
Performance Validation of COVID-19 Self-Conduct Buccal and Nasal Swabs RTK-Antigen Diagnostic Kit

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Settings
2.2. Patients’ Recruitment
2.3. Clinical Sample Collection
2.4. Buccal–Nasal ProdetectTM RTK-Ag Self-Test
2.4.1. ProdetectTM Buccal–Nasal Test Principle
2.4.2. Self-Test Specimen Collection Procedure
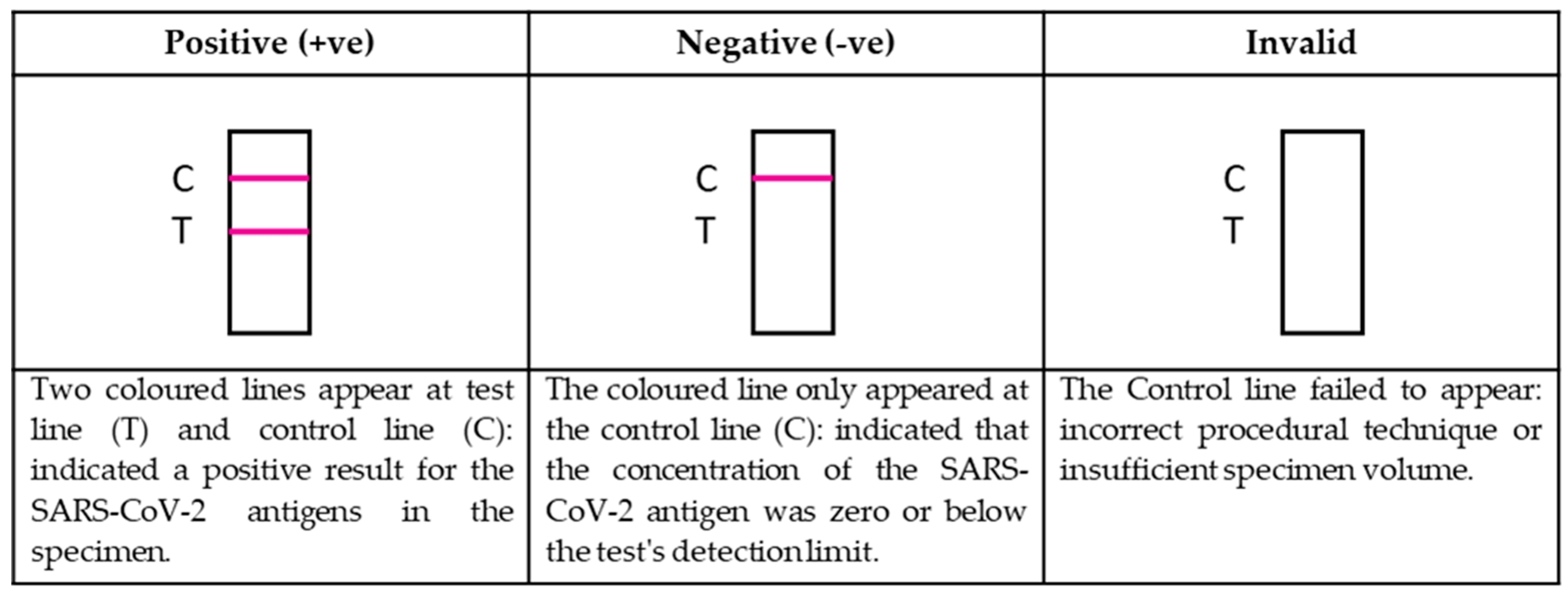
2.4.3. Antigen Detection Using Rapid Self-Test Lateral Flow Chromatographic Immunoassay
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yamayoshi, S.; Sakai-Tagawa, Y.; Koga, M.; Akasaka, O.; Nakachi, I.; Koh, H.; Maeda, K.; Adachi, E.; Saito, M.; Nagai, H.; et al. Comparison of Rapid Antigen Tests for COVID-19. Viruses 2020, 12, 1420. [Google Scholar] [CrossRef] [PubMed]
- Castillo-León, J.; Trebbien, R.; Castillo, J.J.; Svendsen, W.E. Commercially available rapid diagnostic tests for the detection of high priority pathogens: Status and challenges. Analyst 2021, 146, 3750–3776. [Google Scholar] [CrossRef] [PubMed]
- Vandenberg, O.; Martiny, D.; Rochas, O.; van Belkum, A.; Kozlakidis, Z. Considerations for diagnostic COVID-19 tests. Nat. Rev. Microbiol. 2021, 19, 171–183. [Google Scholar] [CrossRef] [PubMed]
- Ji, T.; Liu, Z.; Wang, G.; Guo, X.; Lai, C.; Chen, H.; Huang, S.; Xia, S.; Chen, B.; Jia, H. Detection of COVID-19: A review of the current literature and future perspectives. Biosens. Bioelectron. 2020, 166, 112455. [Google Scholar] [CrossRef] [PubMed]
- Peeling, R.W.; Olliaro, P.L.; Boeras, D.I.; Fongwen, N. Scaling up COVID-19 rapid antigen tests: Promises and challenges. Lancet Infect. Dis. 2021, 21, e290–e295. [Google Scholar] [CrossRef]
- Rashid, Z.Z.; Othman, S.N.; Samat, M.N.A.; Ali, U.K.; Wong, K.K. Diagnostic performance of COVID-19 serology assays. Malays. J. Pathol. 2020, 42, 13–21. [Google Scholar]
- Procop, G.W.; Kadkhoda, K.; Rhoads, D.D.; Gordon, S.G.; Reddy, A.J. Home testing for COVID-19: Benefits and limitations. Clevel. Clin. J. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Davidson, J.L.; Wang, J.; Maruthamuthu, M.K.; Dextre, A.; Pascual-Garrigos, A.; Mohan, S.; Putikam, S.V.S.; Osman, F.O.I.; McChesney, D.; Seville, J.; et al. A paper-based colorimetric molecular test for SARS-CoV-2 in saliva. Biosens. Bioelectron. X 2021, 9, 100076. [Google Scholar] [CrossRef] [PubMed]
- Prince-Guerra, J.L.; Almendares, O.; Nolen, L.D.; Gunn, J.K.L.; Dale, A.P.; Buono, S.A.; Deutsch-Feldman, M.; Suppiah, S.; Hao, L.; Zeng, Y.; et al. Evaluation of Abbott BinaxNOW Rapid Antigen Test for SARS-CoV-2 Infection at Two Community-Based Testing Sites—Pima County, Arizona, November 13–17, 2020. Morb. Mortal. Wkly. Rep. 2021, 70, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Atchison, C.; Pristerà, P.; Cooper, E.; Papageorgiou, V.; Redd, R.; Piggin, M.; Flower, B.; Fontana, G.; Satkunarajah, S.; Ashrafian, H.; et al. Usability and Acceptability of Home-based Self-testing for Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Antibodies for Population Surveillance. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, 72, e384–e393. [Google Scholar] [CrossRef] [PubMed]
- Lei, Z.; Haixia, L.; Junli, Z.; Kang, L. Different methods of COVID-19 detection. Health Sci. J. 2021, 15, 1–6. [Google Scholar]
- Giri, B.; Pandey, S.; Shrestha, R.; Pokharel, K.; Ligler, F.S.; Neupane, B.B. Review of analytical performance of COVID-19 detection methods. Anal. Bioanal. Chem. 2021, 413, 35–48. [Google Scholar] [CrossRef] [PubMed]
- Porte, L.; Legarraga, P.; Vollrath, V.; Aguilera, X.; Munita, J.M.; Araos, R.; Pizarro, G.; Vial, P.; Iruretagoyena, M.; Dittrich, S. Evaluation of a novel antigen-based rapid detection test for the diagnosis of SARS-CoV-2 in respiratory samples. Int. J. Infect. Dis. 2020, 99, 328–333. [Google Scholar] [CrossRef] [PubMed]
- Fenollar, F.; Bouam, A.; Ballouche, M.; Fuster, L.; Prudent, E.; Colson, P.; Tissot-Dupont, H.; Million, M.; Drancourt, M.; Raoult, D. Evaluation of the Panbio COVID-19 rapid antigen detection test device for the screening of patients with COVID-19. J. Clin. Microbiol. 2020, 59, e02589-20. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Mao, B.; Martinez, V.; Chen, X.; Li, Y.; He, L.; Chen, S.; Guo, X.; Shen, X.; Bao, X.; et al. A facile assay for rapid detection of COVID-19 antibodies. RSC Adv. 2020, 10, 28041–28048. [Google Scholar] [CrossRef]
- Seo, G.; Lee, G.; Kim, M.J.; Baek, S.-H.; Choi, M.; Ku, K.B.; Lee, C.-S.; Jun, S.; Park, D.; Kim, H.G.; et al. Rapid Detection of COVID-19 Causative Virus (SARS-CoV-2) in Human Nasopharyngeal Swab Specimens Using Field-Effect Transistor-Based Biosensor. ACS Nano 2020, 14, 5135–5142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brümmer, L.E.; Katzenschlager, S.; Gaeddert, M.; Erdmann, C.; Schmitz, S.; Bota, M.; Grilli, M.; Larmann, J.; Weigand, M.A.; Pollock, N.R.; et al. Accuracy of novel antigen rapid diagnostics for SARS-CoV-2: A living systematic review and meta-analysis. PLoS Med. 2021, 18, e1003735. [Google Scholar] [CrossRef] [PubMed]
- Kissler, S.M.; Fauver, J.R.; Mack, C.; Olesen, S.W.; Tai, C.; Shiue, K.Y.; Kalinich, C.C.; Jednak, S.; Ott, I.M.; Vogels, C.B.F.; et al. Viral dynamics of acute SARS-CoV-2 infection. medRxiv Prepr. Serv. Health Sci. 2021. [Google Scholar] [CrossRef]
- Au, W.Y.; Cheung, P.P.H. Diagnostic performances of common nucleic acid tests for SARS-CoV-2 in hospitals and clinics: A systematic review and meta-analysis. Lancet Microbe 2021. [Google Scholar] [CrossRef]
- World Health Organisation. Antigen-Detection in the Diagnosis of SARS-CoV-2 Infection; Interim guidance (6th October 2021); WHO/2019-nCoV/Antigen_Detection/2021.1; World Health Organisation: Geneva, Switzerland, 2021. [Google Scholar]
- Ministry of Health Malaysia. Nilai R Malaysia. Available online: https://covid-19.moh.gov.my/kajian-dan-penyelidikan/nilai-r-malaysia (accessed on 27 October 2021).


{kind=link}
| No (%) | |||||
|---|---|---|---|---|---|
| Patients (n = 120) | |||||
| RTK Result | True Positives | False Negatives | False Positives | True Negatives | Total |
| RTK (paired buccal + nasal swab) *1 | |||||
| ProdetectTM | 108 (90) | 4 (3.3) | 0 | 8 (6.7) | 120 (100) |
| RTK-Ag kit (nasopharyngeal swab) *2 | |||||
| Abbott # | 100 | 0 | 0 | 8 | 108 |
| Unknown | 12 | 0 | 0 | 0 | 12 |
| Total | 112 (93.3) | 0 | 0 | 8 (6.67) | 120 (100) |
| Characteristics | |||||
| Age | |||||
| 1–17 | 10 (8.3) | 0 | 0 | 0 | 10 (8.3) |
| 18–29 | 13 (10.8) | 2 (1.7) | 0 | 0 | 15 (12.5) |
| 30–49 | 38 (31.7) | 2 (1.7) | 0 | 2 (1.7) | 42 (35) |
| 50 and above | 44 (36.7) | 0 | 0 | 5 (4.2) | 49 (40.8) |
| Unknown | 3 (2.5) | 0 | 0 | 1 (0.8) | 4 (3.3) |
| Total | 120 (100) | ||||
| Sex | |||||
| Female | 59 (49.2) | 2 (1.7) | 0 | 4 (3.3) | 65 (54.2) |
| Male | 49 (40.8) | 2 (1.7) | 0 | 4 (3.3) | 55 (45.8) |
| Total | 120 (100) | ||||
| Nasopharyngeal RTK-Ag Test | Total | ||||
|---|---|---|---|---|---|
| Positive | Negative | ||||
| ProdetectTM | Positive | Count | 108 | 0 | 108 |
| % within ProdetectTM | 100% | 0.0% | 100.0% | ||
| % within RTK | 96.4% | 0% | 90.0% | ||
| % of Total | 90.0% | 0.0% | 90.0% | ||
| Negative | Count | 4 | 8 | 12 | |
| % within ProdetectTM | 33.3% | 66.7% | 100.0% | ||
| % within RTK | 3.6% | 100.0% | 10.0% | ||
| % of Total | 3.3% | 6.7% | 10.0% | ||
| Total | Count | 112 | 8 | 120 | |
| % within ProdetectTM | 93.3% | 6.7% | 100.0% | ||
| % within RTK | 100.0% | 100.0% | 100.0% | ||
| % of Total | 93.3% | 6.7% | 100.0% | ||
| Value | df | Asymp. Sig. (2-Sided) | Exact Sig. (2-Sided) | Exact Sig. (1-Sided) | |
|---|---|---|---|---|---|
| Pearson Chi-Square | 77.143 a | 1 | 0.000 | ||
| Continuity Correction b | 66.801 | 1 | 0.000 | ||
| Likelihood Ratio | 43.507 | 1 | 0.000 | ||
| Fisher’s Exact Test | 0.000 | 0.000 | |||
| Linear-by-Linear Association | 76.500 | 1 | 0.000 | ||
| n of Valid Cases | 120 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kalil, M.N.A.; Yusof, W.; Ahmed, N.; Fauzi, M.H.; Bakar, M.A.A.; Sjahid, A.S.; Hassan, R.; Yean Yean, C. Performance Validation of COVID-19 Self-Conduct Buccal and Nasal Swabs RTK-Antigen Diagnostic Kit. Diagnostics 2021, 11, 2245. https://doi.org/10.3390/diagnostics11122245
Kalil MNA, Yusof W, Ahmed N, Fauzi MH, Bakar MAA, Sjahid AS, Hassan R, Yean Yean C. Performance Validation of COVID-19 Self-Conduct Buccal and Nasal Swabs RTK-Antigen Diagnostic Kit. Diagnostics. 2021; 11(12):2245. https://doi.org/10.3390/diagnostics11122245
Chicago/Turabian StyleKalil, Mohammad Nur Amin, Wardah Yusof, Naveed Ahmed, Mohd Hashairi Fauzi, Mimi Azliha Abu Bakar, Afifah Sjamun Sjahid, Rosline Hassan, and Chan Yean Yean. 2021. "Performance Validation of COVID-19 Self-Conduct Buccal and Nasal Swabs RTK-Antigen Diagnostic Kit" Diagnostics 11, no. 12: 2245. https://doi.org/10.3390/diagnostics11122245