Assessment of Coagulation Parameters in Women Affected by Endometriosis: Validation Study and Systematic Review of the Literature

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Retrospective Case–Control Study
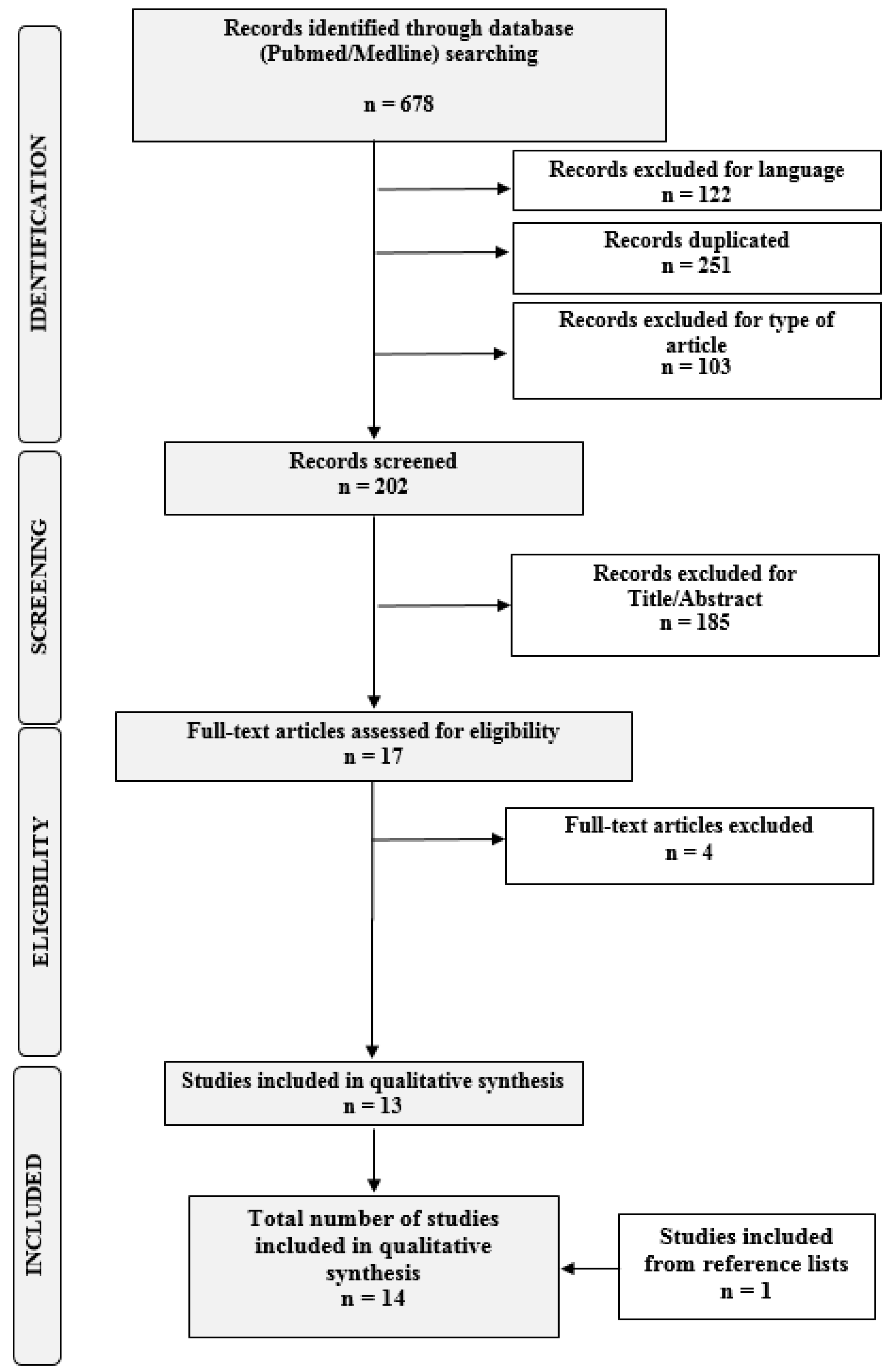
2.2. Systematic Review of the Literature
2.3. Statistical Analysis
3. Results
3.1. Results of the Retrospective Analysis
3.2. Results of the Systematic Review
3.2.1. Coagulation Parameters in Endometriosis Patients
3.2.2. Systemic Inflammatory Markers in Endometriosis Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Vercellini, P.P.; Vigano, P.; Somigliana, E.; Fedele, L. Endometriosis: Pathogenesis and treatment. Nat. Rev. Endocrinol. 2013, 10, 261–275. [Google Scholar] [CrossRef]
- Zondervan, K.; Becker, C.M.; Koga, K.; Missmer, S.A.; Taylor, R.N.; Vigano, P. Endometriosis. Nat. Rev. Dis. Prim. 2018, 4, 9. [Google Scholar] [CrossRef]
- Vigano, P.; Candiani, M.; Monno, A.; Giacomini, E.; Vercellini, P.P.; Somigliana, E. Time to redefine endometriosis including its pro-fibrotic nature. Hum. Reprod. 2018, 33, 347–352. [Google Scholar] [CrossRef]
- Vigano, P.; Ottolina, J.; Bartiromo, L.; Bonavina, G.; Schimberni, M.; Villanacci, R.; Candiani, M. Cellular Components Contributing to Fibrosis in Endometriosis: A Literature Review. J. Minim. Invasive Gynecol. 2020, 27, 287–295. [Google Scholar] [CrossRef]
- Sikora, J.; Mielczarek-Palacz, A.; Kondera-Anasz, Z. Imbalance in Cytokines from Interleukin-1 Family - Role in Pathogenesis of Endometriosis. Am. J. Reprod. Immunol. 2012, 68, 138–145. [Google Scholar] [CrossRef]
- Wickiewicz, D.; Chrobak, A.; Gmyrek, G.B.; Halbersztadt, A.; Gabryś, M.; Goluda, M.; Chełmońska-Soyta, A. Diagnostic accuracy of interleukin-6 levels in peritoneal fluid for detection of endometriosis. Arch. Gynecol. Obstet. 2013, 288, 805–814. [Google Scholar] [CrossRef]
- Birt, J.A.; Nabli, H.; Stilley, J.A.; Windham, E.A.; Frazier, S.R.; Sharpe-Timms, K.L. Elevated Peritoneal Fluid TNF-α Incites Ovarian Early Growth Response Factor 1 Expression and Downstream Protease Mediators. Reprod. Sci. 2013, 20, 514–523. [Google Scholar] [CrossRef] [PubMed]
- Velasco, I.; Acién, P.; Campos, A.; Acién, M.I.; Ruiz-Maciá, E. Interleukin-6 and other soluble factors in peritoneal fluid and endometriomas and their relation to pain and aromatase expression. J. Reprod. Immunol. 2010, 84, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Tokmak, A.; Yildirim, G.; Öztaş, E.; Akar, S.; Erkenekli, K.; Gülşen, P.; Yilmaz, N.; Uğur, M. Use of Neutrophil-to-Lymphocyte Ratio Combined With CA-125 to Distinguish Endometriomas From Other Benign Ovarian Cysts. Reprod. Sci. 2015, 23, 795–802. [Google Scholar] [CrossRef] [PubMed]
- Boss, E.A.; Massuger, L.F.A.G.; Thomas, C.M.; Geurts-Moespot, A.; Van Schaik, J.H.M.; Boonstra, H.; Sweep, F.C.G.J. Clinical value of components of the plasminogen activation system in ovarian cyst fluid. Anticancer. Res. 2002, 22, 275–282. [Google Scholar]
- Esmon, C.T. The interactions between inflammation and coagulation. Br. J. Haematol. 2005, 131, 417–430. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Ding, D.; Liu, X.; Guo, S.-W. Evidence for a Hypercoagulable State in Women With Ovarian Endometriomas. Reprod. Sci. 2015, 22, 1107–1114. [Google Scholar] [CrossRef] [PubMed]
- Chmaj-Wierzchowska, K.; Kampioni, M.; Wilczak, M.; Sajdak, S.; Opala, T. Novel markers in the diagnostics of endometriomas: Urocortin, ghrelin, and leptin or leukocytes, fibrinogen, and CA-125? Taiwan. J. Obstet. Gynecol. 2015, 54, 126–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Also, P.; Ottolina, J.; Sarais, V.; Rebonato, G.; Somigliana, E.; Candiani, M. Coagulation Status in Women With Endometriosis. Reprod. Sci. 2017, 25, 559–565. [Google Scholar] [CrossRef] [Green Version]
- Sanchez, A.M.; Vigano, P.; Somigliana, E.; Panina-Bordignon, P.; Vercellini, P.P.; Candiani, M. The distinguishing cellular and molecular features of the endometriotic ovarian cyst: From pathophysiology to the potential endometrioma-mediated damage to the ovary. Hum. Reprod. Updat. 2013, 20, 217–230. [Google Scholar] [CrossRef] [Green Version]
- Reproductive, A.S.F. Revised American Society for Reproductive Medicine classification of endometriosis: 1996. Fertil. Steril. 1997, 67, 817–821. [Google Scholar] [CrossRef]
- Nisolle, M.; Donnez, J. Peritoneal endometriosis, ovarian endometriosis, and adenomyotic nodules of the rectovaginal septum are three different entities. Fertil. Steril. 1997, 68, 585–596. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- EFSA Scientific Committee; Benford, D.; Halldorsson, T.; Jeger, M.J.; Knutsen, H.K.; More, S.; Naegeli, H.; Noteborn, H.; Ockleford, C.; Ricci, A.; et al. The principles and methods behind EFSA’s Guidance on Uncertainty Analysis in Scientific Assessment. EFSA J. 2018, 16, 5122. [Google Scholar] [CrossRef] [Green Version]
- Vigano, P.; Somigliana, E.; Panina, P.; Rabellotti, E.; Vercellini, P.P.; Candiani, M. Principles of phenomics in endometriosis. Hum. Reprod. Updat. 2012, 18, 248–259. [Google Scholar] [CrossRef]
- World Health Organization Collaborative Study of Cardiovascular Disease and Steroid Hormone Contarception Venous thromboembolic disease and combined oral contraceptives: Results of international multicentre case-control study. Lancet 1995, 346, 1575–1582. [CrossRef]
- Farmer, R.; Lawrenson, R.; Thompson, C.; Kennedy, J.; Hambleton, I.R. Population-based study of risk of venous thromboembolism associated with various oral contraceptives. Lancet 1997, 349, 83–88. [Google Scholar] [CrossRef]
- Cho, S.; Cho, H.; Nam, A.; Kim, H.Y.; Choi, Y.S.; Park, K.H.; Cho, D.J.; Lee, B.S. Neutrophil-to-lymphocyte ratio as an adjunct to CA-125 for the diagnosis of endometriosis. Fertil. Steril. 2008, 90, 2073–2079. [Google Scholar] [CrossRef]
- Yang, H.; Zhu, L.; Wang, S.; Lang, J.; Xu, T. Noninvasive Diagnosis of Moderate to Severe Endometriosis: The Platelet-Lymphocyte Ratio Cannot Be a Neoadjuvant Biomarker for Serum Cancer Antigen 125. J. Minim. Invasive Gynecol. 2015, 22, 373–377. [Google Scholar] [CrossRef] [PubMed]
- Yavuzcan, A.; Caglar, M.; Ustun, Y.; Dilbaz, S.; Ozdemir, I.; Yıldız, E.; Ozkara, A.; Kumru, S. Evaluation of mean platelet volume, neutrophil/lymphocyte ratio and platelet/lymphocyte ratio in advanced stage endometriosis with endometrioma. J. Turk. Gynecol. Assoc. 2013, 14, 210–215. [Google Scholar] [CrossRef]
- Avcioğlu, S.N.; Altinkaya, S.Ö.; Küçük, M.; Demircan-Sezer, S.; Yüksel, H. Can Platelet Indices Be New Biomarkers for Severe Endometriosis? ISRN Obstet. Gynecol. 2014, 2014, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.K.; Park, J.Y.; Jee, B.C.; Suh, C.S.; Kim, S.H. Association of the neutrophil-to-lymphocyte ratio and CA 125 with the endometriosis score. Clin. Exp. Reprod. Med. 2014, 41, 151–157. [Google Scholar] [CrossRef] [Green Version]
- Seckin, B.; Ates, M.C.; Kirbas, A.; Yesilyurt, H. Usefulness of hematological parameters for differential diagnosis of endometriomas in adolescents/young adults and older women. Int. J. Adolesc. Med. Health 2018. [Google Scholar] [CrossRef]
- Ding, D.; Liu, X.; Guo, S.-W. Further Evidence for Hypercoagulability in Women With Ovarian Endometriomas. Reprod. Sci. 2018, 25, 1540–1548. [Google Scholar] [CrossRef]
- Ding, S.; Lin, Q.; Zhu, T.; Li, T.; Zhu, L.; Wang, J.; Zhang, X. Is there a correlation between inflammatory markers and coagulation parameters in women with advanced ovarian endometriosis? BMC Women’s Health 2019, 19, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Turgut, A.; Hocaoglu, M.; Ozdamar, O.; Usta, A.; Gunay, T.; Akdeniz, E. Could hematologic parameters be useful biomarkers for the diagnosis of endometriosis? Bratisl. Med. J. 2019, 120, 912–918. [Google Scholar] [CrossRef] [PubMed]
- Çoşkun, B.; Ince, O.; Erkilinc, S.; Elmas, B.; Saridogan, E.; Çoşkun, B.; Doğanay, M.; Erkılınç, S.; Saridogan, E. The feasibility of the platelet count and mean platelet volume as markers of endometriosis and adenomyosis: A case control study. J. Gynecol. Obstet. Hum. Reprod. 2019, 101626. [Google Scholar] [CrossRef]
- Cassarino, M.F.; Ambrogio, A.G.; Cassarino, A.; Terreni, M.R.; Gentilini, D.; Sesta, A.; Cavagnini, F.; Losa, M.; Giraldi, F.P. Gene expression profiling in human corticotroph tumours reveals distinct, neuroendocrine profiles. J. Neuroendocr. 2018, 30, e12628. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, A.M.; Somigliana, E.; Vercellini, P.; Pagliardini, L.; Candiani, M.; Viganò, P. Endometriosis as a detrimental condition for granulosa cell steroidogenesis and development: From molecular alterations to clinical impact. J. Steroid Biochem. Mol. Biol. 2016, 155, 35–46. [Google Scholar] [CrossRef] [PubMed]
- Krikun, G.; Lockwood, C.J.; Paidas, M.J. Tissue factor and the endometrium: From physiology to pathology. Thromb. Res. 2009, 124, 393–396. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.; Weng, H.; Wang, X.; Zhou, B.; Yu, P.; Wang, Y. The role of tissue factor and protease-activated receptor 2 in endometriosis. Am. J. Reprod. Immunol. 2012, 68, 251–257. [Google Scholar] [CrossRef]
- Osuga, Y. Proteinase-activated receptors in the endometrium and endometriosis. Front. Biosci. 2012, 4, 1201–1212. [Google Scholar] [CrossRef] [Green Version]
- Senthil, M.; Chaudhary, P.; Smith, D.; Ventura, P.E.; Frankel, P.H.; Pullarkat, V.; Trisal, V. A shortened activated partial thromboplastin time predicts the risk of catheter-associated venous thrombosis in cancer patients. Thromb. Res. 2014, 134, 165–168. [Google Scholar] [CrossRef]
- Mina, A.; Favaloro, E.J.; Koutts, J. Relationship between short activated partial thromboplastin times, thrombin generation, procoagulant factors and procoagulant phospholipid activity. Blood Coagul. Fibrinolysis 2012, 23, 203–207. [Google Scholar] [CrossRef]
- Guo, S.-W.; Ding, D.; Geng, J.-G.; Wang, L.; Liu, X. P-selectin as a potential therapeutic target for endometriosis. Fertil. Steril. 2015, 103, 990–1000.e8. [Google Scholar] [CrossRef]
- Zhang, Q.; Duan, J.; Olson, M.; Fazleabas, A.T.; Guo, S.-W. Cellular Changes Consistent With Epithelial–Mesenchymal Transition and Fibroblast-to-Myofibroblast Transdifferentiation in the Progression of Experimental Endometriosis in Baboons. Reprod. Sci. 2016, 23, 1409–1421. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Duan, J.; Liu, X.; Guo, S.-W. Platelets drive smooth muscle metaplasia and fibrogenesis in endometriosis through epithelial–mesenchymal transition and fibroblast-to-myofibroblast transdifferentiation. Mol. Cell. Endocrinol. 2016, 428, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Guo, S.-W.; Du, Y.; Liu, X. Endometriosis-Derived Stromal Cells Secrete Thrombin and Thromboxane A2, Inducing Platelet Activation. Reprod. Sci. 2016, 23, 1044–1052. [Google Scholar] [CrossRef] [PubMed]
- Ding, D.; Liu, X.; Duan, J.; Guo, S.-W. Platelets are an unindicted culprit in the development of endometriosis: Clinical and experimental evidence. Hum. Reprod. 2015, 30, 812–832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mikhailidis, D.P.; Barradas, M.A.; Maris, A.; Jeremy, J.Y.; Dandona, P. Fibrinogen mediated activation of platelet aggregation and thromboxane A2 release: Pathological implications in vascular disease. J. Clin. Pathol. 1985, 38, 1166–1171. [Google Scholar] [CrossRef]
- Kvaskoff, M.; Mu, F.; Terry, K.L.; Harris, H.R.; Poole, E.M.; Farland, L.V.; Missmer, S.A. Endometriosis: A high-risk population for major chronic diseases? Hum. Reprod. Updat. 2015, 21, 500–516. [Google Scholar] [CrossRef] [Green Version]
- Zuin, M.; Rigatelli, G.; Stellin, G.; Faggian, G.; Roncon, L. Should women with endometriosis be screened for coronary artery disease? Eur. J. Intern. Med. 2016, 35, e19–e20. [Google Scholar] [CrossRef]
- Sugiura-Ogasawara, M.; Ebara, T.; Matsuki, T.; Yamada, Y.; Omori, T.; Matsumoto, Y.; Kato, S.; Kano, H.; Kurihara, T.; Saitoh, S.; et al. Endometriosis and Recurrent Pregnancy Loss as New Risk Factors for Venous Thromboembolism during Pregnancy and Post-Partum: The JECS Birth Cohort. Thromb. Haemost. 2019, 119, 606–617. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Baseline Characteristics | Endometriosis Group (n = 324) | Control Group (n = 248) | p-Value |
|---|---|---|---|
| Age (years) | 33.53 ± 5.51 | 31.15 ± 7.9 | 0.001 |
| BMI (kg/m2) | 21.37 ± 3.9 | 22.29 ± 4.0 | 0.028 |
| Smoking habit | 28 (14.7%) | 35 (18.3%) | 0.09 |
| Indication for surgery | |||
| Symptoms | 174 (55.4%) | 69 (29%) | |
| Offspring desire | 113 (36%) | 56 (23.5%) | 0.001 |
| Occasional findings | 12 (3.8%) | 104 (43.7%) | |
| Symptoms and offspring desire | 15 (4.8%) | 8 (3.4%) | |
| Prophylactic surgery | 1 (0.4%) | ||
| HT before surgery | 128 (39.5%) | 64 (25.8%) | 0.43 |
| Previous pelvic surgery | 82 (25.9%) | 85 (34.6%) | 0.027 |
| Diagnosis | L (109/L) | N (109/L) | NLR |
|---|---|---|---|
| Endometriosis (n = 324) | 2.05 ± 0.53 | 4.30 ± 1.51 | 2.21 ± 0.95 |
| Controls (n = 248) | 2.12 ± 0.55 | 4.03 ± 1.57 | 2.05 ± 1.50 |
| p = 0.13 | p = 0.038 | p = 0.13 | |
| OMA (n = 214) | 2.01 ± 0.52 | 4.32 ± 1.51 | 2.27 ± 0.97 |
| DIE (n = 69) | 2.19 ± 0.64 | 4.36 ± 1.51 | 2.12 ± 0.95 |
| SPE (n = 41) | 2.04 ± 0.56 | 4.08 ± 1.55 | 2.04 ± 0.78 |
| Controls (n = 248) | 2.12 ± 0.55 | 4.03 ± 1.57 | 2.05 ± 1.50 |
| p = 0.049 | p = 0.15 | p = 0.27 | |
| Stage I–II (n = 85) | 2.16 ± 0.56 | 4.29 ± 1.49 | 2.06 ± 0.81 |
| Stage III–IV (n = 239) | 2.01 ± 0.52 | 4.30 ± 1.52 | 2.25 ± 0.99 |
| Controls (n = 248) | 2.12 ± 0.55 | 4.03 ± 1.57 | 2.05 ± 1.50 |
| p = 0.032 | p = 0.11 | p = 0.15 |
| Diagnosis | PT Ratio | aPTT Ratio | INR | PLC (109/L) | L (109/L) | N (109/L) | NLR | PLR |
|---|---|---|---|---|---|---|---|---|
| OMA (n = 118) | 1.05 ± 0.06 | 1.01 ± 0.07 | 1.06 ± 0.07 | 253.5 ± 62.0 | 1.93 ± 0.49 | 3.99 ± 1.48 | 2.18 ± 1.03 | 69.81 ± 25.6 |
| DIE (n = 28) | 1.05 ± 0.06 | 1.05 ± 0.08 | 1.05 ± 0.07 | 268.7 ± 73.0 | 2.29 ± 0.64 | 3.96 ± 1.27 | 1.79 ± 0.60 | 72.43 ± 22.7 |
| SPE (n = 17) | 1.07 ± 0.09 | 1.04 ± 0.07 | 1.07 ± 0.12 | 254.5 ± 53.1 | 1.97 ± 0.33 | 3.51 ± 1.26 | 1.80 ± 0.63 | 81.43 ± 33.0 |
| Controls (n = 96) | 1.05 ± 0.06 | 1.03 ± 0.06 | 1.06 ± 0.06 | 249.4 ± 50.2 | 2.11 ± 0.49 | 3.99 ± 1.57 | 1.99 ± 0.96 | 72.93 ± 37.6 |
| p = 0.61 | p = 0.049 | p = 0.59 | p = 0.50 | p = 0.003 b | p = 0.64 | p = 0.117 | p = 0.52 | |
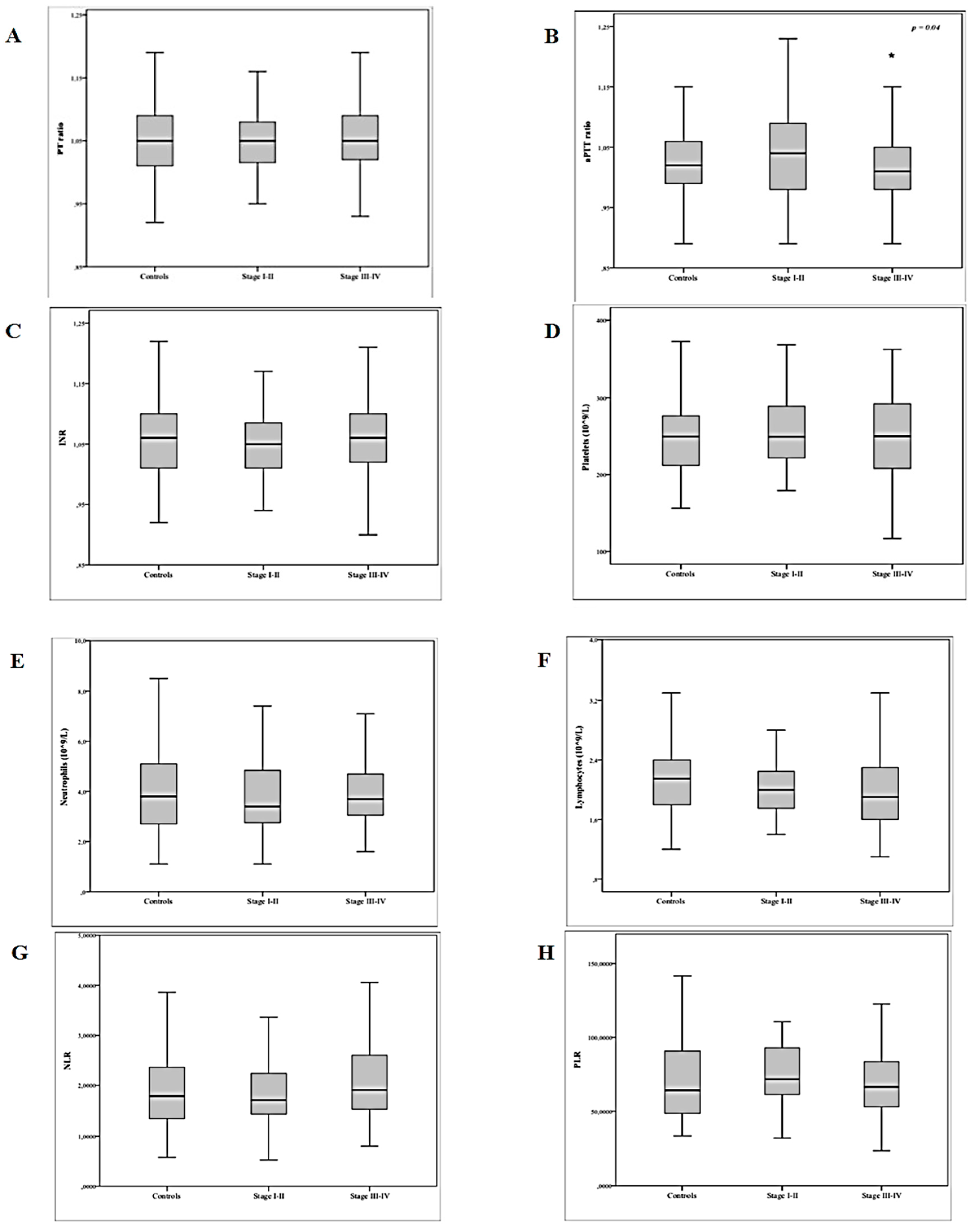
| Stage I–II (n = 35) | 1.06 ± 0.08 | 1.05 ± 0.08 | 1.06 ± 0.09 | 262.3 ± 64.7 | 2.12 ± 0.59 | 3.77 ± 1.36 | 1.83 ± 0.62 | 76.55 ± 27.4 |
| Stage III–IV (n = 128) | 1.02 ± 0.07 | 1.01 ± 0.07 | 1.06 ± 0.06 | 254.6 ± 62.8 | 1.97 ± 0.49 | 3.98 ± 1.45 | 2.14 ± 1.01 | 70.09 ± 25.6 |
| Controls (n = 96) | 1.05 ± 0.06 | 1.03 ± 0.06 | 1.06 ± 0.06 | 249.4 ± 50.2 | 2.11 ± 0.49 | 3.99 ± 1.57 | 1.99 ± 0.96 | 72.93 ± 37.6 |
| p = 0.78 | p = 0.040 b | p = 0.82 | p = 0.53 | p = 0.07 | p = 0.73 | p = 0.18 | p = 0.51 |
| Variable | B Coefficient | SE | OR | p-Value |
|---|---|---|---|---|
| PT ratio | −4.084 | 12.301 | 0.74 | |
| aPTT ratio | −6.091 | 2.695 | 0.002 | 0.024 |
| INR | 3.611 | 11.279 | 0.75 | |
| PLC (109/L) | 0.000 | 0.006 | 0.95 | |
| L (109/L) | −0.587 | 0.728 | 0.42 | |
| N (109/L) | 0.645 | 1.355 | 0.63 | |
| NLR | 1.342 | 1.402 | 0.34 | |
| PLR | −0.007 | 0.018 | 0.71 |
| Author, Years | Country | Study Design | Study Period | Cases/Controls Sample Size (n) | Age (Years) | Parameters Assessed (When) | Confounding Factors |
|---|---|---|---|---|---|---|---|
| Cho et al., 2008 [23] | South Korea | Retrospective case–control study | 01/2004 12/2007 | Endometriosis 1 (231)/ Benign ovarian cysts 1 (231) Healthy women 2 (384) | 33.3 ± 7.3 * (Overall) 32.6 ± 7.35 * (endometriosis) 34.2 ± 8.9 * (benign ovarian cyst) 33.9 ± 5.7 * (healthy women) | Complete blood cell count, NLR, and CA125 (before surgery or as part of routine health examination 3) | Unclear |
| Yavuzcan et al., 2013 [25] | Turkey | Retrospective case–control study | 11/2009 02/2013 | Endometriosis 1 stage III/IV (61) - 33 with OMA - 28 non-OMA/Tubal ligation 1 (33) | 36.21 ± 8.37 * (Overall) | Complete blood cell count, NLR, PLR, and CA125 (before surgery 3) | No |
| Avcioğlu et al., 2014 [26] | Turkey | Retrospective study | 01/2001 06/2013 | Endometriosi 1 stage III/IV (124)/Endometriosis 1 stage I/II (40) | 33.7 ± 7.7 * (Overall) | Complete blood cell count, MPV, PDW, and PCT (before surgery 3) | No |
| Kim et al., 2014 [27] | South Korea | Retrospective study | 04/2005 03/2013 | Endometriosis 1 stage III (189)/Endometriosis 1 stage IV (230) | 15–51 (Overall) 19–49 - 33.8 ± 6.8 * (stage III) 15–51 - 34.7 ± 7.0 * (stage IV) | Complete blood cell count, NLR, CRP, AMH, CEA, CA125, CA 19-9 (<1 month before surgery) | No |
| Chmaj-Wierzchowska et al., 2015 [13] | Poland | Hospital-based case–control | 09/2009 11/2012 | OMA 1 without coexisting foci of peritoneal endometriosis (48)/Mature teratomas 1 (38) | 18–38 (Overall) 30.00 ± 4.6 * (OMA) 27.03 ± 4.52 * (teratomas) | Complete blood cell count, fibrinogen, urocortin, ghrelin, and leptin (<1 day before surgery) | No |
| Yang et al., 2015 [24] | China | Retrospective case–control study | 01/2009 06/2012 4 | Endometriosis 1 - 119 Stage III - 78 Stage IV/ Benign ovarian cysts 1 (102) Healthy women 2 (112) | 32.58 ± 6.37 * (Overall) 32.17 ± 6.50 * (endometriosis) 32.03 ± 6.83 * (benign ovarian cyst) 33.81 ± 5.52 * (healthy women) | Complete blood cell count, PLR, and CA125 (before surgery or as part of routine health examination 3) | Unclear |
| Wu et al., 2015 [12] | China | Hospital-based case–control | 06-12/2012 | OMA 1 (50) -35 stage III −15 stage IV/Age-matched healthy women 2 (50) | 23–44 – 32.9 ± 6.1 * (OMA) 20–48 – 31.4 ± 6.4 * (controls) | Complete blood cell count, aPTT, PT, TT, INR, fibrinogen, D-dimer, fasting serum glucose, and serum cortisol (before surgery 3) | Yes |
| Tokmak et al., 2016 [9] | Turkey | Retrospective case–control study | 01/2008 01/2013 | OMA 1(467)/Age- and BMI-matched benign ovarian cysts 1 (340) | 16–50 (Overall) 18–49 – 33.7 ± 8.4 * (OMA) 16–50 - 33.9 ± 11.6 * (Controls) | Complete blood cell count, NLR, PLR, CA125, AFP, CA 19-9, CA-15.3 (<1 month before surgery) | Unclear |
| Ding et al., 2018 [14] | China | Cross-sectional study | 04/2015 03/2016 | OMA 1(100)/ Women without endometriosis (100): - 60 Healthy women 2 - 40 CINIII or ovarian teratoma 1 | 21–49 (Overall) 32.0 ± 7.1 * (OMA) 33.0 ± 7.1 * (controls) | PLC, platelet activation rate, maximum platelet aggregation rate, D-dimer, fibrinogen, FDPs, sP-sel, F1 + 2, PT; TT; aPTT, INR (before surgery 3 and 3 months later only in OMA) | Unclear |
| Seckin et al., 2018 [28] | Turkey | Retrospective case–control study | 01/2013 12/2016 | OMA 1 (267)/ Benign ovarian cysts 1 (235) | 15–49 – 27.1 ± 7.2 * (overall) 28.3 ± 6.6 * (cases) 25.8 ± 7.6 * (controls) | Complete blood cell count, NLR, PCT, PDW, PLR, and CA125 (before surgery 3) | Yes (only age </> 25 years) |
| Viganò et al., 2018 [14] | Italy | Retrospective case–control study | 01/2013 12/2015 | Endometriosis 1 (169) - 45 Stage I–II - 124 Stage III–IV/ Benign gynecologic pathology 1 (145) | 35.8 ± 5.9 * (endometriosis) 36.9 ± 6.5 * (controls) | Complete blood cell count, NLR, PLR, TT ratio, aPTT, and INR (<1 month before surgery) | Yes |
| Coskun et al., 2019 [32] | Turkey | Retrospective case–control study | 01/2013 01/2015 | Adenomyosis 1 (84) Endometriosis 1 (102)/ Tubal ligation 1 (88) | 52.9 ±7.4 * (adenomyosis) 35.3 ± 8.7 * (OMA) 37.9 ± 4.2 * (Controls) | Complete blood cell count, MPV, and CA125 (<1 week before the surgery) | Unclear |
| Ding et al., 2019 [30] | China | Retrospective case–control study | 06/2015 06/2017 | OMA 1 (226)/ Cyst group 1 (210) Tubal reanastomosis 1 (112) | 35.7 ± 0.4 * (OMA) 35.9 ± 0.4 * (Cyst group) 35.8 ± 0.5 * (Controls) | Complete blood cell count, TT, PT, fibrinogen, CRP, PLR, NLR, aPTT, and CA125 (<1 month before surgery) | Yes |
| Turgut et al., 2019 [31] | Turkey | Retrospective case–control study | 01/2012 02/2017 | Endometriosis 1 (121) - 17 Stage I–II - 104 Stage III–IV/ Healthy women 2 (136) | 22–53 (endometriosis) 17–51 (controls) | Complete blood cell count, MPV, and CA125 (before surgery 3) | Yes (age) |
| Author | Year | Study Population (n) | PT | TT | aPTT | PLC (109/L) | INR |
|---|---|---|---|---|---|---|---|
| Yavuzcan et al. [25] | 2013 | Cases (OMA): 33 | 269.8 ± 65.2 | ||||
| Cases (non-OMA): 28 | 298.9 ± 107.8 | ||||||
| Controls: 33 | 286.4 ± 67.6 | ||||||
| Avcioğlu et al. [26] | 2014 | Stage I–II: 40 | 187 ± 36.18 * | ||||
| Stage III–IV: 124 | 309.15 ± 54.43 * | ||||||
| Kim et al. [27] | 2014 | Stage III (OMA): 189 | NR | ||||
| Stage IV (OMA): 230 | NR | ||||||
| Wu et al. [12] | 2015 | Cases (OMA): 50 | NR | NR * | NR * | NR | NR |
| Controls: 50 | NR | NR * | NR * | NR | NR | ||
| Chmaj-Wierzchowska et al. [13] | 2015 | Cases (OMA): 48 | 267.80 | ||||
| Controls: 38 | 258.90 | ||||||
| Yang et al. [24] | 2015 | Cases: 197 | 253.25 ± 59.98 | ||||
| Benign tumor: 102 | 248.83 ± 61.69 | ||||||
| Controls: 112 | 246.47 ± 52.55 | ||||||
| Tokmak et al. [9] | 2016 | Cases (OMA): 467 | 275.9 ± 72.1 | ||||
| Controls: 340 | 276.2 ± 71.3 | ||||||
| Seckin et al. [28] | 2018 | Cases (OMA): 267 | 292.9 ± 67.6 * | ||||
| Controls: 235 | 269.7 ± 61.3 * | ||||||
| Viganò et al. [14] | 2018 | Cases: 169 | 1.00 ± 0.9 | 1.12 ± 0.19 * | 250.00 ± 55.8 | 0.99 ± 056 | |
| Controls: 145 | 0.970 ± 0.10 | 1.13 ± 0.15 * | 262.20 ± 63.4 | 0.98 ± 0.16 | |||
| Cases (OMA): 98 | 0.99 ± 0.06 | 1.08 ± 0.07 * | 254.5 ± 61.47 | 0.99 ± 0.71 | |||
| Controls: 145 | 0.99 ± 0.09 | 1.14 ± 0.07 * | 254.7 ± 58.62 | 0.99 ± 0.11 | |||
| Ding et al. [29] | 2018 | Cases (OMA): 100 | NR | NR * | NR | NR | NR |
| Controls: 100 | NR | NR * | NR | NR | NR | ||
| Post-surgery (OMA): 100 | NR * | NR * | NR * | NR * | NR * | ||
| Turgut et al. [31] | 2019 | Cases: 121 | 265 ± 86 | ||||
| Controls: 136 | 258 ± 70.5 | ||||||
| Ding et al. [30] | 2019 | Cases (OMA): 226 | 12.69 ± 0.04 * | 15.42 ± 0.04 * | NR | 239.8 ± 3.6 * | |
| Controls: 112 | 12.99 ± 0.06 * | 15.78 ± 0.06 * | NR | 220.0 ± 5.4 * | |||
| Benign cyst: 210 | 13.00 ± 0.04 * | 15.68 ± 0.05 * | NR | 228.4 ± 4.0 * | |||
| Stage III (OMA): 91 | 12.64 ± 0.06 | 15.38 ± 0.06 | 35.68 ± 0.30 | 243.8 ± 5.4 * | |||
| Stage IV (OMA): 135 | 12.72 ± 0.05 | 15.44 ± 0.05 | 35.44 ± 0.26 | 237.1 ± 4.7 * | |||
| Coskun et al. [32] | 2019 | Cases: 102 | 292.9 ± 73.9 * | ||||
| Adenomyosis: 84 | 295.1 ± 77.5 | ||||||
| Controls: 88 | 269.9 ± 59 * |
| Author | Year | Study Population (n) | Neutrophils 109/L | Lymphocytes 109/L | NLR | PLR |
|---|---|---|---|---|---|---|
| Cho et al. [23] | 2008 | Cases: 231 | 4.41 * | 1.82 * | 2.66 * | |
| Benign tumor: 145 | 4.17 * | 1.96 * | 2.31 * | |||
| Controls: 384 | 3.6 * | 1.95 * | 1.99 * | |||
| Yavuzcan et al. [25] | 2013 | Cases (OMA): 33 | 4.14 ± 1.73 | 2.12 ± 0.87 | 2.40 ± 2.04 | 162.84 ± 141.28 |
| Cases (non-OMA): 28 | 4.68 ± 2.18 | 2.02 ± 0.68 | 2.51 ± 1.37 | 159.14 ± 61.20 | ||
| Controls:33 | 4.50 ± 1.57 | 2.25 ± 0.66 | 2.11 ± 0.86 | 132.45 ± 35.74 | ||
| Kim et al. [27] | 2014 | Stage III (OMA): 189 | NR | NR | ||
| Stage IV (OMA):230 | NR | NR | ||||
| Yang et al. [24] | 2015 | Cases: 197 | 1.91 ± 0.52 | 141.79 ± 51.78 * | ||
| Benign tumor:102 | 2.02 ± 0.52 | 129.28 ± 39.20 * | ||||
| Controls: 112 | 2.05 ± 0.49 | 126.68 ± 39.67 * | ||||
| Tokmak et al. [9] | 2016 | Cases (OMA): 467 | 4.8 ± 1.8 * | 1.98 ± 5.92 * | 2.8 ± 2.0 * | 153.3 ± 71.3 * |
| Controls: 340 | 3.8 ± 1.2 * | 2.41 ± 7.17 * | 1.7 ± 0.5 * | 122.4 ± 42.7 * | ||
| Viganò et al. [14] | 2018 | Cases: 169 | 3.76 ± 1.34 | 2.04 ± 0.56 | NR | NR |
| Cases (OMA): 98 | 3.9 ± 1.62 | 2.02 ± 0.66 | 2.08 ± 1.01 | 135.18 ± 68.69 | ||
| Controls:145 | 3.99 ± 1.6 | 1.97 ± 0.55 | 2.16 ± 1.25 | 130.65 ± 52.8 | ||
| Seckin et al. [28] | 2018 | Cases: 267 | 4.6 ± 1.8 | 2.2 ± 0.6 | 2.3 ± 1.3 | 142.3 ± 48.4 * |
| Controls:235 | 4.5 ± 2.1 | 2.2 ± 0.7 | 2.1 ± 1.2 | 129.3 ± 40.4 * | ||
| Turgut et al. [31] | 2019 | Cases: 121 | 4.4 ± 1.9 * | 2 ± 0.8 * | 2.18 ± 0.86 * | |
| Controls:136 | 3.55 ± 1.53 * | 2.15 ± 0.8 * | 1.70 ± 0.8 * | |||
| Ding et al. [30] | 2019 | Cases: 226 (OMA) | 2.56 ± 0.07 * | 146.4 ± 2.8 * | ||
| Benign cyst: 210 | 2.34 ± 0.07 * | 137.7 ± 3.4 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ottolina, J.; Bartiromo, L.; Dolci, C.; Salmeri, N.; Schimberni, M.; Villanacci, R.; Viganò, P.; Candiani, M. Assessment of Coagulation Parameters in Women Affected by Endometriosis: Validation Study and Systematic Review of the Literature. Diagnostics 2020, 10, 567. https://doi.org/10.3390/diagnostics10080567
Ottolina J, Bartiromo L, Dolci C, Salmeri N, Schimberni M, Villanacci R, Viganò P, Candiani M. Assessment of Coagulation Parameters in Women Affected by Endometriosis: Validation Study and Systematic Review of the Literature. Diagnostics. 2020; 10(8):567. https://doi.org/10.3390/diagnostics10080567
Chicago/Turabian StyleOttolina, Jessica, Ludovica Bartiromo, Carolina Dolci, Noemi Salmeri, Matteo Schimberni, Roberta Villanacci, Paola Viganò, and Massimo Candiani. 2020. "Assessment of Coagulation Parameters in Women Affected by Endometriosis: Validation Study and Systematic Review of the Literature" Diagnostics 10, no. 8: 567. https://doi.org/10.3390/diagnostics10080567