
Evaluation of a Novel Teleradiology Technology for Image-Based Distant Consultations: Applications in Neurosurgery

 and
and
Abstract
:1. Introduction
2. Materials and Methods
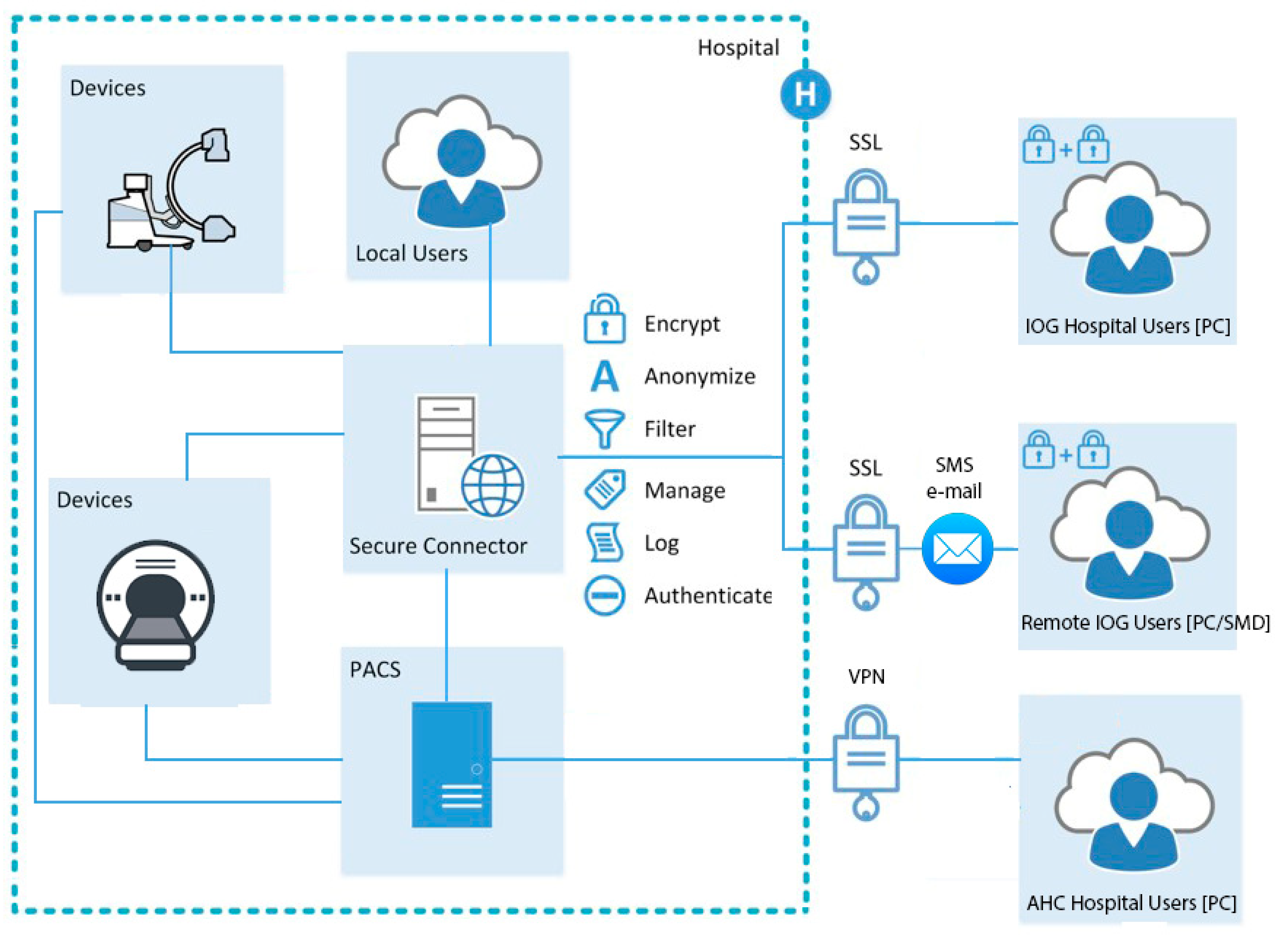
2.1. Basic Characteristics of the Teleradiology Technology
- The cloud segment is installed in AWS’s (Amazon Web Services, Seattle, Washington, USA) HIPAA (Health Insurance Portability and Accountability Act) compliant data center and manages all non-image-related services, like authentication, authorization, security, sharing, integration, APIs, and hosting.
- The on-premise segment is installed locally in the hospital. The main purpose is to authorize user image access to PACS and to send DICOM images directly (no cloud involved) to the user’s web browser, without storing images outside of the hospital.
2.2. Installation and Requirements of the Teleradiology Technology
2.3. Standard Workflows to Access DICOM Datasets
2.4. Hardware for Speed Tests of Standard and Teleradiology Technologies
2.5. Teleradiology Technology Compliance to GDPR and Swedish Regulations
2.6. Workflow Efficacy of the IOG Teleradiology Technology for Standardized Datasets
2.7. Comparison of Access Times for AHC and IOG to Clinical DICOM Datasets
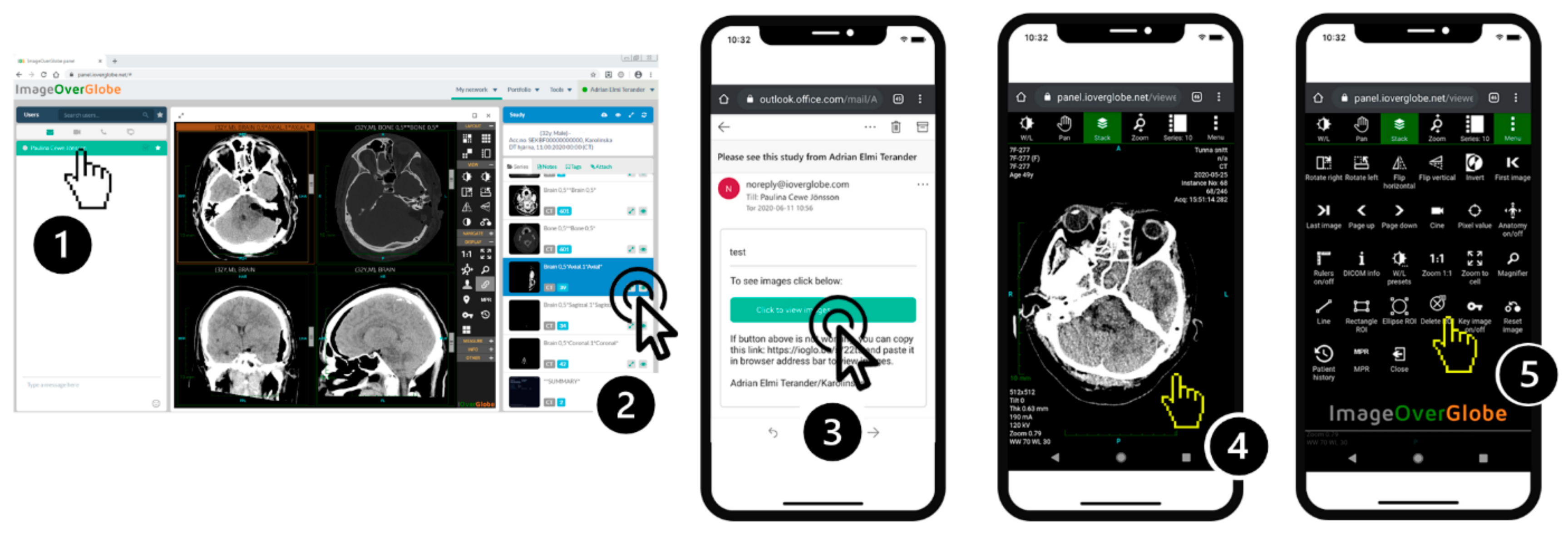
2.8. Accessing Patient DICOM Datasets Using IOG on PC or SMD Per Invitation
2.9. International Consultation Using IOG on PC or SMD
2.10. Statistical Analysis
3. Results
3.1. Subsection Workflow Efficacy Measurements of the IOG Teleradiology Technology
3.2. Clinical Efficacy Measurements of DICOM Dataset Access Using AHC or IOG
3.3. Accessing Patient DICOM Datasets Using IOG on PC or SMD Per Invitation
3.4. International Consultation Using IOG on PC or SMD
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Godinho, T.M.; Viana-Ferreira, C.; Bastião Silva, L.A.; Costa, C. A Routing Mechanism for Cloud Outsourcing of Medical Imaging Repositories. IEEE J. Biomed. Health Inform. 2016, 20, 367–375. [Google Scholar] [CrossRef] [PubMed]
- European Society of Radiology. ESR paper on the proper use of mobile devices in radiology. Insights Imaging 2018, 9, 247–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitchell, J.R.; Sharma, P.; Modi, J.; Simpson, M.; Thomas, M.; Hill, M.D.; Goyal, M. A smartphone client-server teleradiology system for primary diagnosis of acute stroke. J. Med. Internet Res. 2011, 13, e31. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. mHealth: New Horizons for Health through Mobile Technologies; World Health Organization: Geneva, Switzerland, 2011; p. viii+102 p. [Google Scholar]
- Agrawal, J.P.; Erickson, B.J.; Kahn, C.E., Jr. Imaging Informatics: 25 Years of Progress. Yearb. Med. Inform. 2016, 25 (Suppl. 1), S23–S31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laurin, S.; Norberg, K.A. Digital imaging system are rapidly introduced in Swedish departments of radiography. This calls for new strategic planning. Läkartidningen 2000, 97, 4600–4601. [Google Scholar] [PubMed]
- Arenson, R.L.; Andriole, K.P.; Avrin, D.E.; Gould, R.G. Computers in imaging and health care: Now and in the future. J. Digit. Imaging 2000, 13, 145–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mirvis, S.E.; Kubal, W.S.; Shanmuganathan, K.; Soto, J.A.; Yu, J. Problem Solving in Emergency Radiology; Elsevier/Saunders: Philadelphia, PA, USA, 2015; p. 569. [Google Scholar]
- Narenthiranathan, N.R.; Adnan, J.S.; Haspani, M.S. Tailoring teleconsultation to meet the current needs of neurosurgical services: A multimodality oriented neurosurgical consultation. Stud. Health Technol. Inform. 2010, 161, 112–121. [Google Scholar] [PubMed]
- Stormo, A.; Sollid, S.; Størmer, J.; Ingebrigtsen, T. Neurosurgical teleconsultations in northern Norway. J. Telemed. Telecare 2004, 10, 135–139. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.C.; Maeder, A.J. Tailoring teleconsultation. In Global Telehealth: Selected Papers from Global Telehealth 2010 (GT2010): 15th International Conference of the International Society for Telemedicine and EHealth and 1st National Conference of the Australasian Telehealth Society; IOS Press: Amsterdam, The Netherlands, 2010; p. 112. [Google Scholar]
- European Society of Radiology. The new EU General Data Protection Regulation: What the radiologist should know. Insights Imaging 2017, 8, 295–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Services, S.H. Laws and Regulations Stockholms Healthcare Services SLL, Stockholm. 2020. Available online: https://www.slso.sll.se/en/Safeandsecurecare/Lawsandregulations/ (accessed on 1 August 2021).
- Kumar, S.; Krupinski, E.A. Teleradiology; Springer: Berlin/Heidelberg, Germany, 2008; p. 284. [Google Scholar]
- McLaughlin, P.D.; Moloney, F.; O’Neill, S.B.; James, K.; Crush, L.; Flanagan, O.; Maher, M.M.; Wyse, G.; Fanning, N. CT of the head for acute stroke: Diagnostic performance of a tablet computer prior to intravenous thrombolysis. J. Med. Imaging Radiat. Oncol. 2017, 61, 334–338. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, A.; Liu, P.; Cheng, W.C.; Badano, A. Image quality characteristics of handheld display devices for medical imaging. PLoS ONE 2013, 8, e79243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reponen, J.; Ilkko, E.; Jyrkinen, L.; Karhula, V.; Tervonen, O.; Laitinen, J.; Leisti, E.L.; Koivula, A.; Suramo, I. Digital wireless radiology consultations with a portable computer. J. Telemed. Telecare 1998, 4, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Mollura, D.J.; Culp, M.P.; Lungren, M.P. Radiology in Global Health: Strategies, Implementation, and Applications, 2nd ed.; Mobile Strategies for Global Health Radiology; Springer: Cham, Switzerland, 2019; pp. 283–307. [Google Scholar]
- Kammerer, F.J.; Hammon, M.; Schlechtweg, P.M.; Uder, M.; Schwab, S.A. A web based cross-platform application for teleconsultation in radiology. J. Telemed. Telecare 2015, 21, 355–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demaerschalk, B.M.; Vargas, J.E.; Channer, D.D.; Noble, B.N.; Kiernan, T.E.; Gleason, E.A.; Vargas, B.B.; Ingall, T.J.; Aguilar, M.I.; Dodick, D.W.; et al. Smartphone teleradiology application is successfully incorporated into a telestroke network environment. Stroke 2012, 43, 3098–3101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jithoo, R.; Govender, P.; Corr, P.; Nathoo, N. Telemedicine and neurosurgery: Experience of a regional unit based in South Africa. J. Telemed. Telecare 2003, 9, 63–66. [Google Scholar] [CrossRef] [PubMed]
- Ashkenazi, I.; Zeina, A.R.; Kessel, B.; Peleg, K.; Givon, A.; Khashan, T.; Dudkiewicz, M.; Oren, M.; Alfici, R.; Olsha, O. Effect of teleradiology upon pattern of transfer of head injured patients from a rural general hospital to a neurosurgical referral centre: Follow-up study. Emerg. Med. J. 2015, 32, 946–950. [Google Scholar] [CrossRef] [PubMed]
- Lester, N.; Durazzo, T.; Kaye, A.; Ahl, M.; Forman, H.P. Referring physicians’ attitudes toward international interpretation of teleradiology images. AJR Am. J. Roentgenol. 2007, 188, W1–W8. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| AHC User Initiated | IOG PC/SMD User Initiated | IOG PC/SMD Per Invitation | |
|---|---|---|---|
| 1 | Requires predefined user status | Requires predefined user status | Receive SMS or email invitation link |
| 2 | Installed software login | Web application login | Using link bypasses login |
| 3 | Preinstalled VPN provides secure connection | Automatically generated code sent by email/smsCode returned to software for second step authorization | Link bypasses authorization |
| 4 | Query using patient name/ID | Query using patient name/ID | n/a |
| 5 | Accessing DICOM sets on PACS | Accessing DICOM sets on PACS through IOG connector | Accessing DICOM sets on PACS through IOG connector |
| 6 | Images viewed in application | Images viewed in application | Anonymized images viewed in application |
| Series Name | No. of Images/Resolution | Total Original Series Size (MB) | Total Lossless Compressed Series Size (MB) | Total Lossless Compressed Series Size (% of Original Size) | PC Download Speed (Mbps) | SMD Download Speed (Mbps) | PC Median Transfer Time (s) | SMD Median Transfer Time (s) |
|---|---|---|---|---|---|---|---|---|
| “sT2W-FLAIR-401” | 22/288 × 288 | 3.7 | 1.4 | 38% | 88 | 59 | 2 (2–4) | 2 (2–8) |
| “T1-SE-extra-701” | 22/512 × 512 | 12.3 | 4.3 | 35% | 78 | 16 | 4 (2–7) | 3 (2–11) |
| “T1-3D-FFE-C-801” | 100/256 × 256 | 14.2 | 4.9 | 34% | 78 | 16 | 5 (5–6) | 3 (3–8) |
| Distant Consultations | Mean Time (s) | Median Time (s) | p-Value for Comparison to A. |
|---|---|---|---|
| A. Regular hospital PACS using VPN on AHC | 250 ± 10 | 249 (233–274) | |
| Starting computer | 127 ± 7 | 125 (122–135) | |
| Connecting to VPN | 52 ± 9 | 49 (46–65) | |
| Opening PACS and images | 71 ± 6 | 70 (65–77) | |
| B. Senior on call using IOG on PC | 50 ± 8 | 49 (42–60) | p < 0.001 |
| C. Senior on call using IOG on SMD | 39 ± 5 | 38 (33–47) | p < 0.001 |
| D. Using IOG to send access link to senior on call | 68 ± 6 | 69 (59–82) | p < 0.001 |
| Junior on call: starting IOG and opening images | 36 ± 5 | 34 (33–42) | |
| Junior on call: sending access link by SMS to senior on call | 19 ± 6 | 16 (15–25) | |
| Senior on call: image set opened using link on SMD | 13 ± 2 | 12 (11–15) | |
| E. Using IOG for international consultation Iceland-Sweden | n/a | ||
| Providing access link from Iceland to Sweden by email (time from link sent until image viewed on PC) | 23 ± 5 | 21 (16–33) | |
| Providing access link from Iceland to Sweden by SMS (time from access link sent until image viewed on SMD) | 27 ± 1 | 27 (25–29) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cewe, P.; Burström, G.; Drnasin, I.; Ohlsson, M.; Skulason, H.; Vucica, S.; Elmi-Terander, A.; Edström, E. Evaluation of a Novel Teleradiology Technology for Image-Based Distant Consultations: Applications in Neurosurgery. Diagnostics 2021, 11, 1413. https://doi.org/10.3390/diagnostics11081413
Cewe P, Burström G, Drnasin I, Ohlsson M, Skulason H, Vucica S, Elmi-Terander A, Edström E. Evaluation of a Novel Teleradiology Technology for Image-Based Distant Consultations: Applications in Neurosurgery. Diagnostics. 2021; 11(8):1413. https://doi.org/10.3390/diagnostics11081413
Chicago/Turabian StyleCewe, Paulina, Gustav Burström, Ivan Drnasin, Marcus Ohlsson, Halldor Skulason, Stanislav Vucica, Adrian Elmi-Terander, and Erik Edström. 2021. "Evaluation of a Novel Teleradiology Technology for Image-Based Distant Consultations: Applications in Neurosurgery" Diagnostics 11, no. 8: 1413. https://doi.org/10.3390/diagnostics11081413