
Controversies in the Surgical Treatment of Chronic Subdural Hematoma: A Systematic Scoping Review

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
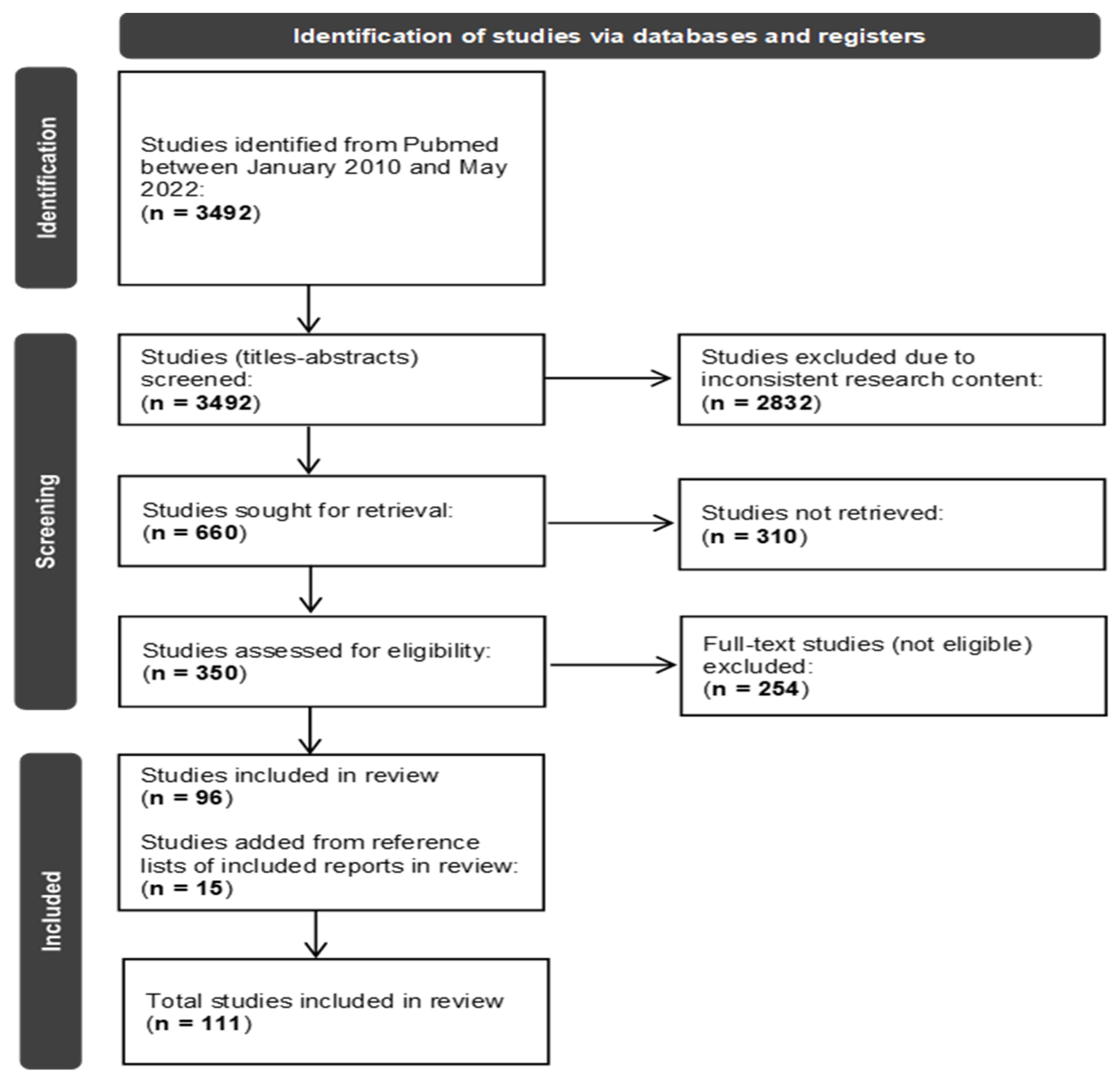
- Information Sources and Search Strategy:
- Eligibility Criteria:
- Selection and Data Collection Process:
- Data Items and Outcomes:
- Study Synthesis:
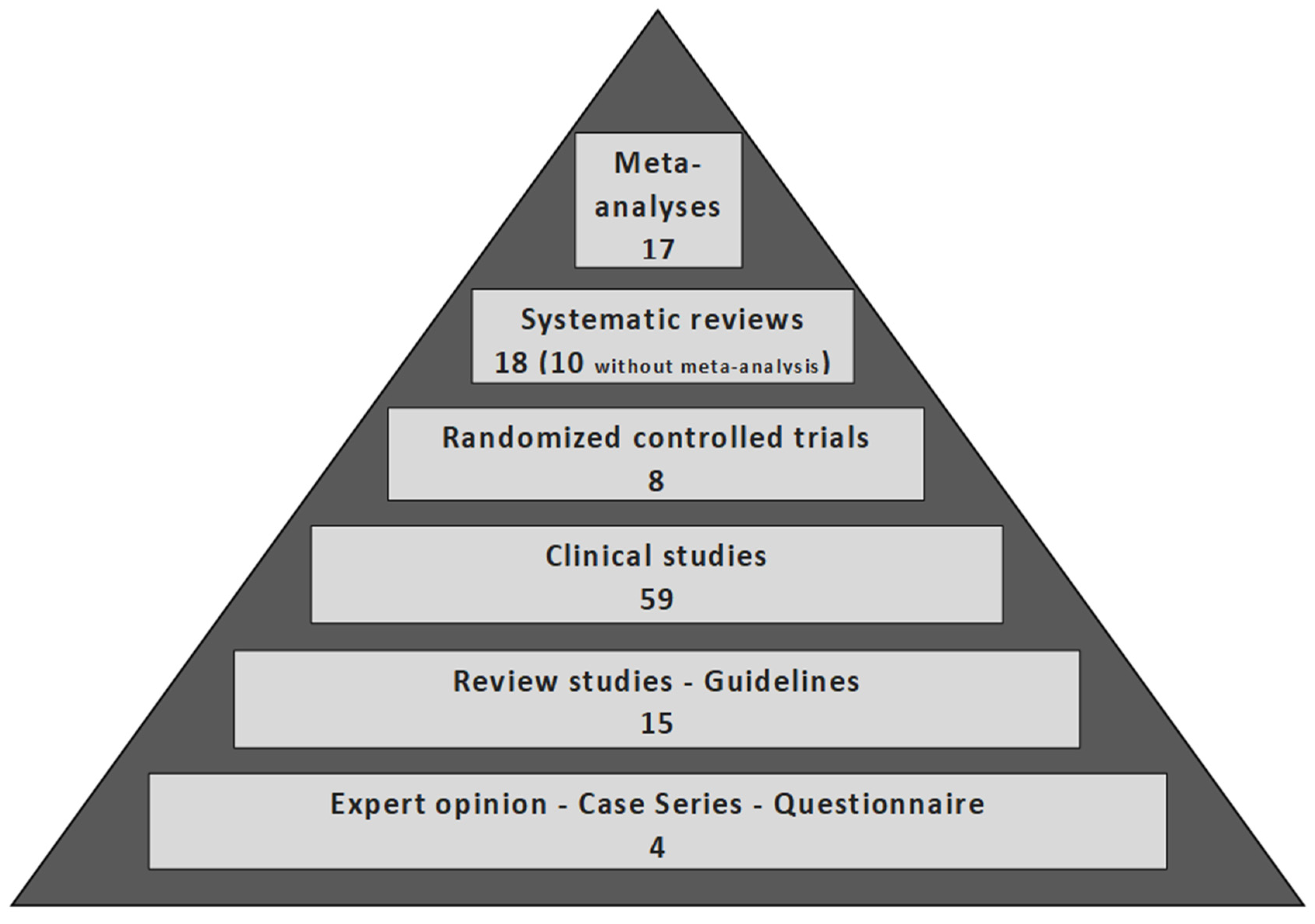
3. Results
3.1. Data of Included Studies
3.2. Result Analysis
4. Discussion
4.1. Indications of Surgery
4.2. Timing of Surgery
4.3. Surgical Method
4.3.1. Twist Drill Craniostomy (TDC)
4.3.2. Burr Hole Craniostomy (BHC)
4.3.3. Craniotomy
4.3.4. Endoscopic Procedures
4.4. Comparison of Surgical Techniques
4.4.1. TDC vs. BHC vs. Craniotomy
4.4.2. BHC vs. Craniotomy
4.4.3. TDC vs. BHC
4.4.4. Endoscope-Assisted BHC (EBHC) vs. BHC/Craniotomy
4.4.5. Refractory cSDH
4.5. Number of Burr Holes
4.6. Irrigation
4.7. Closed System Drainage
Drainage Location
4.8. Duration of Drainage
4.9. Membranectomy
4.10. Embolization of Middle Meningeal Artery (MMA)
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Tamura, R.; Sato, M.; Yoshida, K.; Toda, M. History and current progress of chronic subdural hematoma. J. Neurol. Sci. 2021, 429, 118066. [Google Scholar] [CrossRef] [PubMed]
- Yagnik, K.J.; Goyal, A.; van Gompel, J.J. Twist drill craniostomy vs burr hole drainage of chronic subdural hematoma: A systematic review and meta-analysis. Acta Neurochir. 2021, 163, 3229–3241. [Google Scholar] [CrossRef] [PubMed]
- Catapano, J.S.; Nguyen, C.L.; Wakim, A.A.; Albuquerque, F.C.; Ducruet, A.F. Middle Meningeal Artery Embolization for Chronic Subdural Hematoma. Front. Neurol. 2020, 11, 557233. [Google Scholar] [CrossRef]
- Hamou, H.A.; Clusmann, H.; Schulz, J.B.; Wiesmann, M.; Altiok, E.; Höllig, A. Chronic subdural hematoma—antithrombotics and thrombotic complications. Dtsch. Ärzteblatt Int. 2022, 119, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Miah, I.P.; Tank, Y.; Rosendaal, F.R.; Peul, W.C.; Dammers, R.; Lingsma, H.F.; Hertog, H.M.D.; Jellema, K.; van der Gaag, N.A.; on behalf of the Dutch Chronic Subdural Hematoma Research Group. Radiological prognostic factors of chronic subdural hematoma recurrence: A systematic review and meta-analysis. Neuroradiology 2020, 63, 27–40. [Google Scholar] [CrossRef]
- Takei, J.; Tanaka, T.; Yamamoto, Y.; Hatano, K.; Ichinose, D.; Maruyama, F.; Tochigi, S.; Hasegawa, Y.; Murayama, Y. Significantly high concentrations of vascular endothelial growth factor in chronic subdural hematoma with trabecular formation. Clin. Neurol. Neurosurg. 2021, 202, 106458. [Google Scholar] [CrossRef]
- Chihi, M.; Jabbarli, R.; Parlak, A.; Darkwah-Oppong, M.; Gembruch, O.; Wrede, K.; Sure, U.; Maslehaty, H. Predictors of Brain Natriuretic Peptide Serum Level Elevation in Patients with Symptomatic Chronic Subdural Hematoma: A Prospective Study. J. Clin. Med. 2021, 10, 1791. [Google Scholar] [CrossRef]
- Idowu, O.E.; Oyeleke, S.O.; Vitowanu, J.M. Impact of inflammatory cell ratio, biomarkers, activated partial thromboplastin time and prothrombin time on chronic subdural haematoma severity and outcome. Eur. J. Trauma Emerg. Surg. 2021, 48, 1085–1092. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n712021. [Google Scholar] [CrossRef]
- Weigel, R.; Schmiedek, P.; Krauss, J.K. Outcome of contemporary surgery for chronic subdural haematoma: Evidence based review. J. Neurol. Neurosurg. Psychiatry 2003, 74, 937–943. [Google Scholar] [CrossRef]
- Hallett, M.; Litvan, I. Evaluation of surgery for Parkinson’s disease: A Report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology 1999, 53, 1910. [Google Scholar] [CrossRef] [PubMed]
- Pripp, A.H.; Stanišić, M. Association between biomarkers and clinical characteristics in chronic subdural hematoma patients assessed with lasso regression. PLoS ONE 2017, 12, e0186838. [Google Scholar] [CrossRef] [PubMed]
- Sahyouni, R.; Goshtasbi, K.; Mahmoodi, A.; Tran, D.K.; Chen, J.W. Chronic Subdural Hematoma: A Historical and Clinical Perspective. World Neurosurg. 2017, 108, 948–953. [Google Scholar] [CrossRef] [PubMed]
- Shlobin, N.A.; Kedda, J.; Wishart, D.; Garcia, R.M.; Rosseau, G. Surgical Management of Chronic Subdural Hematoma in Older Adults: A Systematic Review. J. Gerontol. Ser. A 2020, 76, 1454–1462. [Google Scholar] [CrossRef] [PubMed]
- Soleman, J.; Taussky, P.; Fandino, J.; Muroi, C. Evidence-Based Treatment of Chronic Subdural Hematoma. Trauma Brain Inj. 2014. Available online: https://www.intechopen.com/chapters/46053 (accessed on 26 July 2022). [CrossRef]
- Soleman, J.; Noccera, F.; Mariani, L. The conservative and pharmacological management of chronic subdural haematoma. Swiss Med. Wkly. 2017, 147, w14398. [Google Scholar]
- Kolias, A.; Chari, A.; Santarius, T.; Hutchinson, P. Chronic subdural haematoma: Modern management and emerging therapies. Nat. Rev. Neurol. 2014, 10, 570–5782014. [Google Scholar] [CrossRef]
- Yadav, Y.; Parihar, V.; Namdev, H.; Bajaj, J. Chronic subdural hematoma. Asian J. Neurosurg. 2016, 11, 330–342. [Google Scholar] [CrossRef]
- Holl, D.C.; Volovici, V.; Dirven, C.M.; Peul, W.C.; van Kooten, F.; Jellema, K.; van der Gaag, N.A.; Miah, I.P.; Kho, K.H.; Hertog, H.M.D.; et al. Pathophysiology and Nonsurgical Treatment of Chronic Subdural Hematoma: From Past to Present to Future. World Neurosurg. 2018, 116, 402–411. [Google Scholar] [CrossRef]
- Nouri, A.; Gondar, R.; Schaller, K.; Meling, T. Chronic Subdural Hematoma (cSDH): A review of the current state of the art. Brain Spine 2021, 1, 100300. [Google Scholar] [CrossRef]
- Kobayashi, T.; Mochizuki, Y.; Kawashima, A.; Funatsu, T.; Kawamata, T. Chronic subdural hematoma of the posterior fossa treated by suboccipital craniotomy. Surg. Neurol. Int. 2018, 9, 20. [Google Scholar] [CrossRef] [PubMed]
- Takemoto, Y.; Matsumoto, J.; Ohta, K.; Hasegawa, S.; Miura, M.; Kuratsu, J.-I. Bilateral posterior fossa chronic subdural hematoma treated with craniectomy: Case report and review of the literature. Surg. Neurol. Int. 2016, 7, S255–S258. [Google Scholar] [CrossRef] [PubMed]
- Venturini, S.; Fountain, D.M.; Glancz, L.J.; Livermore, L.J.; Coulter, I.C.; Bond, S.; Matta, B.; Santarius, T.; Hutchinson, P.J.; Brennan, P.M.; et al. Time to surgery following chronic subdural hematoma: Post hoc analysis of a prospective cohort study. BMJ Surgery, Interv. Health Technol. 2019, 1, e0000122019. [Google Scholar] [CrossRef] [PubMed]
- Zolfaghari, S.; Ståhl, N.; Redebrandt, H.N. Does time from diagnostic CT until surgical evacuation affect outcome in patients with chronic subdural hematoma? Acta Neurochir. 2018, 160, 1703–1709. [Google Scholar] [CrossRef]
- Heidbuchel, H.; Verhamme, P.; Alings, M.; Antz, M.; Hacke, W.; Oldgren, J.; Sinnaeve, P.; Camm, A.J.; Kirchhof, P. European Heart Rhythm Association Practical Guide on the use of new oral anticoagulants in patients with non-valvular atrial fibrillation. Eur. 2013, 15, 625–651. [Google Scholar] [CrossRef]
- Almenawer, S.A.; Farrokhyar, F.; Hong, C.; Alhazzani, W.; Manoranjan, B.; Yarascavitch, B.; Arjmand, P.; Baronia, B.; Reddy, K.; Murty, N.; et al. Chronic Subdural Hematoma Management. Ann. Surg. 2014, 259, 449–457. [Google Scholar] [CrossRef]
- Ogasawara, K.; Koshu, K.; Yoshimoto, T.; Ogawa, A. Transient Hyperemia Immediately after Rapid Decompression of Chronic Subdural Hematoma. Neurosurgery 1999, 45, 484–489. [Google Scholar] [CrossRef]
- Sastry, R.A.; Pertsch, N.; Tang, O.; Shao, B.; Toms, S.A.; Weil, R.J. Frailty and Outcomes after Craniotomy or Craniectomy for Atraumatic Chronic Subdural Hematoma. World Neurosurg. 2020, 145, e242–e251. [Google Scholar] [CrossRef]
- Lega, B.C.; Danish, S.F.; Malhotra, N.R.; Sonnad, S.S.; Stein, S.C. Choosing the best operation for chronic subdural hematoma: A decision analysis. J. Neurosurg. 2010, 113, 615–621. [Google Scholar] [CrossRef]
- Van der Veken, J.; Duerinck, J.; Buyl, R.; van Rompaey, K.; Herregodts, P.; D’Haens, J. Mini-craniotomy as the primary surgical intervention for the treatment of chronic subdural hematoma—A retrospective analysis. Acta Neurochir. 2014, 156, 981–987. [Google Scholar] [CrossRef]
- Yadav, Y.R.; Ratre, S.; Parihar, V.; Bajaj, J.; Sinha, M.; Kumar, A. Endoscopic Management of Chronic Subdural Hematoma. J. Neurol. Surg. Part A Central Eur. Neurosurg. 2020, 81, 330–341. [Google Scholar] [CrossRef]
- Cofano, F.; Pesce, A.; Vercelli, G.; Mammi, M.; Massara, A.; Minardi, M.; Palmieri, M.; D’Andrea, G.; Fronda, C.; Lanotte, M.M.; et al. Risk of Recurrence of Chronic Subdural Hematomas After Surgery: A Multicenter Observational Cohort Study. Front. Neurol. 2020, 11, 560269. [Google Scholar] [CrossRef] [PubMed]
- Duerinck, J.; van der Veken, J.; Schuind, S.; van Calenbergh, F.; van Loon, J.; Du Four, S.; Debacker, S.; Costa, E.; Raftopoulos, C.; de Witte, O.; et al. Randomized Trial Comparing Burr Hole Craniostomy, Minicraniotomy, and Twist Drill Craniostomy for Treatment of Chronic Subdural Hematoma. Neurosurgery 2022, 91, 304–311. [Google Scholar] [CrossRef]
- Ducruet, A.F.; Grobelny, B.T.; Zacharia, B.; Hickman, Z.; DeRosa, P.L.; Anderson, K.; Sussman, E.; Carpenter, A.; Connolly, E.S. The surgical management of chronic subdural hematoma. Neurosurg. Rev. 2011, 35, 155–169. [Google Scholar] [CrossRef] [PubMed]
- Shim, Y.W.; Lee, W.H.; Lee, K.S.; Kim, S.T.; Paeng, S.H.; Pyo, S.Y. Burr Hole Drainage versus Small Craniotomy of Chronic Subdural Hematomas. Korean J. Neurotrauma 2019, 15, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Raghavan, A.; Smith, G.; Onyewadume, L.; Peck, M.R.; Herring, E.; Pace, J.; Rogers, M.; Momotaz, H.; Hoffer, S.A.; Hu, Y.; et al. Morbidity and Mortality After Burr Hole Craniostomy Versus Craniotomy for Chronic Subdural Hematoma Evacuation: A Single-Center Experience. World Neurosurg. 2019, 134, e196–e203. [Google Scholar] [CrossRef]
- Gazzeri, R.; Laszlo, A.; Faiola, A.; Colangeli, M.; Comberiati, A.; Bolognini, A.; Callovini, G. Clinical investigation of chronic subdural hematoma: Relationship between surgical approach, drainage location, use of antithrombotic drugs and postoperative recurrence. Clin. Neurol. Neurosurg. 2020, 191, 105705. [Google Scholar] [CrossRef]
- Xu, C.; Chen, B.; Xue, L.; Xia, L.; Yang, X.; Wei, M.; Hui, X.; Chen, Q.; Zheng, J.; Li, Z.; et al. Randomized controlled study on the curative effects of twist-drill craniotomy and burr-hole craniotomy in the treatment of chronic subdural hematoma. Exp. Ther. Med. 2018, 16, 959–965. [Google Scholar] [CrossRef]
- Zhang, J.; Liu, X.; Fan, X.; Fu, K.; Xu, C.; Hu, Q.; Jiang, P.; Chen, J.; Wang, W. The use of endoscopic-assisted burr-hole craniostomy for septated chronic subdural haematoma: A retrospective cohort comparison study. Brain Res. 2018, 1678, 245–253. [Google Scholar] [CrossRef]
- Guo, S.; Gao, W.; Cheng, W.; Liang, C.; Wu, A. Endoscope-Assisted Surgery vs. Burr-Hole Craniostomy for the Treatment of Chronic Subdural Hematoma: A Systemic Review and Meta-Analysis. Front. Neurol. 2020, 11, 540911. [Google Scholar] [CrossRef]
- Amano, T.; Miyamatsu, Y.; Otsuji, R.; Nakamizo, A. Efficacy of endoscopic treatment for chronic subdural hematoma surgery. J. Clin. Neurosci. 2021, 92, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Chen, J. The therapeutic effects of craniotomy versus endoscopic-assisted trepanation drainage for isolated chronic subdural haematoma (ICSH): A single-centre long-term retrospective comparison study. Brain Res. Bull. 2020, 161, 94–97. [Google Scholar] [CrossRef] [PubMed]
- Yan, K.; Gao, H.; Zhou, X.; Wu, W.; Xu, W.; Xu, Y.; Gong, K.; Xue, X.; Wang, Q.; Na, H. A retrospective analysis of postoperative recurrence of septated chronic subdural haematoma: Endoscopic surgery versus burr hole craniotomy. Neurol. Res. 2017, 39, 803–812. [Google Scholar] [CrossRef]
- Knopman, J.; Link, T.W.; Navi, B.B.; Murthy, S.B.; Merkler, A.E.; Kamel, H. Rates of Repeated Operation for Isolated Subdural Hematoma Among Older Adults. JAMA Netw. Open 2018, 1, e183737. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, H.; Hanayama, H.; Okada, T.; Sakurai, Y.; Minami, H.; Masuda, A.; Tominaga, S.; Miyaji, K.; Yamaura, I.; Yoshida, Y. Which surgical procedure is effective for refractory chronic subdural hematoma? Analysis of our surgical procedures and literature review. J. Clin. Neurosci. 2018, 49, 40–47. [Google Scholar] [CrossRef]
- Mersha, A.; Abat, S.; Temesgen, T.; Nebyou, A. Outcome of Chronic Subdural Hematoma Treated with Single Burr Hole Under Local Anesthesia. Ethiop. J. Health Sci. 2020, 30, 101–106. [Google Scholar] [CrossRef]
- Khursheed, N.; Ramzan, A.; Shoaib, Y.; Laharwal, M.; Wani, A.; Zahoor, A. Chronic subdural hematomas: Single or double burr hole–results of a randomized study. Turk. Neurosurg. 2013, 24, 246–820. [Google Scholar] [CrossRef]
- Kansal, R.; Nadkarni, T.; Goel, A. Single versus double burr hole drainage of chronic subdural hematomas. A study of 267 cases. J. Clin. Neurosci. 2010, 17, 428–429. [Google Scholar] [CrossRef]
- Heringer, L.C.; Sousa, U.D.O.; Nunes, A.S.; Alves, K.D.A.; Zancanaro, M.L.; Botelho, R.V.; de Oliveira, M.F. The number of burr holes and use of a drain do not interfere with surgical results of chronic subdural hematomas. Arq. Neuro-Psiquiatr. 2017, 75, 809–812. [Google Scholar] [CrossRef]
- Nalin, S.; Sahu, A.; Gupta, K.; Singh, K. Single versus double burr holes evacuation in the treatment of chronic subdural hematoma. Rom. Neurosurg. 2021, 35, 180–188. [Google Scholar] [CrossRef]
- Belkhair, S.; Pickett, G. One Versus Double Burr Holes for Treating Chronic Subdural Hematoma Meta-Analysis. Can. J. Neurol. Sci./J. Can. Des Sci. Neurol. 2013, 40, 56–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, M.D.; Kishikova, L.; Norris, J.M. Surgical management of chronic subdural haematoma: One hole or two? Int. J. Surg. 2012, 10, 450–452. [Google Scholar] [CrossRef] [PubMed]
- Wan, Y.; Xie, D.; Xue, Z.; Xie, J.; Song, Z.; Wang, Y.; Yang, S. Single Versus Double Burr Hole Craniostomy in Surgical Treatment of Chronic Subdural Hematoma: A Meta-Analysis. World Neurosurg. 2019, 131, e149–e154. [Google Scholar] [CrossRef] [PubMed]
- Han, H.-J.; Park, C.-W.; Kim, E.-Y.; Yoo, C.-J.; Kim, Y.-B.; Kim, W.-K. One vs. Two Burr Hole Craniostomy in Surgical Treatment of Chronic Subdural Hematoma. J. Korean Neurosurg. Soc. 2009, 46, 87–92. [Google Scholar] [CrossRef]
- Khan, U.K.S.; Sarker, A.C.; Morshed, M.H.; Hasan, M.; Hoque, S.; Hawlader, R.A.; Islam, R. Single versus Double Burr Holes for Treating Chronic Subdural Hematoma. Bangladesh J. Neurosurg. 2020, 9, 99–104. [Google Scholar] [CrossRef]
- Taussky, P.; Fandino, J.; Landolt, H. Number of burr holes as independent predictor of postoperative recurrence in chronic subdural haematoma. Br. J. Neurosurg. 2008, 22, 279–282. [Google Scholar] [CrossRef]
- Suzuki, K.; Sugita, K.; Akai, T.; Takahata, T.; Sonobe, M.; Takahashi, S. Treatment of chronic subdural hematoma by closed-system drainage without irrigation. Surg. Neurol. 1998, 50, 231–234. [Google Scholar] [CrossRef]
- Zakaraia, A.M.; Adnan, J.S.; Haspani, M.S.M.; Naing, N.N.; Abdullah, J.M. Outcome of 2 different types of operative techniques practiced for chronic subdural hematoma in Malaysia: An analysis. Surg. Neurol. 2008, 69, 608–615. [Google Scholar] [CrossRef]
- Xu, C.; Chen, S.; Yuan, L.; Jing, Y. Burr-hole Irrigation with Closed-system Drainage for the Treatment of Chronic Subdural Hematoma: A Meta-analysis. Neurol. Med.-Chir. 2016, 56, 62–68. [Google Scholar] [CrossRef]
- Bartley, A.; Jakola, A.S.; Tisell, M. The influence of irrigation fluid temperature on recurrence in the evacuation of chronic subdural hematoma. Acta Neurochir. 2019, 162, 485–488. [Google Scholar] [CrossRef]
- Kuwabara, M.; Sadatomo, T.; Yuki, K.; Migita, K.; Imada, Y.; Shimizu, K.; Hara, T.; Oba, H.; Kurisu, K. The Effect of Irrigation Solutions on Recurrence of Chronic Subdural Hematoma: A Consecutive Cohort Study of 234 Patients. Neurol. Med.-Chir. 2017, 57, 210–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, S.; Chen, Z.; Yang, B.; Xu, T.; Tu, X.-K. Use of siphon irrigation during burr-hole craniostomy to evacuate chronic subdural hematoma. Medicine 2020, 99, e20291. [Google Scholar] [CrossRef] [PubMed]
- Santarius, T.; Kirkpatrick, P.J.; Ganesan, D.; Chia, H.L.; Jalloh, I.; Smielewski, P.; Richards, H.K.; Marcus, H.; Parker, R.A.; Price, S.J.; et al. Use of drains versus no drains after burr-hole evacuation of chronic subdural haematoma: A randomised controlled trial. Lancet 2009, 374, 1067–1073. [Google Scholar] [CrossRef]
- Peng, D.; Zhu, Y. External drains versus no drains after burr-hole evacuation for the treatment of chronic subdural haematoma in adults. Cochrane Database Syst. Rev. 2016, 2016, CD011402. [Google Scholar] [CrossRef] [PubMed]
- Alcalá-Cerra, G.; Young, A.M.; Moscote-Salazar, L.R.; Paternina-Caicedo, A. Efficacy and Safety of Subdural Drains After Burr-Hole Evacuation of Chronic Subdural Hematomas: Systematic Review and Meta-Analysis of Randomized Controlled Trials. World Neurosurg. 2014, 82, 1148–1157. [Google Scholar] [CrossRef]
- Gurelik, M.; Aslan, A.; Gurelik, B.; Ozum, U.; Karadag, O.; Kars, H.Z. A safe and effective method for treatment of chronic subdural haematoma. Can. J. Neurol. Sci. J. Can. Des Sci. Neurol. 2007, 34, 84–87. [Google Scholar] [CrossRef]
- Sarnvivad, P.; Chiewchanvechakul, W.; Chumnanvej, S. Chronic subdural hematoma: Drainage vs. no drainage. J. Med. Assoc. Thail. 2011, 94, 1352. [Google Scholar]
- Yadav, Y.R.; Parihar, V.; Chourasia, I.D.; Bajaj, J.; Namdev, H. The role of subgaleal suction drain placement in chronic subdural hematoma evacuation. Asian J. Neurosurg. 2016, 11, 214–218. [Google Scholar] [CrossRef]
- Bellut, D.; Woernle, C.M.; Burkhardt, J.-K.; Kockro, R.A.; Bertalanffy, H.; Krayenbühl, N. Subdural Drainage versus Subperiosteal Drainage in Burr-Hole Trepanation for Symptomatic Chronic Subdural Hematomas. World Neurosurg. 2012, 77, 111–118. [Google Scholar] [CrossRef]
- Greuter, L.; Lutz, K.; Fandino, J.; Mariani, L.; Guzman, R.; Soleman, J. Drain type after burr-hole drainage of chronic subdural hematoma in geriatric patients: A subanalysis of the cSDH-Drain randomized controlled trial. Neurosurg. Focus 2020, 49, E6. [Google Scholar] [CrossRef]
- Oral, S.; Borklu, R.E.; Kucuk, A.; Ulutabanca, H.; Selcuklu, A. Comparison of Subgaleal and Subdural Closed Drainage System in Surgical Treatment of Chronic Subdural Hematoma. N. Clin. Istanb. 2015, 2, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Pranata, R.; Deka, H.; July, J. Subperiosteal versus subdural drainage after burr hole evacuation of chronic subdural hematoma: Systematic review and meta-analysis. Acta Neurochir. 2020, 162, 489–498. [Google Scholar] [CrossRef] [PubMed]
- Hwang, Y.; Choi, S.; Kim, Y.S.; Park, J.-S.; Choi, J.H.; Jeun, S.-S.; Ahn, S. Comparative analysis of safety and efficacy in subperiosteal versus subdural drainage after burr-hole trephination for chronic subdural hematoma. Clin. Neurol. Neurosurg. 2021, 212, 107068. [Google Scholar] [CrossRef]
- Pathoumthong, K.; Jetjumnong, C. Comparative study of subdural drain (SDD) versus sub periosteal drain (SPD) in treating patient with chronic subdural hematoma (CSDH). Surg. Neurol. Int. 2021, 12, 421. [Google Scholar] [CrossRef]
- Soleman, J.; Lutz, K.; Schaedelin, S.; Kamenova, M.; Guzman, R.; Mariani, L.; Fandino, J. Subperiosteal vs Subdural Drain After Burr-Hole Drainage of Chronic Subdural Hematoma: A Randomized Clinical Trial (cSDH-Drain-Trial). Neurosurgery 2019, 85, E825–E834. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.J.; Wang, S.; Foo, A.S.C.; Yang, M.; Quah, B.L.; Sun, I.S.; Ng, Z.X.; Teo, K.; Pang, B.C.; Yang, E.W.; et al. Outcomes of Subdural Versus Subperiosteal Drain After Burr-Hole Evacuation of Chronic Subdural Hematoma: A Multicenter Cohort Study. World Neurosurg. 2019, 131, e392–e401. [Google Scholar] [CrossRef]
- Jensen, T.S.R.; Haldrup, M.; Grønhøj, M.H.; Miscov, R.; Larsen, C.C.; Debrabant, B.; Poulsen, F.R.; Bergholt, B.; Hundsholt, T.; Bjarkam, C.R.; et al. National randomized clinical trial on subdural drainage time after chronic subdural hematoma evacuation. J. Neurosurg. 2021, 1, 1–8. [Google Scholar] [CrossRef]
- Glancz, L.J.; Poon, M.T.C.; Coulter, I.C.; Hutchinson, P.J.; Kolias, A.G.; Brennan, P.M. Does Drain Position and Duration Influence Outcomes in Patients Undergoing Burr-Hole Evacuation of Chronic Subdural Hematoma? Lessons from a UK Multicenter Prospective Cohort Study. Neurosurgery 2018, 85, 486–493. [Google Scholar] [CrossRef]
- Kale, A.; Öz, I.I.; Gün, E.G.; Kalaycı, M.; Gül, Ş. Is the recurrence rate of chronic subdural hematomas dependent on the duration of drainage? Neurol. Res. 2017, 39, 399–402. [Google Scholar] [CrossRef]
- Kim, J.-H.; Kang, D.-S.; Kim, J.-H.; Kong, M.-H.; Song, K.-Y. Chronic Subdural Hematoma Treated by Small or Large Craniotomy with Membranectomy as the Initial Treatment. J. Korean Neurosurg. Soc. 2011, 50, 103–108. [Google Scholar] [CrossRef]
- Elayouty, A.E.D.; Abdelfatah, M.A. Inner membrane opening during the burr-hole evacuation of a chronic subdural hematoma: Risk-adding or recurrence-preventing? Egypt. J. Neurosurg. 2018, 33, 4. [Google Scholar] [CrossRef]
- Sahyouni, R.; Mahboubi, H.; Tran, P.; Roufail, J.S.; Chen, J.W. Membranectomy in Chronic Subdural Hematoma: Meta-Analysis. World Neurosurg. 2017, 104, 418–429. [Google Scholar] [CrossRef] [PubMed]
- Unterhofer, C.; Freyschlag, C.F.; Thomé, C.; Ortler, M. Opening the Internal Hematoma Membrane Does Not Alter the Recurrence Rate of Chronic Subdural Hematomas: A Prospective Randomized Trial. World Neurosurg. 2016, 92, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-Y.; Ebel, H.; Ernestus, R.-I.; Klug, N. Various surgical treatments of chronic subdural hematoma and outcome in 172 patients: Is membranectomy necessary? Surg. Neurol. 2004, 61, 523–527. [Google Scholar] [CrossRef]
- Takizawa, K.; Sorimachi, T.; Ishizaka, H.; Osada, T.; Srivatanakul, K.; Momose, H.; Matsumae, M. Enlargement of the middle meningeal artery on MR angiography in chronic subdural hematoma. J. Neurosurg. 2016, 124, 1679–1683. [Google Scholar] [CrossRef]
- Adusumilli, G.; Ghozy, S.; Kallmes, K.M.; Hardy, N.; Tarchand, R.; Zinn, C.; Lamar, D.; Singeltary, E.; Siegel, L.; Kallmes, D.F.; et al. Common data elements reported on middle meningeal artery embolization in chronic subdural hematoma: An interactive systematic review of recent trials. J. NeuroInterventional Surg. 2022. [Google Scholar] [CrossRef]
- Ironside, N.; Nguyen, C.; Do, Q.; Ugiliweneza, B.; Chen, C.-J.; Sieg, E.P.; James, R.F.; Ding, D. Middle meningeal artery embolization for chronic subdural hematoma: A systematic review and meta-analysis. J. NeuroInterventional Surg. 2021, 13, 951–957. [Google Scholar] [CrossRef]
- Srivatsan, A.; Mohanty, A.; Nascimento, F.A.; Hafeez, M.U.; Srinivasan, V.M.; Thomas, A.; Chen, S.R.; Johnson, J.N.; Kan, P. Middle Meningeal Artery Embolization for Chronic Subdural Hematoma: Meta-Analysis and Systematic Review. World Neurosurg. 2018, 122, 613–619. [Google Scholar] [CrossRef]
- Mehta, V.; Harward, S.C.; Sankey, E.W.; Nayar, G.; Codd, P.J. Evidence based diagnosis and management of chronic subdural hematoma: A review of the literature. J. Clin. Neurosci. 2018, 50, 7–15. [Google Scholar] [CrossRef]
- Feghali, J.; Yang, W.; Huang, J. Updates in Chronic Subdural Hematoma: Epidemiology, Etiology, Pathogenesis, Treatment, and Outcome. World Neurosurg. 2020, 141, 339–345. [Google Scholar] [CrossRef]
- Ivamoto, H.S.; Lemos, H.P.; Atallah, A.N. Surgical Treatments for Chronic Subdural Hematomas: A Comprehensive Systematic Review. World Neurosurg. 2015, 86, 399–418. [Google Scholar] [CrossRef] [PubMed]
- Roh, D.; Reznik, M.; Claassen, J. Chronic Subdural Medical Management. Neurosurg. Clin. N. Am. 2017, 28, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Baschera, D.; Tosic, L.; Westermann, L.; Oberle, J.; Alfieri, A. Treatment Standards for Chronic Subdural Hematoma: Results from a Survey in Austrian, German, and Swiss Neurosurgical Units. World Neurosurg. 2018, 116, e983–e995. [Google Scholar] [CrossRef] [PubMed]
- Inoue, T.; Hirai, H.; Shima, A.; Suzuki, F.; Matsuda, M. Bilateral Chronic Subdural Hematoma in the Posterior Fossa Treated with a Burr Hole Irrigation: A Case Report and Review of the Literature. Case Rep. Neurol. 2019, 11, 87–93. [Google Scholar] [CrossRef]
- Kurisu, K.; Kawabori, M.; Niiya, Y.; Ohta, Y.; Mabuchi, S.; Houkin, K. Bilateral Chronic Subdural Hematomas of the Posterior Fossae. Neurol. Med.-Chir. 2012, 52, 822–825. [Google Scholar] [CrossRef]
- Mondorf, Y.; Abu-Owaimer, M.; Gaab, M.R.; Oertel, J.M. Chronic subdural hematoma—Craniotomy versus burr hole trepanation. Br. J. Neurosurg. 2009, 23, 612–616. [Google Scholar] [CrossRef]
- Abdelfatah, M.R. Recurrence rate of chronic subdural hematoma after evacuating it by two large burr holes, irrigation, and subgaleal low-pressure suction drainage. Asian J. Neurosurg. 2019, 14, 725–729. [Google Scholar] [CrossRef]
- Sale, D. Single versus Double Burr Hole for Drainage of Chronic Subdural Hematoma: Randomized Controlled Study. World Neurosurg. 2020, 146, e565–e567. [Google Scholar] [CrossRef]
- Opšenák, R.; Fejerčák, T.; Hanko, M.; Snopko, P.; Varga, P.; Richterová, R.; Kolarovszki, B. Is there an impact of subdural drainage duration and the number of burr holes on the recurrence rate of unilateral chronic subdural haematoma? Perspect. Surg. 2020, 99. [Google Scholar] [CrossRef]
- Ishibashi, A.; Yokokura, Y.; Adachi, H. A Comparative Study of Treatments for Chronic Subdural Hematoma: Burr Hole Drainage versus Burr Hole Drainage with Irrigation. Kurume Med. J. 2011, 58, 35–39. [Google Scholar] [CrossRef]
- Ram, Z.; Hadani, M.; Sahar, A.; Spiegelmann, R. Continuous irrigation-drainage of the subdural space for the treatment of chronic subdural haematoma. A prospective clinical trial. Acta Neurochir. 1993, 120, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Hennig, R.; Kloster, R. Burr Hole Evacuation of Chronic Subdural Haematomas Followed by Continuous Inflow and Outflow Irrigation. Acta Neurochir. 1999, 141, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Aoki, N. Subdural Tapping and Irrigation for the Treatment of Chronic Subdural Hematoma in Adults. Neurosurgery 1984, 14, 545–548. [Google Scholar] [CrossRef]
- Iftikhar, M.; Rauf, M.Y.; Malik, A.O.; Javed, G.; Siddiqui, U.T. Comparison of Irrigation versus No Irrigation during Burr Hole Evacuation of Chronic Subdural Hematoma. J. Neurol. Surg. Part A Central Eur. Neurosurg. 2016, 77, 416–421. [Google Scholar] [CrossRef]
- Matsumoto, K.; Akagi, K.; Abekura, M.; Ryujin, H.; Ohkawa, M.; Iwasa, N.; Akiyama, C. Recurrence factors for chronic subdural hematomas after burr-hole craniostomy and closed system drainage. Neurol. Res. 1999, 21, 277–280. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.; Wang, Q.-P.; Cao, Y.-L.; Zhang, H.; Burkutally, M.S.N.; Budryte, K.; Xiong, N. Burr hole drainage and burr hole drainage with irrigation to treat chronic subdural hematoma. Medicine 2018, 97, e11827. [Google Scholar] [CrossRef]
- Uda, H.; Nagm, A.; Ichinose, T.; Onishi, Y.; Yoshimura, M.; Tsuruno, T.; Ohata, K. Burr hole drainage without irrigation for chronic subdural hematoma. Surg. Neurol. Int. 2020, 11, 89. [Google Scholar] [CrossRef]
- Wang, Q.-P.; Yuan, Y.; Guan, J.-W.; Jiang, X.-B. A comparative study of irrigation versus no irrigation during burr hole craniostomy to treat chronic subdural hematoma. BMC Surg. 2017, 17, 99. [Google Scholar] [CrossRef]
- Pan, Z.; Bao, J.; Wei, S. Efficacy of the Direct Aspiration-Irrigation Maneuver for the Treatment of Chronic Subdural Hematoma: A Single Hospital’s Experience. Cureus 2021, 13, e16231. [Google Scholar] [CrossRef]
- Ramachandran, R.; Hegde, T. Chronic subdural hematomas—Causes of morbidity and mortality. Surg. Neurol. 2007, 67, 367–372. [Google Scholar] [CrossRef]
- Chih, A.N.W.; Hieng, A.W.S.; Rahman, N.A.A.; Abdullah, J.M. Subperiosteal Drainage versus Subdural Drainage in the management of Chronic Subdural Hematoma (A Comparative Study). Malays. J. Med. Sci. 2017, 24, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Lu, Q.; Lenahan, C.; Yang, S.; Zhou, D.; Qi, X. A Comparison of Subperiosteal or Subgaleal Drainage with Subdural Drainage on the Outcomes of Chronic Subdural Hematoma: A Meta-Analysis. World Neurosurg. 2019, 135, e723–e730. [Google Scholar] [CrossRef] [PubMed]
- Ding, H.; Liu, S.; Quan, X.; Liao, S.; Liu, L. Subperiosteal versus Subdural Drain After Burr Hole Drainage for Chronic Subdural Hematomas: A Systematic Review and Meta-Analysis. World Neurosurg. 2020, 136, 90–100. [Google Scholar] [CrossRef]
- Haldrup, M.; Ketharanathan, B.; Debrabant, B.; Schwartz, O.S.; Mikkelsen, R.; Fugleholm, K.; Poulsen, F.R.; Jensen, T.S.R.; Thaarup, L.V.; Bergholt, B. Embolization of the middle meningeal artery in patients with chronic subdural hematoma—a systematic review and meta-analysis. Acta Neurochir. 2020, 162, 777–784. [Google Scholar] [CrossRef]
- Ng, S.; Derraz, I.; Boetto, J.; Dargazanli, C.; Poulen, G.; Gascou, G.; Lefevre, P.-H.; Molinari, N.; Lonjon, N.; Costalat, V. Middle meningeal artery embolization as an adjuvant treatment to surgery for symptomatic chronic subdural hematoma: A pilot study assessing hematoma volume resorption. J. NeuroInterventional Surg. 2019, 12, 695–699. [Google Scholar] [CrossRef]
- Di Cristofori, A.; Remida, P.; Patassini, M.; Piergallini, L.; Buonanno, R.; Bruno, R.; Carrabba, G.; Pavesi, G.; Iaccarino, C.; Giussani, C.G. Middle meningeal artery embolization for chronic subdural hematomas. A systematic review of the literature focused on indications, technical aspects, and future possible perspectives. Surg. Neurol. Int. 2022, 13, 94. [Google Scholar] [CrossRef] [PubMed]
- Court, J.; Touchette, C.J.; Iorio-Morin, C.; Westwick, H.J.; Belzile, F.; Effendi, K. Embolization of the Middle meningeal artery in chronic subdural hematoma—A systematic review. Clin. Neurol. Neurosurg. 2019, 186, 105464. [Google Scholar] [CrossRef]
- Jumah, F.; Osama, M.; Islim, A.I.; Jumah, A.; Patra, D.P.; Kosty, J.; Narayan, V.; Nanda, A.; Gupta, G.; Dossani, R.H. Efficacy and safety of middle meningeal artery embolization in the management of refractory or chronic subdural hematomas: A systematic review and meta-analysis. Acta Neurochir. 2020, 162, 499–507. [Google Scholar] [CrossRef]
- Désir, L.L.; D’Amico, R.; Link, T.; Silva, D.; Ellis, J.A.; Doron, O.; Langer, D.J.; Ortiz, R.; Serulle, Y. Middle Meningeal Artery Embolization and the Treatment of a Chronic Subdural Hematoma. Cureus 2021, 13, e18868. [Google Scholar] [CrossRef]
- Ban, S.P.; Hwang, G.; Byoun, H.S.; Kim, T.; Lee, S.U.; Bang, J.S.; Han, J.H.; Kim, C.-Y.; Kwon, O.-K.; Oh, C.W. Middle Meningeal Artery Embolization for Chronic Subdural Hematoma. Radiology 2018, 286, 992–999. [Google Scholar] [CrossRef]
- Waqas, M.; Vakhari, K.; Weimer, P.V.; Hashmi, E.; Davies, J.M.; Siddiqui, A.H. Safety and Effectiveness of Embolization for Chronic Subdural Hematoma: Systematic Review and Case Series. World Neurosurg. 2019, 126, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Kim, E. Embolization Therapy for Refractory Hemorrhage in Patients with Chronic Subdural Hematomas. World Neurosurg. 2017, 101, 520–527. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Perez, R.; Rayo, N.; Tsimpas, A. Embolización endovascular de la arteria meníngea media para el tratamiento de hematomas subdurales crónicos: Efectividad, seguridad y controversia actual. Revisión Sist. 2020. [Google Scholar] [CrossRef] [PubMed]
- Nia, A.M.; Srinivasan, V.M.; Siddiq, F.; Thomas, A.; Burkhardt, J.-K.; Lall, R.R.; Kan, P. Trends and Outcomes of Primary, Rescue, and Adjunct Middle Meningeal Artery Embolization for Chronic Subdural Hematomas. World Neurosurg. 2022, 164, e568–e573. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| CONTROVERSIES |
|---|
|
| Subject | Recommendation | Grade | Studies |
|---|---|---|---|
| Indication of Surgery |
| C | Sahyouni et al. [7] 2017 Shlobin et al. [8] 2021 Soleman et al. [9] 2014 Soleman et al. [10] 2017 Kolias et al. [11] 2014 Mehta et al. [12] 2018 Feghali et al. [13] 2020 Yadav et al. [14] 2016 Ivamoto et al. [15] 2016 Holl et al. [16] 2018 Nouri et al. [17] 2021 |
| C | ||
| Timing of Surgery |
| C | Venturini et al. [18] 2019 Soleman et al. [9] 2014 Kolias et al. [11] 2014 Heidbuchel et al. [19] 2013 |
| Surgical Method |
| A | Kolias et al. [11] 2014 Mehta et al. [12] 2018 Soleman et al. [9] 2014 Feghali et al. [13] 2020 Yadav et al. [14] 2016 Almenawer et al. [20] 2014 Lega et al. [21] 2010 Weigel et al. [5] 2003 Cofano et al. [22] 2020 Duerinck et al. [23] 2022 Ducruet et al. [24] 2012 Mondorf et al. [25] 2009 Shim et al. [26] 2019 Raghavan et al. [27] 2020 Gazzeri et al. [28] 2020 Xu et al. [29] 2018 Yagnik et al. [2] 2021 Guo et al. [30] 2020 Zhang et al. [31] 2018 Amano et al. [32] 2021 Zhang et al. [33] 2020 Yan et al. [34] 2017 Matsumoto et al. [35] 2018 |
| B | ||
| Number of burr holes |
| A | Mersha et al. [36] 2020 Abdelfatah et al. [37] 2019 Sale et al. [38] 2021 Nayil et al. [39] 2014 Opšenák et al. [40] 2020 Kansal et al. [41] 2010 Heringer et al. [42] 2017 Nalin et al. [43] 2021 Almenawer et al. [20] 2014 Belkhair et al. [44] 2013 Smith et al. [45] 2012 Wan et al. [46] 2019 |
| Irrigation |
| B | Yadav et al. [14] 2016 Weigel et al. [5] 2003 Ishibashi et al. [47] 2011 Ram et al. [48] 1993 Hennig et al. [49] 1999 Aoki et al. [50] 1984 Lega et al. [21] 2010 Iftikhar et al. [51] 2016 Matsumoto et al. [52] 1999 Suzuki et al. [53] 1998 Zakaraia et al. [54] 2008 Xu et al. [55] 2016 Yuan et al. [56] 2018 |
| Drainage Insertion |
| A | Santarius et al. [57] 2009 Peng et al. [58] 2016 Alcala-Cerra et al. [59] 2014 Ivamoto et al. [15] 2016 Almenawer et al. [20] 2014 |
| Drainage location |
| A | Soleman et al. [9] 2014 Yadav et al. [14] 2016 Bellut et al. [60] 2012 Greuter et al. [61] 2020 Oral et al. [62] 2015 Pranata et al. [63] 2020 Hwang et al. [64] 2022 Pathoumthong [65] 2021 Gazzeri et al. [28] 2020 Feghali et al. [13] 2020 Chin et al. [66] 2017 Xie et al. [67] 2019 Ding et al. [68] 2020 Soleman et al. [5] 2019 Zhang et al. [69] 2019 |
| B | ||
| Drainage duration |
| B | Opšenák et al. [40] 2020 Jensen et al. [70] 2021 Glancz et al. [71] 2019 Kale et al. [72] 2017 |
| Membranectomy |
| B | Mehta et al. [11] 2018 Kim et al. [73] 2011 Elayouty et al. [74] 2018 Sahyouni et al. [75] 2017 |
| MMA embolization |
| B | Adusumili et al. [76] 2022 Catapano et al. [3] 2020 Ironside et al. [77] 2021 Srivatsan et al. [78] 2019 Haldrup et al. [79] 2020 NG et al. [80] 2020 Court et al. [81] 2019 Cristofori et al. [82] 2022 Jumah et al. [83] 2020 Desir et al. [84] 2021 Ban et al. [85] 2018 Waqas et al. [86] 2019 Kim et al. [87] 2017 Martinez-Per. et al. [88] 2020 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Solou, M.; Ydreos, I.; Gavra, M.; Papadopoulos, E.K.; Banos, S.; Boviatsis, E.J.; Savvanis, G.; Stavrinou, L.C. Controversies in the Surgical Treatment of Chronic Subdural Hematoma: A Systematic Scoping Review. Diagnostics 2022, 12, 2060. https://doi.org/10.3390/diagnostics12092060
Solou M, Ydreos I, Gavra M, Papadopoulos EK, Banos S, Boviatsis EJ, Savvanis G, Stavrinou LC. Controversies in the Surgical Treatment of Chronic Subdural Hematoma: A Systematic Scoping Review. Diagnostics. 2022; 12(9):2060. https://doi.org/10.3390/diagnostics12092060
Chicago/Turabian StyleSolou, Mary, Ioannis Ydreos, Maria Gavra, Evangelos K. Papadopoulos, Stamatis Banos, Efstathios J. Boviatsis, Georgios Savvanis, and Lampis C. Stavrinou. 2022. "Controversies in the Surgical Treatment of Chronic Subdural Hematoma: A Systematic Scoping Review" Diagnostics 12, no. 9: 2060. https://doi.org/10.3390/diagnostics12092060