
Reliability of Gradient-Echo Magnetic Resonance Elastography of Lumbar Muscles: Phantom and Clinical Studies

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
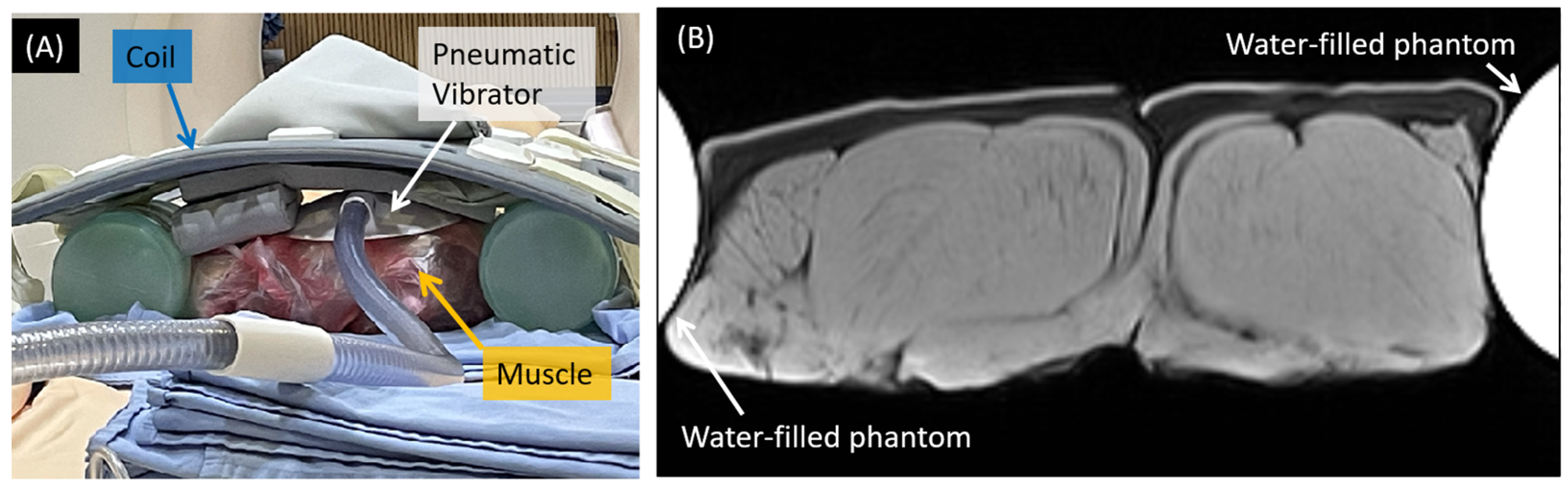
2.1. Phantom Study
2.2. Human Subjects
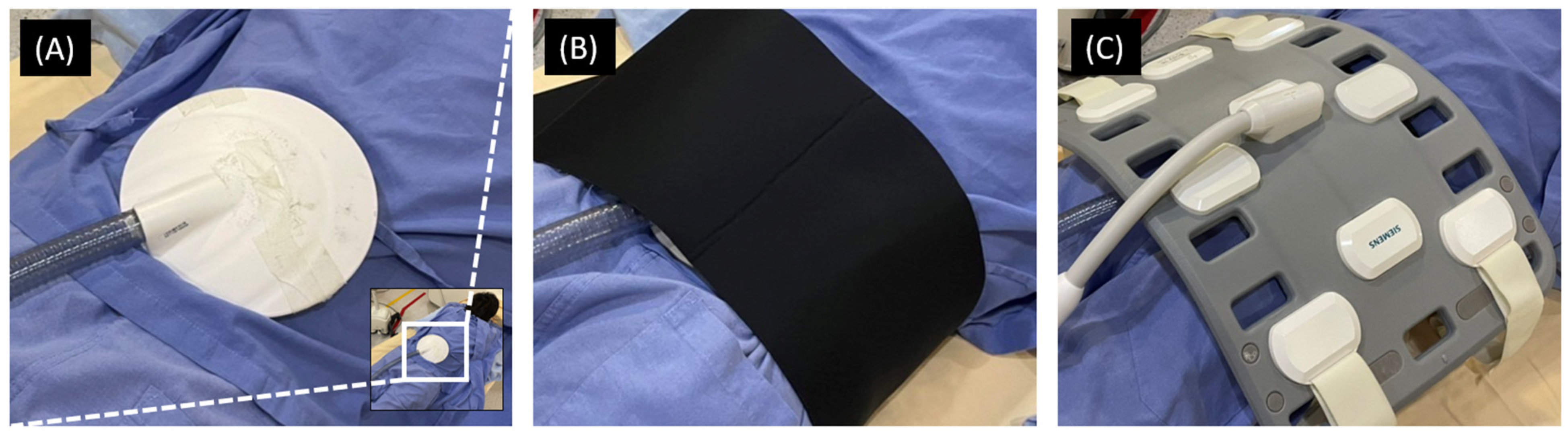
2.3. MRI Acquisition
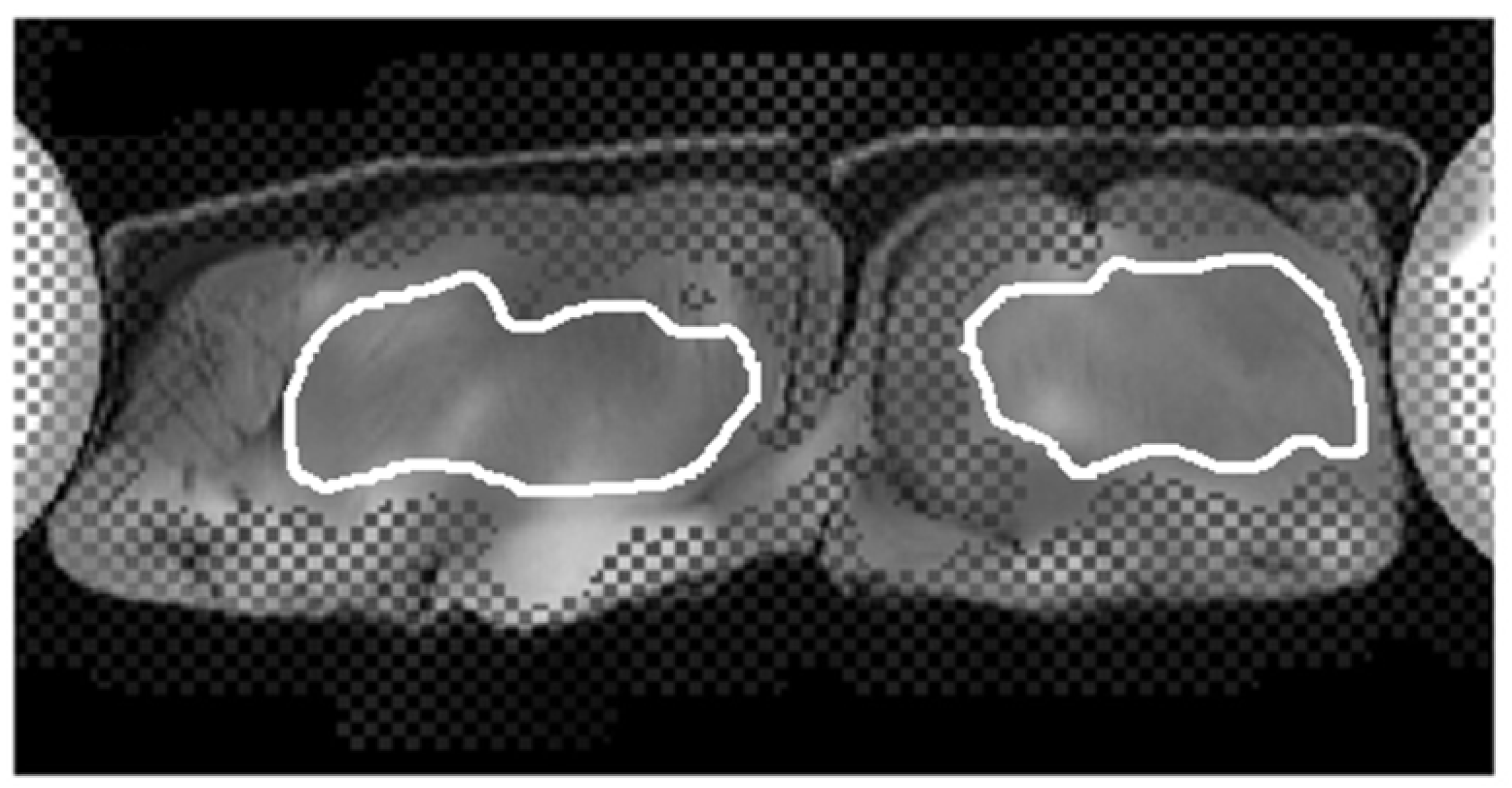
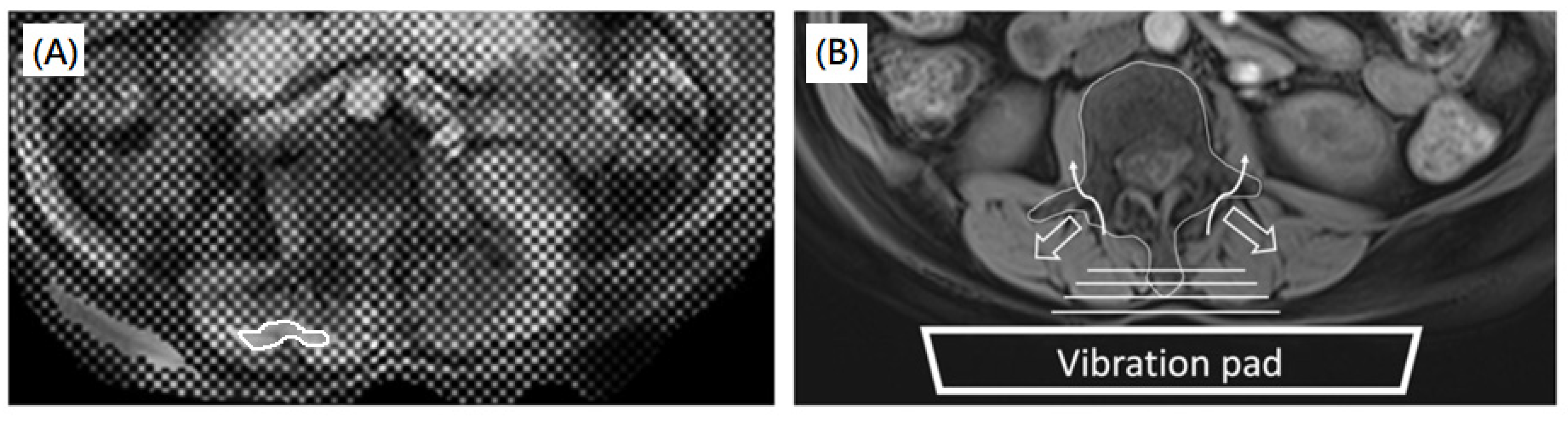
2.4. Image Processing
2.5. Reliability of MRE
2.6. Statistical Analysis
3. Results
3.1. Phantom Study
3.2. Human Subjects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kennedy, D.; Noh, M.Y. The Role of Core Stabilization in Lumbosacral Radiculopathy. Phys. Med. Rehabil. Clin. N. Am. 2011, 22, 91–103. [Google Scholar] [CrossRef] [PubMed]
- Fortin, M.; Lazáry, À.; Varga, P.P.; Battié, M.C. Association between paraspinal muscle morphology, clinical symptoms and functional status in patients with lumbar spinal stenosis. Eur. Spine J. 2017, 26, 2543–2551. [Google Scholar] [CrossRef] [PubMed]
- Kalichman, L.; Carmeli, E.; Been, E. The Association between Imaging Parameters of the Paraspinal Muscles, Spinal Degeneration, and Low Back Pain. BioMed. Res. Int. 2017, 2017, 2562957. [Google Scholar] [CrossRef]
- Cooley, J.R.; Hebert, J.J.; de Zoete, A.; Jensen, T.S.; Algra, P.R.; Kjaer, P.; Walker, B.F. Assessing lumbar paraspinal muscle cross-sectional area and fat composition with T1 versus T2-weighted magnetic resonance imaging: Reliability and concurrent validity. PLoS ONE 2021, 16, e0244633. [Google Scholar] [CrossRef]
- Suri, P.; Fry, A.L.; Gellhorn, A.C. Do Muscle Characteristics on Lumbar Spine Magnetic Resonance Imaging or Computed To-mography Predict Future Low Back Pain, Physical Function, or Performance? A Systematic Review. PMR 2015, 7, 1269–1281. [Google Scholar] [CrossRef] [PubMed]
- Hsu, P.-C.; Chang, K.-V.; Wu, W.-T.; Wang, J.-C.; Özçakar, L. Effects of Ultrasound-Guided Peritendinous and Intrabursal Corticosteroid Injections on Shoulder Tendon Elasticity: A Post Hoc Analysis of a Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2020, 102, 905–913. [Google Scholar] [CrossRef]
- Zúñiga, L.D.O.; López, C.A.G.; González, E.R. Ultrasound Elastography in the Assessment of the Stiffness of Spastic Muscles: A Systematic Review. Ultrasound Med. Biol. 2021, 47, 1448–1464. [Google Scholar] [CrossRef]
- Brandenburg, J.E.; Eby, S.F.; Song, P.; Zhao, H.; Brault, J.S.; Chen, S.; An, K.-N. Ultrasound Elastography: The New Frontier in Direct Measurement of Muscle Stiffness. Arch. Phys. Med. Rehabil. 2014, 95, 2207–2219. [Google Scholar] [CrossRef] [Green Version]
- Bensamoun, S.F.; Ringleb, S.I.; Littrell, L.; Chen, Q.; Brennan, M.; Ehman, R.L.; An, K.-N. Determination of thigh muscle stiffness using magnetic resonance elastography. J. Magn. Reson. Imaging 2006, 23, 242–247. [Google Scholar] [CrossRef]
- Debernard, L.; Robert, L.; Charleux, F.; Bensamoun, S.F. Analysis of thigh muscle stiffness from childhood to adulthood using magnetic resonance elastography (MRE) technique. Clin. Biomech. 2011, 26, 836–840. [Google Scholar] [CrossRef]
- Chakouch, M.K.; Pouletaut, P.; Charleux, F.; Bensamoun, S.F. Viscoelastic shear properties of in vivo thigh muscles measured by MR elastography. J. Magn. Reson. Imaging 2015, 43, 1423–1433. [Google Scholar] [CrossRef] [PubMed]
- Hollis, L.; Barnhill, E.; Perrins, M.; Kennedy, P.; Conlisk, N.; Brown, C.; Hoskins, P.; Pankaj, P.; Roberts, N. Finite element analysis to investigate variability of MR elastography in the human thigh. Magn. Reson. Imaging 2017, 43, 27–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy, P.; Barnhill, E.; Gray, C.; Brown, C.; van Beek, E.J.; Roberts, N.; Greig, C.A. Magnetic resonance elastography (MRE) shows significant reduction of thigh muscle stiffness in healthy older adults. GeroScience 2019, 42, 311–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heers, G.; Jenkyn, T.; Dresner, M.A.; Klein, M.-O.; Basford, J.R.; Kaufman, K.; Ehman, R.L.; An, K.-N. Measurement of muscle activity with magnetic resonance elastography. Clin. Biomech. 2003, 18, 537–542. [Google Scholar] [CrossRef]
- Basford, J.R.; Jenkyn, T.R.; An, K.N.; Ehman, R.L.; Heers, G.; Kaufman, K.R. Evaluation of healthy and diseased muscle with magnetic resonance elastography. Arch. Phys. Med. Rehabil. 2002, 83, 1530–1536. [Google Scholar] [CrossRef]
- Numano, T.; Habe, T.; Ito, D.; Onishi, T.; Takamoto, K.; Mizuhara, K.; Nishijo, H.; Igarashi, K.; Ueki, T. A new technique for motion encoding gradient-less MR elastography of the psoas major muscle: A gradient-echo type multi-echo sequence. Magn. Reson. Imaging 2019, 63, 85–92. [Google Scholar] [CrossRef]
- Koga, A.; Itoigawa, Y.; Suga, M.; Morikawa, D.; Uehara, H.; Maruyama, Y.; Kaneko, K. Stiffness change of the supraspinatus muscle can be detected by magnetic resonance elastography. Magn. Reson. Imaging 2021, 80, 9–13. [Google Scholar] [CrossRef]
- Ito, D.; Numano, T.; Takamoto, K.; Ueki, T.; Habe, T.; Igarashi, K.; Mizuhara, K.; Nishijo, H. Simultaneous acquisition of magnetic resonance elastography of the supraspinatus and the trapezius muscles. Magn. Reson. Imaging 2018, 57, 95–102. [Google Scholar] [CrossRef]
- Huwart, L.; Peeters, F.; Sinkus, R.; Annet, L.; Salameh, N.; Ter Beek, L.C.; Horsmans, Y.; Van Beers, B.E. Liver fibrosis: Non-invasive assessment with MR elastography. NMR Biomed. 2006, 19, 173–179. [Google Scholar] [CrossRef]
- Shire, N.J.; Yin, M.; Chen, J.; Railkar, R.A.; Fox-Bosetti, S.; Johnson, S.M.; Beals, C.R.; Dardzinski, B.J.; Sanderson, S.O.; Talwalkar, J.A.; et al. Test-retest repeatability of MR elastography for non-invasive liver fibrosis assessment in hepatitis C. J. Magn. Reson. Imaging 2011, 34, 947–955. [Google Scholar] [CrossRef] [Green Version]
- Venkatesh, S.K.; Yin, M.; Ehman, R.L. Magnetic resonance elastography of liver: Technique, analysis, and clinical applications. J. Magn. Reson. Imaging 2013, 37, 24092. [Google Scholar] [CrossRef] [Green Version]
- Ito, D.; Numano, T.; Ueki, T.; Habe, T.; Maeno, T.; Takamoto, K.; Igarashi, K.; Maharjan, S.; Mizuhara, K.; Nishijo, H. Magnetic resonance elastography of the supraspinatus muscle: A preliminary study on test-retest repeatability and wave quality with different frequencies and image filtering. Magn. Reson. Imaging 2020, 71, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.-K.; Fang, Y.-H.D.; Lin, L.-C.; Lin, C.-F.; Kuo, L.-C.; Chiu, F.-M.; Chen, C.-H. Magnetic Resonance Elastography in the Assessment of Acute Effects of Kinesio Taping on Lumbar Paraspinal Muscles. J. Magn. Reson. Imaging 2018, 49, 1039–1045. [Google Scholar] [CrossRef] [PubMed]
- Wagner, M.; Corcuera-Solano, I.; Lo, G.; Esses, S.; Liao, J.; Besa, C.; Chen, N.; Abraham, G.; Fung, M.; Babb, J.; et al. Technical Failure of MR Elastography Examinations of the Liver: Experience from a Large Single-Center Study. Radiology 2017, 284, 401–412. [Google Scholar] [CrossRef]
- Wagner, M.; Besa, C.; Bou Ayache, J.; Yasar, T.K.; Bane, O.; Fung, M.; Ehman, R.L.; Taouli, B. Magnetic Resonance Elastography of the Liver: Qualitative and Quantitative Comparison of Gradient Echo and Spin Echo Echoplanar Imaging Sequences. Investig. Radiol. 2016, 51, 575–581. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.J.; Kim, B.; Yu, H.J.; Huh, J.; Lee, J.H.; Lee, S.S.; Kim, K.W.; Kim, J.K. Reproducibility of hepatic MR elastography across field strengths, pulse sequences, scan intervals, and readers. Abdom. Radiol. 2019, 45, 107–115. [Google Scholar] [CrossRef]
- Qin, E.C.; Sinkus, R.; Geng, G.; Cheng, S.; Green, M.; Rae, C.; Bilston, L.E. Combining MR elastography and diffusion tensor imaging for the assessment of anisotropic mechanical properties: A phantom study. J. Magn. Reson. Imaging 2012, 37, 23797. [Google Scholar] [CrossRef]
- Serai, S.D.; Dillman, J.R.; Trout, A.T. Spin-echo Echo-planar Imaging MR Elastography versus Gradient-echo MR Elastography for Assessment of Liver Stiffness in Children and Young Adults Suspected of Having Liver Disease. Radiology 2017, 282, 761–770. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.W.; Kim, S.Y.; Yoon, H.M.; Kim, K.W.; Byun, J.H. Comparison of technical failure of MR elastography for measuring liver stiffness between gradient-recalled echo and spin-echo echo-planar imaging: A systematic review and meta-analysis. J. Magn. Reson. Imaging 2019, 51, 1086–1102. [Google Scholar] [CrossRef]
- Miyamoto, N.; Hirata, K.; Miyamoto-Mikami, E.; Yasuda, O.; Kanehisa, H. Associations of passive muscle stiffness, muscle stretch tolerance, and muscle slack angle with range of motion: Individual and sex differences. Sci. Rep. 2018, 8, 8274. [Google Scholar] [CrossRef]
- Saeki, J.; Ikezoe, T.; Yoshimi, S.; Nakamura, M.; Ichihashi, N. Menstrual cycle variation and gender difference in muscle stiffness of triceps surae. Clin. Biomech. 2019, 61, 222–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagai, T.; Schilaty, N.; Krause, D.A.; Crowley, E.M.; Hewett, T.E. Sex Differences in Ultrasound-Based Muscle Size and Mechanical Properties of the Cervical-Flexor and -Extensor Muscles. J. Athl. Train. 2020, 55, 282–288. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | Female | Male | ||
|---|---|---|---|---|
| Stiffness (kPa) in the entire muscle | n Mean ± SD (95% CI) | n Mean ± SD (95% CI) | n Mean ± SD (95% CI) | p |
| Right paraspinal muscle | 80 1.95 ± 0.35 (1.87, 2.03) | 40 1.98 ± 0.41 (1.85, 2.11) | 40 1.92 ± 0.28 (1.83, 2.01) | 0.442 |
| Left paraspinal muscle | 80 2.01 ± 0.38 (1.93, 2.10) | 40 2.08 ± 0.47 (1.93, 2.23) | 40 1.94 ± 0.23 (1.87, 2.01) | 0.934 |
| Right psoas muscle | 80 1.60 ± 0.32 (1.53, 1.67) | 40 1.70 ± 0.28 (1.60, 1.79) | 40 1.50 ± 0.32 (1.40, 1.60) | 0.005 * |
| Left psoas muscle | 80 1.50 ± 0.30 (1.43, 1.57) | 40 1.59 ± 0.23 (1.52, 1.66) | 40 1.41 ± 0.34 (1.30, 1.52) | 0.006 * |
| Stiffness in 95% confidence (kPa) | ||||
| Right paraspinal muscle | 80 2.09 ± 0.52 (1.97, 2.21) | 40 2.15 ± 0.56 (1.97, 2.33) | 40 2.03 ± 0.48 (1.88, 2.18) | 0.310 |
| Left paraspinal muscle | 78 2.22 ± 0.79 (2.04, 2.40) | 38 2.43 ± 1.01 (2.10, 2.76) | 40 2.02 ± 0.44 (1.88, 2.16) | 0.024 * |
| Right psoas muscle | 32 1.79 ± 0.43 (1.64, 1.95) | 12 2.05 ± 0.52 (1.72, 2.37) | 20 1.64 ± 0.28 (1.51, 1.77) | 0.025 * |
| Left psoas muscle | 27 1.74 ± 0.48 (1.55, 1.93) | 8 1.80 ± 0.47 (1.41, 2.20) | 19 1.71 ± 0.49 (1.48, 1.95) | 0.661 |
| Total (n = 80) | Female (n = 40) | Male (n = 40) | ||
|---|---|---|---|---|
| CV (%) | Mean ± SD (95% CI) | Mean ± SD (95% CI) | Mean ± SD (95% CI) | p |
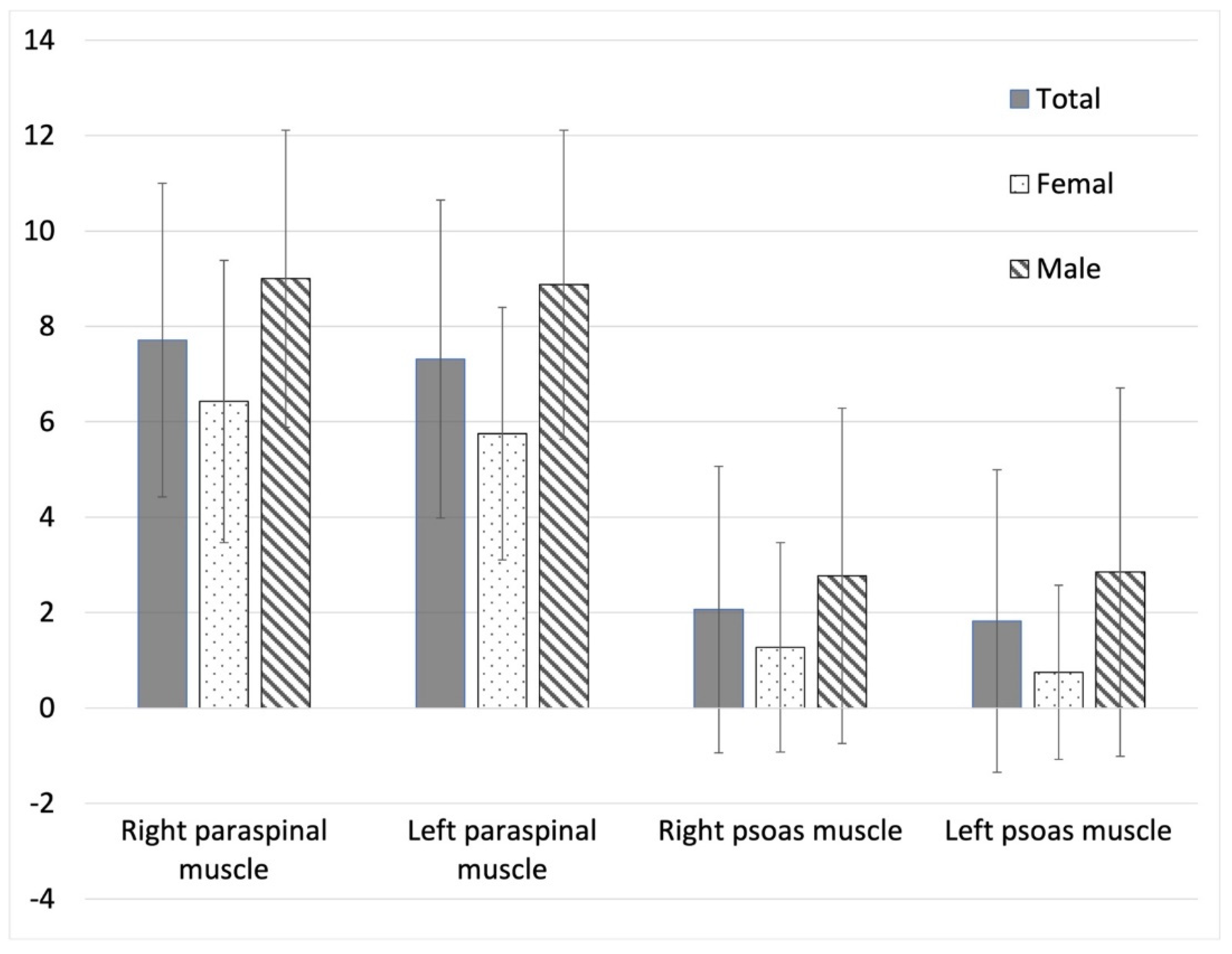
| Right paraspinal muscle | 23.32 ± 7.17 (21.71, 24.92) | 26.10 ± 6.73 (23.92, 28.28) | 20.60 ± 6.59 (18.50, 22.71) | <0.001 * |
| Left paraspinal muscle | 25.24 ± 6.95 (23.68, 26.79) | 27.29 ± 6.96 (25.03, 29.54) | 23.24 ± 6.42 (21.19, 25.29) | 0.009 * |
| Right psoas muscle | 21.57 ± 4.83 (20.49, 22.65) | 22.66 ± 4.45 (21.22, 24.11) | 20.50 ± 4.99 (18.90, 22.10) | 0.045 * |
| Left psoas muscle | 21.95 ± 4.82 (20.86, 23.03) | 23.12 ± 4.87 (21.54, 24.70) | 20.80 ± 4.55 (19.35, 22.26) | 0.032 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsieh, T.-J.; Chou, M.-C.; Chen, Y.-C.; Chou, Y.-C.; Lin, C.-H.; Chen, C.K.-H. Reliability of Gradient-Echo Magnetic Resonance Elastography of Lumbar Muscles: Phantom and Clinical Studies. Diagnostics 2022, 12, 1385. https://doi.org/10.3390/diagnostics12061385
Hsieh T-J, Chou M-C, Chen Y-C, Chou Y-C, Lin C-H, Chen CK-H. Reliability of Gradient-Echo Magnetic Resonance Elastography of Lumbar Muscles: Phantom and Clinical Studies. Diagnostics. 2022; 12(6):1385. https://doi.org/10.3390/diagnostics12061385
Chicago/Turabian StyleHsieh, Tsyh-Jyi, Ming-Chung Chou, Yi-Chu Chen, Yi-Chen Chou, Chien-Hung Lin, and Clement Kuen-Huang Chen. 2022. "Reliability of Gradient-Echo Magnetic Resonance Elastography of Lumbar Muscles: Phantom and Clinical Studies" Diagnostics 12, no. 6: 1385. https://doi.org/10.3390/diagnostics12061385