
Clear Cell Renal Cell Carcinoma Spinal Metastases: Which Factors Matter to the Overall Survival? A 10-Year Experience of a High-Volume Tumor Spine Center
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Capitanio, U.; Bensalah, K.; Bex, A.; Boorjian, S.A.; Bray, F.; Coleman, J.; Gore, J.L.; Sun, M.; Wood, C.; Russo, P. Epidemiology of Renal Cell Carcinoma. Eur. Urol. 2019, 75, 74–84. [Google Scholar] [CrossRef]
- Osawa, T.; Takeuchi, A.; Kojima, T.; Shinohara, N.; Eto, M.; Nishiyama, H. Overview of Current and Future Systemic Therapy for Metastatic Renal Cell Carcinoma. Jpn. J. Clin. Oncol. 2019, 49, 395–403. [Google Scholar] [CrossRef]
- Maralani, P.J.; Winger, K.; Symons, S.; Machnowska, M.; Heyn, C.; Helmi, A.; Chan, A.; Tseng, C.-L.; Sahgal, A. Incidence and Time of Onset of Osseous Pseudoprogression in Patients With Metastatic Spine Disease From Renal Cell or Prostate Carcinoma After Treatment With Stereotactic Body Radiation Therapy. Neurosurgery 2019, 84, 647–654. [Google Scholar] [CrossRef] [PubMed]
- Umer, M.; Mohib, Y.; Atif, M.; Nazim, M. Skeletal Metastasis in Renal Cell Carcinoma: A Review. Ann. Med. Surg. 2018, 27, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Joshi, A.; Sahu, A.; Noronha, V.; Patil, V.; Prabhash, K. Metastatic Renal Cell Cancer-Systemic Therapy. Indian J Surg Oncol 2018, 9, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Gul, A.; Rini, B.I. Adjuvant Therapy in Renal Cell Carcinoma. Cancer 2019, 125, 2935–2944. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, N.; Drake, C.G. Kidney Cancer. Urol. Clin. N. Am. 2020, 47, 419–431. [Google Scholar] [CrossRef] [PubMed]
- Graham, J.; Shah, A.Y.; Wells, J.C.; McKay, R.R.; Vaishampayan, U.; Hansen, A.; Donskov, F.; Bjarnason, G.A.; Beuselinck, B.; Velasco, G.D.; et al. Outcomes of Patients with Metastatic Renal Cell Carcinoma Treated with Targeted Therapy after Immuno-Oncology Checkpoint Inhibitors. Eur. Urol. Oncol. 2021, 4, 102–111. [Google Scholar] [CrossRef] [Green Version]
- Ryu, S.; Rock, J.; Jain, R.; Lu, M.; Anderson, J.; Jin, J.-Y.; Rosenblum, M.; Movsas, B.; Kim, J.H. Radiosurgical Decompression of Metastatic Epidural Compression. Cancer 2010, 116, 2250–2257. [Google Scholar] [CrossRef]
- Teyssonneau, D.; Gross-Goupil, M.; Domblides, C.; Haaser, T.; Pointillart, V.; Daste, A.; Hauger, O.; Ravaud, A. Treatment of Spinal Metastases in Renal Cell Carcinoma: A Critical Review. Crit. Rev. Oncol. Hematol. 2018, 125, 19–29. [Google Scholar] [CrossRef] [PubMed]
- Cox, B.W.; Spratt, D.E.; Lovelock, M.; Bilsky, M.H.; Lis, E.; Ryu, S.; Sheehan, J.; Gerszten, P.C.; Chang, E.; Gibbs, I.; et al. International Spine Radiosurgery Consortium Consensus Guidelines for Target Volume Definition in Spinal Stereotactic Radiosurgery. Int. J. Radiat. Oncol. 2012, 83, e597–e605. [Google Scholar] [CrossRef] [PubMed]
- Sciubba, D.M.; Petteys, R.J.; Dekutoski, M.B.; Fisher, C.G.; Fehlings, M.G.; Ondra, S.L.; Rhines, L.D.; Gokaslan, Z.L. Diagnosis and Management of Metastatic Spine Disease. J. Neurosurg. Spine 2010, 13, 94–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romero-Muñoz, L.M.; Segura-Fragoso, A.; Talavera-Díaz, F.; Guimbard-Pérez, J.; Caba-Mora, D.; Barriga-Martín, A. Neurological Injury as a Complication of Spinal Surgery: Incidence, Risk Factors, and Prognosis. Spinal Cord 2020, 58, 318–323. [Google Scholar] [CrossRef] [PubMed]
- Friendlander, A.H.; Ettinger, R.L. Karnofsky Performance Status Scale. Spec. Care Dent. 2009, 29, 147–148. [Google Scholar] [CrossRef] [PubMed]
- Zoccali, C.; Skoch, J.; Walter, C.M.; Torabi, M.; Borgstrom, M.; Baaj, A.A. The Tokuhashi Score: Effectiveness and Pitfalls. Eur. Spine J. 2016, 25, 673–678. [Google Scholar] [CrossRef]
- Rampersaud, Y.R.; Anderson, P.A.; Dimar, J.R.; Fisher, C.G. Spinal Adverse Events Severity System, Version 2 (SAVES-V2): Inter- and Intraobserver Reliability Assessment. J. Neurosurg. Spine 2016, 25, 256–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodwin, C.R.; Ahmed, A.K.; Boone, C.; Abu-Bonsrah, N.; Xu, R.; Germscheid, N.; Fourney, D.R.; Clarke, M.; Laufer, I.; Fisher, C.G.; et al. The Challenges of Renal Cell Carcinoma Metastatic to the Spine: A Systematic Review of Survival and Treatment. Glob. Spine J. 2018, 8, 517–526. [Google Scholar] [CrossRef] [Green Version]
- Kato, S.; Demura, S.; Murakami, H.; Yoshioka, K.; Shinmura, K.; Yokogawa, N.; Shimizu, T.; Kawahara, N.; Tsuchiya, H. Clinical Outcomes and Prognostic Factors Following the Surgical Resection of Renal Cell Carcinoma Spinal Metastases. Cancer Sci. 2021, 112, 2416–2425. [Google Scholar] [CrossRef]
- Gasbarrini, A.; Cappuccio, M.; Mirabile, L.; Bandiera, S.; Terzi, S.; Barbanti Bròdano, G.; Boriani, S. Spinal Metastases: Treatment Evaluation Algorithm. Eur. Rev. Med. Pharmacol. Sci. 2004, 8, 265–274. [Google Scholar]
- Gasbarrini, A.; Li, H.; Cappuccio, M.; Mirabile, L.; Paderni, S.; Terzi, S.; Boriani, S. Efficacy Evaluation of a New Treatment Algorithm for Spinal Metastases. Spine 2010, 35, 1466–1470. [Google Scholar] [CrossRef]
- Fourney, D.R.; Frangou, E.M.; Ryken, T.C.; Dipaola, C.P.; Shaffrey, C.I.; Berven, S.H.; Bilsky, M.H.; Harrop, J.S.; Fehlings, M.G.; Boriani, S.; et al. Spinal instability neoplastic score: An analysis of reliability and validity from the spine oncology study group. J. Clin. Oncol. 2011, 29, 3072–3077. [Google Scholar] [CrossRef] [PubMed]
- Spratt, D.E.; Beeler, W.H.; de Moraes, F.Y.; Rhines, L.D.; Gemmete, J.J.; Chaudhary, N.; Shultz, D.B.; Smith, S.R.; Berlin, A.; Dahele, M.; et al. An integrated multidisciplinary algorithm for the management of spinal metastases: An International Spine Oncology Consortium report. Lancet Oncol. 2017, 18, e720–e730. [Google Scholar] [CrossRef]
- Laufer, I.; Rubin, D.G.; Lis, E.; Cox, B.W.; Stubblefield, M.D.; Yamada, Y.; Bilsky, M.H. The NOMS framework: Approach to the treatment of spinal metastatic tumors. Oncologist 2013, 18, 744–751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhai, J.; Liu, N.; Wang, H.; Huang, G.; Man, L. Clinical Characteristics and Prognosis of Renal Cell Carcinoma with Spinal Bone Metastases. Front. Oncol. 2021, 11, 659779. [Google Scholar] [CrossRef] [PubMed]
- Ruatta, F.; Derosa, L.; Escudier, B.; Colomba, E.; Guida, A.; Baciarello, G.; Loriot, Y.; Fizazi, K.; Albiges, L. Prognosis of Renal Cell Carcinoma with Bone Metastases: Experience from a Large Cancer Centre. Eur. J. Cancer 2019, 107, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Shinohara, N.; Nonomura, K.; Abe, T.; Maruyama, S.; Kamai, T.; Takahashi, M.; Tatsugami, K.; Yokoi, S.; Deguchi, T.; Kanayama, H.; et al. A New Prognostic Classification for Overall Survival in Asian Patients with Previously Untreated Metastatic Renal Cell Carcinoma. Cancer Sci. 2012, 103, 1695–1700. [Google Scholar] [CrossRef]
- Terzi, S.; Trentin, F.; Carretta, E.; Pipola, V.; Ghermandi, R.; Bròdano, G.B.; Ferrari, C.; Griffoni, C.; Gasbarrini, A. Breast Cancer Spinal Metastases: Prognostic Factors Affecting Survival after Surgery. A Retrospective Study. J. Clin. Neurosci. 2020, 78, 73–78. [Google Scholar] [CrossRef]
- Terzi, S.; Trentin, F.; Griffoni, C.; Carretta, E.; Bandiera, S.; Ferrari, C.; Gasbarrini, A. Indications and Limits of Surgery for Spinal Metastases Derived from Lung Cancer: A Single-Center Experience. Acta Orthop. Belg. 2020, in press. [Google Scholar]
- Park, B.J.; Seaman, S.C.; Noeller, J.L.; Smith, M.C.; Hasan, D.M.; Yasin, H.; Hitchon, P.W. Metastatic Renal Cell Carcinoma to the Spine: Outcomes and Morbidity: Single-Center Experience. World Neurosurg. 2021, 154, e398–e405. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.H.; Park, J.-O.; Kim, H.-S.; Park, Y.-C.; Lee, H.-M.; Moon, S.-H. Perioperative Complication and Surgical Outcome in Patients with Spine Metastases: Retrospective 200-Case Series in a Single Institute. Clin. Neurol. Neurosurg. 2014, 122, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Camino-Willhuber, G.; Cabrera, J.P.; Carazzo, C.; Guiroy, A.; Gagliardi, M.; Terrasa, S.; Joaquim, A.F. Reporting Complications in Spinal Surgery—A Systematic Literature Review. World Neurosurg. 2021, 150, e765–e770. [Google Scholar] [CrossRef]
- Riaz, I.B.; He, H.; Ryu, A.J.; Siddiqi, R.; Naqvi, S.A.A.; Yao, Y.; Husnain, M.; Narasimhulu, D.M.; Mathew, J.; Sipra, Q.U.A.R.; et al. A Living, Interactive Systematic Review and Network Meta-Analysis of First-Line Treatment of Metastatic Renal Cell Carcinoma. Eur. Urol. 2021, 80, 712–723. [Google Scholar] [CrossRef]
- Albiges, L.; Tannir, N.M.; Burotto, M.; McDermott, D.; Plimack, E.R.; Barthélémy, P.; Porta, C.; Powles, T.; Donskov, F.; George, S.; et al. Nivolumab plus Ipilimumab versus Sunitinib for First-Line Treatment of Advanced Renal Cell Carcinoma: Extended 4-Year Follow-up of the Phase III CheckMate 214 Trial. ESMO Open 2020, 5, e001079. [Google Scholar] [CrossRef] [PubMed]
- Siska, P.J.; Beckermann, K.E.; Rathmell, W.K.; Haake, S.M. Strategies to Overcome Therapeutic Resistance in Renal Cell Carcinoma. Urol. Oncol. Semin. Orig. Investig. 2017, 35, 102–110. [Google Scholar] [CrossRef] [Green Version]
- Bruchbacher, A.; Lemberger, U.; Hassler, M.R.; Fajkovic, H.; Schmidinger, M. PD1/PD-L1 Therapy in Metastatic Renal Cell Carcinoma. Curr. Opin. Urol. 2020, 30, 534–541. [Google Scholar] [CrossRef] [PubMed]
- Gatto, L.; Facchini, G.; Saponara, M.; Nannini, M.; Rossi, G.; Di Scioscio, V.; Biasco, G.; Pantaleo, M.A. Successful selective arterial embolizations for bone metastases in renal cell carcinoma integrated with systemic therapies: A case report. Radiol. Case Rep. 2017, 12, 775–779. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | N | % |
|---|---|---|
| Age (years) | ||
| <65 | 36 | 52.2 |
| ≥65 | 33 | 47.8 |
| Gender | ||
| Female | 20 | 29.0 |
| Male | 49 | 71.0 |
| Intact | ||
| Yes | 9 | 13.0 |
| No | 60 | 87.0 |
| Synchronous metastases | ||
| Yes | 26 | 37.7 |
| No | 42 | 60.9 |
| NA | 1 | 1.4 |
| Visceral metastases | ||
| Yes | 28 | 40.6 |
| No | 37 | 53.6 |
| NA | 4 | 5.8 |
| SINS score | ||
| 7–12 | 48 | 69.6 |
| 13–18 | 21 | 30.4 |
| Previous Treatment | ||
| Surgery | 23 | 33.3 |
| Surgery + RT | 4 | 5.8 |
| Surgery + RT + CHT | 13 | 18.9 |
| Surgery + CHT | 10 | 14.5 |
| RT + CHT | 7 | 10.1 |
| CHT | 1 | 1.4 |
| NA | 11 | 16.0 |
| Tokuhashi score | ||
| 0–8 | 17 | 24.6 |
| 9–11 | 35 | 50.7 |
| 12–15 | 12 | 17.4 |
| NA | 5 | 7.3 |
| Sites of visceral metastases | ||
| Lungs | 19 | |
| Spleen | 3 | |
| Liver | 3 | |
| Thyroid | 1 | |
| Esophagus | 1 | |
| Uterus | 1 | |
| Adrenal gland | 3 | |
| Brain | 1 |
| N | % | |
|---|---|---|
| Type of surgery | ||
| MIS | 2 | 2.9 |
| Palliative surgery | 7 | 10.1 |
| Debulking | 50 | 14.5 |
| En-bloc | 10 | 72.5 |
| Margins | ||
| Intralesional | 61 | 88.4 |
| Marginal | 2 | 2.9 |
| Wide | 6 | 8.7 |
| Complications | ||
| Yes | 21 | 69.6 |
| No | 48 | 30.4 |
| Intra-Operative | Post-Operative | ||
|---|---|---|---|
| n/N (%) | n/N (%) | ||
| Dural tear | 4/25 (16%) | Wound dehiscence | 3/25 (16%) |
| Neurological impairment * | 1/25 (4%) | Deep wound infection | 7/25 (28%) |
| Other | 1/25 (4%) | Superficial wound infection | 1/25 (4%) |
| Pulmonary embolism | 1/25 (4%) | ||
| Construct failure without loss of correction | 4/25 (12%) | ||
| CSF leak/meningocele | 1/25 (4%) | ||
| Pneumonia | 1/25 (4%) | ||
| Other | 1/25 (4%) | ||
| Total | 6/25 | 19/25 | |
| Pre-Operative | Post-Operative | p Value | |||
|---|---|---|---|---|---|
| N | % | N | % | ||
| Ambulatory status | <0.0001 | ||||
| Bedridden | 17 | 24.6 | 3 | 4.3 | |
| Wheelchair | 3 | 4.3 | 3 | 4.3 | |
| Walking aids | 8 | 11.6 | 35 | 50.7 | |
| Self-supporting | 41 | 59.4 | 28 | 40.6 | |
| Frankel score | 0.0003 | ||||
| E | 42 | 60.9 | 56 | 81.2 | |
| other | 27 | 39.1 | 13 | 18.8 | |
| Karnofsky score | 0.2809 | ||||
| <70 | 36 | 52.2 | 39 | 56.5 | |
| ≥70 | 32 | 46.4 | 28 | 40.6 | |
| NA | 1 | 1.4 | 2 | 2.9 | |
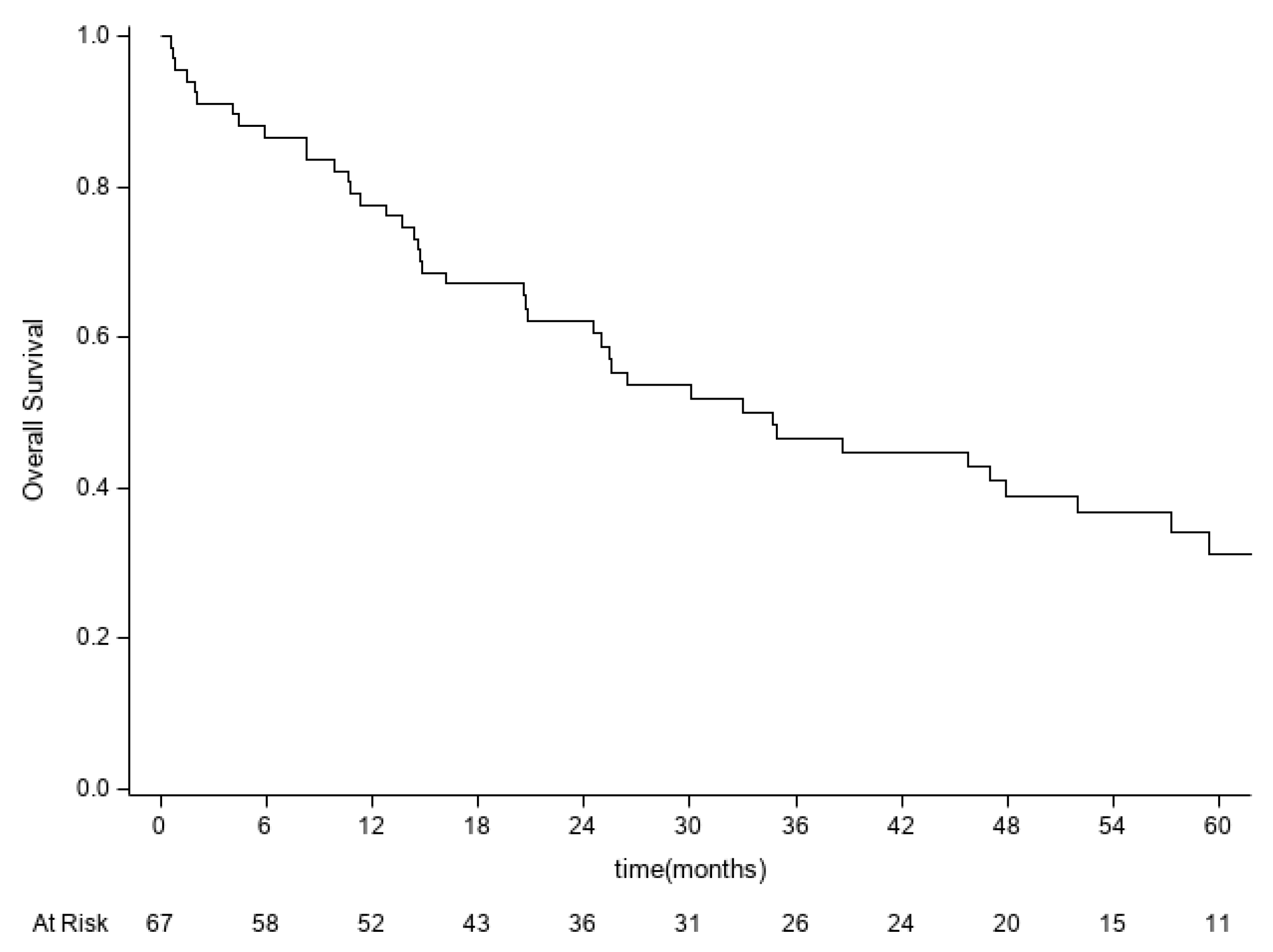
| Variables | Median OS, Months (95% CI) | % 5-Year OS (95% CI) | Log-Rank Test p Value |
|---|---|---|---|
| Age | 0.1742 | ||
| <65 | 26.5 (12.8–57.2) | 25.8% (11.2–43.1) | |
| ≥65 | 47.0 (24.5–70.0) | 37.2% (18.9–55.7) | |
| Gender | 0.0712 | ||
| Female | 58.0 (20.8-nr) | 42.5% (18.6–64.8) | |
| Male | 25.4 (14.8–38.6) | 27.5% (14.4–42.3) | |
| SINS score | |||
| 7–12 | 26.5 (20.5–51.9) | 27.5% (14.9–41.7) | 0.2735 |
| 13–18 | 47.9 (9.8-nr) | 45.0% (18.9–68.2) | |
| Pre-operative Ambulatory status | |||
| Bedridden/Wheelchair/Walking aids | 20.7 (10.6–93.1) | 28.9% (10.3–50.7) | 0.3595 |
| Self-supporting/walking aids | 34.9 (25.4–58.0) | 32.6% (18.0–48.1) | |
| Pre-operative Karnofsky score | 0.5343 | ||
| <70 | 26.5 (14.7–47.9) | 28.0% (13.4–44.5) | |
| ≥70 | 38.6 (16.1–70) | 34.7% (16.3–54.0) | |
| Post-operative Karnofsky score | |||
| <70 | 24.5 (14.3–47.9) | 32.6% (17.5–48.7) | 0.4034 |
| ≥70 | 38.6 (25.4–70) | 32.3% (14.3–51.9) | |
| Intact | |||
| No | 23.7 (62.3- nr) | 33.3% (5.6–65.8) | 0.6630 |
| Yes | 34.9 (24.5–57.2) | 31.6% (18.9–45.1) | |
| Pre-operative Frankel score | |||
| E | 34.7 (20.8–58.0) | 28.7% (13.5–45.9) | 0.7379 |
| other | 26.5 (11.3–93.1) | 34.2% (16.3–53.0) | |
| Post-operative Frankel score | |||
| E | 36.6 (25.0–58.0) | 32.7% (19.0–47.0) | 0.2084 |
| other | 14.6 (1.9-nr) | 30.8% (9.5–55.4) | |
| Tokuhashi score | |||
| 0–8 | 14.7 (1.9–38.6) | 23.4% (6.5–46.3) | 0.0209 |
| 9–11 | 30.1 (16.1–51.9) | 22.5% (9.1–39.4) | |
| 12–15 | nr | 78.6% (36.1–94.4) | |
| Visceral Metastases | |||
| No | 57.2 (34.7–112.3) | 48.8% (29.8–65.4) | <0.001 |
| Yes | 14.8 (8.3–25.0) | 9.0% (0.9–29.3) | |
| Other metastases | |||
| No | 51.9 (25.4–112.3) | 42.0% (23.8–59.2) | 0.0188 |
| Yes | 19.6 (9.8–47.0) | 18.7% (5.8–37.3) | |
| Complications | |||
| No | 45.7 (25.4–58.0) | 33.7% (19.1–49.0) | 0.3632 |
| Yes | 24.5 (14.3-nr)) | 30.6% (12.3–51.2) | |
| Surgery types | |||
| Debulking | 33.1 (20.5–51.9) | 28.0% (14.8–42.8) | 0.0395 |
| En-bloc | nr | 67.5% (29.1–88.2) | |
| other | 14.8 (0.7–47.0) | 16.7% (1.1–49.3) | |
| Pre-radiation | |||
| No | 34.9 (20.8–70.0) | 33.4% (17.3–50.3) | 0.3591 |
| Yes | 25.0 (12.8–93.1) | 33.2% (15.8–51.9) | |
| Post-radiation | |||
| No | 45.7 (16.1-nr) | 39.5% (19.2–59.2) | 0.6594 |
| Yes | 51.9 (26.5–70) | 34.9% (12.5–58.0) | |
| Pre-chemotherapy | |||
| No | 45.7 (20.5–70) | 32.3% (13.4–53.0) | 0.9785 |
| Yes | 25.6 (14.7–93.1) | 35.8% (17.9–54.1) | |
| Post-chemotherapy | |||
| No | nr | 57.1% (17.2–83.7) | 0.6257 |
| Yes | 47.9 (26.5–93.1) | 38.2% (21.0–55.3) |
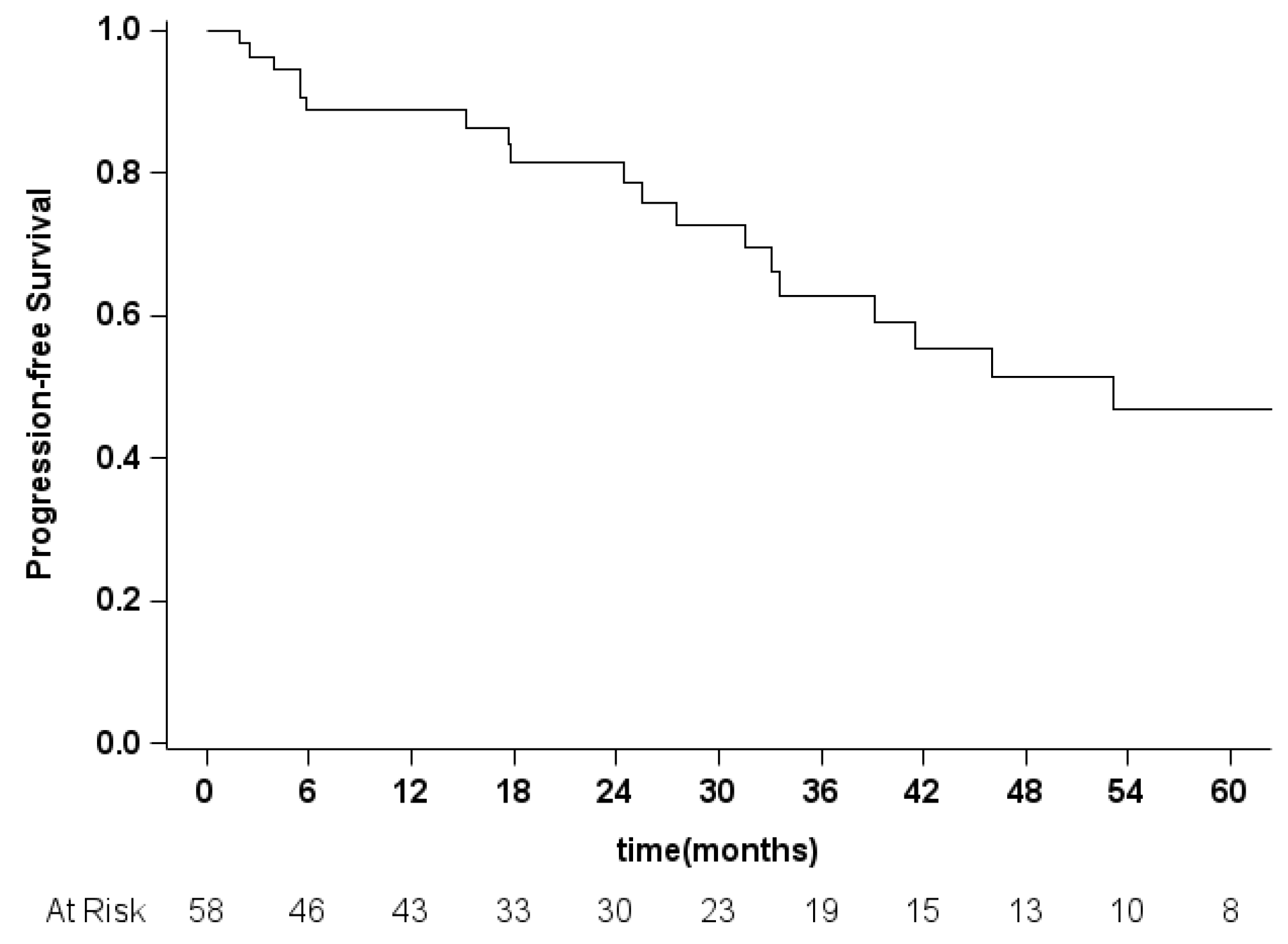
| % 3-Year PFS (95% CI) | Log-Rank Test p Value | |
|---|---|---|
| Age | 0.2452 | |
| <65 | 58.7% (37.1–78.7) | |
| ≥65 | 65.4% (40.8–86.3) | |
| Gender | 0.5787 | |
| Female | 63.9% (33.3–83.3) | |
| Male | 63.3% (40.9–79.2) | |
| SINS score | ||
| 7–12 | 59.5% (38.4–75.5) | 0.3446 |
| 13–18 | 71.8% (34.9–90.0) | |
| Pre-operative Ambulatory status | ||
| Bedridden/Wheelchair/Walking aids | 53.1% (20.3–77.6) | 0.1347 |
| Self-supporting/walking aids | 67.3% (46.4–81.5) | |
| Pre-operative Karnofsky score | 0.8091 | |
| <70 | 57.9% (33.7–76.0) | |
| ≥70 | 67.7% (39.3–84.9) | |
| Post-operative Karnofsky score | ||
| <70 | 62.8% (36.0–80.9) | 0.7643 |
| ≥70 | 63.5% (37.0–81.3) | |
| Intact | ||
| No | 37.5% (1.1–80.8) | 0.2862 |
| Yes | 64.8% (46.2–78.4) | |
| Pre-operative Frankel score | ||
| E | 67.5% (43.6–83.0 | 0.5780 |
| other | 56.7% (29.3–77.0) | |
| Post-operative Frankel score | ||
| E | 63.3% (44.4–77.3) | 0.9992 |
| other | 58.3% (7.7–89.3) | |
| Tokuhashi score | ||
| 0–8 | 42.9% (9.8–73.4) | 0.1523 |
| 9–11 | 61.9% (37.6–79.0) | |
| 12–15 | 100% | |
| Visceral Metastases | ||
| No | 71.7% (48.7–85.7) | 0.1747 |
| Yes | 55.8% (25.5–77.9) | |
| Other metastases | ||
| No | 77.7% (52.8–90.5) | 0.0210 |
| Yes | 44.7% (19.5–67.3) | |
| Complications | ||
| No | 65.4% (43.9–80.4) | 0.5916 |
| Yes | 55.9% (23.0–79.5) | |
| Surgery types | ||
| Debulking | 55.2% (34.3–71.8) | 0.1180 |
| En-bloc | 100% | |
| other | 66.7% (19.5–90.4) | |
| Pre-radiation | ||
| No | 80.4% (55.3–92.2) | 0.0047 |
| Yes | 44.0% (18.0–67.5) | |
| Post-radiation | ||
| No | 62.9% (36.0–81.1) | 0.6380 |
| Yes | 67.0% (39.6–84.2) | |
| Pre-chemotherapy | ||
| No | 73.9% (42.7–89.8) | 0.1973 |
| Yes | 54.4% (28.1–74.7) | |
| Post-chemotherapy | ||
| No | 66.7% (5.4–94.5) | 0.6755 |
| Yes | 65.1% (45.0–79.3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Terzi, S.; Pipola, V.; Griffoni, C.; Trentin, F.; Carretta, E.; Monetta, A.; Vita, F.; Bandiera, S.; Barbanti-Bròdano, G.; Ghermandi, R.; et al. Clear Cell Renal Cell Carcinoma Spinal Metastases: Which Factors Matter to the Overall Survival? A 10-Year Experience of a High-Volume Tumor Spine Center. Diagnostics 2022, 12, 2442. https://doi.org/10.3390/diagnostics12102442
Terzi S, Pipola V, Griffoni C, Trentin F, Carretta E, Monetta A, Vita F, Bandiera S, Barbanti-Bròdano G, Ghermandi R, et al. Clear Cell Renal Cell Carcinoma Spinal Metastases: Which Factors Matter to the Overall Survival? A 10-Year Experience of a High-Volume Tumor Spine Center. Diagnostics. 2022; 12(10):2442. https://doi.org/10.3390/diagnostics12102442
Chicago/Turabian StyleTerzi, Silvia, Valerio Pipola, Cristiana Griffoni, Federica Trentin, Elisa Carretta, Annalisa Monetta, Fabio Vita, Stefano Bandiera, Giovanni Barbanti-Bròdano, Riccardo Ghermandi, and et al. 2022. "Clear Cell Renal Cell Carcinoma Spinal Metastases: Which Factors Matter to the Overall Survival? A 10-Year Experience of a High-Volume Tumor Spine Center" Diagnostics 12, no. 10: 2442. https://doi.org/10.3390/diagnostics12102442