, K.; Okamura, R.; Hida, K.; Sakai, Y. Prognostic impact of the combination of neutrophil-to-lymphocyte ratio and Glasgow prognostic score in colorectal cancer: A retrospective cohort study. Int. J. Color. Dis. 2019, 34, 1303–1315. [Google Scholar] [CrossRef]
- Li, Q.; Dai, W.; Li, Y.; Xu, Y.; Li, X.; Cai, S. Nomograms for predicting the prognostic value of serological tumor biomarkers in colorectal cancer patients after radical resection. Sci. Rep. 2017, 7, 46345. [Google Scholar] [CrossRef]
- Kim, J.H.; Lee, J.Y.; Kim, H.K.; Lee, J.W.; Jung, S.G.; Jung, K.; Kim, S.E.; Moon, W.; Park, M.I.; Park, S.J. Prognostic significance of the neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in patients with stage III and IV colorectal cancer. World J. Gastroenterol. 2017, 23, 505–515. [Google Scholar] [CrossRef] [PubMed]
- Lim, D.H.; Lee, J.H.; Kim, J.W. Feasibility of CYFRA 21-1 as a serum biomarker for the detection of colorectal adenoma and advanced colorectal adenoma in people over the age of 45. J. Clin. Lab. Anal. 2018, 32, e22163. [Google Scholar] [CrossRef] [Green Version]
- Thomas, D.S.; Fourkala, E.O.; Apostolidou, S.; Gunu, R.; Ryan, A.; Jacobs, I.; Menon, U.; Alderton, W.; Gentry-Maharaj, A.; Timms, J.F. Evaluation of serum CEA, CYFRA21-1 and CA125 for the early detection of colorectal cancer using longitudinal preclinical samples. Br. J. Cancer 2015, 113, 268–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harlid, S.; Gunter, M.J.; Van Guelpen, B. Risk-Predictive and Diagnostic Biomarkers for Colorectal Cancer; a Systematic Review of Studies Using Pre-Diagnostic Blood Samples Collected in Prospective Cohorts and Screening Settings. Cancers 2021, 13, 4406. [Google Scholar] [CrossRef] [PubMed]
- Baran, B.; Ozupek, N.M.; Tetik, N.Y.; Acar, E.; Bekcioglu, O.; Baskin, Y. Difference Between Left-Sided and Right-Sided Colorectal Cancer: A Focused Review of Literature. Gastroenterol. Res. 2018, 11, 264–273. [Google Scholar] [CrossRef] [Green Version]
- Mege, D.; Manceau, G.; Beyer, L.; Bridoux, V.; Lakkis, Z.; Venara, A.; Voron, T.; de’Angelis, N.; Abdalla, S.; Sielezneff, I.; et al. Right-sided vs. left-sided obstructing colonic cancer: Results of a multicenter study of the French Surgical Association in 2325 patients and literature review. Int. J. Color. Dis. 2019, 34, 1021–1032. [Google Scholar] [CrossRef]
- Mazaki, J.; Katsumata, K.; Kasahara, K.; Tago, T.; Wada, T.; Kuwabara, H.; Enomoto, M.; Ishizaki, T.; Nagakawa, Y.; Tsuchida, A. Neutrophil-to-lymphocyte ratio is a prognostic factor for colon cancer: A propensity score analysis. BMC Cancer 2020, 20, 922. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | n (%) | |
|---|---|---|
| Age | years (median, range) | 66 (27–91) |
| Sex | Male | 103 (64.8) |
| Female | 56 (35.2) | |
| Physical ASA status (American Society of Anesthesiologists) | 1 | 25 (15.7) |
| 2 | 90 (56.6) | |
| 3 | 44 (27.7) | |
| BMI, kg/m² | <18.5 | 1 (0.6) |
| 18.5–24.9 | 46 (28.9) | |
| 25–29.9 | 72 (21.4) | |
| 30–34.9 | 34 (45.3) | |
| 35–39.9 | 5 (3.1) | |
| ≥40 | 1 (0.6) | |
| UICC classification | Stage I | 13 (8.2) |
| Stage II | 76 (47.8) | |
| Stage III | 48 (30.2) | |
| Stage IV | 22 (13.8) | |
| Tumor location | Right-sided | 92 (57.9) |
| Left-sided | 67 (42.1) | |
| T-stage | T1 | 7 (4.4) |
| T2 | 15 (9.4) | |
| T3 | 115 (72.3) | |
| T4 | 31 (19.5) | |
| N-stage | N0 | 92 (57.9) |
| N1 | 36 (22.6) | |
| N2 | 31 (19.5) | |
| Histological differentiation | G1 well/G2 moderate | 99 (62.3) |
| G3 poor | 60 (37.7) | |
| Demographics | n (%) | |
|---|---|---|
| Age | years (median, range) | 68 (27–90) |
| Sex | Male | 29 (54.7) |
| Female | 24 (45.3) | |
| BMI, kg/m² | <18.5 | 2 (3.8) |
| 18.5–24.9 | 25 (47.2) | |
| 25–29.9 | 20 (37.7) | |
| 30–34.9 | 4 (7.5) | |
| 35–39.9 | 1 (1.9) | |
| ≥40 | 1 (1.9) | |
| UICC classification | Stage I | 0 |
| Stage II | 19 (35.9) | |
| Stage III | 13 (24.5) | |
| Stage IV | 21 (39.6) | |
| Variables | AUC | Cutoff | Sensitivity | Specificity | 95% CI (Upper-Lower Limits) |
|---|---|---|---|---|---|
| NCR | 0.737 | >255.1 | 61.3% | 86.8% | 0.803–0.661 |
| CAR | 0.722 | ≤0.1 | 59.4% | 84.9% | 0.790–0.645 |
| LCR | 0.707 | >0.2 | 66.0% | 77.4% | 0.776–0.629 |
| ALI | 0.679 | >252.2 | 83.7% | 47.2% | 0.75–0.6 |
| sICAM | 0.643 | ≤229.1 | 46.2% | 81.1% | 0.718–0.564 |
| PNI | 0.674 | >42.6 | 65.1% | 67.9% | 0.746–0.595 |
| NLR | 0.641 | ≤3.54 | 70.8% | 58.5% | 0.716–0.561 |
| CEA | 0.680 | 5.0 | 74.5% | 56.6% | 0.8–0.6 |
| Parameter | Groups | Total n (%) | NCR n ≤ 255.1 | NCR n > 255.1 | p Value |
|---|---|---|---|---|---|
| Age | <66 years | 79 (49.7) | 43 | 36 | 0.942 |
| >66 years | 80 (50.3) | 44 | 36 | ||
| Sex | Male | 103 (64.8) | 60 | 43 | 0.225 |
| Female | 56 (35.2) | 27 | 29 | ||
| ECOG PS | 0 | 93 (58.5) | 38 | 55 | <0.001 |
| 1 | 42 (30.2) | 25 | 17 | ||
| 2 | 11 (6.9) | 11 | 0 | ||
| 3/4 | 13 (8.2) | 12 | 1 | ||
| Tumor location | Right-sided | 92 (57.9) | 59 | 33 | 0.005 |
| Left-sided | 67 (42.1) | 28 | 39 | ||
| Histological differentiation | G1/G2 | 99 (62.3) | 48 | 51 | 0.043 |
| G3 | 60 (37.7) | 39 | 21 | ||
| N-stage | N0 | 92 (57.9) | 44 | 48 | 0.041 |
| N+ | 67 (42.1) | 43 | 24 | ||
| Inflammatory stromal reaction | moderate | 62 (39) | 37 | 46 | 0.004 |
| pronounced | 77 (48.4) | 25 | 31 | ||
| unknown | 20 (12.6) | 4 | 16 | ||
| Distant metastasis | no | 137 (86.2) | 69 | 68 | 0.006 |
| yes | 22 (13.8) | 18 | 4 | ||
| UICC classification | Stage I | 13 (8.2) | 5 | 8 | 0.028 |
| Stage II | 76 (47.8) | 37 | 39 | ||
| Stage III | 48 (30.2) | 27 | 21 | ||
| Stage IV | 22 (13.8) | 18 | 4 | ||
| CEA | ≤5 | 102 (64.2) | 46 | 41 | 0.001 |
| >5 | 57 (35.8) | 56 | 16 |
| Variables | Categorical | Hazard Ratio | 95% CI Low | 95% CI High | p Value |
|---|---|---|---|---|---|
| NCR | >255.1 | 4.33 | 2.34 | 8.00 | <0.001 |
| CAR | ≤0.11 | 3.78 | 2.08 | 6.88 | <0.001 |
| LCR | >0.24 | 3.52 | 2.02 | 6.12 | <0.001 |
| ALI | >252.2 | 3.00 | 1.80 | 5.00 | <0.001 |
| sICAM | ≤229.1 | 2.10 | 1.48 | 4.93 | 0.001 |
| PNI | >42.6 | 2.56 | 1.52 | 4.31 | <0.001 |
| CEA | >5.0 | 2.44 | 1.47 | 4.04 | 0.001 |
| NLR | ≤3.54 | 2.06 | 1.25 | 3.41 | 0.005 |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p Value | HR | 95% CI | p Value | |
| Age | 1.037 | 1.010–1.065 | 0.006 | 1.043 | 1.012–1.076 | 0.006 |
| Sex | 2.501 | 1.353–4.620 | 0.003 | 4.280 | 2.177–8.417 | <0.001 |
| Male | ||||||
| Female | ||||||
| BMI | 0.944 | 0.887–1.004 | 0.067 | 0.922 | 0.862–0.986 | 0.018 |
| ASA | ||||||
| 1 | <0.001 | 0.025 | ||||
| 2 | 1.622 | 0.626–4.205 | 0.320 | 1.210 | 0.429–3.412 | 0.719 |
| 3 | 4.473 | 1.724–11.607 | 0.002 | 2.526 | 0.846–7.540 | 0.097 |
| ECOG | ||||||
| 0 | 0.002 | |||||
| 1 | 1.665 | 0.916–3.024 | 0.094 | |||
| 2 | 3.777 | 1.629–8.754 | 0.002 | |||
| 3 | 3.510 | 1.588–7.757 | 0.002 | |||
| 4 | 5.231 | 0.703–38.932 | 0.106 | |||
| T-stage | ||||||
| T1 | 0.11 | |||||
| T2 | 1.229 | 0.238–6.338 | 0.193 | |||
| T3 | 1.241 | 0.300–5.136 | 0.139 | |||
| T4 | 2.703 | 0.604–12.094 | 0.018 | |||
| N-stage | ||||||
| N0 | <0.001 | |||||
| N1 | 1.111 | 0.565–2.186 | 0.760 | |||
| N2 | 3.115 | 1.763–5.506 | <0.001 | |||
| M-stage | ||||||
| M0 | <0.001 | |||||
| M1a (one organ) | 1.834 | 0.727–4.629 | 0.199 | |||
| M1b (several organs) | 3.933 | 0.943–16.402 | 0.060 | |||
| M1c (peritoneum) | 7.779 | 3.699–16.360 | <0.001 | |||
| Tumor location | 1.743 | 1.020–2.978 | 0.042 | |||
| Right | ||||||
| Left | ||||||
| Lymphocytes | 0.989 | 0.639–1.531 | 0.961 | |||
| Thrombocytes | 1.001 | 0.999–1.004 | 0.261 | |||
| Albumin | 0.89 | 0.853–0.945 | <0.001 | |||
| CRP | 1.009 | 1.000–1.017 | 0.041 | |||
| CEA | 1.001 | 1.000–1.002 | 0.007 | |||
| UICC | ||||||
| Stage I | <0.001 | <0.001 | ||||
| Stage II | 0.631 | 0.238–1.672 | 0.354 | 0.375 | 0.131–1.076 | 0.068 |
| Stage III | 0.871 | 0.323–2.352 | 0.786 | 0.451 | 0.152–1.337 | 0.151 |
| Stage IV | 2.673 | 0.976–7.318 | 0.056 | 1.865 | 0.587–5.920 | 0.290 |
| NCR | 4.325 | 2.337–8.003 | <0.001 | 3.305 | 1.628–6.709 | 0.001 |
| ≤255.1 | ||||||
| >255.1 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Langheinrich, M.; Siebenhüner, A.R.; Baecker, J.; Miragall, M.; Wiesmüller, F.; Schellerer, V.; Merkel, S.; Brunner, M.; Krautz, C.; Weber, K.; et al. NCR, an Inflammation and Nutrition Related Blood-Based Marker in Colon Cancer Patients: A New Promising Biomarker to Predict Outcome. Diagnostics 2023, 13, 116. https://doi.org/10.3390/diagnostics13010116
Langheinrich M, Siebenhüner AR, Baecker J, Miragall M, Wiesmüller F, Schellerer V, Merkel S, Brunner M, Krautz C, Weber K, et al. NCR, an Inflammation and Nutrition Related Blood-Based Marker in Colon Cancer Patients: A New Promising Biomarker to Predict Outcome. Diagnostics. 2023; 13(1):116. https://doi.org/10.3390/diagnostics13010116
Chicago/Turabian StyleLangheinrich, Melanie, Alexander Reinhard Siebenhüner, Justus Baecker, Maximilian Miragall, Felix Wiesmüller, Vera Schellerer, Susanne Merkel, Maximilian Brunner, Christian Krautz, Klaus Weber, and et al. 2023. "NCR, an Inflammation and Nutrition Related Blood-Based Marker in Colon Cancer Patients: A New Promising Biomarker to Predict Outcome" Diagnostics 13, no. 1: 116. https://doi.org/10.3390/diagnostics13010116