
Cone Beam Computerized Tomographic Analysis of Collum Angle of the Maxillary Central Incisors in Different Types of Malocclusion: Comparative Assessment in Saudi, Jordan and Egypt Subpopulation

 ,
,  ,
,
Abstract
:1. Introduction
- Determine and compare the mean CA for maxillary central incisor based upon gender
- Determine and compare the mean CA for maxillary central incisor in patients with different nationalities namely, Saudi, Jordanians and Egyptians
- Test for significant differences in the CA of maxillary central incisor with different molar malocclusions.
2. Materials and Methods
2.1. Sample Characteristics
2.2. Studied Parameters
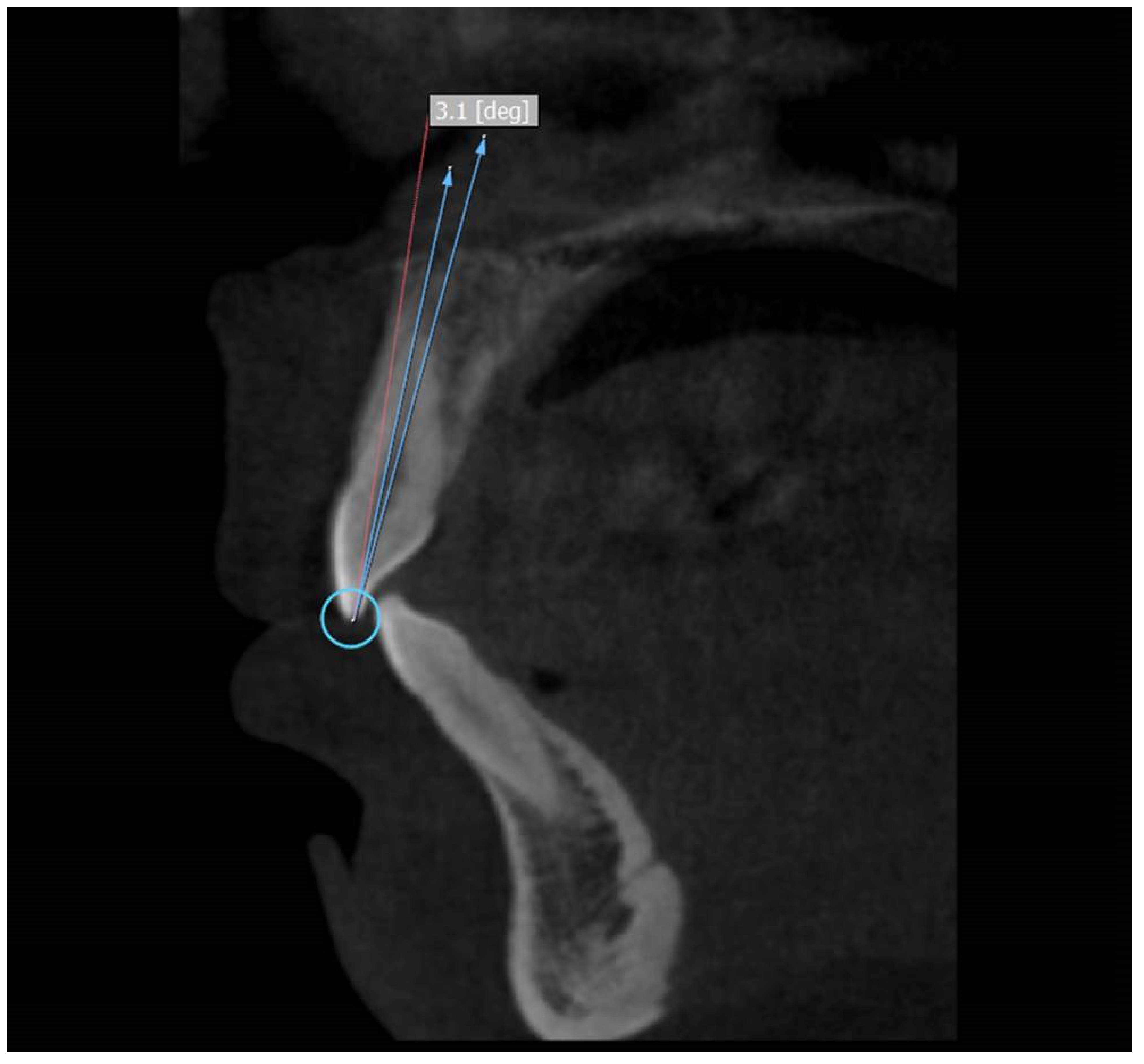
2.3. Measurement of Crown to Root Angle (x)
2.4. Measurement of Error
2.5. Statistical Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bryant, R.; Sadowsky, P.; Dent, M.; Hazelrig, J. Variability in three morphologic features of the permanent maxillary central incisor. Am. J. Orthod. 1984, 86, 25–32. [Google Scholar] [CrossRef]
- Elangovan, B.; Srinivasan, B.; Kailasam, V.; Padmanabhan, S. Comparison of the collum angle of incisors and canines in skeletal malocclusions—A CBCT study. Int. Orthod. 2020, 18, 468–479. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.W.; Hsu, J.T.; Wang, Y.H.; Huang, H.L.; Fuh, L.J. The collum angle of the maxillary central incisors in patients with different types of malocclusion. J. Dent. Sci. 2012, 7, 72–76. [Google Scholar] [CrossRef] [Green Version]
- Abate, A.; Gaffuri, F.; Lanteri, V.; Fama, A.; Ugolini, A.; Mannina, L.; Maspero, C. A CBCT based analysis of the correlation between volumetric morphology of the frontal sinuses and the facial growth pattern in caucasian subjects. A cross-sectional study. Head Face Med. 2022, 18, 4. [Google Scholar] [CrossRef]
- Alam, M.K.; Alzarea, B.K.; Ganji, K.K.; Kundi, I.; Patil, S. 3D CBCT human adult odontometrics: Comparative assessment in Saudi, Jordan and Egypt population. Saudi Dent. J. 2019, 31, 336–342. [Google Scholar] [CrossRef]
- Cavagnetto, D.; Abate, A.; Caprioglio, A.; Cressoni, P.; Maspero, C. Three-dimensional volumetric evaluation of the different mandibular segments using CBCT in patients affected by juvenile idiopathic arthritis: A cross-sectional study. Prog. Orthod. 2021, 22, 32. [Google Scholar] [CrossRef]
- Stirrups, D. Guidance on presentation of cephalometry-based research studies. A personal perspective. Br. J. Orthod. 1993, 20, 359–365. [Google Scholar] [CrossRef]
- Houston, W.J.B. The analysis of errors in orthodontic measurements. Am. J. Orthod. 1983, 83, 382–390. [Google Scholar] [CrossRef]
- Heravi, F.; Salari, S.; Tanbakuchi, B.; Loh, S.; Amiri, M. Effects of crown-root angle on stress distribution in the maxillary central incisors’ PDL during application of intrusive and retraction forces: A three-dimensional finite element analysis. Prog. Orthod. 2013, 14, 26. [Google Scholar] [CrossRef] [Green Version]
- Yatabe, M.; Prieto, J.C.; Styner, M.; Zhu, H.; Ruellas, A.C.; Paniagua, F.; Budin, F.; Benavides, E.; Shoukri, B.; Michoud, L.; et al. 3D superimposition of craniofacial imaging-The utility of multicentre collaborations. Orthod. Craniofac. Res. 2019, 22, 213–220. [Google Scholar] [CrossRef]
- Kau, C.; Olim, S.; Nguyen, J. The Future of Orthodontic Diagnostic Records. Semin. Orthod. 2011, 17, 39–45. [Google Scholar] [CrossRef]
- Cakan, D.G.; Ulkur, F.; Taner, T.U. The genetic basis of facial skeletal characteristics and its relation with orthodontics. Eur. J. Dent. 2012, 6, 340–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Srinivasan, B.; Kailasam, V.; Chitharanjan, A.; Ramalingam, A. Relationship between crown-root angulation (Collum angle) of maxillary central incisors in Class II, division 2 malocclusion and lower lip line. Orthodontics 2013, 14, e66–e74. [Google Scholar] [CrossRef] [PubMed]
- Lapatki, B.; Mager, A.; Schulte-Moenting, J.; Jonas, I. The importance of the level of the lip line and resting lip pressure in Class II division 2 malocclusion. J. Dent. Res. 2002, 81, 323–328. [Google Scholar] [CrossRef]
- Delivanis, H.; Kuftinec, M. Variation in morphology of the maxillary central incisors found in Class II, division 2 malocclusions. Am. J. Orthod. 1980, 78, 438–443. [Google Scholar] [CrossRef]
- Israr, J.; Bhutta, N.; Rafique Chatha, M. Comparison of collum angle of maxillary central incisors in Class II div 1 and 2 malocclusions. Pak. Oral Dent. J. 2016, 36, 91–94. [Google Scholar]
- Feres, M.F.N.; Rozolen, B.S.; Alhadlaq, A.; Alkhadra, T.A.; El-Bialy, T. Comparative tomographic study of the maxillary central incisor collum angle between Class I, Class II, division 1 and 2 patients. J. Orthod. Sci. 2018, 7, 6. [Google Scholar] [CrossRef]
- Williams, A.; Woodhouse, C. The crown to root angle of maxillary central incisors in different incisal classes. Br. J. Orthod. 1983, 10, 159–161. [Google Scholar] [CrossRef]
- McIntyre, G.T.; Millett, D.T. Crown-root shape of the permanent maxillary central incisor. Angle Orthod. 2003, 73, 710. [Google Scholar]
- Li, M.; Wang, S.W.; Zhao, Y.J.; Liu, Y. A cone-beam computed tomography study on crown-root morphology of maxillary anterior teeth in Class II, division 2 malocclusion. J. Peking Univ. Health Sci. 2016, 48, 105–110. [Google Scholar]
- Harris, E.F.; Hassankiadeh, S.; Harris, J.T. Maxillary incisor crown-root relationships in different Angle malocclusions. Am. J. Orthod. Dentofac. Orthop. 1993, 103, 48–53. [Google Scholar] [CrossRef]
- Shailaja, A.M.; Gowda, N.C.; Gowda, S. The collum angle of maxillary central incisors in different skeletal malocclusions—A Cephaometric study. Int. J. Appl. Dent. Sci. 2016, 2, 33–36. [Google Scholar]
- Korda, R.A.; Nikolidakis, D.K.; Xagoraris, M.D.; Athanasiou, A.E.; Papadopoulos, M.A. Crown/root relations and root morphological characteristics of permanent maxillary central incisors in Class II, division 1 and 2 malocclusions. Hell Orthod. Rev. 2000, 3, 89–96. [Google Scholar]
- Wang, X.M.; Wang, J.; Zou, M.; Zheng, J.; Xue, H. Analysis of the discrepancy of crown-root morphology of central incisors among different skeletal malocclusion using cone-beam CT. Chin. J. Stomatol. 2019, 54, 101–106. [Google Scholar]


{kind=link}
| Malocclusion Type | N | Mean | SD | 95% Confidence Interval | F Value | p Value (One Way ANOVA Test) | |
|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||||
| Class I | 100 | 6.06 | 1.75 | 5.71 | 6.40 | 283.9 | <0.0001 * |
| Class II div 1 | 100 | 6.21 | 0.83 | 6.04 | 6.37 | ||
| Class II div 2 | 100 | 10.54 | 1.85 | 10.17 | 10.90 | ||
| Class III | 100 | 5.42 | 0.75 | 5.27 | 5.56 | ||
| Total | 400 | 7.05 | 2.46 | 6.81 | 7.30 | ||
| Variables | Gender | N | Mean | SD | t Value | p Value (Independent t Test) |
|---|---|---|---|---|---|---|
| Class I | M | 69 | 6.18 | 1.89 | 1.029 | 0.306 |
| F | 31 | 5.79 | 1.35 | |||
| Class II div 1 | M | 62 | 6.37 | 0.84 | 2.643 | 0.01 * |
| F | 38 | 5.93 | 0.75 | |||
| Class II div 2 | M | 44 | 10.92 | 1.99 | 2.258 | 0.026 * |
| F | 56 | 10.17 | 1.66 | |||
| Class III | M | 53 | 5.69 | 0.76 | 4.202 | <0.0001 * |
| F | 47 | 5.10 | 0.60 |
| Variables | Nationality | N | Mean | SD | F Value | p Value (One Way ANOVA Test) |
|---|---|---|---|---|---|---|
| Class I | Saudi | 52 | 5.90 | 2.04 | 0.444 | 0.643 |
| Jordan | 23 | 6.29 | 1.33 | |||
| Egypt | 25 | 6.16 | 1.45 | |||
| Class II div 1 | Saudi | 51 | 6.13 | 0.79 | 0.605 | 0.548 |
| Jordan | 19 | 6.20 | 0.71 | |||
| Egypt | 30 | 6.34 | 0.97 | |||
| Class II div 2 | Saudi | 55 | 10.37 | 1.92 | 0.965 | 0.385 |
| Jordan | 21 | 10.43 | 1.77 | |||
| Egypt | 24 | 10.99 | 1.76 | |||
| Class III | Saudi | 49 | 5.41 | 0.80 | 1.271 | 0.285 |
| Jordan | 23 | 5.60 | 0.63 | |||
| Egypt | 28 | 5.27 | 0.75 |
| Malocclusion Groups Compared | p Value |
|---|---|
| Class I/Class II div 1 | 0.872 |
| Class I/Class II div 2 | <0.0001 * |
| Class I/Class III | 0.007 * |
| Class II div 1/Class II div 2 | <0.0001 * |
| Class II div 1/Class III | <0.0001 * |
| Class II div 2/Class III | <0.0001 * |
| Authors’ | N | Class I | Class II Div | Class III | Measurements | Comments | |
|---|---|---|---|---|---|---|---|
| 1 | 2 | ||||||
| Delivanis, H.; Kuftinec, M. (1980) | 106 | 17 | 27 | 53 | 9 | Collum angle | Class I, Class II div 1, and Class III data pooled for comparison with “severe” Class II div 2 cases only |
| Williams, A.; Woodhouse, C. (1983) | 191 | 65 | 66 | 29 | 31 | Crown/root angle | Cephalograms selected having “clarity of upper central incisors” |
| Bryant, R. et al. (1984) | 100 | 25 | 25 | 25 | 25 | Crown/root angle | Only included “severe” cases Priority given to images with “optimal sharpness and clarity” |
| Harris, E.F. et al. (1993) | 79 | 24 | 34 | 0 | 21 | Collum angle | Class II div 2 cases excluded |
| Korda, R.A. et al. (2000) | 43 | 0 | 16 | 27 | 0 | Ratio of root length/crown length and root/crown angle | Cephalograms recorded using two different cephalostats Compared only Class II div 1 with Class II div 2 |
| McIntyre, G.T.; Millett, D.T. (2003) | 361 | 71 | 139 | 60 | 91 | Crown-root shape | Monitor-displayed digital cephalograms |
| Shen, Y.W. et al. (2012) | 124 | 33 | 32 | 28 | 31 | Collum angle | Lateral cephalometric radiographs |
| Li, M. et al. (2016) | 36 | 18 | 0 | 18 | 0 | Crown-root angle and surface-shaft angle | CBCT combined with computer aided measurement technology |
| Israr, J. et al. (2016) | 60 | 0 | 30 | 30 | 0 | Collum angle | Lateral cephalometric radiographs |
| Feres, M.F.N. et al. (2018) | 48 | 16 | 16 | 16 | 0 | Collum angle | Used CBCT images |
| Wang, X.M. et al. (2019) | 66 | 24 | 20 | 22 | Collum angles and labial surface angles with different skeletal malocclusions | Used CBCT images No subdivision of Class II malocclusion | |
| Elangovan, B. et al. (2020) | 60 | 15 | 15 | 15 | 15 | Collum angle | Used CBCT images Studied maxillary and mandibular anterior teeth |
| Current study (2022) | 400 | 100 | 100 | 100 | 100 | Collum angle (mean), gender-wise and race-wise comparison | 3D CBCT |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Issrani, R.; Prabhu, N.; Siddanna, S.; Alanazi, S.H.; Alam, M.K.; Munisekhar, M.S.; Hamza, M.O.; Shabanah, R.F.D.; Gadh, R.S.A. Cone Beam Computerized Tomographic Analysis of Collum Angle of the Maxillary Central Incisors in Different Types of Malocclusion: Comparative Assessment in Saudi, Jordan and Egypt Subpopulation. Diagnostics 2022, 12, 1506. https://doi.org/10.3390/diagnostics12061506
Issrani R, Prabhu N, Siddanna S, Alanazi SH, Alam MK, Munisekhar MS, Hamza MO, Shabanah RFD, Gadh RSA. Cone Beam Computerized Tomographic Analysis of Collum Angle of the Maxillary Central Incisors in Different Types of Malocclusion: Comparative Assessment in Saudi, Jordan and Egypt Subpopulation. Diagnostics. 2022; 12(6):1506. https://doi.org/10.3390/diagnostics12061506
Chicago/Turabian StyleIssrani, Rakhi, Namdeo Prabhu, Sunitha Siddanna, Sarah Hatab Alanazi, Mohammad Khursheed Alam, Manay Srinivas Munisekhar, May Othman Hamza, Reham Fawzi Dawood Shabanah, and Rasha Saleh Ali Gadh. 2022. "Cone Beam Computerized Tomographic Analysis of Collum Angle of the Maxillary Central Incisors in Different Types of Malocclusion: Comparative Assessment in Saudi, Jordan and Egypt Subpopulation" Diagnostics 12, no. 6: 1506. https://doi.org/10.3390/diagnostics12061506