
Ecthyma Gangrenosum Secondary to Methicillin-Sensitive Staphylococcus aureus in an Atopic Child with Transient Neutropenia: A Case Report and Review of the Literature

 , ,
, ,
Abstract
:1. Introduction
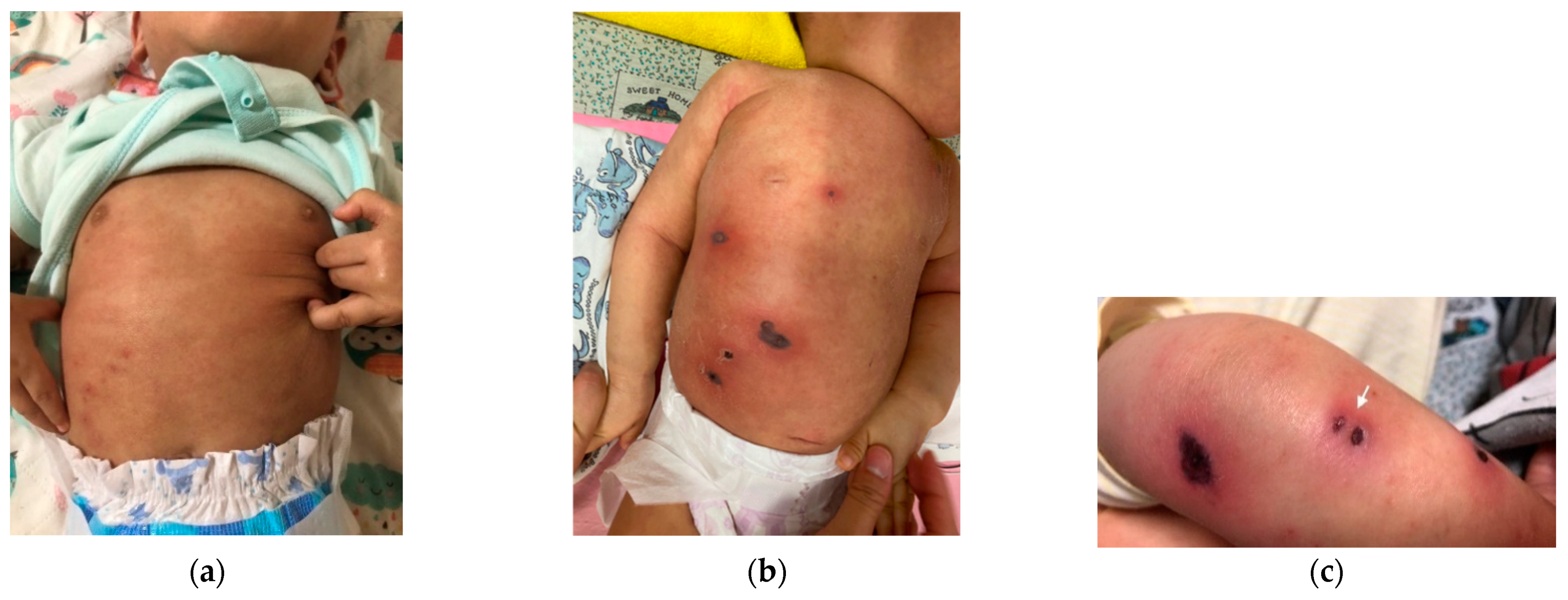
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chang, A.Y.; Carlos, C.A.; Schuster, M.; Xu, X.; Rosenbach, M. Nonpseudomonal ecthyma gangrenosum associated with methicillin-resistant staphylococcus aureus infection: A case report and review of the literature. Cutis 2012, 90, 67–69. [Google Scholar] [PubMed]
- Reich, H.L.; Williams Fadeyi, D.; Naik, N.S.; Honig, P.J.; Yan, A.C. Nonpseudomonal ecthyma gangrenosum. J. Am. Acad. Dermatol. 2004, 50, S114–S117. [Google Scholar] [CrossRef] [PubMed]
- Wasserzug, O.; Valinsky, L.; Klement, E.; Bar-Zeev, Y.; Davidovitch, N.; Orr, N.; Korenman, Z.; Kayouf, R.; Sela, T.; Ambar, R.; et al. A cluster of ecthyma outbreaks caused by a single clone of invasive and highly infective Streptococcus pyogenes. Clin. Infect. Dis. 2009, 48, 1213–1219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ivanaviciene, J.; Chirch, L.; Grant-Kels, J.M.; Kerr, P.E.; Finch, J. Ecthyma gangrenosum secondary to methicillin-sensitive Staphylococcus aureus. Int. J. Womens Dermatol. 2016, 2, 89–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pechter, P.M.; Marchione, R.; Milikowski, C.; Berman, B. Ecthyma gangrenosum secondary to Staphylococcus aureus in an infant with transient neutropenia. Pediatr. Dermatol. 2012, 29, 320–323. [Google Scholar] [CrossRef] [PubMed]
- Sen, H.; Inangil, G.; Sahin, L.; Dere, K.; Ozkan, S.; Dagli, G. Ecthyma-gangrenosum-like lesions associated with methicillin-resistant Staphylococcus aureus infection. Int. J. Infect. Dis. 2009, 13, e173–e175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, D.J.; Leibowitz, R.; Salonia, J. Ecthyma Gangrenosum: A Rare Manifestation of Staphylococcus aureus Infection. J. Sci. Innov. Med. 2021, 4, 17. [Google Scholar] [CrossRef]
- Song, S.S.; Matiz, C.; Tom, W.L.; Calame, A.; Krakowski, A.C.; Friedlander, S.F. Ecthyma Gangrenosum-Like Lesions Secondary to Methicillin-Sensitive Staphylococcus aureus in an Immunocompetent Child. Pediatr. Dermatol. 2015, 32, e259–e262. [Google Scholar] [CrossRef] [PubMed]
- Ungprasert, P.; Permpalung, N.; Kue, A.P.P.; Ammannagari, N.; Chongnarungsin, D. A rare case of ecthyma gangrenosum associated with methicillin-resistant Staphylococcus aureus infection. J. Infect. Chemother 2013, 19, 761–763. [Google Scholar] [CrossRef] [PubMed]
- Gargouri, L.; Maaloul, I.; Kamoun, T.; Maalej, B.; Safi, F.; Majdoub, I.; Hachicha, M.; Mahfoudh, A. Ecthyma gangrenosum: A manifestation of community-acquired Pseudomonas aeruginosa septicemia in three infants. Arch. Pediatr. 2015, 22, 616–620. [Google Scholar] [CrossRef] [PubMed]
- Wuyts, L.; Wojciechowski, M.; Maes, P.; Matthieu, L.; Lambert, J.; Aerts, O. Juvenile ecthyma gangrenosum caused by Pseudomonas aeruginosa revealing an underlying neutropenia: Case report and review of the literature. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 781–785. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Singh Lubana, S.; Dabrowski, L. Isolated Chronic and Transient Neutropenia. Cureus 2019, 11, e5616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dorff, G.J.; Geimer, N.F.; Rosenthal, D.R.; Rytel, M.W. Pseudomonas septicemia. Illustrated evolution of its skin lesion. Arch. Intern. Med. 1971, 128, 591–595. [Google Scholar] [CrossRef] [PubMed]
- Fetzer, A.E.; Werner, A.S.; Hagstrom, J.W. Pathologic features of pseudomonal pneumonia. Am. Rev. Respir. Dis. 1967, 96, 1121–1130. [Google Scholar] [CrossRef] [PubMed]
- Boo, Y.J.; Nam, M.H.; Lee, E.H.; Lee, K.C. Cyclic neutropenia with a novel gene mutation presenting with a necrotizing soft tissue infection and severe sepsis: Case report. BMC Pediatr. 2015, 15, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zergham, A.S.; Acharya, U. Cyclic Neutropenia; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Ceylan, N.; Demir, N.; Kocaman, S.; Peker, E.; Tuncer, O. An Extraordinary Cause of the Sucking Difficulty: Ecthyma Gangrenosum. Case Rep. Med. 2016, 2016, 8502150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geoghegan, J.A.; Irvine, A.D.; Foster, T.J. Staphylococcus aureus and Atopic Dermatitis: A Complex and Evolving Relationship. Trends. Microbiol. 2018, 26, 484–497. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Bayer, A.; Cosgrove, S.E.; Daum, R.S.; Fridkin, S.K.; Gorwitz, R.J.; Kaplan, S.L.; Karchmer, A.W.; Levine, D.P.; Murray, B.E.; et al. Clinical practice guidelines by the infectious diseases society of america for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children: Executive summary. Clin. Infect. Dis. 2011, 52, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Stevens, D.L.; Bisno, A.L.; Chambers, H.F.; Dellinger, E.P.; Goldstein, E.J.; Gorbach, S.L.; Hirschmann, J.V.; Kaplan, S.L.; Montoya, J.G.; Wade, J.C.; et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2014, 59, e10–e52. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Author (Date) | Underlying Medical Condition | Initial Presentation | Blood Cultures | Lesion Cultures | Bacteria in Pathology | Antibiotics | Outcome |
|---|---|---|---|---|---|---|---|
| Pechter et al. (2012) | 8-month-old infant with transient neutropenia | Febrile seizure, acute otitis media and skin rash | Negative | Culture: MRSA | GPC at epidermal area | IV vancomycin + cefepime + amikacin- > vancomycin | Discharged |
| Song et al. (2015) | Healthy 15-month-old girl | Fever and “flea bite-like lesions” on her chest | Negative | Culture: MSSA | Not observed | IV doxycycline- > PO cephalexin | Discharged |
| Chang et al. (2012) | 35-year-old with leukemia | Tender and hemorrhagic skin lesions | Negative | Culture: MRSA | GPC in the dermis | IV vancomycin | Discharged |
| Ungprasert et al. (2013) | 40-year-old male with AIDS | Painful lump in the right side of his neck | Negative | Prior skin abscess: MRSA | No biopsy | PO linezolid | Discharged |
| Ivanaviciene et al. (2015) | 54-year-old female with SLE and metastatic gastric cancer | Fever and painful skin lesions | Negative | Culture: MSSA | GPC within intraepidermal area | IV vancomycin + nafcillin | Discharged |
| Shah et al. (2021) | A 62-year-old male with hypertension and hyperlipidemia | Scattered skin rash | Positive | Culture: MSSA | GPC in dermis | IV vancomycin + cefepime then- > nafcillin | Died of multiple organ failure |
| Sen et al. (2009) | 69-year-old male with COPD | Mottled skin lesions | Positive | Culture: MRSA | No biopsy | IV ampicillin/sulbactam + meropenem + teicoplanin | Died of septic shock |
| Current presenting case | 1-year-old boy with atopic dermatitis and transient neutropenia | Fever and itchy skin wounds | Negative | Culture: MSSA | GPC at subepidermal area | IV cefepime + amikacin + teicoplanin- > cefepime | Discharged |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fang, K.-C.; Lin, F.-J.; Chen, C.-H.; Huang, Y.-N.; Lan, J.; Tseng, H.-C.; Huang, Y.-C. Ecthyma Gangrenosum Secondary to Methicillin-Sensitive Staphylococcus aureus in an Atopic Child with Transient Neutropenia: A Case Report and Review of the Literature. Diagnostics 2022, 12, 1683. https://doi.org/10.3390/diagnostics12071683
Fang K-C, Lin F-J, Chen C-H, Huang Y-N, Lan J, Tseng H-C, Huang Y-C. Ecthyma Gangrenosum Secondary to Methicillin-Sensitive Staphylococcus aureus in an Atopic Child with Transient Neutropenia: A Case Report and Review of the Literature. Diagnostics. 2022; 12(7):1683. https://doi.org/10.3390/diagnostics12071683
Chicago/Turabian StyleFang, Ko-Chun, Fang-Ju Lin, Chih-Ho Chen, Yi-Ning Huang, Jui Lan, Han-Chi Tseng, and Yi-Chuan Huang. 2022. "Ecthyma Gangrenosum Secondary to Methicillin-Sensitive Staphylococcus aureus in an Atopic Child with Transient Neutropenia: A Case Report and Review of the Literature" Diagnostics 12, no. 7: 1683. https://doi.org/10.3390/diagnostics12071683