
Strategy to Reduce the Collective Equivalent Dose for the Lens of the Physician’s Eye Using Short Radiation Protection Curtains to Prevent Cataracts

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
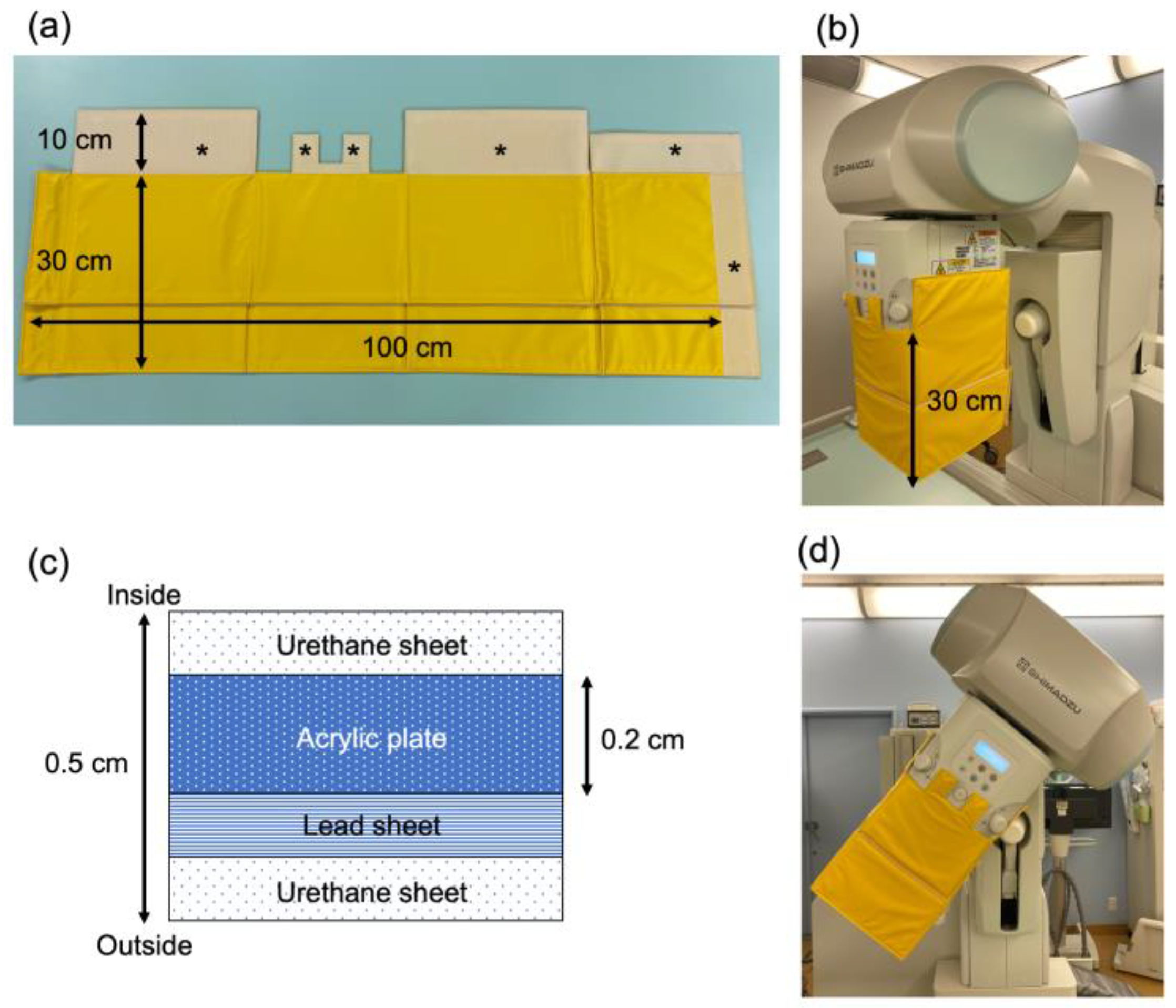
2.1. Development of the Short Curtain
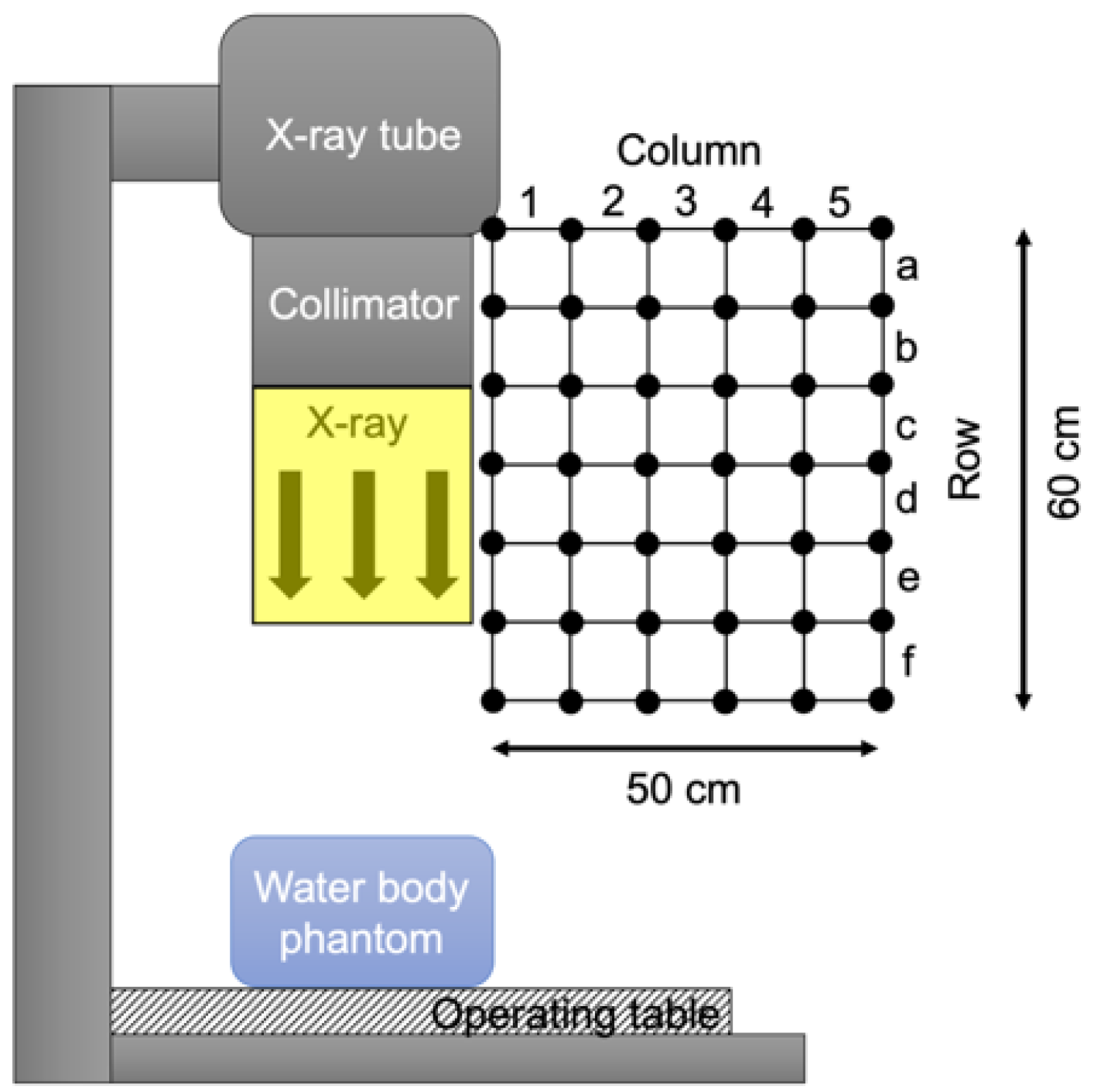
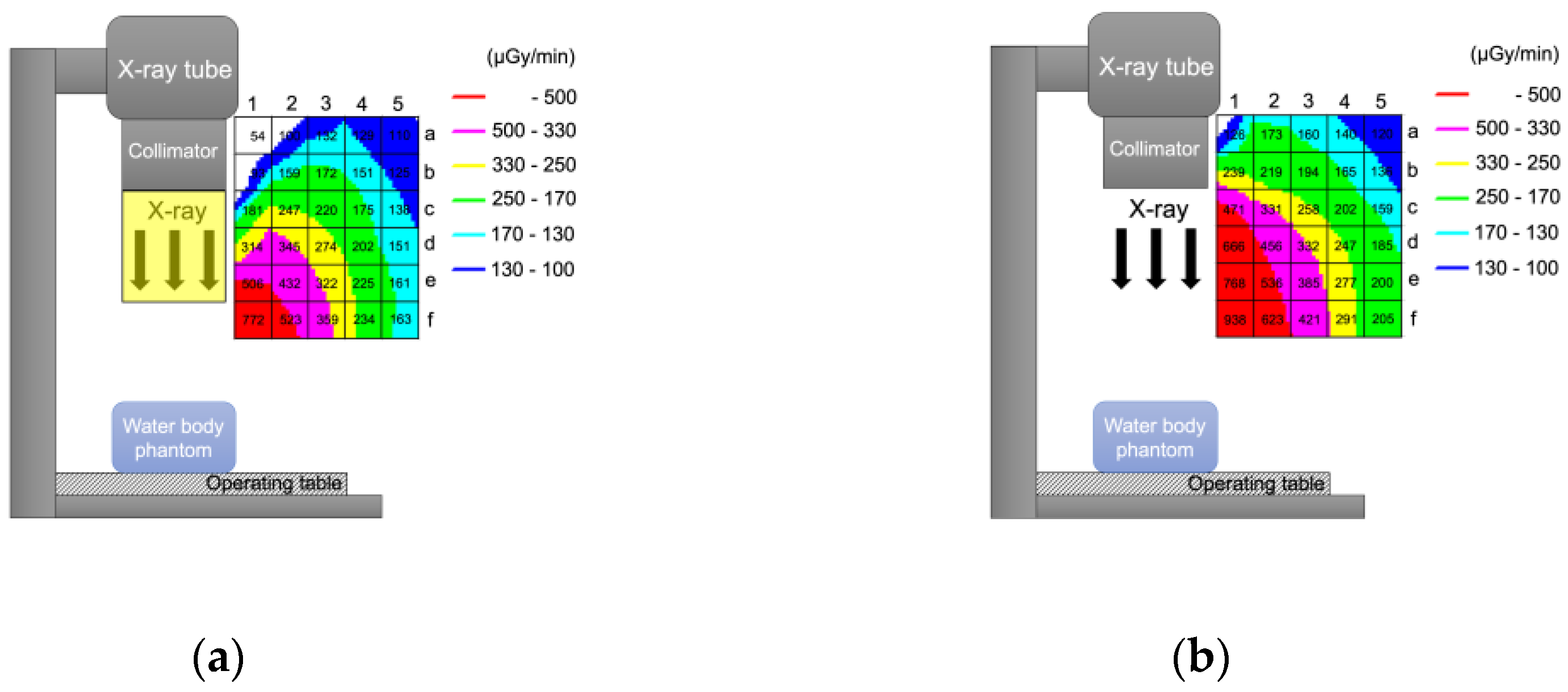
2.2. Analysis of the Air Dose Rate
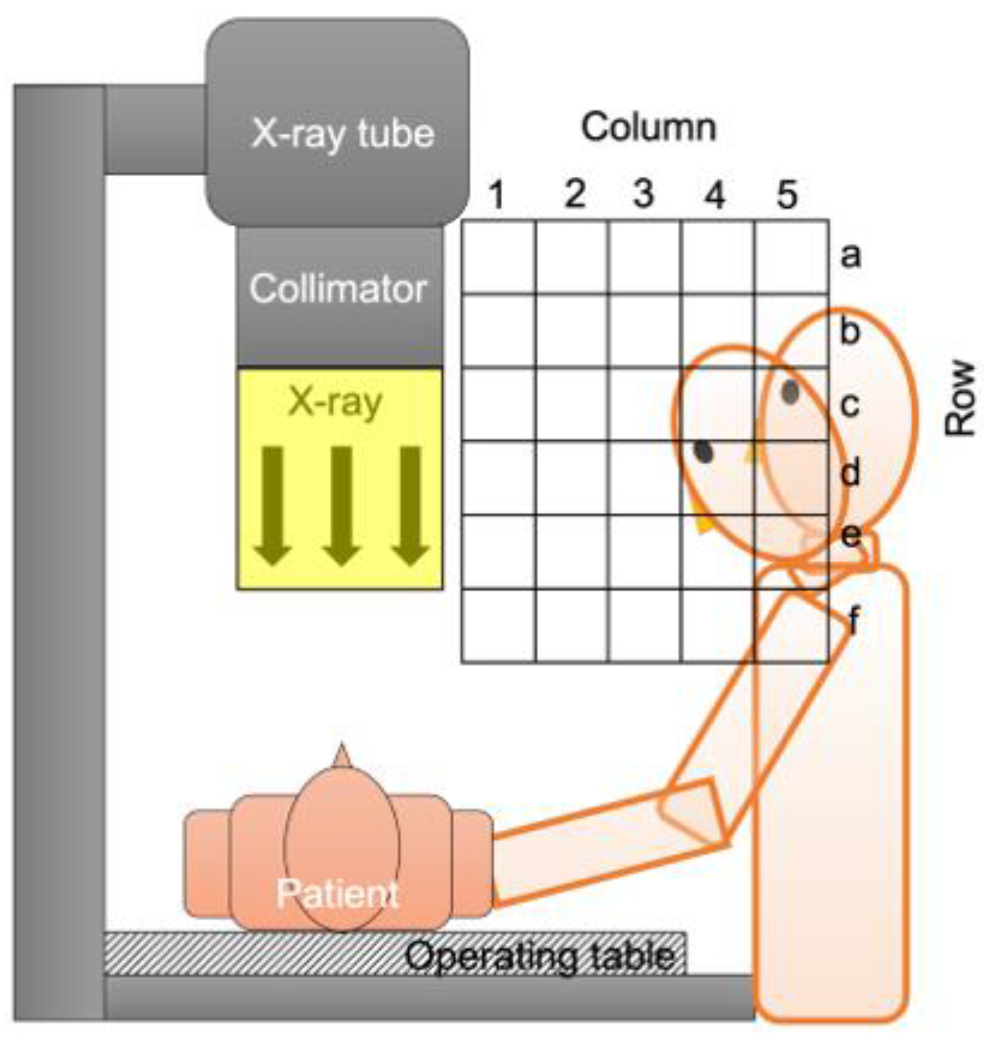
2.3. Analysis of the Physician’s Lens Presence Rate in Grid Squares
2.4. Analysis of the Physician Lens Dose Reduction Rate with the Short Curtain
2.5. Analysis of the Physician Lens Dose Reduction Rate with the Long Curtain
2.6. Analysis of the Reduction Rate in the Collective Equivalent Dose for the Lens of the Physician’s Eye with the Short Curtain and Long Curtain
3. Results
3.1. Physician Lens Dose Reduction Rate with the Short Curtain
3.2. Reduction Rate in the Collective Equivalent Dose for the Lens of the Physician’s Eye with the Short Curtain and the Long Curtain
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- ICRP. ICRP statement on tissue reactions and early and late effects of radiation in normal tissues and organs–threshold doses for tissue reactions in a radiation protection context. ICRP publication 118. Ann. ICRP 2012, 41, 1–322. [Google Scholar] [CrossRef]
- ICRP. Radiological protection in fluoroscopically guided procedures performed outside the imaging department. ICRP Publication 117. Ann. ICRP 2010, 40, 65–70. [Google Scholar]
- Zagorska, A.; Romanova, K.; Hristova-Popova, J.; Vassileva, J.; Katzarov, K. Eye lens exposure to medical staff during endoscopic retrograde cholangiopancreatography. Phys. Med. 2015, 31, 781–784. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, U.; Gallagher, A.; Malone, L.; O’Reilly, G. Occupational radiation dose to eyes from endoscopic retrograde cholangiopancreatography procedures in light of the revised eye lens dose limit from the International Commission on Radiological Protection. Br. J. Radiol. 2013, 86, 20120289. [Google Scholar] [CrossRef]
- Muniraj, T.; Aslanian, H.R.; Laine, L.; Farrell, J.; Ciarleglio, M.M.; Deng, Y.; Ho, H.; Jamidar, P.A. A double-blind, randomized, sham-controlled trial of the effect of a radiation-attenuating drape on radiation exposure to endoscopy staff during ERCP. Am. J. Gastroenterol. 2015, 110, 690–696. [Google Scholar] [CrossRef]
- Garg, M.S.; Patel, P.; Blackwood, M.; Munigala, S.; Thakkar, P.; Field, J.; Wallace, D.; Agarwal, S.; Aoun, E.; Kulkarni, A. Ocular radiation threshold projection based off of fluoroscopy time during ERCP. Am. J. Gastroenterol. 2017, 112, 716–721. [Google Scholar] [CrossRef]
- Oztas, E.; Parlak, E.; Kucukay, F.; Arhan, M.; Daglı, U.; Etik, D.O.; Onder, F.O.; Olcer, T.; Sasmaz, N. The impact of endoscopic retrograde cholangiopancreatography education on radiation exposure to experienced endoscopist:“trainee effect”. Dig. Dis. Sci. 2012, 57, 1134–1143. [Google Scholar] [CrossRef] [PubMed]
- Angsuwatcharakon, P.; Janjeurmat, W.; Krisanachinda, A.; Ridtitid, W.; Kongkam, P.; Rerknimitr, R. The difference in ocular lens equivalent dose to ERCP personnel between prone and left lateral decubitus positions: A prospective randomized study. Endosc. Int. Open 2018, 6, E969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsubara, K.; Takei, Y.; Mori, H.; Kobayashi, I.; Noto, K.; Igarashi, T.; Suzuki, S.; Akahane, K. A multicenter study of radiation doses to the eye lenses of medical staff performing non-vascular imaging and interventional radiology procedures in Japan. Phys. Med. 2020, 74, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Mori, H.; Koshida, K.; Ishigamori, O.; Matsubara, K. A novel removable shield attached to C-arm units against scattered X-rays from a patient’s side. Eur. Radiol. 2014, 24, 1794–1799. [Google Scholar] [CrossRef] [Green Version]
- Uradomo, L.; Cohen, H.; Fried, M.; Petrini, J.; Rehani, M. Radiation protection in the endoscopy suite minimizing radiation exposure for patients and staff in endoscopy: A joint ASGE/IAEA/WGO guideline. Arab J. Gastroenterol. 2010, 11, 116–119. [Google Scholar]
- IAEA. 10 Pearls: Radiation Protection of Staff in Fluoroscopy. Available online: https://www.iaea.org/sites/default/files/documents/rpop/poster-staff-radiation-protection.pdf (accessed on 28 June 2021).
- Sethi, S.; Barakat, M.T.; Friedland, S.; Banerjee, S. Radiation training, radiation protection, and fluoroscopy utilization practices among US therapeutic endoscopists. Dig. Dis. Sci. 2019, 64, 2455–2466. [Google Scholar] [CrossRef] [PubMed]
- Dave, J.K. Why Is the X-Ray Tube Usually Located Underneath the Patient Instead of Above the Patient for Interventional Fluoroscopic Procedures? Am. J. Roentgenol. 2016, 207, W24–W25. [Google Scholar] [CrossRef]
- Minami, T.; Sasaki, T.; Serikawa, M.; Kamigaki, M.; Yukutake, M.; Ishigaki, T.; Ishii, Y.; Mouri, T.; Yoshimi, S.; Shimizu, A. Occupational radiation exposure during endoscopic retrograde cholangiopancreatography and usefulness of radiation protective curtains. Gastroenterol. Res. Pract. 2014, 2014, 1–5. [Google Scholar] [CrossRef]
- Morishima, Y.; Chida, K.; Meguro, T. Effectiveness of additional lead shielding to protect staff from scattering radiation during endoscopic retrograde cholangiopancreatography procedures. J. Radiat. Res. 2018, 59, 225–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altintas, E.; Bahceci, T.; Batur, A.F.; Kaynar, M.; Kilic, O.; Akand, M.; Goktas, S.; Gul, M. A survey analysis of knowledge levels of urologists about radiation safety and fluoroscopy use. Int. J. Clin. Pract. 2021, 75, e13862. [Google Scholar] [CrossRef]
- Barakat, M.T.; Thosani, N.C.; Huang, R.J.; Choudhary, A.; Kochar, R.; Kothari, S.; Banerjee, S. Effects of a brief educational program on optimization of fluoroscopy to minimize radiation exposure during endoscopic retrograde cholangiopancreatography. Clin. Gastroenterol. Hepatol. 2018, 16, 550–557. [Google Scholar] [CrossRef] [PubMed]
- ICRP. occupational radiological protection in interventional procedures. ICRP Publication 139. Ann. ICRP 2018, 47, 1–118. [Google Scholar] [CrossRef]
- Suzuki, A.; Matsubara, K.; Chusin, T.; Suzuki, Y. Lead glasses significantly reduced radiation doses to eye lenses of urologists during procedures involving over-couch X-ray tubes. Radiat. Prot. Dosim. 2020, 189, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, A.; Matsubara, K.; Sasa, Y. Measurement of radiation doses to the eye lens during orthopedic surgery using an C-arm X-ray system. Radiat. Prot. Dosim. 2018, 179, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.H.; Park, Y.S.; Ahn, S.B.; Son, B.K. Radiation protection effect of mobile shield barrier for the medical personnel during endoscopic retrograde cholangiopancreatography: A quasi-experimental prospective study. BMJ Open 2019, 9, e027729. [Google Scholar] [CrossRef] [Green Version]
- Rose, G. Sick Individuals and Sick Populations. Int. J. Epidemiol. 1985, 14, 32–38. [Google Scholar] [CrossRef] [Green Version]
- Feigin, V.L.; Brainin, M.; Norrving, B.; Gorelick, P.B.; Dichgans, M.; Wang, W.; Pandian, J.D.; Martins, S.C.O.; Owolabi, M.O.; Wood, D.A. What Is the Best Mix of Population-Wide and High-Risk Targeted Strategies of Primary Stroke and Cardiovascular Disease Prevention? J. Am. Heart Assoc. 2020, 9, e014494. [Google Scholar] [CrossRef]
- Rose, G.A.; Khaw, K.-T.; Marmot, M. Rose’s Strategy of Preventive Medicine: The Complete Original Text; Oxford University Press: Cary, NC, USA, 2008. [Google Scholar]
- WHO. Gaining Health: The European Strategy for the Prevention and Control of Noncommunicable Diseases; 9289021799; WHO Regional Office for Europe: Copenhagen, Denmark, 2006. [Google Scholar]
- WHO. Action Plan for Implementation of the European Strategy for the Prevention and Control of Noncommunicable Diseases 2012–2016; WHO Regional Office for Europe: Copenhagen, Denmark, 2012. [Google Scholar]
- Vano, E.; Kleiman, N.J.; Duran, A.; Rehani, M.M.; Echeverri, D.; Cabrera, M. Radiation cataract risk in interventional cardiology personnel. Radiat. Res. 2010, 174, 490–495. [Google Scholar] [CrossRef]
- Chodick, G.; Bekiroglu, N.; Hauptmann, M.; Alexander, B.H.; Freedman, D.M.; Doody, M.M.; Cheung, L.C.; Simon, S.L.; Weinstock, R.M.; Bouville, A. Risk of cataract after exposure to low doses of ionizing radiation: A 20-year prospective cohort study among US radiologic technologists. Am. J. Epidemiol. 2008, 168, 620–631. [Google Scholar] [CrossRef] [Green Version]
- Thome, C.; Chambers, D.B.; Hooker, A.M.; Thompson, J.W.; Boreham, D.R. Deterministic effects to the lens of the eye following ionizing radiation exposure: Is there evidence to support a reduction in threshold dose? Health Phys. 2018, 114, 328–343. [Google Scholar] [CrossRef]
- Medici, S.; Pitzschke, A.; Cherbuin, N.; Boldini, M.; Sans-Merce, M.; Damet, J. Eye lens radiation exposure of the medical staff performing interventional urology procedures with an over-couch X-ray tube. Phys. Med. 2017, 43, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, R.M.; Vano, E.; Salinas, P.; Gonzalo, N.; Escaned, J.; Fernández, J.M. High filtration in interventional practices reduces patient radiation doses but not always scatter radiation doses. Br. J. Radiol. 2020, 94, 20200774. [Google Scholar] [CrossRef] [PubMed]
- Salinas, P.; Sanchez-Casanueva, R.M.; Gonzalo, N.; A Gil, J.; Salazar, C.H.; Jimenez-Quevedo, P.; Nombela-Franco, L.; J Nuñez-Gil, I.; Mejia-Renteria, H.; Fernandez-Soto, J.M. Dose-reducing fluoroscopic system decreases patient but not occupational radiation exposure in chronic total occlusion intervention. Catheter. Cardiovasc. Interv. 2020, 1–8. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Localization of the Operator’s Crystalline Lens, Area (Raw, Column) | Area (d, 4) | Area (e, 4) | Area (f, 4) | Area (c, 5) | Area (d, 5) | Area (e, 5) | Total Lens Dose Reduction Rate (Total DRRShort) *** |
|---|---|---|---|---|---|---|---|
| Lens presence rate, PR (raw, column) * (n = 20) | 0.015 (1.5%) | 0.049 (4.9%) | 0.113 (11.3%) | 0.183 (18.3%) | 0.581 (58.1%) | 0.058 (5.8%) | |
| Air dose rate without short curtain, A (raw, column) [μGy/min] (n = 3) | 247 | 277 | 291 | 159 | 185 | 200 | |
| Air dose rate with short curtain, B (raw, column) [μGy/min] (n = 3) | 202 | 225 | 234 | 138 | 151 | 161 | |
| Lens dose reduction rate, DRRShort (raw, column) ** | 0.182 (18.2%) | 0.188 (18.8%) | 0.196 (19.6%) | 0.132 (13.2%) | 0.184 (18.4%) | 0.195 (19.5%) | 0.176 (17.6%) |
| Fluorography Procedures Using Over-Table Tube Fluorographic Imaging Unit | Number of Cases * | Collective PKA ** (Gy·m2) | Physician’s Collective HLens | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Without Curtain | With Long Curtain | With Short Curtain | With Best Curtain Available | ||||||
| Collective HLens (Sv) | Adopted Total DRR | Collective HLens (Sv) | Adopted Total DRR | Collective HLens (Sv) | Adopted Total DRR | Collective HLens (Sv) | |||
| Endoscopic retrograde cholangiopancreatography (ERCP) | 188 | 0.483 | 0.483 t | 0.889 | 0.054 t | 0.176 | 0.398 t | 0.889 | 0.054 t |
| Endoscopic injection sclerotherapy (EIS) | 37 | 0.079 | 0.079 t | 0.889 | 0.009 t | 0.176 | 0.065 t | 0.889 | 0.009 t |
| Endoscopic sphincterotomy (EST) | 32 | 0.096 | 0.096 t | 0.889 | 0.011 t | 0.176 | 0.079 t | 0.889 | 0.011 t |
| Endoscopic retrograde biliary drainage (ERBD) | 17 | 0.033 | 0.033 t | 0.889 | 0.004 t | 0.176 | 0.027 t | 0.889 | 0.004 t |
| Upper gastrointestinal series | 171 | 0.776 | 0.776 t | N.A. | 0.776 t | 0.176 | 0.640 t | 0.176 | 0.640 t |
| Barium enema | 143 | 1.210 | 1.210 t | N.A. | 1.210 t | 0.176 | 0.997 t | 0.176 | 0.997 t |
| Nerve root block | 138 | 0.095 | 0.095 t | N.A. | 0.095 t | 0.176 | 0.078 t | 0.176 | 0.078 t |
| Drain tube change | 111 | 0.203 | 0.203 t | N.A. | 0.203 t | 0.176 | 0.167 t | 0.176 | 0.167 t |
| Lumbar myelography | 106 | 0.494 | 0.494 t | N.A. | 0.494 t | 0.176 | 0.407 t | 0.176 | 0.407 t |
| Ileus tube follow-up | 76 | 0.462 | 0.462 t | N.A. | 0.462 t | 0.176 | 0.381 t | 0.176 | 0.381 t |
| Ileus tube insertion | 71 | 0.807 | 0.807 t | N.A. | 0.807 t | 0.176 | 0.665 t | 0.176 | 0.665 t |
| Percutaneous transhepatic cholangiodrainage | 37 | 0.104 | 0.104 t | N.A. | 0.104 t | 0.176 | 0.086 t | 0.176 | 0.086 t |
| Intravenous hyperalimentation catheter insertion | 33 | 0.015 | 0.015 t | N.A. | 0.015 t | 0.176 | 0.013 t | 0.176 | 0.013 t |
| Central venous catheter placement | 32 | 0.030 | 0.030 t | N.A. | 0.030 t | 0.176 | 0.025 t | 0.176 | 0.025 t |
| Percutaneous transhepatic gallbladder drainage | 14 | 0.015 | 0.015 t | N.A. | 0.015 t | 0.176 | 0.012 t | 0.176 | 0.012 t |
| Small bowel radiography | 15 | 0.112 | 0.112 t | N.A. | 0.112 t | 0.176 | 0.092 t | 0.176 | 0.092 t |
| Others | 613 | 1.224 | 1.224 t | N.A. | 1.224 t | 0.176 | 1.009 t | 0.176 | 1.009 t |
| Total | 1834 | 6.239 | 6.239 t | 5.625 t | 5.141 t | 4.649 t | |||
| Collective HLens Reduction Rate (Collective HLens RR) | 0.098 (9.8%) | 0.176 (17.6%) | 0.255 (25.5%) | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakagami, K.; Moritake, T.; Nagamoto, K.; Morota, K.; Matsuzaki, S.; Kuriyama, T.; Kunugita, N. Strategy to Reduce the Collective Equivalent Dose for the Lens of the Physician’s Eye Using Short Radiation Protection Curtains to Prevent Cataracts. Diagnostics 2021, 11, 1415. https://doi.org/10.3390/diagnostics11081415
Nakagami K, Moritake T, Nagamoto K, Morota K, Matsuzaki S, Kuriyama T, Kunugita N. Strategy to Reduce the Collective Equivalent Dose for the Lens of the Physician’s Eye Using Short Radiation Protection Curtains to Prevent Cataracts. Diagnostics. 2021; 11(8):1415. https://doi.org/10.3390/diagnostics11081415
Chicago/Turabian StyleNakagami, Koichi, Takashi Moritake, Keisuke Nagamoto, Koichi Morota, Satoru Matsuzaki, Tomoko Kuriyama, and Naoki Kunugita. 2021. "Strategy to Reduce the Collective Equivalent Dose for the Lens of the Physician’s Eye Using Short Radiation Protection Curtains to Prevent Cataracts" Diagnostics 11, no. 8: 1415. https://doi.org/10.3390/diagnostics11081415