A Retrospective Comparative Study of Sodium Fluoride (NaF-18)-PET/CT and Fluorocholine (F-18-CH) PET/CT in the Evaluation of Skeletal Metastases in Metastatic Prostate Cancer Using a Volumetric 3-D Radiomics Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.1.1. M Group
2.1.2. N Group
2.2. Imaging PET/CT Protocol
2.3. Image Aanalysis
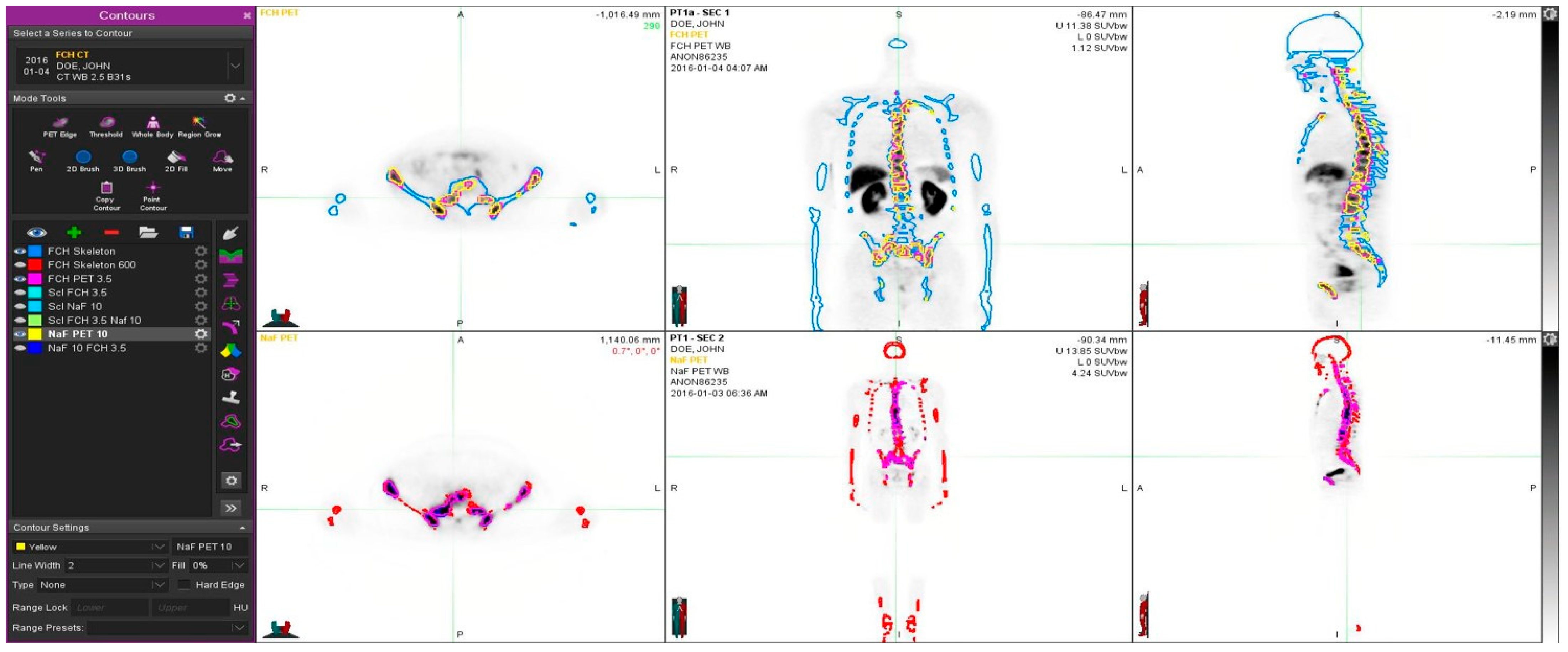
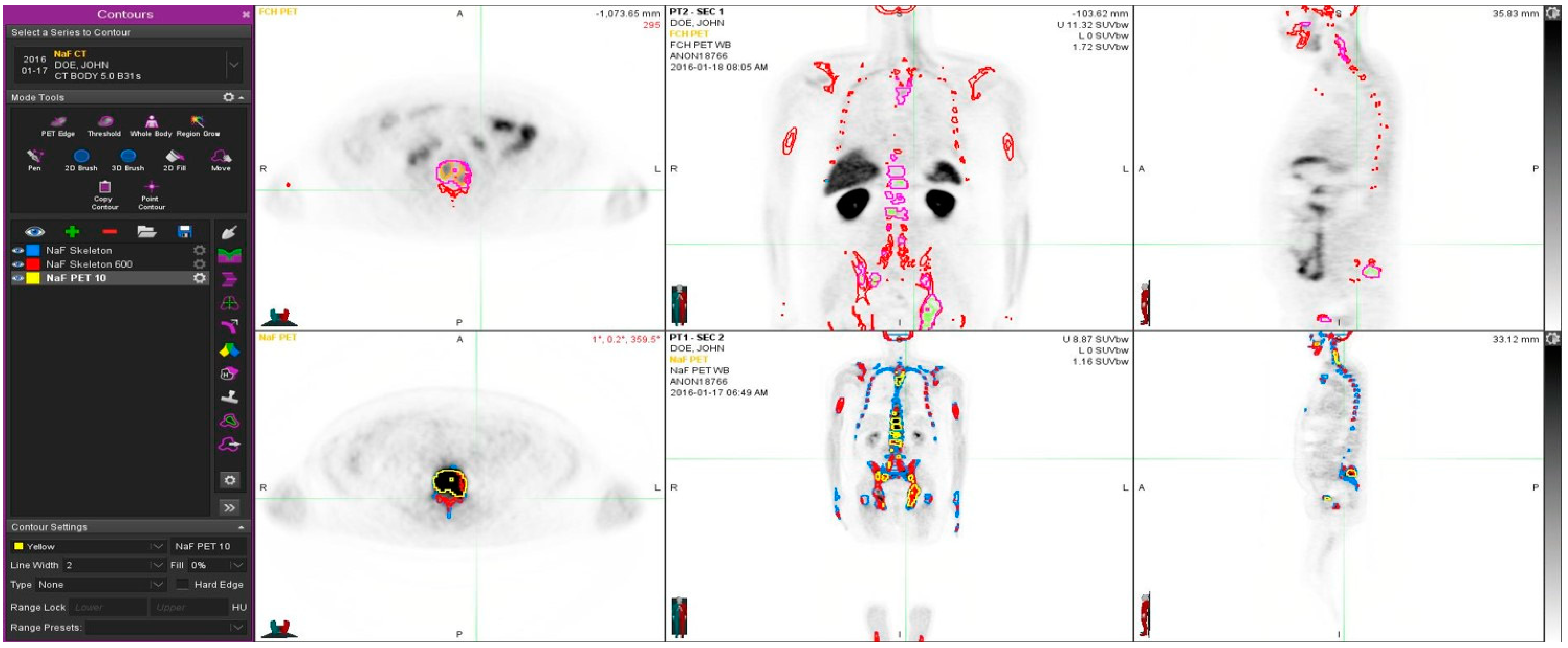
- The skeleton VOI was segmented by selecting voxels with HU > 150 on the CT scans from FCH and NaF PET/CT scans
- A rigid registration of the two skeleton VOIs from FCH PET/CT and NaF PET/CT scans was performed. Now the two PET and CT scans are spatially co-registered in a single frame of reference. The skeleton VOI was labeled as “Skeleton” for figures.
- A subset VOI of sclerotic (pathologic) bone was created by selecting voxels with HU > 600 within the skeleton VOI—labeled as “Skeleton 600”.
- A PET based VOI labeled “FCH PET 3.5” was created that is the fusion of voxels with FCH PET SUVbw > 3.5 and the “Skeleton” VOI.
- A PET based VOI labeled “NaF PET 10” was created that is the fusion of voxels with NaF PET SUVbw > 10 and the “Skeleton” VOI.
- A PET based VOI labeled “NaF 10 FCH 3.5” was the fusion of “FCH PET 3.5” VOI and “NaF PET 10” VOI.
- A PET based VOI labeled “Scl FCH 3.5” was the fusion of “FCH PET 3.5” VOI and “Skeleton 600” VOI.
- A PET based VOI labeled “Scl NaF 10” was the fusion of “NaF PET 10” VOI and “Skeleton 600” VOI.
- A PET based VOI labeled “Scl NaF 10 FCH 3.5” was the fusion of “Scl FCH 3.5” VOI and “Scl NaF 10” VOI.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Alva, A.; Hussain, M. The changing natural history of metastatic prostate cancer. Cancer J. 2013, 19, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Scher, H.I.; Sawyers, C.L. Biology of progressive, castration-resistant prostate cancer: Directed therapies targeting the androgen-receptor signaling axis. J. Clin. Oncol. 2005, 23, 8253–8261. [Google Scholar] [CrossRef] [PubMed]
- Saad, F.; Hotte, S.J. Guidelines for the management of castrate-resistant prostate cancer. Can. Urol. Assoc. J. 2010, 4, 380–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sathiakumar, N.; Delzell, E.; Morrisey, M.A.; Falkson, C.; Yong, M.; Chia, V.; Blackburn, J.; Arora, T.; Kilgore, M.L. Mortality following bone metastasis and skeletal-related events among men with prostate cancer: A population-based analysis of US Medicare beneficiaries, 1999–2006. Prostate Cancer Prostatic Dis. 2011, 14, 177–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lange, P.H.; Vessella, R.L. Mechanisms, hypotheses and questions regarding prostate cancer micrometastases to bone. Cancer Metastasis Rev. 1999, 17, 331–336. [Google Scholar] [CrossRef]
- von Eyben, F.E.; Kairemo, K. Meta-analysis of 11C-choline and 18F-choline PET/CT for management of patients with prostate cancer. Nucl. Med. Commun. 2014, 35, 221–230. [Google Scholar] [CrossRef]
- Segall, G.; Delbeke, D.; Stabin, M.G.; Even-Sapir, E.; Fair, J.; Sajdak, R.; Smith, G.T. SNM practice guideline for sodium 18F-fluoride PET/CT bone scans 1.0. J. Nucl. Med. 2010, 51, 1813–1820. [Google Scholar] [CrossRef] [Green Version]
- von Eyben, F.E.; Kairemo, K.; Kiljunen, T.; Joensuu, T. Planning of External Beam Radiotherapy for Prostate Cancer Guided by PET/CT. Curr. Radiopharm. 2015, 8, 19–31. [Google Scholar] [CrossRef]
- Rohren, E.M.; Etchebehere, E.C.; Araujo, J.C.; Hobbs, B.P.; Swanson, N.M.; Everding, M.; Moody, T.; Macapinlac, A. Determination of Skeletal Tumor Burden on 18F-Fluoride PET/CT. J. Nucl. Med. 2015, 56, 1507–1512. [Google Scholar] [CrossRef] [Green Version]
- Massaro, A.; Ferretti, A.; Secchiero, C.; Cittadin, S.; Milan, E.; Tamiso, L.; Pavan, L.; Tommasi, E.; Marzola, M.C.; Chondrogiannis, S. Optimising 18F-Choline PET/CT Acquisition Protocol in Prostate Cancer Patients. N. Am. J. Med. Sci. 2012, 4, 416–420. [Google Scholar]
- Calabria, F.; Chiaravalloti, A.; Schillaci, O. 18F-choline PET/CT pitfalls in image interpretation: An update on 300 examined patients with prostate cancer. Clin. Nucl. Med. 2014, 39, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Evangelista, L.; Guttilla, A.; Zattoni, F.; Muzzio, P.C.; Zattoni, F. Utility of choline positron emission tomography/computed tomography for lymph node involvement identification in intermediate- to high-risk prostate cancer: A systematic literature review and meta-analysis. Eur. Urol. 2013, 63, 1040–1048. [Google Scholar] [CrossRef] [PubMed]
- Dost, R.J.; Glaudemans, A.W.; Breeuwsma, A.J.; de Jong, I.J. Influence of androgen deprivation therapy on choline PET/CT in recurrent prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2013, 40 (Suppl. 1), S41–S47. [Google Scholar] [CrossRef] [PubMed]
- Fuccio, C.; Schiavina, R.; Castellucci, P.; Rubello, D.; Martorana, G.; Celli, M.; Malizia, C.; Profitos, M.B.; Marzola, M.C.; Pettinato, V.; et al. Androgen deprivation therapy influences the uptake of 11C-choline in patients with recurrent prostate cancer: The preliminary results of a sequential PET/CT study. Eur. J. Nucl. Med. Mol. Imaging 2011, 38, 1985–9198. [Google Scholar] [CrossRef]
- Beheshti, M.; Haim, S.; Zakavi, R.; Steinmair, M.; Waldenberger, P.; Kunit, T.; Nader, M.; Langsteger, W.; Loidl, W. Impact of 18Fcholine PET/CT in prostate cancer patients with biochemical recurrence: Influence of androgen deprivation therapy and correlation with PSA kinetics. J. Nucl. Med. 2013, 54, 833–840. [Google Scholar] [CrossRef] [Green Version]
- Chondrogiannis, S.; Marzola, M.C.; Ferretti, A.; Grassetto, G.; Maffione, A.M.; Rampin, L.; Fanti, S.; Giammarile, F.; Rubello, D. Is the detection rate of 18F-choline PET/CT influenced byandrogen-deprivation therapy? Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 1293–1300. [Google Scholar] [CrossRef]
- Giovacchini, G.; Picchio, M.; Garcia-Parra, R.; Briganti, A.; Abdollah, F.; Gianolli, L.; Schindler, C.; Montorsi, F.; Messa, C.; Fazio, F. 11C-choline PET/CT predicts prostate cancer-specific survival in patients with biochemical failure during androgen deprivation therapy. J. Nucl. Med. 2014, 55, 233–241. [Google Scholar] [CrossRef] [Green Version]
- Reske, S.N.; Moritz, S.; Kull, T. [11C]Choline-PET/CT for outcome prediction of salvage radiotherapy of local relapsing prostate carcinoma. Q. J. Nucl. Med. Mol. Imaging 2012, 56, 430–439. [Google Scholar]
- Zattoni, F.; Agostini, E.; Cattaneo, F.; Maruzzo, M.; Basso, U.; Zattoni, F.; Evangelista, L. Fluorocholine PET/CT predicts skeletal progression, skeletal event and cancer specific survival in patients with biochemical relapse for prostate cancer. Clin. Imaging 2017, 43, 110–116. [Google Scholar] [CrossRef]
- Balogova, S.; Huchet, V.; Egrot, C.; Michaud, L.; Paycha, F.; Kerrou, K.; Montravers, F.; Cussenot, O.; Talbot, J.N. Effect of erythropoietin on bone marrow uptake of 18F-fluorocholine in prostate cancer: Comparison with 18F-fluoride uptake. Clin. Nucl. Med. 2013, 38, 200–202. [Google Scholar] [CrossRef]
- Langsteger, W.; Balogova, S.; Huchet, V.; Beheshti, M.; Paycha, F.; Egrot, C.; Janetschek, G.; Loidl, W.; Nataf, V.; Kerrou, K. Fluorocholine (18F) and sodium fluoride (18F) PET/CT in the detection of prostate cancer: Prospective comparison of diagnostic performance determined by masked reading. Q. J. Nucl. Med. Mol. Imaging 2011, 55, 448–457. [Google Scholar] [PubMed]
- Beheshti, M.; Vali, R.; Waldenberger, P.; Fitz, F.; Nader, M.; Loidl, W.; Broinger, G.; Stoiber, F.; Foglman, I.; Langsteger, W. Detection of bone metastases in patients with prostate cancer by 18F fluorocholine and 18F fluoride PET-CT: A comparative study. Eur. J. Nucl. Med. Mol. Imaging 2008, 35, 1766–1774. [Google Scholar] [CrossRef] [PubMed]
- Kjolhede, H.; Ahlgren, G.; Almquist, H.; Liedberg, F.; Lyttkens, K.; Ohlsson, T.; Bratt, O. Combined 18F-fluorocholine and 18Ffluoride positron emission tomography/computed tomography imaging for staging of high-risk prostate cancer. BJU Int. 2012, 110, 1501–1506. [Google Scholar] [CrossRef] [PubMed]
- Hofman, M.S.; Emmett, L.; Violet, J.; Zhang, A.Y.; Lawrence, N.J.; Stockler, M.; Francis, R.J.; Iravani, A.; Williams, S.; Azad, A.; et al. TheraP: A randomized phase 2 trial of (177) Lu-PSMA-617 theranostic treatment vs cabazitaxel in progressive metastatic castration-resistant prostate cancer (Clinical Trial Protocol ANZUP 1603). BJU Int. 2019, 124 (Suppl. 1), 5–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Even-Sapir, E.; Metser, U.; Mishani, E.; Lievshitz, G.; Lerman, H.; Leibovitch, I. The detection of bone metastases in patients with high-risk prostate cancer: 99mTc-MDP Planar bone scintigraphy, single- and multi-field-of-view SPECT, 18F-fluoride PET, and 18F-fluoride PET/CT. J. Nucl. Med. 2006, 47, 287–297. [Google Scholar] [PubMed]
- Withofs, N.; Grayet, B.; Tancredi, T.; Rorive, A.; Mella, C.; Giacomelli, F.; Mievis, F.; Aerts, J.J.; Waltregny, D.; Jerusalem, G.; et al. 18F-fluoride PET/CT for assessing bone involvement in prostate and breast cancers. Nucl. Med. Commun. 2011, 32, 168–176. [Google Scholar] [CrossRef] [PubMed]
- Kairemo, K.; Macapinlac, H.A. Sodium Fluoride Imaging in Oncology. In Sodium Fluoride PET/CT in Clinical Use; Kairemo, K., Macapinlac, H., Eds.; Springer: Cham, Switzerland, 2019; pp. 19–26. ISBN 978-3-030-23576-5/978-3-030-23577-2. [Google Scholar] [CrossRef]
- Kairemo, K.; Joensuu, T. Radium-223-Dichloride in Castration Resistant Metastatic Prostate Cancer—Preliminary Results of the Response Evaluation Using F-18-Fluoride PET/CT. Diagnostics 2015, 5, 413–427. [Google Scholar] [CrossRef]
- Kairemo, K.; Milton, D.R.; Etchebehere, E.; Rohren, E.M.; Macapinlac, H.A. Final Outcome of 223Ra-therapy and the Role of 18F-fluoride-PET in Response Evaluation in Metastatic Castration-resistant Prostate Cancer—A Single Institution Experience. Curr. Radiopharm. 2018, 11, 147–152. [Google Scholar] [CrossRef]
- Kairemo, K.J.A. PET/Computed Tomography for Radiation Therapy Planning of Prostate Cancer. PET Clin. 2017, 12, 257–267. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Age | GS | TNM | Dgn | iPSA | Previous Treatments | Bone Therapies | PSA at PET-CT |
|---|---|---|---|---|---|---|---|---|
| 1 | 86 | 6 | T1cNxMx | I–04 | 9.8 | TURP, ADT | 204 | |
| 2 | 76 | 8 | T3NxM0 | 400 | Rx, ADT | A, Z | 41 | |
| 3 | 74 | 8 | T3N0M0 | X–11 | 126 | Rx, ADT, Ch | Z, Sm, D | 6.56 |
| 4 | 57 | 10 | T3N0M1 | VII–13 | 790 | Rx, ADT, Ch | Rx, D, Sm, Ra | 52.4 |
| 5 | 85 | 9 | T3bN1M1 | IX–15 | 100 | Rx, ADT | Rx, D | 100 |
| 6 | 63 | 8 | T3NxM1 | IV–13 | 490 | ADT, Ch | D | 29 |
| 7 | 69 | 9 (4 + 5) | T3bN1M1 | III–14 | 86.4 | ADT, Ch | Rx, D | 7.83 |
| 8 | 59 | 7 (3 + 4) | T3bN0M0 | VI–10 | 13 | RRP, ADT, Ch | D | 150 |
| 9 | 76 | 7 (3 + 4) | T2bN0M0 | IV–02 | 16 | RRP, ADT, Ch | D | 390 |
| I | 61 | 7 (3 + 4) | T1cN0M0 | XII–15 | 7.1 | 8 | ||
| 10 | 61 | 8 | T3aN0M1 | XI–15 | 244 | ADT | 244 | |
| 11 | 67 | 9 (4 + 5) | T4N1M1 | XII–15 | 40 | 40 | ||
| II | 70 | 7 (4 + 3) | T3bN0M0 | XII–15 | 17.6 | 17.6 | ||
| III | 70 | 6 | T3bN0M0 | XII–15 | 12.6 | 12.6 | ||
| IV | 93 | 5 | T1cN0M0 | III–99 | 10.5 | ADT | 26 | |
| V | 76 | 7 (4 + 3) | T4N0M0 | XII–15 | 73 | 73 | ||
| 12 | 50 | 9 | T4N1M1 | II–13 | 700 | Rx, ADT, Ch | Rx, D, Sm, Ra | 90.5 |
| FCH-PET (SUV > 3.5) | NaF-PET (SUV > 10) | FCH- & NaF-PET (SUV > 3.5 & > 10) | Sclerosis on CT (HU > 600) | Sclerosis & FCH (HU > 600 & SUV > 3.5) | Sclerosis & NaF (HU > 600 & SUV > 10) | Sclerosis & FCH & NaF (HU > 600 & SUV > 3.5 & > 10) | |
|---|---|---|---|---|---|---|---|
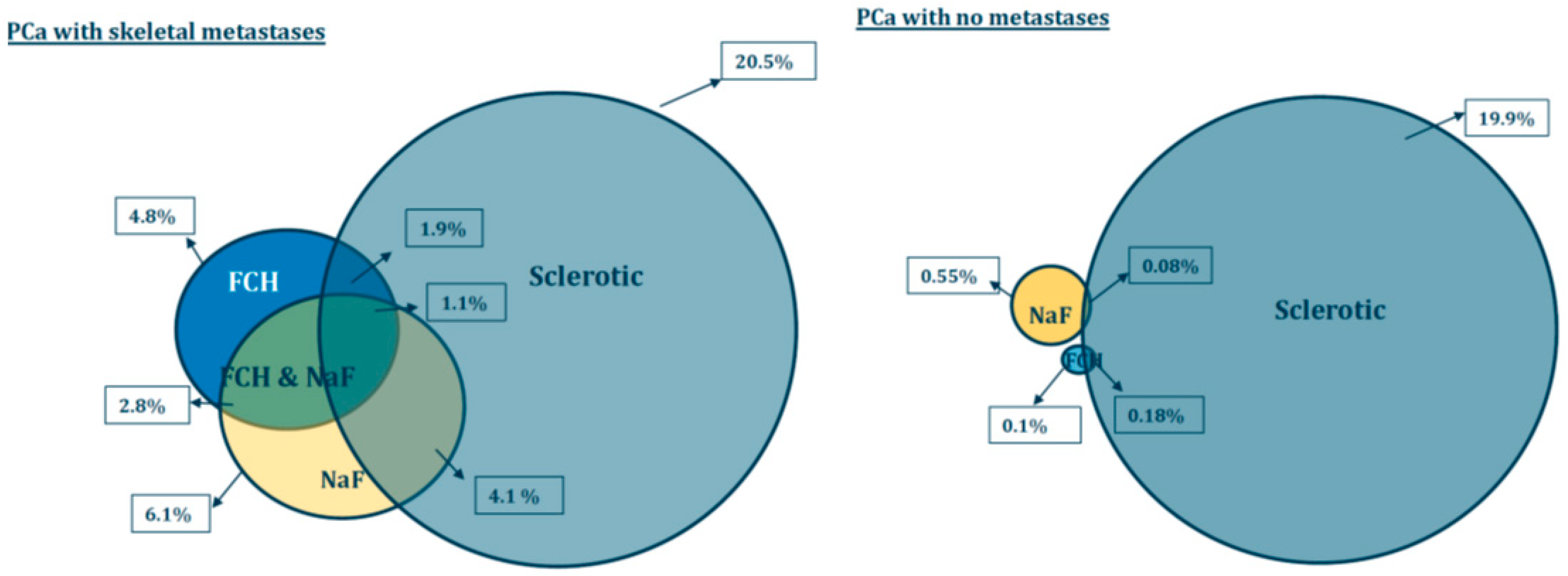
| Skeletal mets (n = 12) | 4.8 ± 5.7% | 6.1 ± 5.5% | 2.8 ± 3.2% | 20.5 ± 6.8% | 1.9 ± 1.7% | 4.1 ± 3.2% | 1.1 ± 1.0% |
| PCa with no mets (n = 5) | 0.11 ± 0.11% | 0.55 ± 0.57% | 0.00 ± 0.00% | 19.9 ± 4.3% | 0.08 ± 0.09% | 0.18 ± 0.19% | 0.00 ± 0.00% |
| p-value | <0.017 | <0.005 | <0.013 | 0.843 | <0.004 | <0.001 | <0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kairemo, K.; Kappadath, S.C.; Joensuu, T.; Macapinlac, H.A. A Retrospective Comparative Study of Sodium Fluoride (NaF-18)-PET/CT and Fluorocholine (F-18-CH) PET/CT in the Evaluation of Skeletal Metastases in Metastatic Prostate Cancer Using a Volumetric 3-D Radiomics Analysis. Diagnostics 2021, 11, 17. https://doi.org/10.3390/diagnostics11010017
Kairemo K, Kappadath SC, Joensuu T, Macapinlac HA. A Retrospective Comparative Study of Sodium Fluoride (NaF-18)-PET/CT and Fluorocholine (F-18-CH) PET/CT in the Evaluation of Skeletal Metastases in Metastatic Prostate Cancer Using a Volumetric 3-D Radiomics Analysis. Diagnostics. 2021; 11(1):17. https://doi.org/10.3390/diagnostics11010017
Chicago/Turabian StyleKairemo, Kalevi, S. Cheenu Kappadath, Timo Joensuu, and Homer A. Macapinlac. 2021. "A Retrospective Comparative Study of Sodium Fluoride (NaF-18)-PET/CT and Fluorocholine (F-18-CH) PET/CT in the Evaluation of Skeletal Metastases in Metastatic Prostate Cancer Using a Volumetric 3-D Radiomics Analysis" Diagnostics 11, no. 1: 17. https://doi.org/10.3390/diagnostics11010017