
Current Status of 68Ga-Pentixafor in Solid Tumours

1
Department of Nuclear Medicine, College of Health Sciences, University of KwaZulu Natal, Private Bag X54001, Durban 4001, South Africa
2
Inkosi Albert Luthuli Central Hospital, Durban 4058, South Africa
3
Department of Nuclear Medicine, Faculty of Health Sciences, University of Pretoria, Pretoria 0002, South Africa
4
Department of Genetics, College of Health Sciences, University of KwaZulu Natal, Durban 4058, South Africa
*
Author to whom correspondence should be addressed.
Diagnostics 2022, 12(9), 2135; https://doi.org/10.3390/diagnostics12092135
Submission received: 3 August 2022
/
Accepted: 26 August 2022
/
Published: 2 September 2022
(This article belongs to the Special Issue Recent Trends in Molecular Image-Guided Theranostic and Personalized Medicine)
Abstract
:Chemokine receptor CXCR4 is overexpressed in neoplasms and its expression is related to tumour invasion, metastasis and aggressiveness. 68Ga-Pentixafor is used to non-invasively image the expression of CXCR4 in tumours and has been widely used in haematological malignancies. Recent evidence shows that therapies targeting CXCR4 can increase the chemosensitivity of the tumour as well as inhibit tumour metastasis and aggressiveness. 68Ga-Pentixafor has shown promise as an elegant radiotracer to aid in the selection of patients whose tumours demonstrate CXCR4 overexpression and who therefore may benefit from novel therapies targeting CXCR4. In addition, its therapeutic partners 177Lu- and 90Y-Pentixather have been investigated in the treatment of patients with advanced haematological malignancies, and initial studies have shown a good treatment response in metabolically active lesions. 68Ga-Pentixafor in solid tumours complements 18F-FDG by providing prognostic information and selecting patients who may benefit from therapies targeting CXCR4. This review summarises the available literature on the potential applications of 68Ga-Pentixafor in solid tumours.
1. Introduction
Cancer is a worldwide public health problem due to its rising prevalence with serious morbidity and high mortality despite advances in surgery and chemotherapy agents. Unfortunately, existing therapies (particularly chemoradiation) are often not successful due to the development of resistance, and oncology patients may have very different outcomes even when receiving the same therapies [1]. Therefore, the one size fits all strategy needs to be replaced with personalised therapies that target the specific molecular processes involved. A lot of research has focused on better understanding tumour biology and the tumour microenvironment (TME) in order to develop novel therapies targeting specific mechanisms that have been implicated in promoting tumour cell survival and progression. Small molecules (chemokines), particularly CXCR4 and its ligand CXCL12, are overexpressed in the tumour microenvironment of most malignant tumours [2]. CXCR4 promotes tumour growth, metastasis, angiogenesis and tumour–cell interaction, and its expression is associated with more aggressive tumour behaviour and poorer prognosis [3]. The CXCR4−CXCL12 axis has been implicated in chemotherapy resistance by providing a protective space for tumour cells in the bone marrow and protecting cancer cells from chemotherapy [4]. Therefore, inhibition of the CXCR4 axis should slow tumour progression and metastasis and improve the chemosensitivity of tumours. Pentixafor is a peptide that targets CXCR4 and a theranostic agent capable of being labelled with Gallium-68 (Ga-68) for positron emission tomography (PET) imaging, and Lutetium-177 (Lu-177) for therapy [5]. Several studies investigating CXCR4 expression in solid tumours have shown variable results and discordance between CXCR4 expression in vivo when compared to immunohistochemistry (in vitro expression of CXCR4) in solid tumours. In this review, the role of 68Ga-Pentixafor in the detection of disease in solid tumours will be discussed.
1.1. The Tumour Microenvironment
The tumour microenvironment (TME) is an intricate network of the extracellular matrix (ECM), stromal cells and immune cells working together to create a favourable home for tumour cells [6]. The stromal component of the TME is composed of many different cell types, including the cancer-associated fibroblasts, platelets and immune cells such as neutrophils, macrophages, regulatory T cells, myeloid-derived suppressor cells, natural killer cells and mast cells. These crucial parts of the surrounding stroma regulate cancer development, including the avoidance of apoptosis, initiation of angiogenesis, de-regulation of the energy metabolism and resistance to immune detection and destruction, as well as the activation of invasion and metastasis. The TME contributes to tumour aggressiveness and chemoresistance and provides a hostile environment for cancer treatment [7].
Cancer-associated fibroblasts (CAFs) are a group of activated fibroblasts that promote tumour cell growth and proliferation by secreting a large variety of autocrine and paracrine cytokines as well as other tumour-promoting factors [8]. These factors include chemokines, cytokines and growth factors, such as the vascular endothelial growth factor (VEGF), CXCL12 and CXCL14, and interleukins (ILs) IL-6 and IL-17A, which are critical for tumour cell proliferation, angiogenesis, invasion, inflammation, metastasis and drug resistance [9].
Tumour-associated macrophages (TAMs) produce pro-inflammatory cytokines, such as IL-12, IL-23 and tumour necrosis factor-α (TNF-α), and chemokines (CCL-5, CXCL9, CXCL10 and CXCL5) [6]. TAMs also contribute to the proliferation, invasion and metastasis of tumour cells, promote tumour progression and angiogenesis and suppress the T cell antitumor immune response. In most solid cancers such as squamous cell carcinoma of the head and neck (HNSCC) and neuroblastoma the level of TAM invasion correlates with patient outcome [10].
1.2. The Role of CXCR-4 in Cancer
Chemokines are small, secreted proteins that organize immunologic and inflammatory processes, such as leukocyte trafficking, adhesion, haematopoiesis and angiogenesis [11]. They are classified into four groups (CXC, CC, C and CX3C) based on the position of the first two cysteines [12]. CXCR4, the receptor of chemokine CXCL12/SDF-1 (stromal cell-derived factor-1), is the most studied chemokine receptor; it has a seven-transmembrane structure with seven helical regions connected by six extra-membrane loops.
CXCR4 is overexpressed in more than 30 types of human cancer, including uterine carcinosarcoma, lung squamous cell carcinoma, colorectal adenocarcinoma, pancreatic adenocarcinoma, bladder urothelial carcinoma, lung adenocarcinoma, breast cancer, melanoma and lymphoid neoplasms such as diffuse large B-cell lymphoma among others [13]. Its ligand, CXCL12, is expressed in several organs including the lung, liver, skeletal muscle, brain, kidney, heart, skin and bone marrow [14]. CXCR4 activation promotes the migration of cancer cells towards CXCL12-expressing organs such as the lymph nodes, lungs, bone marrow and liver, which leads to the deposition of metastasis in these organs [15]. In addition, CXCR4 also enhances vasculogenesis and hypoxia-driven angiogenesis through the recruitment of CXCR4-positive pro-angiogenic cells, which also promote the spread of cancer cells [16,17]. CXCL12 induces vascular permeability and allows tumour cell extravasation, thus promoting the metastatic process [18] as demonstrated in Figure 1.
CXCR4 is not only expressed by cancer cells themselves, but also by tumour-infiltrating immune cells. Within the tumour microenvironment, the major CXCR4-expressing cells are B lymphocytes and plasmacytoid dendritic cells, both potentially contributing to an immunosuppressive state, which promotes tumour progression [19]. The CXCR4−CXCL12 axis also provides a protective niche for tumour cells in the bone marrow thereby protecting cancer cells from chemotherapy. A few studies have shown the role of CXCR4 expression in predicting sensitivity to cisplatin-based chemotherapy and the role of CXCR4 antagonists in increasing sensitivity to chemotherapy and in improving prognosis [20,21]. CXCR4 expression is higher in cisplatin-resistant cells compared to cisplatin-sensitive cells.
Molecular imaging of CXCR4 using the CXCR4-specific positron emission tomography (PET) tracer, 68Ga-labeled cyclopentapeptide, [68Ga]CPCR4-2 or 68Ga-Pentixafor developed by Demmer et al. [22] has become a well-established method to non-invasively measure CXCR4 expression in vivo. 68Ga-Pentixafor attaches to both the CXCR4 and macrophage inhibitory factor (MIF) [23].
The normal biodistribution of 68Ga-Pentixafor includes the spleen, kidneys, bone marrow, heart and the liver, which results in undesired tracer accumulation during 177Lu- and 90Y-Pentixather therapy leading to adverse effects [24,25]. The tumour sink effect, which is characterized by lower tracer accumulation in the normal organs of patients with high tumour burden, has been demonstrated with therapies targeting PSMA and SSTR in prostate cancer and well-differentiated neuroendocrine tumours, respectively [26]. As a result, higher activities can be administered in patients with high tumour burden, resulting in the delivery of a more efficacious ablative dose to the tumours while sparing the non-targeted normal organs. Serfling et al. investigated the potential relationship between tumour burden and radiotracer accumulation in 90 patients with solid cancers using 68Ga-Pentixafor. There was no evidence of any tumour sink effect; therefore, the adverse events due to normal tracer biodistribution may limit the administered activity even in patients with a high tumour burden [25]. The authors attributed this difference to the dynamic nature of the CXCR4, which is expressed mainly in the TME compared to PSMA and SSTR, which are more stable and expressed in the tumour cell surface.
Discordance between CXCR4 expression in vivo when compared to immunohistochemistry (in vitro expression of CXCR4) in solid tumours has been reported. For an example, Vag et al. reported that although CXCR4 positivity was seen in vitro in most solid malignancies, including pancreatic carcinoma, laryngeal carcinoma, hepatocellular carcinoma, melanoma, breast cancer, glioblastoma and sarcoma, only low to moderate 68Ga-Pentixafor positivity was noted on PET/CT imaging [27]. This may be attributed to the fact that in vitro CXCR4 binds to the cytoplasm, whereas 68Ga-Pentixafor binds to membrane-associated chemokine receptors, leading to a significant difference between CXCR4 expression profiles determined by immunohistochemistry and the in vivo quantification of CXCR4 using PET probes.
2. CXCR4 in Solid Malignancies
2.1. Head and Neck Squamous Cell Carcinoma
Head and neck squamous cell carcinoma (HNSCC) is the sixth most common non-skin cancer and the eighth leading cause of cancer death worldwide; its incidence is rising, with approximately 874,000 new cases per year and a mortality rate of ~50% [28]. The number of deaths is expected to increase from an estimated 300,000 to 595,000 deaths per year worldwide [29]. The survival rate still remains very low and up to 25% of patients develop recurrence or a second cancer within 5 years after diagnosis [30]. Once distant metastasis is diagnosed in HNSCC, the median time to death is estimated at 4 months [31]. The prognosis remains poor due to the disease recurrence and poor response to current treatment regimens [32]. This has led to research into other therapeutic avenues including the use of novel therapies targeting small molecules (chemokines), the most studied one being CXCR4, which is implicated in tumour cell migration and the formation of metastasis in HNSCC [33].
Qiao et al. explored the impact of CXCR4 in tumour invasion in nasopharyngeal cancer. They found significantly higher CXCR4 expression in high grade tumours compared to low grade tumours and the significant suppression of apoptosis [34]. Antagonism of CXCR4/CXCR7-CXCL12 downregulated the expression of the chemokines axis and therefore could be used to control and potentially even cure nasopharyngeal cancer. This was confirmed in a study by Chen et al. using oral cancer cell lines where they found that CXCR4 antagonist, AMD3100, could affect the cell migration and cell invasion of oral cancers [10]. In a recent publication of 690 tumours imaged with 68Ga-Pentixafor of which 2 had HNSCC, they demonstrated low tracer uptake with a tumour to a background ratio (TBR) of less than 4 as demonstrated in Figure 2, which shows a patient with squamous cell carcinoma of the oral cavity (subsite tongue) showing intense uptake on the 18F-FDG PET/CT but only mild tracer accumulation on the 68Ga-Pentixafor PET. However, this is insufficient evidence to make any conclusions, and prospective studies with bigger sample sizes are needed to confirm this finding.
2.2. Glioblastoma
Glioblastoma (GBM) is the most common primary malignant brain tumour in adults, and has a poor prognosis with a median survival of only 15 months, despite aggressive treatment [35]. The management of GBM consists of a combination of rescue surgery and temozolomide-based chemoradiation therapy [36]. Delineation of the tumour extent and subsequent treatment planning remains a challenge due to the limited accuracy of MRI. GBM tends to recur and curative treatment does not exist currently; therefore, a theragnostic approach might improve survival rates in patients showing CXCR4 expression. The expression of CXCR4 and CXCL12 mRNAs in glioblastoma increases with tumour grade and is associated with regions of necrosis and angiogenesis [37].
Several studies have demonstrated that CXCR4 expression in glioblastoma is associated with a poorer prognosis and more infiltrative phenotypes. For an example, Jacobs et al. showed that CXCR4 mRNA expression correlates with WHO glioma grade, with a relatively higher expression of CXCR4 in high grade gliomas (obtained from 284 samples), whereas normal brain tissue was CXCR4 mRNA negative [23]. In their study, variable CXCR4 expression was demonstrated in 38% of the cores in glioblastoma cells, and CXCR4 expression was high in only a subset of glioblastomas. This is in contrast with findings by Kamatani et al. where CXCR4 immunoreactivity was observed in 24 of 24 (100%) glioblastomas, 9 of 9 (100%) anaplastic astrocytomas and 10 of 11 (91%) astrocytomas or oligoastrocytomas [37]. Similarly Stevenson et al. demonstrated CXCR4 expression in all five glioblastoma samples [38]. This difference could be due to a smaller sample size in the latter studies.
Jacobs et al. went on to correlate in vitro CXCR4 expression with in vivo 68Ga-Pentixafor uptake on PET/CT imaging in seven patients [23]. Five (71%) of the seven patients showed low to moderate tracer uptake, which did not fully correspond with CXCR4 IHC where all patients showed large intra-tumour variation for CXCR4 staining, even within one section. This discrepancy may be attributed to differences in structures between the CXCR4 antibody used for IHC staining and 68Ga-Pentixafor or variability in the blood–brain barrier (BBB) crossing between patients to allow for 68Ga-Pentixafor uptake. The advantage of 68Ga-Pentixafor when compared to 18F-FDG is the absence of physiological brain uptake, which increases tumour detection.
With respect to CXCR4-targeted therapies in glioblastoma, the first and most studied CXCR4 antagonist, AMD3100 (Plerixafor), has been reported to inhibit the growth of GBM36 and to reduce glioblastoma stem cell survival in preclinical studies [39]. However, AMD31000 also shows increased cardiotoxicity associated with some other adverse events after long-term use. This has prompted the search for new, safer and selective CXCR4 inhibitors that are suitable as anti-GBM agents. The newly synthesized CXCR4 antagonist, PRX177561, significantly attenuates GBM tumour growth and might augment the effects of antitumour chemotherapy and radiation therapy (RT) [39]. In addition, PRX177561 increases the DFS and OS when administered to mice bearing orthotopic brain xenografts. 68Ga-Pentixafor may have a role in selecting patients with glioblastoma who may benefit from therapies targeting CXCR4.
2.3. Oesophageal Cancer
Oesophageal cancer (OC) is the eight most common malignant disease and the sixth cause of cancer-related deaths worldwide [36]. The prognosis of OC patients remains unfavourable with 5-year survival rates of only 20 to 36% after curative surgery due to a high potential for lymph node metastasis and vascular invasion. Endoscopic ultrasonography and computed tomography are routine methods of diagnosis of EC patients; however, they have limited usefulness in the early detection of this malignancy, and, therefore, most patients present late with low curative potential [40]. A theragnostic approach might improve survival rates in patients showing CXCR4 expression.
In vitro CXCR4 expression has been shown to correlate with advanced stage, poor differentiation and worse survival in oesophageal cancer. Kaifi et al. demonstrated CXCR4 protein expression in 75 (55%) of 136 oesophageal tumours, and CXCR4 expression was associated with a poor clinical outcome with a median overall survival of 20 months in patients with CXCR4-positive tumours and 76 months for CXCR4-negative tumours [41]. This was confirmed in a meta-analysis of 7 studies looking at 1055 patients with OC, which demonstrated that the overexpression of CXCR4 in OC correlates with reduced OS as well as with tumour depth, lymph node involvement and TNM staging [42]. In a study by Goto et al., 75.6% of the 172 OC specimens stained positive for CXCR4, which significantly correlated with clinical distant metastasis, pathological lymph node metastasis and vascular invasion [43]. Yang et al. performed CXCR4 staining in 101 patients with oesophageal squamous cell carcinoma. Positive expression of CXCR4 was highly expressed in 37.6% (38/101) of OC specimens, and there was no expression in the adjacent normal tissues [44].
In 2015, Kobe et al. published the first clinical experience comparing 68Ga Pentixafor and 18F-FDG in four patients with oesophageal cancer scheduled for radiotherapy [45]. In all patients, FDG was positive for all tumour-suspicious lesions; however, only three out of four patients demonstrated 68Ga-Pentixafor uptake in the lesions. Similarly, Linde et al. compared 68Ga-Pentixafor and 18F-FDG in 10 patients with oesophageal cancer scheduled for radiotherapy. Of the 26 lesions that were counted, 53% of the lesions were positive on both tracers, while 19% of the lesions were FDG positive and Pentixafor negative. Interestingly, Pentixafor revealed more sites of disease than FDG: 7/26 (27%) of the FDG negative lesions were Pentixafor positive [46]. CXCR4 expression was confirmed immunohistochemically in four lesions of the seven patients, where histopathologic correlation was performed. 68Ga-Pentixafor provided additional information that altered patient management, which resulted in the adjustment of the irradiation field based on a Pentixafor-positive and FDG-negative lesion that was detected outside the radiotherapy field.
2.4. Neuroendocrine Tumours
The management of neuroendocrine carcinomas is challenging because most of them present with metastasis and respond poorly to chemotherapy [47]. There has been interest in identifying other treatment options for patients with poorly differentiated neuroendocrine tumours (NETs) including CXCR4-targeted therapies as strong receptor expression on the tumour cell surface would pave the way for CXCR4-targeted radionuclide therapy in somatostatin receptor (SSTR)-negative patients, given the limited treatment options in de-differentiated NETs.
To this end, Werner et al. compared 68Ga-Pentixafor, 68Ga-DOTA-D-Phe-Tyr3-octreotide (68Ga-DOTATOC) and 18F-fluorodeoxyglucose (18F-FDG) in 12 patients with gastroenteropancreatic NET [48]. 68Ga-Pentixafor was the least sensitive of the three tracers and detected tumour lesions in only 50% of the patients, whereas 18F-FDG was positive in 85% and 68Ga-DOTATOC in 92% patients, respectively. As expected, 68Ga-DOTATOC was more sensitive than Pentixafor in well-differentiated NET (G1 and G2 NET), and CXCR4-directed PET was negative in all G1 NET. Conversely, 50% of G2 and 80% of G3 NET patients demonstrated 68Ga-Pentixafor-positive tumour lesions, which is in keeping with higher CXCR4 expression in more aggressive higher grade tumours [48]. 68Ga-Pentixafor uptake was collaborated by histology in 8/9 (89%) of the participants, and the site of histological biopsy was still present for 9/12 subjects. Similarly, Weich et al. investigated 11 treatment-naïve patients with histologically proven neuroendocrine carcinomas (NEC), who underwent 18F-FDG and CXCR4-directed PET/CT for staging and therapy planning [47]. CXCR4-directed imaging was less sensitive compared to FDG, and 68Ga-Pentixafor visualized tumour lesions in 10/11 patients, while 18F-FDG revealed sites of disease in all 11 patients. 18F-FDG PET/CT detected significantly more tumour lesions (102 vs. 42 of the total 107 lesions). Weak to moderate CXCR4 expression could be corroborated by IHC in 10/11 cases [47]. From these studies, it appears that there may be a role for CXCR4-directed imaging in patients with higher grades (G2 and G3) of neuroendocrine tumours. Despite its inferiority to FDG as demonstrated by Weich et al. [47], 68Ga-Pentixafor has a role in higher grade tumours and offers the potential advantage of targeted radionuclide therapy in NECs with no SSTR expression.
2.5. Lung Cancer
Small cell lung cancer (SCLC) represents 15% of all lung cancers and is characterized by a rapid doubling time, the early development of metastases and a poor prognosis. Only one-third of patients are diagnosed with localized disease, and, as a result, treatment strategies have focused on systemic therapy [49]. SCLC is highly responsive to both chemotherapy and radiotherapy initially; however, it has a high recurrence rate within months of treatment due to the development of multidrug resistance (MDR).
Unfortunately, there are limited therapeutic options for relapsed SCLC to date, and new approaches are urgently needed to overcome the MDR of SCLC, which includes the use of CXCR4 antagonists. A few studies have investigated CXCR4 expression in SCLC to see if these patients could potentially benefit from therapies targeting CXCR4. Emerging research shows SCLCs do expresses CXCR4 in vitro, and CXCR4 expression correlates with poor overall survival. Kaemmerer et al. evaluated 34 small cell lung cancer samples by immunohistochemistry, and, in their study, CXCR4 predominantly localized at the plasma membrane of the tumour cells, which was correlated with clinical data and overall patient survival [50].
In a case report, Watts et al. demonstrated higher tracer accumulation on 68Ga-Pentixafor compared to 18F-FDG in SCLC [51]. Furthermore, SCLC showed higher CXCR4 expression in vitro and a higher uptake (SUVmax = 13.2) of 68Ga-Pentixafor (maximum fluorescence intensity MFI = 142.0) compared to NSCLC (MFI = 120; SUVmax = 8.8). This is in line with the higher aggressiveness of SCLC compared to NSCLC. Lapa et al. evaluated 10 patients with therapy-naïve, 3/10, or pretreated, 7/10, lung cancer using 68Ga-Pentixafor PET/CT. Nine (9) of the 10 patients had SCLC and one had large cell neuroendocrine carcinoma of the lung. A comparison with 18F-FDG was performed in six patients and a comparison with 68Ga-DOTATOC was performed in five patients. 68Ga-Pentixafor PET was positive in 80% of the patients and revealed more lesions with significantly higher tumour to background ratios than 68Ga-DOTATOC-PET. Two patients who were 18F-FDG PET positive were negative on 68Ga-Pentixafor-PET. Interestingly, 68Ga-Pentixafor-detected lesions were not seen on 18F-FDG PET. Furthermore, the CXCR4 expression of tumour lesions could be confirmed by immunohistochemistry [49].
Similarly, in a study by Li et al., CXCR4 and CXCL12 were expressed in 97.6% and 78.0% of the six mesothelioma tissue samples, respectively [52]. Conversely, Lapa et al. also compared 18F-FDG and 68Ga-Pentixafor in six patients with pleural mesothelioma as well as immunohistochemistry obtained from biopsy or surgery, and, in their study, none of the six patients presented 68Ga-Pentixafor-positive lesions, whereas 18F-FDG PET revealed positive lesions in all patients [53]. On immunohistochemistry, no significant CXCR4 surface expression was identified in the samples analysed.
CXCR4-targeted therapies in SCLC show promise in preclinical studies; a study by Otani et al. showed a significant decrease in the number and size of lung metastases in mice with CXCR4-expressing SCLC treated with the peptide-based inhibitor of CXCR4, TF14016 [54]. The heterogenous CXCR4 expression shown in these studies shows that CXCR4-targeted imaging cannot replace 18F-FDG in lung cancer; however, CXCR4-targeted imaging with 68Ga-Pentixafor can be used to select patients who may benefit from these therapies and to monitor treatment response. Moreover, CXCR4-targeted imaging may alter patient management in a select group of patients where it shows more lesions than FDG, but this has to be confirmed in a larger cohort.
2.6. Osteosarcoma
Osteosarcoma (OS) is the most common primary malignant tumour of bone with a 5-year survival rate of 25–30% in metastatic OS, which occur in 30% of cases [28]. Although pre- and postoperative chemotherapy has improved prognosis in osteosarcoma (OS), treatment failure is often seen due to high toxicity and resistance to chemotherapy. Recent research has been directed into better understanding tumour biology in order to identify new biomarkers that can predict chemoresistance and therapeutic strategies that may increase drug sensitivity and better control localized and metastatic disease [55].
Gong et al. evaluated 63 tumour samples with CXCR4 immunohistochemistry, and the patients were followed up for 36 months to evaluate for tumour metastasis and patient survival. In that study, 68.5% of tumours showed CXCR4 expression, and of the 45 patients who developed distant metastasis, 33 (73%) had positive expression of CXCR4. The median metastasis-free survival and overall survival was higher in the CXCR4-negative group compared to the CXCR4-positive group [56]. Similarly, Pollino et al. assessed CXCR4 expression in 48 primary osteosarcoma samples compared to 10 healthy bone tissues samples. They demonstrated that in osteosarcoma, CXCR4 expression was directly proportional to the histological grade of the tumour and aggressiveness [55]. Thus far, there is insufficient evidence on the role of 68Ga-Pentixafor in osteosarcoma; however, from the published data on immunohistochemistry, this tracer may have a role in prognosis and selecting patients who may benefit from therapies targeting CXCR4.
2.7. Gynaecological Malignancies
2.7.1. Vulva Cancer
Vulvar squamous cell carcinoma (VSCC) is a rare disease accounting for about 4% of all gynaecological malignancies; however, the incidence is increasing in HIV-infected patients where VSCC is seen in younger patients [57]. VSCC spreads predominantly via lymphatic spread, and the presence of inguinal lymph nodes is an independent predictor of survival. Patients with histologically negative inguinal lymph nodes (LNs) have survival rates of 90% vs. 50% for those with histologically positive inguinal LNs [58].
In a study by Shiozaki et al., in vitro CXCR4 expression was seen in 68% of the 22 tested VSCC samples [59]. CXCR4 expression correlated with more aggressive disease, and higher expression was seen in FIGO stages (III-IV) compared to lower stages (I-II); however, this correlation was not statistically significant (p = 0.08). In addition, the expression rate of CXCR4 in lymph node-positive metastatic disease was very high and CXCR4 expression was associated with poor disease prognosis [59]. Similarly, Rusetska et al. also evaluated CXCR4 expression on tumour and lymph node tissue samples obtained from 46 patients with VSCC as well as 51 patients with premalignant vulvar lesions. CXCR4 overexpression was noted in VSCC samples and none in vulvar precancers; additionally, 98% of the metastatic LNs of patients with VSCC expressed CXCR4 [58]. Again, in vulvar carcinoma, CXCR4-targeted imaging could potentially be used to prognosticate patients as well as to select patients who may benefit from therapies targeting CXCR4. Furthermore, 68Ga-Pentixafor may be able to differentiate premalignant lesions from carcinoma of the vulva.
2.7.2. Cervical Cancer
Cervical cancer is the second most prevalent cancer in the world after breast cancer [60] and represents 6.6% of all cancers of females, with an estimated 570,000 new cases in 2018. In low- and middle-income countries, cervical cancer has a dismal prognosis with an average death rate of 90% [61]. Better treatment strategies are urgently needed since this condition has a high rate of disease recurrence and/or progression of approximately 75% despite the use of available treatment strategies such as surgery, radiotherapy and chemotherapy. Dai et al. evaluated CXCR4 expression in 57 tissue samples consisting of 9 normal cervical tissue samples and 48 cervical cancer samples using immunohistochemistry stains. Of the 48 cancer tissues, 31 (64.58%) were CXCR4 positive, and, in addition, CXCR4 expression correlated with more aggressive histology; that is, it was significantly higher in patients with squamous cell carcinomas and lymph node metastasis [62]. This was confirmed by Schrevel et al. who found that high CXCR4/CXCR7 co-expression independently correlated with shorter disease-specific survival and it was positively associated with larger tumour size and lymph nodes metastasis [18]. Although there are currently no studies demonstrating the role of 68Ga-Pentixafor in cervical cancer, it appears that CXCR4-targeted imaging could potentially be used to prognosticate patients as well as to select patients who may benefit from therapies targeting CXCR4. Figure 3 shows intense 18F-FDG uptake in the cervical carcinoma primary and metastatic left pelvic lymph node (a) and moderate accumulation of 68Ga-Pentixafor in the cervix and very mild uptake in the metastatic lymph node.
2.7.3. Ovarian Cancer
Ovarian cancer is the seventh most common cancer in women globally, and it contributed to approximately 300,000 new cases in 2018 [35]. Ovarian cancer is the main cause of death in gynaecological malignancies. The high mortality of ovarian cancer patients can be attributed to chemotherapy resistance and extensive intraperitoneal metastasis. Although ovarian cancer is one of the most chemo-sensitive malignancies, the prognosis is still poor, even after radical surgical tumour debulking and subsequent chemotherapy [63]. This is believed to be due to the lack of cancer-specific symptoms during the early stages of disease, with ovarian cancer patients usually diagnosed at a late stage with advanced disease. It is estimated that in the USA 80% of ovarian cancer cases have regional or distant cancer spread at the time of cancer diagnosis, and the five-year relative survival of ovarian cancer is less than 50% [64]. There is evidence that CXCR4 is expressed in ovarian cancer primary tumours and its ligand CXCL12 is expressed in the ascitic fluid [64,65]. In a meta-analysis of seven studies (729 patients), it was shown that CXCR4 expression detected on immunohistochemistry staining correlated with more advanced disease and poorer overall survival [64]. There have not been any studies thus far investigating the role of 68Ga-Pentixafor PET/CT in ovarian cancer.
2.8. Breast Cancer
Breast cancer is the most common cancer among women with an estimated 2.3 million new cases diagnosed globally each year; more than 2 million new breast cancer cases were diagnosed in 2020 [66]. Its incidence and death rate have increased over the last three decades due to the change in risk factor profiles. Metastatic breast cancer has a high mortality, especially for late-stage patients [67]. Despite early detection and improved therapeutic regimens, drug resistance, relapse and metastasis still occur and result in significant reduction in the survival of breast cancer patients [68]. CXCR4 receptor and its ligand CXCL12 play a crucial role in the metastasis of various cancer types including breast cancer [69].
The overexpression of CXCR4 on immunohistochemistry has been shown to be associated with poorer prognosis in breast cancer patients. Muller et al. reported that patients with high levels of CXCR4 had more extensive metastasis to lymph nodes compared to those with low levels of CXCR4 [70]. CXCR4 also promotes breast cancer metastasis to organs (bone, liver and lung) where there is an abundance of its ligand, SDF-1. A meta-analysis by Zhang et al. included 13 eligible studies consisting of 3865 participants and showed that CXCR4 overexpression was associated with lymph node infiltration, distant metastasis and significantly reduced disease free survival (DFS) and overall survival (OS) [71]. This was confirmed in a meta-analysis of 15 studies by Xu et al., which included 3104 patients, that showed that the OS and DFS were lower in breast cancer patients with high levels of CXCR4 expression compared to those with low levels of CXCR4 expression [72].
With respect to 68Ga-Pentixafor PET/CT imaging in breast cancer, tracer accumulation is associated with poorer prognosis; however, there is no statistically significant correlation between tracer uptake and molecular subtypes of breast cancer or Ki67% [19]. In a retrospective analysis, Vag et al. evaluated 18 patients with breast cancer with 68Ga Pentixafor PET/CT, and eight patients additionally underwent 18F-FDG PET/CT for staging purposes. Nine (69%) of 13 primary breast cancers were visually detectable on 68Ga-Pentixafor PET images; furthermore, metastases of recurrent breast cancer and unknown primary cancer were visually detectable in all five cases, with a mean SUVmax of 3.5. In another study comparing 68Ga-Pentixafor with 18F-FDG in a heterogenous group of patients of which two had metastatic breast cancer, 68Ga-Pentixafor was inferior to FDG and detected four of the seven metastatic lesions and both the primary tumours seen on 18F-FDG PET/CT [27]. The SUVmax obtained during 18F-FDG PET was higher in all cases compared to CXCR4-targeted PET. This means that 68Ga-Pentixafor could help guide therapy by identifying tumours that would respond to therapies targeting the CXCR4/CXCL12 axis; however it cannot replace 18F-FDG PET/CT in the staging of breast cancer.
2.9. Prostate Cancer
Prostate cancer is the second most common cancer diagnosed in men and the fifth leading cause of death worldwide, and its incidence is increasing [75]. Despite advances in the treatment of localized disease, many patients progress to metastatic castration-resistant prostate cancer, which is associated with poor survival and significant morbidity [76]. There has been a huge breakthrough in the treatment of prostate cancer with hormonal therapies and targeted radionuclide therapies such as 177Lu-PSMA and 225Ac-PSMA, but these are not yet widely available. In prostate cancer patients, CXCR4 expression is significantly associated with a more aggressive disease, the presence of metastasis and poorer cancer-specific survival.
Schwarzenböck et al. compared 68Ga-Pentixafor, 18F FDG and functional MRI in 19 xenograft mouse models and tumour uptake was lower compared to 18F-FDG. Bladder activity was high on 68Ga-Pentixafor due to the predominant urinary excretion of the tracer, which makes delineation of bladder infiltration challenging, and poses the same problem encountered with 68Ga-PSMA and 18F-FDG where bladder and ureteric activity may interfere with the interpretation of locoregional lymph node and prostatic tracer accumulation. Liver uptake of 68Ga-Pentixafor was comparable, whereas kidney uptake of 68Ga-Pentixafor was slightly less than 18F FDG [77]. These studies show that 68Ga-Pentixafor does accumulate in prostate cancer; however, studies comparing this tracer to 68Ga-PSMA are needed to see if CXCR4 targeted imaging and therapy can replace PSMA, especially with the suboptimal response of 177Lu-PSMA in patients with bone metastasis. The advantage of 177Lu-Pentixather over PSMA might be that 177Lu-Pentixather can be directed at tumour cells and neovasculature when CXCR4 is present, unlike PSMA which only targets the neovasculature [23].
2.10. Vestibular Schwannoma
Vestibular schwannomas (VS) are benign nerve sheath tumours of the vestibulocochlear nerve [78]. They can be sporadic or associated with neurofibromatosis type 2 (NF 2). NF 2 tumours have a propensity to recur and to grow more rapidly, and adhere to the cranial nerves and the brainstem more commonly compared to sporadic schwannomas [79]. They are harder to treat with surgery and, thus, alternative treatment options are being investigated including CXCR4 antagonists.
Breun et al. studied CXCR4 expression in 60 vestibular schwannoma (vs) samples and compared them with nerves from autopsies, which served as controls. They found higher expression of CXCR4 in vs compared to the controls: CXCR4 mRNA levels were 4.6-fold higher in vs versus the controls [80]. Furthermore, even though CXCR4 expression was not associated with tumour size, it showed a correlation with tumour invasiveness; that is, higher CXCR4 expression was seen in vs patients with severe hearing loss and deafness.
In another study, four patients with six vs lesions were evaluated with 68Ga-Pentixafor PET/CT. Even though the sample size was very small, they demonstrated the ability of 68Ga-Pentixafor PET/CT to detect all schwannomas with sufficient tumour to background and tumour to blood pool ratios that matched with membranous CXCR4 expression as assessed by immunohistochemistry [78]. Therefore 68Ga-Pentixafor PET/CT could potentially be used to select patients who would benefit from targeted therapies with a CXCR4 antagonist.
2.11. Adrenocortical Carcinoma
Adrenocortical carcinoma (ACC) is a rare and aggressive disease with limited therapeutic options in advanced disease, which commonly recurs despite complete resection [81]. Mitotane in combination with chemotherapy is used as a first-line systemic therapy in patients with metastatic disease; however, recurrence is seen in approximately 50%, even after mitotane therapy, and all available systemic therapies are only palliative. Disease response is achieved in only a minority of patients; therefore, other treatment options are being investigated including CXCR4 inhibitors.
Chifu et al. evaluated the in vitro expression of CXCR4 in 18 ACC tumour samples and found a strong membrane expression of CXCR4 in 50% of ACC samples [82]. Interestingly, strong cytoplasmic CXCR4 staining was more frequent among samples derived from metastases compared to primary tumours and local recurrences. Moreover, CXCR4 membrane staining positively correlated with the proliferation index Ki67. Similarly, Heinze et al. observed CXCR4 membrane staining in 83% of the 21 tumour tissue sections of primary tumours and metastases of ACC, and there was shorter disease free survival in tumours with high CXCR4 expression [83]. There was no difference in progression-free or overall survival observed between patients with strong and weak staining intensities for CXCR4.
Subsequent to that, Buck al. imaged six ACC patients with 68Ga-Pentixafor and found high tracer accumulation in ACC with good target-to-background ratios [84]. Bluemel et al. compared 68Ga-Pentixafor with 18F-FDG in 22 patients with ACC, and the two tracers demonstrated comparable findings in seven (32%) patients [85]. In nine patients (41%), 18F FDG identified more lesions with a visually higher uptake compared to 68Ga-Pentixafor, whereas 68Ga-Pentixafor identified more metastatic lesions than 18F-FDG in two patients (9%). In their study, 12 out of 22 patients (54%) were rated as suitable and 3 patients (14%) as potentially suitable for targeted radionuclide therapy with [177Lu]/[90Y]-labelled Pentixather. Similarly, in another study of thirty patients with histologically proven advanced metastatic ACC who underwent 18F-FDG PET/CT and 68Ga-Pentixafor to evaluate suitability for CXCR4-targeted therapy, 18F-FDG PET/CT provided a superior detection rate than 68Ga-Pentixafor PET/CT with a visually higher uptake in 43% of patients [86]. Again, 68Ga-Pentixafor PET identified more lesions compared with 18F-FDG PET in 2/30 patients (7%) [86]. Therefore, 68Ga-Pentixafor imaging could potentially be used to identify adrenocortical carcinoma patients who would benefit from CXCR4-targeted therapies as not all lesions express CXCR4.
2.12. Colorectal Cancer
Colorectal cancer (CRC) is the third leading cause of cancer-related death worldwide [28]. Unfortunately, about 30% of patients present with metastatic disease involving predominantly the liver, lungs and lymph nodes. The treatment of advanced diseases is multimodal comprising radiotherapy, surgery, and/or chemotherapy and targeted therapies. CRC cells that express high CXCR4 levels have been shown to be more invasive and are associated with worse long term survival, and expression has been reported to be higher in colorectal liver metastases than the primary tumour [87].
Ottaiano et al. evaluated CXCR4 expression in 78 CRC primary colon cancer samples by immunohistochemistry. CXCR4 expression on the primary tumour was an independent prognostic factor and correlated with the response to first-line chemotherapy in metastatic CRC patients [88]. Furthermore, in a meta-analysis, Jiang et al. confirmed that high CXCR4 expression in oesophagus, gastric and colorectal cancer predicted a worse prognosis [89].
In a pilot study, Ahern et al. compared 68Ga-Pentixafor with 18F-FDG PET/CT imaging in eight patients with colorectal adenocarcinoma. In that study, 68Ga-Pentixafor showed low to moderate tracer accumulation, and none of the patients qualified for targeted radionuclide therapy [90]. Furthermore, 68Ga-Pentixafor was inferior to 18F-FDG; therefore, 68Ga-Pentixafor cannot replace but remains complementary to 18F-FDG PET/CT, and its primary role may be in the selection of patients who will benefit from targeted therapy using a CXCR4 antagonist. However, this was a very small sample size, and more research is needed in order to draw reasonable conclusions.
2.13. Neuroblastoma
Neuroblastoma is the most commonly diagnosed extra-cranial solid tumour of infancy and childhood accounting for 8–10% of all paediatric (0–14 years) tumours, and for approximately 15% of cancer-related paediatric mortality [91]. South Africa has a higher-than-average number of patients with high-risk tumours (75.6%), mainly because of advanced disease (70%) and a 54% MYCN amplification of tumours [92]. The prognosis for neuroblastoma remains poor; therefore, there is a need for the development of effective therapies targeting the tumour microenvironment, which creates an unfavourable environment for most of the current treatment strategies [93]. CXCR4 expression is associated with a highly aggressive undifferentiated histopathologic type [13] and poor prognosis in neuroblastoma tumours [94]. CXCR4 favours neuroblastoma metastasis to the liver as well as the lungs and increased bone marrow invasion [7]. 68Ga-Pentixafor may have a role in identifying patients with a poorer prognosis and those who are candidates for therapies targeting CXCR4.
2.14. Hepatocellular Carcinoma
Hepatocellular carcinoma (HCC) is the sixth most common cancer in the world with a rising incidence, and it is the fourth leading cause of cancer death globally [95]. HCC remains asymptomatic until it is very advanced, which makes early detection important in reducing HCC-related mortality. The management of HCC depends on the stage of the tumour and the severity of the underlying liver disease, with resection and transplant still the best curative options for early-stage disease [96]. The role of cytotoxic chemotherapy is limited in HCC. Recent advances in locoregional therapy and molecular targeted systemic therapy, such as small molecule tyrosine kinase inhibitors (TKIs) and immune check point inhibitors, have changed the management of intermediate and advanced HCC. However, these are not readily available due to the high cost, and TKIs are also limited by their side effects.
CXCR4 is overexpressed in 88.33% (65/78) of HCC, where it plays a significant role in the metastasis of HCC by promoting the migration of tumour cells [97]. In a study by Werner et al. comparing 68Ga-Pentixafor and 18F-FDG in a heterogenous group of solid tumours, of which three were HCCs, 68Ga-Pentixafor detected the tumour in only one of the three HCC patients. [98]. This was confirmed by Vag et al. where CXCR4 was detected in vivo in one of the two patients imaged with 68Ga-Pentixafor PET/MRI [27]. Unfortunately, the sample size was too small to draw any meaningful conclusions except to say that non-invasive detection of CXCR4 expression with 68Ga-Pentixafor PET/CT could be used to select patients who would benefit from therapies targeting CXCR4.
2.15. Melanoma
Malignant melanoma is one of the most aggressive neoplasms with frequent radio- and chemotherapy resistance. Malignant melanoma has an incidence of 15–25 per 100,000 individuals, which is increasing faster than any other cancers [28]. Metastatic malignant melanoma has a poor prognosis, with a 15–20% five-year survival rate [99]. Chemotherapy and radiation therapy are not considered to be good options for the treatment of metastatic melanoma because of treatment resistance [100].
Melanoma has a high immunogenicity and is infiltrated with various immune cells including chemokines. CXCR4 enhances the proliferation and survival of melanoma cells by increasing the number of tumour blood vessels. In vivo CXCR4 overexpression in melanoma has been reported [101] and has been found to be higher in metastasis than primary tumours, and, in addition, it is associated with a higher tumour stage [99]. In a meta-analysis of 13 studies investigating the CXCR4 expression in the tumour samples of 656 patients with malignant melanoma, it was found that the high expression of CXCR4 is associated with ulceration, increased tumour thickness and lymph node metastasis [102]. With respect to imaging, in a study by Vag et al. comparing 68Ga-Pentixafor with 18F FDG in a heterogenous group of patients of whom two had malignant melanoma, 68Ga-Pentixafor detected all four of the four metastatic lesions, as did 18FDG PET. On 18F FDG PET/CT, the SUVmax was slightly higher than on 68Ga-Pentixafor [27]. Thus, CXCR4-targeted imaging cannot replace 18F-FDG but may have a role in the selection of potential candidates for therapy with CXCR4 antagonists.
2.16. Cholangiocarcinoma
Cholangiocarcinoma (CCA) is the second most common malignancy of the liver after hepatocellular carcinoma (HCC). It is aggressive and fatal with a median survival of less than 24 months [103]. While surgery is the most effective treatment for resectable CCA [104], unfortunately the clinical symptoms of CCA are non-specific and early diagnosis is often difficult. As a result, the majority of CCA patients are diagnosed at an advanced stage, at which therapeutic options are limited [105]. Thus, CCA patients are offered palliative care with an overall 5-year survival rate of <10%. Due to the lack of effective medical treatment, molecular imaging is essential to guide the discovery of targeted therapies. CXCR4-targeted imaging provides an alternative for possible therapeutic options with a CXCR4 antagonist; however, there is limited evidence on the CXCR4 expression of CCA.
Leelawat et al. demonstrated the upregulation of CXCR4 in cholangiocarcinoma, which is associated with poorer prognosis [106]. This was confirmed by Zhao et al. who investigated the functional role of CXCR4 in the progression and metastasis in 122 patients with intrahepatic cholangiocarcinoma and found CXCR4 expression in the cytoplasm of most IHCC cells but not in the adjacent non-tumorous tissues [107]. Sixty (49%) of the patients had high CXCR4 expression and 62 had low CXCR4 expression and high CXCR4 expression, which were associated with metastasis and a poor clinical outcome of IHCC. Tan et al. demonstrated a positive correlation between the expression of CXCR4 and lymph node metastasis [108].
Werner et al. imaged 19 patients with solid tumours of which 3 had cholangiocarcinoma, and they demonstrated a high uptake of 68Ga-Pentixafor in CCC in both the primary and metastatic lesions in all the patients with CCC [98]. In fact, one of the patients with cholangiocarcinoma demonstrated the highest level of radiotracer uptake (SUVmax, 16.0; TBR, 7.4). This finding needs to be confirmed in a bigger sample but shows promise.
2.17. Pancreatic Ductal Adenocarcinoma
Pancreatic ductal adenocarcinoma (PDAC) is one of the most aggressive tumour types and the fourth leading cause of tumour-related mortality in developed nations [28]. There are no specific tumour markers for PDAC and symptoms are often not present during early disease; therefore, most patients present with advanced, inoperable disease [109]. Current chemotherapeutic drugs that are used for advanced disease stages show dismal results and toxicity seems to be a major problem. Therefore, there is a need to find safe and more effective therapies that can target PDAC. To this end, a lot of work has been carried out to investigate CXCR4 expression in PDAC with a view to establish whether a CXCR4 antagonist can be used in this condition.
In a meta-analysis by Ding et al. of 11 studies (1439 patients), the pooled findings demonstrate that CXCR4 expression is present in PDAC, and it positively correlated with tumour grade, tumour stage, lymph node invasion and distant metastasis [110]. Furthermore, CXCR4 overexpression was a poor prognostic indicator in patients with PDAC. This was confirmed by Krieg et al. who demonstrated that CXCR4 expression levels were related to metastatic disease and overall survival in patients with PDAC in their meta-analysis of nine studies (1183 patients) [109].
In the study by Werner et al. evaluating the uptake of 68Ga-Pentixafor in solid tumours, 4/19 patients reported on had pancreatic ductal adenocarcinoma, which demonstrated mild tracer accumulation with an average TBR of 2.92 (2.07–3.72) [98]. In a recent study by Buck et al. looking at 68Ga-Pentixafor uptake in 690 patients with solid and haematologic tumours, 8/535 scans belonged to patients with pancreatic adenocarcinoma and there was moderate tracer accumulation with a TBR of >4 (average 4–6) [84]. Based on these results, 68Ga-Pentixafor could potentially have a role in the prognosis of pancreatic cancer and selecting patients who may benefit from therapies targeting CXCR4; however, more research is needed to confirm this.
2.18. Renal Cell Carcinoma
Renal cell carcinoma (RCC) is the most lethal of the common urological cancers with a 5-year relative survival of 75.2% in the US [111]. Approximately a third of the patients have metastatic RCC at the time of presentation, and another third who present with local disease will eventually develop disease recurrence and metastases with a median survival of less than one year. RCC is a highly vascularized tumour, in which the von Hippel Lindau tumour suppressor gene is frequently inactivated, leading to the overexpression of the hypoxia-inducible factor (HIF)-2α oncoprotein and CXCR4 overexpression [112].
In a meta-analysis of fourteen studies with 1203 participants by Si et al., they showed that CXCR4 expression is significantly higher in patients with metastatic RCC than in patients with non-metastatic RCC, and CXCR4 expression is significantly associated with poorer prognosis [113]. Pan et al. compared CXCR4 expression in 21 patients with metastatic RCC with three normal volunteer control subjects and they found high CXCR4 expression in the circulating cells of the RCC patients [114].
Werner et al. imaged 19 patients with solid tumours of whom 1 had renal cell carcinoma, and they demonstrated very low uptake and TBR of 68Ga-Pentixafor in RCC [98]. Thus, CXCR4 expression could be a potential biomarker of prognosis and a drug target for personalized treatments for patients with RCC [113], but the evidence is still lacking and more studies are needed to determine whether 68Ga-Pentixafor can reliably detect CXCR4 expression in vivo in patients with RCC.
2.19. Gastric Cancer
Gastric cancer (GC) is one of the most common malignancies globally, and it is the fourth leading cause of cancer-related death [115]. There has been a decline in the incidence and mortality over the past 5 decades; however, gastric cancer still remains one of the leading causes of cancer-related death [116]. The incidence rates for gastric cancer are 2-fold to 3-fold higher for men than women with a mortality rate of 75% in most countries. CXCR4 overexpression has been reported in gastric adenocarcinoma [117], and its expression is associated with high tumour stage, poorer prognosis [118], larger tumour size, lymphatic invasion [87] and carcinomatosis [119].
Thus far, there are no published reports on 68Ga-Pentixafor accumulation in gastric cancer; however, there is evidence from preclinical studies using GC cell lines that there is CXCR4 overexpression.
Table 1 summarises the available data on CXCR4 and the potential applications of 68Ga Pentixafor in solid tumours.
3. Future Direction
An 18F-radiolabelled cyclam-based small molecule radiotracer, [18F]MCFB, for imaging CXCR4 expression has also been investigated in preclinical studies and shows promise as a molecular probe for CXCR4 expression [16]. 18F has superior properties to 68Ga such as a low positron energy, better image quality and adequate half-life (109.7 min). In addition, a 99mTc-labelled agent, [99mTc]TcAMD3465, has been explored for imaging CXCR4 expression in preclinical studies and has shown a significantly high tumour to background ratio; this will be useful in developing countries where PET imaging is not widely available.
3.1. Therapies Targeting CXCR4
The CXCL12/CXCR4 axis has been identified as a target for drug development in oncology due to its critical role in promoting and maintaining cancer stem cells [47]. CXCR4 is present on both the neovasculature and the tumour cells. Blockade of CXCR4 is thought to inhibit all the steps necessary for the development of metastatic foci: not only tumour cell infiltration into CXCL12-producing predestination organs, but also adhesion, migration, invasion and tumour angiogenesis [54]. Cancer stem cells, which are believed to represent a drug-resistant cell population that can survive even chemotherapy, overexpress CXCR4, which correlates with tumour aggressiveness and metastatic potential [27]. Therefore, targeting CXCR4 slows tumour growth, reduces angiogenesis as well as the expression of VEGF [9] and increases the sensitivity of malignancies to chemotherapy, leading to apoptosis [4,120]. Wang et al. demonstrated that the spread and metastasis of oesophageal cancer stem cells could be inhibited by the blockage of CXCR4 [2].
The CXCR4 antagonist Plerixafor (AMD3100) is the first and most studied CXCR4 antagonist, originally developed to block the entry of HIV-1 viruses into T cells through CXCR4 and induce progenitor/stem cell mobilization from the bone marrow for HIV treatment. It also inhibits the binding of CXCL12 to CXCR4 and inhibits cell proliferation, migration and invasion. Plerixafor was approved by the FDA in 2008 for non-Hodgkin’s lymphoma and multiple myeloma [120]. However it is limited by cardiotoxicity, and this has led to development of other CXCR4 antagonists [13]. Another CXCR4 antagonist, BPRCX807, has been shown to be effective in inhibiting migration and suppressing metastasis in hepatocellular carcinoma [121,122]. In addition, GST-NT21MP, which is a synthetic 21-mer peptide antagonist of CXCR4 (NT21MP) derived from the viral macrophage inflammatory protein II, was found to block the CXCR4 pathway, thus decreasing SDF-1-induced cell growth, adhesion and migration capacities in breast cancer cell lines [123]. The newly synthesized CXCR4 antagonist, PRX177561, significantly attenuates GBM tumour growth and might augment the effects of antitumour chemotherapy and RT. In addition, PRX177561 increases the DFS and OS when administered to mice bearing orthotopic brain xenografts [39].
3.2. CXCR4-Targeted Radionuclide Therapy
Initial reports on the role of CXCR4-targeted radionuclide therapies in haematological malignancies using 177Lu- and 90Y-Pentixather have shown promising results, and the treatment was tolerated well with no acute adverse events [29,30,31]. Unfortunately, because the CXCR4-targeted therapies do not only eradicate the CXCR4-expressing malignant cells but also the haematopoietic stem and progenitor cell niche within the bone marrow, haematological toxicity is the most commonly encountered side effect, which often results in fatal neutropenic sepsis [124]. The resultant cytopenia requires that the treatment has to be followed by autologous or allogenic stem cell transplant [26].
Hermann et al. treated three patients with advanced multiple myeloma and there was a good response initial response in two patients with improvement in the 18F-FDG positive lesions [125]. Two of the three patients died, one as a result of disease relapse and the other due to neutropenic sepsis. Maurer et al. treated 22 patients with lymphoproliferative or myeloid malignancies and, even though all patients developed cytopenia, nephrotoxicity and hepatotoxicity were low (seen in 2/25 treatments) and only one patient developed grade three kidney failure due to tumour lysis syndrome [124]. Lapa et al. administered 177Lu- and 90Y-Pentixather to six heavily pretreated relapsed multiple myeloma and acute leukaemia patients and also reported that the treatment was tolerated with a partial response in 2/6 patients and mixed response in 2/6 patients. However, all patients developed aplasia and required stem cell transplantation [126]. Unfortunately, 3/6 patients succumbed to neutropenic sepsis and 3/6 died due to disease progression with a median progression-free survival of 62 d (range, 29–110 d) and median overall survival of 76 d (range, 29–334 d). However, these were all heavily pretreated patients with no other alternative treatment options. Thus far there have been no reports of targeted radionuclide therapy use in solid tumours, and it is likely that haematological toxicity will limit the application of CXCR4 radionuclide therapies to patients with no other treatment options and who will need an autologous or allogenic stem cell transplant [24].
4. Conclusions
CXCR4 expression forms an integral part of tumour survival and spread in several solid malignancies, and its expression is generally associated with more aggressive cancers, a poorer prognosis and high potential for metastases and/or recurrence.
The most promising applications in solid tumours appear to be theranostic approaches to the treatment of refractory advanced cholangiocarcinoma, adrenocortical carcinoma, vestibular schwannoma, small cell lung cancer, oesophageal cancer and high-grade neuroendocrine tumours, to select patients likely to benefit from therapies targeting CXCR4 including targeted radionuclide therapies with 177Lu- and 90Y-Pentixather in combination with stem cell transplantation in a selected group of patients with no other therapeutic options.
Imaging with a CXCR4-targeting tracer generally results in a lower SUVmax and lower target-to-background ratios when compared to 18F-FDG PET. However, in oesophageal and lung cancer, 68Ga-Pentixafor uptake has been demonstrated in 18F-FDG negative lesions, which requires further investigation.
Although 68Ga-Pentixafor-based imaging currently plays a complimentary role to 18F-FDG PET/CT in the staging of solid tumours, it may provide important prognostic information and aid in the selection of patients who may benefit from therapies targeting CXCR4 and in treatment response evaluation.
Author Contributions
Conceptualization, M.M.S.; writing—original draft preparation, B.H.; writing—review and editing, B.H., M.V. and M.M.S.; visualization, M.V. and M.M.S.; supervision, C.A., M.V. and M.M.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| ACC | Adrenocortical carcinoma |
| BBB | Blood–brain barrier |
| CAFs | Cancer-associated fibroblasts |
| CXCR4 | Chemokine receptor 4 |
| DOTATOC | DOTA-D-Phe-Tyr3-octreotide |
| FDG | Fluorodeoxyglucose |
| GBM | Glioblastoma |
| HCC | Hepatocellular carcinoma |
| HNSCC | Head and neck squamous cell carcinoma |
| IHC | Immunohistochemistry |
| MIF | Macrophage inhibitory factor |
| NEC | Neuroendocrine carcinomas |
| NETs | Neuroendocrine tumours |
| NF 2 | Neurofibromatosis type 2 |
| PDAC | Pancreatic ductal adenocarcinoma |
| PET | Positron Emission Tomography |
| PSMA | Prostate specific membrane antigen |
| OC | Oesophageal cancer |
| RCC | Renal cell carcinoma |
| RT | Radiation therapy |
| SCLC | Small cell lung cancer |
| SDF-1 | Stromal cell-derived factor-1 |
| SSTR | Somatostatin receptor |
| TAMs | Tumour-associated macrophages |
| TBR | Tumour to background ratio |
| TKIs | Tyrosine kinase inhibitors |
| TME | Tumour microenvironment |
| TNF | Tumour necrosis factor |
| VEGF | Vascular endothelial growth factor |
| VSCC | Vulvar squamous cell carcinoma |
| VS | Vestibular schwannomas |
References
- Li, J.; Jiang, K.; Qiu, X.; Li, M.; Hao, Q.; Wei, L.; Zhang, W.; Chen, B.; Xin, X. Overexpression of CXCR4 is significantly associated with cisplatin-based chemotherapy resistance and can be a prognostic factor in epithelial ovarian cancer. BMB Rep. 2014, 47, 33. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Wang, L.; Chen, S.-W. Pan-cancer analysis of CXCR4 carcinogenesis in human tumors. Transl. Cancer Res. 2021, 10, 4180–4195. [Google Scholar] [CrossRef] [PubMed]
- Derlin, T.; Grunwald, V.; Steinbach, J.; Wester, H.J.; Ross, T.L. Molecular Imaging in Oncology Using Positron Emission Tomography. Dtsch. Arztebl. Int. 2018, 115, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Knopf, A.; Fritsche, M.K.; Li, Y. CXCR4: A New Player in an Old Scene? ORL J. Otorhinolaryngol. Relat. Spec. 2017, 79, 34–42. [Google Scholar] [CrossRef]
- Spreckelmeyer, S.; Schulze, O.; Brenner, W. Fully-automated production of [(68)Ga]Ga-PentixaFor on the module Modular Lab-PharmTracer. EJNMMI Radiopharm. Chem. 2020, 5, 8. [Google Scholar] [CrossRef]
- Peltanova, B.; Raudenska, M.; Masarik, M. Effect of tumor microenvironment on pathogenesis of the head and neck squamous cell carcinoma: A systematic review. Mol. Cancer 2019, 18, 63. [Google Scholar] [CrossRef]
- Santagata, S.; Ieranò, C.; Trotta, A.M.; Capiluongo, A.; Auletta, F.; Guardascione, G.; Scala, S. CXCR4 and CXCR7 Signaling Pathways: A Focus on the Cross-Talk Between Cancer Cells and Tumor Microenvironment. Front. Oncol. 2021, 11, 591386. [Google Scholar] [CrossRef]
- Kratochwil, C.; Flechsig, P.; Lindner, T.; Abderrahim, L.; Altmann, A.; Mier, W.; Adeberg, S.; Rathke, H.; Röhrich, M.; Winter, H. 68Ga-FAPI PET/CT: Tracer uptake in 28 different kinds of cancer. J. Nucl. Med. 2019, 60, 801–805. [Google Scholar] [CrossRef]
- Porvasnik, S.; Sakamoto, N.; Kusmartsev, S.; Eruslanov, E.; Kim, W.J.; Cao, W.; Urbanek, C.; Wong, D.; Goodison, S.; Rosser, C.J. Effects of CXCR4 antagonist CTCE-9908 on prostate tumor growth. Prostate 2009, 69, 1460–1469. [Google Scholar] [CrossRef]
- Caspa Gokulan, R.; Devaraj, H. Stem Cell Markers CXCR-4 and CD133 Predict Aggressive Phenotype and Their Double Positivity Indicates Poor Prognosis of Oral Squamous Cell Carcinoma. Cancers 2021, 13, 5895. [Google Scholar] [CrossRef]
- Sung, B.; Jhurani, S.; Ahn, K.S.; Mastuo, Y.; Yi, T.; Guha, S.; Liu, M.; Aggarwal, B.B. Zerumbone down-regulates chemokine receptor CXCR4 expression leading to inhibition of CXCL12-induced invasion of breast and pancreatic tumor cells. Cancer Res. 2008, 68, 8938–8944. [Google Scholar] [CrossRef] [PubMed]
- Busillo, J.M.; Benovic, J.L. Regulation of CXCR4 signaling. Biochim. Biophys. Acta 2007, 1768, 952–963. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.-H.; Zhang, S.-F.; Wu, H.-Y.; Gao, J.; Wang, X.-H.; Gao, T.-H. SOX17 inhibits proliferation and invasion of neuroblastoma through CXCL12/CXCR4 signaling axis. Cell. Signal. 2021, 87, 110093. [Google Scholar] [CrossRef] [PubMed]
- Teicher, B.A.; Fricker, S.P. CXCL12 (SDF-1)/CXCR4 pathway in cancer. Clin. Cancer Res. 2010, 16, 2927–2931. [Google Scholar] [CrossRef]
- Martin, M.; Mayer, I.A.; Walenkamp, A.M.; Lapa, C.; Andreeff, M.; Bobirca, A. At the bedside: Profiling and treating patients with CXCR4-expressing cancers. J. Leukoc. Biol. 2021, 109, 953–967. [Google Scholar] [CrossRef]
- Brickute, D.; Braga, M.; Kaliszczak, M.A.; Barnes, C.; Lau, D.; Carroll, L.; Stevens, E.; Trousil, S.; Alam, I.S.; Nguyen, Q.D.; et al. Development and Evaluation of an (18)F-Radiolabeled Monocyclam Derivative for Imaging CXCR4 Expression. Mol. Pharm. 2019, 16, 2106–2117. [Google Scholar] [CrossRef]
- Bao, Y.; Wang, Z.; Liu, B.; Lu, X.; Xiong, Y.; Shi, J.; Li, P.; Chen, J.; Zhang, Z.; Chen, M. A feed-forward loop between nuclear translocation of CXCR4 and HIF-1α promotes renal cell carcinoma metastasis. Oncogene 2019, 38, 881–895. [Google Scholar] [CrossRef]
- Schrevel, M.; Karim, R.; Ter Haar, N.; Van Der Burg, S.; Trimbos, J.; Fleuren, G.; Gorter, A.; Jordanova, E. CXCR7 expression is associated with disease-free and disease-specific survival in cervical cancer patients. Br. J. Cancer 2012, 106, 1520–1525. [Google Scholar] [CrossRef]
- Vag, T.; Steiger, K.; Rossmann, A.; Keller, U.; Noske, A.; Herhaus, P.; Ettl, J.; Niemeyer, M.; Wester, H.J.; Schwaiger, M. PET imaging of chemokine receptor CXCR4 in patients with primary and recurrent breast carcinoma. EJNMMI Res. 2018, 8, 90. [Google Scholar] [CrossRef]
- Labrosse, B.; Treboute, C.; Brelot, A.; Alizon, M. Cooperation of the V1/V2 and V3 domains of human immunodeficiency virus type 1 gp120 for interaction with the CXCR4 receptor. J. Virol. 2001, 75, 5457–5464. [Google Scholar] [CrossRef] [Green Version]
- Bleul, C.C.; Wu, L.; Hoxie, J.A.; Springer, T.A.; Mackay, C.R. The HIV coreceptors CXCR4 and CCR5 are differentially expressed and regulated on human T lymphocytes. Proc. Natl. Acad. Sci. USA 1997, 94, 1925–1930. [Google Scholar] [CrossRef]
- Demmer, O.; Gourni, E.; Schumacher, U.; Kessler, H.; Wester, H.J. PET imaging of CXCR4 receptors in cancer by a new optimized ligand. ChemMedChem 2011, 6, 1789–1791. [Google Scholar] [CrossRef]
- Jacobs, S.M.; Wesseling, P.; de Keizer, B.; Tolboom, N.; Ververs, F.F.T.; Krijger, G.C.; Westerman, B.A.; Snijders, T.J.; Robe, P.A.; van der Kolk, A.G. CXCR4 expression in glioblastoma tissue and the potential for PET imaging and treatment with [(68)Ga]Ga-Pentixafor /[(177)Lu]Lu-Pentixather. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 481–491. [Google Scholar] [CrossRef]
- Buck, A.K.; Serfling, S.E.; Lindner, T.; Hänscheid, H.; Schirbel, A.; Hahner, S.; Fassnacht, M.; Einsele, H.; Werner, R.A. CXCR4-targeted theranostics in oncology. Eur. J. Nucl. Med. Mol. Imaging 2022, 8, 1–12. [Google Scholar] [CrossRef]
- Serfling, S.E.; Lapa, C.; Dreher, N.; Hartrampf, P.E.; Rowe, S.P.; Higuchi, T.; Schirbel, A.; Weich, A.; Hahner, S.; Fassnacht, M. Impact of tumor burden on normal organ distribution in patients imaged with CXCR4-targeted [68Ga] Ga-PentixaFor PET/CT. Mol. Imaging Biol. 2022, 24, 659–665. [Google Scholar] [CrossRef]
- Beauregard, J.-M.; Hofman, M.S.; Kong, G.; Hicks, R.J. The tumour sink effect on the biodistribution of 68Ga-DOTA-octreotate: Implications for peptide receptor radionuclide therapy. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 50–56. [Google Scholar] [CrossRef]
- Vag, T.; Gerngross, C.; Herhaus, P.; Eiber, M.; Philipp-Abbrederis, K.; Graner, F.-P.; Ettl, J.; Keller, U.; Wester, H.-J.; Schwaiger, M. First experience with chemokine receptor CXCR4–targeted PET imaging of patients with solid cancers. J. Nucl. Med. 2016, 57, 741–746. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Cohen, N.; Fedewa, S.; Chen, A.Y. Epidemiology and Demographics of the Head and Neck Cancer Population. Oral Maxillofac. Surg. Clin. N. Am. 2018, 30, 381–395. [Google Scholar] [CrossRef]
- Lefebvre, J.-L. Current clinical outcomes demand new treatment options for SCCHN. Ann. Oncol. 2005, 16 (Suppl. S6), vi7–vi12. [Google Scholar] [CrossRef]
- Castelli, J.; Depeursinge, A.; Ndoh, V.; Prior, J.O.; Ozsahin, M.; Devillers, A.; Bouchaab, H.; Chajon, E.; De Crevoisier, R.; Scher, N. A PET-based nomogram for oropharyngeal cancers. Eur. J. Cancer 2017, 75, 222–230. [Google Scholar] [CrossRef] [PubMed]
- Chin, D.; Boyle, G.M.; Porceddu, S.; Theile, D.R.; Parsons, P.G.; Coman, W.B. Head and neck cancer: Past, present and future. Expert Rev. Anticancer Ther. 2006, 6, 1111–1118. [Google Scholar] [CrossRef] [PubMed]
- Choi, W.T.; An, J. Biology and clinical relevance of chemokines and chemokine receptors CXCR4 and CCR5 in human diseases. Exp. Biol. Med. 2011, 236, 637–647. [Google Scholar] [CrossRef] [PubMed]
- Qiao, N.; Wang, L.; Wang, T.; Li, H. Inflammatory CXCL12-CXCR4/CXCR7 axis mediates G-protein signaling pathway to influence the invasion and migration of nasopharyngeal carcinoma cells. Tumour Biol. 2016, 37, 8169–8179. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Ostrom, Q.T.; Cioffi, G.; Waite, K.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2014–2018. Neuro-Oncology 2021, 23 (Suppl. S3), iii1–iii105. [Google Scholar] [CrossRef]
- Komatani, H.; Sugita, Y.; Arakawa, F.; Ohshima, K.; Shigemori, M. Expression of CXCL12 on pseudopalisading cells and proliferating microvessels in glioblastomas: An accelerated growth factor in glioblastomas. Int. J. Oncol. 2009, 34, 665–672. [Google Scholar]
- Stevenson, C.B.; Ehtesham, M.; McMillan, K.M.; Valadez, J.G.; Edgeworth, M.L.; Price, R.R.; Abel, T.W.; Mapara, K.Y.; Thompson, R.C. CXCR4 Expression is elevated in glioblastoma multiforme and correlates with an increase in intensity and extent of peritumoral T2-weighted magnetic resonance imaging signal abnormalities. Neurosurgery 2008, 63, 560–570. [Google Scholar] [CrossRef]
- Gravina, G.L.; Mancini, A.; Colapietro, A.; Vitale, F.; Vetuschi, A.; Pompili, S.; Rossi, G.; Marampon, F.; Richardson, P.J.; Patient, L. The novel CXCR4 antagonist, PRX177561, reduces tumor cell proliferation and accelerates cancer stem cell differentiation in glioblastoma preclinical models. Tumor Biol. 2017, 39, 1010428317695528. [Google Scholar] [CrossRef]
- Arnal, M.J.D.; Arenas, Á.F.; Arbeloa, Á.L. Esophageal cancer: Risk factors, screening and endoscopic treatment in Western and Eastern countries. World J. Gastroenterol. WJG 2015, 21, 7933. [Google Scholar] [CrossRef]
- Kaifi, J.T.; Yekebas, E.F.; Schurr, P.; Obonyo, D.; Wachowiak, R.; Busch, P.; Heinecke, A.; Pantel, K.; Izbicki, J.R. ARTICLES Tumor-Cell Homing to Lymph Nodes and Bone Marrow and CXCR4 Expression in Esophageal Cancer. J. Natl. Cancer Inst. 2005, 97, 1840–1847. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Wu, X.; Liang, W.; Chen, C.; Zheng, L.; An, H. Clinicopathological and prognostic significance of chemokine receptor CXCR4 overexpression in patients with esophageal cancer: A meta-analysis. Tumor Biol. 2014, 35, 3709–3715. [Google Scholar] [CrossRef] [PubMed]
- Goto, M.; Yoshida, T.; Yamamoto, Y.; Furukita, Y.; Inoue, S.; Fujiwara, S.; Kawakita, N.; Nishino, T.; Minato, T.; Yuasa, Y.; et al. CXCR4 Expression is Associated with Poor Prognosis in Patients with Esophageal Squamous Cell Carcinoma. Ann. Surg. Oncol. 2017, 24, 832–840. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Lu, Q.; Xu, Y.; Liu, C.; Sun, Q. Clinicopathologic significance of CXCR4 expressions in patients with esophageal squamous cell carcinoma. Pathol.-Res. Pract. 2020, 216, 152787. [Google Scholar] [CrossRef]
- Kobe, C.; Baues, C.; Nast-Kolb, B.; Stockter, S.; Kuhnert, G.; Wester, H.; Fischer, T.; Schomäcker, K.; Drzezga, A. First clinical experience with [68] Ga-Pentixafor PET/CT in esophageal cancer. Soc. Nucl. Med. 2015, 56 (Suppl. S3), 635. [Google Scholar]
- Linde, P.; Baues, C.; Wegen, S.; Trommer, M.; Quaas, A.; Rosenbrock, J.; Celik, E.; Marnitz, S.; Bruns, C.J.; Fischer, T.; et al. Pentixafor PET/CT for imaging of chemokine receptor 4 expression in esophageal cancer—A first clinical approach. Cancer Imaging 2021, 21, 22. [Google Scholar] [CrossRef]
- Weich, A.; Werner, R.A.; Buck, A.K.; Hartrampf, P.E.; Serfling, S.E.; Scheurlen, M.; Wester, H.-J.; Meining, A.; Kircher, S.; Higuchi, T.; et al. CXCR4-Directed PET/CT in Patients with Newly Diagnosed Neuroendocrine Carcinomas. Diagnostics 2021, 11, 605. [Google Scholar] [CrossRef]
- Werner, R.A.; Weich, A.; Higuchi, T.; Schmid, J.S.; Schirbel, A.; Lassmann, M.; Wild, V.; Rudelius, M.; Kudlich, T.; Herrmann, K.; et al. Imaging of Chemokine Receptor 4 Expression in Neuroendocrine Tumors—A Triple Tracer Comparative Approach. Theranostics 2017, 7, 1489–1498. [Google Scholar] [CrossRef]
- Lapa, C.; Lückerath, K.; Rudelius, M.; Schmid, J.-S.; Schoene, A.; Schirbel, A.; Samnick, S.; Pelzer, T.; Buck, A.K.; Kropf, S. [68Ga] Pentixafor-PET/CT for imaging of chemokine receptor 4 expression in small cell lung cancer-initial experience. Oncotarget 2016, 7, 9288. [Google Scholar] [CrossRef]
- Kaemmerer, D.; Reimann, C.; Specht, E.; Wirtz, R.M.; Sayeg, M.; Baum, R.P.; Schulz, S.; Lupp, A. Differential expression and prognostic value of the chemokine receptor CXCR4 in bronchopulmonary neuroendocrine neoplasms. Oncotarget 2015, 6, 3346. [Google Scholar] [CrossRef]
- Watts, A.; Singh, B.; Basher, R.; Singh, H.; Bal, A.; Kapoor, R.; Arora, S.K.; Wester, H.J.; Mittal, B.R.; Behera, D. 68Ga-Pentixafor PET/CT demonstrating higher CXCR4 density in small cell lung carcinoma than in non-small cell variant. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 909–910. [Google Scholar] [CrossRef]
- Li, T.; Li, H.; Wang, Y.; Harvard, C.; Tan, J.L.; Au, A.; Xu, Z.; Jablons, D.M.; You, L. The expression of CXCR4, CXCL12 and CXCR7 in malignant pleural mesothelioma. J. Pathol. 2011, 223, 519–530. [Google Scholar] [CrossRef] [Green Version]
- Lapa, C.; Kircher, S.; Schirbel, A.; Rosenwald, A.; Kropf, S.; Pelzer, T.; Walles, T.; Buck, A.K.; Weber, W.A.; Wester, H.J.; et al. Targeting CXCR4 with [(68)Ga]Pentixafor: A suitable theranostic approach in pleural mesothelioma? Oncotarget 2017, 8, 96732–96737. [Google Scholar] [CrossRef]
- Otani, Y.; Kijima, T.; Kohmo, S.; Oishi, S.; Minami, T.; Nagatomo, I.; Takahashi, R.; Hirata, H.; Suzuki, M.; Inoue, K. Suppression of metastases of small cell lung cancer cells in mice by a peptidic CXCR4 inhibitor TF14016. FEBS Lett. 2012, 586, 3639–3644. [Google Scholar] [CrossRef]
- Pollino, S.; Palmerini, E.; Dozza, B.; Bientinesi, E.; Piccinni-Leopardi, M.; Lucarelli, E.; Righi, A.; Benassi, M.S.; Pazzaglia, L. CXCR4 in human osteosarcoma malignant progression. The response of osteosarcoma cell lines to the fully human CXCR4 antibody MDX1338. J. Bone Oncol. 2019, 17, 100239. [Google Scholar] [CrossRef]
- Gong, C.; Sun, K.; Xiong, H.H.; Sneh, T.; Zhang, J.; Zhou, X.; Yan, P.; Wang, J.H. Expression of CXCR4 and MMP-2 is associated with poor prognosis in patients with osteosarcoma. Histol. Histopathol. 2020, 35, 863–870. [Google Scholar] [CrossRef]
- Firnhaber, C.; Wilkin, T. Human papillomavirus vaccines: Where do they fit in HIV-infected individuals? Curr. HIV/AIDS Rep. 2012, 9, 278–286. [Google Scholar] [CrossRef]
- Rusetska, N.; Kowalski, K.; Zalewski, K.; Zięba, S.; Bidziński, M.; Goryca, K.; Kotowicz, B.; Fuksiewicz, M.; Kopczynski, J.; Bakuła-Zalewska, E. CXCR4/ACKR3/CXCL12 axis in the lymphatic metastasis of vulvar squamous cell carcinoma. J. Clin. Pathol. 2021, 75, 324–332. [Google Scholar] [CrossRef]
- Shiozaki, T.; Tabata, T.; Ma, N.; Yamawaki, T.; Motohashi, T.; Kondo, E.; Tanida, K.; Okugawa, T.; Ikeda, T. Association of CXC chemokine receptor type 4 expression and clinicopathologic features in human vulvar cancer. Int. J. Gynecol. Cancer 2013, 23, 1111–1117. [Google Scholar] [CrossRef]
- Sun, W.-L.; Shen, Y.; Yuan, Y.; Zhou, X.-J.; Li, W.-P. The value and clinical significance of tumor marker detection in cervical cancer. Sci. Program. 2021, 2021, 6643782. [Google Scholar] [CrossRef]
- Oany, A.R.; Mia, M.; Pervin, T.; Alyami, S.A.; Moni, M.A. Integrative Systems Biology Approaches to Identify Potential Biomarkers and Pathways of Cervical Cancer. J. Pers. Med. 2021, 11, 363. [Google Scholar] [CrossRef] [PubMed]
- Dai, Y.; Tong, R.; Guo, H.; Yu, T.; Wang, C. Association of CXCR4, CCR7, VEGF-C and VEGF-D expression with lymph node metastasis in patients with cervical cancer. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 214, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Xi, Y.; Feng, Y. Ovarian cancer risk in relation to blood lipid levels and hyperlipidemia: A systematic review and meta-analysis of observational epidemiologic studies. Eur. J. Cancer Prev. 2021, 30, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.-F.; Liu, S.-Y.; Min, X.-Y.; Ji, Y.-Y.; Wang, N.; Liu, D.; Ma, N.; Li, Z.-F.; Li, K. The prognostic value of CXCR4 in ovarian cancer: A meta-analysis. PLoS ONE 2014, 9, e92629. [Google Scholar] [CrossRef] [PubMed]
- Scotton, C.J.; Wilson, J.L.; Scott, K.; Stamp, G.; Wilbanks, G.D.; Fricker, S.; Bridger, G.; Balkwill, F.R. Multiple actions of the chemokine CXCL12 on epithelial tumor cells in human ovarian cancer. Cancer Res. 2002, 62, 5930–5938. [Google Scholar] [PubMed]
- Łukasiewicz, S.; Czeczelewski, M.; Forma, A.; Baj, J.; Sitarz, R.; Stanisławek, A. Breast Cancer—Epidemiology, Risk Factors, Classification, Prognostic Markers, and Current Treatment Strategies—An Updated Review. Cancers 2021, 13, 4287. [Google Scholar] [CrossRef] [PubMed]
- Dong, J.; Zhu, C.; Zhang, F.; Zhou, Z.; Sun, M. “Attractive/adhesion force” dual-regulatory nanogels capable of CXCR4 antagonism and autophagy inhibition for the treatment of metastatic breast cancer. J. Control. Release 2022, 341, 892–903. [Google Scholar] [CrossRef] [PubMed]
- Zhu, T.; Zheng, J.; Zhuo, W.; Pan, P.; Li, M.; Zhang, W.; Zhou, H.; Gao, Y.; Li, X.; Liu, Z. ETV4 promotes breast cancer cell stemness by activating glycolysis and CXCR4-mediated sonic Hedgehog signaling. Cell Death Discov. 2021, 7, 126. [Google Scholar] [CrossRef]
- Mukherjee, D.; Zhao, J. The Role of chemokine receptor CXCR4 in breast cancer metastasis. Am. J. Cancer Res. 2013, 3, 46. [Google Scholar]
- Muller, A.; Homey, B.; Soto, H.; Ge, N.; Catron, D.; Buchanan, M.; McClanahan, T.; Murphy, E.; Yuan, W.; Wagner, S.; et al. Involvement of chemokine receptors in breast cancer metastasis. Nature 2001, 410, 6824. [Google Scholar] [CrossRef]
- Zhang, Z.; Ni, C.; Chen, W.; Wu, P.; Wang, Z.; Yin, J.; Huang, J.; Qiu, F. Expression of CXCR4 and breast cancer prognosis: A systematic review and meta-analysis. BMC Cancer 2014, 14, 126. [Google Scholar] [CrossRef]
- Xu, T.-p.; Shen, H.; Liu, L.-x.; Shu, Y.-q. The impact of chemokine receptor CXCR4 on breast cancer prognosis: A meta-analysis. Cancer Epidemiol. 2013, 37, 725–731. [Google Scholar] [CrossRef]
- Xu, C.; Zhao, H.; Chen, H.; Yao, Q. CXCR4 in breast cancer: Oncogenic role and therapeutic targeting. Drug Des. Dev. Ther. 2015, 9, 4953. [Google Scholar]
- Yang, Q.; Zhang, F.; Ding, Y.; Huang, J.; Chen, S.; Wu, Q.; Wang, Z.; Chen, C. Antitumour activity of the recombination polypeptide GST-NT21MP is mediated by inhibition of CXCR4 pathway in breast cancer. Br. J. Cancer 2014, 110, 1288–1297. [Google Scholar] [CrossRef] [Green Version]
- Rawla, P. Epidemiology of prostate cancer. World J. Oncol. 2019, 10, 63. [Google Scholar] [CrossRef]
- Vorster, M.; Sathekge, M.M. Theranostics in Metastatic Castrate Resistant Prostate Cancer; Exon Publications: Brisbane, Australia, 2021; pp. 81–96. [Google Scholar]
- Schwarzenböck, S.M.; Stenzel, J.; Otto, T.; Helldorff, H.V.; Bergner, C.; Kurth, J.; Polei, S.; Lindner, T.; Rauer, R.; Hohn, A.; et al. [(68)Ga]pentixafor for CXCR4 imaging in a PC-3 prostate cancer xenograft model—Comparison with [(18)F]FDG PET/CT, MRI and ex vivo receptor expression. Oncotarget 2017, 8, 95606–95619. [Google Scholar] [CrossRef]
- Breun, M.; Monoranu, C.M.; Kessler, A.F.; Matthies, C.; Löhr, M.; Hagemann, C.; Schirbel, A.; Rowe, S.P.; Pomper, M.G.; Buck, A.K.; et al. [(68)Ga]-Pentixafor PET/CT for CXCR4-Mediated Imaging of Vestibular Schwannomas. Front. Oncol. 2019, 9, 503. [Google Scholar] [CrossRef]
- Carlson, M.L.; Link, M.J. Vestibular schwannomas. N. Engl. J. Med. 2021, 384, 1335–1348. [Google Scholar] [CrossRef]
- Breun, M.; Schwerdtfeger, A.; Martellotta, D.D.; Kessler, A.F.; Perez, J.M.; Monoranu, C.M.; Ernestus, R.I.; Matthies, C.; Löhr, M.; Hagemann, C. CXCR4: A new player in vestibular schwannoma pathogenesis. Oncotarget 2018, 9, 9940–9950. [Google Scholar] [CrossRef]
- Kimpel, O.; Bedrose, S.; Megerle, F.; Berruti, A.; Terzolo, M.; Kroiss, M.; Mai, K.; Dekkers, O.M.; Habra, M.A.; Fassnacht, M. Adjuvant platinum-based chemotherapy in radically resected adrenocortical carcinoma: A cohort study. Br. J. Cancer 2021, 125, 1233–1238. [Google Scholar] [CrossRef]
- Chifu, I.; Heinze, B.; Fuss, C.T.; Lang, K.; Kroiss, M.; Kircher, S.; Ronchi, C.L.; Altieri, B.; Schirbel, A.; Fassnacht, M. Impact of the chemokine receptors CXCR4 and CXCR7 on clinical outcome in adrenocortical carcinoma. Front. Endocrinol. 2020, 11, 597878. [Google Scholar] [CrossRef]
- Heinze, B.; Bluemel, C.; Chifu, I.; Schirbel, A.; Burger-Stritt, S.; Hirsch, K.; Lang, K.; Schottelius, M.; Wester, H.; Lapa, C. A novel theranostic concept for adrenocortical neoplasia targeting the chemokine receptor CXCR4. Exp. Clin. Endocrinol. Diabetes 2015, 123, OP1_01. [Google Scholar] [CrossRef]
- Buck, A.K.; Haug, A.; Dreher, N.; Lambertini, A.; Higuchi, T.; Lapa, C.; Weich, A.; Pomper, M.G.; Wester, H.J.; Zehnder, A.; et al. Imaging of C-X-C Motif Chemokine Receptor 4 Expression in 690 Patients with Solid or Hematologic Neoplasms using (68)Ga-PentixaFor PET. J. Nucl. Med. 2022, 63, e29–e34. [Google Scholar] [CrossRef]
- Bluemel, C.; Lapa, C.; Schirbel, A.; Fassnacht, M.; Allolio, B.; Schottelius, M.; Kropf, S.; Wester, H.; Hahner, S.; Herrmann, K. A theranostic approach for adrenocortical neoplasia based on high adrenal CXCR4 expression. Soc. Nucl. Med. 2015, 56, 145. [Google Scholar]
- Bluemel, C.; Hahner, S.; Heinze, B.; Fassnacht, M.; Kroiss, M.; Bley, T.A.; Wester, H.-J.; Kropf, S.; Lapa, C.; Schirbel, A. Investigating the chemokine receptor 4 as potential theranostic target in adrenocortical cancer patients. Clin. Nucl. Med. 2017, 42, e29–e34. [Google Scholar] [CrossRef]
- Daniel, S.K.; Seo, Y.D.; Pillarisetty, V.G. The CXCL12-CXCR4/CXCR7 axis as a mechanism of immune resistance in gastrointestinal malignancies. Semin. Cancer Biol. 2020, 65, 176–188. [Google Scholar] [CrossRef]
- Ottaiano, A.; Scala, S.; Normanno, N.; Botti, G.; Tatangelo, F.; Di Mauro, A.; Capozzi, M.; Facchini, S.; Tafuto, S.; Nasti, G. Prognostic and Predictive Role of CXC Chemokine Receptor 4 in Metastatic Colorectal Cancer Patients. Appl. Immunohistochem. Mol. Morphol. 2020, 28, 755–760. [Google Scholar] [CrossRef]
- Jiang, Q.; Sun, Y.; Liu, X. CXCR4 as a prognostic biomarker in gastrointestinal cancer: A meta-analysis. Biomarkers 2019, 24, 510–516. [Google Scholar] [CrossRef]
- Ahern, E.; Thomas, P.; Campbell, L.; Latter, M.; Eastgate, M.; Wyld, D.; Clark, D.A.; Stevenson, A.R.; O’Rourke, N.; Cavallucci, D. Pentixafor as a Theranostic Agent in Rectal and Pancreatic Adenocarcinoma: Outcomes from a Pilot Study. 2022. Available online: https://assets.researchsquare.com/files/rs-1274952/v2/a428a666-268f-4ecb-ab7b-775009d7d389.pdf?c=1650455491 (accessed on 11 June 2022).
- Karalexi, M.A.; Katsimpris, A.; Panagopoulou, P.; Bouka, P.; Schüz, J.; Ntzani, E.; Petridou, E.T.; Servitzoglou, M.; Baka, M.; Moschovi, M. Maternal lifestyle factors and risk of neuroblastoma in the offspring: A meta-analysis including Greek NARECHEM-ST primary data. Cancer Epidemiol. 2022, 77, 102055. [Google Scholar] [CrossRef]
- Van Heerdena, J. The management and outcomes of neuroblastoma in South African children. Belg. J. Paediatr. 2021, 23, 330–333. [Google Scholar]
- Quinn, C.H.; Beierle, A.M.; Beierle, E.A. Artificial Tumor Microenvironments in Neuroblastoma. Cancers 2021, 13, 1629. [Google Scholar] [CrossRef]
- Liberman, J.; Sartelet, H.; Flahaut, M.; Mühlethaler-Mottet, A.; Coulon, A.; Nyalendo, C.; Vassal, G.; Joseph, J.M.; Gross, N. Involvement of the CXCR7/CXCR4/CXCL12 axis in the malignant progression of human neuroblastoma. PLoS ONE 2012, 7, e43665. [Google Scholar] [CrossRef]
- McGlynn, K.A.; Petrick, J.L.; El-Serag, H.B. Epidemiology of hepatocellular carcinoma. Hepatology 2021, 73, 4–13. [Google Scholar] [CrossRef]
- Samant, H.; Amiri, H.S.; Zibari, G.B. Addressing the worldwide hepatocellular carcinoma: Epidemiology, prevention and management. J. Gastrointest. Oncol. 2021, 12 (Suppl. S2), S361–S373. [Google Scholar] [CrossRef]
- Liu, H.; Pan, Z.; Li, A.; Fu, S.; Lei, Y.; Sun, H.; Wu, M.; Zhou, W. Roles of Chemokine Receptor 4 (CXCR4) and Chemokine Ligand 12 (CXCL12) in Metastasis of Hepatocellular Carcinoma Cells. Cell. Mol. Immunol. 2008, 5, 373–378. [Google Scholar] [CrossRef]
- Werner, R.A.; Kircher, S.; Higuchi, T.; Kircher, M.; Schirbel, A.; Wester, H.J.; Buck, A.K.; Pomper, M.G.; Rowe, S.P.; Lapa, C. CXCR4-Directed Imaging in Solid Tumors. Front. Oncol. 2019, 9, 770. [Google Scholar] [CrossRef] [Green Version]
- Huang, S.; Wang, G.; Kou, M.; Huang, Y.; Yanhong, H.; Yunpeng, B.; Yingbang, L.; Huang, W. The Therapeutic and Prognostic Value of Chemokine Receptors (CXCRs) in Skin Cutaneous Melanoma (SKCM) Progression. 2021. Available online: https://assets.researchsquare.com/files/rs-618975/v1/5863050f-b9f2-4c8e-a64b-b8944e2e167c.pdf?c=1631884921 (accessed on 12 June 2022).
- Soltantoyeh, T.; Akbari, B.; Karimi, A.; Mahmoodi Chalbatani, G.; Ghahri-Saremi, N.; Hadjati, J.; Hamblin, M.R.; Mirzaei, H.R. Chimeric Antigen Receptor (CAR) T Cell Therapy for Metastatic Melanoma: Challenges and Road Ahead. Cells 2021, 10, 1450. [Google Scholar] [CrossRef]
- Dong, L.; You, S.; Zhang, Q.; Osuka, S.; Devi, N.S.; Kaluz, S.; Ferguson, J.H.; Yang, H.; Chen, G.; Wang, B. Arylsulfonamide 64B inhibits hypoxia/HIF-induced expression of c-Met and CXCR4 and reduces primary tumor growth and metastasis of uveal melanoma. Clin. Cancer Res. 2019, 25, 2206–2218. [Google Scholar] [CrossRef]
- Alimohammadi, M.; Rahimi, A.; Faramarzi, F.; Alizadeh-Navaei, R.; Rafiei, A. Overexpression of chemokine receptor CXCR4 predicts lymph node metastatic risk in patients with melanoma: A systematic review and meta-analysis. Cytokine 2021, 148, 155691. [Google Scholar] [CrossRef]
- Liu, J.; Ren, W.X.; Shu, J. Multimodal molecular imaging evaluation for early diagnosis and prognosis of cholangiocarcinoma. Insights Imaging 2022, 13, 10. [Google Scholar] [CrossRef]
- Saffioti, F.; Mavroeidis, V.K. Review of incidence and outcomes of treatment of cholangiocarcinoma in patients with primary sclerosing cholangitis. World J. Gastrointest. Oncol. 2021, 13, 1336–1366. [Google Scholar] [CrossRef] [PubMed]
- Sahu, R.; Sharma, P.; Kumar, A. An Insight into Cholangiocarcinoma and Recent Advances in its Treatment. J. Gastrointest. Cancer 2022, 13, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Leelawat, K.; Keeratichamroen, S.; Leelawat, S.; Tohtong, R. CD24 induces the invasion of cholangiocarcinoma cells by upregulating CXCR4 and increasing the phosphorylation of ERK1/2. Oncol. Lett. 2013, 6, 1439–1446. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Wang, J.; Qin, C. Blockade of CXCL12/CXCR4 signaling inhibits intrahepatic cholangiocarcinoma progression and metastasis via inactivation of canonical Wnt pathway. J. Exp. Clin. Cancer Res. 2014, 33, 103. [Google Scholar] [CrossRef]
- Tan, X.-Y.; Chang, S.; Liu, W.; Tang, H.-H. Silencing of CXCR4 inhibits tumor cell proliferation and neural invasion in human hilar cholangiocarcinoma. Gut Liver 2014, 8, 196–204. [Google Scholar] [CrossRef]
- Krieg, A.; Riemer, J.C.; Telan, L.A.; Gabbert, H.E.; Knoefel, W.T. CXCR4-A prognostic and clinicopathological biomarker for pancreatic ductal adenocarcinoma: A Meta-Analysis. PLoS ONE 2015, 10, e0130192. [Google Scholar] [CrossRef] [Green Version]
- Ding, Y.; Du, Y. Clinicopathological significance and prognostic role of chemokine receptor CXCR4 expression in pancreatic ductal adenocarcinoma, a meta-analysis and literature review. Int. J. Surg. 2019, 65, 32–38. [Google Scholar] [CrossRef]
- Capitanio, U.; Bensalah, K.; Bex, A.; Boorjian, S.A.; Bray, F.; Coleman, J.; Gore, J.L.; Sun, M.; Wood, C.; Russo, P. Epidemiology of renal cell carcinoma. Eur. Urol. 2019, 75, 74–84. [Google Scholar] [CrossRef]
- Heidegger, I.; Pircher, A.; Pichler, R. Targeting the tumor microenvironment in renal cell cancer biology and therapy. Front. Oncol. 2019, 9, 490. [Google Scholar] [CrossRef]
- Si, X.; Ma, J.; Yu, F.; Zhao, H.; Huang, H.; Sun, Y.-W. Clinicopathological and prognostic significance of CXCR4 high expression in renal cell carcinoma: A meta-analysis and literature review. Int. J. Surg. 2019, 71, 12–18. [Google Scholar] [CrossRef]
- Pan, J.; Mestas, J.; Burdick, M.D.; Phillips, R.J.; Thomas, G.V.; Reckamp, K.; Belperio, J.A.; Strieter, R.M. Stromal derived factor-1 (SDF-1/CXCL12) and CXCR4 in renal cell carcinoma metastasis. Mol. Cancer 2006, 5, 1–14. [Google Scholar] [CrossRef]
- Machlowska, J.; Baj, J.; Sitarz, M.; Maciejewski, R.; Sitarz, R. Gastric cancer: Epidemiology, risk factors, classification, genomic characteristics and treatment strategies. Int. J. Mol. Sci. 2020, 21, 4012. [Google Scholar] [CrossRef]
- Thrift, A.P.; El-Serag, H.B. Burden of gastric cancer. Clin. Gastroenterol. Hepatol. 2020, 18, 534–542. [Google Scholar] [CrossRef]
- Lee, H.J.; Kim, S.W.; Kim, H.Y.; Li, S.; Yun, H.J.; Song, K.S.; Kim, S.; Jo, D.Y. Chemokine receptor CXCR4 expression, function, and clinical implications in gastric cancer. Int. J. Oncol. 2009, 34, 473–480. [Google Scholar]
- Wen, F.; Lu, X.; Huang, W.; Chen, X.; Ruan, S.; Gu, S.; Gu, P.; Li, Y.; Liu, J.; Liu, S.; et al. Characteristics of immunophenotypes and immunological in tumor microenvironment and analysis of immune implication of CXCR4 in gastric cancer. Sci. Rep. 2022, 12, 5720. [Google Scholar] [CrossRef]
- Yasumoto, K.; Koizumi, K.; Kawashima, A.; Saitoh, Y.; Arita, Y.; Shinohara, K.; Minami, T.; Nakayama, T.; Sakurai, H.; Takahashi, Y. Role of the CXCL12/CXCR4 axis in peritoneal carcinomatosis of gastric cancer. Cancer Res. 2006, 66, 2181–2187. [Google Scholar] [CrossRef]
- Debnath, B.; Xu, S.; Grande, F.; Garofalo, A.; Neamati, N. Small molecule inhibitors of CXCR4. Theranostics 2013, 3, 47. [Google Scholar] [CrossRef] [Green Version]
- Song, J.-S.; Chang, C.-C.; Wu, C.-H.; Dinh, T.K.; Jan, J.-J.; Huang, K.-W.; Chou, M.-C.; Shiue, T.-Y.; Yeh, K.-C.; Ke, Y.-Y.; et al. A highly selective and potent CXCR4 antagonist for hepatocellular carcinoma treatment. Proc. Natl. Acad. Sci. USA 2021, 118, e2015433118. [Google Scholar] [CrossRef]
- Kircher, M.; Herhaus, P.; Schottelius, M.; Buck, A.K.; Werner, R.A.; Wester, H.J.; Keller, U.; Lapa, C. CXCR4-directed theranostics in oncology and inflammation. Ann. Nucl. Med. 2018, 32, 503–511. [Google Scholar] [CrossRef]
- Ling, X.; Spaeth, E.; Chen, Y.; Shi, Y.; Zhang, W.; Schober, W.; Hail, N., Jr.; Konopleva, M.; Andreeff, M. The CXCR4 antagonist AMD3465 regulates oncogenic signaling and invasiveness in vitro and prevents breast cancer growth and metastasis in vivo. PLoS ONE 2013, 8, e58426. [Google Scholar]
- Maurer, S.; Herhaus, P.; Lippenmeyer, R.; Hänscheid, H.; Kircher, M.; Schirbel, A.; Maurer, H.C.; Buck, A.K.; Wester, H.-J.; Einsele, H. Side effects of CXC-chemokine receptor 4–directed endoradiotherapy with pentixather before hematopoietic stem cell transplantation. J. Nucl. Med. 2019, 60, 1399–1405. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, K.; Schottelius, M.; Lapa, C.; Osl, T.; Poschenrieder, A.; Hanscheid, H.; Luckerath, K.; Schreder, M.; Bluemel, C.; Knott, M.; et al. First-in-Human Experience of CXCR4-Directed Endoradiotherapy with 177Lu- and 90Y-Labeled Pentixather in Advanced-Stage Multiple Myeloma with Extensive Intra- and Extramedullary Disease. J. Nucl. Med. 2016, 57, 248–251. [Google Scholar] [CrossRef] [PubMed]
- Lapa, C.; Hänscheid, H.; Kircher, M.; Schirbel, A.; Wunderlich, G.; Werner, R.A.; Samnick, S.; Kotzerke, J.; Einsele, H.; Buck, A.K. Feasibility of CXCR4-directed radioligand therapy in advanced diffuse large B-cell lymphoma. J. Nucl. Med. 2019, 60, 60–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
The CXCR4 overexpression in tumours increases angiogenesis, tumour migration and metastasis.
Figure 1.
The CXCR4 overexpression in tumours increases angiogenesis, tumour migration and metastasis.

Figure 2.
18F-FDG and 68Ga-Pentixafor images of a 60-year-old female with squamous cell carcinoma of the oral cavity with intense uptake in the primary lesion and left cervical lymph node metastasis on 18F-FDG (a). There was mild tracer accumulation on the 68Ga-Pentixafor PET (b). Interestingly, the inflammatory mediastinal lymph nodes appear more intense on the 68Ga-Pentixafor PET.
Figure 2.
18F-FDG and 68Ga-Pentixafor images of a 60-year-old female with squamous cell carcinoma of the oral cavity with intense uptake in the primary lesion and left cervical lymph node metastasis on 18F-FDG (a). There was mild tracer accumulation on the 68Ga-Pentixafor PET (b). Interestingly, the inflammatory mediastinal lymph nodes appear more intense on the 68Ga-Pentixafor PET.

Figure 3.
18F-FDG and 68Ga-Pentixafor images of a 36-year-old female patent with squamous cell carcinoma of the cervix with intense uptake in the primary lesion and pelvic lymph node metastasis on 18F-FDG (a). There is moderate heterogenous tracer accumulation on the 68Ga-Pentixafor PET and very low uptake on the metastatic lymph node (b).
Figure 3.
18F-FDG and 68Ga-Pentixafor images of a 36-year-old female patent with squamous cell carcinoma of the cervix with intense uptake in the primary lesion and pelvic lymph node metastasis on 18F-FDG (a). There is moderate heterogenous tracer accumulation on the 68Ga-Pentixafor PET and very low uptake on the metastatic lymph node (b).


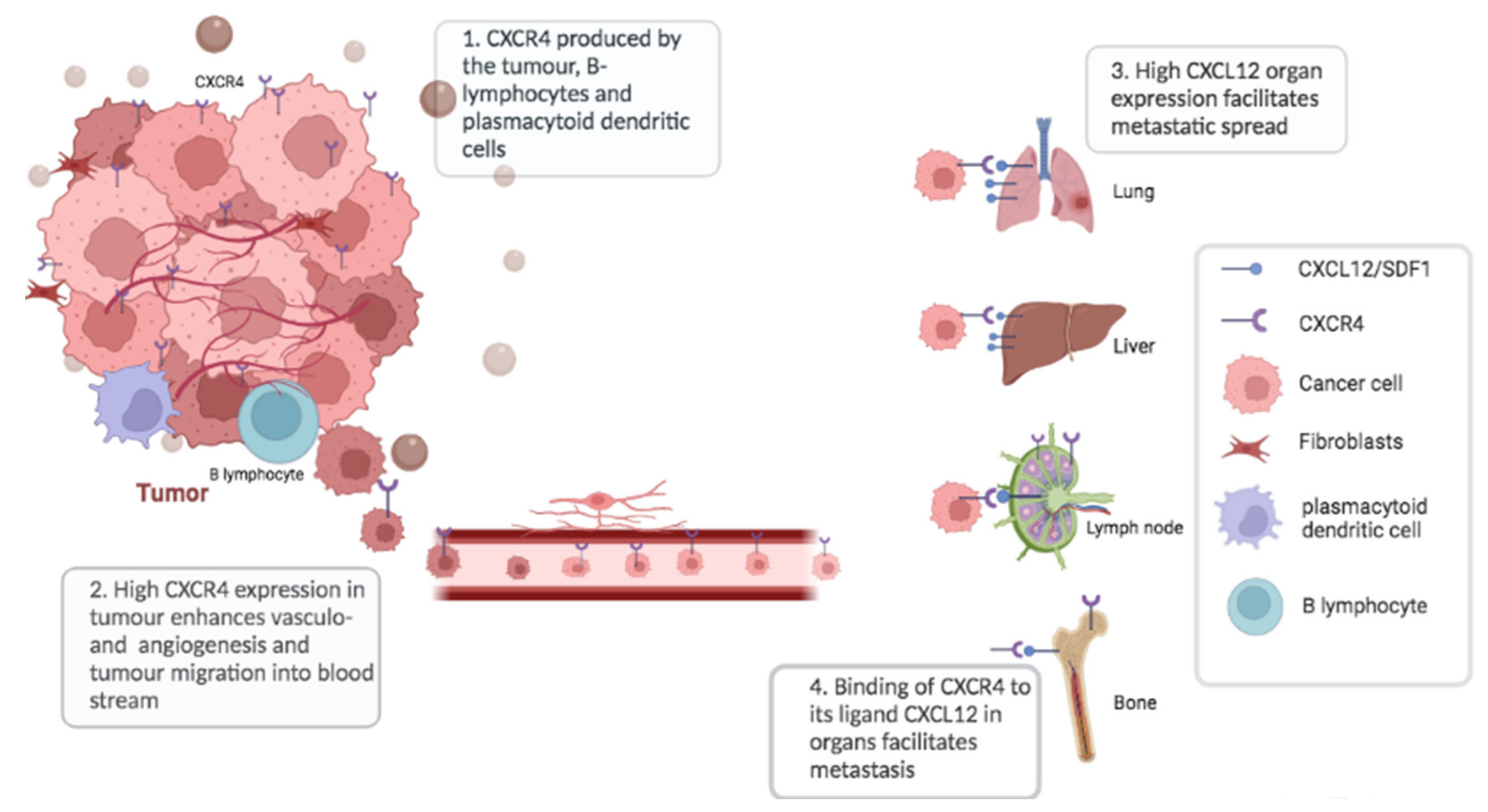{kind=link}
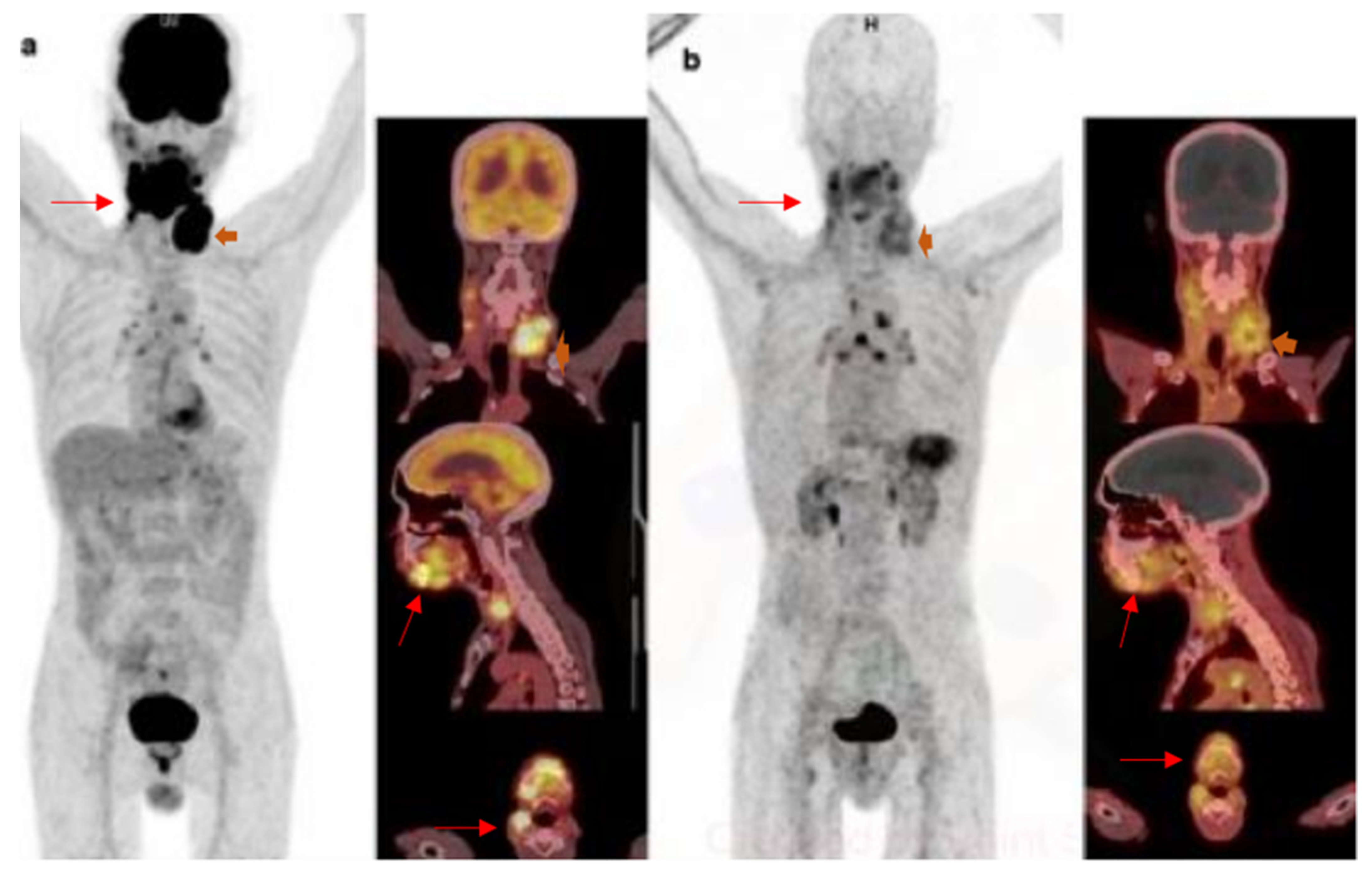{kind=link}
{kind=link}
Table 1.
Potential applications of CXCR4 in solid tumours.
| Tumour | CXCR4 Immunohistochemistry | Pentixafor | Pentixafor vs. FDG | Potential Application |
|---|---|---|---|---|
| HNSCC | + in high grade tumours [34] | 2 patients-low uptake [84] | No published data | Select potential candidates for anti-CXCR4 therapies |
| Glioblastoma | +++ in high grade tumours [37] | Low–moderate uptake [23] | Select potential candidates for anti-CXCR4 therapies | |
| Oesophageal cancer | ++ in 38–50% [41,43] | Most lesions + [45,46] | FDG > Pentixafor [46,47] (7/26 lesions Pentixafor +, FDG −) [46] | Select potential candidates for anti-CXCR4 therapies Monitor treatment response Alter treatment plan (upstaging) [45] |
| NET | Weak–moderate expression | 80% of Gr3 NET +, 50% Gr 2, Gr 1 neg [98] | Inferior to FDG and SSTR [47] | Role in higher grade tumours Prognosis Select potential candidates for anti-CXCR4 therapies |
| Lung cancer | + [50] | SCLCa higher than NSCLCa [51] Mesothelioma controversial [52,53] | More sensitive than FDG in 6/10 patients [49] | More sensitive than 68Ga DOTANOC Select potential candidates for anti-CXCR4 therapies Monitor treatment response |
| Osteosarcoma | + 68% of 36 tumours Worse prognosis [55,56] | No published data | No published data | Prognosis [54] Potentially select patients for CXCR4-targeted therapy Monitor treatment response |
| Vulva cancer | + correlates with poorer prognosis [59] | No published data | No published data | Differentiate tumour from premalignant lesion [59] Prognosis Select patients who may benefit from therapy |
| Cervix | + = poorer prognosis [62] | No data | No data | Prognosis |
| Ovarian | + primary = more advanced disease, poorer prognosis [63] | No data | No data | Prognosis |
| Breast | + but no correlation with molecular subtype, Ki67 or ER/PR [70,71,73] | 9/13 + [19] Recurrence metastasis 5/5 [27] 4/7 metastatic lesions | No data | Potentially select patients for therapy Monitor treatment response |
| Prostate cancer | + = poorer prognosis | ++ In tumour models [77] Bladder activity seen | No published data | Insufficient evidence |
| Vestibular schwannoma | +++ correlates with tumour invasiveness [80] | 6/6 sufficient uptake TBR matched w IHC [78] | No published data | Potentially to select patients for therapy Prognosis |
| Adrenocortical cancer | +++ 9/18 samples + Ki67, poorer prognosis [82] | + in 6 patients adrenocortical [86] | Pentixafor + in 2/9 FDG negative lesions [85] FDG superior to Pentixafor 9/22 | Prognosis Treatment response Select patients for Rx [83] |
| Colorectal | + in 76 samples = metastasis = aggressiveness [88,89] | Low to moderate 8 pts [90] | No published data | Potentially to select patients for therapy |
| Neuroblastoma | + = tumour aggressiveness [13,94] | No published data | No published data | Potentially to select patients for therapy Prognosis |
| HCC | + 65/78 patients [97] | Limited data + 2/5 pts [27,98] | No published data | Potential for selecting pts who may benefit from Rx |
| Melanoma | + = higher tumour stage Mets > primary [99,101,102] | Limited data + 4/4 metastasis [27] | FDG SUVmax slightly higher [27] | Select potential candidates for anti-CXCR4 therapies |
| Cholangiocarcinoma | 49% (122 pts) +++ = poorer prognosis [106,107] | 3 cases = high uptake [98] | No published data | Prognosis Select potential candidates for anti-CXCR4 therapies |
| Pancreatic cancer | + = poorer prognosis [109,110] | Low–moderate uptake 12 patients (TBR 2.92- >4) [84,98] | No published data | |
| Renal cell cancer | +++ with metastasis and poorer prognosis [113,114] | Low [98] | n/a | May be a marker of disease aggressiveness Select potential candidates for anti-CXCR4 therapies |
| Gastric cancer | + = poorer prognosis [87,117,118] | No published data | No published data | Potentially select patients who may benefit from Rx |
Key: − no uptake, + low uptake, ++ moderate, +++ high uptake, Rx: CXCR4-targeted therapies.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Hadebe, B.; Sathekge, M.M.; Aldous, C.; Vorster, M. Current Status of 68Ga-Pentixafor in Solid Tumours. Diagnostics 2022, 12, 2135. https://doi.org/10.3390/diagnostics12092135
AMA Style
Hadebe B, Sathekge MM, Aldous C, Vorster M. Current Status of 68Ga-Pentixafor in Solid Tumours. Diagnostics. 2022; 12(9):2135. https://doi.org/10.3390/diagnostics12092135
Chicago/Turabian StyleHadebe, Bawinile, Machaba Michael Sathekge, Colleen Aldous, and Mariza Vorster. 2022. "Current Status of 68Ga-Pentixafor in Solid Tumours" Diagnostics 12, no. 9: 2135. https://doi.org/10.3390/diagnostics12092135
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.